Epidemiology, Equilibria, and Ebola: A Dynamical Analysis 1 Abstract
advertisement

Epidemiology, Equilibria, and Ebola:
A Dynamical Analysis
Graham Harper
Department of Mathematics
Colorado State University - Pueblo
May 1, 2015
1
Abstract
In order to understand the forces that drive outbreaks such as the recent Ebola
outbreak in West Africa, the force of infection must be broken down into a
system of differential equations. With the current understanding of how the
equations and diseases interact, it’s possible to build diseases from equations and
build equations from diseases. Breaking down the differential equations farther
leads to a deeper understanding of what ”stability” looks like for a disease and
ultimately enables the prediction of the behavior of diseases, including points
of peak infection rates and the total number of people affected by the disease.
This paper will break down the mathematics behind compartmental epidemic
models and then use them to develop a model which affirms a hopeful future
with the decline of Ebola in West Africa so that it may take its place in history
as another disease scare that never fully developed.
Acknowledgements
• Thanks to Dr. Frank Zizza for advising, supporting, and giving me muchappreciated assistance throughout the semester
• Thanks to Haven Hall and many other classmates for allowing me to talk
with them and giving me inspirations that allowed me to move forward
• Thanks to the Mathematics Department at Colorado State University Pueblo and the University Honors Program for supporting this undergraduate thesis
1
2
Introduction
2.1
Compartmental Epidemic Models
In order to model how a disease behaves in a relevant population, the modeler must determine a population to study. This population may be as small
as a town, or as large as a state, country, or planet. Then each person in the
population must be labeled based on his or her status with regards to the disease. The healthy people are called susceptible. This category is denoted with
S. The people infected with the disease are called infected (or infective). This
category is denoted with I. These two categories are the most important to
understanding the way a disease moves through a population; however, some
diseases require other categories like R, for recovered (with immunity); E, for
exposed (but not yet contagious); D, for dead (when death is significant); V ,
for vaccinated (and immune), which may not be significantly different from R,
depending on the model. These categorical divisions of the population are by
no means permanent, however, because at any time someone in S may fall ill
and move into I. Thus in order to count the number of people in each category, counting functions S(t), I(t), etc. must be constructed. These are the
compartments for the compartmental epidemic model. These compartments
are partitions of the population because any given person must fall under one
group and no person may belong to more than one group.
In order to understand how these groups interact, a system of ordinary
differential equations must be constructed. The basis for the equations lies in
the Lotka-Volterra model for population dynamics in a predator-prey system.
If X is the prey, and Y is the predator, then the Lotka-Volterra equations are
Ẋ = αX − βXY
Ẏ = δXY − γY
where α, β, δ, and γ are constants. According to the model, in the absence of
the predator (Y ), the prey (X) will reproduce exponentially, but in the absence
of the prey, the predator will starve and die out; however, the most important
part of this model is the XY factor. This factor, along with the coefficient β or
δ represents the probability of an encounter between predator prey as well as
the outcome. If the predator and prey meet, there is a chance that the prey will
be eaten, which gives the predator a better chance of survival. Now consider a
population of susceptible people and infected people. De Jong et al. point out
that there are three factors which are relevant in the spread of the disease, but
they have meaning in both models:
1. The number of significant contacts with other people per unit time
2. The probability of this contact taking place with an infected individual
3. The probability that the contact with an infected results in a transmission
of disease
2
The first factor is a measure of the density of a population. A dense population is going to see more contacts per unit time than a sparse population,
regardless of whether it’s predator and prey or people and illness. The second
factor is what the XY factor represents in the Lotka-Volterra model. Thus the
probability of a susceptible and an infected coming into contact must be related
to S(t)I(t). The third factor is a success factor. If a predator and prey meet,
there is a chance that the prey will escape, but there is also a chance that the
prey will not escape. This represents the contagiousness of the disease being
studied. The disease transferring is a success, otherwise it is a failure.
This is as good of a time as any to bring in the basic reproduction number, which is commonly denoted with R0 . R0 is a factor which is described
as the number of people 1 person will infect before losing contagiousness if he
or she only comes in contact with others who are susceptible. R0 is directly
related to the third factor on the list. R0 is based on several factors, including
the medium through which the disease moves. If the disease is airborne, like
measles, then R0 is quite large, but if the disease if only transferred through
bodily fluids, like the Ebola virus disease, then R0 may be small. Also, if the
disease has a longer contagious period, then R0 will be larger because there is
more time to infect others.
The culmination of all of this information leads to the force of infection in
compartmental disease models, which is written as −βSI. From here forward,
S and I are assumed to be functions of time. β is a constant that represents a
combination of both societal and viral factors to decide the speed of the spread
of the disease. Sometimes it’s referred to as the contact rate for a disease,
but since β is related to R0 , it may be more appropriate to refer to it as the
infection factor. −βSI is used when writing the differential equations for a
model to describe what happens when a successful contact takes place. Here’s
what the most basic compartmental model, the SI model, looks like
Ṡ = −βSI
I˙ = βSI
Every time there is a successful contact, 1 person leaves S and enters I.
Notice that, unlike the Lotka-Volterra equations, there are no growth or death
factors for the population in this model. That’s because unless this model is
considered over a significantly long period of time, total population changes may
not have an impact on the behavior of the disease. The SI model the foundation
for all compartmental epidemic models.
3
2.2
Pseudo Mass-Action vs. True Mass-Action Models
While it was stated above that S and I are used to represent the number of
individuals in a population who are susceptible or infected, it is also possible to
use them to represent the ratio of individuals in a population who are susceptible or infected.
The model where the compartments represent the number of individuals
in a population who are susceptible or infected is called a True Mass-Action
model. When writing the differential equations for an SI true mass-action model,
and I˙ = βSI
one normally writes Ṡ = −βSI
N
N where N is the total number of
people in the population as a function of time. This model is the most accurate for modeling the way a population changes over time because it takes
into account each and every person in the population instead of ratios. This
also allows for factors that account for growth and death in the population to
be taken into account, and those will influence the progression of the disease
through changes in N . It is worth noting, however, that this model is much
harder to manipulate algebraically and computationally because generally N
looks like N = S + I with the possibility of additional terms being added in
based on the number of compartments in the model. If there are no births or
deaths in a population, then it may be more beneficial to write N (t) = k where
k is the constant population size.
The model where the compartments represent the ratio of individuals in a
population who are susceptible or infected is called a Pseudo Mass-Action
model. In an SI pseudo mass-action model, N (t) ≡ 1 so Ṡ simplifies to −βSI
and I˙ simplifies to βSI. This kind of model is much simpler to manipulate
algebraically and it will be the focus for the analysis in section 4.
