")
Health Care Reform Strategies
Iowa Superintendents Finance & Leadership Consortium
(ISFLC)
February 13, 2013
Outline – Healthcare Reform
Market Developments
Strategies that Work
Employer Requirements
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
2
Market Developments
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
3
#1: The Rules Change…
Employer Mandate
Individual Mandate
Guaranteed Availability
•Penalties apply for insufficient
coverage.
•Penalties apply for lack of
coverage.
•Incentives/subsidies
•Limitations due to Pre-Existing
conditions are removed.
Most large employer, 200+
employees, will not likely find
it financially feasible to exit
group health benefits.
Income levels weigh in on
subsidy/incentives.
Removes Pre-X for individual
and group insurance.
Pricing & Products are not
issued for 2014.
Medicaid Expansion
Plan requirements - ongoing
Public Exchanges and COOPs
still in development.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
4
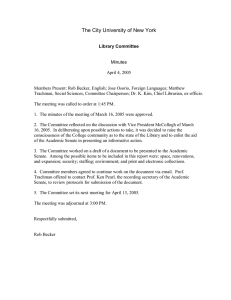
#2: The Prices Change…
Health Insurance Costs By Gender & Age
Using Actual Individual Medical Rates for 2012
(Iowa Based Rates)
Monthly Individual Rates (Non-Smoker)
$1,600
$1,400
$1,200
$1,000
$800
$600
$400
$200
$18 & Under
23
28
33
38
43
48
53
58
63
Age Category
Single Male
Single Female
Married + 2 Kids
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
5
What Direction to Take?
…Strategies that Work
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
6
Strategies that Work
1. Collaboration
2. Analytics
3. Risk Management
4. Behavioral Change
5. Repositioning
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
7
1. Collaboration
Reform/create an effective team.
An Insurance Advisory Committee - An often overlooked and
under utilized resource within any employer.
The effective use of a dedicated team with diverse
stakeholders from your District can be the key to:
Cost management
Benefit selection
Value based change
Employee satisfaction
Bargaining
…and more.
Consider the “playbook” from Ankeny CSD…
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
8
The Process
Overview
• Task – Ensure equitable representation of all certified and non-certified
staff as it pertains to benefits.
• Purpose – The purpose of the Insurance Advisory Committee is to
serve as an advisory body and accept some fiduciary responsibility to
School officials as it pertains to the selection, management, and design of
designated employee benefits.
• Desired Outcome – provide input towards the efficient and
effective use and delivery of designated employee benefits.
Your Logo
©Copyright 2013, Mark J. Becker & Associates, LLC
9
The Process
Keys for Success
Survey Stakeholders
• Gain input
• Identify action
items/need
Create Committee
• Keys to Success
• Unbiased Approach
• Fiduciary Responsibility
• Common Good
• Purpose, Principles, Role
Implement/Manage Change
Hire Consultant
• Targeted Objectives
• Measurable Goals
• Mutual Benefit
• Strategic Orientation
• Analytics/Insight
• Educate
• Process/Results Driven
• Advocacy/Representation
Your Logo
©Copyright 2013, Mark J. Becker & Associates, LLC
10
The Process
Cumulative Changes
Managed Change
Strategic Change
Insufficient Change
©Copyright 2013, Mark J. Becker & Associates, LLC
11
2. Analytics
“You can’t manage, what you can’t measure…”
Identification
Quantification
Modeling
Solving
….a problem, solution, conditions through measuring and
nesting organization strategy, mission, vision into Key
Performance Indicators
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
12
Analytics/Metrics Expanded
Some examples of Benefit Metrics include:
Cost per FTE
Trend & Regressions
Diagnostic categories
Bio-metrics
Rx Measures
PTO integration with Disability
Employee premium sharing versus plan design cost
sharing
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
13
3. Risk Management
Insurance is a tool to transfer/accept risk
If you don’t know your risk, how do you know what your
insurance needs are?
Some benefits do not need insuring…
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
14
Risk Evaluation
Risk Analysis:
Key Questions:
Is your group a super/sub-standard Risk?
Risk Tolerance
What can you afford/absorb?
What do you need to transfer/retain
What is your contractual, financial, philosophical &
social obligation?
Risk Tools
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
15
Risk Tools
Financial Tension – Sharing risk with employees
through Plan Design and Premiums (CDHP’s, etc.).
