$10-0 HMO Plan $25 - 500 w/Chiro HMO Plan
advertisement

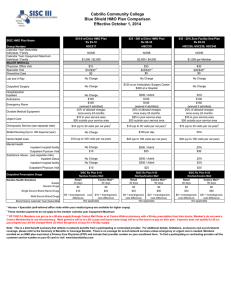
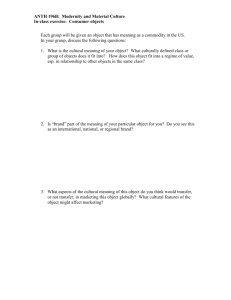
Cabrillo Community College Blue Shield HMO Plan Comparison Effective October 1, 2015 $10-0 HMO Plan Rx $5-10 $25 - 500 w/Chiro HMO Plan Rx $9-35 $30 - 20% Zero Facility Ded Plan Rx $9-35 HSC217 HSC218 HSC238, HSC239, HSC240 NONE NONE NONE $1,000 / $2,000 $2,000 / $4,000 $1,500 / $3,000 $10 $10/$30*1 $0 $25 $25/$30*1 $0 $30 $30/$45*1 $0 Lab and X-Ray No Charge No Charge No Charge Outpatient Surgery No Charge $150 at an Ambulatory Surgery Center $300 at a Hospital No Charge No Charge $100 $100 (waived if admitted) 20% of allowed charges once every 24 months $10 in your service area $50 outside your service area $10 (up to 30 visits conbined with Acupuncture per cal year)1 $500 / Admit $100 $100 (waived if admitted) 20% of allowed charges once every 24 months $25 in your service area $50 outside your service area $10 (up to 30 visits conbined with Acupuncture per cal year)1 20% $100 $150 (waived if admitted) 20% of allowed charges once every 24 months $30 in your service area $50 outside your service area $10 (up to 30 visits conbined with Acupuncture per cal year)1 No Charge $100 per day 20% $10 (up to 100 visits per cal year) $25 (up to 100 visits per cal year) $30 (up to 100 visits per cal year) No Charge $10 $500 / Admit $25 20% $30 No Charge No Charge $500 / Admit $500 / Admit 20% 20% $10 $25 $30 SISC HMO Plan Name Group Number Calendar Year Deductible Individual / Family Calendar Year Out-of-Pocket Maximum Individual / Family MAJOR MEDICAL Physician Office Visit Specialist Visit Preventive Care Hospitalization Inpatient Ambulance Emergency Room Durable Medical Equipment Urgent Care Chiropractic Service/Acupuncture (services through ASH) Skilled Nursing (Up to 100 days/cal year) Home Health Care Mental Health Inpatient hospital facility Outpatient Pysician Visit Substance Abuse - (see separate rider) Inpatient Detox Inpatient hospital facility Outpatient Physican Visit Outpatient Prescription Drugs Navitus Health Solutions Supply Generic Drugs Single Source Brand Name Drugs Multi Source Brand Drugs Brand Name Calendar Year Deductible SISC Rx Plan 5-10 Navitus /Costco Mail Retail Costco Mail** 30 days 90 days SISC Rx Plan 9-35 Navitus/Costco Mail Retail Costco Mail** 30 days 90 days SISC Rx Plan 9-35 Navitus/Costco Mail Retail Costco Mail** 30 days 90 days $5 $0 $9 $0 $9 $0 $10 $20 $35 $90 $35 $90 $5 + brand/generic cost $15 + brand/generic difference cost difference Not applicable $9 + brand/generic $27 + brand/generic cost difference cost difference Not applicable $9 + brand/generic $27 + brand/generic cost difference cost difference Not applicable * Access + Specialist (self-referred office visits within your medical group are available for higher copay) 1 These member payments do not apply to the member calendar year Copayment Maximum ** Eff 10/01/14, Members can get up to a 90-day supply through Costco Mail Order or at Costco Walk-in pharmacy with a 90-day prescription from their doctor. Member's do not need a Costco Membership to use the pharmacy. Most generics will be at a $0 co-pay and brand name drugs will be at the brand co-pay on their plan. If generic does not qualify for $0 copay program you will be charged three (3) times the generic co-pay for a 90-day supply. Note: This is a brief benefit summary that reflects in-network benefits from a participating or contracted provider. For additional details, limitations, exclusions and out-of-network coverage, please refer to the Summary of Benefits or Coverage Booklet. There is no coveage for out-of-network services unless emergency or urgent care is needed. Members enrolled on an HMO plan must elect a Primary Care Physician (PCP) and include their provider number on your enrollment form. To find a participating or contracting provider call the customer service number on your ID card or visit www.blueshieldca.com