Handling drug-related problems in rehabilitation patients: a randomized study
advertisement

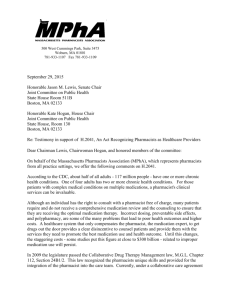
Int J Clin Pharm (2012) 34:382–388 DOI 10.1007/s11096-012-9623-5 RESEARCH ARTICLE Handling drug-related problems in rehabilitation patients: a randomized study Karin Willoch • Hege Salvesen Blix • Anne Marit Pedersen-Bjergaard • Anne Kathrine Eek Aasmund Reikvam • Received: 15 May 2011 / Accepted: 17 February 2012 / Published online: 3 March 2012 Springer Science+Business Media B.V. 2012 Abstract Background Drug-related problems (DRPs) have been found to be associated with increased morbidity, mortality, and health costs. Objective To investigate whether the inclusion of pharmacists in a rehabilitation team influences the handling of DRPs in the ward and whether an intervention in hospital affects drug use after discharge. Setting The rehabilitation ward of a general hospital in Oslo, Norway. Methods Patients were randomized into an intervention group (IG) or a usual care group (CG). The IG patients were followed prospectively by a pharmacist, who reviewed the patients’ drug therapies using information from their medical records and patient interviews. The pharmacist identified DRPs and suggested solutions during multidisciplinary team meetings. The IG patients received targeted drug counselling from the pharmacist before discharge. The drug therapy in the CG, for the period from study randomization to discharge, was assessed retrospectively by the pharmacist, who identified DRPs and recorded how they were acted upon. Three months after discharge, pharmacists who were blinded to the patient randomization, K. Willoch (&) H. S. Blix A. M. Pedersen-Bjergaard A. K. Eek Lovisenberg Diakonale Hospital Pharmacy, Lovisenberggate 17, 0440 Oslo, Norway e-mail: karin.willoch@apotek.no H. S. Blix Department of Pharmacoepidemiology, Norwegian Institute of Public Health, Oslo, Norway A. Reikvam Department of Pharmacology/Department of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway 123 visited the patients at home and interviewed them about their medication. Main outcome measures: Types and frequencies of DRPs in the IG and CG were compared at hospital admission, at discharge, and 3 months after discharge. Results Of the 77 patients included, 40 belonged to the IG and 37 to the CG. Patient characteristics (IG vs CG) were as follows: age 73.5 versus 76.8 years; female 58 versus 68%; mean number of drugs at admission 8.3 versus 7.8; and mean number of drugs at discharge 8.5 versus 7.7. At admission, 4.4 DRPs per patient were recorded in the IG and 4.2 in the CG. Significantly more DRPs were acted upon and resolved in the IG; at discharge, the IG had 1.2 DRPs per patient and the CG had 4.0 (P \ 0.01). At the home visit, a significant difference between the groups was found: 1.63 versus 2.62 DRPs (P = 0.02) for the IG and the CG, respectively. Conclusion Involvement of a pharmacist in drug-therapy management, including participation in multidisciplinary team discussions, markedly improved the identification and resolution of DRPs during a hospital stay. The benefit persisted after discharge. Keywords Clinical pharmacy Drug-related problem Medication review Norway Randomised trial Rehabilitation ward Impact of findings on practice • • • The participation of pharmacists in hospital multidisciplinary teams markedly improves the identification and resolution of DRPs during hospital stays. This benefit—reduced number of DRPs—persists after discharge. Changes in patients’ medication in hospital frequently generate compliance problems after discharge. Int J Clin Pharm (2012) 34:382–388 Introduction Drug-related problems (DRPs) have been found to be associated with increased morbidity, mortality, and health costs [1–3]. Many hospital admissions are the results of adverse drug reactions, and a sizeable proportion of these are regarded as preventable [4–6]. Therefore, reducing DRPs should benefit both patients and society. Strategies to optimize drug therapy in hospitals have been developed and the results of a multidisciplinary approach, involving the expertise of clinical pharmacists, have been promising [7]. During hospitalization, patients’ drug therapies are frequently changed [8, 9]. New drugs are added, doses are adjusted, and existing drugs are