Risk Transfer – reinsurance contracts (self-insured)
and pooling points (fully-insured)
Funding – reassessing insurance vs. non-insurance
based benefits
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
16
Risk Transfer
High Cost
Too Little Protection
Cost Curve
Too Much Protection
Least Cost
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
17
Funding
Funding Arrangements/tools:
Funding methods shift - risk , timing, & cost
Financial and Legal
Administrative contracts vary in legal risk
accepted/transferred.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
18
The Continuum of Funding Alternatives
Fixed Costs
Insured
100% Pooled
Transfer of Financial &
Legal Risk
Minimum
Premium
Variable Cash Flow
Self-insured
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
19
4. Behavioral Change
Wellness Initiatives – Health screening, smoking
cessation, weight control programs, etc. (Accountability
Measures)
Value-Based Benefits – Waiving or lowering cost
sharing for preventive and chronic conditions. (Steerage
Measures)
Employee Education – Improve the amount and
quality of data available on health care costs and
quality outcomes measurements. (Education Measures)
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
20
5. Repositioning
Sharing – philosophical/cultural
Open Enrollment versus annual election
Cash out/waiver options
How much does/should the Employer pay versus Employee?
Premium or Plan Design
Premium sharing socializes the cost equally
Plan design individualizes the cost
Variable (coinsurance) vs fixed components (copays/deductibles)
Tiering of Rates
To help one tier pay less, another tier must pay more - algebra
Spousal Carve-out – how much to pay for another
employers employee?
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
21
5. Repositioning
Additional Strategic Considerations
Par-Contracts – expand upside, reduce downside
Reserving
Pay or Play modeling
New Markets (i.e. Exchanges)
Avoiding/Embracing ACA fees/penalties
Expected pricing shift due to community rating
Cadillac Tax avoidance
Various Fees
Etc.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
22
Strategies that Work
1. Collaboration
2. Analytics
3. Risk Management
4. Behavioral Change
5. Repositioning
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
23
Employer Requirements
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
24
Patient Protection and Affordable Care Act
Compliance –
• For the most part, the burden of compliance has first fallen to Government entities,
the health care industry, and insurance vendors.
• For example, insurance vendors have, and will continue, to prompt group
customers on compliance requirements when/where the burden falls on the
vendor.
• Fully-Insured: To date, many of the 2010-2012 required ACA provisions have
been prompted by and implemented by insurance vendors for their fullyinsured groups.
• Self-Insured: To date, most insurance vendors have also notified self-insured
groups of required provisions….however implementation of such is not always
included and the burden falls to the self-insured plan sponsor.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
25
PPACA Fees Imposed on or Passed to Employers
2013:
• Patient-Centered Outcomes Research Institute (PCORI) Trust Fund: Establishes a research
fee to be assessed from all health plans including retiree-only plans which are generally exempt
from most PPACA requirements. Fees are due by July 31, 2013 for calendar year plans. For fiscal
year plans ending before October 1, the first fee is due by July 31, 2014. Employers will be
assessed this annual fee that begins as $1 times the average number of covered lives. The fee
increases the following year to $2 and is indexed thereafter. Four methods for calculation are
available. Plan sponsors and issuers must report the fees under Code Sections 4375 and 4376 on
Form 720. Most insurance vendors will incorporate the fees into the rates and file Form 720 for
fully-insured plans.
2014:
• Transitional Reinsurance Fee: Established to help stabilize premiums for coverage in the
individual market during the first three years of exchange operations. Designed to mitigate the
potential impact of adverse selection resulting from a large pool of previously uninsured
individuals seeking coverage. HHS estimates the fee for 2014 to be $5.25 per member per month
which is $63 annually for each covered employee, spouse and dependent. HHS will require
enrollment information to be submitted (by insurers and third party administrators) by Nov. 15,
2014 and will notify them within a month of contributions due, which must be paid within 30
days of notification.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
26
PPACA Fees Imposed on or Passed to Employers
2014:
• Annual Fee on Health Insurance Companies “Users Fee or Insurance Fee”:
Beginning in 2014, health insurance companies with net premiums exceeding $25
million will pay an annual fee expected to raise a total of $60 billion thru 2019. The fees
begin at $8 billion in 2014 and are assessed based on an insurance company’s market
share and are non-deductible for federal tax purposes. These fees are the
responsibility of the insurance carrier to pay; however, they are expected to be passed
along to both grandfathered and non-grandfathered small groups and fully-insured
large group customers.
