Daily weight monitoring as a method of weight gain prevention Article 589446

589446
HPQ Katterman et al.
Article
Daily weight monitoring as a method of weight gain prevention in healthy weight and overweight young adult women
Journal of Health Psychology
1 –11
© The Author(s) 2015
Reprints and permissions: sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/1359105315589446 hpq.sagepub.com
Shawn N Katterman
1,2
, Meghan L Butryn
2
,
Megan M Hood
1
and Michael R Lowe
2
Abstract
Experimental research is needed to examine whether weight monitoring impacts weight and whether it has unintended harmful effects. This study randomly assigned 49 first-year university women (body mass index: 20–30 kg/m 2 ) to daily weight monitoring or a control condition and measured weight, mood, body dissatisfaction, and unhealthy weight control behaviors at baseline and 8 weeks, and weight at 20-week follow-up. No harmful effects of daily weighing were detected; acceptability and adherence were high.
Weight monitoring did not impact weight; both groups showed little weight gain. Results suggest that weight monitoring has minimal harmful effects and may be useful for preventing weight gain.
Keywords obesity, prevention, weight control, weight monitoring
Introduction
Effective methods of weight gain prevention are needed to significantly reduce obesity and improve public health. Several studies suggest that individuals who are successful with weight loss (Qi and Dennis, 2000) and weight loss maintenance (Wing and Phelan, 2005; Wing et al.,
2006) frequently monitor their weight. Studies have shown an association between interventions that include daily weighing and weight gain prevention (e.g. Gokee et al., 2010) and experimental data have provided evidence that daily weighing alone may prevent weight gain among healthy weight young adult women (Levitsky et al., 2006).
Although accumulating research suggests that weight monitoring does not have harmful effects among adults aiming to maintain weight loss (e.g.
Wing et al., 2007), less is known about the effects of weight monitoring in young adults attempting to prevent weight gain. Epidemiological studies have found women aged 18–29 years to be at highest risk of obesity onset (Mokdad et al., 1999), and recent trends in weight suggest that individuals who are already heavier are more likely to continue to gain weight (Ogden et al., 2007). In a
1 Rush University Medical Center, USA
2 Drexel University, USA
Corresponding author:
Michael R Lowe, Department of Psychology, Drexel
University, Stratton Hall, 3141 Chestnut St. Philadelphia,
PA 19104, USA.
Email: ml42@drexel.edu
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
2 Journal of Health Psychology large study of adults in the United States, overweight women with a body mass index (BMI, kg/m 2 ) greater than or equal to 25 were more likely to experience a major weight gain (i.e. more than 10 kg over 10 years) than any other subgroup
(Williamson et al., 1990). Given indications that young adults, particularly women who are already overweight, are at risk of weight gain, further understanding of the impact of weight monitoring in this population is needed to inform obesity prevention efforts.
Extant research of weight monitoring in young adults has been mixed both in terms of whether it results in intended effects (i.e. prevention of weight gain) and whether it has harmful effects. While daily weighing was found to prevent a weight gain of approximately 6 pounds over 12 weeks in healthy weight women in their first year of university (Levitsky et al., 2006), others found that weight monitoring alone did not impact weight and only had an effect on weight among first-year university men and women of all weight ranges when students also received a six session online psychoeducation program about maintaining a healthy lifestyle
(Gow et al., 2010). Both of these findings provide preliminary evidence that weight monitoring may be useful, but await replication with other samples and weight ranges to determine whether this prevention effect is generalizable.
Harmful effects of weighing and weight monitoring have also been noted as a potential concern, and research in this area is mixed
(Gow et al., 2010; Neumark-Sztainer et al.,
2006; Ogden and Evans, 1996; Quick et al.,
2012). One potential concern is the impact on body dissatisfaction and resulting disordered eating behaviors (e.g. purging, fasting) that could occur when individuals are asked to bring their attention to their weight on a daily basis, particularly if it falls outside of the “normal” range. Observational studies have shown associations between frequency of self-weighing and unhealthy behaviors like binge eating (e.g.
Neumark-Sztainer et al., 2006), but these studies are unable to determine temporal and causal relationships or rule out the possibility of a third variable (e.g. preoccupation with weight or drive for thinness) that might cause both an increase in self-weighing and binge eating.
