Cognitive development in VCFS
advertisement

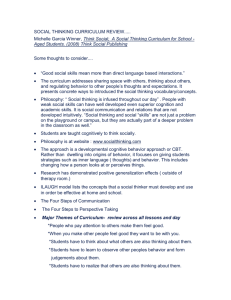
Progress in Pediatric Cardiology 15 (2002) 109–117 Cognitive development in VCFS Tony J. Simona,b,*, Carrie E. Beardenb, Edward M. Mossb, Donna McDonald-McGinnb, Elaine Zackaia,b, Paul P. Wanga,b a University of Pennsylvania School of Medicine, Philadelphia, PA, USA b Children’s Hospital of Philadelphia, Philadelphia, PA, USA Abstract The 22q11.2 microdeletion (velocardiofacial syndrome, VCFS) results in a complex pattern of psychoeducational and neurocognitive deficits. Mean full-scale IQ scores are in the range of borderline intellectual function, but academic achievement scores are generally in the low–normal range. A dichotomy is often found between higher Verbal IQ scores and lower Performance IQ, paralleled by relative strength in Reading and Spelling, but weakness in Math. Language skills are also typically delayed and remain impaired later in life, and psychiatric disorders can be found in both children and adults with the syndrome. On-going neurocognitive research suggests that the impairment in mathematical ability may be associated with poor visual–spatial skills. This would be consistent with theoretical models that link arithmetic skills with visual attention and spatially referenced representations of magnitude. Neuroimaging investigations indicate that these skills may all depend critically on the inferior parietal lobes, and lead to our hypothesis that these may be dysfunctional in the 22q11.2 syndrome. Early reports find no association between cognitive ability in the syndrome and the presence of cardiac malformations. 䊚 2002 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Cognition; Neuropsychology; Numeracy; Visuospatial; Brain; Magnetic resonance imaging (MRI) 1. Introduction The purpose of this review is to address issues relating to the cognitive development of children with velocardiofacial syndrome (VCFS). Compared with work focusing on the medical implications of the syndrome, this is an area of relative novelty. Many questions have yet to be asked concerning the intellectual outcomes of affected children. These questions can be addressed at different levels and each requires its own set of methodologies. In this review, we focus on two levels of analysis where some progress has been made. The first is the area of standardized testing of intelligence, academic achievement and neuropsychological function. At present, this represents the largest body of knowledge regarding intellectual function in children with VCFS. Despite considerable variation in the phenotype, there is general consensus in the picture that has emerged. The second area, just getting underway, focuses on functional *Corresponding author. Children’s Seashore House, Rm. 207, 3405 Civic Center Boulevard, Philadelphia, PA 19104, USA. Tel.: q1215-590-7198; fax: q1-215-590-6804. E-mail address: tjsimon@mail.med.upenn.edu (T.J. Simon). neurocognitive analysis. Taking the neuropsychological testing data as its starting point, these studies are now examining specific cognitive processes and the neural substrates involved in their implementation in order to provide mechanistic and integrative explanations as to why certain clusters of cognitive dysfunction are observed. This work also will also lay the groundwork for subsequent cognitive interventions that may be able to reduce, or even remove, some deficits by ‘retraining’ the brains of children with VCFS early in development to process certain kinds of information in ways that are more suited to their areas of strength. Although some brain and cognition findings have been published about adults with VCFS, we focus this review on children. 2. Psycho-educational findings and neuropsychological What is known so far about the cognitive implications of VCFS? The broad psychoeducational picture is, in fact, fairly clear. Children with VCFS show mean fullscale IQ scores (FSIQ) in the range of borderline intellectual abilities, with verbal IQ (VIQ) significantly 1058-9813/02/$ - see front matter 䊚 2002 Elsevier Science Ireland Ltd. All rights reserved. PII: S 1 0 5 8 - 9 8 1 3 Ž 0 2 . 0 0 0 3 5 - 8 110 T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 Fig. 1. Psychoeducational and language profiles in VCF. Verbal IQ (VIQ) is typically higher than both Performance IQ (PIQ) and language (CELF) scores. Reading scores are typically higher than Math scores. Lines connect data from individual subjects; dashed lines indicate atypical profiles. higher than performance IQ scores (PIQ) w1–3x (Fig. 1). In the largest study to date, Moss et al. w1x reported a FSIQ of 71.2"12.8 (mean"standard deviation), VIQ 77.5"14.9, and PIQ 69.1"12.0, in a group of 33 subjects. Moss et al. w1x also reported a typical pattern of results on academic achievement tests (e.g. w2,3x). Math composite scores (80.1"15.2) were significantly lower than Reading composite (86.7"18.2) and composite Spelling scores (88.3"16.4). Thus, while many children with the 22q deletion often show IQ scores that are in the borderline or mild range of mental retardation, their academic achievement scores are typically in the low–average range or higher. A majority of children have IQ scores above the range of mental retardation, and moderate or severe retardation is rare w1,4x. Moss et al. pointed out that the profile of weakness in math, with a PIQ score lower