Analysis of hospital infection data: dynamics, inference, policy, and future directions. Ben Cooper
advertisement

Analysis of hospital infection
data: dynamics, inference,
policy, and future directions.
Ben Cooper
Centre for Clinical Vaccinology and Tropical Medicine, Nuffield Dept. of Clinical Medicine,
University of Oxford
Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol
University, Bangkok, Thailand
Dynamics
Inference
1. Dynamics of healthcare associated
infections (HCAIs)
2. Inference for models of HCAIs
3. Policy evaluation
4. The future
Policy
Future
Dynamics
x
C*P1*xv
uncolonized
u
uncolonized
Inference
Policy
Future
y
colonized
C*P2*u
handwash
v
colonized
Estimated IRR for MRSA
bacteraemia for a 1 ml per bed
day increase in alchohol hand
rub by quarter
Cooper et al. J Hosp Infect 1999
Austin et al. PNAS 1999
Sébille et al. ICHE 1997
Ross Proc R Soc Lon 1916
Dynamics
Inference
Policy
Cooper et al. PNAS 2004
Smith et al. PNAS 2004
Bootsma et al. PNAS 2006
Future
Dynamics
Inference
Insights from “data free” models
1. Stochastic effects dominant
2. Resistance levels change quickly in response to changes in drug use
and resistance can disappear quickly after a drug is discontinued or in
response to other interventions (if resistance is rare in the community).
3. Non-specific control (e.g. hand hygiene) disproportionately reduces
resistance (if resistance is rare in the community).
4. Long-term dynamics can be driven by a build-up of resistance in the
community reservoir.
5. Long-term control failure is possible, even when all outbreaks are
controlled successfully in the short-term.
Grundmann & Hellriegel, Lancet Inf Dis 2006
Policy
Future
Inference
Dynamics
Policy
Future
Maximum likelihood estimation of
parameters for a simple transmission
model for a hospital ward
Susceptible
patients
Colonized or
infected
Bed
1
Assumptions:
• Susceptible patients become colonized faster as the number of
colonized
patients on the ward increases (colonization pressure).
•Colonization assumed to last a long time compared to length of
stay
• The Markov assumption (what happens next depends only on the
current state of the system, not on history).
Parameters
• rate of replacement of colonized by non-colonized
patientsTransmission rate (c)
• spontaneous colonization rate (a)
• transmission rate (θ)
Proposed by Pelupessy et al. (PNAS 2002) for analysing hospital
infection data.
uncolonized
2
3
colonized
colonized
uncolonized
uncolonized colonized
1
2
3
4
5
Day
uncolonized
6
7
Dynamics
Inference
Policy
Future
If only those patients who develop infections are observed :
Susceptible
patients
Colonized or
infected
Markov assumption violated.
Structured Hidden Markov Models are required.
Cooper & Lipsitch, Biostatistics 2004, 5, 223-237
Dynamics
Inference
Policy
Future
Structured Hidden Markov Models
o1
h1
o2
h2
o3
o4
h3
Hidden (unobserved) state
Observation.
h4
Transmission model
Pr(Ht+h =i+1|Ht=i)=βi(N-i)h + ν(N-i)µh + o(h)
If i<N (0 otherwise).
Pr(Ht+h =i-1|Ht=i)=(1- ν)iµh + o(h)
If i>0 (0 otherwise).
N is number of patients or beds,
µ is discharge rate
ν is probability patient is +ve on admission
β is transmission parameter
h is a short time interval
i can be interpreted as the number of colonized
Observation model
Pr(Yt =y|Ht=i)=exp(-λi)(λi)y/y!
i.e. Poisson with mean λi
Cooper & Lipsitch, Biostatistics 2004, 5, 223-237
Dynamics
Inference
Policy
Future
Bayesian formulation of the HMM
Likelihood methods may fail due to:
sparse data (convergence failure)
state space being too large (numerical problems)
MLE may correspond to a biologically implausible region of parameter space
Problems may be overcome by adopting a Bayesian perspective, using prior information (e.g. for
proportion colonized on admission).
McBryde et al., J R Soc Interface, 2007 ; 4: 745-754
Bed
1
2
3
colonized
uncolonized
colonized
uncolonized
1
2
uncolonized
colonized
3
4
Day
uncolonized
5
6
7
Dynamics
Inference
Policy
Future
1. We observe an individual’s “state”
only at certain time points. This
leads to censored data.
Right censored data
uncolonized
1
2
3
4
Day
colonized
5
6
7
Dynamics
Inference
Policy
1. We may observe an individual’s
“state” only at certain time points.
This leads to censored data.
Interval censored data
uncolonized
1
2
3
4
Day
colonized
5
6
7
Future
Dynamics
Inference
Policy
2. The probability that a person’s state
changes at a particular time depends on the
states that other patients are in
uncolonized
colonized
colonized
uncolonized
2
0
1
2
3
4
Day
5
6
7
Future
Dynamics
Inference
Policy
3. There may be ascertainment error:
false negative results: e.g. a negative
MRSA screening swab when a patient
is MRSA positive
false positive results: positive
screening result when a patient is
negative
Future
Solution: Bayesian data augmentation
Likelihood of data given augmented data
(observation model)
Likelihood of augmented data given parameters
(transmission model)
Prior probabilities of parameters
(prior model)
D=data. A=augmented data.
