A prostate MRI atlas of biochemical failures following cancer treatment
advertisement

A prostate MRI atlas of biochemical failures following cancer
treatment
Mirabela Rusua , John Kurhanewiczb , Ashutosh Tewaric , Anant Madabhushia,*
a Case
Western Reserve University, Cleveland, Ohio; b University of California San Francisco,
San Francisco, California; c Icahn School of Medicine at Mount Sinai Hospital, New York, New
York; * Corresponding author
ABSTRACT
Radical prostatectomy (RP) and radiation therapy (RT) are the most common treatment options for prostate
cancer (PCa). Despite advancements in radiation delivery and surgical procedures, RP and RT can result in
failure rates as high as 40% and >25%, respectively. Treatment failure is characterized by biochemical recurrence
(BcR), which is defined in terms of prostate specific antigen (PSA) concentrations and its variation following
treatment. PSA is expected to decrease following treatment, thereby its presence in even small concentrations
(e.g 0.2 ng/ml for surgery or 2 ng/ml over the nadir PSA for radiation therapy) is indicative of treatment
failure. Early identification of treatment failure may enable the use of more aggressive or neo-adjuvant therapies.
Moreover, predicting failure prior to treatment may spare the patient from a procedure that is unlikely to be
successful. Our goal is to identify differences on pre-treatment MRI between patients who have BcR and those
who remain disease-free at 5 years post-treatment. Specifically, we focus on (1) identifying statistically significant
differences in MRI intensities, (2) establishing morphological differences in prostatic anatomic structures, and
(3) comparing these differences with the natural variability of prostatic structures. In order to attain these
objectives, we use an anatomically constrained registration framework to construct BcR and non-BcR statistical
atlases based on the pre-treatment magnetic resonance images (MRI) of the prostate. The patients included in
the atlas either underwent RP or RT and were followed up for at least 5 years. The BcR atlas was constructed
from a combined population of 12 pre-RT 1.5 Tesla (T) MRI and 33 pre-RP 3T MRI from patients with BcR
within 5 years of treatment. Similarly, the non-BcR atlas was built based on a combined cohort of 20 pre-RT
1.5T MRI and 41 pre-RP 3T MRI from patients who remain disease-free 5 years post treatment. We chose the
atlas framework as it enables the mapping of MR images from all subjects into the same canonical space, while
constructing both an imaging and a morphological statistical atlas. Such co-registration allowed us to perform
voxel-by-voxel comparisons of MRI intensities and capsule and central gland morphology to identify statistically
significant differences between the BcR and non-BcR patient populations. To assess whether the morphological
differences are valid, we performed an additional experiment where we constructed sub-population atlases by
randomly sampling RT patients to construct the BcR and non-BcR atlases. Following these experiments we
observed that: (1) statistically significant MRI intensity differences exist between BcR and non-BcR patients,
specifically on the border of the central gland; (2) statistically significant morphological differences are visible
in the prostate and central gland, specifically in the proximity of the apex, and (3) the differences between the
BcR and non-BcR cohorts in terms of shape appeared to be consistent across these sub-population atlases as
observed in our RT atlases.
Keywords: gland morphology, biochemical recurrence, MRI atlas, prostate cancer
1. DESCRIPTION OF PURPOSE
Radical prostatectomy (RP) and radiation therapy (RT) are the most common treatment strategies for clinically
localized prostate cancer (PCa), accounting for roughly 110 000 annual interventions in US alone.1, 2 Despite
the good prognosis associated with treating low grade PCa, disease recurrence following either treatment occurs
frequently. At 5 years post treatment, biochemical recurrence (BcR) occurs in up to 40% of patients3 undergoing
RP and more than 25% of patients4 treated via RT. BcR is generally defined in terms of PSA concentrations
and its variations following treatment, although the absolute thresholds vary based on the treatment type. A
PSA concentration > 0.2 ng/ml3 indicates BcR following RP, while concentrations > 2 ng/ml5 from the lowest
value post-RT, also referred to as the PSA nadir, indicate BcR following RT.