discontinued. This is challenging for the patient, and, once at home, the patient might be confused about which drugs and doses are still applicable. Pharmacist counselling during and after hospitalization may reduce DRPs and mortality [10, 11]. In general, few randomized controlled studies have assessed the inclusion of clinical pharmacists in hospital care teams. The few that have been undertaken predominantly investigated patients admitted to acute care wards, such as intensive care units and acute medical clinics, etc. [7, 12]. On rehabilitation wards, patients are beyond the acute stage of illness and there is time to optimize and stabilize their therapies. Furthermore, at this time, patients are in a phase that is well suited to supervision. Whether clinical pharmacists could contribute to the optimization of the drug therapies of rehabilitation patients has not yet been investigated. 383 for training and rehabilitation to a rehabilitation ward at Lovisenberg Diakonale Hospital, a general hospital in Oslo, Norway, were eligible for the study. The patients were admitted for either medical or surgical rehabilitation. Study participants were included if they used at least three drugs on a daily basis and were clinically judged to have adequate cognitive function. Patients were excluded if there were plans to discharge them to a nursing home or if they had professional help to take their medication at home. The study was carried out between November 2005 and February 2008. The usual length of stay in the rehabilitation department is 3 weeks, so it provides a convenient setting for health-care professionals to evaluate and adjust patients’ medicine regimens. A clinical pharmacist enrolled the patients into the study (Fig. 1). At admission, all eligible patients underwent a general interview, based on a standardized questionnaire designed for this purpose. The questionnaire included open questions about actual drug use and the patient’s knowledge of his/her own medications, as well as whether he/she had experienced any adverse drug reactions or insufficient efficacy of the drug therapy. The patients were then randomized into either the intervention group (IG) or the usual care group (controls, CG). The IG patients were followed prospectively during their hospital stays by a clinical pharmacist, who reviewed the patients’ drug therapies using information available in Aim of the study We used a prospective randomized controlled methodology to investigate whether pharmacists, as part of a multidisciplinary care team, improve drug therapy and prevent inhospital DRPs in rehabilitation patients, and assessed whether this intervention would affect drug use after discharge. Methods Patients and study design A prospective randomized controlled trial was designed. Hospitalized patients receiving usual care were compared with patients receiving care from a multidisciplinary team that included a clinical pharmacist, who was involved in the patients’ medical treatment from immediately after randomization (see below) until discharge. Patients admitted Fig. 1 Study design (flow chart) 123 384 the hospital medical records, laboratory data, and the standardized interview form (see above). If there were any discrepancy between the hospital medical records and the drug use reported by the patient, the patient’s general practitioner (GP) was contacted. During this advanced medication review and during the patients’ stay in hospital, the clinical pharmacist identified any DRPs, and most of these were discussed in the meetings of the medical multidisciplinary team led by physicians. Moreover, through a patient counselling talk before discharge, the pharmacist systematically informed the IG patients about their medications, particularly about any changes in their drug therapies. In this way, the entire intervention undertaken was the inclusion of the clinical pharmacist in the multidisciplinary care team. The CG patients were given usual care, insofar as a pharmacist was not part of their treatment teams. No pharmacist counselling was given at discharge. In both groups, counselling by physicians was part of the usual clinical routine. After discharge, the CG patients were reviewed retrospectively by the same clinical pharmacist who followed the IG patients. For the CG, DRPs at admission