Preparing for an Anthrax Attack: the Impact of Distributing MedKits
advertisement

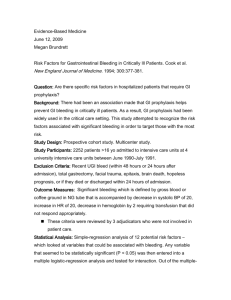
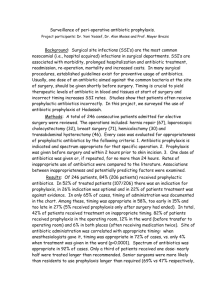
Proceedings of the 2011 Industrial Engineering Research Conference T. Doolen and E. Van Aken, eds. Preparing for an Anthrax Attack: the Impact of Distributing MedKits Abstract ID: 480 Michelle L. Houck Jeffrey W. Herrmann University of Maryland College Park, Maryland Abstract Finding feasible strategies to distribute antibiotics quickly to the general public in response to an anthrax attack remains a difficult challenge. Among the proposed strategies is the pre-event placement of pharmaceuticals in individual households for use only as directed by public health authorities. These medications (known as “MedKits”) would allow many exposed persons to begin treatment quickly while reducing the number who visit points of dispensing, the primary distribution strategy. This paper describes a model that estimates the expected number of deaths in an anthrax attack by modeling the logistics of the response and the use of MedKits and discusses the results obtained from modeling various scenarios. Beyond the scenarios considered here, the ability to predict this benefit in other scenarios will be valuable to public health officials who are considering this option. Keywords Anthrax, bioterrorism, homeland security, compartmental models. 1. Introduction The deliberate release of aerosolized anthrax spores in a large city could expose many thousands of residents to this deadly disease. Promptly distributing antibiotics to those exposed is a key step in preventing illness and deaths. Avoiding delays in this distribution is critical, but such a response will require enormous resources. State and local health departments have developed plans for points of dispensing (PODs), the primary distribution channel. These health departments realize, however, that they do not have the staff required to operate enough PODs to distribute medication to a large number of people sufficiently quickly. Therefore, other strategies have been proposed and tested [1]. These include employing the U.S. Postal Service to deliver antibiotics directly to residences, predeploying pharmaceuticals to hospitals, pre-event dispensing of pharmaceuticals to first responders, and the preevent placement of pharmaceuticals in individual households for use only as directed by public health authorities. This paper focuses on using this last option along with PODs. The pre-deployed medications are commonly known as “MedKits.” The use of MedKits has been advocated because they can reduce the time needed to distribute medication [2]. Concerns about safety and the inappropriate use of MedKits have slowed the development of this option [3]. We are unaware, however, of any efforts to model how pre-deploying MedKits would reduce the mortality resulting from an anthrax attack. Predictions of this benefit should be valuable to public health officials who are considering this option. The study described in this paper extends a compartmental model that predicts the deaths from an anthrax attack [4]. Although that model was used to consider a broad set of questions, it focused on PODs and did not consider the impact of pre-deploying MedKits. The disease progression model used here is based upon a review of all of the cases of inhalational anthrax that have been published since 1900 [5]. The purpose of the work described in this paper was to develop a model that could estimate the impact of deploying MedKits in a community and to use that model to consider some possible scenarios to get some insight into the Houck and Herrmann effectiveness of the MedKit strategy. This paper will briefly describe the model and the results. A complete description of the model is provided in [6]. 2. Model Overview For this study, we developed a compartmental model that includes both the progression of the disease and the logistics of treatment. A compartmental model represents the flows of individuals between compartments. Each compartment represents a number of homogeneous individuals (that is, they are identical with respect to their condition and treatment status). The compartments are mutually exclusive and collectively exhaustive. Compartmental models can be analyzed using differential equations (which can be solved exactly in some situations) or difference equations (which we will use here). Compartmental models have been used in studies of biology, medicine, ecosystems, populations, and economics [7, 8]. The model used here (the “MedKits model”) extends the