P I E
advertisement

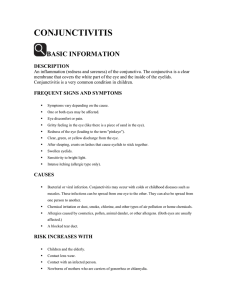
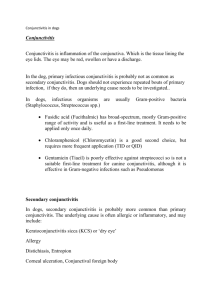
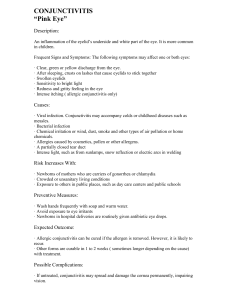
P ROTOCOLS I N EYE CONDITIONS PROTOCOL BOOKLET BIANCA MARIA S TIVALA This booklet was compiled by Bianca Maria Stivala as part of an undergraduate project entitled “Protocols in Eye Conditions” carried out for the partial fulfilment of the requirements of the course leading to the Degree of Bachelor of Pharmacy (Honours). The study was carried out under the supervision of Professor Lilian M. Azzopardi, Head of Department, Department of Pharmacy, University of Malta. The validation panel: Dr. Joseph Farrugia, M.D., M.M.C.F.D. Mr. Demis Fsadni, B.Pharm. (Hons.) Dr. Marco Grech, M.D., Cert. Diab. (ICGP), M.M.C.F.D. Dr. Jan Janula, M.D., Ph.D., S.D.S.Oph. (Prague) Mr. Franco Mercieca, M.D., F.R.C.Ophth. (UK) Mr. Mark Mercieca, B.Pharm. (Hons.) Sponsored by: Actavis Malta Ltd. Printed by: FiveStar Printing Ltd. The author makes no representation, expressed or implied, with regards to the accuracy of the information contained in this booklet and cannot accept any legal responsibility or liability for any errors or omissions that may be made. Bianca Maria Stivala Department of Pharmacy Faculty of Medicine and Surgery University of Malta Msida, Malta Published in August 2011 PROTOCOLS IN EYE CONDITIONS BIANCA MARIA S 2011 TIVALA PREFACE Pharmacists are commonly consulted about the management of signs and symptoms of common eye conditions. Pharmacists are in a position to identify signs and symptoms that require immediate referral. They are in a position to support patients in selfmanagement of dryness, conjunctivitis and external segment and eyelid conditions. In the management of eye conditions patients need to be educated about the proper use of ophthalmic medications. The protocols presented in this handbook have been developed by Bianca Maria Stivala, a pharmacy student as part of her project. This project is part of a research study being undertaken at the Department of Pharmacy with the aim of developing and disseminating protocols for the local scenario that are evidencebased. Professor Lilian M.Azzopardi Head, Department of Pharmacy CONTENTS How to use this booklet 2 Interpretation of shapes 3 Protocol for External Segment & Eyelid Conditions 4 Protocol for Conjunctivitis 10 Protocol for Dry Eye Disease 15 References 21 HOW TO USE THIS BOOKLET This booklet contains three flow chart protocols whose aim is to guide pharmacists in diagnosing and managing ocular conditions and recognising conditions which warrant referral. The protocols are guidelines compiled using evidence-based medicine, which when coupled with the pharmacist’s experience provide the best pharmaceutical care to the patient. This booklet is to be used with a companion explanatory text handbook which contains explanations and references for each protocol step. The text which corresponds with treatment and management steps provides more detail about pharmacological and non-pharmacological patient advice, which is of practical significance. The handbook is available online as a downloadable and printable A4 size document entitled “Protocols in Eye Conditions Handbook” at URL http://www.um.edu.mt/ms/pharmacy/research/protocols 2 INTERPRETATION OF SHAPES Data box Known information about the patient Action box Pharmacist is required to perform an action Yes Decision box Pharmacist is required to make a decision which leads to different paths No Connector box Directs pharmacist to another step on another page Terminator box Pharmacist is required to perform an action and exit the protocol 3 Step number label 3 EXTERNAL SEGMENT & EYELID CONDITIONS 1 Patient presents with inflammation of the eyelid and/or eyelid margin 2 Pharmacist greets patient 4 3 Is pharmacist familiar with patient? No Pharmacist asks questions to know identity of patient. Go to box 5. Yes 5 Does patient wear contact lenses? 6 Yes Refer No 7 Yes Go to box 8 4 Is there any lump or localised swelling present? No Go to box 25 From box 7 8 9 Is there any redness on the lump? No There is no redness on the lump Yes 10 Go to box 12 Patient reports tenderness to touch 12 11 Is the lump painful? No Swelling is tender but not painful Yes 13 Check if swelling points towards lid margin or towards conjunctiva Go to box 15 Go to box 14 5 EXTERNAL SEGMENT & EYELID CONDITIONS From box 13 15 14 Does swelling point towards lid margin? No Chalazion (meibomian cyst) Yes 19 Does the redness have a white/ yellowish core? No Evert patient’s eyelid after cl hands with an appropriate c agent Yes 20 External hordeolum (stye) No 21 Is there any pus on the inside of the eyelid? Yes Treatment Warm compresses applied 3-4 times daily for 10-15 minutes. Refer to general practitioner as antibiotic therapy is required. 