and at discharge were identified using information from hospital medical records, laboratory data, and the standardized interview undertaken at admission, i.e., before randomization. For example, identification of adverse drug reactions in the CG at discharge was based on information from the medical records. For both the IG and CG patients, a follow-up home visit by pharmacists was carried out 3 months after discharge, an interval that was regarded as appropriate for the evaluation of any possible post-discharge effects of the intervention undertaken in hospital. At home, the patients went through the same type of interview as the admission interview, and the same standardized questionnaire was used. However, the pharmacist who conducted the home interview did not have access to the patient’s medical records or laboratory data. This was because of privacy protection. Only members of the multidisciplinary care team who were involved in the patient’s treatment, were allowed access to the medical records. For this reason, no information on diagnoses or risk factors was available. However, the patient’s discharge medication list (information routinely given to all patients) was used as background information when the pharmacist was preparing for the home visit. The power estimation of the study showed that with 40 patients in each group and an estimated average of two DRPs per patient, it would be possible to identify a difference of 0.31 DRPs between the groups with a power of 80% and a significance level of 5%. The study protocol was approved by the Regional Committees for Medical and Health Research Ethics and the study participants gave their written informed consent. 123 Int J Clin Pharm (2012) 34:382–388 Randomization and blinding After enrolment in the study, the participants were randomized to either the IG or the CG. Block randomization was applied, with blocks of 20 patients. The clinical pharmacist who carried out the intervention knew whether the patients belonged to the IG or CG, but the physicians and nurses in the department were blinded to the group assignments. The pharmacists who visited the patients at home were blinded to whether the patients belonged to the IG or CG. Data collection During the hospital stay, the following data were recorded from the medical chart of each patient: age, sex, presenting complaints, medications (brand name, formulation, strength, dose), changes in drug therapy during the hospital stay, relevant medical history, and the results of laboratory tests. Specific factors that are assumed to increase the risk of DRPs were also recorded. These, which by nature are a composition of pharmacological, clinical, and patient-related factors, here called ‘clinical/pharmacological risk factors’ were the following: polypharmacy (defined as[5 drugs at admission), reduced renal function [glomerular filtration rate (GFR) below 60 mL/min, as calculated with the Modification of Diet in Renal Disease (MDRD) formula], reduced liver function (aspartate aminotransferase or alanine aminotransferase three times above the normal value), confirmed diabetes mellitus, cardiac failure, history of allergy or adverse reactions to drugs, non-compliance reported in the medical record, and the use of drugs with narrow therapeutic index. We also recorded abuse of alcohol, centrally acting psychostimulants, and benzodiazepines or opioids when these were reported in the medical record. From the patients’ interviews at admission, the following data were collected: medication used before hospital admission, patient’s knowledge of his/her own drugs (name, formulation, strength, dose, administration, and indication), possible adverse effects, and insufficient drug effects, if experienced. At the home visit, the patient’s ongoing medications were recorded, together with the same type of information obtained in the admission interview. Drug-related problems ‘‘DRPs’’ were defined in accordance with the definition of the Pharmaceutical Care Network Europe: a drug-related problem is an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes [13]. In this study, a classification system containing six main classes (drug choice, dosing, adverse drug Int J Clin Pharm (2012) 34:382–388 reactions, interactions, drug use, and others) was used to categorize the DRPs [14]. This