Predicting infected but undetected infections during the 2007 Foot-and-Mouth Disease outbreak
advertisement

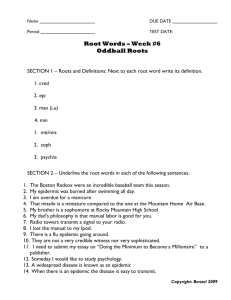
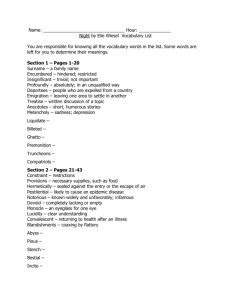
Predicting infected but undetected infections during the 2007 Foot-and-Mouth Disease outbreak Jewell CP, Keeling MJ, Roberts GO April 24, 2008 Active disease surveillance during epidemics is of utmost importance in detecting and eliminating new cases quickly, and targetting such surveillance to high-risk individuals is generally more efficient than applying a random strategy 7;12 . Contact tracing has been used as a form of at-risk targetting, and a variety of mathematical models have indicated that it is likely to be highly efficient 4;14 . However for fast-moving epidemics, resource constraints limit the ability of the authorities to perform, and follow up, contact-tracing effectively. Here, as an alternative, we present a real-time Bayesian statistical methodology to determine currently undetected (occult) infections 10 . For the UK Foot-and-Mouth epidemic of 2007, we use real-time epidemic data synthesised with previous knowledge of FMD outbreaks in the UK to predict which premises might have been infected, but remained undetected, at any point during the outbreak. This provides both a framework for targetting surveillance in the face of limited resources, and also an indicator of the current severity and spatial extent of the epidemic. Our results demonstrate how statistical approaches to real-time prediction can yield meaningful results in the face of small amounts of data and, therefore, a high degree of statistical uncertainty. This methodology thus provides a compromise between targetted manual surveillance and random or spatially targetted strategies. We anticipate such methods to be of substantial benefit in future outbreaks of livestock diseases, providing a rigorously quantitative base for the assessment of control measures, targetting of disease surveillance, and assessment of the current extent of the outbreak. Epidemic control essentially focuses on reducing the risk of transmission between susceptible and infected individuals. Traditional methods such as vaccination or pre-emptive culling serve to decrease the size of the susceptible population and may be used with varying success 1;13;22 . An alternative strategy is to focus on infected individuals, either quarantining or culling to prevent onward transmission. In such cases, early detection is vital to reduce the time for which the individual is actively shedding infection 5;9;22 . When infection occurs significantly before the onset of symptoms, mechanisms of contact tracing become vital with the aim of indentifying at-risk individuals by their interaction with known infectious cases 19 . 1 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism Contact tracing has traditionally and successfully been used for a variety of human diseases, including the 2003 SARS outbreak when high-risk individuals were quarantined and a variety of sexually transmitted infections where at-risk contacts are tested and treated 2;3 . For foot-and-mouth disease, contact tracing from known Infected Premises (IPs) is manditory, generating Dangerous Contacts (DCs) whose livestock must be culled. During the 2001 Footand-Mouth outbreak in the UK, contact tracing only was deemed insufficient to control the epidemic – the high number of cases and the limited veterinary resources meant that contacts could not be identified and removed quickly enough 5;6;13 . Indeed, subsequent studies have demonstrated that for epidemics where the number of cases and/or contacts is high, contact tracing loses its efficacy due to resource constraints 4;11;14 . Given these resource constraints, the Contiguous Premises (CP) cull policy (where animals on premises neighbouring IPs were culled) was implemented as a cude but rapid method of identifying and removing potentially at-risk premises 8;21 . During the 2007 FMD outbreak in Surrey, however, the number of cases was small and policy better developed in the wake of 2001, so that effective contact tracing was implemented. This lead to a large number of dangerous contacts being identified and subsequently culled; to what extent this would have been kept up if the epidemic had been larger is unclear. Here we analyse the 2007 FMD outbreak, and as the epidemic unfolds we focus on predicting which premises may be infected but currently undetected – we term such premises occult infections. Using prior information determined from the 2001 FMD outbreak in the UK 15 , we use recently developed Bayesian methodology designed for making quantitative riskpredictions in real-time as epidemics progress 10;17;18 . This methodology therefore addresses two major epidemiological concerns: it predicts the uncertain scale of the current epidemic; and it rapidly identifies high-risk premises which can be targetted for further epidemiological investigation or control. The model treats each premises as an individual which can be Susceptible, Infected, Notified (Reported), or Removed. We