contra costa county community health indicators for
advertisement

community health indicators
for
contra costa county
December 2010
December 2010
1
Quick Start Guide
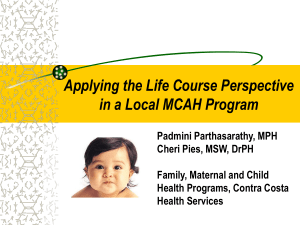
RATES are the best way to compare
risk between groups. A group with
a higher rate of death than another
group is at greater risk, even if they
don’t have a larger number of deaths
Table 1 Heart disease deaths by race/ethnicity
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
3,465
74.3%
151.9
African American
538
11.5%
258.8*
Hispanic
321
6.9%
107.4**
Asian/Pacific Islander
299
6.4%
99.5**
4,664
100.0%
White
Total
147.5
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The PERCENT gives you an easy way
to see how a health problem is spread
across different groups in the county.
The TOTAL provides a sense of
the overall size of the problem.
For more help understanding the rates and numbers used in this report, see the “Understanding the Data” section.
2
community health indicators
for
contra costa county
December 2010
Prepared for the Hospital Council of Northern & Central California by
the Community Health Assessment, Planning and Evaluation (CHAPE)
Unit of Contra Costa Health Services’ Public Health Division.
Key Contributors:
Debbie Casanova, MPH
Lisa Diemoz, MPH
Jennifer Lifshay, MBA, MPH
Chuck McKetney, PhD
3
Table of Contents
Quick Start Guide..............................2
Executive Summary...........................3
“Quick Look” Table.............................9
Demographics................................. 11
2005-07 American Community
Survey Table................................ 24
Health Inequities............................. 34
Leading Causes of Death
Leading Causes of Death,
Contra Costa and California.......... 50
Leading Causes of Death,
by Age...................................... 53
Leading Causes of Death,
by Race & Ethnicity..................... 63
Leading Causes of Death,
by Gender................................. 69
Leading Causes Appendix.............. 72
Prostate Cancer.......................... 145
Diabetes................................... 150
Heart Disease............................ 157
Stroke...................................... 162
Childhood Asthma...................... 167
Adult Overweight
and Obesity............................. 176
Childhood Overweight
and Obesity............................. 181
Injuries
Fatal and Non-fatal
Unintentional Injuries.................. 188
Homicide & Non-fatal
Assault.................................... 201
Suicide & Non-fatal
Self-Inflicted Injuries................ 211
Domestic Violence...................... 222
Mental Health
& Substance Abuse
Mental Health............................ 231
Substance Abuse........................ 239
Family, Maternal and Child Health
Overview of Local Births................ 74
Births to Teens............................. 77
Early Prenatal Care....................... 81
Low Birth Weight Infants............... 85
Fetal and Infant Deaths................. 90
Breastfeeding.............................. 95
Children’s Oral Health................. 102
Communicable Diseases
Childhood Immunizations &
Vaccine-Preventable
Diseases................................ 252
HIV/AIDS.................................. 256
Sexually Transmitted
Diseases................................ 264
Chronic Diseases
Cancer – All types...................... 106
Female Breast Cancer................. 117
Colorectal Cancer....................... 123
Lung Cancer.............................. 131
Pancreatic Cancer....................... 139
Understanding the Data.................. 270
Acknowledgements........................ 273
4
Executive Summary
This summary highlights key findings from the 2010 report Community Health Indicators for
Contra Costa County. This report was prepared by Contra Costa Health Services’ Community Health
Assessment, Planning and Evaluation Unit for the Hospital Council of Northern and Central California
and is intended to help health service providers and the broader community understand the health
status and health issues of the communities within Contra Costa and to guide local efforts to develop
programs, strategies and policies to improve the health of the county.
This report provides an update to the 2007 report Community Health Indicators for Contra Costa
County. It also includes several new features to help explore new topics and present others through a
different lens: a new section that illustrates important health disparities among different populations
in the county and some of the underlying social determinants of these unfair differences in health,
other new sections on breastfeeding and domestic violence, and maps illustrating hospitalizations for
non-fatal injuries and childhood asthma. Below are some of the key findings from the report.
Key Findings
DEMOGRAPHICS
From 2005–2007, Contra Costa had more than 1,011,000 residents. The racial/ethnic composition of the
county’s population was 51.9% white, 21.8% Hispanic, 13.5% Asian/Pacific Islander and 9.1% African
American. Between 2005-2007, there was an average of 13,398 births per year: 36.0% to Hispanic mothers, 35.7% to white mothers, 14.8% to Asian/Pacific Islander mothers and 8.9% to African American
mothers. With more births to Hispanic mothers than any other racial/ethnic group, Hispanics are the
fastest growing ethnic group in the county.
Contra Costa compares favorably with the state and nation on income and education, but looking at
the county as a whole masks the vast differences in experience of the county’s more than 1 million
residents. The median household income for Contra Costa in 2009 was $75,139 compared to just
$58,931 in California and $50,221 in the United States. Similarly, Contra Costa had a greater percentage of college graduates (37.6%) than the state (29.9%) or nation (27.9%) in 2009. Within the county,
however, distribution of income and education was not uniform and this unequal distribution was
echoed in disparities in health outcomes.
HEALTH INEQUITIES
Contra Costa residents of low-income and poorly educated communities, and African American
residents experience worse health outcomes and dramatically lower life expectancy.
Poverty was associated with poorer health status and shorter life expectancy among Contra Costa
residents. A child born in a low-poverty area in 2000 could expect to live more than six years longer
than a child born in a high-poverty area. Life expectancy in low-poverty areas was 81.4 years compared
to 74.9 years in high-poverty areas.
5
Lower educational attainment was associated with poorer health and shorter life expectancy among
Contra Costa residents. A child born in a high-education area in Contra Costa in 2000 could expect
to live more than seven years longer than a child born in a low-education area. Life expectancy in
high-education areas in the county was 82.0 years compared to 74.6 years in low-education areas.
African American residents in Contra Costa had a shorter life expectancy than other county residents
and were at greater risk for a number of poor health outcomes throughout the life course. African
Americans in Contra Costa had a shorter life expectancy (73.1 years) than any other racial/ethnic group
in the county. An Asian/Pacific Islander or Hispanic baby born between 2005 and 2007 in Contra Costa
could expect to live more than five years longer than a white baby and more than 12 years longer than
an African American baby born at the same time.
African American residents also had significantly higher rates of death than the county overall for
a number of specific causes of death, including heart disease, cancers (all types combined as well as
female breast, colorectal, lung and prostate cancers), diabetes, stroke, homicide, unintentional injuries,
fetal and infant deaths, and HIV disease. Compared to county residents overall, African Americans
also experienced higher rates of new cases of colorectal, lung and prostate cancer, new cases of HIV
and AIDS, hospitalization for non-fatal assault and self-inflicted injuries, low birth weight infants and
teen births, and a higher percent overweight and obese fifth-graders.
CAUSES OF DEATH AND DISABILITY
Most deaths in Contra Costa were from chronic diseases. Cancer and heart disease were the top
two causes of death in the county, accounting for 47.7% of all deaths, followed by stroke (7.1%). Lung,
colorectal and breast cancer were the leading causes of cancer death.
Smoking and obesity, key risk factors for heart disease, stroke and cancer, continue to plague local
residents. The prevalence of current smoking was 10.7% among adults in Contra Costa. More than half
of adults (56.2%) and more than one-quarter (26.5%) of fifth-graders in the county were overweight or
obese. A greater percentage of fifth-graders in the Antioch, West Contra Costa and Pittsburg unified
school districts were overweight or obese compared to fifth-graders countywide.
Of Contra Costa’s top 10 leading causes of death, only homicide was more likely in the county
than the state. Among younger residents (ages 15–24), unintentional injury, homicide and suicide
are the three leading causes of death. People ages 15–24 were also more likely to be hospitalized for
non-fatal assaults and self-inflicted injuries than other age groups. Because deaths from these causes
affect young people disproportionately, they have a greater impact on years of “potential life” lost. Large
numbers and high rates of homicide threatened the health and well-being of some communities more
than others, including Richmond, Antioch, Pittsburg and San Pablo.
Unintentional injury is an important health issue for residents of all ages. Unintentional injury was
one of the top three leading causes of death among residents ages one to 54 years. Residents ages 65
years and older were most likely to be hospitalized and die from unintentional injury. The unintentional
injury death rate was higher for residents of Martinez and Walnut Creek than for residents of the county
overall, driven by poisonings and falls.
6
HIV/AIDS continues to spread in Contra Costa. Most HIV and AIDS cases were among men; men
who have sex with men (MSM) accounted for almost three-quarters (73.5%) of transmissions among
men. Almost half of the HIV cases (49.6%) were diagnosed among whites, but African Americans
had higher rates of new HIV and AIDS cases than the county overall. Among people diagnosed with
AIDS, residents of Richmond, Concord, Antioch and Walnut Creek accounted for more than half
(54.5%) of AIDS cases. Richmond residents were more likely to be diagnosed with AIDS than county
residents as a whole. People ages 25-44 years were most likely to be diagnosed with HIV and AIDS.
Rates of chlamydia and gonorrhea were also higher among younger people. Residents ages 15–29
years had higher rates of chlamydia and those ages 15-34 had higher rates of gonorrhea than county
residents overall.
DATA SOURCES AND LIMITATIONS
The information presented in this report helps provide a picture of the health of the county. It includes
data that is available and traditionally measured by health departments. But it is important to be aware
of the limitations of data presented and to understand what is missing. Contra Costa is a large county
with wide differences in the health of its diverse communities. A health indicator for the county as a
whole, such as all-cause mortality, is an average of extremes and does little to help us identify problems
in specific communities or evaluate successes of targeted programs. When available, data in this report
is presented at a sub-county level, by age, race/ethnicity and community to provide information about
the distribution of key health issues among different populations in the county. Data from the U.S.
Census and American Community Survey provide information about demographic factors such as
education, income and employment, all strongly linked to health. More current information on these
issues will be available at a detailed sub-county level in 2011 with the release of Census 2010 data,
which will allow for further exploration of these social determinants of health in the county.
Other traditional health data sources used for this report, however, are often late-stage indicators of
health problems or offer limited information about how or why these health issues vary throughout
the county. At best, they often provide only hints of the kinds of interventions that might be needed or
effective. The leading causes of death in the county, certainly a late-stage measure of community health
status, come from death certificates. Information about the causes of morbidity, such as hospitalization
data from the Office of Statewide Health Planning and Development for asthma, diabetes and injury
indicate what kinds of diseases result in hospitalization, but not why people develop these health issues.
Asthma, for example, can be managed successfully as an outpatient condition and should seldom result
in hospitalization. Yet some communities in West County have higher rates of asthma hospitalization
than the county as a whole. Although there may be a higher prevalence of asthma in this part of the
county, high hospitalization rates might also be the result of poor management of this chronic condition
and related social and environmental factors. Information about the prevalence of chronic conditions,
such as asthma, diabetes and obesity, come from self-reported data though a random-digit telephone
survey conducted by the California Health Interview Survey. Yet too few people are sampled in Contra
Costa to develop reliable estimates for many health conditions by ethnicity or region of the county.
Although these data sources are imperfect, they allow us to begin to get an understanding of the health
of Contra Costa and what might be done to improve it.
7
Conclusions
Inadequate information about some of these issues does not mean we must wait to act. Lung cancer is
highly preventable by eliminating smoking. Deaths from colorectal and breast cancer can be greatly
reduced by screening, early diagnosis and effective treatment. Policies restricting secondhand smoke
clear the air and change the social environment to discourage smoking, and licensing tobacco retailers
reduces sales to minors and helps prevent youths from becoming addicted. While HIV/AIDS deaths
continue to decline as a result of more effective treatment, persistently confronting social barriers to
emphasize prevention messages remains key to controlling this disease.
Newer ways of looking at community health suggest examining additional kinds of data to develop
and evaluate new strategies to address the underlying causes of the most important health issues in
our community. Understanding the role of the built environment on health, for example, could lead
us to look at miles of complete streets, the availability of healthy food through a retail food index, the
existence of safe routes to school, or opportunities for pedestrian and bicycle transportation. What we
measure drives the focus of our attention. As Contra Costa Health Services and other health service
providers and community agencies work to improve the health of the county in new ways, additional
health indicators need to be developed to guide our efforts to measure our progress.
Although our current health data starkly illuminates the problem of health inequities, it is not as
forthcoming about its causes and solutions. One approach to understanding and addressing health
inequities is suggested by the California Department of Public Health (CDPH), which outlines what
the department has identified as the core elements of a healthy community: 1) meets the basic needs
of all, 2) has a quality and sustainable environment, 3) supports adequate levels of economic and
social development, and 4) promotes health and social equity. According to this model, we should be
measuring and addressing things like the availability of housing, the quality of health care, the impact
of secondhand smoke, the availability of jobs at living wage, the opportunities for physical activity,
or the effectiveness of our school parent teacher associations. These may be the kinds of issues key to
addressing health inequities and improving the quality of life for all in Contra Costa.
8
Quick Look Table
Contra Costa Health Indicators 2005–2007
Is Contra Costa
different from
California?