6 Internal hordeolum 16 Did patient ever manifest these symptoms before? 17 Yes Refer No 22 leaning cleaning 18 Treatment Warm compresses applied twice daily for 3-5 minutes. The lesion should be massaged in the direction of the eyelashes with clean fingers or cotton tips. Refer to general practitioner if swelling does not subside or becomes red. 23 24 7 EXTERNAL SEGMENT & EYELID CONDITIONS From box 7 25 26 Does patient have seborrhoeic dermatitis of scalp and/or eyebrows? Yes Are there gr scales presen the eyelid Yes No Seborrhoeic ble 30 Are there dry scales present on the eyelid margin? No Go to box 26 Yes 31 Are there greasy scales also present? No Staphylococcal bleph Yes Treatment 33 Mixed infection blepharitis Warm compresses applied for seve Eyelid hygiene once daily or as oft effective may be required on a long Refer to general practitioner for appro 8 reasy nt on d? No Meibomian gland dysfunction (posterior blepharitis) 28 29 Treatment 27 epharitis Warm compresses applied for several minutes. Eyelid hygiene once daily or as often as required. If effective may be required on a long-term basis. Keep scalp, eyebrows, and other areas affected by seborrhoeic dermatitis clean by means of soap and water shampoo. Refer to general practitioner for appropriate antibiotic therapy. 32 haritis 34 eral minutes. ten as required. If g-term basis. opriate antibiotic therapy. 9 CONJUNCTIVITIS 1 Patient presents with a red eye 2 Pharmacist greets patient 4 3 Is pharmacist familiar with the patient? No Pharmacist asks questions to know identity of patient. Go to box 5. No 5 Are the eyes painful? 6 Yes Refer No 7 Does the patient wear contact lenses? No Go to box 9 10 8 Yes Refer From box 7 9 Yes Does the patient have physical injury? 10 Refer 14 Refer No 11 Check if redness is unilateral or bilateral. Yes 13 12 Are symptoms unilateral? Have symptoms been unilateral for more than 2 days? Yes No No 16 15 Were symptoms initially unilateral? No Yes Infectious conjunctivitis Go to box 22 Go to box 17 11 CONJUNCTIVITIS From box 15 17 Symptoms were always bilateral 18 19 Are the eyes itchy? No Refer Yes 20 Allergic conjunctivitis 21 Treatment Non-pharmacological advice: Minimise exposure to allergens as much as possible Wash clothes and fabric frequently Shower/bathe before bedtime Cool compresses to alleviate itching and remove any dry crusts Pharmacological treatment: Topical antihistamine/vasoconstrictor agent Topical histamine H1-receptor antagonist (levocabastine, emedastine) Artificial tears to dilute allergens (carboxymethyl cellulose, hydroxypropyl methylcellulose) For recurrent or persistent cases: mast cell stabilisers (sodium cromoglicate) 12 From box 16 23 22 No Is there any discharge present? Refer Yes 24 Is the discharge purulent/ mucopurulent? No No 25 Is the discharge serous (watery)? Yes Yes 28 26 Bacterial conjunctivitis Adenoviral conjunctivitis 27 Go to box 29 Treatment Supportive treatment with cool compresses, artificial tears and/or topical antihistamines. Give advice on good hygiene to prevent spread of infection (frequent hand washing, avoid sharing of towels and facecloths with other people) to other people and/or the other eye in cases where infection is still unilateral. Advise patient that infection remains contagious for up to 2 weeks after the second eye becomes infected. Refer to specialist if symptoms do not resolve within 2 weeks. 13 CONJUNCTIVITIS From box 28 30 29 Is there a palpable preauricular node? Yes Chlamydial inclusion conjunctivitis No 32 31 Is there associated blepharitis? No Acute bacterial conjunctivitis Refer 34 Yes Treatment 33 Chronic bacterial conjunctivitis Warm compresses and eyelid hygiene to remove blepharitis crusts. Refer to specialist for antibiotic treatment. 14 DRY EYE DISEASE 1 Patient presents with complaint of foreign body sensation 2 Pharmacist greets patient 4 3 Is pharmacist familiar with patient? No Pharmacist asks questions to know identity of patient. Go to box 5. Yes 5 Does patient wear contact lenses? 