than VIQ, resembles the profile known as a ‘Non-Verbal Learning Disorder’ (NVLD), because of the concentration of deficits in areas of visual–spatial cognition, which we discuss in more detail later. However, NVLD is probably something of a misnomer, since children with VCFS do show early deficits in verbal skills as well, some starting at an early age and typically persisting into later life w1,5x. In a study of early language development in children with VCFS below the age of 5 years 3 months, Gerdes and colleagues w6x found delays in the emergence of language skills in all 32 children assessed by a speech pathologist. A total of 20 from 32 children were not yet speaking when they reached 2 years of age. In addition, 14 of these children scored 2 or more standard deviations (S.D.) below the mean and 13 scored 1–2 S.D. below, on the Clinical Evaluation of Language Fundamentals test (CELF-R), a comprehensive assessment of language functions. Five had caught up and scored in the average range. Expressive language lagged behind receptive language with mean scores of 71.2"16.0 and 78.2"12, respectively. In the study by Moss et al. w1x of 33 VCFS patients from 6 to 27 years, it is clearly evident that language problems persist into the school years. A total of 20 children with similar FSIQ, VIQ and PIQ profiles to the whole group were tested on the CELF-R, and showed moderately impaired mean total scores (66.9"14.9). By this age, receptive and expressive scores no longer differed, but the total and expressive language scores were significantly lower than VIQ for this group (Fig. 1). In an overlapping group, full clinical evaluation revealed that 50% were diagnosed with specific language impairments involving receptive and expressive deficits. Clearly, there is not an absence of language problems in the NVLD-like profile, and these undoubtedly have a negative effect on developing cognition and educational outcomes. However, as we shall see, the T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 greatest deficits are to be found in other areas of cognitive function. In a larger group of patients (including those studied by Moss et al.), Woodin et al. w3x examined the more detailed neuropsychological profiles of 50 children with VCFS whose mean age was 10 years 3 months. Within neuropsychological domains, some interesting distinctions emerged. For example, in the domain of ‘executive function,’ subjects scored higher on tests requiring simple, focused attention than on tests that requiring more planning and cognitive flexibility. More detailed testing of reading comprehension also suggested that this was an area of weakness relative to the decoding of single words. Woodin et al. also reported that rote verbal memory skills were in the average to above-average range, while memory for stories was in the borderline range, as was memory for geometric objects. Therefore, these findings further support the picture of relative strength for simple verbal memory and simple reading skills compared to deficits in complex verbal memory, visual–spatial memory and math achievement. This final pair of weaknesses may be more than coincidental. Wang et al. w7x pointed out the link that has been established between deficits in visuospatial and arithmetical ability, but not reading or spelling difficulties. One of the most direct links comes from the work of Dehaene w8x, who makes the claim that some of the simpler numerical operations that are carried out, such as judging the relative magnitude of two values, are done on the basis of spatial representations that resemble an analog ‘number line’. Using the Kaufman Assessment Battery for Children, Wang et al. showed that almost two-thirds of the 36 school aged children with VCFS that they tested scored higher on the Number Recall subtest (verbal repetition of numbers) than the Spatial Memory subtest (remembering locations). The former scores were in the normal range, while the latter were 1 S.D. below it. This suggests that the problem is not some global numerical processing weakness, but can indeed be traced to spatial representations. Further evidence linking visuospatial and numerical deficits in these children comes from the study by Bearden et al. w9x, which employed specific tests of visual and language learning and memory functions on a population overlapping those studied by Moss et al. and Woodin et al. There were 29 children with VCFS between the ages of 5 and 17 years (mean 10.34 years). As expected, scores on visual–spatial memory were significantly lower than those for verbal learning. Furthermore, these children scored significantly higher on a test of memory for object designs than on a test of memory for spatial location. This distinction fits quite well with the distinct visual processing pathways in the human brain which process identity information about visual inputs (the so-called ‘what’ pathway) and location or information (the so- 111 called ‘where’ pathway) within separate neural substrates w10x. The patients of Bearden et al., it seems, had most trouble in processing location information in visual stimuli that would be primarily handled in the ‘where’ pathway, which runs from the primary visual cortex into the posterior parietal lobes. They had less trouble with featural information, processing of which would be primarily implemented by the ‘what’ pathway, running from the primary visual cortex into the inferior temporal cortex. 