Groups at higher risk than the
county overall
(except for male/female
comparisons)
Communities at
higher risk than the
county overall
DEATHS
CHRONIC DISEASES
Heart disease
Better
Men; African Americans
San Pablo, Oakley,
Antioch, Richmond,
Martinez, Pittsburg
Cancer (all types)
Better
Men; African Americans,
whites
San Pablo, Oakley,
Martinez, Antioch
Cancer (female breast)
Similar
African Americans
None
Cancer (colorectal)
Similar
African Americans
Antioch
Cancer (lung)
Similar
Men; African Americans,
whites
San Pablo, Antioch
Cancer (prostate)
Better
African Americans
None
Cancer (pancreatic)
Similar
None
None
Diabetes
Better
Men; African Americans
San Pablo,
Pittsburg, Antioch,
Richmond
Stroke
Better
African Americans
San Pablo,
Pittsburg,
Richmond
Homicide
Worse
Men; African Americans;
Adults 21-44 years
Richmond, San
Pablo
Suicide
Similar
Men; whites
Martinez, Walnut
Creek
Unintentional injuries
Better
Men; African Americans,
whites; adults 65 years or
older
Martinez, Walnut
Creek
INJURY++
FAMILY MATERNAL & CHILD HEALTH
Fetal deaths
Similar
African Americans
+
Infant deaths
Better
African Americans
+
Worse
CASES
CHRONIC DISEASES
Cancer (all types)
Men; blacks, whites;
+
Invasive:Worse
Invasive: white women
+
In situ: Worse
In situ: none
Cancer (colorectal)
Similar
Men; blacks
+
Cancer (lung)
Similar
Men; blacks
+
Cancer (prostate)
Worse
Black men
+
Cancer (pancreatic)
Similar
None
+
Childhood asthma
hospitalizations
Worse
Boys; African Americans
Cancer (female breast)
9
(See Childhood
Asthma Section)
Quick Look Table
Contra Costa Health Indicators 2005–2007
Is Contra Costa
different from
California?
Groups at higher risk than the
county overall
(except for male/female
comparisons)
Communities at
higher risk than the
county overall
CASES
CHRONIC DISEASES (continued)
Diabetes
Similar
None (Bay Area)
+
Overweight & obese adults
Similar
Men; American Indian/Alaska
Natives, African Americans,
Latinos (Greater Bay Area)
+
Overweight & obese
fifth-graders
Better
Boys; Hispanics/Latinos;
African Americans/blacks
Antioch, West
Contra Costa,
Pittsburg unified
school districts
Non-fatal assault
hospitalizations
Better
Men, African Americans;
15-34 year olds
(See Homicide &
Non-Fatal Assault
Section)
Non-fatal self-inflicted
hospitalizations
Better
Women; whites, African
Americans; 15-54 year olds
(See Suicide &
Non-Fatal SelfInflicted Section)
Non-fatal unintentional
injury hospitalizations
Better
Women; whites; Adults
65 years or older
(See Fatal & NonFatal Unintentional
Injury Section)
INJURY (HOSPITALIZATIONS)
FAMILY MATERNAL & CHILD HEALTH
Low birth weight
Similar
African Americans
Richmond
Teen births
Better
Hispanics, African Americans
San Pablo, Bay
Point, Richmond,
Pittsburg and
Antioch
AIDS
Better
Men; African Americans,
25-44 year olds
Richmond
Chlamydia
Better
Women; 15-29 year olds
COMMUNICABLE DISEASES
Note: race/ethnicity data not
available.
+ Data not available at a geographic sub-county level.
++ These comparisons are based on crude rates and do not include late effects.
10
+
contra costa county
Demographics
Geography
Contra Costa County is located in the San Francisco Bay Area of Northern California, northeast of San
Francisco and southwest of Sacramento. The county covers roughly 806 square miles and includes 19
incorporated cities (see map above) and numerous unincorporated areas that are dispersed throughout
its East, West and Central regions.1,2
Population
In 2008, Contra Costa County had an estimated population of 1,029,703, making it the ninth most
populous county in California.1 Richmond, Concord and Antioch were each home to more than 100,000
residents, making them the three largest cities in the county. Between 2000 and 2008, the county gained
76,399 residents. Four cities in East County became home to nearly two-thirds (61.1%) of these residents:
Brentwood, Antioch, Pittsburg and Oakley. Each of these four cities added more than 6,000 residents
to their respective populations. Brentwood gained almost 25,000 residents during this time period.
Between 2000 and 2008, the overall county population grew by 8.0%. This rate was similar to California’s
growth rate of 8.1%. During this time period, all selected cities listed above experienced population change
at different rates than the county overall. Brentwood (100.0%), Hercules (25.6%), Oakley (23.9%), Pittsburg
(12.4%), Antioch (9.5%) and San Ramon (9.4%) had higher rates of growth than the county overall. The
remaining communities listed in Table 1 had lower rates of growth than the county overall.
Between 2004 and 2008, the county population growth rate (3.5%) was higher than California’s rate
(3.2%). Brentwood (26.5%), Oakley (21.0%), Hercules (6.7%) and Pittsburg (4.5%) had higher growth
rates than the county overall (3.5%). All remaining communities listed in Table 1, except for Orinda,
Clayton, Moraga and Lafayette had lower growth rates than the county overall.
11
Table 1. Population change in selected cities
Contra Costa County and California, 2000–2008
2000
2004
2008
Brentwood
24,741
39,117
49,480
Antioch
91,564
99,211
100,219
Pittsburg
57,081
61,395
Oakley
25,849
Hercules
2000 – 08 Pop.
change
# / %
2004-08 Pop.
change
# / %
24,739 / 100.0%*
10,363 / 26.5%*
9.5%*
1,008 /
1.0%**
64,148
7,067 / 12.4%*
2,753 /
4.5%*
26,483
32,035
6,186 / 23.9%*
5,552 / 21.0%*
19,493
22,946
24,484
4,991 / 25.6%*
1,538 /
6.7%*
San Ramon
44,922
48,532
49,161
4,239 /
9.4%*
629 /
1.3%**
Richmond
99,812
100,641
102,285
2,473 /
2.5%**
1,644 /
1.6%**
Lafayette
23,985
24,232
25,011
1,026 /
4.3%**
779 /
3.2%
Orinda
17,645
17,845
18,445
800 /
4.5%**
600 /
3.4%
Moraga
16,342
16,532
17,050
708 /
4.3%**
518 /
3.1%
Clayton
10,795
10,923
11,278
483 /
4.5%**
355 /
3.3%
San Pablo
30,250
30,394
30,729
479 /
1.6%**
335 /
1.1%**
Pleasant Hill
33,060
33,094
32,862
-198 /
-0.6%**
-232 /
-0.7%**
Pinole
19,193
19,035
18,808
-385 /
-2.0%**
-227 /
-1.2%**
Danville
41,773
41,429
41,182
-591 /
-1.4%**
-247 /
-0.6%**
Martinez
35,943
35,648
35,145
-798 /
-2.2%**
-503 /
-1.4%**
El Cerrito
23,205
22,726
22,222
-983 /
-4.2%**
-504 /
-2.2%**
Concord
122,255
122,184
121,160
-1,095 /
-0.9%**
-1,024 /
-0.8%**
Walnut Creek
64,687
63,741
63,486
-1,201 /
-1.9%**
-255 /
-0.4%**
Contra Costa
953,304
994,844
1,029,703
76,399 /
8.0%
33,998,767
35,629,666
California
8,655 /
36,756,666 2,757,899 /
Contra Costa and California totals include cities not listed above.
* Significantly higher growth rate than the county overall.
** Significantly lower growth rate than the county overall.
12
34,859 /
3.5%
8.1% 1,127,000 / 3.2%**
All cities experienced population change between 2000 and 2008, but the change was not constant during
the entire time period. Some communities experienced more of their population growth or population loss
between 2004 and 2008. Oakley, Orinda, Clayton, Moraga, Lafayette, Richmond and San Pablo experienced
more than half of their overall population growth between 2004 and 2008. Pleasant Hill, Concord, Pinole,
Martinez and El Cerrito experienced more than half of their overall population loss between 2004 and 2008.
GENDER & AGE
In 2008, Contra Costa’s population was 51.0% women (523,000) and 49.0% men (506,000).3 The median
age was 38.1 years.3 Nearly a quarter (24.2%) of the population was younger than 18 years and more
than a tenth (12.0%) was 65 years and older.
The percentages of Contra Costa residents from three age groups (18–24, 45–64, and 65 years and
older) were greater in 2008 compared to 2000. The percentage of residents 18–24 years grew from 7.6%
in 2000 to 9.4% in 2008, residents 45–64 years grew from 23.8% to 27.9% and residents 65 years and
older grew from 10.8% to 12.0%. This pattern was consistent with the state findings for the same years.
The percentages of residents younger than 18 years and 25–44 years were lower in 2008 than in 2000.
Figure 1. Age distribution of population
Contra Costa County and California, 2000
30.9%**
26.8%**
31.6%
27.8%
% of total population
23.8%*
20.8%
10.8%* 10.3%
9.4%
7.6%**
Under 18
18-24
25-44
Contra Costa
45-64
California
* Significantly higher than the California estimate for the same age group.
** Significantly lower than the California estimate for the same age group
13
65+
Figure 2. Age distribution of population
Contra Costa County and California, 2008
28.8%
25.5%
% of total population
24.2%**
27.9%*
26.5%**
24.0%
12.0%*
9.4%**
Under 18
10.6%
18-24
25-44
Contra Costa
45-64
11.2%
65+
California
* Significantly higher than the California estimate for the same age group.
** Significantly lower than the California estimate for the same age group.
The population of Contra Costa has been shifting toward older adults. The 2008 percentage of county
residents 45 years and older (39.9%) was higher than the percentage in 2000 (34.7%) and it increased
each year between 2001 and 2008. Contra Costa’s percentage of adults age 45 and older was higher
than California’s percentage in both 2000 and 2008.
The California and Contra Costa populations of residents 65 years and older grew between 2000 and
2008, and Contra Costa’s percentage was higher than the state’s every year. The percentage of county
residents 65 years and older increased from 10.8% in 2000 to 12.0% in 2008 and California’s percentage
of residents 65 years and older increased from 10.3% to 11.2%.
14
28.8%
24.2%**
27.9%*
26.5%**
25.5%
24.0%
Figure 3 Percentage of population 65 years and older by year
% of total population
% of total population
Contra Costa County and California, 2000–2008
12.5
12
11.5
11
12.0%*
9.4%**
10.6%
11.2%
10.5
10
9.5
9
Under2000
18
2001
18-242002
2003
25-442004
Contra Costa
2005
45-64 2006
2007
65+
2008
California
RACE AND ETHNICITY
In 2008, half of Contra Costa’s residents were white (520,021), followed by Hispanic (235,475), Asian/
Pacific Islander (142,235) and African American (92,819).
Table 2 Racial/ethnic composition of population
Contra Costa County, 2008
People
Percent
White
520,102
50.5%
Hispanic
235,475
22.9%
Asian/Pacific Islander
142,235
13.8%
92,819
9.0%
1,029,703
100.0%
African American
Total
Total includes some racial/ethnic groups not listed above.
Between 2000 and 2008, the percentage of white residents in Contra Costa declined while the percentage
of Hispanic, Asian/Pacific Islander and African American residents increased. The percentage of white
residents fell from 58.2% in 2000 to 50.5% in 2008. The percentage of Hispanics (17.8% to 22.9%) Asians/
Pacific Islanders (11.5% to 13.8%) and African Americans (8.4% to 9.0%) grew between 2000 and 2008.
15
In 2008, Contra Costa had higher percentages than California of whites (50.5% vs. 42.0%), Asians/
Pacific Islanders (13.8% vs. 12.5%) and African Americans (9.0% vs. 5.9%). Contra Costa had a lower
percentage of Hispanics (22.9%) than California (36.6%).
Figure 4 Racial/ethnic composition of population
Contra Costa County, 2000 and 2008
58.2%
% of total population
50.5%**
17.8%
22.9%*
13.8%*
11.5%
White
Hispanic
API
2000
8.4% 9.0%*
African American
2008
* Significantly higher than the 2000 estimate for the same race/ethnic group.
** Significantly lower than the 2000 estimate for the same race/ethnic group.
Figure 5 Racial/Ethnic Composition of Population
Contra Costa County and California, 2008
*50.5%
% of total population
42.0%
36.6%
**22.9%
*13.8%
12.5%
*9.0%
5.9%
White
Hispanic
API
Contra Costa
African American
California
* Significantly higher than the California estimate for the same race/ethnic group.
** Significantly lower than the California estimate for the same race/ethnic group.
16
LANGUAGE
In 2008, 67.4% (649,582) of Contra Costa residents 5 years and older reported speaking only English
at home. The remaining 32.6% of residents (313,725) spoke a language other than English at home. Of
these residents, 52.6% (164,944) spoke Spanish and 26.1% (81,858) spoke an Asian or Pacific Islander
language at home.4
NATIVITY
In 2008, 24.1% (248,583) of Contra Costa residents were born outside of the United States. The largest
groups of foreign-born residents came from Latin America (42.7%, 106,110) and Asia (41.6%, 103,463),
followed by Europe (9.9%, 24,554) and Africa (3.2%, 7,942).4
EDUCATION
In 2008, 88.1% of Contra Costa residents 25 years and older had at least graduated from high school.
Contra Costa’s percentage (88.1%) was higher than the state’s (80.2%). The county also had a higher
percentage (38.5%) of residents with a bachelor’s degree or higher compared to California (29.6%).5
Twelve percent (12.0%) of Contra residents were dropouts, meaning they were not enrolled in school
and had not graduated from high school.3
INCOME
Contra Costa’s 2008 median household income was $78,618. This amount was higher than the 2008
California median household income of $61,021. The median household income in the county and the
state both increased by more than $15,000 between 2000 and 2008.