Medical Imaging 2014: Computer-Aided Diagnosis, edited by Stephen Aylward, Lubomir M. Hadjiiski,
Proc. of SPIE Vol. 9035, 903513 · © 2014 SPIE · CCC code: 1605-7422/14/$18 · doi: 10.1117/12.2043775
Proc. of SPIE Vol. 9035 903513-1
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
T (2) Voxel by Voxel Comparison
(la) BcR Atlas Construction
(3) 3D Morphologic Differences
1
1
(lb) Non BcR Atlas Construction
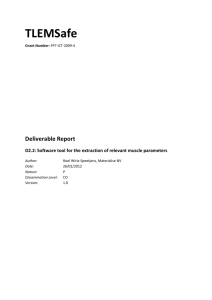
Figure 1: MRI atlases are built for the BcR (1a) and non-BcR population (1b); (2) Statistical tests are applied to
assess differences between corresponding voxels (pink and red) within the two atlases; (3) morphologic prostate
shape comparison between and within the two populations are also performed.
The early prediction of recurrence is essential, as BcR is prognostic of disease progression, metastasis, and
disease-related mortality.6 Predicting which patients might experience BcR would enable the early administration
of more aggressive or neo-adjuvant therapies and may potentially improve patient outcome. Moreover, if obtained
prior to treatment, such predictions might facilitate choosing alternative therapies to spare the patient from a
procedure that is likely to fail.
Pre-treatment nomograms7–9 that employ statistical models based on patient specific risk criteria have been
introduced to predict BcR post-treatment. For example, the Kattan nomograms7–9 predict 5 year cancer-free
likelihood following RP7 or RT8, 9 by incorporating pre-treatment PSA, biopsy Gleason score and clinical stage.
Additionally, Kattan nomograms predicting BcR post RT also include radiation dose. Other approaches used
MRI alone10 or in combination with magnetic resonance spectroscopy (MRS)11 or molecular profiles12 to improve
the prediction of BcR. These studies employ qualitative, reader-derived MRI measurements of disease, such as
the number of sextants involving the index lesion, tumor volume, extracapsular spread or seminal vesicle invasion.
However, to our knowledge, no study to date has investigated characteristics on MRI that are correlated with
BcR following RT or RP.
In this study, we focus on identifying imaging and morphological differences associated with BcR that are
visible on pre-treatment MRI between patients with and without BcR. The use of treatment planning MRI
allows the study of differences independent of the treatment, while facilitating the early intervention to adjust
treatment.
In this work, we specifically test the hypothesis that differences exist in the anatomy and tissue appearance
of the prostate which may provide clues regarding BcR risk at 5 years after the treatment. Tiwari et. al.13, 14
has shown that MRI can distinguish indolent from aggressive cancers, the latter of which are also more likely to
cause BcR. In this work, we test whether BcR can be predicted by pre-treatment MRI intensity or gland shape.
In order to identify these differences, the atlas construction framework previously introduced by us in15 will
be utilized to build BcR and non-BcR atlases. Statistical atlases have been previously utilized to characterize
the anatomical differences of brain16 and the prostate15 structures. We choose to use the atlas construction
framework as it allows us to generate a canonical representation of a population by mapping the MRI from all
subjects into the same space. The anatomically constrained registration ensures proper alignment of anatomic
Proc. of SPIE Vol. 9035 903513-2
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
structures by combining anatomic surface and intensity similarity terms in the optimization process. Such
anatomic constraints are required to account for the large variability in appearance and shape of the prostate
and its anatomical substructures, the central gland and peripheral zone.15 The resulting prostate statistical
atlas is composed of 1) a statistical MRI intensity atlas, 2) a morphological atlas of the prostate, and 3) a
morphological atlas of the central gland.
The prostate atlas, AB , was constructed for the patients who had BcR following either treatment, while
AN B included subjects without BcR at 5 years following treatment. Moreover, treatment-specific atlases were
constructed from the cohorts stratified by treatment strategy. The RP atlas, AB (RP), was constructed from
33 subjects with BcR within 5 years, while 41 patients were included in the non-BcR atlas, AN B (RP). The
RT BcR atlas, AB (RT), incorporated 12 patients, whereas 20 patients were included in the non-BcR atlas,
AN B (RT). The atlas construction procedure allowed us to map both populations into the same canonical space,
enabling voxel-by-voxel comparisons via the Wilcoxon test. To assess whether the morphologic and intensity
differences ascertained between the BcR and non-BcR atlases for RT were significant, we created atlases from
sub-populations within the BcR and non-BcR cohorts and evaluated the differences between these populations.
The objective of this experiment was to determine whether differences observed were real or by random chance
resulting from the natural variability of the prostate.