Dynamics
Observed data
Patient 1
Patient 2
Patient 3
= positive swab (observed data)
= negative swab (observed data)
time
Inference
Policy
Future
Dynamics
Observed data & unobserved process
Patient 1
Patient 2
Patient 3
= carriage episode (latent or unobserved process)
= positive swab (observed data)
= negative swab (observed data)
time
Inference
Policy
Future
Dynamics
Observed data & unobserved process
Patient 1
Patient 2
Patient 3
= carriage episode (latent or unobserved process)
= positive swab (observed data)
= negative swab (observed data)
time
Inference
Policy
Future
Dynamics
Observed data & unobserved process
Patient 1
Patient 2
Patient 3
= carriage episode (latent or unobserved process)
= positive swab (observed data)
= negative swab (observed data)
time
Inference
Policy
Future
!"!#
Inference
!"$!
!
!&
!'
Future
!(
!$
!
!"%!
!"!!%(
!"%$
!"!'*
!"!*&
!!"%*
!!"%(
!!"!%*
!"!')
!"!(#
!"!*&
!!"%'
!!"*'
!"&!
!!"%!
Policy
!")#
Dynamics
"
#
!"!'(
!!"!$)
!!"!&#
!"%$
!"!++
!!"!&(
!"!%(
!!"()
!"!#*
!"!!!&*
!"!%(
!!"#$
!"!! !"!*
!"!)'
$%
$$
!(
!$
!"*+
!
!&
!'
!(
!"!#
!"$!
!!"!&
$*
!$
!
!"$+
!"&!
!")#
!"!! !"!*
!(
!$
!
ξ - swab sensitivity; ν - probability colonized on admission
Φ – carriage clearance rate; β1, β2, β3 - transmission rates in phases 1-3
Biostatistics 2007
Am J Epidemiol 2008
Dynamics
Policy
Inference
Future
Policy questions
Which screening technologies and screening strategies should
be used for controlling MRSA when combined with isolation
and decolonisaiton measures?
Is it worth investing in new molecular screening test that gives a
result in a few hours instead of a few days (with higher
sensitivity)? If so, who should we screen with a rapid test?
Benefits of a change a screening policy have to be weighed
against costs. We have to ask, could the money have had
greater health benefit if invested elsewhere in the health
service?
3
Dynamics
Inference
Policy
Future
Many hospitals screen patients for asymptomatic MRSA
carriage (colonisation), but practices vary greatly and
there is wide selection of screening technologies:
Conventional Culture
Chromogenic Agar: CHROMagar; MRSA-ID; MRSA-Select
PCR: IDI-MRSA/gene-ohm; Genotype MRSA direct; Hyplex StaphyloResist; Easy-plex
all with different characteristics:
Sensitivity
Turn around time
(prob. screen is +ve if
(time from screen to
patient has MRSA)
action taken based
Specificity
on screen result)
(1-prob. screen is
Costs
Throughput
+ve if patient does
not have MRSA)
Who and when to screen?
Different combinations of admission,
discharge, periodical (i.e. weekly or
twice weekly) and targeted screening.
What screening technology to use?
Combine with what control measures?
Isolation (single rooms, isolation wards,
patient and staff cohorting, and contact
precautions)
Therapy to suppress colonisation (e.g.
chlorhexidine body washes, mupirocin)
Downloaded from bmj.com on 21 October 2004
Consideration of potential confounders, measures to prevent
bias, and appropriate statistical analysis were mostly lacking. No
conclusions
be drawn
a third
of studies.
Most others
Isolationcould
measures
in in
the
hospital
management
of methicillin
Staphylococcus
aureus
provided
evidenceresistant
consistent with
a reduction of MRSA
(MRSA):Six
systematic
review
of series
the literature
acquisition.
long interrupted
time
provided the
strongest
evidence.
of these
provided
B S Cooper,
S P Stone,Four
C C Kibbler,
B D Cookson,
J Aevidence
Roberts, G that
F Medley,
G Duckworth, R Lai and S Ebrahim
intensive
control measures including patient isolation were
BMJ 2004;329;533
effective
in controlling MRSA. In two others, isolation wards
doi:10.1136/bmj.329.7465.533
failed to prevent endemic MRSA.
Conclusion Major methodological weaknesses and inadequate
Updated information and services can be found at:
reporting
in published research mean that many plausible
http://bmj.com/cgi/content/full/329/7465/533
alternative explanations for reductions in MRSA acquisition
associated with interventions cannot be excluded. No well
These include:
designed
studies exist that allow the role of isolation measures
This article
cites
66 articles,
9 of which
can be
accessed
free at:
eferences alone
to
be
assessed.
