D V S
advertisement

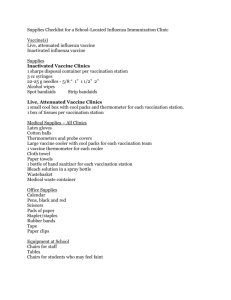
INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY 494 May 2005 DURATION OF VIRUS SHEDDING AFTER TRIVALENT INTRANASAL LIVE ATTENUATED INFLUENZA VACCINATION IN ADULTS Thomas R. Talbot, MD, MPH; Deidre D. Crocker, MD; Jody Peters, BS; Jennifer K. Doersam, BS; Mine R. Ikizler, BS; Edith Sannella, MA; Peter F. Wright, MD; Kathryn M. Edwards, MD ABSTRACT OBJECTIVE: To characterize the probability and duration of viral shedding among adults given trivalent live attenuated influenza vaccine (LAIV). DESIGN: Prospective sur veillance study. METHODS: Nasal wash samples were collected from adult volunteers at baseline and on days 3, 7, and 10 and between days 17 and 21 following intranasal LAIV vaccination. The presence, titer, and identification of each specific strain of influenza virus shed were determined by standard methodology. RESULTS: Twenty subjects received LAIV. No samples were positive for influenza virus at baseline. After LAIV vaccination, influenza virus was recovered from 10 of 20 vaccinees on day 3, from 1 of 18 vaccinees on day 7, and from none of the samples on days 10 or 17 through 21. Vaccinees who shed vaccine virus were significantly younger than those who did not (mean age, 26.4 vs 38.6 years; P < .01). Although the presence of specific mucosal immunoglobulin A to influenza B was associated with significantly less shedding of influenza B after vaccination (P = .02), associations of shedding with other measures of immunity were not detected. CONCLUSION: The duration of shedding of vaccine virus after LAIV in adults is limited and may be associated with an individual’s prior influenza vaccination histor y (Infect Control Hosp Epidemiol 2005;26:494-500). Vaccination with inactivated influenza virus has been a cornerstone of efforts to reduce the burden of disease due to influenza for many years.1 However, live attenuated influenza vaccines targeted to strains of influenza A (monovalent H1N1 or H3N2 or bivalent H1N1/H3N2 vaccines), influenza B (monovalent vaccines), or both (trivalent H1N1/ H3N2/B vaccines) have also been extensively evaluated as an attractive method to prevent influenza infection.2 In 2003, the trivalent vaccine FluMist (MedImmune Vaccines, Inc., Gaithersburg, MD) became the first live attenuated influenza vaccine approved for use in the United States. Administered intranasally, the trivalent live attenuated influenza vaccine has been shown to be efficacious against influenza infection, leading to a reduction in the incidence of cultureconfirmed influenza in children3,4 and a decrease in febrile upper respiratory tract episodes and days of work lost due to illness in adults.5 However, one concern with the use of the live attenuated influenza vaccines has been the potential risk of secondar y transmission of the vaccine virus from recent vaccinees to non-immune, high-risk individuals. As a result, FluMist was not recommended for use in immunocompromised individuals,6 and vaccine recipients were strongly advised to avoid close contact with immunocompromised individuals for at least 21 days after vaccination.6 Due to this advisor y, some hospitals furloughed employees who had been vaccinated with live attenuated influenza vaccine from direct patient care duties for several weeks.7 Specific data regarding mucosal shedding of vaccine virus following intranasal administration of live attenuated influenza vaccine are limited. Studies in children noted that vaccinees could shed vaccine virus for up to 21 days after vaccination,6,8 but data from adults suggested the degree and duration of shedding was substantially lower.9 Thus, we conducted a prospective study of mucosal shedding of vaccine virus at various intervals in adults following vaccination. Dr. Talbot is from the Division of Infectious Diseases, Departments of Medicine and Preventive Medicine; Drs. Crocker, Wright, and Edwards, Ms. Peters, Ms. Doersam, Ms. Ikizler, and Ms. Sannella are from the Division of Infectious Diseases, Department of