HD C I F
advertisement

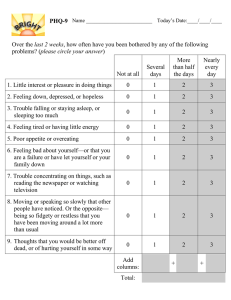
HDSA Center of Excellence at UC Davis Medical Center Rev. 10/2013 HD CLINIC INTAKE FORM Welcome to the HDSA Center of Excellence HD Clinic. Please take a moment to answer the questions below as best as you can. If you need assistance, a caregiver/companion may complete this form for you. Date: _________________________________________________ GENERAL HEALTH: Yes No 1. Have you had any changes to your general health and/or hospitalizations since your last visit with us? If Yes, please describe? 2. Did you visit a doctor, emergency room or experience any injuries since your last visit? If yes, please describe? Yes No 3. Are you having trouble swallowing or choking/coughing on foods or liquids? 4. Have you experienced any weight loss since your last visit? 5. Have you had any falls? 6. Do you exercise regularly? 7. How many days per week do you exercise? What type of exercise do you do? 8. Are you experiencing any difficulty with sleep? (i.e. trouble falling asleep, staying asleep, restlessness, etc.) If yes, please describe? 9. Have you completed an Advance Health Care Directive, Living Will or Durable Power of Attorney for Health Care? --If no, would you like more information about this subject? HDSA Center of Excellence at UC Davis Medical Center 1 HDSA Center of Excellence at UC Davis Medical Center Rev. 10/2013 MOVEMENT: Yes No 1. Are you having chorea? If you answered YES, please use the scale below to answer the additional questions. If you answered NO, please skip to Thinking Skills on this page. Very Disruptive Not at all 2. How much is the chorea bothering you? 1 2 3 4 5 3. How much is it bothering your caregiver/partner? 1 2 3 4 5 4. How much does your chorea interfere with your ability to do things? 1 2 3 4 5 THINKING SKILLS: Have you or your companion/caregiver noticed any difficulties with the following tasks? Yes No Keeping track of schedules and/or organizing things? Being unaware of your HD symptoms? Not understanding things that are said to you? Having trouble concentrating or paying attention? Having trouble initiating activities or conversations? Problems with memory? Any difficulties with speaking or making conversation? Keeping track of appointments and/or taking your medications? FUNCTIONAL STATUS: Are you having any difficulties in your ability to do any of the following activities? Yes No Describe difficulties Ability to work Managing money/finances Ability to do usual chores Ability to perform grooming, bathing or dressing Ability to feed yourself Ability to drive safely Do you need caregiving help from your family member or others? HDSA Center of Excellence at UC Davis Medical Center 2 HDSA Center of Excellence at UC Davis Medical Center MEDICAL EQUIPMENT: Are you currently using any medical assistive devices? Yes No Cane Bathroom rails/safety bars Walker Raised toilet seat Wheelchair Bath/Shower bench or chair Bedside Commode Hand held shower nozzle Hospital Bed Other ___________________ Rev. 10/2013 Yes No MOOD: Have you or your family noticed any difficulties in your mood or behavior since your last visit? None Mild Moderate Severe Sadness/Depression Irritability Anxiety Anger outbursts or aggression Obsessional thoughts Compulsive behaviors Apathy (lack of energy) Impulsiveness Difficulty initiating activities Have you experienced any suicidal thoughts since your last medical visit? None Fleeting Actively Planning **Please also complete the PHQ-9 on the following page with additional questions about your mood.** HD RESEARCH: Yes No Maybe Are you interested in participating in HD Research at this time? Would you give your permission to be contacted in the future about research you may be eligible for? Please complete the information below if you are willing to be contacted for HD research? Name: Address: Contact Numbers: Signature: HDSA Center of Excellence at UC Davis Medical Center 3 HDSA Center of Excellence at UC Davis Medical Center Rev. 10/2013 Patient Health Questionnaire (PHQ-9) Over the last 2 weeks, how often have you been bothered by any of the following problems? (Please put an “X” to indicate the best answer) More than half the days Nearly every day Not at all Several days 1. Little interest or pleasure in doing things 0 1 2 3 2. Feeling down, depressed or hopeless 0 1 2 3 3. 0 1 2 3 4. Trouble falling or staying asleep, or sleeping too much Feeling tired or having little energy 0 1 2 3 5. Poor appetite or overeating 0 1 2 3 6. Feeling bad about yourself—or that you are a failure or have let yourself or your family down Trouble concentrating on things, such as reading the newspaper or watching television Moving or speaking so slowly that other people could have noticed. Or the opposite—being so fidgety or restless that you have been moving around a lot more than usual Thoughts that you would be better off dead, or of hurting yourself in some way 0 1 2 3 0 1 2 3 0 1 2 3 0 1 2 3 7. 8. 9. Add columns + + TOTAL 10. If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home or get along with other people? Not difficult at all Somewhat difficult Very difficult Extremely difficult PHQ-9 is adapted from PRIME MD TODAY, developed by Drs Robert L. Spitzer, Janet B.W. Villiams, Kurt Kroenke, and colleagues, with an educational grant from Pfizer Inc. For research information, contact Dr. Spitzer at rls8@columbia.edu. Use of the PHQ-9 may only be made in accordance with the Terms of Use available at http://www.pfizer.com. Copyright 1999 Pfizer Inc. All rights reserved. PRIME MD TODAY is a trademark of Pfizer, Inc. Are there any other issues you would like to discuss today? HDSA Center of Excellence at UC Davis Medical Center 4