INTEGRATING HEALTH CARE INTEGRATING HEALTH CARE THROUGH INTEGRATED
advertisement

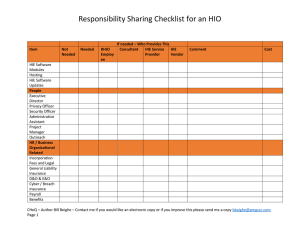
INTEGRATING HEALTH CARE INTEGRATING HEALTH CARE THROUGH INTEGRATED THROUGH INTEGRATED INFORMATION K Kenneth W. Kizer, MD, MPH th W Ki MD MPH California HIE Stakeholder Summit Sacramento CA Sacramento, CA May 8, 2013 Presentation Preview Provide an update on California Health e‐Quality (CHeQ) activities Review ongoing work Note some new activities about to be launched Provide a preview of some ways that we are planning to use HIE to improve population health 2 What is the problem we are trying to fix? Modern health care has become one of the most information‐intense and knowledge‐based activities that human beings have ever engaged in that human beings have ever engaged in Health care and health care information has become highly fragmented because of the highly fragmented because of the Explosion of biomedical knowledge and technology Increased medical specialization and sub‐specialization Increased prevalence of chronic conditions Increased complexity of care As a result, the quality of health care is insufficient and costs increases are unsustainable 3 California Health eQuality ACTIVITIES CHeQ Mission and Strategic Objectives Mission – Promote coordinated and integrated care by catalyzing health i f information exchange ti h Strategic Objectives Strategic Objectives – Improve integration of care and health outcomes by mobilizing information needed for health‐related decision making – Demonstrate measurable impact within the ARRA funding D t t bl i t ithi th ARRA f di period while laying a foundation for future growth and sustainability – Create a trusted environment for clinicians to exchange C t t t d i tf li i i t h information supporting local autonomy – Integrate HIE with similarly aimed health care reform initiatives 5 Trusted Exchange Infrastructure $1 million Integrating Clinical Care with Public Health Increasing Public Health Public Health Capacity $1 8 million $1.8 million $0.7 million California Health eQuality $16.6 million Accelerating HIE Accelerating HIE Adoption Federal HIE Funds Federal HIE Funds Monitoring HIE Adoption $4 million $0.9 million $0.9 million Communications and Education $0.6 million Personnel $4.1 million Operations $1 million Indirects $2.5 million CHeQ Activities – National, Statewide & Local National activities: promoting standards Trust environment P id di t i Provider directories HIE Ready New LOINC mapping Statewide public health activities Immunization gateway service Project INSPIRE Regional and local HIE investments Six programs focusing on infrastructure, interface implementation, Six programs focusing on infrastructure interface implementation new data analytics, new coordination in the greater LA area, new rural health initiative, new California Blue Button ® initiative® 7 National Activities: Promoting Standards National Initiative: Create a Trust Environment Goal: Create an environment that protects health information privacy and promotes f p y p exchange of health information between and among organizations and across political j i di ti jurisdictions. 9 Trust Environment: The “4 Knows” 2. Know who you are talking to – Provider Directories Provider Directories 4. Know you have consent to have the conversation – Patient consent management nexxt steps 3. Know who you are talking about – Patient matching current aactivities 1. Know your conversation is secure – Trust Communities ONC refers to these concepts as “Scalable Trust”. 10 Creating Trust Communities: Problem Community, enterprise HIOs create Community enterprise HIOs create information stovepipes. Thousands of point‐to‐point data sharing agreements between organizations are not practical nor affordable on a statewide or ti l ff d bl t t id national level. 11 Trust Communities: Solution Create Trust Communities based on a common set of polices and practices, a multiparty sharing agreement, and a simple technical framework. W Western States Consortium created the nation’s first Trust t St t C ti t d th ti ’ fi t T t Community; under pilot November 1, 2012 ONC now promoting Trust Communities as the preferred method for inter‐organizational trust h df l California participated in creating a consensus national technical standard in March 2013 and that has entered pilot testing California adopting model for inter‐HIO exchange in pilot program this summer p g 12 Provider Directories: Problem No way to discover exchange methods with y g a provider. “What is Dr. Smith’s Direct address?” No way to ensure the identity of an exchange partner. “How do I know this is h t “H d I k thi i really the right Dr. Smith?” 13 Provider Directories: Solution Create a searchable, federated Provider Directory that Is maintained by HIOs, clinics, hospitals with provider relationships so data is correct relationships so data is correct Establishes provider identity Identifies how to exchange data with individuals or organizations Western States Consortium (California and Oregon) entered production in April. ONC recognized the importance of California ONC recognized the importance of California’ss approach and approach and is creating a national standard for Stage 3 certification. p gp p g g California planning pilot program for inter‐HIO exchange this Summer. WSC transitioning to National Association for Trusted E h Exchange (NATE) (NATE) 14 National Initiatives: Promoting Standards nextt steps LOINC Mapping Assistance Logical Observation Identifiers Names and Codes (LOINC) is a Names and Codes (LOINC) is a database and universal standard for identifying medical laboratory observations Preparing clinical laboratories to meet Stage 2 Meaningful Use requirements curren nt activities HIE Ready Uses