Pediatrics; and Dr. Edwards is also from the Pediatric Clinical Research Office, Vanderbilt University School of Medicine, Nashville, Tennessee. Address reprint requests to Thomas R. Talbot, MD, MPH, A-2200 Medical Center North, 1161 21st Avenue South, Vanderbilt University Medical Center, Nashville, TN 37232. tom.talbot@vanderbilt.edu Supported in part by National Institute of Allergy and Infectious Diseases, Division of Microbiology and Infectious Diseases, contract #N01-AI25462 and General Clinical Research Center grant #M01-RR-00095. The authors thank all of the members of the Vanderbilt Pediatric Clinical Research Office, especially Alice O’Shea, RN; Nancy Olsen, MD; the Vanderbilt General Clinical Research Center; and colleagues at the National Institute of Allergy and Infectious Diseases, Division of Microbiology and Infectious Diseases, particularly Linda Lambert, Mamodikoe Makhene, and Holli Hamilton, for their support of and guidance with this project. They also thank Henry Hsu and Chiron Biocine for providing antigens for the humoral immunity studies. Presented in part at the 14th Annual Meeting of the Society for Healthcare Epidemiology of America; April 18-20, 2004; Philadelphia, PA. SHEDDING AFTER LIVE INFLUENZA VACCINE Vol. 26 No. 5 495 TABLE 1 RECOVERY OF INFLUENZA VIRUS FROM NASAL WASH SPECIMENS IN ADULTS FOLLOWING INTRANASAL VACCINATION WITH THE TRIVALENT LIVE ATTENUATED INFLUENZA VACCINE No. of Subjects Tested No. of Specimens Positive Proportion of Subjects With Shedding 0 20 0 0% 0–16.8% None 3 20 10 50% 27.2–72.8% A H1N1 alone (1), A H3N2 alone (1), both A strains (1), B alone (6), all three strains (1) 7 18 1 5.5% 0.1–27.3% B (1) 10 19 0 0% 0–17.6% None 17–21 20 0 0% 0–16.8% None Post-Vaccination Day Exact CI95 Influenza Strain(s) Shed (No. of Subjects) CI95 = 95% confidence interval. METHODS Study Subjects Healthy adults 18 to 49 years old were recruited for this study. Individuals with a current or past history of egg or egg product allergy, allergic reactions to prior influenza vaccinations, immunodeficiency due to underlying conditions or medications, a previous history of Guillain–Barré syndrome, or any medical or psychiatric condition that precluded their compliance were excluded. Individuals with an acute respiratory tract infection or immunocompromised household contacts were also excluded. This study was reviewed and approved by the Vanderbilt University Institutional Review Board. All subjects provided written informed consent. Vaccination All enrolled subjects were vaccinated with trivalent live attenuated influenza vaccine (FluMist), administered intranasally (0.25 mL in each nostril). Each 0.5-mL total dose was formulated to contain 106.5–7.5 50% tissue culture infectious doses (TCID50) of each of the live attenuated influenza vaccine reassortants of the influenza strains recommended by the U.S. Public Health Service for the 2003–2004 season: A/New Caledonia/20/99 (H1N1), A/ Panama/2007/99 (H3N2) (A/Moscow/10/00-like), and B/ Hong Kong/330/2001. Patient Follow-Up and Specimen Collection Subjects were obser ved during scheduled clinic visits on days 3, 7, and 10 and between days 17 and 21 after vaccination. At each visit, subjects were assessed for histor y of symptoms (including headache, sore throat, rhinorrhea, myalgias, fatigue, cough, or fever). Nasal wash specimens were collected from each subject immediately prior to vaccination and at each visit after vaccination. Specifically, 15 mL of lactated Ringer’s solution was instilled into one nostril using a bulb syringe, and the resulting nasal wash was collected from the opposite FIGURE. Quantitative influenza B mucosal IgA at baseline in subjects vaccinated with live attenuated influenza vaccine, by presence or absence of influenza B shedding after vaccination. Gray horizontal bars denote mean baseline nasal wash influenza B IgA enzyme-linked immunosorbent assay (ELISA) units corrected for total mucosal IgA in each group (as described in reference 13). The comparison of mean baseline IgA values in