None
the
less,
there
is
evidence
that
http://bmj.com/cgi/content/full/329/7465/533#BIBL
concerted efforts that include isolation can reduce MRSA even
3 online articles that cite this article can be accessed at:
inhttp://bmj.com/cgi/content/full/329/7465/533#otherarticles
endemic settings. Current isolation measures recommended
in3national
guidelines
should
towhich
be applied
until for
rapid responses
have been
posted continue
to this article,
you can access
esponses
free at: research establishes otherwise.
further
http://bmj.com/cgi/content/full/329/7465/533#responses
You can respond to this article at:
http://bmj.com/cgi/eletter-submit/329/7465/533
que
but
sion
Mor
a qu
infe
syst
isol
Me
Sea
We
area
and
with
Em
Syst
198
also
sear
the
Bed
1
colonized
uncolonized
isolated
2
colonized
uncolonized
isolated
3
uncolonized
1
2
colonized
3
4
Day
uncolonized
5
6
7
Dynamics
Inference
Policy
Future
BMC Infectious Diseases 2010
Model fitted to data from 8 adult
ICUs in Boston.
Admission and weekly n
nares screening for MRSA
Newly-identified and previously known
MRSA+ patients were placed
under contact precautions
(gloves+gowns).
Dynamics
Isolation Effectiveness
Effectiveness of isolation (gloves and gowns)
in reducing transmission estimated by fitting a
stochastic transmission model to 17 months of
MRSA surveillance data from 10 ICUs.
Parameters estimated within a Bayesian data
augmentation framework using MCMC.
Kypraios et al. BMC Infectious Dis 2010
admission
Susceptible
Di
sc
h
Isolated
Colonised
ge
ar
ar
h
isc
ge
D
Removed
Figure 1: A graphical representation of the stochastic epidemic model described in Section 3.2.
where
YjC
YjQ
:=
:=
{i : aj < min (qi , di , TE )} ∩ {i : ci < cj < min (qi , di , TE )}
{i : aj < min (di , TE )} ∩ {i : qi < cj < min (di , TE )}
Furthermore the amount of time during which a colonised but non-isolated individual i exerts colonisation
pressure to a susceptible individual j is denoted by Dij and is equal to:
Inference
Policy
Future
Dynamics
Inference
Policy
Background
transmission rate
Transmission rate from
unisolated MRSA
patients
Transmission rate from
isolated MRSA patients
Future
Dynamics
Ward
Estimated
probability
isolation
reduced
transmission
Estimated
probability
isolation
reduced
transmission
P(β1 > β2)
Median
(β1/β2)
M1
0.82
2.7
M2
0.51
1.0
GS1
0.27
0.5
GS2
0.50
1.0
SS1
0.73
2.7
SS2
0.79
3.3
SS3
0.44
0.8
SS4
0.58
1.3
Inference
Isolation
effectiveness
effect ->
Policy
Future
Dynamics
Inference
Policy
Future
Model1
Rate of transmission from susceptible to colonized = a0 +a1× number colonized + a2×
number colonized and isolated
Eiso=P(MRSA aquisition given 1 colonized patient in isolation)
P(MRSA acquisition given 1 colonized not in isolation)
=1-exp(-a0 -a2)
1-exp(-a0 -a1)
Model 2
Rate of transmission from susceptible
to colonized = a0 +a1× number colonized
+ a2× number colonized & isolated on open ward
+ a3× number colonized & isolated in a single room
29
was performed in R 2.10.1 (www.r-project.org).
Inference
Dynamics
Figures
0.25
P(colonised on admission)
(estimates & 95% CI)
Ward Type
!
!
0.20
!
Surgery
Elderly
Oncology
0.15
!
0.10
p
!
!
!
!
0.05
!
!
!
!
0.00
!
1
2
3
4
5
6
Ward
7
8
9
10
Policy
Future
Inference
Dynamics
Policy
Future
1.0
Sensitivity
(estimates & 95% CI)
0.8
!
!
!
!
!
!
!
0.6
!
!
0.2
0.4
z
!
Ward Type
!
0.0
!
!