90000
The median household income for Contra Costa was higher than California’s every year between
2000 and 2008. However, California’s median household income climbed almost every year whereas
80000
Contra Costa’s remained
more stagnant. From 2000 to 2008, California showed year-to-year increases
in median household income except for year 2002–2003, when it remained stable. Contra Costa’s only
year-to-year increases
70000 were 2000–2001 and 2005–2006, otherwise the median household income did
not differ from the previous year.
90000
Figure
6 Median household income by year
60000
Median income
Contra Costa County and California, 2000–2008
Median income
$ 80000
50000
70000
40000
60000
30000
50000
20000
40000
10000
2000
2001
2002
2003
2004
Contra Costa
30000
20000
17
2005
California
2006
2007
2008
Poverty
In 2008, 21.6% (220,350) of Contra Costa’s population lived below 200% of the federal poverty level
(200% FPL). In 2008, the income level for a family of four living at 200% FPL was at $42,400.
Between 2000 and 2008, the percent of county residents living below 200% FPL increased from 16.8%
in 2000 to 21.6% in 2008. Over this time period, the county percentage of the population living below
200% FPL increased every year except for 2004–2005 and 2006–2007. California’s, on the other hand,
fluctuated throughout. California had a lower percentage of the population living below 200% FPL in
2008 (31.9%) than in 2000 (32.8%). Contra Costa’s percentage of the population living below 200%
FPL was consistently lower than California’s.
Figure 7 Percent of residents living below 200% of federal poverty level
by year
Contra Costa County and California, 2000–2008
35.0%
% of total population
30.0%
25.0%
20.0%
15.0%
10.0%
5.0%
0.0%
2000 2001 2002 2003 2004 2005 2006 2007 2008
CCC
18
CA
Employment
In 2009, the annual unemployment rate for Contra Costa adults 16 years and older was 10.3%. This was
significantly higher than the Contra Costa rate of 3.5% in 2000. The state unemployment rate increased
from 4.9% in 2000 to 11.4% in 2009. The state unemployment rate was higher than Contra Costa’s rate
every year between 2000 and 2009 and followed a similar pattern to the county.
Figure 8 Unemployment Rate by Year
Contra Costa County and California, 2000–2009
12.0%
10.0%
% of total population
8.0%
6.0%
4.0%
2.0%
0.0%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
California
Contra Costa
Access to Health Care
One’s ability to access health care can be dependent upon many factors, including health care insurance
and English language skills. Not having insurance is associated with a much lower likelihood of seeing
a doctor within the past year, and a higher likelihood of experiencing delays in obtaining medical and
mental health services.6 Proficiency in the English language facilitates entry into and navigation of the
health care system and understanding of important health information.7 This section presents data on
how these two factors play out within the county.
19
HEALTH INSURANCE
In 2007, 13.5% (123,000) of Contra Costa residents younger than 65 years were uninsured. The percent
of uninsured residents in Contra Costa (13.5%) was similar to the greater Bay Area (13.1%), and
lower than California (19.5%). In Contra Costa, adults between the ages of 18 to 64 comprised 87.8%
(108,000) of the county’s uninsured.
Table 3 Residents younger than 65 years without
health insurance, 2007
People without
health insurance Prevalence
California
6,400,000
In this section,
“uninsured” refers
to people uninsured
for all or part of
the last 12 months.
19.5%*
Greater Bay Area
820,000
13.1%
Contra Costa County
123,000
13.5%
Estimates are not age-adjusted.
*Significantly higher prevalence than the county and greater Bay Area overall.
More men (72,000) than women (52,000) were uninsured for all or part of the year in 2007, but the
percentages of uninsured men (15.9%) and women (11.2%) were similar.
Table 4 Residents younger than 65 years without
health insurance by gender
Contra Costa County, 2007
People without
health insurance Prevalence
Men
72,000
15.9%
Women
52,000
11.2%
123,000
13.5%
Total
Estimates are not age-adjusted.
Editor’s note: Analyses of Contra Costa’s uninsured by race/ethnicity were not
possible due to small sample size, but we can look to the Greater Bay Area
data for an indication of how lack of health coverage affects our community
disproportionately.
In the greater Bay Area, the largest number of uninsured residents was among Latinos (315,000),
followed by whites (231,000), Asians/Pacific Islanders (188,000) and African Americans (55,000). A
20
greater percentage of Latinos (21.4%) in the greater Bay Area were uninsured compared to the region
overall (13.1%). A lower percentage of whites (8.2%) were uninsured compared to the region overall.
Table 5 Residents under 65 years without health
insurance by race/ethnicity
Greater Bay Area, 2007
People without
health insurance
Prevalence
Latino
315,000
White
213,000
Asian/Pacific Islander
188,000
14.0%
55,000
13.6%
820,000
13.1%
African American
Total
21.4%*
8.2%**
Estimates are not age-adjusted.
Total includes racial/ethnic groups not listed above.
* Significantly higher than the greater Bay Area overall.
** Significantly lower than the greater Bay Area overall.
LIMITED ENGLISH PROFICIENCY
In 2008, 13.9% (133,847) of Contra Costa’s population 5 years and older reported speaking English
less than “very well”, which is categorized as limited English proficiency (LEP).4 Almost two-thirds
(63.7%, 85,238) of Contra Costa County’s LEP population reported speaking Spanish at home, and
nearly a quarter (23.0%, 30,833) spoke an Asian/Pacific Islander language at home.4
Language barriers in the health care setting can lead to problems including denial or delay of services,
issues with medication management and underutilization of preventive services.7 Difficulty in communication can also limit clinicians’ ability to understand the patient’s condition and effectively provide
treatment.7 The quality of communication between patients and providers is strongly associated with
providers’ ability to deliver better and safer care for LEP patients.7
Language services, such as translation and interpretation, can facilitate this communication and thus
improve health care quality, the patient experience, compliance with recommended care and ultimately
health outcomes.7
21
Data Sources: Demographics
tables and figures
Table 1, 2 and Figures 1-7: The data are limited to the household populations and exclude the population living in
institutions, college dormitories and other group quarters. Any analyses, interpretations or conclusions of the data
have been reached by Community Health Assessment, Planning and Evaluation (CHAPE) unit of Contra Costa Health
Services.
Table 1: Population data from U.S. Census Bureau Population Estimates Program’s Population Estimates 2000 through
2008 by place. Data retrieved January 8, 2010.
Figures 1–3: Population data by age from the U.S. Census Bureau Population Supplementary Survey Summary Tables
2000, 2001 and American Community Survey Demographic and Housing Summary Tables 2002–2008. Data retrieved
January 8, 2010.
Table 2 and Figure 4,5: Population data by race/ethnicity from the U.S. Census Bureau Population by Race/Ethnicity
Supplementary Survey Tables 2000, 2001, and American Community Survey Estimates 2002–2008. Data retrieved July
30, 2010. The U.S. Census Bureau “Black or African American” is used for African American, and “Latino/Hispanic” is
used for Hispanic. Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/
Pacific Islanders and African Americans include non-Hispanic residents.
Figure 6: Median household income data from the U.S. Census Bureau Supplementary Survey Summary Tables 2000,
2001 American Community Survey. Contra Costa County and California Selected Economic Characteristics 2002–2008.
Retrieved January 5, 2010 from http://factfinder.census.gov/servlet/ADPTable. The data are limited to median household
income in the past 12 months.
Figure 7: Poverty data from the U.S. Census Bureau Supplementary Survey Tables Contra Costa County And California
2000,2001 and American Community Survey Tables Contra Costa County and California 2002–2008. The data are limited
to median household income in the past 12 months.
Figure 8: Unemployment rate data from the U.S. Bureau of Labor Statistics, Local Area Unemployment Statistics 1999–
2009. Estimates are annual rates and are not seasonally adjusted. Any analyses, interpretations or conclusions of the data
have been reached by Community Health Assessment, Planning and Evaluation (CHAPE) unit of Contra Costa Health
Services.
Tables 3–5: Local data about the uninsured from the California Health Interview Survey’s AskCHIS data query system,
copyright© 2007 the Regents of the University of California, all rights reserved, available online at: http://www.chis.ucla.
edu/. Not all race/ethnicities are shown but all are included in totals for the county, county by gender, and Greater Bay
Area. Data presented for Latinos include Latino residents of any race. Data presented for whites, Asians/Pacific Islanders
and African Americans include non-Latino residents. Greater Bay Area data includes the following counties: Alameda,
Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano and Sonoma. Ask CHIS data are generated
from a telephone survey that asks questions to a randomly selected group of residents in Contra Costa and other counties
in California. Responses are then weighted to represent the county, region, and state as whole. The variable analyzed
was created from multiple health insurance questions and reveals whether persons are currently uninsured, experienced
uninsurance at some point during the last 12 months, or were insured all of the last 12 months. Data analysis performed
August 2, 2010 by the Community Health Assessment, Planning and Evaluation unit of Contra Costa Health Services.
text
1.
Contra Costa County official county website – “Visiting” and “Cities of Contra Costa” webpages. Retrieved August 3,
2010 from http://www.co.contra-costa.ca.us
22
2.
3.
4.
5.
6.
7.
National Association of Counties website – “Find a County” webpage. Retrieved January 8, 2010 from
http://www.naco.org
U.S. Census Bureau, 2008 American Community Survey. Contra Costa County Population and Housing Narrative
Profile: 2008. Retrieved January 5, 2010 from http://factfinder.census.gov/servelet/NPTable
U.S. Census Bureau, 2008 American Community Survey. Contra Costa County Selected Social Characteristics from
2008 ACS 1-Year Estimates. Retrieved January 5, 2010 from http://factfinder.census.gov/servlet/ADPTable
U.S. Census Bureau, 2008 American Community Survey. Contra Costa County and California Selected Social
Characteristics from 2008 ACS 1-Year Estimates. Retrieved January 5, 2010 from
http://factfinder.census.gov/servlet/ADPTable
ER Brown, R Kronick, NA Ponce, J Kencheloe, SA Lavarreda, EC Peckham. The State of Health Insurance in
California: Findings from the 2007 California Health Interview Survey, Los Angeles, CA; UCLA Center for Health
Policy Research, 2009.
Au M., Taylor E.F., Gold M. (2009). Improving Access to Language Services in Health Care; A Look at National and
State Efforts Policy Brief. Mathematica Policy Research, Inc. Retrieved August 3, 2010 from
http://www.mathematica-mpr.com/publications/PDFs/health/languageservicesbr.pdf
23
American Community Survey 2005–2007 Summary Table
California
TOTAL POPULATION
GENDER
Male
Female
AGE
Under 5 years
5 to 9 years
10 to 14 years
15 to 19 years
20 to 24 years
25 to 29 years
30 to 34 years
35 to 39 years
40 to 44 years
45 to 49 years
50 to 54 years
55 to 59 years
60 to 64 years
65 to 69 years
70 to 74 years
75 to 79 years
80 to 84 years
85 years and over
Median age (years) (both sexes)
Male
Female
RACE/ETHNICITY
White
Hispanic or Latino
Black or African American
American Indian and Alaska
Native
Asian
Native Hawaiian and
Other Pacific Islander alone
Some other race
Two or more races
PLACE OF BIRTH
U.S. born
Foreign born
36,264,467
#
%
Contra Costa
County
1,011,372
#
%
Antioch
Bay Point
100,432
#
%
20,374
#
%
18,122,719
18,141,748
50.0%
50.0%
496,617
514,755
49.1%
50.9%
50,137
50,295
49.9%
50.1%
9,956
10,418
48.
51.
2,630,827
2,471,647
2,661,180
2,722,939
2,696,958
2,615,154
2,592,484
2,726,023
2,761,672
2,674,259
2,345,501
1,970,226
1,467,671
1,104,513
900,204
779,823
619,874
523,512
34.5
33.4
35.6
7.3%
6.8%
7.3%
7.5%
7.4%
7.2%
7.1%
7.5%
7.6%
7.4%
6.5%
5.4%
4.0%
3.0%
2.5%
2.2%
1.7%
1.4%
(x)
(x)
(x)
65,347
69,060
71,353
72,815
65,277
60,632
61,784
72,963
78,917
82,843
75,465
66,083
50,740
34,069
27,168
22,900
17,817
16,139
37.7
36.4
38.8
6.5%
6.8%
7.1%
7.2%
6.5%
6.0%
6.1%
7.2%
7.8%
8.2%
7.5%
6.5%
5.0%
3.4%
2.7%
2.3%
1.8%
1.6%
(x)
(x)
(x)
7,813
7,584
9,239
8,466
8,475
5,958
5,236
8,431
7,111
8,605
6,728
5,177
3,772
2,413
1,970
1,735
952
767
32.3
30.6
33.7
7.8%
7.6%
9.2%
8.4%
8.4%
5.9%
5.2%
8.4%
7.1%
8.6%
6.7%
5.2%
3.8%
2.4%
2.0%
1.7%
0.9%
0.8%
(x)
(x)
(x)
1,979
1,667
1,530
1,588
1,522
1,783
1,341
1,854
1,328
1,516
1,168
936
472
731
247
370
137
205
30.7
28.7
32.3
9.
8.
7.
7.
7.
8.
6.
9.
6.
7.
5.
4.
2.
3.
1.
1.
0.
1.
15,593,822
12,954,535
2,205,637
170,156
43.0%
35.7%
6.1%
0.5%
525,270
220,862
92,046
2,610
51.9%
21.8%
9.1%
0.3%
40,970
29,376
16,119
672
40.8%
29.2%
16.0%
0.7%
5,990
9,206
2,048
134
29.
45.
10.
0.
