VICTOR VALLEY COLLEGE STUDENT REPORT
advertisement

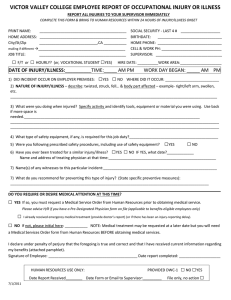
VICTOR VALLEY COLLEGE STUDENT REPORT OF OCCUPATIONAL INJURY OR ILLNESS REPORT ALL INJURIES TO YOUR INSTRUCTOR IMMEDIATELY COMPLETE THIS FORM & BRING TO HUMAN RESOURCES WITHIN 24 HOURS OF INJURY/ILLNESS ONSET PRINT NAME: __________________________________________ HOME ADDRESS: __________________________________________ City/St/Zip ____________________________,CA ___________ mailing if different →__________________________________________ JOB TITLE: __________________________________________ CLASS NAME: _____________________________________________ SOCIAL SECURITY - LAST 4 # ___________________ BIRTHDATE: _______________________________ HOME PHONE: _______________________________ CELL & WORK PH: _____________________________ INSTRUCTOR: ________________________________ BUILDING NO./NAME:_________________________ DATE OF INJURY/ILLNESS:__________TIME:_____ AM PM 1) DID INCIDENT OCCUR ON DISTRICT PREMISES: □YES □ NO CLASS TIME BEGAN: _____ AM PM WHERE DID IT OCCUR: __________________________ 2) NATURE OF INJURY/ILLNESS – describe: twisted, struck, fell… & body part affected – example- right/left arm, swollen, etc. _____________________________________________________________________________________________________ 3) What were you doing when injured? Specify activity and identify tools, equipment or material, if any, you were using. _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ 4) What type of safety equipment, if any, is required for this activity?____________________________________________ 5) Were you following prescribed safety procedures, including use of safety equipment? □ □YES □ NO □ 6) Have you ever been treated for a similar injury/illness? YES NO IF YES, what date?______________ Name and address of treating physician at that time:_____________________________________________________ 7) Name(s) of any witnesses to this particular incident:________________________________________________________ 8) What do you recommend for preventing this type of injury? (State specific preventive measures): _____________________________________________________________________________________________________ DO YOU REQUIRE OR DESIRE MEDICAL ATTENTION AT THIS TIME? □ YES If so, you must request a Medical Service Order from Human Resources prior to obtaining medical service. □ I already received emergency medical treatment (provide doctor’s report) (or if there has been an injury-reporting delay). □ NO If not, please initial here: ___________ NOTE: Medical treatment may be requested at a later date but you will need a Medical Services Order form from Human Resources BEFORE obtaining medical services. I declare under penalty of perjury that the foregoing is true and correct and that I have received current information regarding my benefits (attached pamphlet). Signature of Employee: ___________________________________________ Date report completed: ____________________ HUMAN RESOURCES USE ONLY: Date Report Received________ Date Form or Email to Supervisor:_________ 10/21/2014 □ NO □YES File only, no action □ PROVIDED DWC-1