1
2
3
4
5
6
7
8
Surgery
Elderly
Oncology
9
10
Ward
31
Inference
Dynamics
Policy
Future
Figure 4. Isolation effectiveness. This shows the estimates for the reduction in transmission rate
32
Log-effect of isolation
Log−effect of isolation
RRRelative
(95%
CI)
risk
estimates & 95% CI
Ward Type
Surgery
Elderly
Oncology
1
2
3
4
5
Ward
6
7
8
9
10
Summary
−4
−3
−2
−1
0
1
2
log(effect)
Dynamics
Inference
Policy
Future
1
Log-effect of open-ward isolation
Log−effect of open ward isolation
Relative
risk estimates & 95% CI
RR (95%
CI)
Log-effect of side-room isolation
Log−effect of side room isolation
Relative riskCI)
estimates & 95% CI
RR (95%
Ward Type
Surgery
Elderly
Oncology
1
2
2
3
3
4
4
5
5
6
6
Ward
1
7
7
8
8
9
9
10
10
Summary
Summary
−4
−2
log(effect)
0
1
2
3
4
5
−4
−2
0
1
2
3
4
5
log(effect)
5. Isolation effectiveness by type. This shows the estimates for the reduction in
33
Dynamics
Inference
Effectiveness of interventions:
•
•
•
Screening
Eradication therapy
Isolation
Health Economic parameters:
•
•
•
•
Cost of interventions
QALY loss due to MRSA
Attributable mortality
Additional length of stay
Transmission
parameters
Transmission
model
(individual-based,
microsimulation model)
MRSA deaths, infections,
admissions, …
Assessment of effectiveness and cost effectiveness of interventions
Policy
Future
Inputs:
Evidence Synthesis
Literature
Few good studies on
effectiveness of
interventions but
methodological quality of
research is getting better
Data
Analysis or reanalysis of
original data sources
required in the absence
of reliable published
estimates
Dynamics
Inference
Policy
Future
Expert opinion
Where there were knowledge
gaps
formal elicitation techniques
used to produce subjective
prior distributions
12
Dynamics
Inference
Policy
Future
4
5
6
7
8
9
10
2
Scenario number
3 'Inappropriate'
4
5
6
7 isolation
8
9
10
11
12
1
11
12
80
Scenario number
204
02
1
2
3
5
6
7
8
9
10
11
12
1
2
Scenario number
3
4
5 MRSA+
6
7 bed
8
9
10
Unisolated
days
11
12
8
0
4
2
4
6
Scenario number
4
2
0
8
9
10
11
12
10
11
12
Scenario number
80
'Inappropriate' isolation
1
2
3
4
5
6
7
8
9
Scenario number
Unisolated MRSA+ bed days
Clinical cultures only
Conventional Culture
Chromogenic Agar
Chromogenic Agar (early result)
PCR
40 6
60 8
Unisolated MRSA+ bed days
7
6
3
6
60
6
80
4
60
2
40
0
20
2
0
1
5
40
Scenario number
'Inappropriate' isolation
4
20
12
3
0
11
2
4
10
1
2
4
5
6
7isolation
8
9
'Appropriate'
Policy
Inference
Hashed = pre-emptive
Outlined = Intervention applies to high risk group only
0
3
Dynamics
8
4
2
0
2
8
1
Unisolated MRSA+ve bed days per 100 bed daysMRSA−ve isolated bed days per 100 bed days MRSA+ve isolated bed d
6
MRSA+ve bed days per 100 Unisolated
bed daysMRSA−ve
isolated
bedper
days
perbed
100days
bedMRSA−ve
days MRSA+ve
bed
days
bedMRSA+ve
days
MRSA+ve
bed days
100
isolatedisolated
bed days
per
100per
bed100
days
isolated bed days p
Model outputs: effectiveness
1
2
3
4
5
6
7
8
Scenario number
9
10
11
12
Future
3
4
5
6
7
8
9
10
11
Dynamics
1
2
3
4
1
2
3
3
4
4
5
6
7
8
number
5Scenario
6
7
8
5
6
7
8
9
10
11
12
9
9
10
10
11
11
12
12
9
10
11
12
1.0
2.0
MRSA Infections
0.0
2
MRSA infections per 100 admissions
2.0 1.0 2.2 2.0 2.4
MRSA Transmission
1
Policy
Inference
Scenario number
MRSA Infections
0.0
MRSA MRSA
acquisitions
per 100
infections
per admissions
100 admissions
Model outputs:Scenario
effectiveness
number
12
0.0
2
MRSA acquisitio
MRSA
1
1
2
3
4
5
6
7
8
Scenario number
Scenario number
3
4
5
6
7
8
10
11
12
20
15
10
5
Hashed = pre-emptive
39
Outlined = Intervention applies to high risk group only
1
1
2
3
4
number
5Scenario
6
7
8
Deaths
20
9
Clinical cultures only
Conventional Culture Chromogenic Agar
Chromogenic Agar (early result)
PCR
0
2
Deaths per 100 admissions
1
Scenario number
sions
Deaths
MRSA Infections
0.0 21.001.0 21.102.0 21.20
MRSA infections
Deathsper
per100
100admissions
admissions
Deaths
9
10
11
12
2
3
4
5
6
7
8
9
Scenario number
39
10
11
12
Future
Dynamics
Model Outputs:Total
Costs
costs
1
106
3
19
4
5
6
7
8
9
10
Total
costs
106
19number
22
108
Scenario
22 108
12
Bed day costs
Scenario number
Scenario
number
Combined screening costs
Isolation
106
19 22 costs
108
Decolonization
costs