adopt a similar model to Keeling et al. 13 which assumes heterogeneity in infectivity and susceptibility according to the number and type of species present on each premises, as well as using a spatial kernel to allow the probability of infection to vary over distance. However, in contrast to Keeling’s model, we prefer to make direct inference on a parametric distance function, rather than to use an empirical kernel derived from contact tracing data obtained in the 2001 outbreak (see Methods). Our analysis of the 2007 FMD outbreak began once it became apparent that the disease was concentrating around the Surrey town of Egham. Throughout the epidemic, the MCMC algorithm was run daily to give updated predictions. Figure 1(a) shows the number of infected individuals at each stage in the epidemic, as well as the median predicted number of undetected infections. For selected timepoints, Figure 2 then gives the probabilities that supposedly susceptible farms are in fact infected. This gives an estimate of the current extent of the epidemic given the uncertainties in parameter estimates and the routes of transmission. Figure 2 shows that at each stage of the epidemic, the greatest occult probabilities were associated with premises close to the known IPs, and were those with large numbers of cattle or sheep – in agreement with qualitative understanding. Taken together with Figure 2 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism 1(a), this figure also demonstrates how the algorithm learns about the epidemic as data is gathered from the field. The first map (13th September) is drawn based on only 4 data points. The dataset here contains very little information on spatial transmission since only two farms are closer than 10km, and results in a very diffuse prediction which is heavily influenced by the priors (cf the fast-moving FMD 2001 outbreak). As the epidemic progresses and the number of datapoints increase so does the amount of statistical information, leading to a more precise estimate (see Posteriors in Supplementary Information). This is shown most strikingly by the difference between 13th September and 17th September where just the addition of one data point drastically reduces the median number of predicted undetected infections, and correspondingly reduces the extent of the distribution of high probability premises. Moreover, knowing in hindsight the time-frame of the epidemic we see how the spatial distribution of high-risk farms localises towards the end, reflecting the fact that the epidemic was being controlled effectively. In disease control terms, it is necessary to have an idea on the extent of the resources needed to cope with the outbreak. To answer this question, Figure 1(b) shows the predicted number of new infections in a period of 7 days from the observation time. Consistent with the priors and large amount of uncertainty, this prediction is high early in the epidemic with wide 95% credibility intervals ranging from 0 to 1196 new cases. However, this is soon refined as the epidemic progresses to give the small value consistent with the final outcome of the epidemic. We postulate that, taken together, these results give an overview of the extent of the epidemic, the short-term risk posed by the presence of undetected infections, and the resource required for control measures. From this ability to predict occult infections, we can consider whether the Baysian occult probabilities provide a better guide for targeted control than other measures. Table 1 gives the occult ranking of the last four Infected Premises for dates in September before their detection. For the Baysian analysis this ranking simply sorts the undetected farms in order of highest probability, and this is compared to ranking farms by their proximity to known Infected Premises. This table reflects the same patterns that were observed in Figure 2; early predictions (based on just 4 IPs) by Baysian are highly diffuse, but once the fifth infected premise is identified Baysian analysis outperforms simple spatial measures of risk. However, the practical use of the Baysian occult ranking requires some careful consideration in that many more factors should also influence effective surveillance, such as the centrality of occults in known contact networks. Such model based assessment will, of course, never be a replacement for the detailed contact-tracing performed by veterinarians when identifying Dangerous Contacts, but may help to direct additional resources. The “epidemiological triangle” is an important concept in studying the spread of infectious diseases and states that the characteristics of an outbreak depend on the host, pathogen, and environment in which they co-exist 16 . Changes over time in one or more of the three vertices are therefore likely to alter the dynamics of outbreaks of the same disease recurring in the population. This is demonstrated in the differences between FMD outbreaks in 1967 and 2001 where large differences in farming practices accounted for very different patterns of transmission (Defra FMD information