shedders versus non-shedders yielded a P value of .03. nostril. The specimens were then inoculated into two tissue culture tubes containing rhesus monkey kidney cells. After incubation at room temperature for 1 hour to allow for virus adsorption, the cultures were incubated in serum-free Eagle/199 medium (Invitrogen, Carlsbad, CA) supplemented with antibiotics. Cultures were read at regular inter vals for cytopathic effect. On days 5 and 10 following inoculation, the rhesus monkey kidney cells were hemadsorbed with 0.1% guinea pig red blood cells in phosphate-buffered saline. Specimens were considered positive for influenza if they exhibited the presence of cytopathic effect or hemadsorption. Positive specimens were initially characterized as influenza A or B using indirect immunofluorescent assay analysis. Positive tissue culture harvests were then plaqued in Madin–Darby canine kidney cells, and the plaques were stained with immunoperoxidase using MVB 18–40 y 26 Gruber et al. King et al.25 Vesikari et al.8 a) 44 c) 47 Yes HIV negative: 25 HIV positive: 24 98 19 20 b) 19 a) 15 32 b) Dose 6.6: 14 a) Dose 7.6: 29 b) 21 a) 38 HIV negative: 27 HIV positive: 28 20 No. of Subjects c) BVA 6.2 No Yes No No Yes Yes Yes Yes Yes No Only Studied Seronegative Subjects? b) 45 a) MV H1N1A 6–18 mo 7.0 Not noted 7.8 6.2–7.2 7.5 7.5 6.6–7.6 7.1 7.0 6.5–7.5 Vaccine Dose† 6, 11 3–5, 7–10, 28–35 Approximately 3 times/wk for 3 wk Daily days 1–5 Daily days 1–5 Daily days 1–4 Daily days 1–3 1, 2, 3, 4, 5, 6, 7, 28 Daily days 1–7 3–5, 7–10, 28–35 0, 3, 7, 10, 17–21 c) 55 b) 36 a) 16 HIV negative: 28 HIV positive: 13 80 11 10 21 Not measured Not measured 7.6 0 Seropositive: 0 2.2 2.0–2.8 b) 0.6 ± 1.1 a) 1.9 ± 1.7 0.6 ± 0.2 b) 2.7 ± 1.4 a) 2.4 ± 1.1 b) 2.7–3.4 a) 3.8–4.2 Not measured Not measured Average Duration of Shedding (d) 4.0 Not noted 4 Not noted Not noted Not noted Not noted 5 7 Last Day Shedding Detected Equivocal: 14 Seronegative: 50 85 b) 26 a) 60 28 b) 79 a) 100 b) 95 a) 92 HIV negative: 0 HIV positive: 4 50 Subjects With Viral Shedding (%) Not measured 2.7 1.2 0 1.7 1.7 2.5–3.0 b) 0.7 ± 0.3 a) 1.8 ± 1.4 0.8 ± 0.1 b) 0.7 ± 0.3 a) 0.9 ± 0.2 b) 0.5–1.6 a) 0.5–2.1 Peak Titer of Shed Virus‡ INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY b) MV H3N2A TV TV 1–7 y 8–36 mo Mortiz et al.24 Studies of children MVB MV H3N2A 20–24 y Not noted Reeve et al.23§ b) MV H3N2A a) MV H1N1A 18–40 y b) TV a) MVB or BVA Sears et al.22 Clements et al. 18–35 y Keitel et al.20 21 MVB (varying doses‡) 18–40 y Keitel et al.11§ TV 18–58 y King et al.9 TV 19–49 y Age Range Current Studies of adults Study Vaccine Studied* Days of Specimen Collection PostVaccination TABLE 2 SUMMARY OF STUDIES OF NASAL MUCOSAL SHEDDING OF INFLUENZA VIRUS AFTER VACCINATION WITH A LIVE ATTENUATED INFLUENZA VACCINE 496 May 2005 SHEDDING AFTER LIVE INFLUENZA VACCINE Not measured a) 3.6 ± 0.4 b) 3.5 ± 0.3 Not measured a) 9.8 ± 0.9 b) 6.9 ± 0.9 b) 100 b) 10 Yes a) 11 Daily days 1–15 a) 73 6 Wright et al.29 b) MV H3N2A 7.8 a) MV H1N1A 1.5–4.5 y a) 31 b) 29 0, 3, 6 a) 29 b) 28 Yes 7.5–7.8 a) MV H1N1A b) MV H3N2A Seronegative: 91 1–7 y Feldman et al. 28 497 monoclonal antibodies specific for the hemagglutinin of the H1N1 influenza A, H3N2 influenza A, and B influenza viruses to further characterize the specific influenza strains shed.10,11 Viral quantification was also performed using serial 1:10 dilutions of aliquots of positive samples that had been frozen directly in the lactated Ringer’s solution, as described previously.12 HIV = human immunodeficiency virus; TV = trivalent vaccine; MV H1N1A = monovalent H1N1 A vaccine; MV H3N2A = monovalent H3N2 A vaccine; MVB = monovalent B vaccine; BVA = bivalent H1N1 and H3N2 A vaccine. *All vaccines studied were cold adapted. † Expressed as log10 50% tissue culture infectious doses (TCID50). ‡ Expressed as TCID50 log10/mL. § Only data following primary vaccination are included. Seronegative studies conducted in ages 6 to 48 months only. 3.4 9.0 Not noted 0.9 MVB Edwards et al.27 6 mo–9 y 7.2 No 24 Daily days 