The rest of this paper is organized as follows. In Section 2, we describe the anatomically constrained registration framework and its application to construct the BcR and non-BcR atlases. Section 3 introduces and discusses
the results of the various comparative experiments performed. Finally, in Section 4 we discuss the implications
of our findings.
2. METHODOLOGY AND EXPERIMENTAL DESIGN
2.1 Preprocessing
Bias field correction via low-pass filtering approach described in17 was applied to the MRI prior to atlas construction. Moreover, a histogram alignment was performed to correct the inter-patient MRI intensity drift, allowing
for per voxel MRI intensity comparisons.
2.2 Atlas construction framework
The construction of the BcR atlas AB and non-BcR atlas AN B was accomplished using the anatomically constrained registration framework, previously described in.15 A summary of the atlas construction framework is
provided below, and the notations used in this work are outlined in Table 1. The framework uses an iterative
registration approach to simultaneously create the MRI intensity and shape atlases while increasing the degrees
of freedom of the optimized transformation from a simple affine to an elastic deformation.
In the first step, the outline of the prostate and central gland are obtained through interactive segmentation
using either 3D Slicer18 or MeVisLab.19 Next, a first atlas is created from all datasets once the MRI is centered
and isotropically scaled to ensure a constant prostate volume, defined here as the median prostatic volume in
the input cohort. The atlas is created via median filtering of the MRI intensity and the prostate and central
gland outline of all subjects. The framework generates 1) an MRI intensity atlas, denoted by AM , 2) a statistical
shape atlas of the prostate, Apr and 3) a statistical shape atlas of the central gland Acg . This first atlas served
as registration template for the second step, affine registration. Following the affine registrations, the atlas is
updated and used as a reference template for the deformable registration step. The final atlas is obtained via
median filtering of the elastically aligned MRI.
A combination of MRI intensity similarity and regional overlap defined relative to the prostate and central
gland shapes are used to drive the registration of every subject Xi , ∀i ∈ {1, . . . , N } to the template atlas A:
X
ψ(A, Xiσ ) = I2 (AM , XiM ) +
wσ · ψ σ (Aσ , Xiσ ),
(1)
σ∈{cg,pr}
where Xiσ , ∀i ∈ {1, . . . , N }, σ ∈ {M, cg, pr} represents the MRI intensity, the prostate (pr) and the central gland
(cg) shapes of subject Xi . A is the template atlas composed of Aσ , σ ∈ {M, cg, pr}. The mutual information,20
Proc. of SPIE Vol. 9035 903513-3
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
Symbol
A
AM
Aσ
Xiσ = (C, fi (c)),
∀i ∈ {1, . . . , N }
XiM
Xiσ
I2
ψσ
wσ
N, M
Aσθ
Description
Prostate atlas, composed of Aσ , σ ∈ {M, pr, cg}
MRI intensity atlas
Statistical shape atlas, σ ∈ {pr, cg}
Subject i scene with ∀c ∈ C, fi (c) represents data at location c, σ ∈ {M, pr, cg}
MRI intensity scene of subject Xi
Outline scene of the region σ ∈ {pr, cg} for subject Xi
Mutual information
Surface similarity metric for σ ∈ {pr, cg}
Weight associated with the surface σ ∈ {pr, cg}
Subject count in the BcR and non-BcR cohort
Atlas σ ∈ {M, pr, cg} constructed from the cohort θ ∈
{B, N B};
AσB→N B
Difference between BcR and Non-BcR for σ ∈ {M, pr, cg}
AB
BcR atlas of the combined RT + RP patient cohort
AN B
Non-BcR atlas of the combined RT + RP patient cohort
AB (RP)
BcR atlas of the RP patient cohort
AN B (RP)
Non-BcR atlas of RP patient cohort
AB (RT)
BcR atlas of the RT patient cohort
AN B (RT)
Non-BcR atlas of RT patient cohort
AB,k , k ∈ {1, ..., 4}
Atlas obtained from a subset of BcR subjects
AN B,l , l ∈ {1, ..., 4} Atlas constructed from a subset of non-BcR subjects
Table 1: Symbols and notations employed in this paper.
I2 , is used to assess the similarity of MRI intensities, while ψ σ (Aσ , Xiσ ) quantifies the alignment of the anatomic
structures σ ∈ {cg, pr}, and wσ is an empirically determined weight.15 In this work, we choose the normalized
squared error to evaluate the regional alignment.