Gow et al. (2010) used random assignment to weight monitoring and found that it did not have a significant effect on body dissatisfaction, disordered eating, or binge eating, but that assignment to weekly weighing in the absence of psychoeducation was associated with a small but significant increase in cigarette smoking.
Increases in state measures of depression and anxiety, and a decrease in self-esteem have also been observed with random assignment to daily weight monitoring (Ogden and Whyman,
1997), although the same study failed to find significant effects of daily weighing on disordered eating attitudes and behaviors or body dissatisfaction. While concerns have been raised about the possibility that frequent weighing might increase body dissatisfaction, meal skipping, purging, or laxative use (Dionne and
Yeudall, 2005), these variables have not been examined experimentally in a nonobese population looking to prevent weight gain.
Given the importance of identifying simple and effective weight control strategies for young adult women and the mixed findings regarding the efficacy and potentially harmful effects of weight monitoring, this study aimed to replicate previous findings that daily weight monitoring has a weight gain prevention effect in healthy weight women and to examine the impact of the intervention in young adult women in the overweight range. Specifically, the study aimed to examine the impact of daily weight monitoring in terms of both intended (e.g. weight gain prevention) and unintended (e.g. increased negative mood, body dissatisfaction, or unhealthy weight control behaviors like meal skipping or smoking) effects. Analyses were conducted in the overall sample, and exploratory analyses examined the impact of weight monitoring within the healthy and overweight sub-samples.
Method
Participants
First-year female students were recruited with fliers and mass emails at Drexel University and Cornell University. All advertisements
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
Katterman et al. 3 emphasized that participants may learn ways to prevent weight gain without mention of monetary compensation in an attempt to capture participants motivated by a desire to prevent weight gain rather than earn money.
Inclusion criteria were female gender, in their first year of college and between the ages of 18 and 25 years, living on campus, and a selfreported BMI of 20 to 29.9 kg/m includes both healthy weight and overweight and is sufficiently above the weight criteria threshold for anorexia nervosa. Exclusion criteria included self-reported current or past eating disorder diagnosis. The study received approval from the appropriate ethical review boards.
Procedures
2 , a value that
Interested participants completed a brief phone screen and if eligible were invited to come to the lab at their respective campuses for their initial assessment where they completed informed consent and anthropometric measurements. All baseline assessments were conducted in the months of
September and October 2009. Participants were then asked to complete two tasks: (1) complete baseline questionnaires online (see below for details) and (2) email the research team each morning over the next 7 days to demonstrate that they can make the daily commitment to weighing if assigned to that condition. If participants emailed on at least 5 of 7 days and completed the questionnaires, they were assigned to a condition using a matched pair design (i.e. as participants were ready to be randomized, they were paired with a participant from their school who had a
BMI that was most similar to theirs, differences ranged from 0 to 2.8 units difference, and then assigned via a 1:1 random numbers table to the daily weighing or control group). Participants assigned to daily weight monitoring were given a digital scale and asked to weigh themselves each morning when they woke up and record it on a secure website. Once seven weights were entered, they began to receive information about their weight trajectory over the past 7 days including a line graph plotting their actual weights, the overall regression line, and an average weight change per day value (e.g. “−0.8 lbs/day”).
Participants were instructed to focus on the change in weight over time instead of on specific daily weights. If participants failed to record or email their weight for three consecutive days, they were sent an email reminder. To replicate previous procedures (Levitsky et al., 2006), intervention group participants were not given any other specific instructions other than those above and to try to avoid weight gain. Participants assigned to the control group were not given any specific instructions except to return for future assessments.
After 8 weeks, all participants completed the same self-report measures online and came back to the lab for their post-intervention assessment. During the post-intervention assessment, their height and weight were measured and all participants completed a semistructured interview designed to assess their use of any unhealthy weight control behaviors, their subjective experience of daily weighing (intervention group only), and to assess frequency of daily weighing among the control group (see section “Measures” for details). Between the post-intervention assessment and the follow-up assessment, which occurred approximately
20 weeks after their baseline assessment (i.e. a 12-week follow-up), participants were encouraged to continue monitoring their weight, but were not prompted via email if they failed to do so. Payment for completing the post- intervention and follow-up assessments was
US$5 and US$15, respectively.