It’s important to note that while these two models appear significantly different, de Jong et al. show evidence supporting the claim that there is no
significant difference in the way these models behave when applied to real world
data. This means that either model may be chosen for the user’s convenience,
so while the stability analysis may focus on the pseudo mass-action models, the
parameter estimation section may focus on using a true mass-action model with
a fixed population assumption.
4
2.3
Application to the Ebola Virus Disease
With the current understanding of the Ebola Virus Disease (hereafter referred to as Ebola), the most common deterministic epidemic model that can be
applied is the SEIR model, which assumes immunity after the patient recovers,
which has not been proven by science yet. Letting β be the same as mentioned
in section 2.1, the other coefficients and γ, are defined as the reciprocals of the
exposed and infectious periods (in the same units of time as β), respectively.
Assuming that S, E, I, and R are functions of time, a pseudo mass-action model
for Ebola may look like
Ṡ = −βSI
Ė = βSI − E
I˙ = E − γI
Ṙ = γI
˙ Ṙ = 0, the population in this model is a conserved
Notice that since Ṡ+Ė+I+
quantity (hence why the pseudo mass-action model was chosen). This model
may be applied if the time period under consideration is small enough to see
no significant change in the population due to births or death, or if birth and
death rates are not important enough to be considered. While this model works
well for modeling Ebola, there is one problem in applying this model with real
data: making measurements to track movement in and out of the exposed group
is near impossible. This means that when using real data, a simpler model is
required. An SIR model may work just as well, and it looks like
Ṡ = −βSI
I˙ = βSI − γI
Ṙ = γI
Since data is available through the WHO for the cumulative infected counts,
and cumulative death tolls, it makes sense to utilize this model instead.
One slightly difficult part of applying this model to real data is that if a
country like Guinea has 12 million people, this model claims the entire population will fall ill and recover eventually. This is erroneous to assume, so S
must be calculated by predicting the total number of cases and subtracting the
cumulative infections. This introduces some error that will be accounted for in
section 5.
5
2.4
Disease Building through Differential Equations
Using compartmental epidemic models, it’s possible to build a disease with
a physical interpretation in mind. For example, assume there is a disease which
is characterized by the following:
1. After the disease infects the victim, the victim spends an average of 5 days
unaware that he is ill and without being contagious.
2. The victim then shows symptoms and is contagious for an average of 10
days.
3. The victim has a 40% chance of developing an immunity and a 60% chance
of entering the cycle again immediately.
In order to construct a pseudo mass-action model, the compartments must
be defined first. Based on the description, there are S, E, I, and V compartments,
where V represents permanent immunity, which is equivalent to a vaccination.
Then the transfer speeds between the groups are based on the number of people
who leave a specific group every day. This is calculated by the reciprocal of the
time spent in the compartment times the number of people in the compartment.
Thus the model should look like
Ṡ = −βSI + 0.06I
Ė = βSI − 0.2E
I˙ = 0.2E − 0.1I
V̇ = 0.04I
Once again, the 0.06I term in the first equation is because 60% of infected go
straight to being susceptible again after a 10 day infectious period. The 0.2E
term in the second and third equations is because 1 person per 5 days in the
exposed category moves on. The 0.1I term in the third equation is because 1
person per 10 days in the infected category moves on. The 0.04I term in the
last equation is because 40% of people who are infected move on to being permanently immune after a 10 day infectious period. β is not given for this model,
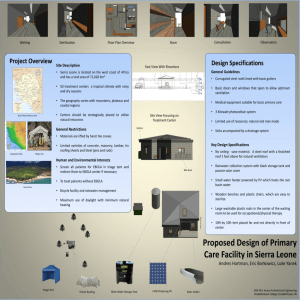
but any value can likely be justified. Assuming β = 1 and initial conditions of
S = 0.99, I = 0.01, and E = V = 0, here is a plot of the solution to this system
from Mathematica. It’s important to note that most of these systems cannot
be solved analytically by hand because of the SI term that is always required
to show up in the equations.
This model is interesting because it looks like the number of vaccinated people in the population is increasing close to 95%, while the remaining 5% never
stay immune to the disease. The peak infected growth period seems to occur
around 20 days, and the infected category peaked at 30 days.
6
The point is without knowing how a disease fits into the framework of the
model system, a model can be logically constructed relatively easily, and then
it can be solved. This is beneficial for improvising models when presented with
diseases that don’t quite fit the most common models.
Figure 1: Solutions to the SEIV Model
7
3
Common Compartmental Models and Representations
Here is a list of commonly used compartmental models, their definitions,
and some diseases that match the models well. These are not intended to be
exact matchings to the diseases, but each model is given a line of reasoning as
to why it is a good fit to help recognize the reasoning behind the model. Each
of the models are pseudo mass-action models without accounting for population
growth. The constant β represents the infection factor, represents the reciprocal of the length of the exposed period, γ represents the reciprocal of the length
of the infectious period, and ρ represents the reciprocal of the recovery period
before becoming susceptible again.
Table 1: Compartmental
Model Formulation
SI
Ṡ = −βSI
I˙ = βSI
SIS
Ṡ = −βSI + γI
I˙ = βSI − γI
SIR
Ṡ = −βSI
I˙ = βSI − γI
Ṙ = γI
Ṡ = −βSI + ρR
I˙ = βSI − γI
Ṙ = γI − ρR
Ṡ = −βSI
Ė = βSI − E
I˙ = E − γI
Ṙ = γI
Ṡ = −βSI + ρR
Ė = βSI − E
I˙ = E − γI
Ṙ = γI − ρR
SIRS
SEIR
SEIRS
Disease Models and Example Diseases
Example Diseases
AIDS (Once the disease is caught, there is no
cure for it, and the victim is contagious forever)
The Common Cold (Due to the many strains,
it may be caught anytime, but this needs to
assume a common γ for all colds)
Chickenpox (It may only be caught once in a
lifetime, but once it is caught and the victim
recovers, it cannot be caught again)
One strain of seasonal influenza (Once immunity is developed to an influenza strain, immunity lasts until the next season)
Ebola (A victim may walk around exposed
but not yet showing symptoms or being contagious, and after being contagious the victim
may either die or recover)
Ebola (Assuming that Ebola may be caught
again, although there is no scientific evidence
for this yet)
Beyond this list of compartmental models, there is another way to represent
the way a model looks. This is done with a flow diagram. They visually convey
all of the same exact information that the equations do, but in a much less
difficult way. The flow diagram is constructed by creating a box for each of
the compartments, and then drawing flow arrows between the compartments
to represent how people are moving between the compartments. Each of the
arrows are labeled with the factor from the differential equation. For example,
in the SIRS model, there are 3 compartments. This means a box should be
drawn for S, I, and R. People flow from S to I, I to R, and R to S, so arrows
8
should be drawn appropriately. The rate that people leave S and enter I is βSI,
the rate that people leave I and enter R is γI, and the rate that people leave R
and re-enter S is ρR. This means the flow diagram for an SIRS model should
look like this.