106 19 22 108
0.012000
0.5
Combined
costs
3 4 106
5 6 197screening
8229 10
108 12
Treatment costs
2
106
19
Scenario
number
22 108
Scenario number
Scenario number
1.0 50
1
Scenario number
Scenario number
12600
12400
12300
12000
12000
2
3
4
5
6
7
8
9
10
12
Scenario
number
106Bed
19day
22costs
108
Scenario
number costs
Decolonization
0.5
12400
1.0
Clinical cultures only
Conventional Culture Chromogenic Agar
Chromogenic Agar (early result)
PCR
Decolonization costs
0.0
12800
1.012400
2
1.012400−1.0 12800 0.012000
0.5
Isolation costs
Decolonization costs
1
Hashed = pre-emptive
Outlined = Intervention applies to high risk
group only
−1.0
12
10 20 12000
30 40
10
12
9
12400 0
8
8
7
1
2
3
4
5
6
7
8
106Bed
19day
22costs
108
Scenario number
9
10
12
10
12
Scenario number
Treatment costs
Decolonization
costs
106 19 22 108
Scenario number
4
6
0
5
Future
Bed day costs
12
0 10 20 12000
30 40
4
Costsper
per admission
admission (£)(£)
Costs
3
Costs
per(£)
admission
(£)Costs
Costs per
admission
(£) (£)
ission
Costs(£)
per admission
Costs
per admission
(£)per admission
Costs
(£)
per
admission
12800
12400
12000
Costs per admission (£)
12800
12400
12400
12000
12000
120
80
12400
40
0
10 20 12000
30 40
0
50
30
0 10
admission (£)
CostsCosts
perper
admission
(£)
Total costs
Scenario
Total
costs
106
19number
22
108
Bed
day
costs
106 19 22 108
Scenario
Isolation
costsnumber
Scenario number
ission
Costs(£)
per admission
Costs(£)
per admission
Costs(£)per admission
Costs(£)
per admission (£)
g costs
2 10 2012000
30 40 12400
s
Costs per
per
(£)
Costs
per admission
(£) (£)
sion
osts(£)
per admission
Costs
(£)admission
admission
Costs
(£)per admission
Costs
(£)
per
admission
s
2
Policy
Bed day costs
Bed day costs
1
Inference
Treatment
319 4 22
5 6costs
7 8
108
1106
2
Scenario number
Scenario number
9
Dynamics
0
Cost-Effectiveness
Results:
Isolation
106
!
Policy
Inference
Future
2
1. Isolate clinical cases only
2. Preemptive isolation of all
3. Preemptive isolation of high
risk
4. Preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
23 high risk with
11.
Screen
!
CA_early
12. Screen high risk with PCR
−20
100
!
−40
40 Admission
60 (!
Cost per
!£) 80
!
17
−60
!
8
−80
!
7
12
5
−100
20
9
3
!
!
!
4
10 !6
!
!
!
!
11
!
24
−120
1 Baseline
!
!
0
0.000
0.001
−140
Cost per Admission (!
!£)
18
Dynamics
0.002
20
21
!
19 22 !
0.003
!
!
Health Benefit per Admission (!
!QALY)
Inference
0.000
Policy
0.005
Future
0.010
0.015
0.020
0.025
Step 1 - exclude dominated options
106
Inference
Policy
Future
2
!
0
Dynamics
−20
18
−40
!
17
−60
!
8
!
−80
7
12
5
−120
−100
9
3
!
!
!
4
10 !6
!
!
!
!
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
11.
Screen high risk with
23 CA_early
! high risk with PCR
12. Screen
11
!
Baseline
1
24
!
!
0.000
−140
0
20
40
60
Cost per Admission (!
!£)
Cost per Admission (!
!£)
80
100
!
0.001
0.002
Health Benefit per Admission (!
!QALY)
0.003
20
21
!
19 22 !
!
!
Step 1 - exclude dominated options
Dynamics
Inference
Policy
Future
106
0
!
2
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
11.
Screen
23 high risk with
! CA_early
12. Screen high risk with PCR
−20
100
!
−40
!
17
−60
!
8
−80
!
7
12
5
9
3
!
!
!
−100
20
40
60
Cost per Admission (!
!£)
4
10 !6
!
!
!
!
−120
11
!
Baseline
1
24
!
!
0.000
−140
0
Cost per Admission (!
!£)
80
18
0.001
0.002
20
21
!
19 22 !
0.003
!
!
Health Benefit per Admission (!
!QALY)
0.000
0.005
0.010
0.015
0.020
0.025
Dynamics
Step 2 - evaluate remaining options
Inference
Policy
Future
106
0
!
2
−20
−40
!
17
!
12000 −80 12400−60
−100
20
40
60
Costs
perAdmission
admission (!
(£)
Cost
per
!£)
−120
0
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
23
11.
Screen
high risk with
!
CA_early
12. Screen high risk with PCR
Cost/QALY
=
18
Bed day £1135.90
costs
8
!
7
12
5
106
19
22
108
3
9
4
10 !6
!
!
!
Baseline
!
!
!
Scenario number
!
11
!
24
1
!
!
20
21
!
19 22 !
Decolonization costs
40−140
0.000
sion (£)
Cost per Admission (!
!£)
80
100
!
0.001
0.002
0.003
!
!
Health Benefit per Admission (!
!QALY)
0.000
0.005
0.010
0.015
0.020
0.025
Dynamics
Step 2 - evaluate remaining options
Inference
Policy
Future
106
0
!
2
−20
−40
!
17
!
12000 −80 12400−60
−100
20
40
60
Costs
perAdmission
admission (!