1–10 Seropositive: 54 10 5.0 Vol. 26 No. 5 Immunity Assays Hemagglutination inhibition antibody titers to each of the three influenza strains included in the live attenuated influenza vaccine were determined at baseline prior to vaccination and between days 17 and 21 after vaccination, as described previously.13-16 Mucosal and serum IgA antibodies were detected using a kinetic enzyme-linked immunosorbent assay run in triplicate, as described previously.17 Those subjects with a hemagglutination inhibition titer greater than 1:32 or the presence of detectable serum or mucosal IgA prior to vaccination were noted and correlations with vaccine shedding were evaluated.18,19 Cell-mediated immunity assays were not performed. Analysis Comparisons between subjects with and without evidence of nasal shedding were made using Fisher’s exact test for categorical data and the Mann–Whitney U test for nonparametric continuous data. Analyses were conducted using Stata software (version 7.0; StataCorp, College Station, TX). RESULTS Twenty subjects underwent live attenuated influenza vaccine vaccination. The mean age of the cohort was 31.6 years (standard deviation, ± 8.9 years; range, 19 to 49 years). The majority of the subjects were women (11 of 20; 55%) and white (18 of 20; 90%). All subjects completed the study, although three missed one of the four scheduled follow-up visits (two subjects missed the day 7 visit and one missed the day 10 visit). Influenza was not detected in any of the nasal wash specimens obtained at baseline (0 of 20; 95% confidence interval, 0 to 16.8%; Table 1). In contrast, half of the specimens obtained on day 3 after vaccination (10 of 20; 95% confidence interval, 27.2% to 72.8%) were positive for influenza virus. By day 7 after vaccination, the degree of mucosal shedding had markedly declined, with only 1 of 18 nasal wash specimens obtained (5.5%; 95% confidence interval, 0.1% to 27.3%) being culture positive for influenza virus. Influenza was not recovered from any of the subjects on days 10 (95% confidence interval, 0 to 17.6%) or 17 to 21 (95% confidence interval, 0 to 16.8%) after vaccination. In total, virus was recovered from 10 subjects; 1 subject shed on day 3 and day 7 after vaccination. The specific influenza strain shed varied: one subject shed influenza A H1N1 alone, one shed influenza A H3N2 alone, one shed both influenza A strains, six shed influenza B alone, and one shed all three strains (Table 1). The subject who shed on multiple visits had influenza B isolated 498 INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY on day 3 and day 7 after vaccination. Characterization of preimmunization status in that subject revealed a baseline hemagglutination inhibition titer to influenza B of 1:64, suggesting exposure to that strain through previous influenza vaccination. However, she did not have any detectable mucosal IgA to influenza B at baseline. Quantitative titrations were performed on all positive specimens. Only 1 of the 11 positive samples contained a detectable quantity of virus with a peak titer of 5 100 plaque-forming units (PFU)/mL (the lowest level of detection). Shedding of vaccine virus was significantly associated with younger age (mean age, 26.4 years for those with shedding vs 38.6 years for those without; P < .01). Although those who did not shed vaccine virus were more likely to report prior influenza vaccination (8 of 10) than those who did (3 of 10), this did not achieve statistical significance (P = .07). Absence of shedding of influenza B vaccine virus was significantly associated with influenza B–specific mucosal IgA antibody at baseline (Figure; P = .03). However, no associations were noted between the shedding of influenza A vaccine virus and baseline mucosal IgA antibody titers nor with any baseline strain-specific serum IgG or IgA antibody titers to any of the vaccine strains (data not shown). DISCUSSION The licensure of trivalent live attenuated influenza vaccine has raised questions and concerns regarding the use of this vaccine in some