Figure 2: Flow Diagram for SIRS Model
Likewise, since everybody in an SEIR model ultimately progresses to the R
stage, a flow diagram for an SEIR model needs 4 boxes, and it looks like
Figure 3: Flow Diagram for SEIR Model
This is a useful tool for conveying ideas about almost any epidemic model
when the differential equations may not be appropriate. This is also a great intermediate step between describing the disease and writing down the differential
equations.
9
4
Equilibria of Disease Models
Many epidemic models can be solved for equilibrium points in order to better
understand the system, and these equilibrium points can be taken and analyzed
farther to see what behavior is being predicted by the differential equations
around the points. For example, the SIS pseudo mass-action model is
Ṡ = −βSI + γI
I˙ = βSI − γI
where S and I are functions of time, and beta and gamma are constants.
Setting Ṡ = I˙ = 0 yields a trivial fixed point of S = I = 0, and in fact, any
point of the form (S,0) is a fixed point since setting I = 0 solves all equations
simultaneously. However, this only means that a population that starts with no
sick people in it isn’t going to have a spontaneous illness appear. Excluding the
case where I = 0 yields S = βγ . Since this model is pseudo-mass action, there
is the additional constraint of S + I = 1, so substitution yields I = β−γ
(or
β
1 − βγ may be written when convenient), so the two fixed points of the pseudo
mass-action SIS system are (1, 0) and ( βγ , β−γ
β ).
In order to assess what the system’s behavior at these fixed points, it’s important to linearize the differential equation around the points by forming the
matrix of partials
ṠS ṠI
J=
I˙S
I˙I
In the case for the SIS model, this matrix is
−βI −βS + γ
βI
βS − γ
One of the eigenvalues of this matrix must be 0 because the matrix has
determinant 0, but the other eigenvalue requires much more work, and in this
case it is −βI + βS − γ. At any point on the line S + I = 1, the eigenvectors
for this system are
γ
− SI
−1
, βI
1
1
where the second vector corresponds to the 0 eigenvalue. These vectors
aren’t significant without considering them at an equilibrium point, so plugging
in S = βγ and I = β−γ
β yields the eigenvalues γ − β and 0 with eigenvectors
−1
0
,
1
1
10
respectively, while plugging in S = 1 and I = 0 yields the eigenvalues −γ
and 0 with eigenvectors
γ
−1
β −1
,
1
1
respectively. This means that, as suspected, the eigenvector corresponding
to the negative (attracting) eigenvalue is parallel to the line S + I = 1 but the
eigenvector corresponding to the 0 eigenvalue is pointing off of S + I = 1, but
this only holds in both cases if γ − β ≤ 0.
Considering the eigenvalues of γ − β and 0 brings the concern that γ − β may
be positive, forcing ( βγ , β−γ
β ) to be a repelling fixed point. Letting γ − β = 0
γ
yields β = 1, which means that since S = βγ = 1, this crossover from attracting
to repelling happens when the fixed point reaches the susceptible axis at the
point (1,0).
Figure 4: Phase Portrait of Solutions to an SIS model
1
with β = 21 and γ = 12
The figure above is a phase portrait of multiple directed solutions to an SIS
pseudo mass-action model. The fixed point of interest in this phase portrait is
the point ( 16 , 56 ), and it is attracting because the eigenvalue is −β(1− βγ )+β( βγ )−
1
γ = γ − β = 12
− 12 = −5
12 , so this is a stable fixed point. The phase portrait
of this system also explains the eigenvalue of 0. Leaving the line S + I = 1 is
impossible here because a crucial assumption was S + I = 1, so the eigenvector corresponding to the eigenvalue 0 should be a vector that is not parallel to
S + I = 1.
11
Figure 5: Phase Portrait of Solutions to an SIS model
1
1
with β = 20
and γ = 12
The figure above, in different from Figure 4, only in that β changed from 12
to
Since β ≤ γ now, the equilibrium point that was so obvious in Figure 4 of
( βγ , 1 − βγ ) has shifted to the point ( 53 , − 23 ), and it is now an unstable fixed point
1
because its eigenvalues are 0 and γ − β = 30
. This means that the fixed point
at (1, 0) is the one drawing everything in now because it still has eigenvalues of
1
0 and −γ = − 12
.
1
20 .
Similar methods can be applied to any compartmental models to determine
simple behavior, including the following SEIS model:
Ṡ = −βSI + γI
Ė = βSI − E
I˙ = E − γI
Setting Ṡ = Ė = I˙ = 0 still provides an equilibrium point at (1,0,0)
S ∈ R for this system, but excluding this case yields S = βγ again. Using
S + E + I = 1 yields a more complicated solution, which is found with the
substitution γI = E from I˙ = 0, so βγ + γ I + I = 1 and βγ + E + γ E = 1.
(β−γ)
This ultimately yields S = βγ , E = γ(β−γ)
β(γ+) , and I = β(γ+) . It’s important to
note that unlike the SIS model, the SEIS model has 3 compartments and thus
it may leave the line S + I = 1 in the SI phase diagram. When finding the
equilibrium
point
in the SI phase diagram, the E term is dropped because and
only βγ , (β−γ)
is plotted.
β(γ+)
12
Figure 6: Phase Portrait of Solutions to an SEIS model
1
1
with β = 21 , = 20
, and γ = 12
The above figure shows solutions to an SEIS model plotted in the SI plane
using various initial conditions along the line S + I = 1 and E = 0, with β = 12 ,
1
1
, and γ = 12
. Using
from the previous page, the equilibrium
= 20
the equations
1 5
point in the SI plane is βγ , (β−γ)
β(γ+) = ( 6 , 16 ), which is where all of the solutions
are heading. While much more work can be done to calculate the eigenvalue of
the point, the importance of this work on the SEIS model is that the procedures
to find the equilibria can be broadly applied in order to understand a variety of
epidemic models.
