Document 12464935
advertisement

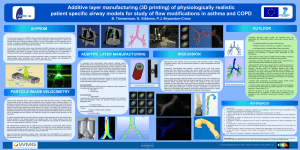
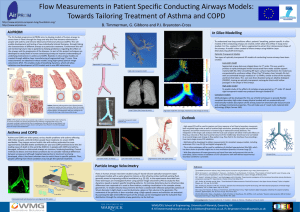
16th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, 09-12 July, 2012 Flow Measurements in Patient Specific Conducting Airways Models B. Timmerman1,*, G. Gibbons1, P.J. Bryanston-Cross2 1: WMG, University of Warwick, Coventry, UK 2: OEL, School of Engineering, University of Warwick, Coventry, UK * correspondent author: B.H.Timmermanl@warwick.ac.uk Abstract The paper presents the development of techniques to study flows in human conducting airways in order to improve understanding of underlying mechanisms in asthma and COPD. These include high-speed particle image velocimetry (PIV) as well as tomo-PIV measurements in geometrically realistic transparent airway models obtained through additive layer manufacturing (ALM) of segmented lung CT scans. This enables study of breathing dynamics, which will allow validation and development of CFD models and in vivo MRI velocimetry. 1. Introduction Asthma and COPD (chronic obstructive pulmonary disease) are wide-spread, serious health problems with asthma affecting 300 million people, while 80 million people have moderate–to– severe COPD worldwide. They impose serious health risks with asthma estimated to cause approximately 239,000 deaths worldwide per year and COPD predicted to be the 3rd leading cause of death in the world by 2030 (AirPROM, 2012). In people with COPD and asthma damaged, inflamed or obstructed airways are common, hindering breathing. Current methods to detect and treat these conditions do not consider individual differences between airways and although targeted approaches to treatment are being developed, often it has been unknown how to match these to specific patients. Thus, people suffering from these conditions may not get the optimal treatment. The EU-funded programme AirPROM aims to develop models of the airways to assess how air flows through the lungs and why this flow becomes obstructed in people with asthma and COPD. This will enable development and testing of new individually tailored therapies, through linking the characteristics of different airways to a particular treatment. Furthermore this will aid monitoring future risks to patients by helping predictions regarding the effect on the airways and the progression of the diseases. As part of this project, techniques are developed to study flows in human conducting airways to improve understanding of underlying mechanisms in asthma and COPD. For this, realistic patientspecific anatomical models of the conducting airways are created through additive layer manufacturing (ALM) of segmented lung CT scans, which allow the airflow in lungs to be studied to understand how lung-conditions affect the patients’ breathing. The paper discusses the preliminary results in the development of high-speed and tomographic particle image velocimetry (PIV) to investigate breathing dynamics and flow characteristics through high order (up to 7th) ALM airway models. 2. PIV in lungs Understanding flows in human airways is vital for combating respiratory complications. Issues include aerosolised drug delivery, high frequency ventilation and pulmonary disease diagnosis and treatment (Freitas, 2008). The work presented here is focused on flow modifications seen in asthma -1- 16th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, 09-12 July, 2012 and COPD. Patients suffering asthma have inflamed airways, making them swollen and very sensitive. When the airways react, mucus production increases and the muscles around airways tighten, narrowing them and thus causing less air to flow into the lungs. COPD typically involves two separate lung conditions: chronic bronchitis and emphysema. In chronic bronchitis, the airways (bronchi) become inflamed, congested with mucus, and narrowed, resulting in obstructed air flow. In emphysema, the walls of the air sacs (alveoli) are destroyed, leading to fewer but larger alveoli, making them less efficient in transferring oxygen from the lungs to the bloodstream. Flows in human airways have been studied using silicone models based on typical airways geometries (Adler and Brücker, 2007) derived from data from e.g. Horsfield et al (1971) and Weibel (1963), as well as using silicone optically transparent ALM models based on patient CTdata, generally aimed at improving artificial ventilation (e.g. Vermeulen et al., 2010; Soodt et al., 2011; S. Große et al, 