model developed in [4] (the “POD model”) by adding additional compartments for the population that has MedKits and revising the transition equations used to predict the flow between compartments. The MedKits model has 28 compartments to represent distinct groups within a population. The primary distinctions between the compartments are the exposure of the individuals, the progression of the disease (including the definitive conditions of death or recovery), the treatment status, and the possession of MedKits. The model includes the 21 compartments of the POD model and adds seven more: one for death, two for potential exposures who possess MedKits, three for exposed individuals who possess MedKits, and one for those who adhere to prophylaxis (and cannot become ill). Table 1 (at the end of this paper) lists all 28 compartments. Figure 1 is a schematic that shows the possible flows in the MedKits model. Like the POD model, the MedKits model is a deterministic, discrete-time model. The time period is one hour. Let X i (t ) be the number of individuals in compartment i at time t. The model calculates these values for a 2400-hour (100-day) time horizon. At each point in time, we calculate the transitions, where φij (t ) is the number of individuals who move from compartment i to compartment j due to illness, recovery, or death, and ψ ij (t ) is the number of individuals who move from compartment i to compartment j due to awareness, prophylaxis, or treatment. Yi (t ) is the number of individuals in compartment i at time t after the transitions due to illness, recovery, and death, and these values are used to determine the values of ψ ij (t ) , as described in detail in [6]. Note that many of the transitions are always zero; the notation used here allows a compact expression of the transition equations, which can be written as follows: 28 28 Y j (t ) =X j (t ) + ∑ φij (t ) − ∑ φ ji (t ) =i 1 =i 1 28 28 X j (t + 1)= Y j (t ) + ∑ψ ij (t ) − ∑ψ ji (t ) (1) =i 1 =i 1 In general, during each time period, a certain fraction of the individuals in a compartment will move to another compartment. This flow is governed by the values of parameters describing the disease progression (the rates at which individuals become ill, recover, or die) and the prophylaxis and treatment capacity. For a given flow, the fraction may be time-invariant (like a death rate) or may change over time as available treatment capacity changes. Many of the parameters given below and used in the MedKits model are the same as those used in the POD model, but the model can be changed easily to consider scenarios with other parameters. The model includes two types of flows. The first type of flow corresponds to changes in the disease in those who were exposed. The transition path is from the incubation stage to the prodromal stage, to the fulminant stage, and then to death. The second type of flow corresponds to changes in awareness and treatment. Exposed persons and potential exposures are first unaware of their exposure or the need for prophylaxis. When they become aware, then they seek prophylaxis (essentially, they are in a queue for prophylaxis). Exposed persons who become sick then seek treatment and receive treatment. Those who are treated may recover. Houck and Herrmann 25 26 27 1 2 3 4 5 6 7 8 28 13 17 9 18 19 23 20 10 11 12 14 15 16 21 24 22 Figure 1. Schematic of the flows between compartments in the MedKits model. Because many of the compartments have multiple outflows (corresponding to different transitions), it is important to define the relative priority of the transitions. In the MedKits model, the highest priority transitions are those that correspond to the progression of the disease, recovery, and death. The second priority transitions are those that correspond to awareness, prophylaxis, and treatment. The number who can be given prophylaxis is limited by the prophylaxis dispensing capacity, which is spread proportionally across all of the compartments with persons waiting for prophylaxis. Likewise, the number who can be treated is limited by treatment capacity, which is spread proportionally across all of the compartments with persons waiting for treatment. 