In short, since the equilibrium points can be found regardless of the model,
it makes more sense to compile all of the information into a table.
From the table on the next page, it’s much easier to see the equilibrium
points, and this table is very useful for determining where a disease likes to
”settle” in a population because it may move toward a state where the population has consistent proportions of susceptible, infected, exposed, or recovered.
For example, if a disease has a long infectious period and a high infection factor,
and people continuously revert back to being susceptible to it, it’s likely that
the disease will settle in the population with a high number of infected at any
given point in time, and a low number of susceptible people.
13
Table 2: Compartmental Disease Models and Equilibrium Points
Model Formulation
Equilibria
SI
(S, I): (1, 0), (0, 1)
Ṡ = −βSI
I˙ = βSI
SIS
Ṡ = −βSI + γI
(S, I): (1, 0), ( βγ , β−γ
β )
˙
I = βSI − γI
SIR
(S, I, R): Any point of the form (t, 0, 1 − t),
Ṡ = −βSI
where t ∈ [0, 1]
I˙ = βSI − γI
Ṙ = γI
SIRS
SEI
SEIS
SEIR
SEIRS
Ṡ = −βSI + ρR
I˙ = βSI − γI
Ṙ = γI − ρR
Ṡ = −βSI
Ė = βSI − E
I˙ = E
(S, I, R): (1, 0, 0),
Ṡ = −βSI + γI
Ė = βSI − E
I˙ = E − γI
Ṡ = −βSI
Ė = βSI − E
I˙ = E − γI
Ṙ = γI
Ṡ = −βSI + ρR
Ė = βSI − E
I˙ = E − γI
Ṙ = γI − ρR
(S, E, I): (1, 0, 0),
γ ρ(β−γ) γ(β−γ)
β , β(γ+ρ) , β(γ+ρ)
(S, E, I): (1, 0, 0), (0, 0, 1)
γ γ(β−γ) (β−γ)
β , β(γ+) , β(γ+)
(S, E, I, R): Any point of the form
(t, 0, 0, 1 − t), where t ∈ [0, 1]
(S,
E, I, R): (1, 0, 0, 0),
γρ(β−γ)
ρ(β−γ)
γ(β−γ)
β
,
,
,
γ β(ρ+γ+ργ) β(ρ+γ+ργ β(ρ+γ+ργ)
The reason that some of these equilibria have parametric definitions is because with the SIR model, for example, as long as I = 0, the entire system
goes to 0, so this means that S can be a free variable in [0, 1], so setting S = t,
with t ∈ [0, 1] forces R = 1 − t from the requirement that S + I + R = 1. This
condition may also be simply expressed as follows: a population without any
illness is never going to develop illness. Thus there are an infinite number of
equilibria for the SIR model.
One way to show off the behavior of epidemics may also be to develop a
program that switches between phase portraits and also allows for changes in
parameters. Luckily Mathematica has a Manipulate function that allows for a
lot of those features to be realized. The following image is a manipulator of an
SEIRS model that allows for switching between different phase portraits while
changing parameters and the number of solutions to plot.
14
Figure 7: Phase Portrait of Solutions to an SEIRS model
The code for this is located in section 7.1, but the interactivity of this model
makes it another excellent way to analyze or track equilibria. Notice that in this
phase portrait, it looks like the S and R are settling to 45% and 40%. Utilizing
the tabs can provide a totally different image of how the disease is settling.
15
5
Parameter Estimation of the Ebola Outbreak
in West Africa
It’s possible to estimate the parameters of an outbreak given the data on the
outbreak. Start by taking the collection of data (for Ebola, there is definitive
data on infected and deaths with respect to time provided by the WHO) and
form a hypothesized total effective population for the disease. Certainly for a
country like Guinea it may not make sense to consider the entire population
of 12 million people to be at risk for catching Ebola because the model would
claim that all 12 million people will fall ill, so the data in this section is based
on a population of only 5000 people in Guinea, and 10000 people in Sierra
Leone, which may be unsanitary rural populations that spread Ebola and don’t
have much contact with the more hygienic part of the countries. WHO data is
available for Guinea and Sierra Leone for cumulative infected and cumulative
death counts, but the data available for Liberia is limited to cumulative infected.
Having cumulative cases and deaths is beneficial because an average mortality
rate may also be calculated for the disease in both Guinea and Sierra Leone.
Here is a summary of the data available from the WHO
Figure 8: West Africa Cumulative Cases (since 8/29/2014)
16
Figure 9: West Africa Deaths (since 8/29/2014)
Notice that the cumulative cases data jumps by almost 2000 for Liberia at
October 29, 2014, and the Liberia death data is scattered and scarce. This is
why Liberia will not be studied in this section, although its data is present.
The difficulty in constructing a model to model the West Africa Ebola outbreak is that the available data counts cumulative cases and deaths. This means
there is a need for functions to count the total cases, and not just the present
cases. In the style of Chowell et al., the most appropriate model for this is a
SIJDR model. Here is the flow chart for it
Figure 10: Flow Diagram for SIJDR Model
The dashed line represents that J, the counting function, is counting the
number of cases that pass through the solid line. Here δ represents the death
rate in the population for the disease, which is about 40% in Sierra Leone and
60% in Guinea. The equations for this model look like
17
Ṡ = −βSI
I˙ = βSI − γI
J˙ = βSI
Ḋ = δγI
Ṙ = (1 − δ)γI
In order to calculate an estimation for β and γ, an error function needs to
be defined. This function, G : R2 → R, is defined as
X
G(β, γ) =
k (S(ti ), J(ti ), D(ti )) − (Sti , Jti , Dti ) k
i
Where S, J, and D are solutions of the SIJDR model utilising β and γ,
and Jti , Dti are the data sets from the WHO. Recall that Sti is calculated with
k −Jti where k is the assumed total population size. Once this work is done, this
function may be programmed into Mathematica, which can do a comprehensive
search for the minimum error of this function and return the β and γ values.
The code for this function is given in section 7.2.
For Sierra Leone, the minimum is G(0.045153, 0.018449) = 26762.15, and
for Guinea, the minimum is G(0.034935, 0.023391) = 7386.19. Notice that the
error for the Guinea model is much lower than the error for the Sierra Leone
model. This suggests that either the assumed populations of 5000 and 10000
caused variation, or that the Guinea data is much smoother. Both β and γ
aren’t separated by more than 0.03, which means it seems like the estimates
respect each other well.
Since the assumptions about the populations under consideration also seem
like they could be erroneous, the minimum of G was found based on many
different total population assumptions to see if there is are more appropriate
population assumptions that could be made.