Measures
Anthropometrics.
Height was measured without shoes using a stadiometer or mounted tape measure. Weight was measured in light clothing using a digital scale.
Body satisfaction.
Body satisfaction was measured with the Berscheid Body Satisfaction Test
(BBS; Berscheid et al., 1973), a measure that asks participants to indicate their level of satisfaction with nine aspects of one’s body
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
4 Journal of Health Psychology
(e.g. weight, thighs, stomach). The scale has shown adequate internal consistency and predictive validity (e.g. Stice and Bearman, 2001; Stice et al., 2002). In this study, the scale demonstrated excellent internal consistency (
Mood.
The Profile of Mood States (POMS;
McNair et al., 1971) was used to measure mood. To replicate previous research, the anxiety and depression subscales were used to examine whether increases in these variables were found in response to daily weighing, as noted in a previous experimental study (Ogden and Whyman, 1997). Both of these scales have been found to have adequate internal consistency and validity (Bourgeois et al., 2010). Calculation of Cronbach’s alpha for the depression subscale revealed good reliability ( α = 0.82); however, the coefficient for the anxiety subscale was 0.51, which is lower than the generally recommended cutoff of 0.60 or 0.70 for acceptability.
α = 0.90).
without eating, skipping meals, laxative use, and smoking. Participants were given a Likert scale to refer to and were asked to report a number from 0 ( Never ) to 8 ( Constantly ). If participants reported engaging in these behaviors, the interviewer would ask follow-up questions to assess whether these behaviors were engaged in for the purpose of weight control or for another reason (e.g. going for long periods of time without eating because they happened to be in a place where food was not available) and only those behaviors done with the purpose of controlling weight were recorded. Responses to these items were examined individually (i.e. means for each item were examined by condition) and also added together to create an interviewerassessed frequency of unhealthy weight control behaviors index. Additionally, any other behaviors reported in response to the open-ended questions that could be deemed unhealthy (e.g. purging, excessive or driven exercise) were also tracked, if present.
Unhealthy weight control behaviors.
Both selfreport measures and a clinical interview were used to assess a variety of unhealthy weight control behaviors. The Weight Control Behavior Questionnaire (Stice and Presnell, 2004) is a
15-item scale which asks participants to report whether or not they have engaged in 15 weight control behaviors over the past 30 days. Four items made up the Unhealthy Behavior subscale (i.e. skipping breakfast, skipping lunch, skipping dinner, and smoking). This measure demonstrated a reliability estimate of α = 0.60 in the current sample.
Additionally, a semi-structured clinical interview was conducted at the post-intervention assessment to assess the weight control behaviors participants engaged in during the 8-week intervention period. In the interview, participants were first asked an open-ended question where they were asked to list the ways they controlled their weight over the past 8 weeks. Next, they were asked about the frequency with which they engaged in the following unhealthy weight behaviors over the past 8 weeks: going for long periods of time (i.e. six or more waking hours)
Experience of daily weighing.
During the clinical interview, all participants assigned to daily weighing were asked to rate the experience of daily weighing on a scale of 0 to 8 in terms of its helpfulness (i.e. in controlling their weight or affecting other things, like their mood, that might impact their weight), its harmfulness, and whether it made them feel more in control of their weight and/or less in control of their weight. Participants were then asked to elaborate on their responses to clarify why they rated daily weighing in a given way.
Adherence.
Adherence to daily weight monitoring was assessed by extracting weight data from the secure website at the end of the 8-week intervention period and averaging the percentage of days out of 8 weeks that intervention group participants recorded their weight on the site. Notably, there was not a timestamp function on the site, so the exact time the weight data were entered on the site (i.e. the day of measurement or several days/weeks after) is unknown.
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
Katterman et al. 5
Statistical analyses
Independent samples t -tests and chi-square tests were used to test whether there were baseline differences between condition or school (i.e. Drexel
University vs Cornell University) on any of the demographic or outcome variables. Independent samples t -tests were used to examine whether assignment to weight monitoring had a significant effect on change in weight from baseline to post-intervention and 20 weeks and change in the following dependent variables from baseline to post-intervention: body dissatisfaction, mood, and unhealthy weight control behaviors (i.e. via self-report questionnaire). Independent samples t -tests were also used to test for the effect of condition on the frequency of unhealthy weight control behaviors index as assessed by post- intervention semi-structured interview. All analyses were first conducted with the entire sample
( N = 49), and then exploratory analyses were conducted with healthy weight participants ( n = 39) and overweight participants ( n = 10) to identify potential differential effects among subgroups.