populations.7 In particular, the potential for inadvertent secondary transmission of vaccine virus led to an initial advisory in the package insert that individuals recently vaccinated with live attenuated influenza vaccine avoid close contact with immunocompromised individuals for at least 21 days after vaccination,6 a duration based on the recovery of influenza in one transmission study from a single child 21 days after vaccination.8 However, data regarding mucosal shedding after live attenuated influenza vaccine vaccination in adults have been limited, with investigations rarely assessing shedding past the first week after vaccination. The current study clearly demonstrated that the degree and duration of viral shedding in adults markedly declined within the first week after live attenuated influenza vaccine vaccination and that shedding could not be documented after that time. Previous studies of nasal shedding of vaccine virus after administration of live attenuated influenza vaccine are summarized in Table 2.8,9,11,20-29 These studies vary regarding type of live attenuated influenza vaccine studied (monovalent or bivalent influenza A, monovalent influenza B, or trivalent vaccines), study population (adults or children), and number of specimens collected and the timing of that collection after vaccination, impeding inter-trial comparisons. In general, the duration of shedding after vaccination has been greater in children compared with adults (range of duration in children, 5.0 to 9.8 days; range of duration in adults, 0 to 4.0 days). In addition, prior serologic immunity to the vaccine strains was associated with a reduced frequency and duration of viral shedding.24,27 In the current study, the finding of an association between baseline muco- May 2005 sal immunity to influenza B and the shedding of influenza B after vaccination and the absence of baseline nasal IgA in the one subject who shed virus on two visits further support the importance of prior mucosal immunity for shedding risk. Although no correlation between baseline serum immunity and detection of shedding was found in the current investigation, such analyses may have been limited by our small sample size. Studies specifically investigating the degree of mucosal shedding after use of the newly licensed trivalent live attenuated influenza vaccine are limited. In one study of human immunodeficiency virus–infected and healthy adults, only one human immunodeficiency virus–positive subject (1 of 28; 3.6%) shed influenza virus, detected on day 5 after vaccination. Shedding was not documented in any human immunodeficiency virus–negative subjects.9 A similar study of children 1 to 7 years old noted a greater duration (up to 10 days after vaccination) and frequency (13% to 28%) of shedding.25 In contrast, all 11 healthy adults vaccinated with the trivalent live attenuated influenza vaccine in another study shed virus during the first week after vaccination, with an average of shedding of 3.4 days.11 In the largest investigation of shedding after trivalent live attenuated influenza vaccine vaccination, a randomized, placebo-controlled trial conducted in Finland using a cohort of 197 day care attendees, 78% (76 of 98) of vaccinated children shed virus for an average of 7.6 days.8 Shedding was detected up to 21 days after vaccination in one child. Even fewer studies have directly examined the transmission of vaccine-based virus from vaccinated subjects. In the Finnish day care trial mentioned above, transmission of a vaccine-type influenza B virus from a vaccinee to one of 99 placebo recipients was documented.6,8 Four other subjects receiving placebo shed influenza A, but these isolates could not be characterized further to determine their origin (wild type vs vaccine). In this study, the probability of acquiring vaccine virus after close contact with a single live attenuated influenza vaccine vaccinee was estimated to be between 0.58% and 2.4%.8 Despite the transmission to one unvaccinated subject in the Finnish study, the transmitted