4,369,567
119,571
12.0%
0.3%
132,623
3,916
13.1%
0.4%
9,473
261
9.4%
0.3%
1,500
450
7.
2.
140,571
710,608
0.4%
2.0%
5,309
28,736
0.5%
2.8%
493
3,068
0.5%
3.1%
277
769
1.
3.
26,398,930
9,865,537
72.8%
27.2%
775,017
236,355
76.6%
23.4%
78,392
22,040
78.1%
21.9%
13,765
6,609
67.
32.
24
American Community Survey 2005–2007 Summary Table
California
TOTAL POPULATION
36,264,467
#
%
LANGUAGE (population 5 years and over)
Speak only English at home
19,406,677
57.7%
Language other than English at
14,226,963
42.3%
home (All)
Spanish
9,502,512
28.3%
Asian and Pacific Island
3,015,326
9.0%
languages
EDUCATION (population 25 years and over)
No high school diploma
4,625,044
20.0%
High school graduate (includes
equivalency)
5,288,363
22.9%
Some college, no degree
4,698,527
20.4%
Associate's degree
1,757,763
7.6%
Bachelor's degree
4,315,630
18.7%
Graduate or prof. degree
2,395,589
10.4%
Total
23,080,916 100.0%
INCOME & POVERTY
Total (for whom poverty status
is determined)
All ages, below 200% of
federal poverty level
Under 18 years:
18 to 64 years:
65 years and over:
Median household income ($)
EMPLOYMENT
Civilian population 25–64 years
old, in labor force
Unemployed
VETERAN STATUS
Civilian population (18 & over)
Civilian veterans
DISABILITY STATUS
Population 5 to 15 years
with any disability
Population 16 to 64 years
with any disability
Population 65 years and older
with any disability
Contra Costa County
1,011,372
#
%
Antioch
100,432
#
%
Bay
20,374
#
649,697
296,328
68.7%
31.3%
64,429
28,190
69.6%
30.4%
9,432
8,963
158,310
79,548
16.7%
8.4%
18,374
5,616
19.8%
6.1%
7,385
1,336
80,297
12.0%
9,338
15.9%
3,181
138,856
145,557
54,798
158,237
89,775
667,520
20.8%
21.8%
8.2%
23.7%
13.4%
100.0%
15,485
26.3%
15,705
26.7%
6,025
10.2%
9,174
15.6%
3,128
5.3%
58,855 100.0%
3,533
2,541
976
1,572
285
12,088
99,967 100.0%
20,282
35,482,447
100.0%
999,614
100.0%
11,374,010
32.1%
204,586
20.5%
24,003
24.0%
8,451
3,829,508
6,384,141
1,160,361
58,361
33.7%
56.1%
10.2%
x
65,492
116,110
22,984
75,483
32.0%
56.8%
11.2%
x
9,713
12,907
1,383
69,165
40.5%
53.8%
5.8%
x
3,487
4,299
665
52,594
14,464,438
100.0%
423,967
100.0%
39,077 100.0%
7,347
795,267
5.5%
20,708
4.9%
26,726,775
2,152,091
100.0%
8.1%
758,811
65,790
5,679,344
265,555
23,577,830
2,446,635
3,809,961
1,558,810
100.0%
4.7%
100.0%
10.4%
100.0%
40.9%
156,126
8,007
667,337
70,178
114,850
43,092
2,305
5.9%
373
100.0%
8.7%
70,490 100.0%
6,712
9.5%
14,082
999
100.0%
5.1%
100.0%
10.5%
100.0%
37.5%
18,663 100.0%
986
5.3%
66,018 100.0%
7,781
11.8%
7,676 100.0%
3,294
42.9%
3,624
195
13,081
2,154
1,690
911
Source: U.S. Census Bureau American Factfinder, American Community Survey 3-year Estimates 2005-2007. The 2005-2007 ACS three-year
estimates are based on data collected between January 2005 and December 2007 and published for selected geographic areas with populations of
20,000 or greater. The data represent the average characteristics over the 3-year period of time. The data was assembled by the Community Health
25
Assessment, Planning and Evaluation (CHAPE) unit of Contra Costa Health Services.
American Community Survey 2005–2007 Summary Table
TOTAL POPULATION
Bay Point
20,374
#
GENDER
Male
Female
AGE
Under 5 years
5 to 9 years
10 to 14 years
15 to 19 years
20 to 24 years
25 to 29 years
30 to 34 years
35 to 39 years
40 to 44 years
45 to 49 years
50 to 54 years
55 to 59 years
60 to 64 years
65 to 69 years
70 to 74 years
75 to 79 years
80 to 84 years
85 years and over
Median age (years) (both sexes)
Male
Female
RACE/ETHNICITY
white
Hispanic or Latino
Black or African American
American Indian and Alaska
Native
Asian
Native Hawaiian and
Other Pacific Islander alone
Some other race
Two or more races
PLACE OF BIRTH
U.S. born
Foreign born
Brentwood
43,750
%
#
Concord
120,737
%
#
%
E
25,6
#
9,956
10,418
48.9%
51.1%
21,170
22,580
48.4%
51.6%
60,545
60,192
50.1%
49.9%
12,0
13,6
1,979
1,667
1,530
1,588
1,522
1,783
1,341
1,854
1,328
1,516
1,168
936
472
731
247
370
137
205
30.7
28.7
32.3
9.7%
8.2%
7.5%
7.8%
7.5%
8.8%
6.6%
9.1%
6.5%
7.4%
5.7%
4.6%
2.3%
3.6%
1.2%
1.8%
0.7%
1.0%
(x)
(x)
(x)
3,582
4,582
4,287
3,139
1,726
1,764
3,445
4,045
4,085
3,295
2,228
1,613
1,441
1,540
1,132
1,045
582
219
34.2
34.2
34.3
8.2%
10.5%
9.8%
7.2%
3.9%
4.0%
7.9%
9.2%
9.3%
7.5%
5.1%
3.7%
3.3%
3.5%
2.6%
2.4%
1.3%
0.5%
(x)
(x)
(x)
7,813
7,212
7,405
7,722
9,338
9,210
8,296
9,446
9,125
10,368
8,554
7,128
5,142
4,446
3,287
2,742
1,938
1,565
36.6
34.9
38.6
6.5%
6.0%
6.1%
6.4%
7.7%
7.6%
6.9%
7.8%
7.6%
8.6%
7.1%
5.9%
4.3%
3.7%
2.7%
2.3%
1.6%
1.3%
(x)
(x)
(x)
1,0
1,4
9
1,0
1,2
1,5
2,1
1,7
2,1
1,6
1,9
2,0
1,6
9
8
9
1,1
1,1
4
4
4
5,990
9,206
2,048
134
29.4%
45.2%
10.1%
0.7%
25,717
11,907
1,834
71
58.8%
27.2%
4.2%
0.2%
66,249
34,365
3,099
160
54.9%
28.5%
2.6%
0.1%
13,0
2,8
2,1
1,500
450
7.4%
2.2%
2,118
402
4.8%
0.9%
11,835
854
9.8%
0.7%
6,2
277
769
1.4%
3.8%
364
1,337
0.8%
3.1%
757
3,418
0.6%
2.8%
3
8
13,765
6,609
67.6%
32.4%
36,151
7,599
82.6%
17.4%
86,225
34,512
71.4%
28.6%
17,1
8,5
26
American Community Survey 2005–2007 Summary Table
TOTAL POPULATION
Bay Point
20,374
#
LANGUAGE (population 5 years and over)
Speak only English at home
9,432
Language other than English at
8,963
home (All)
Spanish
7,385
Asian and Pacific Island
1,336
languages
EDUCATION (population 25 years and over)
No high school diploma
3,181
High school graduate (includes
3,533
equivalency)
Some college, no degree
2,541
Associate's degree
Bachelor's degree
Graduate or prof. degree
Total
Brentwood
43,750
%
#
Concord
120,737
%
#
%
El
25,659
#
51.3%
48.7%
29,718
10,450
74.0%
26.0%
69,575
43,349
61.6%
38.4%
15,40
9,18
40.1%
7.3%
7,536
1,538
18.8%
3.8%
26,699
6,959
23.6%
6.2%
2,18
4,47
26.3%
29.2%
3,570
6,242
13.5%
23.6%
11,778
20,396
14.5%
25.1%
1,30
2,68
21.0%
7,000
26.5%
18,922
23.3%
3,33
976
1,572
285
12,088
8.1%
13.0%
2.4%
100.0%
2,518
5,071
2,033
26,434
9.5%
19.2%
7.7%
100.0%
6,629
16,039
7,483
81,247
8.2%
19.7%
9.2%
100.0%
1,39
5,81
5,42
19,96
20,282
100.0%
43,717
100.0%
119,687
100.0%
24,69
8,451
41.7%
6,043
13.8%
30,620
25.6%
4,78
3,487
4,299
665
52,594
41.3%
50.9%
7.9%
x
2,264
3,097
682
87,068
37.5%
51.2%
11.3%
x
9,099
18,265
3,256
62,831
29.7%
59.7%
10.6%
x
70
3,24
83
77,65
7,347
100.0%
16,260
100.0%
53,268
100.0%
11,71
373
5.1%
681
4.2%
2,582
4.8%
71
14,082
999
100.0%
7.1%
29,088
2,735
100.0%
9.4%
93,360
7,654
100.0%
8.2%
21,48
1,34
3,624
195
13,081
2,154
1,690
911
100.0%
5.4%
100.0%
16.5%
100.0%
53.9%
9,731
793
25,894
2,572
4,518
1,640
100.0%
8.1%
100.0%
9.9%
100.0%
36.3%
16,315
883
82,307
9,201
13,261
5,649
100.0%
5.4%
100.0%
11.2%
100.0%
42.6%
2,60
10
16,79
1,43
4,23
1,40
INCOME & POVERTY
Total (for whom poverty status
is determined)
All ages, below 200% of
federal poverty level
Under 18 years:
18 to 64 years:
65 years and over:
Median household income ($)
EMPLOYMENT
Civilian population 25–64 yrs
old, in labor force
Unemployed
VETERAN STATUS
Civilian population (18 & over)
Civilian veterans
DISABILITY STATUS
Population 5 to 15 years
with any disability
Population 16 to 64 yrs
with any disability
Population 65 yrs and over
with any disability
27
American Community Survey 2005–2007 Summary Table
El Cerrito
25,659
TOTAL POPULATION
#
GENDER
Male
Female
AGE
Under 5 years
5 to 9 years
10 to 14 years
15 to 19 years
20 to 24 years
25 to 29 years
30 to 34 years
35 to 39 years
40 to 44 years
45 to 49 years
50 to 54 years
55 to 59 years
60 to 64 years
65 to 69 years
70 to 74 years
75 to 79 years
80 to 84 years
85 years and over
Median age (years) (both sexes)
Male
Female
RACE/ETHNICITY
White
Hispanic or Latino
Black or African American
American Indian and Alaska
Native
Asian
Native Hawaiian and
Other Pacific Islander alone
Some other race
Two or more races
PLACE OF BIRTH
U.S. born
Foreign born
Hercules
24,156
%
#
Martinez
33,842
%
#
%
O
29,045
#
12,057
13,602
47.0%
53.0%
11,644
12,512
48.2%
51.8%
16,482
17,360
48.7%
51.3%
15,06
13,98
1,071
1,402
915
1,064
1,239
1,519
2,192
1,707
2,168
1,655
1,919
2,046
1,670
964
861
915
1,170
1,182
44.2
41.8
47.1
4.2%
5.5%
3.6%
4.1%
4.8%
5.9%
8.5%
6.7%
8.4%
6.4%
7.5%
8.0%
6.5%
3.8%
3.4%
3.6%
4.6%
4.6%
(x)
(x)
(x)
1,410
1,472
1,330
2,019
1,650
1,432
2,006
1,517
2,000
2,642
2,292
1,434
842
588
472
486
359
205
37.4
34.8
40.2
5.8%
6.1%
5.5%
8.4%
6.8%
5.9%
8.3%
6.3%
8.3%
10.9%
9.5%
5.9%
3.5%
2.4%
2.0%
2.0%
1.5%
0.8%
(x)
(x)
(x)
1,500
1,832
2,050
2,236
1,525
2,330
1,891
2,181
2,954
2,767
3,558
3,085
1,977
1,251
868
892
418
527
42.7
42.6
42.9
4.4%
5.4%
6.1%
6.6%
4.5%
6.9%
5.6%
6.4%
8.7%
8.2%
10.5%
9.1%
5.8%
3.7%
2.6%
2.6%
1.2%
1.6%
(x)
(x)
(x)
2,29
2,85
3,00
2,41
1,81
1,89
2,17
2,23
2,48
2,33
1,41
1,20
1,03
42
49
44
36
15
30
29
31
13,063
2,889
2,155
52
50.9%
11.3%
8.4%
0.2%
4,476
3,378
4,844
-
18.5%
14.0%
20.1%
0.0%
24,384
4,539
948
107
72.1%
13.4%
2.8%
0.3%
15,54
9,81
1,44
4
6,238
-
24.3%
0.0%
10,385
275
43.0%
1.1%
2,418
167
7.1%
0.5%
1,23
363
899
1.4%
3.5%
151
647
0.6%
2.7%
21
1,258
0.1%
3.7%
1
94
17,108
8,551
66.7%
33.3%
15,339
8,817
63.5%
36.5%
29,866
3,976
88.3%
11.7%
24,53
4,51
28
American Community Survey 2005–2007 Summary Table
Hercules
Pittsburg
Pleasant Hill El Cerrito
Richmond
San Pablo
25,659
24,156
TOTAL
POPULATION
62,670
33,980
97,867
31,155
% %
%
#
%
#
%#
#%
% #
#
LANGUAGE (population 5 years and over)
only English
at home
15,400 47,672
62.6% 48.7%11,812
51.9% Speak
30,275
48.3%
16,496
48.5%
15,43051.9%
49.5%
than English
at
9,188 50,195
37.4% 51.3%10,934
48.1% Language
32,395other51.7%
17,484
51.5%
15,72548.1%
50.5%
home (All)
2,185 6,628
8.9% 6.8% 2,2372,276 9.8%
7.9% Spanish
5,570
8.9%
2,115
6.2%
7.3%
and Pacific
Island 2,161
4,476 7,178
18.2% 7.3% 6,7312,00229.6%
9.8% Asian4,538
7.2%
6.4%
6.4%
10.4% languages
4,521
7.2%
1,680
4.9%
7,283
7.4%
2,928
9.4%
25
years and
over) 6,832
8.3% EDUCATION
5,130 (population
8.2%
2,426
7.1%
7.0%
2,121
6.8%
school diploma
1,306 6,711
6.5% 6.9% 1,4212,705 8.7%
6.3% No high
5,737
9.2%
2,144
6.3%
8.7%
2,687 8,077
13.5% 8.3% 2,7202,29116.7%
6.5% High school
4,996 graduate
8.0% (includes
1,896
5.6%
7.4%
7.5% equivalency)
3,667
5.9%
2,314
6.8%
7,721
7.9%
2,622
8.4%
college, no
degree 2,684
3,333 7,212
16.7% 7.4% 3,3953,27320.9%
7.7% Some3,916
6.2%
7.9%
10.5%
1,396 6,222
7.0% 6.4% 1,8221,68711.2%
8.5% Associate's
4,387 degree
7.0%
2,447
7.2%
5.4%
5,818 7,196
29.1% 7.4% 5,3031,62232.6%
8.1% Bachelor's
4,790degree
7.6%
2,701
7.9%
5.2%
degree 2,662
5,428 7,031
27.2% 7.2% 1,6141,938 9.9%
4.9% Graduate
3,693or prof.