(£)
Cost
per
!£)
−120
0
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
11.
Screen
23 high risk with
! CA_early
12. Screen high risk with PCR
Cost/QALY
=
18
Bed day £1056.69
costs
8
!
7
12
5
106
19
22
108
3
9
4
10 !6
!
!
!
Baseline
!
!
!
Scenario number
!
11
!
24
1
!
!
20
21
!
19 22 !
Decolonization costs
40−140
0.000
sion (£)
Cost per Admission (!
!£)
80
100
!
0.001
0.002
0.003
!
!
Health Benefit per Admission (!
!QALY)
0.000
0.005
0.010
0.015
0.020
0.025
Dynamics
Step 2 - evaluate remaining options
Inference
Policy
Future
106
0
!
2
−20
−40
!
17
!
12000 −80 12400−60
−100
20
40
60
Costs
perAdmission
admission (!
(£)
Cost
per
!£)
−120
0
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
11.
Screen
23 high risk with
! CA_early
12. Screen high risk with PCR
Cost/QALY
=
18
Bed day
costs
£26,196.87
8
!
7
12
5
106
19
22
108
3
9
4
10 !6
!
!
!
Baseline
!
!
!
Scenario number
!
11
!
24
1
!
!
20
21
!
19 22 !
Decolonization costs
40−140
0.000
sion (£)
Cost per Admission (!
!£)
80
100
!
0.001
0.002
0.003
!
!
Health Benefit per Admission (!
!QALY)
0.000
0.005
0.010
0.015
0.020
0.025
Dynamics
Step 2 - evaluate remaining options
Inference
Policy
Future
106
0
!
2
−20
−40
!
17
!
12000 −80 12400−60
−100
20
40
60
Costs
perAdmission
admission (!
(£)
Cost
per
!£)
−120
0
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
11.
Screen
23 high risk with
! CA_early
12. Screen high risk with PCR
Cost/QALY
=
18
Bed day
costs
£48,680.22
8
!
7
12
5
106
19
22
108
3
9
4
10 !6
!
!
!
Baseline
!
!
!
Scenario number
!
11
!
24
1
!
!
20
21
!
19 22 !
Decolonization costs
40−140
0.000
sion (£)
Cost per Admission (!
!£)
80
100
!
0.001
0.002
0.003
!
!
Health Benefit per Admission (!
!QALY)
0.000
0.005
0.010
0.015
0.020
0.025
Dynamics
Step 2 - evaluate remaining options
Inference
Policy
Future
106
0
!
2
−20
−40
!
−120
0
X
!
17
12000 −80 12400−60
−100
20
40
60
Costs
perAdmission
admission (!
(£)
Cost
per
!£)
Cost/QALY
=
18
Bed day
costs
£48,680.22
8
!
7
12
5
106
19
22
108
3
9
4
10 !6
!
!
!
Baseline
!
!
!
Scenario number
!
1. isolate clinical cases only
2. preemptive isolation of all
3. preemptive isolation of high
risk
4. preemptive isolation of high
risk (amended following CC
screen result)
5.
Screen all admissions
(+wkly screens) with CC
(isolate known +ves)
6.
Screen all with CA
7. Screen all with CA_early
8.
Screen all with PCR
9. Screen high risk with CC
10. Screen high risk with CA
11.
Screen
23 high risk with
! CA_early
12. Screen high risk with PCR
11
!
24
1
!
!
20
21
!
19 22 !
Decolonization costs
40−140
0.000
sion (£)
Cost per Admission (!
!£)
80
100
!
0.001
0.002
0.003
!
!
Health Benefit per Admission (!
!QALY)
0.000
0.005
0.010
0.015
0.020
0.025
Dynamics
Inference
Accounting for parameter uncertainty
13400
!
!
!
!
!
!
!
! !
!
!
!
!
!
!
13000
!!
!!
!!!
!!
12800
!!!
!!!
!!
!
!
!!
!
!!
!!!
!
!
!
!
!!!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!!!
!!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
! !!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!!
!
!!
!
!
!
!
!
!
!!!
!
!
!!
!!
!! !
12600
Cost per Admission (£)
13200
!
Strategy 1
Strategy 2
Strategy 3
Strategy 4
Strategy 5
Strategy 6
Strategy 8
Strategy 9
Strategy 10
Strategy 12
7.28
7.30
7.32
7.34
7.36
7.38
Health Benefit per Admission (QALY)
7.40
Policy
Future
Dynamics
Inference
Policy
NMB, CEAC, CEAF
•
Net Monetary Benefit (NMB)=ΔE × λ -ΔC
•
ΔE is change in health outcomes (QALYs)
•
ΔC is change in costs
•
λ is willingness to pay per QALY gain
•
Cost-effectiveness acceptability curves (CEACs) show the
probability that each strategy has the highest NMB as λ varies.
•
Cost-effectiveness acceptability frontiers (CEAFs) show the
probability that the strategy with the highest expected NMB has
the highest NMB as λ varies.