Interaction terms were not used due to low power to detect more complex effects and the inequality of sub-sample sizes. Based on power analyses conducted in GPower (Faul et al., 2007), this study had over 90 percent power to detect a large effect size (i.e. d = 0.95) when the entire sample or the healthy weight participants only are analyzed (i.e. d = 0.95 and 1.0, respectively). This level of power would likely be adequate to replicate the effect sizes reported in previous research for the effect of weight monitoring on weight among healthy weight women ( d ≅ 4.00; Levitsky et al., 2006) on mood ( d = 0.76–1.00; Ogden and
Whyman, 1997), but is less likely to detect effect sizes in the small to moderate range. When subsamples were examined (i.e. healthy weight or overweight participants only), power to detect large effects was lower than 80 percent. Given that some of the potentially harmful effects may be smaller, Cohen’s d values were calculated and examined for each analysis to examine whether small to moderate effects were present but not statistically significant. Finally, descriptive analyses (means and standard deviations ( SD s)) were used to report the results from the semi-structured interview assessing participant’s use of unhealthy weight control behaviors and the intervention group’s subjective experience of daily weighing.
Results
Participant flow
Of the 123 women who responded to the initial flyer or email, 20 did not respond to additional attempts to contact them, and 103 completed the phone screen. Of these, 15 were no longer interested after receiving information about the study, and 22 were found ineligible, 16 due to the fact that they had a BMI below 20 kg/m 2 .
Of the 58 who attended their baseline assessment, 50 completed the behavioral run-in requirements and 25 were randomized to the intervention group and 25 to the control group.
Of the 66 participants who were scheduled for a baseline assessment, 50 participants were enrolled in the study and randomized to a condition, 49 completed the post-intervention assessment, and 47 completed the 20-week assessment, representing a 98- and 94-percent completion rate, respectively. Of those who were randomized, 11 had a BMI greater than
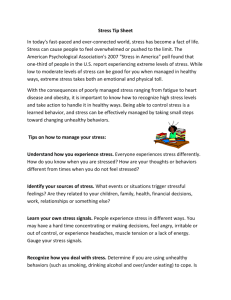
25, and of these, 4 were randomized to the intervention group and 7 were randomized to the control group. For a Consolidated Standards of Reporting Trials (CONSORT; Schulz et al.,
2010) figure documenting participant flow, see
Figure 1.
Compliance and treatment fidelity
Among the intervention group participants, participants entered their weights online on an average of 93 percent of days over the 8-week intervention period ( SD = 10%). Only one control participant reported weighing herself daily over the intervention period but did not record her weight anywhere. Analyses were conducted with and without this participant and results were unchanged, and therefore, all analyses are presented with this participant included.
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
6 Journal of Health Psychology
123 women responded to flyer/email
103 completed phone screen
66 scheduled for inperson assessment
58 attended baseline assessment
20 could not be reached
50 randomized
15 no longer interested after receiving more information
22 ineligible
16 BMI < 20
3 BMI > 30
1 over 25 years old
2 had history of eating disorder
8 did not show
7 did not complete behavioral run-in requirements
1 had a BMI > 30
Post-
Intervention
8 Weeks
Follow Up
20 Weeks
Intervention ( n = 25)
21 BMI 20-25
4 BMI 25-30
25 (100%) weighed
21 BMI 20-25
4 BMI 25-30
24 (96%) weighed
20 BMI 20-25
4 BMI 25-30
Control ( n = 25)
18 BMI 20-25
7 BMI 25-30
24 (96%) weighed
18 BMI 20-25
6 BMI 25-30
23 (92%) weighed
17 BMI 20-25
6 BMI 25-30
Figure 1.
Participant flow.
Body mass index (BMI) categories are based on baseline BMI.