2008). Typically a water-glycerine mixture is used as the working fluid, allowing refractive index matching of fluid and model to minimise refraction effects in resulting images. Generally planar 2C PIV measurements are obtained in different planes and combined to find the three-dimensional flow distribution. The flow in the trachea and upper bronchi has been found to be highly three-dimensional and asymmetric with counter-rotating vortices in the bronchi (e.g. Große et al., 2007). There is no consensus on the influence of different inflow conditions on the flow in the subsequent bifurcations., e.g. to what extent the upstream flow conditions have an impact on the flow field in sub-branches as a function of the local Reynolds number. Ball et al (2006) showed strong vortex shedding in numerical simulation of the flow from the laryncheal region with flow impact up to 8D. Van Ertbruggen (2005) found highly three-dimensional flow in numerical simulations, showing the importance of non-fully developed flows in the branches due to their relatively short lengths. Thus physically relevant studies require realistic models of the lung geometry, including effects from the laryncheal region (e.g. Lizal et al., 2012). Studies to date have shown a quantitative evaluation of volumetric flow will require time-resolved three-dimensional measurements. In the experiments described here these techniques are investigated further using particle image velocimetry (PIV) to enable study the flow dynamics in two types of optically transparent ALM models of conducting human airways. 3. Patient-specific anatomical models In the measurements presented two types of anatomical model have been used, which are both optically transparent: a low-order model made by casting an optically clear elastomer around a CTbased, ALM produced core, which is subsequently removed, and a high-order CT-based model produced through standard ALM techniques (Fig. 1). Both are based on CT's obtained in vivo. The elastomer used in the first model (Clear Flex® 50 water clear urethane rubber, Smooth-On Inc) possesses a level of elasticity similar to that of the cartilage in the trachea and left and right bronchial tubes (Young's modulus ~2.47MPa vs. averages ranging from 2.5-7.7MPa for trachea (Lambert et al., 1991)), thus allowing flow study at near-realistic compliance. The second model provides a full airway geometry up to 7th order, enabling study of the effects of the various branches on total and local flow dynamics. -2- 16th th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, Portugal 09-12 July, 2012 Figure 1: Transparent ALM models of conducting human airways. Left: 7th generation model, Right: 2nd order model obtained by dissolving an ALM core. 4. Experiments For preliminary measurements, the flow was generated using a peristaltic pump rig providing a controlled input flow rate. Distortions istortions due to refractive index differences were minimised by using rapeseed oil was as flow medium, enabling visualisation in the complex airway geometries by matching refractive index of the models (~1.49) to that of the flow (~1.47 (Wesolowski and Erecinska, 1998)). ). To enable velocity measurements the flow was seeded with reflective polyamide particles of 50 µm diameter. A light sheet was generated using a 200mW green laser diode (SD(SD 301) and used to illuminate a 2D plane or thin volume in the geometr geometry. y. The movement of the particles was recorded from which velocities were calculated (DaVis, LaVision). The anatomical ALM phantoms used were mounted on a traversing system allowing fully automated accurate scanning of the flow region of interest througho throughout ut the airway models (Fig. 2). Thus, by effectively scanning the light sheet different parts of the airways can be investigated and the turbulent flow distribution through the complete airway geometry can be built up. Figure 2: Measurement system. Le Left: ft: Overview showing traversing system enabling accurate movement of the lung model in x, y and zz-direction direction on the left. Right: Illumination system and flow tank with 7th order model. Note: in this picture the tanks is not filled causing distortions and opaqueness in lung model,, which are removed when oil is added added. To investigate the dynamics of the flow, time time-resolved resolved measurements were obtained using highhigh speed PIV (Olympus i-Speed3). Speed3). Furthermore, to allow volumetric measurements