2.1 Attack and Response Timeline The MedKits model can be used for a wide range of scenarios, but those considered in this study were based on the following timeline. The attack occurs at t = 0 hours. The attack is detected at t = 48 hours. Local supplies of both intravenous antibiotics (IVs) for treatment and antibiotics for dispensing will become available 5 hours later at t = 53 hours. Intravenous antibiotics (IVs) for treatment, antibiotics for dispensing, and additional ventilators from the push pack will become available 16 or 28 hours after attack detection at t = 64 or 76 hours. (This is due to a 12 or 24 hour delay in receiving the push pack and another 4 hour delay in getting the material from the push pack ready.) Intravenous antibiotics (IVs) for treatment and antibiotics for dispensing from vendor-managed inventory (VMI) will become available 36 hours after attack detection at t = 84 hours. At t = 96 hours (48 hours after attack detection), complete POD capacity will be available. In the MedKits model, these times are all parameters that can be changed to consider multiple scenarios. 2.2. Exposure The population consists of three large subpopulations: those who were exposed to the anthrax attack, those who were not exposed to the anthrax attack (or inhaled too few anthrax spores to become ill), and those who believe that they may have been exposed (because of their proximity to the attack or for other reasons). The persons in this last group, called “potential exposures,” will undergo prophylaxis (by going to PODs and taking their MedKits) but cannot become ill. Like the POD model, the MedKits model does not divide the population by age because we assume that the progression of anthrax does not depend upon age. We assume that exposure to the attack is independent of MedKit possession. Therefore, the proportion who possess MedKits is the same in all three subpopulations. Because those who were not exposed cannot become ill and do not seek prophylaxis whether they have a MedKit or not, the model treats all of these persons in one compartment. Those who are exposed are initially Houck and Herrmann unaware of their exposure. Some become aware during incubation, some when they are prodromal, and some when they are fulminant. 2.3. Disease Progression The disease progresses from the incubation stage to the prodromal stage, to the fulminant stage, and then to death. An exposed person in the incubation stage is infected with anthrax but is asymptomatic. A person in the prodromal stage has nonheadache neurological symptoms (e.g., fever, muscle aches, fatigue) that are similar to flu. A person in the fulminant stage is severely ill, has respiratory distress, and may die within days. We assume that only persons in the fulminant stage can die. Because it considers a short period of time, this model does not consider any other causes of death. Those in the prodromal and fulminant stages who start treatment may recover. The rates at which persons become ill, recover, or die vary based on their status. The times to become ill, recover, or die are modeled as geometric distributions (thus, they are memoryless), and the probability of this event per time unit is the reciprocal of the mean time. The specific rates are based on those in [4, 5] and are given in [6]. 2.4. Awareness and Prophylaxis Those who become ill can become aware at any time: for those who are in the prodromal stage, the probability, each hour, of becoming aware equals 1/72; for those who are in the fulminant stage, the probability equals 1/48. After the attack is detected, for those who are in the incubation stage and for potential exposures, the probability, each hour, of becoming aware equals 1/72. This awareness process is a special case of the Bass diffusion process, and the rates are the same as those in the POD model [4]. Those who have MedKits do not go to PODs, so those who were exposed and potential exposures can start prophylaxis as soon as they become aware. However, some of those to whom MedKits were distributed may be unable to use them, so we assume that 5% of those given MedKits do not have them at the time of the attack. Those who do not have MedKits will go to PODs, where the prophylaxis dispensing consists of an oral antibiotic, either ciprofloxacin or doxycycline. Prophylaxis dispensing capacity is limited. It depends upon the facilities and staff available. In the scenarios considered in this paper, we assume that there is a fixed maximum prophylaxis dispensing capacity, which is 5,833.33 persons per hour. Prophylaxis dispensing is also limited by the availability of medication. Although a complete regimen has 60 days of medication, we assume that only 14-day abbreviated regimens are dispensed until the VMI becomes available. We assume that the local stockpile has 50,000 doses (3,571 abbreviated regimens), the push pack provides 2,718,000 doses (194,143 abbreviated regimens), and the VMI provides sufficient doses for everyone to receive a complete regimen and enough IV