3. Cognitive process findings Therefore, everything we have reviewed so far, from IQ subscores to specific neuropsychological function tests, suggests that a common pathway between visuospatial and numerical deficits in VCFS may lie in the dysfunction of brain areas primarily responsible for representing spatial information and for supporting the cognitive functions common to visuospatial and numerical competence. A good deal of evidence points to the inferior parietal lobes (IPL) as that substrate. Clinical findings and cognitive experimentation have consistently reported that patients who suffer IPL damage due to stroke and other insults present with deficits in perception of peripersonal space w11x, visual attentional control w12x, and numerical competence w13x. Cognitive process studies have directly linked mechanisms involved in visual attention and enumeration w14,15x, and these mechanisms have been shown to rely on common neural substrates, a major component of which is IPL w16x. Finally, Dehaene’s w17x ‘triple code’ theory associates three kinds of numerical representations with specific brain areas or pathways. The mature store of numerical facts on which adults rely for exact calculation w18x are in left frontal language areas. Interpretation of visual forms, such as numerals or number words, takes place in the occipito-temporal ‘what’ pathway. Finally, analog magnitude representations are represented spatially in IPL, which is also the source of magnitude comparison and approximate calculation processing w18,19x. To investigate whether the reported numerical and visuospatial deficits in VCFS are indeed due to dysfunction in areas of IPL that are involved in visuospatial and numerical cognitive processes, we have recently embarked on a study employing cognitive tests and neuroimaging analysis specifically designed to evaluate that hypothesis. A group of 7–13-year-old children with VCFS is being compared to a group of their siblings. All children complete an ‘endogenous cueing’ task, an ‘enumeration’ task, and a ‘distance effect’ task in our lab. They also carry out a functional MRI (fMRI) version of distance effect task and undergo three structural MRI scans in order to measure the volume of brain tissue and the amount of and patterns of connectivity in white matter. 112 T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 Fig. 2. Example stimuli from Enumeration Task for (a) small (subitizing range) and (b) large (counting range) set sizes. (a) For small quantities, typical observers can quickly determine the number of objects without resorting to counting individual items. This process is known as ‘subitizing.’ (b) Larger quantities cannot be subitized, but must be counted to determine the number of objects. We use a Cueing experiment to evaluate visual orienting abilities. The task involves responding to a single target object flashed on the screen to the right or left of a central fixation point. The target’s appearance is preceded either by a ‘valid’ cue (pointing briefly to the side of the target’s appearance, and hence drawing attention there) or an ‘invalid’ cue (where the cue points to the opposite side and draws attention away from where the target will appear). The child’s task is to press one key for a target on the left and another for a target on the right. We predicted that children with VCFS would show increased difficulty in orienting attention in the absence of facilitatory information if there was parietal dysfunction involving directing and engagement processes. Our preliminary results show that patients perform no worse than their siblings when their attention is directed to the target location by a valid cue 400 ms before its appearance. However, if the target is preceded by a neutral cue, which does not direct attention to the target location, or an invalid cue, which directs attention to the wrong location and which requires IPL function to disengage that location and reorient to the correct location, reactions times are much longer and more errors are evident in the performance of the patients. This suggests that if children with VCFS need to search for and extract information within a complex scene (e.g. a map), they should be provided with strong cues to the critical information, such as the use of arrows or distinct colors. Problems with managing visual attentional orienting are likely to have contributed to the worse performance we predicted and observed for quantities larger than three on the part of children with VCFS in our enumeration experiment. Enumeration of just a few objects is known as ‘subitizing’ (Fig. 2a). This ability is largely captured by the experience of instantly ‘knowing’ how many entities comprise collections of up to three or four. It is thought to be implemented by widely focused, low-resolution attentional mechanisms that rely on extrastriate occipital cortex. In contrast, counting larger sets takes place through serial visual search (Fig. 2b) in which IPL plays an important role w16,20x, and for this reason we expected worse performance in that range. The task requires each child to sit in front of a computer screen and complete trials in which one to eight objects are displayed on the screen. The child’s task is to respond by speaking into a microphone, as quickly as possible, the number of objects that were