6 Yes Refer No 8 7 Does the eye appear red? Yes See conjunctivitis protocol No Go to box 9 15 DRY EYE DISEASE From box 7 Management 9 Does patient manifest symptoms of posterior blepharitis? Eyelid hygiene and Artificial tears app Increase intake of f reduce alcohol inge Yes Refer to ophthalmolog No 12 11 Is the patient exposed to cigarette smoke? Yes Dry eye due to expo to cigarette smok No 15 14 Is the patient using any topical products? No Go to box 17 16 Yes Dry eye due to use o topical products 10 d warm compresses applied at least once daily. plied 3-4 times daily or as required. foods containing omega-3 fatty acids and vitamin A; estion. gist is symptoms to not improve after one week. osure ke of Management 13 Reduce exposure to cigarette smoke. Increase intake of foods containing omega-3 fatty acids and vitamin A; reduce alcohol ingestion. Artificial tears applied 3-4 times daily or as required. Management 16 If patient is taking non-prescription medications: Advise patient to stop taking medication or suggest alternatives without preservatives. Dispense artificial tears to be applied 3-4 times daily or as required. Advise patient to wait 15 minutes before applying second product. If patient is taking prescription medications, refer to ophthalmologist for re-evaluation of treatment. 17 DRY EYE DISEASE From box 14 17 18 Is the patient female? Yes Is the patient taking oestrogen only HRT? No No 20 Is patient taking any systemic medications? No 21 No Go to box 25 Does the patient have symptoms of dry mouth? Yes 22 Sjögren’s syndrome Refer to rheumatologist 18 19 Yes Refer 23 Yes Dry eye as a side-effect of systemic medication 24 Management If patient is taking non-prescription medications: Advise patient to stop taking medications. Dispense artificial tears to be applied 3-4 times daily or as required. If symptoms do not improve refer to ophthalmologist. If patient is taking medications with specialist prescription, refer patient to specialist for re-evaluation of treatment. 19 DRY EYE DISEASE From box 17 25 Does the patient spend a long time in front of a screen or reading? 28 No Refer Yes 26 Episodic dry eye due to extended visual tasking 27 Management Environmental modifications: control humidity, take frequent breaks when using computer, blink frequently. Dietary modifications: increase intake of foods containing omega-3 fatty acids and vitamin A; reduce alcohol ingestion. Pharmacotherapy: artificial tears 3-4 times daily or as required. Refer to ophthalmologist if symptoms do not improve or if patient reports frequent use of artificial tears. 20 REFERENCES American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern® Guidelines. Blepharitis. San Francisco, CA: American Academy of Ophthalmology; 2008. American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern® Guidelines. Conjunctivitis. San Francisco, CA: American Academy of Ophthalmology; 2008. American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern® Guidelines. Dry Eye Syndrome. San Francisco, CA: American Academy of Ophthalmology; 2008. Bertino JS. Impact of antibiotic resistance in the management of ocular infections: the role of current and future antibiotics. Clinical Ophthalmology 2009; 3: 507–521. Blenkinsopp A, Paxton P, Blenkinsopp J. Symptoms in the Pharmacy: A guide to the management of common illness. 5th ed. Oxford (UK): Blackwell Publishing Ltd.; 2005. Gaby AR. Nutritional Therapies for Ocular Disorders: Part Three. Altern Med Rev 2008; 13(3): 191-204. Galor A, Jeng BH. Red eye for the internist: When to treat, when to refer. Cleve Clin J Med 2008; 75(2): 137-144. Gayton J. Etiology, prevalence, and treatment of dry eye disease. Clinical Ophthalmology 2009; 3: 405-412. Gilchrist H, Lee G. Management of chalazia in general practice. Aust Fam Physician 2009; 38(5): 311-314. Granet D. Allergic rhinoconjunctivitis and differential diagnosis of the red eye. Allergy Asthma Proc 2008; 29: 565-574. Høvding G. Acute bacterial conjunctivitis. Acta Ophthalmol 2008; 86: 5–17. Khurana AK. Comprehensive Ophthalmology. 4 th ed. New Delhi (India): New Age International (P) Ltd.; 2007. 21 REFERENCES Manaviat MR, Rashidi M, Afkhami-Ardekani M, Shoja MR. Prevalence of dry eye syndrome and diabetic retinopathy in type 2 diabetic patients. BMC Ophthalmol 2008; 8:10. Martin EA, editor; Oxford Concise Colour Medical Dictionary. 4th ed. Oxford (UK): Oxford University Press; 2007. Morrow GL, Abbott RL. Conjunctivitis. American Family Physician. February 15, 1998. Available at: www.aafp.org/afp/980215ap/morrow.html Riordan-Eva P, Whitcher JP, editors; Vaughan & Asbury’s General Ophthalmology. 17th ed. USA: McGraw-Hill Lange; 2007. Schlote T, Rohrbach J, Grueb M, Mielke J. Pocket Atlas of Ophthalmology. Stuttgart (Germany): Thieme; 2006. Sharma NS, Ooi JL, Li MZ. A painful red eye. Aust Fam Physician 2009; 38(10): 805-807. Tarabishy AB, Jeng BH. Bacterial conjunctivitis: A review for internists. Cleve Clin J Med 2008; 75(7): 507-512. 22