is a validated classification system used in clinical practice in hospitals, nursing homes, and ambulatory care in Norway. The data collectors had been using the system in their daily work as clinical pharmacists, so the system was well suited for the classification of the DRPs in a standardized way. Drug interactions were only recorded when they were clinically relevant to the individual patient. The subdivision of the main DRP classes appears in Table 2. The DRPs noted at admission and discharge were recorded either prospectively (IG) or retrospectively (CG). The DRPs experienced by patients at home were recorded if they were related to the medications the patients were taking at the time of discharge and still used at the time of the home visit. If the DRPs had been resolved by the patient’s GP or if a DRP was related to changes to the patient’s drugs/medication made after hospital discharge, they were not included. Statistical analysis A database was established. The data were analysed using SPSS 17.0 for Windows. Descriptive statistics are shown as means and frequencies with standard deviations. P values less than 0.05 (P \ 0.05) were deemed to be statistically significant. To test the differences between groups, an independent-samples t test was used for continuous variables and a Chi-square test was used for categorical variables. Results A total of 77 patients were included, 40 in the IG and 37 in the CG; three patients, all belonging to a total of 40 in the CG group, were lost to follow-up immediately after the randomization and data on these were not included in the result analyses. Table 1 presents the patient characteristics and shows that the two groups were well balanced before the intervention. Of the 77 enrolled patients, 59 were visited at home 3 months after discharge, 30 in the IG and 29 in the CG. The reasons that the other home visits were not made were: five patients had moved to nursing homes; six did not want or were unable to have home visits; no contact could be made with five patients; and two patients had died. At admission, 176 DRPs were identified in the IG (4.4 DRPs per patient) and 155 DRPs in the CG (4.2 DRPs per patient). The corresponding figures in the two groups at discharge were 49 DRPs (1.23 DRPs per patient) in the IG and 148 DRPs (4.0 DRPs per patient) in the CG, implying a 385 reduction of 72% in the IG patients and of 5% in the CG patients. Table 2 shows the DRPs for the IG and CG at hospital admission and at discharge. The most common DRP in both groups was medication chart error, mainly related to imperfect or insufficient information about the patient’s medication before hospital admission. This DRP occurred so frequently that it was taken out of the category others and specified separately. The structured patient interview performed at admission identified 30% of all DRPs at admission, so these DRPs would have remained undetected if the patients had not been interviewed by the pharmacist. Medication chart errors, compliance problems and adverse drug reactions were most often only detected in patient interviews. The remaining DRPs identified at admission were detected by the pharmacist through the use of medical records and laboratory data. Table 3 shows the types and frequencies of the DRPs recorded 3 months after discharge. At the home visits, the most frequent DRP identified in both groups was patient compliance problems (category drug use). Fifty-four of the 125 DRPs registered at home belonged to this category. Half of the compliance problems (27/54) were directly related to changes made in medication during the hospital stay. In the IG, 11% of patients (3/30) did not use their medication appropriately (i.e., they were non-compliant) because of misunderstanding, compared with 38% (11/29) of the patients in the CG (P = 0.015). The types of noncompliance were: continued use of drugs that had been discontinued in hospital; non-use of hospital-prescribed drugs; and misunderstandings about the new dosage regimens. Three months after hospital discharge, 11 of 40 patients in the IG and 10 of 37 in the CG had been readmitted to hospital, and one patient in each group had died. Discussion In this randomized study, we demonstrated that the participation of a pharmacist in a hospital multidisciplinary team substantially reduced