Baseline characteristics Intended effects of the intervention
Participants ranged in age from 18 to 19 years at the time of their baseline assessment
( M = 18.0 years, SD = 0.2 years). A total of
30 participants (58.5%) identified themselves as Caucasian, 9 as Asian American
(17.6%), 6 as African American (11.8%), and
5 (9.8%) as another ethnicity and/or mixed ethnicity. At baseline, participants had a mean BMI of 23.58 kg/m 2 ( SD = 2.49) and a mean weight of 62.12 kg. Independent samples t -tests and chi-square tests revealed no significant baseline differences between conditions or school on any of the demographic or outcome variables.
Across the entire sample, there was no effect of condition on weight change from baseline to
8 weeks, t (48) = −1.24, p = 0.22, or baseline to
20 weeks, t (46) = −0.12, p = 0.91, and effect size was small at 8 weeks ( d = 0.35) and very small at 20 weeks ( d = 0.04), suggesting little to no impact of assignment to weight monitoring on weight across the entire sample. When healthy and overweight participants were examined separately within each group, however, a different pattern emerged. Among healthy weight participants, the effect on weight appeared to be absent or minimal, with both intervention and control groups showing a small and not statistically
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
Katterman et al.
Table 1.
Change in body satisfaction, mood, and unhealthy weight control behaviors from baseline to post-intervention.
Measure All participants
( N = 47)
Change ( SD ) d
Healthy weight
( n = 37)
Change ( SD ) d
Overweight
( n = 10)
Change ( SD ) d
Body satisfaction
Intervention
Control
Depression
Intervention
Control
Anxiety
Intervention
Control
Unhealthy weight control
Intervention
Control
1.28 (4.19)
2.04 (7.42)
0.84 (7.51)
3.20 (11.09)
1.08 (5.48)
1.05 (5.03)
0.13 (1.01)
0.26 (0.81)
−0.13
−0.25
0.01
−0.34
0.38 (3.53)
2.56 (8.44)
1.52 (7.63)
1.31 (7.00)
1.57 (5.78)
0.40 (4.67)
0.05 (1.00)
0.06 (0.75)
−0.36
0.03
0.22
−0.01
4.60 (5.13)
0.67 (3.78)
−2.75 (6.55)
8.25 (18.09)
−1.50 (2.65)
2.67 (5.99)
0.67 (1.15)
0.83 (0.75)
0.88
−0.89
−0.48
−0.17
SD: standard deviation.
When Cohen’s d values are positive, it indicates greater increases in the intervention group compared to the control group.
7 different weight gain over 8 weeks, t (37) = 0.27, p = 0.52, and 20 weeks, t (35) = 0.28, p = 0.62.
When overweight participants were examined
( n = 10), there was a trend-level effect of condition on weight at both post-intervention, t (9) = 0.12, p = 0.09, d = −1.14, and 20-week follow-up, t (9) = 0.24, p = 0.08, d = −1.20, where overweight participants assigned to daily weight monitoring lost 1.94 kg ( SD = 1.80 kg) at
20 weeks, and those assigned to the control condition gained 0.82 kg ( SD = 2.02 kg).
Unintended effects of the intervention
There were no statistically significant effects on mood, body satisfaction, meal skipping, smoking, or other disordered eating behaviors across the entire sample or within groups divided by weight status; however, as noted above, this study is underpowered to detect potential small- to-moderate effect sizes. Table 1 displays means and SD s for changes in these variables as well as between-group effect sizes to explore the possibility that a smaller effect was present that would have been detected in a larger sample. Notably, all mean changes in potentially harmful variables are in the direction of the control group having worsening symptoms, with the exception of body satisfaction among healthy weight participants.
Among healthy weight control participants, there was a small mean increase in body satisfaction
( M = 2.56, SD = 8.44) whereas mean change in intervention group participants was very close to zero ( M = 0.38, SD = 3.53; see Table 1). Among overweight participants, however, the weight monitoring group showed an increase in body satisfaction ( d = 0.88) which also coincided with a decrease in depression ( d = −0.89), and a smaller increase in anxiety compared to controls
( d = −0.48; see Table 1). There was no significant effect of condition on the combined score for unhealthy weight control behaviors as assessed by the post-intervention clinical interview, t (46) = −0.96, p = 0.34. Notably, smoking for the purpose of weight control was only observed at post-intervention in one participant and this participant was in the control condition. Furthermore, responses to open-ended questions in the semistructured clinical interview failed to detect the use of any weight control behaviors (e.g. purging,
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
8 Journal of Health Psychology
( excessive or driven exercise) that would be deemed unhealthy.