presented. Our results showed no differences between patients and siblings in their ability to enumerate one or two objects. However, children with VCFS took increasingly longer and made increasing errors in their efforts to count sets as they increased in size. This suggests that children with VCFS might be able to count more accurately if objects can be grouped together in sets of no more than two objects. Based on Dehaene’s triple code theory, we also predicted that our VCFS patients might not show the standard ‘distance effect’. This is evident when individuals are asked to judge whether a given quantity is larger or smaller than some other reference quantity, e.g. five. Since judgments are thought to take place on spatially represented ‘number lines’ (constructed in IPL), quantities near the reference (e.g. four) are more confusable than those further away (e.g. one) and the judgment takes longer and produces more errors. However, we predicted that if there is some dysfunction in IPL that disturbs the association between space and quantity in the representations that are created, then this distance effect might not be seen. Our Distance Effect task is a replication of the one that Temple and Posner w21x successfully used with young children. The task involves making a judgment about whether the value of a stimulus is ‘greater than’ or ‘less than’ five. The T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 stimuli have the values one, four, six and nine. Each of the four stimuli is presented five times in both Arabic numeral and dot pattern form. As predicted, our preliminary data indicate that the siblings produced the normal distance effect of longer reaction times to four and six than one and nine for both stimulus types. However, the children with VCFS did not. For dot patterns, the patients took approximately the same time to judge the relative magnitude of one, four and six to five, with nine being the fastest. This stimulus type engages IPL for both stimulus interpretation (how many spatially arranged dots) and for the magnitude comparison itself. However, when the stimuli were in numeral form, which neuroimaging data (e.g. w19x) indicate would move some task processing to take place in the inferior temporal lobes, the patients’ performance came closer to exhibiting the actual distance effect. One implication of this finding is that children with VCFS may benefit from much earlier than usual mapping of quantities to some form of notation (either numerals or number words) to help them to represent more accurately the quantity they need to think about. We need to collect much more data to see if this pattern holds up, but, at present, it does appear that dysfunction in IPL, as detected by tasks which are heavily dependent on processes implemented by that neural substrate, may explain why children with VCFS have problems in the areas of visuospatial and numerical cognition. This also suggests that there may be cognitive interventions that can designed, so that, instead of waiting for these children to be diagnosed with numerical learning problems in early grade school, the problem can be intercepted early in life and children might be helped to form functional spatio-numerical representations in ways that their brains can handle. In order to do this, we must know whether there are brain regions that may be able to handle these reformatted tasks. To this end, we have recently begun fMRI experiments using the distance effect task with VCFS patients. A single child studied so far exhibited two interesting patterns. One is that there was little of the appropriate IPL activity that we would expect to see based on fMRI studies of normal adults or of ERP studies with children. The other is that quite diverse and perhaps unusual patterns of activation are evident. How unusual these really are can only be determined when we have imaged sufficient numbers of patients and unaffected control subjects to determine what the normal pattern of immature brain activity is. Eliez et al. w22x reported a related result from a study that required children with VCFS and control subjects to carry out simple arithmetic in an fMRI task. On the more difficult problems, patients showed higher levels of activation in the left supramarginal gyrus (SMG) within IPL than did the control subjects, which also suggested a relocation of processing in this higher-order task. There were also higher levels 113 of activation in patients on the difficult tasks in two large clusters of voxels, one extending from the left precentral gyrus to the left SMG, and the other from right insular areas to the right SMG. These unusually activated areas can be considered candidates for alternative processing sites if it can be established that their recruitment can be used to improve performance. Once we have established if there is a consistent pattern, we will need to go about the task of creating alternative processing trajectories to numerical competence that can exploit these functional and apparently ‘willing’ alternate regions. 