2.3 BcR and non-BcR atlas construction
The MRI, prostate shape and central gland shape atlases are constructed for the BcR and the non-BcR cohort,
resulting in Aσθ σ ∈ {M, pr, cg}, θ ∈ {B, N B}. Moreover, due to the patient specific criteria for RT or RP, we
not only constructed the combined RP+RT atlases, denoted by AB and AN B respectively, but we also generated
the individual atlases AB (RP) and AN B (RP) for the RP cohorts, and AB (RT) and AN B (RT) for the RT cohorts
(see Table 1).
2.4 Experiments
We performed 3 experiments. In experiment E1 (see Section 2.4.1), we investigate the MRI differences that
can be identified between patients with or without BcR within 5 years following treatment. Experiment E2
(see Section 2.4.2) was performed to assess the statistically significant differences between the morphology of
the prostate and central gland of the BcR vs non-BcR patients. Finally, experiment E3 (see Section 2.4.3) is
designed to assess morphological differences within the BcR and non-BcR cohorts independently.
2.4.1 Experiment E1: Voxel-by-voxel comparison of MRI intensities
The atlas construction enables the mapping of all patients within a common canonical space, which allows us
to test whether differences exist between MRI intensities of BcR and non-BcR patients on a per-voxel basis.
The statistical significance of MRI differences is assessed using the non-parametric Wilcoxon test. Here, we test
whether the mean MRI intensity is statistically significantly different between the N subjects used to generate
AB and the M subjects considered when creating AN B . The Wilcoxon test was performed for each voxel c ∈ C,
yielding a statistical significance map. We chose a lower significance level α = 0.01 to account for the large
Proc. of SPIE Vol. 9035 903513-4
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
number of comparisons done in this study. Rejection of the null hypothesis indicates a statistically significant
difference in the mean MRI intensities.
Moreover, we also computed the normalized mean difference between the BcR and non-BcR cohorts, and
uses it to establish qualitative correlations with the statistical significance map, defined ∀c ∈ C by:
D(c) =
1
N
PN
i=1
fB,i (c) −
PM
1
M
j=1
1
M
PM
j=1
fN B,j (c)
fN B,j (c)
(2)
where fB,i (c) and fN B,i (c) represent the MRI intensities at location c for subject Xi from the BcR cohort and Xj
from the non-BcR cohort, respectively. Large D(c) are expected to correspond to voxels that show statistically
significant differences between the BcR and non-BcR patients, while values close to zero indicate similar MRI
intensities when comparing BcR and non-BcR subjects.
2.4.2 Experiment E2: Variability in gland morphology
The atlas construction framework allowed us to generate the statistical shape of the prostate and central gland
based on the cohorts considered. Statistical shapes of the prostate and central gland were computed for both AB
and AN B , and distances between these gland shapes were evaluated to estimate the inter-population variability in
gland morphology. The non-parametric Wilcoxon test is used to investigate whether the levelset representations
of the prostate surfaces and central glands are significantly different between AB and AN B using α = 0.01.
The levelset representation provides a continuous version of the region segmentations corresponding to different
anatomic areas. We chose such a representation to limit boundary effects. Two tests were performed for each
voxel c, comparing the N levelset representations of the prostate surface and central gland in AB to the M
levelset representations in AN B . As in experiment E1, rejection of the null hypothesis indicates a statistically
significant difference in the structural morphology of the gland and anatomical regions.
2.4.3 Experiment E3: Prostate morphological variability assessed within cohort
In order to assess whether the morphological differences observed in experiment E2 are meaningful, we also
constructed four sub-atlases AB,k , k ∈ {1, ..., 4}, from a randomly selected subset of patients of the RT BcR set.
Similarly, four sub-atlases AN B,l , l ∈ {1, ..., 4}, were constructed from the set of patients that did not have BcR.
We estimate the intra-population variability in gland shape based on the four sub-atlases, and we estimate the
variability as the average distances to the statistical shape of the prostate gland within each of the sub-population
atlases.
2.5 Data Description
Table 2 summarizes the characteristics of the 106 patients included in this study. The 75 subjects included in
the RP group had 1) biopsy confirmed cancer, 2) surgery to remove the prostate and 3) 3 Tesla(T) T2 weighted
MRI acquired prior to the surgery using an endo-rectal coil. BcR was defined by 0.2 ng/ml PSA concentration.
The median follow up period for the BcR patients was 10 months (range: 0-46 months), while the non-BcR
patients had a median follow up period of 68 months (range 65-78).