Treatment acceptability
Of the participants assigned to daily weighing n = 25), 23 reported that daily weighing was
“helpful” in controlling their weight, and 2 felt
“neutral or indifferent” about its helpfulness.
All 25 participants stated that it was “not harmful.” A total of 21 participants (84%) said daily weighing made them feel more in control of their weight, while 4 (16%) responded that it did not make them feel more in control. Notably, while 18 participants (78%) answered “no” to the question “did daily weighing make you feel less in control of your weight?,” 5 participants
(10%) said “yes” to this question, and each of the five reported that at times, they had a difficult time noticing a consistent pattern between their behaviors and the number on the scale.
Discussion
This study aimed to examine intended (i.e. weight gain prevention) and unintended (e.g. increased body dissatisfaction) effects of daily weight monitoring in nonobese young adult females. To our knowledge, this was the first study to systematically examine weight monitoring as a method of weight gain prevention among overweight women and also the first to assess subjective experiences of daily weighing with a semi-structured interview. Adherence to daily weighing and acceptability ratings were high. Daily weight monitoring in this study did not result in any of the potentially harmful effects observed in some previous research.
Notably, healthy weight participants in this study did not appear to be particularly weightgain prone, and weight monitoring did not show a weight gain prevention effect in the healthy weight or overall sample. Exploratory analyses with a small sub-sample of overweight participants suggested that weight loss may occur among overweight individuals assigned to daily weighing, though future research is needed to test these effects in a larger sample size.
Although preliminary, results suggest that among young adult women without a history of an eating disorder who are trying to prevent weight gain, daily weight monitoring appears to have high acceptability and relatively low risk of harmful effects.
It is important to note first that this study participants did not appear to be particularly prone to weight gain. Overall, this study showed less weight gain than previous studies of firstyear university women (e.g. Levitsky et al.,
2004; Vella-Zarb and Elgar, 2009) so results should be generalized with caution to samples that may be more prone to gain over time.
However, among those who were overweight and attended follow-up assessments ( n = 10), those assigned to daily weighing ( n = 4) lost
1.94 kg ( SD = 1.80) at 20 weeks, and those assigned to the control condition ( n = 6) gained
0.82 kg ( SD = 2.02), suggesting that daily weight monitoring may facilitate weight loss in the overweight subset of this population, who may be prone to weight gain over time.
Results suggest that for some young adult women without a history of an eating disorder, daily weight monitoring does not have significant undesirable effects such as increased body dissatisfaction, negative mood, or unhealthy eating behaviors. This mirrors findings in adults, which have suggested that weight monitoring was not associated with problematic effects on eating or mood and actually predicted decreased likelihood of binge eating (Wing et al., 2007). In fact, there was an indication of a potential positive effect on body satisfaction and mood in the small sample of overweight individuals assigned to weight monitoring compared to controls, which may be related to the weight loss observed in this group. Notably, this study included participants who volunteered to be part of a weight gain prevention study and who are attending college. Taken together with the fact that group sizes were small, more research is needed before results can be applied to the general population. Furthermore, although interventions such as this one may be generally safe to recommend, research studies cannot predict whether such an intervention
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
Katterman et al. 9 might not have harmful effects for a few individuals, which was either not detected or not reported by the affected participant(s). As with any intervention, it is important to follow up with the individual to ensure that they are using weight monitoring as a useful tool and not noticing harmful effects on their mood, attitudes, or behaviors.
This study failed to replicate previous research that found that assignment to weight monitoring increased smoking (Gow et al.,
2010) and negative mood (Ogden and Whyman,
1997). There are few potential explanations for these discrepant findings. First, previous studies used different populations (e.g. men and women of all weight ranges; Gow et al., 2010; women recruited for a study of “seasonal weight fluctuations”; Ogden and Whyman, 1997).
Therefore, the current results may be more indicative of effects on women interested in controlling their weight and preventing future weight gain. Finally, power for this was able to detect moderate to large effects which would be adequate to detect effects found in previous research but may have failed to detect small effects.