18
Table 3: Min(G(β, γ)) Based on Assumed Population Size
Population (S + I)
Guinea
Sierra Leone
4000
10281.90
−
4900
7524.90
−
5000
7386.19
−
5500
6930.68
−
5600
6875.66
−
6000
6743.35
−
6100
6730.71
−
6200
6728.04
−
6300
6731.86
−
6500
6751.11
−
7000
6858.07
−
8000
7217.15
−
8600
−
58671.75
8700
−
54697.67
9000
−
44257.98
9200
−
38518.94
9500
−
31809.36
9800
−
27777.32
9900
−
27100.23
10000
−
26762.15
10100
−
26706.45
10200
−
26824.97
10500
−
27613.24
11000
−
29624.66
Looking at this table shows that the minimum error is minimized for Guinea
when a model with a population size of about 6200 is assumed and for Sierra
Leone when a population size of about 10100 is assumed. Looking back at the
SIJDR model, this means that G(0.034016, 0.025537) = 6728.04 for Guinea and
G(0.044932, 0.018703) = 26706.45 for Sierra Leone are better estimates of the
parameter, but these also help predict the end behavior of the disease.
19
6
Results
With the refined values of β = 0.034016, γ = 0.025537 for Guinea and β =
0.044932, γ = 0.018703 for Sierra Leone. Utilizing the β and γ values and
solving the SIJDR model again yields the following solutions
Figure 11: SIJD Model for Guinea
Figure 12: SIJD Model for Sierra Leone
For Guinea, the solution predicts a total of 3509.98 cases and a total of
2392.94 deaths by May 25, 2017, which corresponds to t = 1000. Assuming
20
this model is an accurate model of the real world situation, this means that the
worst of the Ebola outbreak in Guinea is in the past, and there won’t be much
more progression of the disease in the future. Likewise for Sierra Leone, the
solution predicts a total of 9030.22 cases and a total of 3992.08 deaths by May
25, 2017. This means that the worst is behind Sierra Leone, and Ebola is not
going progress much more.
This means that if this model is an accurate representation of the Ebola
outbreak in West Africa, it is likely that the outbreak is coming to a close. Beyond that, these models are just some of the tools that can be used to predict
the progression of Ebola if another outbreak occurs in another country. The
β and γ factors, or even the death ratios, may be used as estimators for an
outbreak in a nearby country like Côte d’Ivoire, should one happen. Knowing the way these models behave can help determine critical time periods for
fighting the disease in future events so that funding to fight the outbreak can
be appropriately allocated to reduce the damage caused by the disease in its
early stages, and then funding can be slowly removed as the disease slows down.
Looking forward, taking derivatives of this model and finding the points
where the derivative is maximized will help determine when future outbreaks
may take the largest toll on countries and aid in the prediction and prevention
of full-fledged outbreaks.
21
7
Code Index
7.1
Plotting Figures
To plot Figure 1:
sol = (NDSolve[
{s’[t] == -s[t] i[t] + 0.06 i[t],
e’[t] == s[t] i[t] - 0.2 e[t],
i’[t] == 0.2 e[t] - 0.1 i[t],
v’[t] == 0.04 i[t],
s[0] == 0.99, i[0] == 0.01, e[0] == v[0] == 0},
{s, e, i, v}, {t, 0, 100}][[1]]);
{a, b, c, d} = {s, e, i, v} /. sol;
Legend = SwatchLegend[{Blue, Red, RGBColor[0.8, 0.6, 0.],
RGBColor[0.1, 0.6, 0.1]}, {"Susceptible", "Exposed", "Infected",
"Vaccinated"},
LegendMarkers ->
Graphics[{EdgeForm[Black], Opacity[0.5], Rectangle[]}],
LegendLabel -> "Categories",
LegendFunction -> (Framed[#, RoundingRadius -> 5] &),
LegendMargins -> 5];
ParametricPlot[
{{t, a[t]}, {t, b[t]}, {t, c[t]}, {t, d[t]}}, {t, 0, 100},
AspectRatio -> 1, AxesLabel -> {"Time (days)", "Count"},
PlotLegends -> Legend]
To plot Figures 4 and 5:
Show[
Table[ParametricPlot[Evaluate[First[{s[t], i[t]} /. NDSolve[
{s’[t] == (-\[Beta] s[t] i[t] + \[Gamma] i[t]),
i’[t] == \[Beta] s[t] i[t] - \[Gamma] i[t],
Thread[{s[0], i[0]} == {j, 1 - j}]} /. {\[Beta] ->
1/2, \[Gamma] -> 1/12}, {s, i}, {t, 0, 5}]]], {t, 0, 5},
PlotRange -> {{0, 1}, {0, 1}}, AspectRatio -> 1,
AxesLabel -> {Susceptibles, Infected}],
{j, 0, 1, .05}] /.
Line[x_] :> {Arrowheads[Table[.03, {1}]], Arrow[x]},
ParametricPlot[{t, 1 - t}, {t, 0, 1}]]
To plot Figure 6:
Show[
Table[ParametricPlot[Evaluate[First[{s[t], i[t]} /. NDSolve[
{s’[t] == (-\[Beta] s[t] i[t] + \[Gamma] i[t]),
e’[t] == \[Beta] s[t] i[t] - \[Epsilon] e[t],
22
i’[t] == \[Epsilon] e[t] - \[Gamma] i[t],
Thread[{s[0], e[0], i[0]} == {j, 0, 1 - j}]} /. {\[Beta] ->
1/2, \[Epsilon] -> 1/20, \[Gamma] -> 1/12}, {s, i}, {t, 0,
50}]]], {t, 0, 25}, PlotRange -> {{0, 1}, {0, 1}},
AspectRatio -> 1, AxesLabel -> {Susceptibles, Infected}],
{j, 0, 1, .05}] /.