The subjects included in the RT group had biopsy confirmed cancer, underwent either external beam RT or
brachytherapy, and had 1.5T T2 weighted endo-rectal MRI acquired prior to treatment. The 12 BcR subjects
were followed up for at least 20 months, with a median period of 59 months, and BcR was assessed at a median
period of 47 months post treatment using either of the following two criteria: 1) increased PSA concentration of
2ng/ml or more above nadir PSA;5 or 2) medical evidence that PCa recurred as indicated by medical notes or
follow-up intervention, e.g. brachytherapy. The 20 non-BcR subjects either did not have BcR during the entire
follow-up period (median 87 months, with minimum 60 months of follow up) or had BcR after 5 years or more
following RT (median 89 months with range of 73-118 months).
Proc. of SPIE Vol. 9035 903513-5
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
Cohort MRI
Grade ¶
Follow up \
Failure time \
Size
Strength
AB (RP)
RP
BcR
33
3.0T
1,25,8,0
46.5 (18-73)
10 (0-46)
AN B (RP)
RP
Non-BcR
41
3.0T
3,34,4,0
68 (65-78)
AB (RT)
RT
BcR
12
1.5T
8,3,1,0
59 (20-90)
47 (19-68)
AN B (RT)
RT
Non-BcR
20
1.5T
13,6,0,1
87 (60-123)
89 (73-118)§
AB
RT+RP
BcR
45
AN B
RT+RP
Non-BcR
61
Table 2: Data description; ¶shows Gleason grade stratified as low (≤ 6), intermediate (7), high (≥ 8) and not
available; \ time provided in months showing median and range in parenthesis; §Included in the non-BcR cohort
was a subgroup of patients who had BcR failure later than 5 years (between 73-118 months)
Atlas
Cohort
Status
(a)
(b)
(c)
(e)
(f)
(g)
(d)
£'0
e'o
Z'0l
s'o
0
z'o
a0j
(j)
0
(i)
(h)
(l)
(k)
M
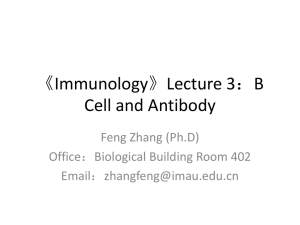
Figure 2: Per voxel differences are visible between the BcR and non-BcR patients. (a) AM
B ; (b) AN B ; (c) normalM
M
M
M
ized difference D (AB→N B ) (eq 2); (d) p-value for AB→N B ; (e) AB (RP); (f) AN B (RP); (g) D(AM
B→N B (RP));
M
M
M
M
(h) p-value for AM
B→N B (RP); (i) AB (RT); (j) AN B (RT); (k) D(AB→N B (RT)); (l) p-value for AB→N B (RT). Legend: (c,g,k) red, blue - large difference, green-close to 0 difference; (d,h,l) purple p-value ≤ 0.01, green p-value
> 0.01.
3. EXPERIMENTAL RESULTS AND DISCUSSION
3.1 Experiment E1: MRI intensity atlas
In experiment E1, we constructed the BcR atlases of the combined cohort AB (Figure 2a) and individual cohorts
AB (RP) (Figure 2e) and AB (RT) (Figure 2i), as well as the non-BcR atlases of the combined cohort AN B
(Figure 2b) and individual cohorts AN B (RP) (Figure 2f) and AN B (RT) (Figure 2j). By constructing the atlases,
the patients were projected in the same canonical space, which allowed us to make per-voxel comparisons of the
same anatomic regions. Sharp hypo-intense boundaries of the prostate and the central gland can be observed
indicating a good alignment of the anatomic regions (Figure 2a,b,e,f). The smaller number of patients included
in the RT BcR cohort caused less defined boundaries within the MRI intensity atlas AM
B (RT) (Figure 2i).
Proc. of SPIE Vol. 9035 903513-6
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
Metalmage'
.]14102
1714102
1.6
1.6
1.2
-0.8
-0.8
0.
0. 4
a4
(a)
(b)
(e)
(c)
(f)
0
(d)
(g)
(h)
cg
Figure 3: Morphological distances viewed from different perspectives (a-b) Apr
B→N B ; (c-d) AB→N B ; (e-f)
pr
cg
AB→N B (RP); (g-h) AB→N B (RP). Legend: red colors are used to depict large distances, while close to zero
distances are shown in green.