the number of DRPs observed in rehabilitation patients. Other researchers have reported benefits from pharmacists’ participation in the identification and handling of DRPs in other types of wards [7, 12, 15–20]. Although the inclusion of a pharmacist in the multidisciplinary team was the only intervention, the positive effects might be partly attributable to factors other than just the pharmacist’s practical handling of the DRPs. It is likely that a synergistic effect was achieved with the multidisciplinary collaboration. Communication between team members with different skills allows a more comprehensive evaluation and probably results in improved pharmacotherapy. Among 123 386 Int J Clin Pharm (2012) 34:382–388 Table 1 Demographic characteristics, number of drugs, number of clinical/pharmacological risk factors, and number of drug-related problems (DRPs) of the 77 study patients Intervention group (N = 40) Sex, female, % (no.) 57.5% (23) Control group (N = 37) 67.6% (25) P value 0.48 Mean (SD) [range] Mean (SD) [range] Age No. drugs on admission 73.5 (12.153) [33–96] 8.25 (2.99) [4–15] 76.8 (11.71) [42–94] 7.8 (2.55) [3–13] 0.22 0.47 No. drugs at discharge 8.53 (3.54) [2–18] 7.7 (2.52) [2–13] 0.25 % (No.) % (No.) Clinical/pharmacological risk factors Diabetes 20 (8) 19 (7) 0.57 Heart failure 17.5 (7) 19 (7) 0.55 Polypharmacy ([5 drugs) 75 (30) 76 (28) 0.58 Renal impairment, GFR B 60 mL/min Reduced liver function 27.5 (11) 0.3 (1) 32 (12) 0 0.57 0.34 History of allergic reactions/ADRs 15 (6) 24 (9) 0.31 Known non-compliance 5 (2) 5 (2) 0.94 Misuse of alcohol/drugs 30 (12) 19 (7) 0.27 Use of narrow therapeutic index drugs 40 (16) 40.5 (15) 0.57 No. DRPs per patient on admission 4.40 (2.88) [0–13] 4.19 (2.78) [0–12] No. DRPs per patient at discharge 1.23 (1.21) [0–5] 4.0 (2.24) [0–11] Home visit (N = 59) (N = 30) 0.74 \0.01 (N = 29) No. drugs at home 8.93 (3.98) [1–17] 8.0 (2.58) [2–13] 0.29 No. DRPs per patient at home 1.63 (1.40) [0–5] 2.62 (1.74) [0–7] 0.02 Standard deviations (SD) are given in parentheses and ranges in square brackets other things, the direct communication between pharmacists and other staff members during ward rounds or in the multidisciplinary team meetings, where prescribing decisions are made, allows the pharmacist to explain the background of his/her recommendations. All types of DRPs were reduced between admission and discharge in the IG, but in particular, ‘‘medication chart errors’’ showed the most substantial reduction. In contrast, in the CG, the total number of DRPs and the DRP pattern remained largely unchanged. The lower level of chart errors in the IG at discharge was attributed to the pharmacists’ intervention, thus confirming the benefit achieved by including a pharmacist in the drug reconciliation process. Moreover, it seems clear that unintended discrepancies between the medication regimens in hospital and at home were a common problem. This has also been reported by others [21, 22]. The patients’ compliance was notably improved in the IG. Several studies have approached the problem of patient compliance and a recent Cochrane report concluded that drug adherence in patients with chronic health conditions is complex and that new methods are required to improve 123 compliance [23]. Our results indicate that pharmacists are particularly well suited to address the compliance problem. A strength of our study is its randomized controlled design, in contrast with similar studies, which have been observational. In fact, to the best of our knowledge, this is the first randomized study of DRPs in rehabilitation patients. The pharmacists who identified the DRPs during the home visit 3 months after hospital discharge did not participate in the hospital part of the study and they were blinded to whether the patients belonged to the IG or CG. This circumvented any information bias. One limitation of the study was the temporal difference between the two groups in the identification of the DRPs present in hospital: the IG was followed prospectively and the DRPs of the CG were assessed retrospectively after discharge. This could have led to fewer observed DRPs in the CG, because less information was available to the pharmacist who identified the DRPs retrospectively. Ethical considerations were taken into account when a retrospective approach