antibiotics for everyone who needs them. Those who adhere to their prophylaxis will not become ill, but some who begin prophylaxis during the incubation stage will not adhere and may become ill. (We assume that those who are in the prodromal and fulminant stages will always adhere.) We considered two different adherence rates: 65% and 90%. During the 2001 anthrax attack in Washington, D.C., only 64% of those who received prophylaxis adhered fully to prophylaxis [9]. Other studies [10] assumed that 90% of those who receive prophylaxis will adhere. If the regimens in the MedKits and those dispensed at the PODs are not complete regimens, then these persons will need to obtain the remainder. We assume that the process of dispensing the remainder will be done on a less urgent basis and will not interfere with primary dispensing capacity. 2.5. Treatment Persons who become ill need treatment, which consists of three antibiotics administered intravenously in an intensive care unit (ICU). All who begin treatment adhere to it. Treatment capacity is limited by the availability of IV antibiotics, ventilators, respiratory technicians, and ICU beds. We assume that the local stockpile has 500 days of IV antibiotics, the push pack provides 21,492 days of IV antibiotics, and the VMI provides sufficient IV antibiotics for everyone who is being treated. We assume that 100 ventilators are available when the attack occurs, and the push pack provides 100 more. We assume that each respiratory technician can monitor 10 patients, 200 respiratory technicians are available when the attack occurs, and 2,000 ICU beds are available when the attack occurs. There must be at least one day’s worth of IV antibiotics to begin treatment of one patient. Houck and Herrmann 60% N=1,250,000, b=0.5 N=1,250,000, b=0.1 Percentage of those exposed who die 50% N=1,250,000, b=0.01 N=500,000, b=0.5 N=500,000, b=0.1 40% N=500,000, b=0.01 30% 20% 10% 0% 0 500,000 1,000,000 1,500,000 2,000,000 2,500,000 3,000,000 3,500,000 4,000,000 4,500,000 5,000,000 Number of Medkits Distributed Figure 2. The mortality rate decreases when more MedKits are distributed before an attack. The results shown are for scenarios in which the prophylaxis adherence rate is 90% and the push pack delay is 24 hours. N is the number exposed. b is the fraction of non-exposed persons who will seek prophylaxis (potential exposures). 2.6. Antibiotic Inventory The model also keeps track of the inventory of antibiotics available for prophylaxis and the IVs available for treatment. Each hour, the inventory of antibiotics (days of medication) is reduced by the number of days of medication dispensed (the product of the number who receive prophylaxis and the number of days in the dispensed regimen at that time). In addition, the inventory of IVs (days of IVs) is reduced by the number of those being treated divided by 24. The inventory for antibiotics and IVs increases when the local inventory becomes available (at t = 53 hours), when the push pack inventory is available and ready, and when the VMI becomes available (at t = 84 hours). The number of ventilators also increases when the push pack inventory is available and ready. 3. Results To illustrate the use of the model to predict the impact of MedKits, we considered a range of scenarios like those in [4] and varied the number of pre-deployed MedKits. The population was 5 million people. We ran the model on several scenarios on this population varying the number of people exposed, the fraction of unexposed people who believe they were exposed (and thus use medication that could be reserved for exposed people), the time until the push pack becomes available, and the prophylaxis adherence rate. We considered attack scenarios with 50,000 exposed, 500,000 exposed and 1,250,000 exposed. Rates of 0.01, 0.1, and 0.5 were used for the fraction of the unexposed population seeking prophylaxis. Values of 12 hours and 24 hours were used for push pack availability. We used prophylaxis adherence rates of 65% and 90%. We also varied the number of MedKits distributed prior to an attack scenario. We considered increments of 500,000 MedKits from 0 to 5,000,000. Distributing zero MedKits corresponds to the scenario in [4], and distributing 5,000,000 MedKits corresponds to the entire population receiving MedKits. Some expected trends were evident in our results. When all other factors were held constant and the adherence rate increased from 65% to 90%, the number of deaths decreased, and the average reduction in mortality rate was 2.6%. When the push pack availability decreased from 24 to 12 