existing standards to promote transparency Reduces the need for creating interfaces 15 HIE Ready: Problem Stage 1 Meaningful Use doesn 1 Meaningful Use doesn’tt actually actually promote standards for interoperability. Stage 2 still has gaps. Too expensive to custom‐develop interfaces each time. 16 HIE Ready: Solution Create HIE Ready, a set of interface capabilities Based on standards in current products vs. future plans; Bundled with a single price so they are easy to buy; and Published as side‐by‐side comparison so buyers are informed. Published the first Buyers’ Guide in November 2012. Currently have 13 participants with many more interested. ONC and several states interested in joining or encouraging their vendors to participate. Vendors now bidding HIE Ready pricing. g yp g All Rural Incentive Program service providers are HIE Ready. Planning version 2.0 for Summer 2013 to align with Stage 2 MU MU. 17 HIE Ready Buyers’ Guide 18 New National Standards Initiative: LOINC Mapping Problem – Providers must receive and incorporate lab results using LOINC terminology in Stage 2 MU – Clinical laboratories are not yet ready and do not Clinical laboratories are not yet ready and do not receive incentives Solution – Create the LOINC Mapping Assistance program to convert high‐volume, independent and hospital labs to LOINC terminology gy produce materials and tools so they can maintain them Key – Partnering with California HealthCare Foundation Advances – Will recruit first labs this Summer 19 S Statewide Public Health Activities id P bli H l h A i i i State Initiatives: Expanding Public Health Capacity next stteps 2. INSPIRE Advancing workflow and standards for breast cancer reporting Creating a “health information home” for high impact conditions starting with cancer high‐impact conditions, starting with cancer Exploring how the “health information home” can be used by providers for population health management curre ent activitties 1. Immunization Gateway Service Streamlining the process to register for reporting and test interface capabilities reporting and test interface capabilities Increasing the capacity to receive reports 3. Open Library of HIE Project Creating an online ecosystem of ARRA funded work products to be shared and reused work products to be shared and reused 21 Immunization Gateway Service: Problem Immunization Immunization reporting is part of Stage 1 & 2 reporting is part of Stage 1 & 2 Meaningful Use California (like most states) lacks the capacity to meet current provider demand for to meet current provider demand for information. Providers forced to ask for waivers for MU 22 Immunization Gateway Service: Solution Create Immunization Gateway Services automates portions of registration using an online portal automates portions of registration using an online portal streamline testing by validating test messages receives ongoing reports and route them to the correct regional registry g g y Prepares for CAIR 2.0 Established a strong collaboration between state CDPH, g , regional CAIR registries, CHHS, CHeQ and STC (vendor) Completing extensive testing in CDPH’s IT environment in Mayy Starting pilot submissions in mid‐May Enabling submissions for all providers in June 23 Immunization Gateway Service 7 CAIR Regions Legacy Registration R i t ti Portal Provider Gateway G Service Validation lid i Service EHR in T ti Testing Community HIO Enterprise HIO EHR Hosted ERH or EHR Hub EHR H b 24 Project INSPIRE Integrating Clinical Care with Public Health Integrating Clinical Care with Public Health Project INSPIRE INSPIRE – INteroperability p y to Support Practice pp Improvement, Disease REgistries, and Care Coordination Improve the acquisition and exchange of patient d t f hi h i data for high impact conditions in order to t diti i d t support care coordination, practice improvement and longitudinal disease registries longitudinal disease registries INSPIRE’s Two Initiatives 1. Next Generation Registries 2. The “Health Information Home” Next Generation Disease Registries: Transforming Disease Registries With EHRs and HIE Problem Registry reporting utilizes manual abstraction from charts – expensive and slow Registry knowledge of a new cancer takes 24‐36 months, which significantly impacts data usability i ifi l i d bili Data needed by registries are also needed to provide good care Structured data capture from EHRs and transfer through EHRs and transfer through Opportunity Structured data capture HIEs can dramatically improve registry case ascertainment while also improving care coordination for cancer patients Solution Implement EHR‐based capture of structured f breast cancer case data at point‐of‐care from clinicians in the Athena Breast Health Network D Demonstrate use of new HL‐7/ASCO “clinical oncology data t t f HL 7/ASCO “ li i l l d t exchange standards” Demonstrate the benefits of making the same case data available for both registries and clinical care available for both registries and clinical care The “Health Information Home” ‐ Improving Care with an HIE Document Repository Problem Patients with high impact conditions receive care from multiple providers across time and space No provider has a complete view of the patient record This leads to poor care coordination, duplicative testing, errors This leads to poor care coordination duplicative testing errors of omission, and missed opportunities for health improvement Opportunity A “health information home” will facilitate accountable care by providing a shared common view of the patient for all b d h d f h f ll providers Data going to disease registries has clinical care value Solution Implement a “health information home” using HIE technology Make the health information home accessible to providers as an HIE ‘node’ for