was chosen for the CG group. The pharmacist could not passively follow the control group prospectively without intervening if he/she became aware of potentially harmful Int J Clin Pharm (2012) 34:382–388 Table 2 Types and numbers of DRPs at admission and at discharge in 77 hospitalized patients 387 Categories of DRPs 1. Drug choice 23 52 53 17 20 Unnecessary drug 15 4 13 9 Inappropriate drug choice 20 8 22 24 23 11 24 21 6 2 6 6 11 6 6 3 8 10 3 12 4. Drug interaction 5. Drug use Patient compliance Administrative error by health-care professionals 6. Others Need for monitoring Medication chart error arising from incorrect medical records Others Summary Table 3 Types and numbers of DRPsa recorded 3 months after discharge No. IG DRPs (N = 30) No. CG DRPs (N = 29) 5 15 Need for additional drug 1 3 Unnecessary drug Inappropriate drug choice 0 4 3 9 8 5 Too-high dose 4 1 Too-low dose 3 1 Non-optimal drug formulation or dosing schedule 1 3 10 19 3. Adverse drug reaction 4. Drug interaction 0 1 24 34 23 31 1 3 6. Others 2 2 Summary 49 76 5. Drug use Patient compliance Administrative error by healthcare professionals IG intervention group, CG control group a CG at discharge 11 3. Adverse drug reaction 2. Dosing CG at admission IG at discharge 57 Too-low dose Non-optimal drug formulation or dosing schedule 1. Drug choice IG at admission 22 Too-high dose Categories of DRPs No. CG DRPs (N = 37) Need for additional drug 2. Dosing The main DRP categories and subdivisions are given. IG intervention group, CG control group No. IG DRPs (N = 40) The method of identifying DRPs at the home visit differed somewhat from the method used in hospital because the medical records were not available to the pharmacists 15 2 5 8 4 2 5 6 17 3 20 15 16 3 20 14 60 8 49 45 7 4 8 51 4 39 1 1 33 2 0 2 4 176 49 155 148 DRPs. It is also noteworthy that our study could not distinguish which of the different tasks of the pharmacist was most powerful in reducing the DRPs. Our aim was to investigate the impact of the whole role executed by the pharmacist within the hospital care team. However, separate clinical pharmacy tasks, such as medication reconciliation and patient counselling before discharge, have been assessed in some studies [21, 22, 24, 25]. The results of the home visits showed a significantly lower number of DRPs in the IG than in the CG 3 months after discharge. This difference was attributed to the fewer DRPs in the IG at discharge, thus demonstrating that the benefit achieved between hospital admission and discharge was still present 3 months later. However, the DRPs could not be assessed with the same completeness at the home visits as in hospital because at the home visits, the pharmacists did not have access to the patients’ medical information. Therefore, the evaluation was largely based on the standardized questionnaire, direct patient communication, and information in the medication list provided by the hospital at discharge. Consequently, for example, the DRP ‘‘medication chart error’’, which was frequently recorded in hospital, was not evaluated at the home visit. Conversely, an obvious advantage of the home visit was that the pharmacists could check on the medicines in the patients’ possession in their homes. 123 388 Int J Clin Pharm (2012) 34:382–388 In Norway, there has been growing interest in medication reviews and patient counselling by pharmacists, both in ambulatory care and in hospital. Although no legal regulations have been put in place, the Norwegian Ministry of Health and Care has encouraged projects that provide information about how to improve the use of medicines [26]. Conclusion In conclusion, the involvement of a pharmacist in drug therapy management, including his/her participation in multidisciplinary team discussions, markedly improved the identification and resolution of DRPs during patients’ hospital stays. The benefit of the pharmacist’s involvement persisted after the patients were discharged. Acknowledgments We thank Jan Egil Røe and Anne Gerd Granås for their general support during the study, and Teresa Lüdde for database registration. Funding We thank the Norwegian Directorate of Health for financial support. Conflicts of interest None to declare. References 1. Ernst FR, Grizzle AJ. Drug-related morbidity and mortality: updating the cost-of-illness model. J Am Pharm Assoc. 