Line[x_] :> {Arrowheads[Table[.03, {1}]], Arrow[x]},
ParametricPlot[{t, 1 - t}, {t, 0, 1}]]
To plot Figure 7:
MakeFunction[l_] := Table[(l[[k]])[t], {k, 1, Length[l]}]
MakeFunction[a_, b_, c_, d_] :=
Table[MakeFunction[x], {x, {a, b, c, d}}]
bound = ParametricPlot[{t, 1 - t}, {t, 0, 1}];
Manipulate[
Sol = Table[
NDSolve[
{s’[t] == -\[Beta] s[t]*i[t] + \[Rho] r[t],
e’[t] == \[Beta] s[t]*i[t] - \[Epsilon] e[t],
i’[t] == \[Epsilon] e[t] - \[Gamma] i[t],
r’[t] == \[Gamma] i[t] - \[Rho] r[t],
Thread[{s[0], e[0], i[0], r[0]} == {j, 0, 1 - j, 0}]},
{s, e, i, r}, {t, 0, 100}][[1]],
{j, 0, 1 - 1/Res, 1/Res}];
Show[ParametricPlot[
Transpose[
MakeFunction[s /. Sol, e /. Sol, i /. Sol, r /. Sol][[{x,
y}]]], {t, 0, 100}, PlotRange -> {{0, 1}, {0, 1}},
AspectRatio -> 1,
AxesLabel -> {{"Susceptible", "Exposed", "Infected", "Recovered"}[[
x]], {"Susceptible", "Exposed", "Infected", "Recovered"}[[y]]}]
, bound, ImageSize -> 400]
, {{x, 1}, {1 -> "S", 2 -> "E", 3 -> "I", 4 -> "R"}},
{{y, 2}, {1 -> "S", 2 -> "E", 3 -> "I", 4 -> "R"}},
{{Res, 5}, 1, 15, 1, Appearance -> "Labeled"},
{{\[Beta], 1./3}, 0, 1, Appearance -> "Labeled"}, {{\[Gamma], 1./8},
0, 1, Appearance -> "Labeled"},
{{\[Epsilon], 1./9}, 0, 1,
Appearance -> "Labeled"}, {{\[Rho], 1./20}, 0, 1,
Appearance -> "Labeled"}]
To plot Figure 8:
ListPlot[{ICS[[All,{1,3}]],ICG[[All,{1,3}]],ICL[[All,{1,3}]]},
23
PlotRange->{{0,250},{0,10000},
PlotLegends->{"Sierra Leone","Guinea","Liberia"},
AxesLabel->{"Time","Infected"}]
To plot Figure 9:
ListPlot[{ICS[[All,{1,4}]],ICG[[All,{1,4}]],ICL[[All,{1,4}]]},
PlotRange->{{0,250},{0,10000},
PlotLegends->{"Sierra Leone","Guinea","Liberia"},
AxesLabel->{"Time","Deaths"}]
To plot Figures 11, 12:
Below
7.2
Estimating Parameters
To estimate parameters for the Guinea and Sierra Leone outbreaks and then
build a plot for them:
IC = Import[
"EbolaData_Sierra.xlsx", {"Data", 1,
Table[n, {n, 2, 95(*95*)}], {2, 3, 4, 7}}];
n = IC[[1, 2]] + IC[[1, 3]];
G[\[Beta]_, \[Gamma]_] :=
Module[{sol, u, v, w, x, s, i, j, d},
sol = NDSolve[
{s’[t] == -\[Beta] s[t] i[t]/n,
i’[t] == \[Beta] s[t] i[t]/n - \[Gamma] i[t],
j’[t] == \[Beta] s[t] i[t]/n,
d’[t] == \[Gamma] (\[Delta]) i[t],
s[0] == IC[[1, 2]], i[0] == IC[[1, 3]], j[0] == i[0],
d[0] == IC[[1, 4]]}, {s, j, d}, {t, 0, 500}];
{u, v, w} = {s, j, d} /. sol[[1]];
Sum[Norm[{u[IC[[k, 1]]], v[IC[[k, 1]]],
w[IC[[k, 1]]]} - {IC[[k, 2]], IC[[k, 3]], IC[[k, 4]]}], {k, 2,
94}]]
ans = FindMinimum[G, {0., 1.}, {0., 1.}, Method -> "PrincipalAxis",
WorkingPrecision -> 10]
\[Beta] = Last[ans][[1]];
\[Gamma] = Last[ans][[2]];
{SS, II, JJ, DD} = {s, i, j, d} /. NDSolve[
{s’[t] == -\[Beta] s[t] i[t]/n,
i’[t] == \[Beta] s[t] i[t]/n - \[Gamma] i[t],
j’[t] == \[Beta] s[t] i[t]/n,
d’[t] == \[Gamma] (\[Delta]) i[t],
24
s[0] == IC[[1, 2]], i[0] == IC[[1, 3]], j[0] == i[0],
d[0] == IC[[1, 4]]}, {s, i, j, d}, {t, 0, 1000}][[1]];
Legend = SwatchLegend[{Blue, Red, RGBColor[0.8, 0.6, 0.],
RGBColor[0.1, 0.6, 0.1]}, {"Susceptible", "Infected",
"Cumulative Infected", "Cumulative Dead"},
LegendMarkers ->
Graphics[{EdgeForm[Black], Opacity[0.5], Rectangle[]}],
LegendLabel -> "Categories",
LegendFunction -> (Framed[#, RoundingRadius -> 5] &),
LegendMargins -> 5];
Show[ParametricPlot[{{t, SS[t]}, {t, II[t]}, {t, JJ[t]}, {t,
DD[t]}}, {t, 0, 1000}, PlotRange -> {{0, 1000}, {0, n}},
AspectRatio -> 1, AxesLabel -> {"Time (days)", "Count"},
PlotLegends -> Legend, PlotStyle -> Thick],
ListPlot[IC[[All, {1, 2}]]],
ListPlot[IC[[All, {1, 4}]], PlotStyle -> RGBColor[0.1, 0.4, 0.1]]]
{SS[1000], II[1000], JJ[1000], DD[1000]}
25
8
WHO Data (for reference)
Here is the data that was utilized in this paper from the WHO. Each of these
data sets represents the date versus the number of total confirmed cases/deaths
in a specific country. The data came from https://data.hdx.rwlabs.org/ebola
where much more Ebola data is stored, but this specific data came from the csv
file on https://data.hdx.rwlabs.org/dataset/ebola-cases-2014 The 4 data points
marked with * are missing death counts that were set to an arbitrary close value
instead of 0 to prevent large amounts of error entering the models.