5.9%
7.8%
6.2%
19,968 6,184
100.0% 6.3%16,2751,412
100.0%
4.1% Total 3,645
5.8%
2,309
6.8%
4.5%
Oakley
5
60
85
99
53
08
18
19
96
73
36
80
39
14
00
33
27
91
40
66
53
0.6
9.3
1.9
43
13
49
49
35
-
16
40
34
11
INCOME
& POVERTY
3.6%
2,850
4.5%
1,946
1.5% Total (for
1,803
1,503
whom 2.9%
poverty status
1.7% is determined)
1,406
2.2%
767
200% of 770
1.5% All ages,
705 below
1.1%
level
1.3% federal
834poverty
1.3%
605
Under
0.5%
482 18 years:
0.8%
850
1830.9
to 64 years:
(x)
(x)
39
6530.1
years and (x)
over:
(x)
39
household(x)
income ($)
(x) Median31.5
39.1
EMPLOYMENT
population
25–64 23,693
yrs
53.5% Civilian
14,603
23.3%
in labor force
33.8% old, 24,311
38.8%
2,528
Unemployed
5.0%
10,353
16.5%
1,126
VETERAN
STATUS
0.2%
203
0.3%
107
Civilian population (18 & over)
4.3% Civilian
10,319veterans
16.5%
4,727
DISABILITY
0.0%
289 STATUS
0.5%
66
Population 5 to 15 years
0.1% with any
928 disability
1.5%
44
64 yrs
3.2% Population
1,664 16 to2.7%
1,689
with any disability
and over
84.5% Population
42,770 65 yrs
68.2%
26,423
any disability
15.5% with
19,900
31.8%
7,557
5.7%
4.4%
24,691
2.3%
4,784
2.3%
4,271
2,519
100.0%
2,403
19.4%
1,587
1.8%
707
2.5%
3,243
(x)
834
(x)
77,650
(x)
1,680
14.8%
1,132
67.8%
34
17.4%
33.9
34.2 x
4.4%
1,289
4.1%
2.6%24,052 732
2.3%
100.0%
2.5%
759
2.4%
1.6% 2,374 661 9.9%
2.1%
1.7%
360
1.2%
1.2% 633 47726.7%
1.5%
(x) 1,385 3358.3% (x)
(x) 356 31.815.0% (x)
x (x)
(x)88,966 34.1
11,714
69.7%
7.4%
717
3.3%
0.3%
21,488
1,342
13.9%
100.0%
18,941
32,768
6.1%
29,336
38
100.0%
6.2%
14,046
100.0%
19.4%11,5353,521
11.3%
33.5%
16,752
53.8%
608
5.3%
30.0%
4,894
15.7%
0.0%
72
0.2%
18,547
100.0%
14.4% 1,0515,483 5.7%
17.6%
0.2%
145
2,608
100.0%
108
4.1%
0.1%
593
16,793 2,000
100.0%
5.0%
1,434
8.5%
4,239 67,459
100.0%
77.8%
1,402 30,408
33.1%
22.2%
29
0.1%
0.0%
3,053
100.0%
0.6% 219 156 7.2%
0.5%
100.0%
2.0%17,546 277
0.9%
1,289
7.3%
100.0%
68.9% 2,110
18,013
57.8%
31.1% 966
13,14245.8%
42.2%
Martinez
Walnut
Creek
33,842
65,068
# #
%%
29,04
#
27,400
29,967
4,942
35,101
84.7%
46.1%
15.3%
53.9%
19,6
7,1
2,345
2,388
1,040
2,595
7.3%
3.7%
3.2%
4.0%
5,9
5
2,737
4.2%
4,061
6.2%
1,724
7.0%
3,500
5.4%
5,155
3,409 20.9%
5.2%
3,330
5.1%
6,152
3,203 24.9%
4.9%
2,800
4,563 11.3%
7.0%
6,111
4,584 24.7%
7.0%
2,757
5,340 11.2%
8.2%
24,699
5,146 100.0%
7.9%
3,842
5.9%
3,245 100.0%
5.0%
32,759
3,651
5.6%
4,651
2,855 14.2%
4.4%
3,083
4.7%
1,246
3,536 26.8%
5.4%
2,654
48.1 57.1%
(x)
751
45.9 16.1%
(x)
73,668
x
50
(x)
16,392
50,111 100.0%
77.0%
4,730
7.3%
771
4.7%
1,122
1.7%
127
0.2%
27,041 100.0%
3,033
7,730 11.2%
11.9%
54
0.1%
4,148 100.0%
285
6.9%
170
0.3%
23,437
1,024 100.0%
1.6%
2,428
10.4%
3,674 100.0%
52,093
80.1%
1,243
33.8%
12,975
19.9%
2,7
5,3
4,5
1,7
1,8
3
16,6
28,6
6,0
2,3
2,9
7
72,7
11,7
3
19,2
1,6
6,4
4
18,3
2,1
1,8
8
American Community Survey 2005–2007 Summary Table
Oakley
29,045
TOTAL POPULATION
#
GENDER
Male
Female
AGE
Under 5 years
5 to 9 years
10 to 14 years
15 to 19 years
20 to 24 years
25 to 29 years
30 to 34 years
35 to 39 years
40 to 44 years
45 to 49 years
50 to 54 years
55 to 59 years
60 to 64 years
65 to 69 years
70 to 74 years
75 to 79 years
80 to 84 years
85 years and over
Median age (years) (both sexes)
Male
Female
RACE/ETHNICITY
White
Hispanic or Latino
Black or African American
American Indian and Alaska
Native
Asian
Native Hawaiian and
Other Pacific Islander alone
Some other race
Two or more races
PLACE OF BIRTH
U.S. born
Foreign born
Pittsburg
62,670
%
#
Pleasant Hill
33,980
%
#
%
Ric
97,867
#
15,060
13,985
51.9%
48.1%
30,275
32,395
48.3%
51.7%
16,496
17,484
48.5%
51.5%
47,67
50,19
2,299
2,853
3,008
2,418
1,819
1,896
2,173
2,236
2,480
2,339
1,414
1,200
1,033
427
491
440
366
153
30.6
29.3
31.9
7.9%
9.8%
10.4%
8.3%
6.3%
6.5%
7.5%
7.7%
8.5%
8.1%
4.9%
4.1%
3.6%
1.5%
1.7%
1.5%
1.3%
0.5%
(x)
(x)
(x)
5,570
4,538
4,521
5,130
5,737
4,996
3,667
3,916
4,387
4,790
3,693
3,645
2,850
1,803
1,406
705
834
482
30.9
30.1
31.5
8.9%
7.2%
7.2%
8.2%
9.2%
8.0%
5.9%
6.2%
7.0%
7.6%
5.9%
5.8%
4.5%
2.9%
2.2%
1.1%
1.3%
0.8%
(x)
(x)
(x)
2,115
2,161
1,680
2,426
2,144
1,896
2,314
2,684
2,447
2,701
2,662
2,309
1,946
1,503
767
770
605
850
39
39
39.1
6.2%
6.4%
4.9%
7.1%
6.3%
5.6%
6.8%
7.9%
7.2%
7.9%
7.8%
6.8%
5.7%
4.4%
2.3%
2.3%
1.8%
2.5%
(x)
(x)
(x)
6,62
7,17
7,28
6,83
6,71
8,07
7,72
7,21
6,22
7,19
7,03
6,18
4,27
2,51
2,40
1,58
1,68
1,13
3
33
34
15,543
9,813
1,449
49
53.5%
33.8%
5.0%
0.2%
14,603
24,311
10,353
203
23.3%
38.8%
16.5%
0.3%
23,693
2,528
1,126
107
69.7%
7.4%
3.3%
0.3%
18,94
32,76
29,33
3
1,235
-
4.3%
0.0%
10,319
289
16.5%
0.5%
4,727
66
13.9%
0.2%
14,04
14
16
940
0.1%
3.2%
928
1,664
1.5%
2.7%
44
1,689
0.1%
5.0%
59
2,00
24,534
4,511
84.5%
15.5%
42,770
19,900
68.2%
31.8%
26,423
7,557
77.8%
22.2%
67,45
30,40
30
American Community Survey 2005–2007 Summary Table
chmond
San Pablo
7
TOTAL 31,155
POPULATION
%
#
%
72
95
28
78
83
32
11
77
21
12
22
96
31
84
71
19
03
87
80
32
34
3.9
4.2
41
68
36
38
46
45
93
00
59
08
Walnut Creek
Oakley
65,068
29,045
#
%
#
%
LANGUAGE (population 5 years and over)
48.7%
15,430
49.5%
46.1%
Speak only
English
at home 29,967 19,609
73.3%
51.3%
15,725
50.5%
35,101
53.9%
Language other than English at
7,137
26.7%
home (All)
6.8%
7.3%
2,388
3.7%
Spanish 2,276
5,995
22.4%
7.3%
2,002
6.4%
2,595
4.0%
Asian and Pacific Island
541
2.0%
7.4%
2,928
9.4%
2,737
4.2%
languages
7.0%
2,121 (population
6.8% 25 4,061
EDUCATION
years and6.2%
over)
6.9%
2,705 diploma
8.7%
3,500
5.4%
No high school
2,761
16.6%
8.3%
2,291
7.4%
5.2%
High school
graduate
(includes3,409
5,337
32.1%
equivalency)
7.9%
2,622
8.4%
3,330
5.1%
Some college,
degree
4,599
27.6%
7.4%
3,273 no 10.5%
3,203
4.9%
Associate's
degree5.4%
1,701
10.2%
6.4%
1,687
4,563
7.0%
Bachelor's
degree 5.2%
1,854
11.1%
7.4%
1,622
4,584
7.0%
Graduate1,938
or prof. degree
396
2.4%
7.2%
6.2%
5,340
8.2%
Total
100.0%
6.3%
1,412
4.5%
5,146 16,648
7.9%
4.4%
1,289
4.1%
3,842
5.9%
INCOME &
POVERTY
2.6%
732 poverty
2.3%status3,245 28,607
5.0%
Total (for whom
100.0%
2.5%
759
2.4%
3,651
5.6%
is determined)
1.6%All ages,661
2.1% of
2,855
4.4%
below 200%
6,004
21.0%
1.7%federal poverty
360
1.2%
3,083
4.7%
level
1.2% Under477
1.5%
3,536
5.4%
18 years:
2,313
38.5%
(x) 18 to 64
33years: (x)
48.1
(x)
2,919
48.6%
(x) 65 years
31.8 and over:
(x)
45.9
(x)
772
12.9%
(x)
34.1
(x)
50
(x)
Median household income ($)
72,756
x
EMPLOYMENT
19.4%
3,521
11.3%
Civilian population
25–64 yrs50,111
old, in labor
force 53.8%
33.5%
16,752
4,730
30.0%Unemployed
4,894
15.7%
1,122
VETERAN STATUS
0.0%
72
0.2%
127
Civilian population (18 & over)
14.4%Civilian
5,483
17.6%
7,730
veterans
0.1%
0.0%
54
DISABILITY STATUS
Population 5 to 15 years
0.6%with any156
disability0.5%
2.0%
Population277
16 to 640.9%
yrs
77.0%
11,707
7.3%
344
1.7%
0.2%
19,217
11.9%
1,608
0.1%
170
1,024
6,471
0.3%
433
1.6%
18,313
with any disability
68.9%
18,013
Population
65 yrs 57.8%
and over 52,093
31.1%with any
13,142
42.2%
12,975
disability
2,145
80.1%
1,877
19.9%
814
Pittsburg
62,670
%
Rich
97,867
#
%
#
30,887
26,213
54.1%
45.9%
24,207
7,658
76.0%
24.0%
50,893
40,346
17,661
5,735
30.9%
10.0%
1,921
3,176
6.0%
10.0%
26,707
9,146
9,228
10,542
24.8%
28.4%
1,480
3,817
6.3%
16.3%
13,341
16,510
8,578
3,081
4,228
1,517
37,174
23.1%
8.3%
11.4%
4.1%
100.0%
5,851
2,003
6,859
3,444
23,454
24.9%
8.5%
29.2%
14.7%
100.0%
13,296
4,404
10,498
5,186
63,235
62,247
100.0%
33,958
100.0%
95,177
20,531
33.0%
4,787
14.1%
34,825
8,271
11,156
1,104
56,333
40.3%
54.3%
5.4%
x
955
2,971
861
80,737
19.9%
62.1%
18.0%
x
12,249
20,003
2,573
50,346
100.0%
22,595
100.0%
15,179
100.0%
40,160
2.9%
1,512
6.7%
598
3.9%
3,334
100.0%
8.4%
44,847
3,900
100.0%
8.7%
26,648
2,760
100.0%
10.4%
72,520
5,020
100.0%
6.7%
100.0%
11.7%
100.0%
43.4%
10,071
750
41,677
6,325
4,987
1,918
100.0%
7.4%
100.0%
15.2%
100.0%
38.5%
4,384
149
22,958
2,036
4,495
1,882
100.0%
3.4%
100.0%
8.9%
100.0%
41.9%
15,918
888
63,811
8,469
9,229
4,922
31
#
Pleasant Hill
33,980
American Community Survey 2005–2007 Summary Table
Richmond
97,867
TOTAL POPULATION
#
GENDER
Male
Female
AGE
Under 5 years
5 to 9 years
10 to 14 years
15 to 19 years
20 to 24 years
25 to 29 years
30 to 34 years
35 to 39 years
40 to 44 years
45 to 49 years
50 to 54 years
55 to 59 years
60 to 64 years
65 to 69 years
70 to 74 years
75 to 79 years
80 to 84 years
85 years and over
Median age (years) (both sexes)
Male
Female
RACE/ETHNICITY
White
Hispanic or Latino
Black or African American
American Indian and Alaska
Native
Asian
Native Hawaiian and
Other Pacific Islander alone
Some other race
Two or more races
PLACE OF BIRTH
U.S. born
Foreign born
San Pablo
31,155
%
#
Walnut Creek
65,068
%
#
%
47,672
50,195
48.7%
51.3%
15,430
15,725
49.5%
50.5%
29,967
35,101
46.1%
53.9%
6,628
7,178
7,283
6,832
6,711
8,077
7,721
7,212
6,222
7,196
7,031
6,184
4,271
2,519
2,403
1,587
1,680
1,132
34
33.9
34.2
6.8%
7.3%
7.4%
7.0%
6.9%
8.3%
7.9%
7.4%
6.4%
7.4%
7.2%
6.3%
4.4%
2.6%
2.5%
1.6%
1.7%
1.2%
(x)
(x)
(x)
2,276
2,002
2,928
2,121
2,705
2,291
2,622
3,273
1,687
1,622
1,938
1,412
1,289
732
759
661
360
477
33
31.8
34.1
7.3%
6.4%
9.4%
6.8%
8.7%
7.4%
8.4%
10.5%
5.4%
5.2%
6.2%
4.5%
4.1%
2.3%
2.4%
2.1%
1.2%
1.5%
(x)
(x)
(x)
2,388
2,595
2,737
4,061
3,500
3,409
3,330
3,203
4,563
4,584
5,340
5,146
3,842
3,245
3,651
2,855
3,083
3,536
48.1
45.9
50
3.7%
4.0%
4.2%
6.2%
5.4%
5.2%
5.1%
4.9%
7.0%
7.0%
8.2%
7.9%
5.9%
5.0%
5.6%
4.4%
4.7%
5.4%
(x)
(x)
(x)
18,941
32,768
29,336
38
19.4%
33.5%
30.0%
0.0%
3,521
16,752
4,894
72
11.3%
53.8%
15.7%
0.2%
50,111
4,730
1,122
127
77.0%
7.3%
1.7%
0.2%
14,046
145
14.4%
0.1%
5,483
-
17.6%
0.0%
7,730
54
11.9%
0.1%
593
2,000
0.6%
2.0%
156
277
0.5%
0.9%
170
1,024
0.3%
1.6%
67,459
30,408
68.9%
31.1%
18,013
13,142
57.8%
42.2%
52,093
12,975
80.1%
19.9%
32
American Community Survey 2005–2007 Summary Table