This study also utilized a qualitative approach to understanding participant’s experiences with daily weighing by conducting semistructured interviews. By asking open-ended questions, we aimed to examine whether participants had any negative experiences with daily weighing that they might be willing to share in the interview but that might not be detected in self-report measures. Notably, no participants reported that daily weight monitoring was harmful in the open- or close-ended sections of the interview. Five participants
(10%) indicated that, at times, daily weighing made them feel less in control of their weight.
These participants reported having a difficult time noticing a consistent pattern between their behaviors and the number on the scale. This finding points to the importance of ensuring that individuals are able to identify a pattern between eating and exercise behaviors and weight change, to utilize the weight monitoring tool effectively.
Study strengths included a randomized design; physical measurement of weight, qualitative and quantitative assessment of participant experience, and high retention as postintervention and 20-week follow-up. However, the overall sample size was small, particularly the group of overweight participants ( n = 10 attended all follow-up assessments), and limited to college students who appeared to be less prone to weight gain than previously studied samples, so it is possible that these effects are specific to this sample and replication with larger and more diverse samples is needed.
Additionally, given that there was not a timestamp function on the website to assess when participants entered their weights, we are unable to determine whether participants may have filled in weights at a later date. Although this limitation is similar to those inherent to other studies (e.g. those that used the same website, or paper and pencil methods of monitoring as in the two independent studies in Levitsky et al.,
2006), we are unable to determine whether participants actually engaged in the intervention exactly as intended.
Additionally, although this study failed to find a decrease in measures of mood at postintervention, we cannot rule out the possibility that participants may have experienced a decrease in mood over the course of the intervention that was not captured at post-intervention and not reported in the post-intervention clinical interview. Also, a few of the measures had reliability estimates that are considered lower than the standard limits of acceptability
(e.g. anxiety measure, unhealthy weight control behavior measure), so future research should test these hypotheses with other measures of mood and unhealthy weight control behaviors.
Finally, future research could explore the role of expectations about weight maintenance or loss in this population, as these expectations could impact relevant factors such as effort, motivation, and mood during weight control efforts (e.g. De Vet et al., 2013).
In summary, this study found that daily weight monitoring was not sufficient to prevent weight gain overall but also did not find
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
10 Journal of Health Psychology evidence of harmful effects of daily weighing on mood, body dissatisfaction, meal skipping, disordered eating, or smoking. Notably, weight monitoring in overweight young adult women may facilitate weight loss. Because daily weighing has been implicated as a method of weight gain prevention and weight loss maintenance
(Levitsky et al., 2006; Wing and Phelan, 2005), it is important to determine whether this effect is present and to understand the potential mechanism and whether its effects extend beyond
20 weeks. Future research should examine this relationship in larger samples to examine whether daily weighing could be used as part of a readily disseminated treatment package for obesity prevention in this group of women at risk of weight gain and obesity onset.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-forprofit sectors.
References
Berscheid E, Walster E and Bohrnstedt GW (1973)
The happy American body: A survey report.
Psychology Today , November, pp. 119–131.
Bourgeois A, LeUnes A and Meyes M (2010) Fullscale and short-form of the Profile of Mood
States: A factor analytic comparison. Journal of
Sport Behavior 33: 355–376.
De Vet E, Nelissen RMA, Zeelenberg M, et al. (2013)
Ain’t no mountain high enough? Setting high weight loss goals predict effort and short-term weight loss. Journal of Health Psychology 18:
638–647. DOI: 10.1177/1359105312454038.
Dionne MM and Yeudall F (2005) Monitoring of weight in weight loss programs: A doubleedged sword? Journal of Nutrition Education and Behavior 37: 315–318. DOI: 10.1016/
S1499-4046(06)60162-0.
Faul F, Erdrelder E, Lang A, et al. (2007) G*Power 3:
A flexible statistical power analysis program for the social, behavioral, and biomedical sciences.
Behavior Research Methods 39: 175–191.
DOI: 10.3758/BF03193146.
Gokee LJ, Tate DF, Gorin AA, et al. (2010)
Preventing weight gain in young adults: A randomized controlled pilot study. American
Journal of Preventive Medicine 39: 63–68.
DOI: 10.1016/j.amepre.2010.03.011.