http://www.defra.gov.uk/footandmouth), and 3 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism also in the recent 2007 outbreak which occurred in a sparsely populated area of the country. This shows that by basing predictions of epidemic spread simply on past information, it is impossible to quantify how relevant they are to the current outbreak. On the other hand, early in the epidemic, there is inherently very little data from the current epidemic on which to base a prediction. A Bayesian analysis provides a framework for learning about a current disease outbreak. At the beginning of an epidemic, the prediction process begins with prior information based on our past experience and expert opinion and then updates this by incorporating data obtained from the field during the epidemic under study. Using this methodology therefore provides a very natural way to make as accurate a prediction as possible, whilst quantifying the amount of uncertainty we have about the quantities on which the predictions are based. We have shown, therefore, that a Bayesian approach to real-time inference on disease epidemics is feasible in the agricultural context. This provides a framework for monitoring disease-control efforts, and provides information to adapt policy in the event that the outbreak does not behaving as expected based on past experience. Since this work demonstrates its capability in probabilistically identifying occult cases, it is anticipated that such techniques will form the basis of statistical contact tracing to provide a targetted surveillance strategy even in the face of limited contact-tracing resource. Acknowledgements We would like to thank the following individuals for their assistance with this work: Dr Mike Tildesley, Dr Theodore Kypraios. We also thank Defra for the provision of data and funding for this research. Methods The methodology used in this analysis is based on recently developed Bayesian techniques 10 . The model treats each premises as an individual which can be Susceptible, Infected, Notified, or Removed. We define a Notification as the moment that, according to current FMD control policy, a premises is placed under restrictions, and a Removal as the time when the subsequent herd or flock cull is completed. Thus we allow for Infected and Notified premises to be infective, the latter albeit at a potentially different level due to the upregulation of biosecurity demanded by policy. In contrast to 2001, a national movement ban was imposed in 2007 swiftly after the first case was detected. For this reason we adopt a similar model to Keeling et al. 13 which assumes heterogeneity in infectivity and susceptibility according to the species present on each premises, as well as using a spatial function to allow the probability of infection to vary over distance. We thus parameterise the disease transmission rate between infective (i) and susceptible (j) premises as: βij = (β1 nci ψ + nsi ψ ) · (β2 ncj ψ + nsj ψ ) · β3 β52 ρ2ij + β52 i ∈ I, j ∈ S 4 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism βij? = (β1 nci ψ + nsi ψ ) · (β2 ncj ψ + nsj ψ ) · β4 β52 ρ2ij + β52 i ∈ N, j ∈ S (1) where nc and ns represent the number of cattle and sheep respectively on premises i and j , and ρij the Euclidean distance between them. β1 is then interpreted as the relative infectivity of cattle versus sheep, β2 as the relative susceptibility of cattle versus sheep, β3 and β4 as the rate of spatial transmission for Infected and Notified premises respectively, with β5 governing its rate of decay with increasing distance. We allow for a latent period in which an individual is infected but not yet infectious by multiplying βij by a time-dependent infectivity function (see Supplementary Information). Since we make inference using Bayesian methodology, we require prior distributions for each of the parameters in the model. For this, we turn to previous studies as our source of prior information. Kypraios 15 provides a Bayesian analysis of the UK Foot-and-Mouth outbreak in 2001 using a similar model from which we take priors for β1 ,β2 , and ψ. A combination of the posterior distance kernel provided in Kypraios 15 and the empirical kernel provided by Savill et al. 20 , which are remarkably consistent, inform our choice of β3 ,β4 , and β5 . For each parameter, we use a Gamma-distribution with mean and variance chosen to match our prior information (see Posterior plots in Supplementary Information). Finally, since the infection times are not observed, we use a m odified Gumbel distribution to model the time between Infection and Notification: −bx −1) FD (d) = e−a(e with parameters a and b fixed to give a mean Infection - Notification time of 7.5 days 15 . The posterior distributions are then evaluated for each observational timepoint using the Adaptive Reversible-Jump Markov chain Monte Carlo algorithm described in the Supplementary Information. References [1] R. M. Anderson and R. M. May. Infectious diseases of humans:Dynamics and Control. Oxford University Press, New York, 1991. [2] F. M. Cowan, R. French, and A. M. Johnson. The role and effectiveness of partner notification in STD control: a review. Genitourinary Medicine, 72:247–252, 1996. [3] C. Donnelly, A. Ghani, G. Leung, H. AJ, C. Fraser, S. Riley, L. Abu-Raddad, L.