virus retained the attenuated phenotype and did not lead to clinical disease.8 In another study in which 31 adult subjects recently vaccinated with monovalent avian–human influenza A H3N2 live attenuated influenza virus were housed for 7 to 9 days after vaccination with 6 placebo recipients, no episodes of transmission were detected.30 A larger issue regarding secondary transmission of vaccine-based influenza virus is whether such transmission is harmful to the exposed individual. Modification of the vaccine virus to restrict replication above 37°C (similar to the temperature of the lower airways) as well as attenuation to non-virulent viral reassortants markedly restricts the potential for clinical infection following inadvertent transmission of vaccine virus.6 Although reversion of the vaccine virus to a wild genotype is a concern, an investigation of individuals vaccinated with a trivalent live attenuated influenza vaccine who exhibited mucosal shedding after vaccination found that the shed viruses were genotypically stable, Vol. 26 No. 5 SHEDDING AFTER LIVE INFLUENZA VACCINE retaining the attenuated vaccine genotype in all instances.31 Transmission of vaccine virus may, in fact, be beneficial, as transmission of the attenuated strain of influenza may result in a de facto vaccination of the exposed subject, providing protection from circulating wild-type influenza. Effective secondary transmission of vaccine virus from vaccinees also requires a significant quantity of virus to be shed from the nasal mucosa. Based on prior investigations with live attenuated influenza vaccine, the dose of vaccine virus required to effectively infect an individual is approximately 105 to 107 PFU/mL.21,22,32 From our investigation and from other studies of mucosal shedding after live attenuated influenza vaccine use, the quantity of virus shed after live attenuated influenza vaccine vaccination was exponentially lower (from 100 to 102 PFU/mL) and likely would not have been able to infect other individuals. In our study, although 50% of subjects shed at day 3 after vaccination, only one subject shed virus above the lower limit of quantification. Studies further evaluating the magnitude of shedding after live attenuated influenza vaccine vaccination are now needed to assist with assessment of the risk of secondary transmission of the vaccine virus. Healthcare workers have been among those most affected by the recommendations restricting contact with immunocompromised individuals following live attenuated influenza vaccine vaccination. Following live attenuated influenza vaccine licensure, some facilities instituted policies requiring a 21-day furlough of any healthcare worker vaccinated with live attenuated influenza vaccine.7 Such restrictions created staffing shortages during influenza season, a time of year typically associated with high patient volume. Some vaccine experts speculate that intranasal live attenuated influenza vaccine is a more acceptable method of delivery than the intramuscular vaccine, an idea supported by recent investigations.33,34 Although annual influenza vaccination is recommended for all healthcare workers to reduce work absenteeism and prevent the nosocomial transmission of influenza, only 37% of surveyed healthcare workers reported having received influenza vaccination in 2001.1 Expanding the use of live attenuated influenza vaccine to healthcare workers and reducing or removing post-vaccination work restrictions may improve vaccine acceptance and coverage, limiting the risk of nosocomial transmission of wild influenza. The licensure of the live attenuated influenza vaccine provides an additional tool in the armamentarium against influenza infection. As with other live viral vaccines, secondar y transmission to those at risk for clinical infection from transmitted virus is a concern; however, previous guidelines on restriction of contacts after live attenuated influenza vaccine vaccination were too restrictive. In this investigation, we found that mucosal shedding in 20 