4. Cognitive development and cardiac status An important question regarding the findings discussed above, particularly for this review, concerns the role of cardiac anomalies in these deficits. While the actual prevalence of cardiac defects associated with the deletion is not definitively known, such a diagnosis was made in 74% of the 250 patients observed by the Children’s Hospital of Philadelphia clinic w23x. The most common anomalies reported in an earlier survey of this sample were tetralogy of Fallot (TOF), interrupted aortic arch (IAA), ventricular septal disorder (VSD), and truncus arteriosus (TA) w23x. Clearly, cardiac problems cannot be the sole cause of cognitive deficits, as individuals with VCFS but without heart defects also show the intellectual profile described above w9 x . So far, no direct link between cardiac status and cognitive outcome has been established in the VCFS population, although it should be noted that no study focusing specifically on this question has yet taken place. Gerdes et al. w6x reported finding no association between cardiac diagnosis and outcome scores in their study of preschool children, in which 29 of 40 children involved had a cardiac anomaly. Swillen at al. w4x reported that FSIQ scores were actually higher in their child and adolescent subjects who had a heart defect than in those who did not. However, the difference was not statistically significant. Given the possibility that congenital heart defects (CHD) could affect cognitive skills, it is helpful to evaluate the mechanisms through which such effects could be transmitted. The two most obvious, which may not be independent of each other, are the effects of surgicalyanesthetic interventions, and the direct effects of abnormal cardiovascular physiology. In both cases, the damage would likely take place via the hypoxic– ischemic effects on brain tissue. With respect to surgical intervention, Bellinger et al. w24x evaluated developmental outcomes at 4 years of age in 158 children who had undergone arterial-switch operations for transposition of the great arteries (TGA). Although this malformation is not typically found in 114 T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 VCF, the profile of IQ scores in these subjects is reminiscent of the profile observed in VCF. These children showed a mean Verbal IQ score of 95.1, which was significantly higher than their mean Performance IQ score of 91.6. The authors state that ‘‘the subtests on which scores tended to the lowest were those that assessed visual-spatial and visual-motor integration skills (p. 527).’’ The subjects also showed below average scores on almost every measure of language skill that was administered. A diagnosis of VSD was an independent risk factor for lower IQ scores and speech apraxia. A separate study of 13-year-old children who had undergone repairs for hypoplastic left heart syndrome (HLHS) w25x also showed VIQ scores higher than PIQ scores, with weaknesses in language skills as well. Thus, by the age of four it appears that an effect of some heart defects or their repair on intellectual function can be measured, and that this effect resembles the profile of VCFS. However, the mean IQ scores of children with VCFS are notably lower than for children with either TGA or HLHS. Furthermore, the pathogenesis of these cognitive deficits remains unclear, bringing us to the second mechanism, the neurocognitive effects of pre- and post-natal hypoxia–ischemia. There appears to be some evidence that hypoxia–ischemia has a particularly negative impact on neural white matter, particularly in the periventricular regions w26x, and these effects can be well detected using diffusion-weighted MRI methods w27x. This is important, because quantitative MRI studies of the brains of children with VCFS have shown that there are considerable reductions in non-frontal lobar volumes and that the preponderance of that loss is in white matter w28,29x. Currently, the etiology of the specific cognitive and neuroanatomic profile in VCFS remains unknown. However, other physical anomalies that result from the 22q11.2 gene deletion, including the cardiac abnormalities and facial malformations, are thought to result from anomalous migration of the neural crest during early embryogenesis w30x. During this time, anomalies in events that are reliant on neural induction may produce secondary effects in proliferation or migration, thereby leading to cerebral white matter pathology w31x. The reports of focal white matter hyperintensities in VCFS patients offer tentative support for hypotheses of defective white matter. Also referred to as ‘leuko-araiosis’ or ‘lesions’, these white matter abnormalities are usually not present in healthy persons under age 45. Although of unknown etiology, the presence of these abnormalities is known to increase with age and with the existence of co-morbid medical conditions, and may indicate an underlying ischemia process w32–34x. Given the high prevalence of cardiac defects and cardiac repair in VCFS patients, these hyperintensities may represent effects of cardiac status, rather than an expression of the genetic deletion itself. Although the functional significance of white matter hyperintensities is not entirely clear at present, their presence has been associated with poorer cognitive function on neuropsychological tests in a number of studies w35,36x, suggesting that these structural brain abnormalities may mediate the cognitive impairments observed in VCFS. Recently, modern neuroimaging techniques have been brought together with cognitive studies to show that specific disruptions in white matter connectivity might account for deficits in reading ability w37x. These recent developments provide