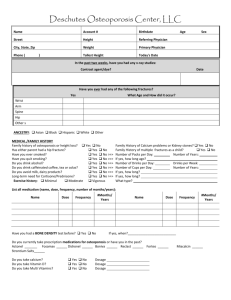
DATE:_______________________________ WEIGHT__________________________ AM PM
advertisement

DATE:_______________________________ WEIGHT__________________________ AM PM TEMPERATURE BLOOD PRESSURE/HEART RATE BREAKFAST LUNCH DINNER BEDTIME BLOOD SUGAR INSULIN DOSE MEDICATIONS TIME NAME OF MEDICINE DOSAGE (mg) *Use the other side of this page to document any questions or findings that you think are out of the ordinary for this day. You may refer to it at a later visit or if a problem should arise.