adults vaccinated with the trivalent live attenuated influenza vaccine was markedly diminished within 1 week after vaccination. Although the sample size of this investigation was small, such results have provided a more detailed description of the duration of shedding after vaccination, 499 leading to a modification of recommendations for live attenuated influenza vaccine use in healthcare workers that reduces the period of separation from patients after live attenuated influenza vaccine vaccination to at most 7 days.35 In addition, the amount of virus shed was much lower than the estimated dose needed for effective infection with vaccine virus in immunocompetent individuals, suggesting that the risk of infection from secondar y transmission of vaccine virus is low. Additional studies refining estimates of the degree of mucosal shedding after live attenuated influenza vaccine vaccination and the risk of secondar y transmission of the attenuated vaccine virus to immunocompromised individuals are needed to further explore the necessity for healthcare workers to be restricted from patients after live attenuated influenza vaccine vaccination. REFERENCES 1. Bridges CB, Harper SA, Fukuda K, Uyeki TM, Cox NJ, Singleton JA. Prevention and control of influenza: recommendations of the Advisor y Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2003;52:1-34. 2. Harper SA, Fukuda K, Cox NJ, Bridges CB. Using live, attenuated influenza vaccine for prevention and control of influenza: supplemental recommendations of the Advisor y Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2003;52:1-8. 3. Belshe RB, Mendelman PM, Treanor J, et al. The efficacy of live attenuated, cold-adapted, trivalent, intranasal influenza virus vaccine in children. N Engl J Med 1998;338:1405-1412. 4. Belshe RB, Gruber WC, Mendelman PM, et al. Efficacy of vaccination with live attenuated, cold-adapted, trivalent, intranasal influenza virus vaccine against a variant (A/Sydney) not contained in the vaccine. J Pediatr 2000;136:168-175. 5. Nichol KL, Mendelman PM, Mallon KP, et al. Effectiveness of live, attenuated intranasal influenza virus vaccine in healthy, working adults: a randomized controlled trial. JAMA 1999;282:137-144. 6. MedImmune Vaccines, Inc. Influenza Virus Vaccine, Live Intranasal FluMist [package insert]. Gaithersburg, MD: MedImmune Vaccines, Inc.; 2003. 7. Anonymous. Flu mystified: hospitals are in a fog of live viral vaccine issues. Hospital Infection Control 2004;31:1-5. 8. Vesikari T, Kar vonen A, Korhonen T, et al. A randomized, double-blind, placebo-controlled trial of the safety, transmissibility and phenotypic stability of a live, attenuated, cold-adapted influenza virus vaccine (CAIV-T) in children attending day care. Presented at the 41st Annual Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16-19, 2001; Chicago, IL. Abstract G-450. 9. King JC Jr, Treanor J, Fast PE, et al. Comparison of the safety, vaccine virus shedding, and immunogenicity of influenza virus vaccine, trivalent, types A and B, live cold-adapted, administered to human immunodeficiency virus (HIV)-infected and non-HIV-infected adults. J Infect Dis 2000;181:725-728. 10. Belshe RB, Swierkosz EM, Anderson EL, Newman FK, Nugent SL, Maassab HF. Immunization of infants and young children with live attenuated trivalent cold-recombinant influenza A H1N1, H3N2, and B vaccine. J Infect Dis 1992;165:727-732. 11. Keitel WA, Couch RB, Quarles JM, Cate TR, Baxter B, Maassab HF. Trivalent attenuated cold-adapted influenza virus vaccine: reduced viral shedding and serum antibody responses in susceptible adults. J Infect Dis 1993;167:305-311. 12. Meguro H, Br yant JD, Torrence AE, Wright PF. Canine kidney cell line for isolation of respirator y viruses. J Clin Microbiol 1979;9:175179. 13. Boyce TG, Gruber WC, Coleman-Docker y SD, et al. Mucosal immune response to trivalent live attenuated intranasal influenza vaccine in children. Vaccine 1999;18:82-88. 14. Snyder MH, Banks S, Murphy BR. Determination of antibody response to influenza virus surface glycoproteins by kinetic enzymelinked immunosorbent assay. J Clin Microbiol 1988;26:2034-2040. 