novel ways to determine the precise nature of cognitive deficits in VCFS, while at the same time providing another tool in the task of evaluating the role played by cardiac anomalies. They also offer the chance to examine a claim made by Rourke w38x that it is disturbances in white matter connectivity that are at the root of NVLD, the very pattern of cognitive deficit which seems to best characterize children with VCFS. 5. Psychiatric concerns A wide range of behavioral and psychiatric concerns has been reported in children with the 22q microdeletion. These include concerns related to hyperactivity and inattention, and anxieties and social withdrawal w4,6x. Studies utilizing parent report data (i.e. Child Behavior Checklist) indicate significantly elevated rates of attention and internalizing problems in children with VCFS w4,51,52x. It is not clear whether the attentional concerns are specific to the syndrome or whether they simply reflect the commonly observed traits of children with developmental disabilities, but the social skills deficits and anxieties may relate to the NVLD profile w1,2x. Autism also has been reported in a small number of children with the microdeletion w39x, but this again may be related to the mental retardation that is found in some subjects, rather than to the direct effects of the microdeletion. More severe psychiatric disorders have been reported in older adolescents and adults with VCFS. The first indication of these came from Shprintzen et al. w40x, who reported that a large percentage developed psychotic disorders. This finding was confirmed in subsequent reports, all of which noted an elevated incidence of schizophrenia and schizoaffective disorders among adults with this genetic condition w41x. Furthermore, at least four studies have demonstrated an overrepresentation of the 22q11.2 deletion in samples of persons with a diagnosis of schizophrenia; 2–6% of persons with schizophrenia in these samples had the 22q11.2 deletion w42,43x. Moreover, recent reports by Nicolson et al. w44x indicate that 3 of 47 children with child-onset schizophrenia were discovered to have a 22q deletion upon T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 115 FISH testing. Publications that address the association between VCFS and schizophrenia generally concur that 25–30% of children with the syndrome will eventually develop schizophrenia or psychosis w45x, making VCFS the highest known risk factor identified to date for development of this psychiatric disorder. However, the exact nature of the psychiatric manifestations of the disorder remains unclear: Papolos et al. w46x have reported an unusually high prevalence (64%) of bipolar spectrum disorders in VCFS patients, and some studies have linked bipolar disorder to this region of chromosome 22 w47,48x. While fewer studies have employed structured diagnostic interviews in younger children with VCFS, colleagues at CHOP found psychotic disorders were present in 3y31 cases (9%), which is over 50-fold the base rate of these disorders in children w49x. Rates of ADHD, ODD and anxiety disorders were also elevated, although at only two to three times their base rates. Furthermore, sub-syndromal symptoms of attention and mood disturbance were endorsed in almost all cases (88%). Similarly, a recent study by Arnold et al. w50x found psychiatric disorders to be present in 12y20 adolescent VCFS patients (60%), as compared to 3y11 (27%) of their unaffected siblings. Mood disorder was the most frequent diagnosis. Notably, three patients diagnosed with depressive disorder also had prominent schizotypal traits, and two of these three later developed schizophrenia. These findings indicate that the psychiatric disorders observed in adult patients are present, at least to some degree, in early childhood, and highlight the importance of investigating the developmental trajectory of VCFS. deletions. This could be partly explained by the lower educational status of the affected parent providing a less enriched environment within which to learn. With a growing number of children with VCFS approaching adulthood, and the fact that 50% of children they produce are also likely to have the deletion, this should be an area of real concern. Finally, it is clear that the development of psychiatric disorders, schizophrenia in particular, can have an independent, negative effect on cognitive outcome. 6. Summary Acknowledgments Clearly, most children with VCFS have some serious cognitive deficits that have negative implications for outcomes. Little or no formal investigation appears to have taken place concerning what might be called ‘situational’ implications of the syndrome for cognitive development. However, children with VCFS face a range of medical challenges and procedures early in life, and the effect of these on opportunities for early learning and the implications for brain development will be important to understand. Once these children proceed from preschool to regular classes, they will have adjustment problems. The social withdrawal often described may be as much due to situational factors, including their relatively small stature, unclear speech and lack of academic or sporting prowess. This has the potential to engender a negative attitude towards school, and thus have a deleterious effect on outcome in the educational domain. In addition, Swillen et al. w4x reported that patients with a deletion inherited from one parent had lower mean FSIQ scores than those with de novo We thank the children, adults and families who have participated in our studies of VCFS. Dr Michael F. Woodin, Mr David O. Aleman and others have greatly contributed to these studies. Much of the research described and the writing of this manuscript were supported in part by grants from the National Institutes of Health, DC 02027 and HD 01174. 