•
Future
Screening & isolation in the ICU
CEACs
Dynamics
Inference
CEAF
Policy
Future
Screening & isolation in the ICU
CEACs
•
Dynamics
Inference
Policy
CEAF
Expected value of perfect information (EVPI) tells us how much we would
benefit if we knew all parameters perfectly
–
EVPI=Eθ[maxj{NMB(j, θ)}]-maxj{Eθ[NMB(j, θ)]}
Future
Dynamics
Inference
Policy
Screening & isolation in General Medical Wards
CEACs
CEAF
Future
Dynamics
Inference
Screening & decolonization in ICUs
CEACs
CEAF
Policy
Future
Dynamics
Inference
Policy
Screening & decolonization in General Medical Wards
CEACs
CEAF
Future
Dynamics
Inference
Policy
Future challenges
How to account for resistance selection
in health economic models of antibiotic
use?
How to account for strain diversity?
How to evaluate control strategies in
low and middle income countries?
EVPPI, EVSI...
How to make use of sequencing data?
Future
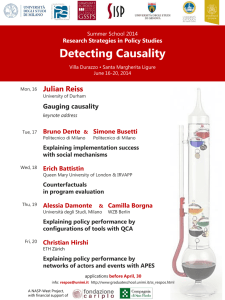
Concurrent outbreak of
ST239 MRSA (TW clone)
and endemic
UK clones of MRSA at St
Thomas’s Hospital
London.
Epidemic trees
probabilistically
reconstructed using
hazards (as proposed
by Kenah et al.. Math
Biosciences 2008).
4
5
6
7
0
1
2
3
4
5
6
7
1
2
3
4
5
6
7
0
1
2
3
4
5
6
7
0
0
0
0
1
2
3
4
5
6
7
0
1
2
3
4
5
6
7
0
1
2
3
4
5
6
7
0
1
2
3
4
5
6
7
8
6
6
4
0
2
2
0
0
0
2
5
4
4
6
10
8
8
10
10 12
3
12
2
10 12
1
50
10 20 30 40 50 60
20
10
0
5
50
0
0
Phase 4
100 150 200 250
Phase 3
30
100 150 200 250
Phase 2
15
Frequency
Phase 1
A
B
C
!
!
ST239−TW MRSA
Other MRSA
5
6
!
!
4
!
!
!
!
3
!
2
1
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
0
Expected secondary cases per case
7
Expected number of secondary cases per case
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!!
!
!
!
! !!
!
!
!
!
!
!
!
!
!
!
!!
!
! !!!
!!
! ! !!
! ! !!
!
!!
!
!
!
!
!!!
!!!
!
!
!!
!
!
! !
!
!
!! !
!
!!
!!
!
!
! ! !!
!
!
!
!
!
!
!
!
!
! !!
!
!!
!
!
!
!! ! ! !
!
! ! !
!
!
!
!
!
!!
!
!
!
!
!!
!
!
!
!
!
!! !
! !!!
!
!
!
!!
! ! !!! !
! !! ! !
! !!
!!
!!
! ! !!
!
!! !! ! !
!!! ! !!! !
!! !
!
!
!
!
!
!
!
!!
!!! !
!
!
!
!
!
!
!
!
! !!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!! !!
!!!
!
!
!!!
! !!!! !
!
! !!
!
!! !
!!!
!
!!
!!
! !!
!
!
!
! ! ! ! !! !
! !!!
!! !!!!
!!!! !
!!! !!
!!
!
!!
!!
! !
!!
! !! ! !
! !!
!
!
! !!
!!
!!
!
!!
!!
!! !
! ! !!! !!
!!
!!
!
! ! ! !!!
!
!
!!!
!!
!
!
!
! ! !!
!!!!
! !! !
!
!
!!!!! !
! ! !!!!!!!
!
! !
! !!
!!
!!
! !! !!!
!!!
!
! !!
!! !!
!!!!! !!!
!!
!!!!!
!
!
!!
! !!!!!
! !!! !
!
!!!
!
!
!! !
!
!!
!!
!
!
!!!!!! !!!!
!!! !!!!!
!
!!
!
!!!
!!!!!!
! !!!! ! !!
!!!!!!
!!
!! !
!
!!!!
!!!
!
! ! ! !!
!
!! !
!!! !!
! !
!!!!!!!!! !!!
!!!
! !!
!!
! !!! ! ! !!! !
!!!
!! !
!!!! !
!!
!!
!!!! !!
!!!!
! !!!!!!!!!
!!
!! ! ! !!
!!!!
!!!!
!
!!!! !!
!!! !!!
!!! ! !
!
!
!!!
!!
!! !! !!!!!!!!!!!!
!! !
0
50
100
150
!
!
!
!
!! !
!! !
!!!! !
200
Week
Figure 3. Distribution of secondary cases per case for both wards combined: red is TW MRSA,
black is non-TW. Lines in scatterplot are smoothed trend lines (lowess smoothing).