a novel hybrid -3- 16th th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, Portugal 09-12 July, 2012 tomo-PIV system (Elsinga, 2007) was designed based on the use of three to five synchronised (high-speed/PIV) speed/PIV) cameras (Fig. 3) for simultaneous capture of PIV data from a thick light sheet. Depending on the configuration used this enables (quasi) time time-resolved resolved 3C volumetric v measurements allowing study of different aspects of flow behaviour including flow development inside the airways (Fig. 4). Figure 3: Tomo-PIV PIV measurement systems. Left: 33-camera camera arrangement. Right: Hybrid tomo/hightomo/high speed system. on in a cross plane exiting one of the lower Figure 5 shows a short sequence of the flow distribution bronchi. A clear unsteady behaviour can be seen. Figure 4:: Velocity distribution in trachea and upper bronchi of 7th order model. Left: instantaneous, Right: mean velocity distribution. Note the turbulence for flow directed towards right bronchus. -4- 16th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, 09-12 July, 2012 Figure 5 Instantaneous velocity maps of flow exiting lower bronchus. Note image of ALM model superimposed as background. Figure 6 shows three simultaneous views of the flow in the 7th order model. Using this data a 3D3C velocity can be extracted over a thin volume. Figure 6 Simultaneous images of seeded flow captured using three cameras from left, centre and right viewing direction. -5- 16th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, 09-12 July, 2012 5. Conclusions A measurement system capable of high-speed and tomographic PIV has been designed for measurements in optically transparent airway models of realistic configuration. Preliminary results have been presented, with further data being processed. To investigate flow behaviour at realistic breathing conditions a flow rig is being designed to produce an oscillating flow representing inspiration and expiration. The mass flow rate and oscillation frequency of the model flows need to be corrected for properties of the flow medium by matching the Reynolds number, Re, and Wormersley number, α, in order to mimic realistic velocities and breathing rates respectively. The Reynolds number is matched based on the maximum velocity in the trachea, Umax : ܷ௫ ∙ ܦ ܴ݁ = ν where D is the diameter of the trachea and ν is the kinematic viscosity. The Wormersley number, α, is given by: ߱ ܦ ߙ= ට 2 ν where ω is the angular frequency. Typically, this implies a lower breathing frequency for liquid media compared to air (0.25Hz), as well as a higher flow velocity for liquid versus air (Umax ~0.8m/s). The controlled pneumatic flow rig will be used to generate flows simulating the patient specific breathing patterns. To obtain volumetric 3D-3C data, in addition to tomo-PIV and digital holography (Claus et al, 2011a,b), the multi-plane stochastic estimation technique of Hunter et al (2012) will be further developed to extract the time-resolved volumetric flow distribution. Further work includes potential derivation of pressure distribution from this PIV-based velocity data (van Oudheusden et al, 2007), which is of particular interest to understand behaviour of airway surfaces. The visualization techniques will be further developed for use in novel multi-material ALM models (Objet Connex 260), including endoscopic PIV and X-ray PIV (Dubsky et al, 2011; Lee et al, 2009). Methodologies will be developed for the use of ALM techniques to provide flexible compliant boundary high order airway physical models with a mechanically-realistic description of the airway, based on bronchial tube tissue mechanical properties. High-speed measurements will be used to capture real time response of air flow to boundary movement, both on global large-scale as well as localised high-resolution, providing insight into ventilation dynamics and airflow mechanisms in human lungs in obstructive airway diseases. The integration of the large scale analysis with the local scale analysis will allow small scale effects on flow (e.g. reduced air flow due to partial closure of the middle lobar bronchus) to be correlated to an overall large-scale change in flow pattern (e.g. flow field in the trachea), thus providing a true macro-large airway CFD validation. The anatomical ALM prototypes will subsequently be used for validation of hyperpolarised 3He MRI, for in vivo imaging of flow in human lungs. Ultrafast imaging of 3He