hours, the number of deaths decreased only slightly, as the average reduction in mortality rate was less than 0.5%. In every case, the number of deaths decreased as more MedKits were distributed. In some cases this decrease was substantial while in other cases it was minimal. A key factor that affected the size of the decrease was the rate at which those who were not exposed believed that they were (which determined the number of potential exposures). When the number of potential exposures was large, then medication was not immediately available for those who truly needed it, which delayed their prophylaxis. In these scenarios, distributing more MedKits saved many lives. Houck and Herrmann For example, in the scenario where 1,250,000 people were exposed and another 1,875,000 were potential exposures, with an adherence rate of 65% and push pack availability at 24 hours, the number of deaths decreased from 621,907 (if no MedKits had been distributed) to 140,368 (if Medkits had been distributed to the entire population). When the number of potential exposures was small, the antibiotics were going to those who needed it with minimal delay, and distributing more MedKits had minimal impact on the number of deaths. Figure 2 shows how the mortality rate decreases when more MedKits are distributed before an attack. The results in this figure are for scenarios in which the prophylaxis adherence rate is 90% and the push pack delay is 24 hours. The mortality rates are highest when the number of potential exposures is large, but distributing more MedKits mitigates this phenomenon. Regardless of the number of MedKits distributed, it appears that some number of deaths is unavoidable. Even in the scenario with the smallest attack (50,000 persons exposed), and the smallest number of potential exposures (1% of those not exposed, which is 49,500 in this case), a 90% adherence rate, and a 12 hour push pack availability, the estimated number of deaths was 4,102 (a mortality rate of 8.2%) even when MedKits were distributed to the entire population. The unavoidable deaths result from the delays in detecting the attack and starting prophylaxis (during which time some exposed persons become very ill), the loss of MedKits among those who received them, and the imperfect adherence rate. 4. Summary and Conclusions The MedKits model can estimate the number of deaths that result from an anthrax attack when a community predeploys MedKits and uses PODs to dispense prophylaxis to those without MedKits. Predictions of this benefit will be valuable to public health officials who are considering this option. The results show that, as more MedKits are pre-deployed, the mortality rate decreases and fewer deaths occur. The reduction in mortality rate is greater when the number of potential exposures is large. Essentially, distributing MedKits counteracts the problems caused by the large number of potential exposures delaying the prophylaxis of those who were truly exposed. The numerical results discussed here are for some particular scenarios. The MedKits model is capable of modeling many different scenarios by changing the parameters used in the model. While not discussed here, the MedKits model can estimate the number of persons hospitalized and the total number of patient-days. Because the MedKits model is based on the POD model, it has many of the same limitations. Both models make certain assumptions about the progression of anthrax, most particularly the assumption that the progression is not affected by age. Neither considers the impact of the disease on prophylaxis and treatment capacity. Both models assume that becoming aware of the attack is a simple diffusion process. In real communities, however, the spread of information may be quite different, which could affect the rate at which exposed persons and potential exposures seek and begin prophylaxis. Both models are deterministic compartmental models that estimate the expected outcome but give no insight into the distribution of possible outcomes for a given scenario. We are currently working to characterize this distribution. The MedKits model assumes that those who possess MedKits have the same chance to be exposed or to be potential exposures as those who do not have MedKits. Moreover, the model assumes that the progression of anthrax in exposed persons who take the antibiotics in the MedKits is the same as in exposed persons who receive prophylaxis from a POD. The compartments and flows in the model could be modified to represent scenarios in which these assumptions and others are replaced by other conditions. Of