Gow RW, Trace SE and Mazzeo SE (2010)
Preventing weight gain in first year college students: An online intervention to prevent the “freshman fifteen.” Eating Behaviors 11:
33–39. DOI: 10.1016/j.eatbeh.2009.08.005.
Levitsky DA, Garay J, Nausbaum M, et al. (2006)
Monitoring weight daily blocks the freshman weight gain: A model for combating the epidemic of obesity. International Journal of Obesity 30: 1003–1010. DOI: 10.1038/ sj.ijo.0803221.
Levitsky DA, Halbmaier CA and Mrdjenovic G
(2004) The freshman weight gain: A model for the study of the epidemic of obesity.
International Journal of Obesity 28: 1435–
1442. DOI: 10.1038/sj.ijo.0802776.
McNair D, Lorr M and Droppleman L (1971) Manual for the Profile of Mood States . San Diego, CA:
Educational and Industrial Testing Service.
Mokdad AH, Serdula MK, Dietz WH, et al. (1999)
The spread of the obesity epidemic in the
United States, 1991-1998. Journal of the
American Medical Association 282: 1519–1522.
DOI: 10.1001/jama.282.16.1519.
Neumark-Sztainer D, van den Berg P, Hannan PJ, et al. (2006) Self-weighing in adolescents:
Helpful or harmful? Longitudinal associations with body weight changes and disordered eating. Journal of Adolescent Health 39: 811–818.
DOI: 10.1016/j.jadohealth.2006.07.002.
Ogden CL, Carroll MD, McDowell MA, et al. (2007)
Obesity among adults in the United States — No statistically significant change since 2003-
2004 . Data Brief No. 1, pp. 1–8. Atlanta, GA:
Centers for Disease Control and Prevention.
Ogden J and Evans C (1996) The problem with weighing: Effects on mood, self-esteem and body image. International Journal of Obesity
20: 272–277.
Ogden J and Whyman C (1997) The effect of repeated weighing on psychological state.
European Eating Disorders Review 5: 121–130.
DOI: 10.1002/(SICI)1099-0968(199706)5:2.
Qi BB and Dennis KE (2000) The adoption of eating behaviors conducive to weight loss. Eating
Behaviors 1(1): 23–31. DOI: 10.1016/S1471-
0153(00)00003-9.
Quick V, Larson N, Eisenberg ME, et al. (2012) Selfweighing behaviors in young adults: Tipping the scale towards unhealthy eating behaviors?
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015
Katterman et al. 11
Journal of Adolescent Health 51: 468–474.
DOI: 10.1016/j.jadohealth.2012.02.008.
Schulz KF, Altman DG and Moher D (2010)
CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Medicine 8: 18.
Stice E and Bearman SK (2001) Body image and eating disturbances prospectively predict increases in depressive symptoms in adolescent girls: A growth curve analysis. Developmental
Psychology 37: 597–607.
Stice E and Presnell K (2004) Weight control behavior questionnaire . Unpublished measure.
Stice E, Presnell K and Spangler D (2002) Risk factors for binge eating onset in adolescent girls:
A 2-year prospective investigation. Health
Psychology 21: 131–138.
Vella-Zarb RA and Elgar FJ (2009) The ‘Freshman
5’: A meta-analysis of weight gain in the freshman year of college. Journal of American
College Health 58(2): 161–166. DOI: 10.1080/
07448480903221392.
Williamson DF, Kahn HS, Remington PL, et al.
(1990) The 10-year incidence of overweight and major weight gain in US adults. Archives of
Internal Medicine 150: 665–672. DOI: 10.1001/ archinte.150.3.665.
Wing RR and Phelan S (2005) Long-term weight loss maintenance. American Journal of Clinical
Nutrition 82: 222S–225S. Available at: http:// www.ajcn.org/content/82/1/222S.short
Wing RR, Tate DF, Gorin AA, et al. (2006) A selfregulation program for maintenance of weight loss. New England Journal of Medicine 355:
1563–1571. DOI: 10.1056/NEJMoa061883.
Wing RR, Tate DF, Gorin AA, et al. (2007) “STOP regain”: Are there negative effects of daily weighing? Journal of Consulting and Clinical
Psychology 75: 652–656. DOI: 10.1037/0022-
006X.75.4.652.
Downloaded from hpq.sagepub.com
at DREXEL UNIV LIBRARIES on July 27, 2015