gas has been shown to provide insight into ventilation dynamics in human lungs (Wild et al, 2003). Acknowledgements The project is funded through the EU 7th Framework Programme AirPROM "Airway Disease -6- 16th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, 09-12 July, 2012 PRedicting Outcomes through Patient Specific Computational Modelling", contract no 270194, http://www.airprom.eu. The authors gratefully acknowledge Olympus KeyMed Ltd. for use of a high-speed camera and to P. Hackett for invaluable technical assistance. Further thanks to G. Canham, B. Falconer, C. Maske, A. Patronis, T. Bradbury, S. Final and D. Carter. References • • • • • • • • • • • • • • • • • • Adler K, Brücker C (2007) Dynamic flow in a realistic model of the upper human lung airways, Exp. Fluids 43: 411-423 AirPROM consortium website (2012), http://www.airprom.european-lung-foundation.org/ or http://www.airprom.eu Ball CG, Uddin M, Pollard A (2006) Lattice Bolzmann simulation of flow in the human upper airway. Proceedings of the 5th conference on turbulence, heat and mass transfer, 305– 308 Claus D, Fritzsche M, Iliescu D, Timmerman B, Bryanston-Cross P (2011a), " Highresolution digital holography utilized by the subpixel sampling method", Applied Optics, Vol. 50, Issue 24, pp. 4711-4719 Claus D, Iliescu D, Timmerman BH, Bryanston-Cross PJ (2011b), "Resolution improvement in digital holography: comparison between synthetic aperture method and spatial averaging method", Proc. SPIE 8001, 80010Z; doi:10.1117/12.893430 Dubsky S, Hooper SB, Siu KKW, Fouras A(2011), “Dynamic four-dimensional X-ray PIV of the lung”, 9th International Symposium on Particle Image Velocimetry –PIV’11, Kobe, Japan, July 21-23. Elsinga G, Scarano F, Wieneke B, van Oudheusden B (2007) Tomographic particle image velocimetry. Exp. Fluids, 41:933–947 van Ertbruggen C, Hirsch C, Paiva M (2005), Anatomically based three-dimensional model of airways to simulate flow and particle transport using computational fluid dynamics, J Appl Physiol 98: 970–980 Freitas, RK, Schröder W (2008), Numerical investigation of the three-dimensional flow in a human lung model. Journal of Biomechanics, 41(11): p. 2446-2457. Große S, Schröder W, Klaas M (2007) “Time resolved analysis of steady and oscillating flow in the upper human airways”, Exp. Fluids 42: 955-970 Große S, Schröder W, Klaas M (2008) “Time-Resolved PIV Measurements of Vortical Structures in the Upper Human Airways”, Topics in Applied Physics,112: 35-53 Horsfield K, Dart G, Olsen DE, Filley GF, Cumming G (1971) Models of the human bronchial tree. J. Appl. Physiol. 31(2):207-217 Hunter D, Timmerman BH, Bryanston-Cross PJ (2012), Prediction of a Flow Volume using Multi-Plane Volumetric Stochastic Estimation, in preparation Lambert RK, Baile EM, Moreno R, Bert J, Paré PD (1991), A method for estimating the Young’s modulus of complete tracheal cartilage rings. J. Appl. Physiol. 70(30): 1152-1159 Lee SJ, Kim GB, Yim DH, Jung SY (2009), Development of a compact x-ray particle image velocimetry for measuring opaque flows, Review of Scientific Instruments, 80, 033706 Lizal F, Elcner J, Hopke PK, Jedelsky J, Jicha M (2012) Development of a realistic human airway model, Proc IMechE Part H: J Engineering in Medicine 226(3):197-207 van Oudheusden BW, Scarano F, Roosenboom EWM, Casimiri EWF, Souverein LJ (2007) Evaluation of integral forces and pressure fields from planar velocimetry data for incompressible and compressible flows, Exp Fluids 43:153–162 Soodt T, Schröder F, Klaas M, van Overbrüggen T, Schröder W (2011), Experimental investigation of the transitional bronchial velocity distribution using stereo scanning PIV, -7- 16th Int Symp on Applications of Laser Techniques to Fluid Mechanics Lisbon, Portugal, 09-12 July, 2012 • • • • Experiments in Fluids, Online First 4May. Vermeulen M, van Holsbeke C, Claessens T, de Backer J, van Ransbeeck P, Verdonck P (2010), Flow Analysis in Patient Specific Lower Airways using PIV, 15th Int Symp on Applications of Laser Techniques to Fluid Mechanics, Lisbon, Portugal, 05-08 Jul. Wesolowski, M, ErecinskaJ (1998), Thermal analysis in quality assessment of rapeseed oils. Thermochimica Acta, 1998. 323(1-2): p. 137-143. Wild JM, Paley MNJ, Kasuboski L, Swift A, Fichele1 S, Woodhouse N, Griffiths PD, van Beek EJR (2003), Dynamic radial projection MRI of inhaled hyperpolarized 3He gas, Magn Reson Med 49:991–997 Weibel ER (1963) Morphometry of the human lung. Springer, Berlin -8-