VOL. 192, 2010
Dynamics
NOTES
Inference
Policy
889
Future
J Bacteriology, 2010
“...genomic analysis of TW20 provides evidence of its adaptation to survive in
a health care setting through acquisition of drug and antiseptic resistance
genes carried on MGEs, large chromosomal insertions, and point mutations in
housekeeping genes. The large size of the TW20 genome reflects the ability of
the ST239 lineage to undergo prolonged and continuing evolution to adapt to
the hospital environment.
FIG. 1. Schematic circular diagram of the S. aureus TW20 chromosome. Key for the circular diagram (outer to inner): outer colored segments
on the gray outer ring represent genomic islands and horizontally acquired DNA (see the key in the figure); scale (in Mb); annotated CDSs colored
according to predicted function are shown on a pair of concentric circles, representing both coding strands; S. aureus reciprocal Fasta matches
shared with the S. aureus strains: MRSA252, (accession number BX571856) (16), MSSA476 (accession number BX571857) (16), MW2 (accession
number BA000033) (4), N315 (accession number BA000018) (20), Mu50 (accession number BA000017) (20), Mu3 (accession number AP009324)
(23), COL (accession number CP000046) (13), NCTC8325 (accession number CP000253) (14), USA3000 FPR3757 (accession number CP000255)
(11), JH9 (accession number CP000703) (22), Newman (accession number AP009351) (3), and RF122 (accession number AJ938182) (15); regions
of the chromosome derived from a CC8 ancestor (light green) or the CC30 ancestor (brown). Color coding for TW20 CDS functions: dark blue,
pathogenicity/adaptation; black, energy metabolism; red, information transfer; dark green, surface associated; cyan, degradation of large molecules; magenta, degradation of small molecules; yellow, central/intermediary metabolism; pale green, unknown; pale blue, regulators; orange,
conserved hypothetical; brown, pseudogenes; pink, phage and IS elements; gray, miscellaneous.
Science, 2010
a large block of DNA (26). The approximate boundaries of the
recombination were identified from pairwise comparisons of
the TW20 chromosome with MRSA 252 (CC30) and USA300
TCH1516 (CC8). A marked shift in DNA percent identity of
approximately 1 percentage point was observed across the approximate recombination breakpoints (data not shown), demonstrating that 635 kb (!20.6% of the TW20 chromosome;
SATW20_26800 to SATW20_03960) may have been transferred from a CC30 donor. This transfer event also contributes
to the high level of reciprocal Fasta matches between TW20
and MRSA252 (ST36).
The origins of SCCmecIII in the TW20 genome are unclear,
since SCCmecIII has not been found in the CC30 lineage. Each
of the SCC elements contains further MGEs: SCCmercury
contains Tn554, encoding a streptomycin 3"-adenylyltransferase and an erythromycin resistance protein, ErmA1, and
SCCmec contains an integrated plasmid, pT181, and #Tn554,
containing cadmium resistance CDSs. In addition to Tn554
and #Tn554 in the SCCmec region, the TW20 chromosome
contains an additional Tn554 and a Tn552 transposon, encoding the $-lactamase BlaZ, within an integrative conjugative
element (ICE) (31).
Further resistance determinants are found on plasmid
pTW20_1. Importantly, it carries a gene encoding an antiseptic
Staphylococcus aureus in northeastDynamics
Thailand
Inference
Policy
Future
Harris et al., Science
2010 EK, Amornchai P, Parkhill J, Wuthiekanun V, Holden MTJ, Hongsuwan M, Bentley SD, Chantratita N,
B, Limmathurotsakul
D, Nickerson
Day NP, Peacock SJ
Monday, February 14, 2011
s et al., Science 2010
Acknowledgements
Colin Worby
Theodore Kypraios
Julie Robotham
Graham Medley
Phil O’Neill
Nick Graves
Susan Huang
Dakshika Jeyaratnam
Jonathan Edgeworth
Rahul Batra
Barry Cookson
Jennie Wilson
Sharon Peacock
Emma Nickerson
Maliwan Hongsuwan
Funding: UK Dept of Health, Wellcome Trust, EU FP6 (MOSAR)
Data: 50 months MRSA infection data from an 11 bed
MICU in Vellorre, south India (no screening data).
Hidden Markov Model used to impute colonization data
and estimate transmission parameters.
Estimated that 4% of patients were MRSA+ on
admission, with a ward level reproduction number of 0.4
(indicating substantial transmission).
Future Challenges
CID January 2010
Health Benefits (Quality Adjusted Life Years gained)
Differences in mortality between strategies will account for almost all differences in
QALY gain
Annual mortality
We estimated the expected quality adjusted life expectancy of someone
discharged alive from an ICU is 9.34 years (calculated from quality weighted
survival data)
Dynamics
Future
antibiotic-resistant bacteria
0.6000
.
Community
Hospital
Policy
Fraction resistant
antibiotic-sensitive bacteria
Inference
0
-30
60
Time (days)
Infection control (70% transmission reduction)
Infection control + switch antibiotics
Resistance quickly increases in frequency
in response to drug use, and quickly
decreases in response to intervention.
Non-specific control does appreciably
reduce resistance (when resistance is rare
in the community).
Formulary changes can rapidly eradicate
resistant bacteria.
Lipsitch et al. PNAS 2000