course, the decision to distribute MedKits depends upon many factors besides the expected impact on deaths. The cost of purchasing, deploying, and replacing the MedKits may be substantial. The distribution should be fair, but issues of equity will appear if the number of MedKits available is not enough for everyone who wants them. The risks of individuals using the MedKits for unauthorized, possibly dangerous, uses must be assessed as well. The MedKits model could be modified to evaluate the response to attacks with other noncommunicable agents such as tularemia, botulism, ricin, or yellow fever. It could be extended to consider other countermeasures strategies or to consider the dispensing of additional medication to those who receive incomplete initial regimens. Finally it could be extended to consider communicable diseases such as smallpox, but this would require considering the spread of the disease from those exposed to those who are not exposed. Houck and Herrmann References 1. Centers for Disease Control and Prevention, 2007, “Emergency MedKit Evaluation Study Summary,” November 15, 2007. http://www.bt.cdc.gov/agent/anthrax/prep/pdf/medkit-evaluation-summary-2007.pdf. 2. Kaplan, E.H., Bicknell, W.J., and Wein, L.M., 2003, “How Best to Fight Against Bioterrorism,” August 5, 2003. http://www.cato.org/pub_display.php?pub_id=3189 3. Troy, Tevi, 2010, “Preparing for Bioterrorism,” Weekly Standard, February 23, 2010. http://www.hudson.org/index.cfm?fuseaction=publication_details&id=6785 4. Zaric, G.S., Bravata, D.M., Holty, J.-E.C., McDonald, K.M., Owens, D.K., and Brandeau, M.L., 2008, “Modeling the Logistics of Response to Anthrax Bioterrorism,” Medical Decision Making, 28, 332-350. 5. Holty, J.E., Bravata, D.M., Liu, H., Olshen, R.A., McDonald, K., and Owens, D.K., 2006, “Systematic review: a century of inhalational anthrax cases from 1900 to 2005,” Annals of Internal Medicine, 144(4), 270–280. 6. Houck, M.L., and Herrmann, J.W., 2011, “Predicting the Impact of Placing Pre-event Pharmaceuticals for Anthrax,” Technical Report, Institute for Systems Research, University of Maryland, College Park. 7. Jacquez, J.A., 1996, Compartmental Analysis in Biology and Medicine, third edition, BioMedware, Ann Arbor, Michigan. 8. Walter, G.G., and Contreras, M., 1999, Compartmental Modeling with Networks, Birkhäuser, Boston. 9. Shepard, Colin W., Montse Soriano-Gabarro, Elizabeth R. Zell, James Hayslett, Susan Lukacs, Susan Goldstein, S.F., Jones, J., Ridzon, R., Williams, I., Rosenstein, N., and the CDC Adverse Events Working Group, 2002, “Antimicrobial postexposure prophylaxis for anthrax: adverse events and adherence,” Emerg Infect Dis, 8(10), 1124–1132. 10. Wein, L.M., Craft, D.L., and Kaplan, E.H., 2003, “Emergency response to an anthrax attack,” Proc Natl Acad Sci, 100(7), 4346–4351. NOTE: Table 1 follows on the last page. ` Houck and Herrmann Compartment 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 Table 1. The compartments in the MedKits model. Exposure, Disease Treatment treatment status stage began Exposed, unaware Incubation n.a. of exposure Exposed, unaware Prodromal n.a. of exposure Exposed, unaware Fulminant n.a. of exposure Aware of exposure Incubation n.a. Aware of exposure Prodromal n.a. Aware of exposure Fulminant n.a. Not adhering to Incubation Prophylaxis begun in incubation stage prophylaxis In prophylaxis Prodromal Prophylaxis begun in incubation stage In prophylaxis Prodromal Prophylaxis begun in prodromal stage In prophylaxis Fulminant Prophylaxis begun in incubation stage In prophylaxis Fulminant Prophylaxis begun in prodromal stage In prophylaxis Fulminant Prophylaxis begun in fulminant stage In treatment Prodromal Treatment begun in prodromal stage In treatment Fulminant Prophylaxis or treatment begun in prodromal stage In treatment Fulminant Prophylaxis begun in incubation stage, treatment begun in fulminant stage In treatment Fulminant No prophylaxis or prophylaxis begun in fulminant stage Exposed Recovered n.a. Not exposed n.a. n.a. Potential exposure, n.a. n.a. not seeking prophylaxis Potential exposure, n.a. n.a. seeking prophylaxis Potential exposure, n.a. n.a. in prophylaxis Exposed Dead n.a. Potential exposure, n.a. n.a. not seeking prophylaxis Potential exposure, n.a. n.a. in prophylaxis Exposed, unaware Incubation n.a. of exposure Exposed, unaware Prodromal n.a. of exposure Exposed, unaware Fulminant n.a. of exposure Adhering to Prophylaxed Prophylaxis begun in incubation stage prophylaxis MedKit No No No No No No Both Both Both Both Both Both Both Both Both Both Both Both No No No Both Yes Yes Yes Yes Yes Both