7. Future approaches Clearly the time and conditions are now right for extensive studies of brain and cognitive implications of VCFS. Links to specific cognitive processes underlying a range of deficits in VCFS are now being made. In addition, new neuroimaging techniques allow researchers to examine how and why differences in brain structure and function may alter the way these processes work in individuals with VCFS. Many questions remain about the precise role of cardiac defects in those neurocognitive processes, and there is a clear need for controlled, prospective brain and cognition studies involving children with and without the 22q11.2 deletion who have undergone the same cardiac repairs early in life, as well as deleted patients who do not have a cardiac defect. Finally, findings in all of these areas will hopefully contribute to the design and implementation of cognitive and other kinds of interventions that can exploit early brain plasticity to change the trajectory of cognitive development in VCFS, and hopefully contribute to more positive outcomes. References w1x Moss EM, Batshaw ML, Solot CB, et al. Psychoeducational profile of the 22q11.2 microdeletion: a complex pattern. J Pediatr 1999;134(2):193 –198. w2x Swillen A, Vogels A, Devriendt K, Fryns JP. Chromosome 22q11 deletion syndrome: update and review of the clinical features, cognitive-behavioral spectrum, and psychiatric complications. Am J Med Genet (Semin Med Genet) 2000;97:128 – 135. w3x Woodin MF, Wang PP, Aleman D, McDonald-McGinn DM, Zackai EH, Moss EM. Neuropsychological profile of children and adolescents with the 22q11.2 microdeletion. Genet Med 2001;3(1):34 –39. 116 T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 w4x Swillen A, Devriendt K, Legius E, et al. Intelligence and psychosocial adjustment in velocardiofacial syndrome: a study of 37 children and adolescents with VCFS. J Med Genet 1997;34(6):453 –458. w5x Solot CB, Gerdes M, Kirschner R, et al. Communication issues in 22q11.2 deletion syndrome: children at risk. Genet Med 2001;3:67 –71. w6x Gerdes M, Solot CB, Wang PP, et al. Cognitive and behavior profile of preschool children with chromosome 22q11.2 deletion. Am J Med Genet 1999;85:127 –133. w7x Wang PP, Woodin MF, Kreps-Falk R, Moss EM. Research on behavioral phenotypes: velocardiofacial syndrome (deletion 22q11.2). Dev Med Child Neurol 2000;42:422 –427. w8x Dehaene S. Varieties of numerical abilities. Cognition 1992;44:1 –42. w9x Bearden CE, Woodin MF, Wang PP, et al. The neurocognitive phenotype of the 22q11.2 deletion syndrome: Selective deficit in visual-spatial memory. J Clin Exp Neuropsychol 2001;23:447 –464. w10x Ungerleider LG, Haxby JV. ‘What’ and ‘where’ in the human brain. Curr Opin Neurobiol 1994;4:157 –165. w11x Chatterjee A. Neglect. In: D’Esposito M, editor. Neurological Foundations of Cognitive Neuroscience. Cambridge, MA: MIT Press, in press. w12x Posner MIP, Walker JA, Friedrich FJ, Rafal RD. Effects of parietal injury on covert orienting of attention. J Neurosci 1984;4(7):1863 –1874. w13x Cipolotti L, Butterworth B, Denes G. A specific deficit for numbers in a case of dense acalculia. Brain 1991;114:2619 – 2637. w14x Simon TJ, Vaishnavi S. Subitizing and counting depend on different attentional mechanisms: evidence from visual enumeration in afterimages. Percept Psychophys 1996;58:915 – 926. w15x Trick LM, Pylyshyn ZW. What enumeration studies can tell us about spatial attention. Evidence for limited capacity preattentive processing. J Exp Psychol: Hum Percept Perform 1993;19:331 –351. w16x Sathian K, Simon TJ, Peterson S, Patel GA, Hoffman JM, Grafton ST. Neural evidence linking visual object enumeration and attention. J Cognit Neurosci 1999;11(1):36 –51. w17x Dehaene S, Cohen L. Towards an anatomical and functional model of number processing. Math Cogn 1995;1:83 –120. w18x Dehaene S, Spelke ES, Pinel P, Stanescu R, Tsivkin S. Sources of mathematical thinking: behavioral and brain imaging evidence. Science 1999;284:970 –974. w19x Pinel P, Le Clec’H G, van de Moortele P, Naccache L, Le Bihan D, Dehaene S. Event-related fMRI analysis of the cerebral circuit for number comparison. Neuroreport 1999;10(7):1473 – 1479. w20x Trick LM, Pylyshyn ZW. Why are small and large numbers enumerated differently? A limited capacity preattentive stage in vision. Psychol Rev 1994;101:80 –102. w21x Temple E, Posner MIP. Brain mechanisms of quantity are similar in 5-year-old children and adults. Proc Natl Acad Sci USA 1998;95:7836 –7841. w22x Eliez S, Blasey CM, Menon V, White CD, Schmitt JE, Reiss AL. Functional brain imaging study of mathematical reasoning abilities in velocardiofacial syndrome (Del 22q11.2). Genet Med 2001;3(1):49 –55. w23x McDonald-McGinn DM, Kirschner R, Goldmuntz E, et al. The Philadelphia story: the 22q11.2 deletion: report on 250 patients. Genet Couns 1999;10(1):11 –24. w24x Bellinger DC, Wypij D, Kuban KCK, et al. Developmental and neurological status of children at 4 years of age