0.75
035
0.5
0.5
0.25
0.25
0.75
0,5
-0.25
5.56a
5.56a11
1
5,6e -11
(a)
(b)
(c)
(d)
075
075
05
05
05
025
0.25
11075
0.25
1.7e -13
1.7e -13
2e-13
(e)
(f)
(g)
(h)
Figure 4: Significance of morphological distances viewed from different perspectives (a-b) Apr
B→N B ; (c-d)
pr
cg
Acg
;
(e-f)
A
(RP);
(g-h)
A
(RP).
Legend:
purple
indicates
p-value
≤
0.01
while
green is used
B→N B
B→N B
B→N B
for p-value > 0.01.
3.2 Experiment E1: MRI intensity differences
Figure 2 also shows the normalized difference D (eq. 2) and the p-value to assess the statistical significance
M
of these differences. The normalized mean differences revealed up to 30% differences between AM
B and AN B .
Furthermore, some of these differences were found to be statistically significant (column 4 in Figure 2). Such statistically significant differences were visible across the entire gland but were consistently found at the boundary
of the central gland and peripheral zone, in the proximity of the apex. The RP atlases showed more structured
statistically significant differences in MRI intensity particularly at the boundary of the central gland and peripheral zone. Such pronounced differences may be attributed to BcR in those patients that underwent radical
prostatecomy. Although MRI differences appear larger when comparing the AB (RT) and AN B (RT) (Figure 2k),
these differences are not typically statistically significant, in part due to the small RT population size.
Proc. of SPIE Vol. 9035 903513-7
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
(a)
o
)
(D
(1)
lul
(o)
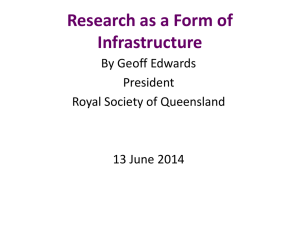
Figure 5: Prostate morphology in the RT cohort viewed from different angles. Colors represent (a-d) the statispr
r
tical significance of AP
B→N B (RT) or (e-p) surface distances: (e-h) AB→N B (RT); (i-l) BcR variability obtained via
the subatlas AB,k (RT); (m-p) non-BcR intra-class variability assessed via AN B,l (RT), k, l = 1, 2, . . . , 4. Legend:
(a-d) purple indicates p-value ≤ 0.01 while green is used for p-value > 0.01. (e-p) Red colors are used to depict
large distances, while close to zero distances are shown in green.
3.3 Experiment E2: Morphological differences in the prostate
Figure 3 shows the morphological distances for the combined RP+RT cohort (Figures 3a-d) and the RP cohort
alone (Figures 3e-h). These morphological distances are measured by the Euclidean distance of the mean regional
shapes, σ ∈ {pr, cg}, obtained via the atlas construction framework. Figure 3 shows the apex of the prostate
(Figures 3a,e), the prostate side (Figures 3b,f), the apex of the central gland (Figures 3c,g), and the side of
the central gland (Figures 3d,h). Large differences are visible close to the apex for both the prostate and the
central gland in both the RP+RT or RP cohorts. Moreover, statistically significant differences are apparent
cg
pr
cg
when comparing Apr
B→N B , AB→N B , AB→N B (RP), and AB→N B (RP) (Figure 4). The statistically significantly
different regions are visible in the proximity of the apex both the prostate and central gland.
Figure 5 shows the statistically significant differences (Figures 5a-d) of prostate morphological distances
Apr
B→N B (RT) (Figure 5e-h) for the patients who had RT. Distances of up to 2.67 mm can be observed between
Proc. of SPIE Vol. 9035 903513-8
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
the prostate shape, indicating the existence of morphologic gland differences between the two populations.
Statistically significant differences are visible on the rectal wall (Figure 5a) and on the prostate side (Figure 5c),
while other regions do not show significant differences, attributable to the smaller population size.
3.4 Experiment E3: Morphological differences in the prostate
The intra-class variability in prostate shape was assessed for the BcR cohort via AB,k (Figures 5i-l) and non-BcR
cohort via AN B,l (Figures 5m-p), k, l ∈ {1, 2, . . . , 4}. Figures 5i-p indicate that the intra-class variability in gland
morphology is larger in AN B (RT) compared to AB (RT). It is important to note that the inter-class morphologic
differences (Figure 5e-h) surpass the intra-population variability, which barely reaches 2mm.