15. Hierholzer JC, Suggs MT. Standardized viral hemagglutination and hemagglutination-inhibition tests: I. Standardization of er ythrocyte suspensions. Appl Microbiol 1969;18:816-823. 16. Hierholzer JC, Suggs MT, Hall EC. Standardized viral hemagglutina- 500 17. 18. 19. 20. 21. 22. 23. 24. 25. INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY tion and hemagglutination-inhibition tests: II. Description and statistical evaluation. Appl Microbiol 1969;18:824-833. Crowe JE Jr, Sannella EC, Pfeiffer S, et al. CD154 regulates primate humoral immunity to influenza. Am J Transplant 2003;3:680-688. Plotkin SA. Immunologic correlates of protection induced by vaccination. Pediatr Infect Dis J 2001;20:63-75. Treanor J, Wright PF. Immune correlates of protection against influenza in the human challenge model. Dev Biol (Basel) 2003;115:97104. Keitel WA, Couch RB, Cate TR, Six HR, Baxter BD. Cold recombinant influenza B/Texas/1/84 vaccine virus (CRB 87): attenuation, immunogenicity, and efficacy against homotypic challenge. J Infect Dis 1990;161:22-26. Clements ML, Snyder MH, Sears SD, Maassab HF, Murphy BR. Evaluation of the infectivity, immunogenicity, and efficacy of live coldadapted influenza B/Ann Arbor/1/86 reassortant virus vaccine in adult volunteers. J Infect Dis 1990;161:869-877. Sears SD, Clements ML, Betts RF, Maassab HF, Murphy BR, Snyder MH. Comparison of live, attenuated H1N1 and H3N2 cold-adapted and avian-human influenza A reassortant viruses and inactivated virus vaccine in adults. J Infect Dis 1988;158:1209-1219. Reeve P, Pibermann M, Bachmayer H, et al. Studies in man with a coldrecombinant live influenza B virus vaccine. J Med Virol 1982;9:1-9. Mortiz AJ, Kunz C, Hofman H, Liehl E, Reeve P, Maassab HF. Studies with a cold-recombinant A/Victoria/3/75 (H3N2) virus: II. Evaluation in adult volunteers. J Infect Dis 1980;142:857-860. King JC Jr, Fast PE, Zangwill KM, et al. Safety, vaccine virus shedding and immunogenicity of trivalent, cold-adapted, live attenuated influenza vaccine administered to human immunodeficiency virusinfected and noninfected children. Pediatr Infect Dis J 2001;20:11241131. May 2005 26. Gruber WC, Belshe RB, King JC, et al. Evaluation of live attenuated influenza vaccines in children 6-18 months of age: safety, immunogenicity, and efficacy. J Infect Dis 1996;173:1313-1319. 27. Edwards KM, King JC, Steinhoff MC, et al. Safety and immunogenicity of live attenuated cold-adapted influenza B/Ann Arbor/1/86 reassortant virus vaccine in infants and children. J Infect Dis 1991;163:740745. 28. Feldman S, Wright PF, Webster RG, et al. Use of influenza A virus vaccines in seronegative children: live cold-adapted versus inactivated whole virus. J Infect Dis 1985;152:1212-1218. 29. Wright PF, Okabe N, McKee KT Jr, Maassab HF, Karzon DT. Coldadapted recombinant influenza A virus vaccines in seronegative young children. J Infect Dis 1982;146:71-79. 30. Murphy BR, Clements ML, Tierney EL, Black RE, Stienberg J, Chanock RM. Dose response of influenza A/Washington/897/80 (H3N2) avian-human reassortant virus in adult volunteers. J Infect Dis 1985;152:225-229. 31. Cha TA, Kao K, Zhao J, Fast PE, Mendelman PM, Ar vin A. Genotypic stability of cold-adapted influenza virus vaccine in an efficacy clinical trial. J Clin Microbiol 2000;38:839-845. 32. Belshe RB. Current status of live attenuated influenza virus vaccine in the US. Virus Res 2004;103:177-185. 33. Gruber WC, Hinson HP, Holland KL, Thompson JM, Reed GW, Wright PF. Comparative trial of large-particle aerosol and nose drop administration of live attenuated influenza vaccines. J Infect Dis 1993;168:1282-1285. 34. Sendi P, Locher R, Bucheli B, Battegay M. Intranasal influenza vaccine in a working population. Clin Infect Dis 2004;38:974-980. 35. Harper SA, Fukuda K, Uyeki TM, Cox NJ, Bridges CB. Prevention and control of influenza: recommendations of the Advisor y Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2004;53:1-40.