population health management p p g Work with providers to have registry‐bound data sent to the health information home Use standards‐based data transfer New Open Library of HIE Project (OLHIE) The Problem ARRA funded assets are generally lost or impossible to find Our Solution OLHIE is developing an online ecosystem “Authors” of HIE‐related contracts, best practices, and software have a place to share their work “Readers” with real‐world resources can use to inform their work Key K Promotes reuse, cooperation, and learning to reduce P t ti dl i t d Advances the cost of building and operating HIE Prevents the loss of ARRA funded assets Enables peer review and co‐authorship of assets Streamlines workflow for authors to publish, version, p , make private, and remove assets 30 Regional and Community HIE Investments HIE Acceleration Award Program: Problem Eligible providers need access to information g Meaningful g exchange services in order to achieve Use p EHR’s are not interoperable and the costs of interface development for connectivity between unaffiliated providers is expensive, sometimes cost‐ prohibitive Medical care occurs locally California’s size and diversity precludes it from effectively implementing a “one‐size‐fits‐all” state HIE 32 HIE Acceleration Award Program: Solution Design targeted award programs aimed at accelerating the development of local/regional HIE accelerating the development of local/regional HIE infrastructure, connectivity and capacity to increase the flow of private and secure health information between unaffiliated health professionals and between unaffiliated health professionals and entities throughout the state Invest in building HIE infrastructure and expanding HIE services at the local/regional level to better serve patients integrate/coordinate care and serve patients, integrate/coordinate care and decrease cost 33 HIE Acceleration Award Program: Key Advances Funding Progress – Nearly $6,000,000 awarded to date – Half ($2.8M) awarded since HIE programs transitioned to CHeQ Half ($2 8M) awarded since HIE programs transitioned to CHeQ in Fall 2012 in Fall 2012 – CHeQ currently administering 17 awards to 13 different HIE organizations participating in 5 distinct HIE Acceleration programs (not including Rural Incentive Program) g ) HIE Progress – More than 270 HIE connections established by awardees to transmit health More than 270 HIE connections established by awardees to transmit health information electronically (not necessarily all through CHeQ funding) – More than 15 million lives potentially covered by HIE through awardees (nearly 40% of CA population) – Patient lives covered by HIE up 6.5 million lives or 80% from estimates given in 2012 (8M lives to 14.5M lives – mainly attributed to IEHIE & OCPRHIO) 34 New Rural HIE Incentive Program: Problem – Many obstacles to coordinated care in rural California – Patients travel long distances to receive care. Scarcity and distance i increase likelihood providers don’t have access to all of a patient’s lik lih d id d ’ h ll f i ’ health information resulting in fragmented and inefficient care – Implementation of Affordable Care Act (more patients) combined p ( p ) with declining number of rural physicians poised to exacerbate situation – HIE supports care integration strategies to address these challenges, HIE supports care integration strategies to address these challenges however, very limited uptake of HIE in rural California – Need for additional resources and transparency in funding for rural areas; need for standardized HIE implementations df d d d l – Sizeable or under‐serviced areas (“white space”) in many rural parts of the state 37 New Rural HIE Incentive Program: Solution Launch Rural HIE Incentive Program Promote HIE in rural areas by subsidizing the implementation services p p for rural hospitals, clinics, and individual providers Enable rural providers to adopt high‐priority, standards‐based HIE services from qualified service providers at manageable prices Program Structure g Selected five Designated Rural HIE Service Providers that offer: 1)Direct services 2) Results delivery using traditional HL7 messaging 2) Results delivery using traditional HL7 messaging 3) Community longitudinal patient record through a repository and portal or federated repository Allows new rural participants to choose services that best meet their Allows new rural participants to choose services that best meet their needs $1M fund available to subsidize 65% of the cost of qualifying service implementations through November 2013 38 New Rural HIE Incentive Program: Designated Rural HIE Service Providers Directed Exchange Services Informatics Corporation of America (ICA) Informatics Corporation of America (ICA) Redwood Mednet Directed Exchange and Longitudinal Community Record Services Di t dE h dL it di l C it R dS i Axesson Inland Empire Health Information Exchange Orange County Partnership Regional Health Information Organization (OCPRHIO) 39 New Patient Access Initiative: Blue Button for Medi‐Cal Opportunity Medi‐Cal is moving most beneficiaries into managed care plans Medi‐Cal Cal Managed Care offers an important source of Managed Care offers an important source of Medi health information for patients to access Solution Create the California Create the California Blue Button Initiative to Blue Button Initiative to Partner with one or two Medi‐Cal managed care plans Fund implementations of Blue Button functionality for patient access to health information Share as a replicable solution for Medi‐Cal managed care Advances Coordinating with Department of Health Care Services Coordinating with Department of Health Care Services Assessment of readiness among plans Will select partner health plans this summer 40 Q QUESTIONS ???