-M. Ho, T.-Q. Thach, P. Chau, K.-P. Chan, T.-H. Lam, L.-Y. Tse, T. Tsang, S.-H. Liu, J. Kong, E. Lau, N. Ferguson, and R. Anderson. Epidemiological determinants of spread of causal agent of severe acute respiratory syndrome in Hong Kong. The Lancet, 361:1761–1766, 2003. [4] K. Eames and M. Keeling. Contact tracing and disease control. Proc R Soc Lond B, 270:2565–2571, 2003. 5 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism [5] N. Ferguson, C. Donnelly, and R. Anderson. Transmission intensity and impact of control policies on the foot and mouth epidemic in Great Britain. Nature, 413:542–548, 2001. [6] N. M. Ferguson, C. A. Donnelly, and R. M. Anderson. The Foot-and-Mouth Epidemic in Great Britain: Pattern of Spread and Impact of Interventions. Science, 292(5519): 1155–1161, 2001. ISSN 0036-8075. [7] N. M. Ferguson, D. A. T. Cummings, S. Cauchemez, C. Fraser, S. Riley, A. Meeyai, S. Iamsirithaworn, and D. S. Burke. Strategies for containing an emerging influenza pandemic in southeast asia. Nature, 437(7056):209–214, 2005. [8] D. Haydon, R. Kao, and R. Kitching. The UK foot-and-mouth disease outbreak - the aftermath. Nat Rev Microbiol, 2:675–681, August 2004. [9] S. Howard and C. Donnelly. The importance of immediate destruction in epidemics of foot and mouth disease. Res Vet Sci, 69:189–196, 2000. [10] C. Jewell, T. Kypraios, G. Roberts, and R. Christley. A novel approach to real-time risk-prediction for emerging infectious diseases: a case study in Avian Influenza H5N1. Prev. Vet. Med., Submitted 2007. [11] R. Kao. The impact of local heterogeneity on alternative control strategies for foot-andmouth disease. Proc R Soc Lond B, 270:2557–2564, 2003. [12] D. Kault. Modelling aids reduction strategies. Int J Epidemiol, 24(1):188–197, 1995. [13] M. J. Keeling, M. E. J. Woolhouse, D. J. Shaw, L. Matthews, M. Chase-Topping, D. T. Haydon, S. J. Cornell, J. Kappey, J. Wilesmith, and B. T. Grenfell. Dynamics of the 2001 uk foot and mouth epidemic: Stochastic dispersal in a heterogeneous landscape. Science, 294(5543):813–818, 2001. ISSN 0036-8075. [14] I. Kiss, D. Green, and R. Kao. Disease contact tracing in random and clustered networks. Proc Royal Soc B, 272:1407, 2005. [15] T. Kypraios. Efficient Bayesian Inference for Partially Observed Stochastic Epidemics and A New class of Semi−Parametric Time Series Models. PhD thesis, Department of Mathematics and Statistics, Lancaster University, Lancaster, 2007. [16] D. Morens, G. Folkers, and A. Fauci. The challenge of emerging and re-emerging infectious diseases. Nature, 430:242, 2004. [17] P. J. Neal and G. O. Roberts. Statistical inference and model selection for the 1861 Hagelloch measles epidemic. Biostatistics, 5(2):249–261, 2004. [18] P. D. O’Neill and G. O. Roberts. Bayesian inference for partially observed stochastic epidemics. J. Roy. Statist. Soc. Ser. A, 162:121–129, 1999. 6 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism [19] S. Riley and N. M. Ferguson. From the Cover: Smallpox transmission and control: Spatial dynamics in Great Britain. Proceedings of the National Academy of Sciences, 103(33):12637–12642, 2006. [20] N. J. Savill, D. J. Shaw, R. Deardon, M. J. Tildesley, M. J. Keeling, M. E. Woolhouse, S. P. Brooks, and B. T. Grenfell. Topographic determinants of foot and mouth disease transmission in the UK 2001 epidemic. BMC Vet Res, 2:3, 2006. [21] The Royal Society. Inquiry into infectious diseases in livestock. Technical report, The Stationary Office, London, 2002. [22] M. Woolhouse and A. Donaldson. Managing foot-and-mouth. Nature, 410:515–516, 2001. 7 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism 50 40 30 20 10 0 Number of individuals Known IPs Median undetected IPs IP4 IP5 Sep 14 IP6 IP7 IP8 Sep 24 Oct 04 Date in 2007 50 100 Median 95% credibility interval 0 New cases in (Date,7+Date] 150 (a) The epidemic time line. Solid line shows the number of detected premises. Dashed line gives the predicted median number of undetected infections. Sep 14 Sep 24 Oct 04 Date in 2007 (b) Predicted numbers of new cases within a 7 day time period after the observation time. Figure 1: Epidemic time line, occult and new cases predictions. 8 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism Occult prob. 0.005 - 0.010 0.011 - 0.050 0.051 - 0.100 0.101 - 0.350 13th Sept 17th Sept 0.351 - 1.000 Known IP Susceptibles 21st Sept 24th Sept 30th Sept 5th Oct Figure 2: Probability of infected-but-undetected farms during Foot-and-Mouth 2007 outbreak IP IP5 IP6 IP7 IP8 Method ba sp ba sp ba sp ba sp 13th Sept 17 (0.42) 11 50 (0.17) 14 35 (0.23) 6 34 (0.23) 24 17th Sept 21st Sept 24th Sept 12 (0.11) 30 11 (0.11) 14 13 (0.11) 42 13 (0.08) 10 1 (0.34) 2 1 (0.25) 10 Table 1: Occult risk ranking calculated from Baysian Analysis (ba) occult probabilities (in brackets), and by spatial proximity to currently infected individuals (sp) 9 CRiSM Paper No. 08-16, www.warwick.ac.uk/go/crism