4. CONCLUDING REMARKS
In this work, we investigate imaging and morphological differences that may be associated with biochemical
recurrence (BcR) following prostate cancer treatment by either radical prostatectomy or radiotherapy. In order
to investigate these differences, we constructed prostate atlases for patients with and without BcR 5 years post
treatment. Through the atlas construction, the pre-treatment MRI of the subjects were projected into the same
canonical space, which allowed us to perform per voxel comparisons within the spatially normalized images. Such
comparisons were done relative to the MRI intensity and the prostate and central gland morphology.
Statistically significant MRI differences were observed between the BcR and non-BcR patients that had
radical prostatectomy. These differences were visible at the border of the central gland and peripheral zone close
to the apex. Similarly, statistically significant differences were observed near the apex in the atlas constructed
from the combined radical prostatectomy and radiotherapy patients. On the other hand, the small sample size in
the radiotherapy cohort prevented us from observing statistical significant differences in MRI intensity between
the patients that had BcR and those that did not have BcR following radiation therapy. Moreover, morphologic
differences in the prostate and the central gland shapes were localized towards the apex and were found to
be statistically significant between the BcR and non-BcR populations, regardless of treatment. Furthermore,
morphological differences were observed on the rectal wall of the prostate in the radiation therapy patients who
had BcR versus those who did not have it 5 years post treatment. In the radiation therapy cohort, the differences
between the BcR and non-BcR subjects were larger than the variability within each individual cohort (BcR or
non-BcR) which suggests that the observed differences are meaningful. These results suggests that we may be
able to predict early BcR even before treatment which may allow for early intervention via more aggressive or
neo-adjuvant treatments.
The lack of precise mapping of cancer on MRI prevented us from quantifying the influence of cancer size
and shape in assessing gland morphology variability. In future studies, we will attempt to carefully map the
extent of tumor from the ex vivo prostatectomy specimens onto the pre-operative MRI for those patients in
the radical prostatectomy cohort. Such mapping could allow us to build more detailed atlases for predicting
biochemical recurrence following surgery. Moreover, we envision extending the current atlas to incorporate
information pertaining to type of treatment, radiation dose, cancer grade or extra-capsular spread to predict risk
of biochemical failure.
5. ACKNOWLEDGMENTS
Research reported in this publication was supported by the Department of Defense Postdoctoral Prostate Cancer
Award W81XWH-12-PCRP-PTA, National Cancer Institute of the National Institutes of Health under award
numbers R01CA136535-01, R01CA140772-01, and R21CA167811-01; the National Institute of Diabetes and
Digestive and Kidney Diseases under award number R01DK098503-02, the DOD Prostate Cancer Synergistic
Idea Development Award (PC120857); the QED award from the University City Science Center and Rutgers
University, the Ohio Third Frontier Technology development Grant. The content is solely the responsibility of
the authors and does not necessarily represent the official views of the National Institutes of Health.”
Proc. of SPIE Vol. 9035 903513-9
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms
REFERENCES
[1] Djavan, B., Moul, J. W., Zlotta, A., Remzi, M., and Ravery, V., “PSA progression following radical prostatectomy and radiation therapy: new standards in the new Millennium.,” Eur. Urol. 43, 12–27 (Jan 2003).
[2] Penson, D. F., Chan, J. M., and , U. D. i. A. P., “Prostate cancer.,” J. Urol. 177, 2020–2029 (Jun 2007).
[3] Trock, B. J., Han, M., Freedland, S. J., Humphreys, E. B., DeWeese, T. L., Partin, A. W., and Walsh, P. C.,
“Prostate cancer-specific survival following salvage radiotherapy vs observation in men with biochemical
recurrence after radical prostatectomy.,” J.A.M.A 299, 2760–2769 (Jun 2008).
[4] Rukstalis, D. B., “Treatment Options After Failure of Radiation Therapy - A Review,” Rev. Urol. 4, S12
(2002).
[5] Roach III, M., Hanks, G., Thames Jr, H., Schellhammer, P., Shipley, W. U., Sokol, G. H., and Sandler, H.,
“Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically
localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference,” Int. J.
Radiat. Oncol. Biol. Phys. 65(4), 965–974 (2006).
[6] Uchio, E. M., Aslan, M., Wells, C. K., Calderone, J., and Concato, J., “Impact of biochemical recurrence
in prostate cancer among US veterans.,” Arch Intern Med 170, 1390–1395 (Aug 2010).