Guinea Cases
8/29/2014 482
9/5/2014 604
9/8/2014 664
9/12/2014 678
9/16/2014 743
9/18/2014 750
9/22/2014 818
9/24/2014 832
9/26/2014 876
10/1/2014 950
10/3/2014 977
10/8/2014 1044
10/10/2014 1097
10/15/2014 1184
10/17/2014 1217
10/22/2014 1289
10/25/2014 1312
10/29/2014 1391
10/31/2014 1409
11/5/2014 1457
11/7/2014 1479
11/12/2014 1612
11/14/2014 1647
11/19/2014 1698
11/21/2014 1745
11/26/2014 1850
12/1/2014 1921
12/3/2014 1929
12/10/2014 2051
12/15/2014 2115
12/17/2014 2127
12/22/2014 2259
12/23/2014 2284
12/24/2014 2284
12/26/2014 2342
12/29/2014 2384
12/30/2014 2397
12/31/2014 2397
1/2/2015 2435
1/5/2015 2465
1/6/2015 2471
1/7/2015 2471
1/8/2015 2477
1/9/2015 2493
1/12/2015 2508
1/13/2015 2508
1/14/2015 2514
1/15/2015 2522
1/16/2015 2525
1/19/2015 2539
1/20/2015 2539
1/21/2015 2539
1/22/2015 2542
1/23/2015 2545
1/26/2015 2559
1/27/2015 2569
1/28/2015 2569
1/29/2015 2571
1/30/2015 2575
2/2/2015 2593
2/3/2015 2608
2/4/2015 2608
2/5/2015 2621
26
2/6/2015 2628
2/10/2015 2674
2/11/2015 2674
2/12/2015 2685
2/13/2015 2693
2/16/2015 2720
2/17/2015 2727
2/18/2015 2727
2/19/2015 2732
2/20/2015 2734
2/23/2015 2758
2/25/2015 2762
2/26/2015 2781
2/27/2015 2790
3/2/2015 2808
3/4/2015 2808
3/5/2015 2833
3/6/2015 2840
3/10/2015 2871
3/11/2015 2871
3/12/2015 2901
3/13/2015 2911
3/16/2015 2957
3/17/2015 2966
3/18/2015 2966
3/20/2015 2988
3/23/2015 3007
3/24/2015 3011
3/25/2015 3011
3/26/2015 3032
3/27/2015 3042
Liberia Cases
8/29/2014 322
9/5/2014 614
9/8/2014 634
9/12/2014 654
9/16/2014 790
9/18/2014 812
9/22/2014 863
9/24/2014 890
9/26/2014 914
10/1/2014 927
10/3/2014 931
10/8/2014 941
10/10/2014 943
10/15/2014 950
10/22/2014 965
10/25/2014 965
10/29/2014 2515
10/31/2014 2515
11/5/2014 2451
11/7/2014 2514
11/12/2014 2553
11/14/2014 2562
11/19/2014 2643
11/21/2014 2669
11/26/2014 2727
12/1/2014 2801
12/3/2014 2801
12/10/2014 2830
12/15/2014 2946
12/17/2014 2946
12/22/2014 3085
12/23/2014 3085
12/24/2014 3085
12/26/2014 3085
12/29/2014 3108
12/30/2014 3108
12/31/2014 3110
1/2/2015 3110
1/5/2015 3116
1/6/2015 3118
1/7/2015 3118
1/8/2015 3118
1/9/2015 3123
1/12/2015 3123
1/13/2015 3123
1/14/2015 3127
1/15/2015 3127
1/16/2015 3127
1/19/2015 3131
1/20/2015 3135
1/21/2015 3135
1/22/2015 3136
1/23/2015 3136
1/26/2015 3136
1/27/2015 3138
1/28/2015 3138
1/29/2015 3138
1/30/2015 3138
2/2/2015 3138
2/3/2015 3143
2/4/2015 3143
2/5/2015 3143
2/6/2015 3143
2/10/2015 3146
2/11/2015 3146
2/12/2015 3146
2/13/2015 3147
2/16/2015 3149
2/17/2015 3149
2/18/2015 3149
2/19/2015 3152
2/20/2015 3152
2/23/2015 3153
2/25/2015 3153
2/26/2015 3153
2/27/2015 3153
3/2/2015 3153
3/4/2015 3153
3/5/2015 3150
3/6/2015 3150
3/10/2015 3150
3/11/2015 3150
3/12/2015 3150
3/13/2015 3150
3/16/2015 3150
3/17/2015 3150
3/18/2015 3150
3/20/2015 3150
3/23/2015 3151
3/24/2015 3151
3/25/2015 3151
3/26/2015 3151
3/27/2015 3151
Sierra Leone Cases
8/29/2014 935
9/5/2014 1146
9/8/2014 1234
9/12/2014 1287
9/16/2014 1464
9/18/2014 1513
9/22/2014 1640
9/24/2014 1745
9/26/2014 1816
10/1/2014 2076
10/3/2014 2179
10/8/2014 2455
10/10/2014 2593
10/15/2014 2849
10/17/2014 2977
10/22/2014 3223
10/25/2014 3389
10/29/2014 3700
10/31/2014 3778
11/5/2014 4057
11/7/2014 4149
11/12/2014 4523
11/14/2014 4683
11/19/2014 5056
11/21/2014 5152
11/26/2014 5441
12/1/2014 5831
12/3/2014 5978
12/10/2014 6375
12/15/2014 6638
12/17/2014 6702
12/22/2014 6975
12/23/2014 7017
12/24/2014 7017
12/26/2014 7160
12/29/2014 7326
12/30/2014 7354
12/31/2014 7354
27
1/2/2015 7476
1/5/2015 7570
1/6/2015 7602
1/7/2015 7602
1/8/2015 7759
1/9/2015 7759
1/12/2015 7766
1/13/2015 7766
1/14/2015 7786
1/15/2015 7802
1/16/2015 7825
1/19/2015 7883
1/20/2015 7903
1/21/2015 7903
1/22/2015 7909
1/23/2015 7921
1/26/2015 7963
1/27/2015 7968
1/28/2015 7968
1/29/2015 7977
1/30/2015 7989
2/2/2015 8042
2/3/2015 8059
2/4/2015 8059
2/5/2015 8063
2/6/2015 8084
2/10/2015 8135
2/11/2015 8135
2/12/2015 8138
2/13/2015 8155
2/16/2015 8199
2/17/2015 8212
2/18/2015 8212
2/19/2015 8223
2/20/2015 8223
2/23/2015 8223
2/25/2015 8289
2/26/2015 8308
2/27/2015 8320
3/2/2015 8353
3/4/2015 8353
3/5/2015 8383
3/6/2015 8389
3/10/2015 8428
3/11/2015 8428
3/12/2015 8463
3/13/2015 8469
3/16/2015 8484
3/17/2015 8487
3/18/2015 8487
3/20/2015 8508
3/23/2015 8518
3/24/2015 8520
3/25/2015 8520
3/26/2015 8529
3/27/2015 8532
Guinea Deaths
8/29/2014 287
9/5/2014 362
9/8/2014 400
9/12/2014 403