TOTAL POPULATION
Richmond
97,867
#
LANGUAGE (population 5 years and over)
Speak only English at home
50,893
Language other than English at
40,346
home (All)
Spanish
26,707
Asian and Pacific Island
9,146
languages
EDUCATION (population 25 years and over)
No high school diploma
13,341
High school graduate (includes
16,510
equivalency)
Some college, no degree
13,296
Associate's degree
4,404
Bachelor's degree
10,498
Graduate or prof. degree
5,186
Total
63,235
San Pablo
31,155
%
#
Walnut Creek
65,068
%
#
%
55.8%
44.2%
10,244
18,635
35.5%
64.5%
48,500
14,180
77.4%
22.6%
29.3%
10.0%
14,053
3,334
48.7%
11.5%
3,477
4,708
5.5%
7.5%
21.1%
26.1%
5,416
6,996
28.3%
36.6%
1,991
7,221
4.0%
14.5%
21.0%
7.0%
16.6%
8.2%
100.0%
2,649
1,177
2,179
706
19,123
13.9%
6.2%
11.4%
3.7%
100.0%
9,551
3,331
15,762
11,931
49,787
19.2%
6.7%
31.7%
24.0%
100.0%
95,177
100.0%
30,443
100.0%
64,669
100.0%
34,825
36.6%
12,233
40.2%
8,282
12.8%
12,249
20,003
2,573
50,346
35.2%
57.4%
7.4%
x
4,430
7,029
774
46,326
36.2%
57.5%
6.3%
x
1,086
4,457
2,739
76,522
13.1%
53.8%
33.1%
x
40,160
100.0%
11,744
100.0%
26,775
100.0%
3,334
8.3%
1,004
8.5%
837
3.1%
72,520
5,020
100.0%
6.9%
22,385
1,148
100.0%
5.1%
54,646
6,012
100.0%
11.0%
15,918
888
63,811
8,469
9,229
4,922
100.0%
5.6%
100.0%
13.3%
100.0%
53.3%
5,799
74
19,971
2,344
2,623
806
100.0%
1.3%
100.0%
11.7%
100.0%
30.7%
6,450
138
39,747
3,359
16,060
5,760
100.0%
2.1%
100.0%
8.5%
100.0%
35.9%
INCOME & POVERTY
Total (for whom poverty status
is determined)
All ages, below 200% of
federal poverty level
Under 18 years:
18 to 64 years:
65 years and over:
Median household income ($)
EMPLOYMENT
Civilian population 25–64 yrs
old, in labor force
Unemployed
VETERAN STATUS
Civilian population (18 & over)
Civilian veterans
DISABILITY STATUS
Population 5 to 15 years
with any disability
Population 16 to 64 yrs
with any disability
Population 65 yrs and over
with any disability
Source: U.S. Census Bureau American Factfinder, American Community
33Survey 3-year Estimates 2005-2007. The 2005-2007 ACS three-year
estimates are based on data collected between January 2005 and December 2007 and published for selected geographic areas with populations
of 20,000 or greater. The data represent the average characteristics over the 3-year period of time. The data were assembled by the Community
Health Assessment, Planning and Evaluation (CHAPE) unit of Contra Costa Health Services.
HEALTH INEQUITIES
Health Inequities
Introduction
We think of health as a product of our genes, lifestyle choices, and medical services, but the social,
economic and community environments also have profound impacts on our health.1 According to
University of California, San Francisco professor Paula Braverman, a person’s health is not only a product
of good medical care and genes; health and the likelihood of becoming sick and dying prematurely
are greatly influenced by powerful social factors such as levels of education and income.1 Income and
educational attainment, however, do not fully explain health disparities. Race and ethnicity, while
strongly linked to education and income, have their own influence on health outcomes. Race and
socioeconomic status (a combined measure of income and educational attainment), independently
and jointly, contribute to health inequities in the United States.1
The influence of income, education and race/ethnicity on health is evident in Contra Costa, a diverse
county with wide variation in these factors across communities. These differences contribute to major
health inequities, with residents of low-income and poorly educated communities and African American
residents experiencing worse health outcomes and dramatically lower life expectancy. This section
illustrates health disparities and inequities based on income, education and race/ethnicity in Contra
Costa, and begins to explore the interplay and distribution of these factors in our county.
Poverty was associated with poorer health status
and shorter life expectancy among Contra Costa residents.
In Contra Costa, greater wealth equated to better health and longer life. Among adults 25 years of age
and older, 8.4% of those with household incomes at or above 300% of the federal poverty level (FPL)
reported “fair” or “poor” health status compared to almost one-third (29.5%) of those living below
200% of the FPL. Self-reported health as poor, fair, good, very good or excellent is considered a reliable
indicator of health status.1
FIGURE 1
34
A child born in a low-poverty area (all census tracts with less than 10% of households living below 200%
of federal poverty level) in 2000 could expect to live more than six years longer than a child born in a
high-poverty area (all census tracts with more than 30% of households living below 200% of federal
poverty level). Life expectancy in low-poverty areas was 81.4 years and 74.9 years in high-poverty areas.
Life Expectancy in Contra Costa by Poverty, 2000
81.4
79.8
77.7
74.9
Less than 10% of census tract <
2xFPL
10 - 19.9% of census tract < 2xFPL 20 - 29.9% of census tract < 2xFPL
30% or more of census tract <
2xFPL
FIGURE 2
Individual poverty and neighborhood poverty have been associated with poorer health outcomes.
Poverty limits access to health-promoting resources such as healthy foods, safe recreation areas, and
clean air and water.2 American adults living in poverty experience considerably worse health on average
than their more affluent peers. Health differences across income groups are seen in a range of health
conditions throughout the life course. American adults in families with incomes below the federal
poverty level are more likely to be diagnosed with diabetes or coronary artery disease and be limited
in their activity by a chronic disease than those living above the poverty level.1 Living in high-poverty
neighborhoods increases exposure to environmental conditions that threaten health such as crime
and air pollution.2
Lower educational attainment was associated with poorer health
and shorter life expectancy among Contra Costa residents.
In Contra Costa, only 5.3% of adults age 25 years and older with at least a master’s degree and 7.8% of
those with a bachelor’s degree or some graduate training reported that their health status was “fair” or
“poor” compared to 22.6% of residents with a high school diploma or less education.
35
FIGURE 3
A child born in a high-education area in Contra Costa (i.e., all census tracts with less than 5% of
residents with less than a high school diploma) in 2000 could expect to live more than seven years
longer than a child born in a low-education area (all census tracts with 25% or more residents with
less than a high school diploma). Life expectancy in high-education areas in the county was 82.0 years
compared to 74.6 years in low-education areas.
Life Expectancy in Contra Costa by Education, 2000
82.0
80.0
77.3
74.6
Less than 5% of census tract < HS
5 - 14.9% of census tract < HS
15 - 24.9% of census tract < HS
25% or more of census tract < HS
FIGURE 4
People with more education are likely to live longer and experience better health outcomes. A large
body of evidence links education with health, even when factors like income are taken into account.3
Research suggests that higher educational attainment can impact health in a variety of ways. More
36
education can increase health knowledge and healthy behaviors, such as exercising regularly, refraining
from smoking, and obtaining timely health care check-ups and screenings. Highly educated people
have better employment opportunities with healthier working conditions and greater likelihood of
employer-based health care. Better employment opportunities often result in higher income, which
in turn is linked to improved social and psychological factors that affect health and directly to better
health as shown in Figures 1 and 2.3
African American residents in Contra Costa had a shorter life expectancy
than other county residents.
African Americans in Contra Costa had a shorter life expectancy (73.1 years) than any other racial/
ethnic group in the county. An Asian/Pacific Islander or Hispanic baby born between 2005 and 2007
in Contra Costa could expect to live more than five years longer than a white baby born at the same
time and more than 12 years longer than an African American baby born at the same time.
Life Expectancy in Contra Costa by Race, 2005- 2007
86.0
85.7
80.4
73.1
Asian Pacific Islander
Hispanic
White
African American
FIGURE 5
On average, African Americans experience disability earlier in life and die sooner than others in the
United States. While African Americans are generally poorer, have less education, and are employed in
lower status occupations than are European Americans, they have relatively worse health outcomes even
at the same level or higher on the socioeconomic ladder. This suggests that there is an added burden of
race, independent of its effect on socioeconomic status. Although race affects health largely through its
effects on income and education, additional effects beyond socioeconomic disadvantage are present.4
37
DISTRIBUTION OF SOCIAL FACTORS:
INCOME, EDUCATION & RACE/ETHNICITY
When compared with the state or the nation on income and education, Contra Costa County compares
favorably, but looking at the county as a whole masks the vast differences in experience of the county’s
more than 1 million residents. The median household income in Contra Costa in 2009 was $75,139
compared to just $58,931 in California and $50,221 in the United States. Similarly, Contra Costa had
a greater percentage of college graduates (37.6%) than the state (29.9%) or nation (27.9%) in 2009.