[7] Kattan, M. W., Eastham, J. A., Stapleton, A. M., Wheeler, T. M., and Scardino, P. T., “A preoperative
nomogram for disease recurrence following radical prostatectomy for prostate cancer.,” J. Natl. Cancer
Inst. 90, 766–771 (May 1998).
[8] Kattan, M. W., Zelefsky, M. J., Kupelian, P. A., Scardino, P. T., Fuks, Z., and Leibel, S. A., “Pretreatment
nomogram for predicting the outcome of three-dimensional conformal radiotherapy in prostate cancer,” J.
Clin. Oncol. 18(19), 3352–3359 (2000).
[9] D’Amico, A. V., Whittington, R., Malkowicz, S. B., Fondurulia, J., Chen, M.-H., Kaplan, I., Beard, C. J.,
Tomaszewski, J. E., Renshaw, A. A., Wein, A., and Coleman, C. N., “Pretreatment nomogram for prostatespecific antigen recurrence after radical prostatectomy or external-beam radiation therapy for clinically
localized prostate cancer,” J. Clin. Oncol. 17(1), 168 (1999).
[10] Fuchsjäger, M. H., Pucar, D., Zelefsky, M. J., Zhang, Z., Mo, Q., Ben-Porat, L. S., Shukla-Dave, A., Wang,
L., Reuter, V. E., and Hricak, H., “Predicting Post-External Beam Radiation Therapy PSA Relapse of
Prostate Cancer Using Pretreatment MRI,” Int. J. Radiat. Oncol. Biol. Phys. 78(3), 743–750 (2010).
[11] Westphalen, A. C., Koff, W. J., Coakley, F. V., Muglia, V. F., Neuhaus, J. M., Marcus, R. T., Kurhanewicz,
J., and Smith-Bindman, R., “Prostate cancer: prediction of biochemical failure after external-beam radiation
therapy - Kattan nomogram and endorectal MR imaging estimation of tumor volume,” Radiology 261(2),
477–486 (2011).
[12] Shukla-Dave, A., Hricak, H., Ishill, N., Moskowitz, C. S., Drobnjak, M., Reuter, V. E., Zakian, K. L.,
Scardino, P. T., and Cordon-Cardo, C., “Prediction of prostate cancer recurrence using magnetic resonance
imaging and molecular profiles.,” Clin. Cancer Res. 15, 3842–3849 (Jun 2009).
[13] Tiwari, P., Kurhanewicz, J., Rosen, M., and Madabhushi, A., “Semi supervised multi kernel (SeSMiK)
graph embedding: identifying aggressive prostate cancer via magnetic resonance imaging and spectroscopy,”
MICCAI 13(Pt 3), 666–73 (2010).
[14] Tiwari, P., Viswanath, S., Kurhanewicz, J., and Madabhushi, A., “Weighted combination of multiparametric mr imaging markers for evaluating radiation therapy related changes in the prostate,” MICCAI
, 80–91 (2011).
[15] Rusu, M., Bloch, B. N., Jaffe, C. C., Rofsky, N., Genega, E., Lenkinski, R., and Madabhushi, A., “Statistical
3D Prostate Imaging Atlas Construction via Anatomically Constrained Registration,” in [SPIE Medical
Imaging], 8669 (2013).
[16] Evans, A., Collins, D., Mills, S., Brown, E., Kelly, R., and Peters, T., “3d statistical neuroanatomical
models from 305 MRI volumes,” in [Nuclear Science Symposium and Medical Imaging Conference], 1813–
1817 (1993).
[17] Cohen, M. S., DuBois, R. M., and Zeineh, M. M., “Rapid and effective correction of RF inhomogeneity for
high field magnetic resonance imaging,” Human Brain Mapping 10(4), 204–211 (2000).
[18] Pieper, S., Halle, M., and Kikinis, R., “3D Slicer,” IEEE Int. Sym. on Biomed. Imaging , 632–635 (04 2004).
[19] http://www.mevislab.de/, “Mevislab.”
[20] Pluim, J. P., Maintz, J. A., and Viergever, M. A., “Mutual-information-based registration of medical images:
a survey,” IEEE Trans. Pattern Anal. Mach. Intell. 22(8), 986–1004 (2003).
Proc. of SPIE Vol. 9035 903513-10
Downloaded From: http://proceedings.spiedigitallibrary.org/ on 09/30/2014 Terms of Use: http://spiedl.org/terms