9/16/2014 429
9/18/2014 435
9/22/2014 465
9/24/2014 468
9/26/2014 481
10/1/2014 535
10/3/2014 562
10/8/2014 587
10/10/2014 598
10/15/2014 653
10/17/2014 671
10/22/2014 710
10/25/2014 732
10/29/2014 732*
10/31/2014 732*
11/5/2014 837
11/7/2014 850
11/12/2014 934
11/14/2014 958
11/19/2014 982
11/21/2014 998
11/26/2014 1050
12/1/2014 1102
12/3/2014 1117
12/10/2014 1207
12/15/2014 1255
12/17/2014 1262
12/22/2014 1323
12/23/2014 1344
12/24/2014 1344
12/26/2014 1385
12/29/2014 1422
12/30/2014 1433
12/31/2014 1433
1/2/2015 1463
1/5/2015 1488
1/6/2015 1499
1/7/2015 1499
1/8/2015 1504
1/9/2015 1515
1/12/2015 1523
1/13/2015 1523
1/14/2015 1530
1/15/2015 1537
1/16/2015 1541
1/19/2015 1556
1/20/2015 1557
1/21/2015 1557
1/22/2015 1560
1/23/2015 1561
1/26/2015 1574
1/27/2015 1578
1/28/2015 1578
1/29/2015 1579
1/30/2015 1581
2/2/2015 1595
2/3/2015 1597
2/4/2015 1597
2/5/2015 1600
2/6/2015 1608
2/10/2015 1643
2/11/2015 1643
2/12/2015 1651
2/13/2015 1659
2/16/2015 1678
2/17/2015 1683
2/18/2015 1683
2/19/2015 1686
2/20/2015 1688
2/23/2015 1699
2/25/2015 1704
2/26/2015 1714
2/27/2015 1721
28
3/2/2015 1735
3/4/2015 1735
3/5/2015 1749
3/6/2015 1755
3/10/2015 1778
3/11/2015 1778
3/12/2015
3/13/2015
3/16/2015
3/17/2015
3/18/2015
3/20/2015
Liberia Deaths
8/29/2014 225
9/5/2014 431
9/8/2014 508
9/12/2014 498
9/16/2014 563
9/18/2014 631
9/22/2014 670
9/24/2014 671
9/26/2014 792
10/1/2014 890
10/3/2014 934
10/8/2014 1018
10/10/2014 1072
10/22/2014 1241
10/25/2014 1241
2/10/2015 3826
2/11/2015 3826
2/12/2015 3826
2/13/2015 3858
Sierra Leone Deaths
8/29/2014 380
9/5/2014 443
9/8/2014 461
9/12/2014 478
9/16/2014 514
9/18/2014 517
9/22/2014 545
9/24/2014 552
9/26/2014 557
10/1/2014 574
10/3/2014 575
10/8/2014 725
10/10/2014 753
10/15/2014 926
10/17/2014 932
10/22/2014 986
10/25/2014 1008
10/29/2014 1008*
10/31/2014 1008*
11/5/2014 893
11/7/2014 921
11/12/2014 960
11/14/2014 978
11/19/2014 1041
11/21/2014 1058
11/26/2014 1189
12/1/2014 1321
12/3/2014 1374
12/10/2014 1559
12/15/2014 1824
12/17/2014 1876
12/22/2014 2190
12/23/2014 2216
12/24/2014 2216
12/26/2014 2289
12/29/2014 2366
12/30/2014 2392
12/31/2014 2392
1/2/2015 2461
1/5/2015 2549
1/6/2015 2577
1/7/2015 2577
1/8/2015 2611
1/9/2015 2611
1/12/2015 2683
1/13/2015 2683
1/14/2015 2696
1/15/2015 2701
1/16/2015 2717
1/19/2015 2766
1/20/2015 2779
1/21/2015 2779
1/22/2015 2787
1/23/2015 2793
1/26/2015 2829
1/27/2015 2833
1/28/2015 2833
1/29/2015 2841
1/30/2015 2850
2/2/2015 2908
2/3/2015 2910
2/4/2015 2910
2/5/2015 2920
2/6/2015 2935
2/10/2015 2975
2/11/2015 2975
2/12/2015 2984
2/13/2015 2997
2/16/2015 3035
2/17/2015 3042
2/18/2015 3042
2/19/2015 3057
2/20/2015 3057
2/23/2015 3057
2/25/2015 3095
2/26/2015 3113
2/27/2015 3124
3/2/2015 3164
3/4/2015 3164
3/5/2015 3199
3/6/2015 3210
3/10/2015 3263
3/11/2015 3263
3/12/2015 3289
3/13/2015 3297
3/16/2015 3321
3/17/2015 3325
3/18/2015 3325
3/20/2015 3346
3/23/2015 3376
3/24/2015 3381
3/25/2015 3381
3/26/2015 3398
3/27/2015 3407
1792
1797
1821
1829
1829
1846
29
3/23/2015
3/24/2015
3/25/2015
3/26/2015
3/27/2015
1863
1865
1865
1875
1878
References
[1]
Roy M Anderson and Robert M May. “Population biology of infectious
diseases: Part I.” In: Nature 280 (1979), pp. 361–7.
[2]
Gerardo Chowell et al. “SARS outbreaks in Ontario, Hong Kong and Singapore: the role of diagnosis and isolation as a control mechanism”. In:
Journal of Theoretical Biology 224.1 (2003), pp. 1–8.
[3]
Herbert W Hethcote. “The mathematics of infectious diseases”. In: SIAM
review 42.4 (2000), pp. 599–653.
[4]
John A Jacquez and Philip O’Neill. “Reproduction numbers and thresholds
in stochastic epidemic models I. Homogeneous populations”. In: Mathematical Biosciences 107.2 (1991), pp. 161–186.
[5]
Mart CM de Jong, Odo Diekmann, and Hans Heesterbeek. “How does
transmission of infection depend on population size”. In: Epidemic models:
their structure and relation to data 5.2 (1995), pp. 84–94.
[6]
Denis Mollison. Epidemic models: their structure and relation to data. Vol. 5.
Cambridge University Press, 1995.
[7]
S Towers and Z Feng. Pandemic H1N1 influenza: Predicting the course of
vaccination programme in the united states. 2009.
[8]
Sherry Towers, Oscar Patterson-Lomba, and Carlos Castillo-Chavez. “Temporal variations in the effective reproduction number of the 2014 West
Africa Ebola outbreak”. In: PLoS currents 6 (2014).
30