after heart w25x w26x w27x w28x w29x w30x w31x w32x w33x w34x w35x w36x w37x w38x w39x w40x w41x w42x surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. Circulation 1999;100:526 –532. Mahle WT, Clancy R, Moss EM, Gerdes M, Jobes DR, Wernovsky G. Neurodevelopmental outcomes and lifestyle assessment in school-aged and adolescent children with hypoplastic left heart syndrome. Pediatrics 2000;105(5):1082 –1089. Skoff RP, Bessert DA, Barks JD, Song D, Cerghet M, Silverstein FS. Hypoxic–ischemic injury results in acute disruption of myelin gene expression and death of oligodendroglial precursors in neonatal mice. Int J Dev Neurosci 2001;19(2):197 –208. Wolf RL, Zimmerman RA, Clancy R, Haselgrove JH. Quantitative apparent diffusion coefficient measurements in term neonates for early detection of hypoxic–ischemic brain injury: initial experience. Radiology 2001;218(3):825 –833. Eliez S, Schmitt JE, White CD, Reiss AL. Children and adolescents with velocardiofacial syndrome: a volumetric study. Am J Psychiatry 2000;157(3):409 –415. Kates WR, Burnette CP, Jabs EW, et al. Regional cortical white matter reductions in velocardiofacial syndrome: a volumetric MRI analysis. Biol Psychiatry 2001;49:677 –684. Fuerst KB, Dool CB, Rourke BP. Velocardiofacial syndrome. In: Rourke BP, editor. Syndrome of Non-Verbal Learning Disabilities: Neurodevelopmental Manifestations. New York: Guilford Press, 1995. p. 119 –137. Menkes JH. Textbook of Child Neurology. 4th ed.. Philadelphia: Lea & Febiger, 1990. Altshuler LL, Curran JG, Hauser P, Mintz J, Denicoff K, Post R. T2 hyperintensities in bipolar disorder: magnetic resonance imaging comparison and literature meta-analysis. Am J Psychiatry 1995;152(8):1139 –1144. Coffey CE, Figiel GS, Djang WT, Weiner RD. Subcortical hyperintensity on magnetic resonance imaging: a comparison of normal and depressed elderly subjects. Am J Psychiatry 1990;147(2):187 –189. Coffman JA, Bornstein RA, Olson SC, Schwarzkopf SB, Nasrallah HA. Cognitive impairment and cerebral structure by MRI in bipolar disorder. Biol Psychiatry 1990;27(11):1188 – 1196. Dupont RM, Butters N, Schafer K, Wilson T, Hesselink J, Gillin JC. Diagnostic specificity of focal white matter abnormalities in bipolar and unipolar mood disorder. Biol Psychiatry 1995;38(7):482 –486. Junque C, Pujol J, Vendrell P, et al. Leuko-araiosis on magnetic resonance imaging and speed of mental processing. Arch Neurol 1990;47(2):151 –156. Klingberg T, Hedehus M, Temple E, et al. Microstructure of temporo-parietal white matter as a basis for reading ability: evidence from diffusion tensor magnetic resonance imaging. Neuron 2000;25:493 –500. Rourke BP. Syndrome of non-verbal learning disabilities: the final common pathway of white matter diseaseydysfunction? Clin Neuropsychol 1987;1:209 –234. Kozma C. On cognitive variability in velocardiofacial syndrome: profound mental retardation and autism. Am J Med Genet (Neuropsychiatr Genet) 1998;81:269 –270. Shprintzen RJ, Goldberg R, Golding-Kushner KJ, Marion RW. Late-onset psychosis in the velo-cardio-facial syndrome. Am J Med Genet 1992;42(1):141 –142. Murphy KC, Jones LA, Owen MJ. High rates of schizophrenia in adults with velo-cardio-facial syndrome. Arch Gen Psychiatry 1999;56(10):940 –945. Bassett AS, Chow EW. 22q11 deletion syndrome: a genetic T.J. Simon et al. / Progress in Pediatric Cardiology 15 (2002) 109–117 w43x w44x w45x w46x w47x subtype of schizophrenia. Biol Psychiatry 1999;46(7):882 – 891. Bassett AS, Chow EW, Weksberg R. Chromosomal abnormalities and schizophrenia. Am J Med Genet 2000;97(1):45 –51. Nicolson R, Giedd JN, Lenane M, et al. Clinical and neurobiological correlates of cytogenetic abnormalities in childhoodonset schizophrenia. Am J Psychiatry 1999;156(10):1575 – 1579. Bassett AS, Hodgkinson K, Chow EW, Correia S, Scutt LE, Weksberg R. 22q11 deletion syndrome in adults with schizophrenia. Am J Med Genet 1998;81(4):328 –337. Papolos DF, Faedda GL, Veit S, et al. Bipolar spectrum disorders in patients diagnosed with velo-cardio-facial syndrome: does a hemizygous deletion of chromosome 22q11 result in bipolar affective disorder? Am J Psychiatry 1996;153(12):1541 –1547. Edenberg HJ, Foroud T, Conneally PM, et al. Initial genomic scan of the NIMH genetics initiative bipolar pedigrees: chromosomes 3, 5, 15, 16, 17, and 22. Am J Med Genet 1997;74(3):238 –246. 117 w48x Lachman HM, Kelsoe JR, Remick RA, et al. Linkage studies suggest a possible locus for bipolar disorder near the velocardio-facial syndrome region on chromosome 22. Am J Med Genet 1997;74(2):121 –128. w49x Bearden CE, Woodin MF, Weller E, Jessani N, Emanuel BS, Cannon TD. Emerging psychiatric dysfunction in children with 22q deletion syndrome. Schizophr Res 2001;49(1-2):66 –67. w50x Arnold PD, Siegel-Bartelt J, Cytrynbaum C, Teshima I, Schachar R. Velo-cardio-facial syndrome: Implications of microdeletion 22q11 for schizophrenia and mood disorders. Am J Med Genet 2001;105(4):354 –362. w51x Heineman-de Boer JA, Van Haelst MJ, Cordia-de Haan M, Beemer FA. Behavior problems and personality aspects of 40 children with velo-cardio-facial syndrome. Genet Couns 1999;10(1):89 –93. w52x Swillen A, Vandeputte L, Cracco J, et al. Neuropsychological, learning and psychosocial profile of primary school aged children with the velo-cardio-facial syndrome (22q11 deletion): evidence for a non-verbal learning disability? Child Neuropsychol 1999;5(4):230 –241.