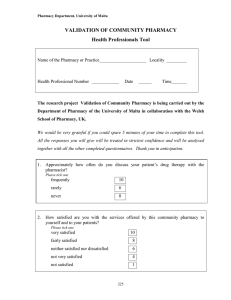
Name of the Pharmacy Locality Consumer Number Date Time External Validation Tool
advertisement

External Validation Tool Consumer Services Tool Name of the Pharmacy Locality Consumer Number Date Time We would be very grateful if you could spare some of your time so that we can interview you to complete this tool. All the responses you will give will be treated in strictest confidence and will be analysed together with all the other completed questionnaires. Thank you in anticipation. Approximately how often do you go to a community pharmacy? Please tick one at least once a week 2-3 times a month once a month less often 1. When you need to go to a pharmacy do you come to this pharmacy? Please tick one always 10 frequently 8 rarely 5 2. How satisfied are you with the services offered by this community pharmacy? Please tick one very satisfied 10 fairly satisfied 8 neither satisfied nor dissatisfied 5 not very satisfied 3 not satisfied 1 3. How do you rate the pharmacy on the following factors? the cleanliness of the Very Poor Fairly Poor Fairly Good Very Good 0 1 3 4 0 1 3 4 0 1 3 4 0 1 3 4 0 1 3 4 0 1 3 4 pharmacy the comfort and convenience of the waiting areas having in stock the medicines/appliances you need offering a clear and well organised layout how long you have to wait to be served having somewhere available where you could speak to the pharmacist in private without being overheard 4. How satisfied are you with the following characteristics of the pharmacist? (Please tick each characteristic) Please give an answer for each one Very Fairly Neither Not very satisfied satisfied satisfied satisfied Not satisfied nor dissatisfied 4 3 2 1 0 helpfulness of the staff 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 greeting by pharmacist The privacy of your conversations with the pharmacist politeness and professionalism of the staff efficiency with which the pharmacist deals with your request the pharmacist’s 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 professional relationship with you the advice given by the pharmacist when dispensing a medicine The pharmacist’s instructions about how to take your medications the written information the pharmacist provides you about drug therapy and/or diseases questions asked by the pharmacist before dispensing an overthecounter medicine how well the 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 pharmacist explains what your medication is and how it works the advice the pharmacist gives you about proper storage of your medication how well the pharmacist explains possible side effects How well the pharmacist works with your doctor to make sure your medications are the best for you 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 the amount of time the 4 3 2 1 0 3 2 1 0 the pharmacist’s interest in your health the advice given by the pharmacist on a current health problem or a longer term health condition providing general advice on leading a more healthy lifestyle how well the pharmacist answers your questions pharmacist offers to spend with you language used by the pharmacist (i.e. simple or complicated) 4 disposing of 4 3 2 1 0 4 3 2 1 0 medicines you no longer need providing advice on health services or information available elsewhere 5. Could you please rate the importance of the following factors? Please give an answer for each one Very Fairly Neither Fairly Very Important Important Important unimportant unimportant Nor unimportant longer 4 3 2 1 0 4 3 2 1 0 opening hours of the pharmacy pharmacist is accessible even when the pharmacy is closed the 4 3 2 1 0 4 3 2 1 0 4 3 2 1 0 pharmacist handles complaints efficiently having an area in the pharmacy to speak to the pharmacist in privacy diagnostic & monitoring services such as urine testing, cholesterol, blood sugar measuremen t and blood pressure monitoring keeping 4 3 2 1 0 patient medication records by the pharmacist. 6. How satisfied are you with the quality of advice you receive from the pharmacist? Please tick one very satisfied -10 fairly satisfied -8 neither satisfied nor disatisfied -5 not very satisfied -4 not at all satisfied -1 7. Have you ever been given advice about any of the following by the pharmacist or pharmacy staff? Yes No Stopping smoking 4 0 Healthy eating 4 0 Physical exercise 4 0 8. How likely are you to: Please give an answer for each one go to a Highly Likely Fairly likely Don’t know Not likely 4 3 2 0 4 3 2 0 pharmacist first when you feel a symptom confirm with your pharmacist the use of over-thecounter medicines follow the 4 3 2 0 advice given by the pharmacist 9. Which of the following best describes how you use this pharmacy? This is the pharmacy that you choose to visit if possible 10 This is one of several pharmacies that you use when you need to 5 This pharmacy was just convenient for you today 2 Remarks Total Grade