Within the county, however, distribution of income and education is not uniform and this unequal
distribution is echoed in disparities in health outcomes.
Income level varies widely across the county.
Even within a relatively affluent county like Contra Costa there are pockets of extreme poverty. In 2009,
23.3% of the county’s population lived below 200% of the federal poverty threshold. (The average federal
poverty threshold for 2009 was $21,954 for a family of four.) The map below shows the distribution
of poverty in the county by census tract in 2000, with red indicating high rates of poverty and green
denoting the more affluent areas.
Map 1. Contra Costa County Poverty by Census Tract 2000
The share of total income among households in the county is a key measure of income inequality. If
Contra Costa households were divided into quintiles by income in 2009, the lowest quintile (20% of
all households) made less than $30,839. The second made between $30,839 and $59,455; the third
between $59,456 and $92,781; the fourth between $92,782 and $145,075; and the highest made more
than $145,075.
38
In 2009, the poorest 20% of Contra Costa households based on income (i.e., those with less than
$30,839 in household income) earned only 3.5% of total household income in Contra Costa. The
wealthiest 20% of households (those with incomes of more than $145,075) earned almost half of all
income in the county (49.2%); this group earned approximately 14 times the income of the poorest
group. Figure 7 shows the percentage of total household income earned by each quintile of the county
population. Although the difference is most extreme between the poorest and wealthiest households,
even the 20% of households with $59,456 to $92,781 in income got less than 20% of total household
income in the county.
Percent of Housholds by Income
Contra Costa 2009
20%
Share of Total Household Income
Contra Costa 2009
3.5%
20%
15.0%
HH inco me <= $ 30,838
20%
20%
HH inco me $ 30,839 to
$ 59,455
HH inco me $ 59,456 to
$ 92,781
HH inco me $ 92,782 to
$ 145,075
HH inco me >$ 145,075
9.0%
HH inco me <= $ 30,838
HH inco me $ 30,839 to $ 59,455
49.2%
HH inco me $ 59,456 to $ 92,781
HH inco me $ 92,782 to $ 145,075
23.2%
HH inco me >$ 145,075
20%
FIGURE 6
FIGURE 7
Many households in Contra Costa
did not earn enough to achieve self-sufficiency.
Although differences in earnings and poverty provide some information about financial disparities in
Contra Costa, they do not fully illustrate the number of households that struggle to survive financially.
The federal poverty standards, which were developed in the 1960s, are based solely on food costs and
assume that a family’s budget is three times its food costs.5 The Self-Sufficiency Standard was developed to
provide a more accurate, nuanced and up-to-date measure of the income required to survive financially.
It is based on family size and composition and measures how much income is needed for different
family types living in a particular county to adequately meet minimal, basic needs including housing,
food, child care, out-of-pocket medical expenses, transportation and other necessary spending. The
standard is a very conservative budget and includes nothing for restaurant food, savings, emergency
funds, or credit card or loan payments.5
In 2008, the poorest 20% of households in Contra Costa (i.e., those earning less than $31,610) did
not have enough income to achieve self-sufficiency for even a family of two. The 2008 Self-Sufficiency
Standard for a family of two ranged from $32,687 for two adults to $44,272 for one adult and a
preschool-aged child. Since the Self-Sufficiency Standard was as high as $58,872 for a family of three
and up to $87,760 for a family of four, even households with higher incomes may not have met the
Self-Sufficiency Standard.
39
Education likewise varies widely across the county.
In 2009, more than half of Contra Costa adults age 25 years and older had completed at least some
college and more than one-third had a bachelor’s or more advanced degrees: some college, including
those with an associate’s degree (30.0%), bachelor’s degree (24.5%), master’s or professional degree
(13.1%). Only 11.8% of county residents had less than a high school diploma.
However, in some census tracts throughout the county more than 25% of the adult population has
less than a high school diploma. Map 2 shows the distribution of educational attainment by census
tract in 2000, with red indicating areas with a high concentration of low-education adults (i.e., 25%
or more residents with less than a high school diploma) and green denoting a low concentration of
low-education adults (i.e., less than 5% of residents with less than a high school diploma).
Map 2. Contra Costa County Educational Attainment by Census Tract 2000
Racial/ethnic groups are widely but unevenly distributed
throughout the county.
Contra Costa is a racially and ethnically diverse county. In 2009, whites made up 49.7% of the county,
followed by Hispanics (23.2%), Asians/Pacific Islanders (14.2%) and African Americans (9.0%). The
distribution of different racial/ethnic groups, however, was not uniform across the county. Certain
racial and ethnic groups are concentrated in certain areas.
40
Map 3. Contra Costa County White Population by Census Tract 2000
Map 4. Contra Costa County Hispanic Population by Census Tract 2000
41
Map 5. Contra Costa Asian/Pacific Islander Population by Census Tract 2000
Map 6. Contra Costa County African American Population by Census Tract 2000
42
RELATIONSHIP BETWEEN SOCIAL FACTORS
Low educational attainment is associated with
greater poverty and lower earnings.
Contra Costa residents with more education were less likely to live below the federal poverty level
and earned more than less-educated residents. In 2009, almost 17% of residents with less than a high
school diploma lived below poverty compared to only 3.1% of those with a bachelor’s degree or higher
education. The percent of county residents living below the federal poverty level was lower with each
increase in educational attainment. County residents with higher educational attainment also earned
more than less-educated residents during this time. The median earnings for those with less than a
high school diploma was $21,766 compared to $78,366 for those with a graduate or professional degree.
Median earnings increased significantly with each increase in educational attainment.
Percent of Adults 25 Years & Older Living Below Poverty,
by Education Contra Costa 2009
20%
16.9%
15%
11.0%
10%
6.6%
5%
3.1%
0%
Less than high
school diploma
High school
graduate (includes
equivalency)
FIGURE 8
43
Some college,
Bachelor's degree or
associate's degree
higher
Median Earnings of Adults 25 years & older
Contra Costa 2009
$80,000
$60,748
$60,000
$40,000
$20,000
$78,366
$41,466
$21,766
$29,752
$0
Less than
high school
diploma
High school
graduate
(includes
equivalency)
Some
college or
associate's
degree
Bachelor's
degree
Graduate or
professional
degree
FIGURE 9
Low-education households in Contra Costa did not earn enough to achieve self-sufficiency. The
percent of households with inadequate income to achieve self-sufficiency in the county in 2007 varied
by educational attainment: less than a high school diploma (61.8%); high school graduates (35.5%);
some college (20.0%); and bachelor’s degree or higher (8.2%).5
The relationship between education and poverty
also existed at a city level.
Geographic differences in health often reflect underlying differences in income, education and racial or
ethnic composition in those regions.1 From 2006-2008, cities in Contra Costa with a greater percentage
of residents who had less than a high school diploma also had a greater percentage of residents with
incomes less than 200% of the federal poverty level.
From 2006–2008, six cities in Contra Costa had lower educational attainment and higher poverty than
the county overall. San Pablo, Bay Point, Pittsburg, Richmond, Antioch and Concord had a higher
percentage of residents who did not achieve a high school diploma and had incomes less than 200%
of the federal poverty level compared to the county overall. Five cities had both higher educational
attainment and lower poverty than the county overall. Lafayette, Walnut Creek, Pleasant Hill, Martinez
and Hercules had a lower percentage of residents with less than a high school diploma and with incomes
less than 200% of federal poverty compared to county residents overall. Information about the varied
racial composition for each of these cities is available in the American Community Survey table at the
beginning of this report.
44
Percent of Residents 25 Years & Older with Less Than a High
School Diploma, 2006-2008
35%
33.0%
29.4%
30%
25%
20.7%
20%
15.0%
15%
17.5%
11.9%
10%
5%
16.3%
23.2%
3.9%
2.3%
5.2% 5.3%
6.7%
7.8%
tts
bu
rg
Ba
y
Po
in
t
Sa
n
Pa
bl
o
on
d
Pi
ey
hm
Ri
c
O
ak
l
La
fa
ye
W
tte
al
nu
tC
re
ek
Pl
ea
sa
nt
H
ill
El
C
er
rit
o
M
ar
t in
ez
He
rc
ul
es
Br
en
tw
oo
d
Co
nc
or
d
An
tio
ch
0%
FIGURE 10
Percent of Residents with Income Less Than 200% Federal Poverty
2006-2008
50%
42.8%
40%
34.5%
30%
44.7%
37.2%
25.9% 26.4%
22.5%
20%
11.2% 11.8%
10%
13.5% 14.2%
16.6%
18.6%
6.8%
ey
Co
nc
or
d
An
tio
ch
Pi
tts
bu
rg
Ri
ch
m
on
d
Sa
n
Pa
bl
o
Ba
y
Po
in
t
O
ak
l
La
fa
ye
tte
He
rc
ul
W
es
al
nu
tC
re
ek
Br
en
tw
oo
Pl
d
ea
sa
nt
H
ill
M
ar
t in
ez
El
C
er
rit
o
0%
FIGURE 11
The distribution of income is not equal across all
racial/ethnic groups in the county.
In 2009, the median household income in Contra Costa was $75,139 and 9.6% of residents were living
in poverty. Black/African American and Hispanic/Latino residents of Contra Costa earned less and had
higher rates of poverty than white and Asian residents. The income gap was greatest between blacks/
African Americans and whites (a difference of $36,212) followed by Hispanic/Latinos and whites (a
45
difference of $34,611). Almost one in five (19.1%) blacks/African Americans and about one in seven
Hispanics/Latinos (14.8%) were living in poverty compared to about one in 17 whites (6.0%).
Median HH Income by Race/Ethnicity
Contra Costa 2009
$90,000
$80,000
$83,983
$86,185
Asian
White
$70,000
$60,000
$49,973
$51,574
Black/African
American
Hispanic/Latino
$50,000
$40,000
$30,000
$20,000
$10,000
$0
FIGURE 12
FIGURE
Figure
13 13
In 2007, the percent of households with inadequate income to achieve self-sufficiency in the county
also varied by race/ethnicity: Latino (42.0%), black/African American (37.0%), Asian/Pacific Islander
(16.5%) and white (12.4%).5
The distribution of education is not equal across
all racial/ethnic groups in the county.
Educational attainment also varied by race/ethnicity. Hispanic and African American residents were
generally less educated and white and Asian residents were more educated. In 2009, Hispanics/Latinos
had the highest percentage of adults 25 years and older with less than a high school diploma (34.6%).
Hispanics/Latinos also had the lowest percentage of bachelor’s and more advanced degrees (11.8%)
46
followed by blacks/African Americans (23.7%). Asians had the highest percentage of bachelor’s and
more advanced degrees (53.9%) followed by whites (44.5%).
Educational Attainment
Educational Attainment
Black/African American Adults 25 years & older, Contra
Costa 2009
Hispanic/Latino Adults 25 years & older, Contra Costa 2009
11.8%
10.7%
23.7%
Less than high school diploma
Less than high school diploma
34.6%
High school graduate (includes
equivalency)
23.0%
25.4%
Some college or associate's
degree
High school graduate (includes
equivalency)
Some college or associate's degree
Bachelor's degree and above
Bachelor's degree and above
40.2%
30.5%
Educational Attainment
Educational Attainment
White Adults 25 years & older, Contra Costa 2009
Asian Adults 25 years & older, Contra Costa 2009
4.7%
11.1%
Less than high school diploma
18.9%
Less than high school diploma
11.6%
High school graduate (includes
equivalency)
High school graduate (includes
equivalency)
44.5%
Some college or associate's
degree
Some college or associate's
degree
53.9%
23.4%
Bachelor's degree and above
Bachelor's degree and above
31.9%
FIGURE 14
Conclusion
Poverty, education and race/ethnicity play an important role in determining life expectancy and other
health outcomes for Contra Costa residents. Each factor explored in this section impacts the others
and has its own effect on health. The relationship between race and life expectancy cannot be fully
explained by differences in income and education. Clearly, the experience of race and ethnicity over
the life course of people in our communities, as well as education and income, has a profound impact
on health.
In most of this report, data for key health indicators are presented for the county overall and by gender,
race/ethnicity and city. Although these sub-county analyses of the data can be useful for identifying
populations that are most impacted by various health issues, they do not identify all of the underlying
factors that influence health disparities. We need to develop a better understanding of how income,
education, ethnicity and other factors lead to health inequities so that we can work as a community
to improve the health of all our residents and to ensure that every child born has an opportunity for
a long and healthful life.
47
Data Sources: Health Inequities
text
1.
2.
3.
4.
5.
Braverman P, Egerter S. et al (2008) Overcoming Obstacles to Health. Robert Wood Johnson Foundation.
Alameda County Public Health Department (2008), Life and Death from Unnatural Causes. Health and Social
Inequity in Alameda County. August 2008.
Robert Wood Johnson Foundation. (2009) Issue Brief 6: Education and Health, Commission to Build a Healthier
America.
Adler N, Stewart J, et al. Reaching for a Healthier Life – Facts on Socioeconomic Status and Health in the U.S. The
John D. and Catherine T. MacArthur Foundation.
Pearce et al. (2009) Overlook and Undercounted 2009: Struggling to Make Ends Meet in California. Diane Pearce and
United Way of the Bay Area, December 2009.
figures
Figures 1,3. Self-reported health status data from the California Health Interview Survey. Retrieved 12/2/10. For selfreported health, respondents were asked: “In general, would you say your health is excellent, very good, good, fair or
poor?” For educational attainment, respondents were asked: “What is the highest grade of education you have completed
and received credit for?”
Figures 2, 4. Census tract demographic data from the 2000 Census. Death data from the Death Address and Death
Statistical Master files, 1999-2001, California Department of Public Health.