2001;41: 192–9. 2. Winterstein AG, Sauer BC, Hepler CD, Poole C. Preventable drugrelated hospital admissions. Ann Pharmacother. 2002;36(7–8): 1238–48. doi:10.1345/aph.1A225. 3. Patel P, Zed PJ. Drug-related visits to the emergency department: how big is the problem? Pharmacotherapy. 2002;22(7):915–23. 4. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279(15):1200–5. 5. Beijer HJ, de Blaey CJ. Hospitalisations caused by adverse drug reactions (ADR): a meta-analysis of observational studies. Pharm World Sci. 2002;24(2):46–54. 6. Howard RL, Avery AJ, Slavenburg S, Royal S, Pipe G, Lucassen P, et al. Which drugs cause preventable admissions to hospital? A systematic review. Br J Clin Pharmacol. 2007;63(2):136–47. 7. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care: a systematic review. Arch Intern Med. 2006;166(9):955–64. 8. Kripalani S, Jackson AT, Schnipper JL, Coleman EA. Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–23. 9. Mansur N, Weiss A, Beloosesky Y. Relationship of in-hospital medication modifications of elderly patients to postdischarge medications, adherence, and mortality. Ann Pharmacother. 2008; 42(6):783–9. 123 10. Schnipper JL, Kirwin JL, Cotugno MC, Wahlstrom SA, Brown BA, Tarvin E, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–71. 11. Wu JY, Leung WY, Chang S, Lee B, Zee B, Tong PC, et al. Effectiveness of telephone counselling by a pharmacist in reducing mortality in patients receiving polypharmacy: randomised controlled trial. Br Med J. 2006;333(7567):522. 12. Gillespie U, Alassaad A, Henrohn D, Garmo H, HammarlundUdenaes M, Toss H, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894–900. 13. van Mil JW, Westerlund LO, Hersberger KE, Schaefer MA. Drug-related problem classification systems. Ann Pharmacother. 2004;38(5):859–67. 14. Ruths S, Viktil KK, Blix HS. Classification of drug-related problems. Tidsskr Nor Laegeforen. 2007;127(23):3073–6. 15. Castelino RL, Bajorek BV, Chen TF. Targeting suboptimal prescribing in the elderly: a review of the impact of pharmacy services. Ann Pharmacother. 2009;43(6):1096–106. 16. Kaur S, Mitchell G, Vitetta L, Roberts MS. Interventions that can reduce inappropriate prescribing in the elderly: a systematic review. Drugs Aging. 2009;26(12):1013–28. doi:10.2165/11318 890-000000000-00000. 17. Viktil KK, Blix HS. The impact of clinical pharmacists on drugrelated problems and clinical outcomes. Basic Clin Pharmacol Toxicol. 2008;102(3):275–80. 18. Nkansah N, Mostovetsky O, Yu C, Chheng T, Beney J, Bond CM, et al. Effect of outpatient pharmacists’ non-dispensing roles on patient outcomes and prescribing patterns. Cochrane Database Syst Rev. 2010;(7):CD000336. 19. Koshman SL, Charrois TL, Simpson SH, McAlister FA, Tsuyuki RT. Pharmacist care of patients with heart failure: a systematic review of randomized trials. Arch Intern Med. 2008;168(7): 687–94. 20. Spinewine A, Swine C, Dhillon S, Lambert P, Nachega JB, Wilmotte L, et al. Effect of a collaborative approach on the quality of prescribing for geriatric inpatients: a randomized, controlled trial. J Am Geriatr Soc. 2007;55(5):658–65. 21. Unroe KT, Pfeiffenberger T, Riegelhaupt S, Jastrzembski J, Lokhnygina Y, Colón-Emeric C. Inpatient medication reconciliation at admission and discharge: a retrospective cohort study of age and other risk factors for medication discrepancies. Am J Geriatr Pharmacother. 2010;8(2):115–26. 22. Gizzi LA, Slain D, Hare JT, Sager R, Briggs F III, Palmer CH. Assessment of a safety enhancement to the hospital medication reconciliation process for elderly patients. Am J Geriatr Pharmacother. 2010;8(2):127–35. 23. Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;(2):CD000011. 24. Hellström LM, Bondesson A, Höglund P, Midlöv P, Holmdahl L, Rickhag E, et al. Impact of the Lund Integrated Medicines Management (LIMM) model on medication appropriateness and drug-related hospital revisits. Eur J Clin Pharmacol. 2011;67(7): 741–52. 25. Hugtenburg JG, Borgsteede SD, Beckeringh JJ. Medication review and patient counselling at discharge from the hospital by community pharmacists. Pharm World Sci. 2009;31(6):630–7. 26. The Norwegian Ministry of Health and Care Services. http:// www.regjeringen.no/en/dep/hod/dok/regpubl/stmeld/20042005/ stmeld-nr-18-2004-2005-.html?id=406517. Accessed September 5, 2011.