At this time the fee expected to be passed on to employers with Wellmark insurance is
approximately $7 - $9 per member per month. Other carriers may be applying the fee using
different calculation methods such as a percent of annual premium. The amount of the fee from
carriers will differ since market share differs. Employers need to be aware and include this in their
budget setting process.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
27
Patient Protection and Affordable Care Act
2014:
Health Insurance Premium and Cost Sharing Subsidies: Beginning January 1, 2014,
various refunds and tax credits become available to eligible individuals. Families with
incomes between 133-400% of the Federal Poverty Level (FPL) can use such monies to
purchase insurance through the Exchanges. Subsidies are available to those with incomes
up to 250% of the FPL. Tax credits and subsidies will not be available to individuals who
have “affordable” employer sponsored coverage available to them that also provides
“minimum value.” Similarly, an employer will not be subject to a penalty tax if it offers to
full-time employees “affordable” health coverage that provides “minimum value”.
Affordable = Cost of coverage to the employee does not exceed 9.5% of the wages the employer pays that
employee as stated in Box 1 of the W2; affordability test applies to single coverage on the lowest-cost plan
option available to the employee. Coverage may also be deemed affordable if it satisfies either of two other
design-based safe harbors.
Minimum Value = The plan covers at least 60% of the total allowed cost of benefits expected to be incurred
under the plan. Employers can input plan design data into actuarial value calculators that the HHS is making
available in order to determine if the plan is providing minimum value.
Health Insurance Exchanges: Effective January 1, 2014, the State exchanges are to be
operational and available to individuals and small employers with up to 100 employees.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
28
Patient Protection and Affordable Care Act
2014:
Employer Shared Responsibility (pay or play): Effective January 1, 2014, a fee is
imposed on employers with more than 50 employees (using an equivalent for part-time
employees) that fail to offer coverage to all full-time employees (defined as employees
who work an average of at least 30 hours/week). The fee is $2,000 per full-time
employee, excluding the first 30 employees. An employer who offers coverage to all fulltime employees could also be subject to a fee if the coverage is not “affordable” or does
not provide a “minimum level” of coverage. In this case, the fee is the lesser of (a) $3,000
for each full-time employee who receives a premium tax credit for coverage purchased on
the exchange or (b) $2,000 for each full-time employee excluding the first 30 employees.
Determining Full Time Employees:
•
A teacher or another employee working an average of at least 30 hours/week during the school
year is considered full-time. Count actual hours worked and all periods of paid leave. Summer
breaks or other periods of unpaid leave generally cannot reduce the average hours they work
during the school year.
•
Count actual hours worked for substitute teachers. If they work an average of at least 30
hours/week during the school year then they will be considered full-time.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
29
Patient Protection and Affordable Care Act
2018:
• Tax on High-Cost Insurance: Commonly referred to as the “Cadillac Tax” and
effective January 1,2018. This is an excise tax on employer-sponsored health
plans that have expenses exceeding $10,200 for individual coverage and
$27,500 for family coverage.
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
30
Cadillac Tax Example
Illustrative Health Insurance Premium Projections for Family Coverage
Assuming Average Growth Rate of 7.3% from 2012-2020
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
31
IN CONCLUSION…….
1. Engage in strategies that
work.
2. Reposition as necessary.
3. Check your progress
toward compliance.
Sources:
Quarles & Brady LLP – “Health Care Reform Pay or Play Guide”; via
the International Foundation of Employee Benefits
National Institute For Health Care Management – “The Challenges
of Pricing Health Insurance for the 2014 Exchanges”
Truven Health Analytics – “Modeling the Impact of Pay or Play
Strategies on Employer Health Costs”
Henry j. Kaiser Family Foundation – “Focus on Health Reform”
Keri K. Farrell-Kolb; Attorney at Law, Nyemaster Goode, P.C.
Mark J. Becker & Associates, LLC – proprietary analytical tools
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
32
Thank you!
Mark J. Becker
President
Mark J. Becker & Associates, LLC
Keri K. Farrell-Kolb
Attorney at Law
Nyemaster Goode, P.C.
Brenda J. Plantz
Assistant Vice President
Mark J. Becker & Associates, LLC
Mark J. Becker & Associates, LLC
5501 NW 86th St., Suite 700
Johnston, IA 50131
515-273-5140
www.MJBAconsulting.com
©Copyright 2013 by Mark J. Becker & Associates – All Rights Reserved
33
")