Figure 5. Death Statistical Master file, 2005-2007, California Department of Public Health.
Figures 6–7. Quintile data from the 2009 American Community Survey 1-Year Estimates, File B19080: Household income
quintile upper limits and File B19082: Shares of aggregate household income by quintile, retrieved 12/1/10.
Figure 8. Poverty status by educational attainment data from the 2009 American Community Survey 1-Year Estimates, File
C17003: Poverty status in the past 12 months of individuals by educational attainment among the population 25 years and
older for whom poverty status is determined. Retrieved 11/6/10.
Figure 9. Median earnings by educational attainment from the 2009 American Community Survey 1-Year Estimates, File
B20004: Median earnings in the past 12 months (in 2009 inflation-adjusted dollars) by sex by educational attainment for
the population 25 years and older among those 25 years and older with earnings, retrieved 11/3/10.
Figure 10. Educational attainment by city data from the 2006-2008 American Community Survey 3-Year Estimates, File
C15002: Sex by educational attainment for the population 25 years and older.
Figure 11. Percent below 200% of federal poverty level by city data from the 2006-2008 American Community Survey
3-Year Estimates, File C17002: Ratio of income to poverty level in the past 12 months among the population for whom
poverty status is determined, retrieved 12/1/10.
Figure 12. Median household income by race/ethnicity data from the 2009 American Community Survey 1-Year
Estimates, File S0201: Selected population profile in the United States using income in the past 12 months (in 2009
inflation-adjusted dollars). Retrieved 11/16/10.
Figure 13. Poverty by race/ethnicity data from the 2009 American Community Survey 1-Year Estimates, File S0201:
Selected population profile in the United States. Retrieved 11/16/10.
48
Figure 14. Educational attainment by race/ethnicity data from the 2009 American Community Survey 1-Year Estimates,
File S0201: Selected population profile in the United States. Retrieved 11/16/10.
maps
Map 1-3: Census tract level poverty, education and race/ethnicity data from the 2000 Census.
Note: Throughout this section, data presented for Hispanics/Latinos include Hispanic residents of any race.
Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic residents.
49
LEADING CAUSES OF DEATH
Leading Causes of Death
Contra Costa and California
Cancer, heart disease and stroke were the most common
causes of death in Contra Costa County.
• Heart disease and cancer accounted for roughly half
of all deaths in Contra Costa and California.
• Contra Costa residents were more likely to die from
homicide compared to California residents.
Between 2005–2007, there were 20,515 deaths among Contra Costa residents. This means that on
average 6,838 county residents died each year. Contra Costa’s age-adjusted death rate from all causes
was significantly lower (651.2 per 100,000) than California’s age-adjusted rate (754.6 per 100,000).
The top 10 leading causes accounted for a full 77.2% of the deaths in Contra Costa County and 79.5%
of the deaths in California. The top four leading causes of death (cancer, heart disease, stroke and
lower respiratory disease) were common to the county and state and accounted for 60.3% and 62.0%
of deaths, respectively. Cancer and heart disease alone accounted for roughly half of all deaths—47.7%
in the county and 50.3% in the state.
Table 1 Leading causes of death
Contra Costa County, 2005–2007
Deaths
Percent
Cancer
5,131
25.0%
162.0**
Heart disease
4,664
22.7%
147.5**
Stroke
1,462
7.1%
46.7**
Chronic lower respiratory disease
1,112
5.4%
36.0**
Alzheimer's disease
870
4.2%
27.8**
Unintentional injury
841
4.1%
26.8**
Diabetes
592
2.9%
18.9**
Influenza/pneumonia
575
2.8%
18.2**
Essential hypertension/hypertensive
renal disease/hypertensive renal
disease
308
1.5%
9.7**
Homicide
292
1.4%
20,515
100.0%
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than the state overall.
** Significantly lower rate than the state overall.
50
Rate
10.0*
651.2**
Leading causes of
death are those that
are responsible for
the greatest number
of deaths. In this
report, the leading
causes of death are
ranked according to
number of deaths,
which provides a
picture of the overall
burden of deaths
from specific causes.
The tables provide
the top 10 leading
causes of death for
each group.
LEADING CAUSES OF DEATH
Table 2 Leading causes of death
California, 2005–2007
Deaths
Percent
Rate
Heart disease
194,082
27.1%
212.9*
Cancer
165,284
23.1%
168.6*
Stroke
44,802
6.3%
49.5*
Chronic lower respiratory disease
38,791
5.40
42.0*
Unintentional injury
34,673
4.8%
32.4*
Alzheimer's disease
24,473
3.4%
28.9*
Diabetes
22,591
3.2%
23.4*
Influenza/pneumonia
21,588
3.0%
24.5*
Chronic liver disease/cirrhosis
11,835
1.7%
10.8*
Suicide
10,263
1.4%
9.4
715,022
100.0%
Total
The injury, homicide
and suicide rates
here differ slightly
from others in the
report. See this
section’s table
footnotes for further
explanation.
754.6*
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than the county overall.
Editor’s note: See the Leading Causes Appendix for more complete numbers and
age-adjusted rates for leading causes of death.
Contra Costa and California had the top eight leading causes of death in common. Essential hypertension/hypertensive renal disease was the ninth leading cause in Contra Costa and accounted for 308
deaths. Homicide was the 10th leading cause of death in Contra Costa. It accounted for 292 deaths in
the county and was the only leading cause for which the Contra Costa rate was significantly higher
than the California rate. Chronic liver disease/cirrhosis and suicide were the ninth and 10th leading
causes of death in the state but were 11th and 12th in Contra Costa.
Like the all-cause death rate, the death rates for cancer, heart disease, stroke, chronic lower respiratory
disease, Alzheimer’s disease, unintentional injuries, diabetes, influenza and pneumonia, essential
hypertension/hypertensive renal disease and chronic liver disease/cirrhosis were lower in Contra
Costa compared to California. The rate for suicide was similar for the county and state (see Appendix
table for a full list of available rates).
51
LEADING CAUSES OF DEATH
Data Sources: Leading Causes of Death for Contra Costa and California
Tables 1, 2: These tables include total deaths and age-adjusted average annual death rates per 100,000 for 2005-2007.
Mortality data from the California Department of Public Health (CDPH), http://www.dph.ca.gov/, Center for Health
Statistics’ Death Statistical Master File, 2005–2007. Any analyses or interpretations of the data were reached by the
Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the
CDPH.
In this section, the number of deaths for unintentional injuries, homicide and suicide include late effects. In the Injury
sections of this report, late effects are not included and the rates are crude, not age-adjusted so numbers, rates and
conclusions may differ. A late effect is the residual effect (condition produced) after the acute phase of an illness or injury
has terminated.
Population estimates for Contra Costa rates for 2005–2007 were provided by the Urban Strategies Council, Oakland, CA.
January, 2010. Data sources used to create these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association
of Bay Area Governments (ABAG) 2009 Projections, and California Department of Finance Population Estimates for
Cities, Counties and the State 2001-2009, with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
52
LEADING CAUSES OF DEATH
Leading Causes of Death, by Age
Cancer was among the top four leading causes of death
for all age groups except infants.
• Nearly three-quarters of deaths in Contra Costa were among
residents ages 65 years and older.
• Most deaths among older residents were from chronic diseases and
most deaths among younger residents were from unintentional injuries.
Between 2005–2007, almost three-quarters (73.9%) of deaths in Contra Costa were among residents
ages 65 years and older. Almost one-fifth of deaths (18.3%) in the county were among residents 45–64
years old and 7.8% of deaths were among residents younger than 45 years of age.
The leading causes of death change over a person’s life span. Chronic diseases such as cancer, heart
disease, stroke, chronic lower respiratory disease and diabetes develop over time and eventually lead
to death as people age. Chronic disease accounted for the greatest number of deaths in Contra Costa
residents 55 years and older. Unintentional injury accounted for the greatest number of deaths among
residents 1–34 years of age. A mix of chronic diseases and injuries made up the leading causes of death
among residents 35–54 years of age. Cancer was among the top four leading causes of death for all age
groups in Contra Costa, except for infants under 1 year of age.
53
LEADING CAUSES OF DEATH
65+ years
Between 2005–2007, there were 15,163 deaths among residents 65 years and older. This means that
on average 5,054 county residents in this age group died each year. Deaths among residents 65 years
of age and older accounted for almost three-quarters (73.9%) of all deaths among county residents.
Residents 65 years and older had the highest age-specific death rate (4,096.2 per 100,000); higher than
the age-specific death rates of all other age groups included in this section.
Table 1 Leading causes of death for residents 65 years or older
Contra Costa County, 2005 – 2007
Deaths
Percent
Rate
Heart disease
3,853
25.4%
1,040.9
Cancer
3,559
23.5%
961.5
Stroke
1,286
8.5%
347.4
Chronic lower respiratory disease
972
6.4%
262.6
Alzheimer's disease
861
5.7%
232.6
Influenza/pneumonia
518
3.4%
139.9
Diabetes
437
2.9%
118.1
Essential hypertension
/hypertensive renal disease
262
1.7%
70.8
Pneumonitis due to solids and liquids
229
1.5%
61.9
Unintentional injury
219
1.4%
59.2
15,163
100.0%
4,096.4
Total
This section
includes agespecific rates for
specific age groups
(e.g., 65 years and
older, etc.) These
rates should not
be compared to
age-adjusted rates
in this report or
others.)
The injury,
homicide and
suicide rates in
this section differ
slightly from others
in the report.
See this section’s
table footnotes for
further explanation.
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 65 years and older.
Heart disease was the leading cause of death among residents 65 years and older, accounting for onequarter (25.4%) of all deaths in this age group. Cancer, which accounted for 23.5% of deaths, ranked a
close second, followed by stroke (8.5%), chronic lower respiratory disease (6.4%), Alzheimer’s disease
(5.7%) and other causes listed. The top 10 leading causes of death accounted for 80.4% of all deaths
in this age group.
54
LEADING CAUSES OF DEATH
55–64 years
Between 2005–2007, there were 2,349 deaths among Contra Costa residents 55–64 years of age. This
means that on average 783 county residents in this age group died each year. Deaths among residents
55–64 years old accounted for 11.5% of all deaths in the county.
The death rate for residents 55–64 years old was 675.3 per 100,000.
Table 2 Leading causes of death for residents 55–64 years
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Cancer
944
40.2%
271.4
Heart disease
426
18.1%
122.5
Chronic lower respiratory disease
100
4.3%
28.7
Unintentional injury
99
4.2%
28.5
Diabetes
95
4.0%
27.3
Stroke
92
3.9%
26.4
Chronic liver disease and cirrhosis
89
3.8%
25.6
Suicide
38
1.6%
10.9
Essential hypertension/hypertensive
renal disease
27
1.1%
7.8
Viral hepatitis
27
1.1%
7.8
2,349
100.0%
675.3
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 55-64 years.
Cancer was the leading cause of death among residents 55–64 years old, accounting for 40.2% of all
deaths in this age group. Heart disease, which accounted 18.1% of deaths, was the second leading cause
of death, followed by chronic lower respiratory disease (4.3%), unintentional injury (4.2%), diabetes
(4.0%) and other causes listed. The top 10 leading causes of death accounted for 82.5% of all deaths
in this age group.
55
LEADING CAUSES OF DEATH
45–54 years
Between 2005–2007, there were 1,413 deaths among Contra Costa residents 45–54 years of age. This
means that on average 471 county residents in this age group died each year. Deaths among residents
45–54 years of age accounted for 6.9% of all deaths among county residents.
The death rate for residents 45–54 years old was 297.4 per 100,000.
Table 3 Leading causes of death for residents 45–54 years
Contra Costa County, 2005 – 2007
Deaths
Percent
Rate
Cancer
419
29.7%
88.2
Heart Disease
265
18.8%
55.8
Unintentional Injury
159
11.3%
33.5
Chronic liver disease and cirrhosis
69
4.9%
14.5
Suicide
59
4.2%
12.4
Stroke
51
3.6%
10.7
Diabetes
45
3.2%
9.5
Chronic lower respiratory disease
30
2.1%
6.3
Homicide
24
1.7%
5.1
Influenza/pneumonia
23
1.6%
4.8
1,413
100.0%
297.4
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 45-54 years.
Cancer was the leading cause of death among residents 45–54 years old, accounting for more than
one-quarter (29.7%) of all deaths in this age group. Heart disease, which accounted for 18.8% of deaths,
ranked second, followed by unintentional injury (11.3%), chronic liver disease/cirrhosis (4.9%), suicide
(4.2%) and other causes listed. The top 10 leading causes of death accounted for 81.0% of all deaths
in this age group.
56
LEADING CAUSES OF DEATH
35–44 years
Between 2005–2007, there were 699 deaths among Contra Costa residents 35–44 years of age. This
means that on average 233 county residents in this age group died each year. Deaths among residents
35-44 years of age accounted for 3.4% of all deaths in the county.
The death rate for residents 35-44 years old was 150.3 per 100,000.
Table 4 Leading causes of death for residents 35–44 years
Contra Costa County, 2005 – 2007
Deaths
Percent
Rate
Cancer
146
20.9%
31.4
Unintentional Injury
142
20.3%
30.5
Heart Disease
93
13.3%
20.0
Homicide
53
7.6%
11.4
Suicide
50
7.2%
10.7
Stroke
29
4.1%
6.2
Chronic liver disease and cirrhosis
28
4.0%
6.0
HIV disease
23
3.3%
4.9
Diabetes
13
1.9%
NA
8
1.1%
NA
699
100.0%
150.3
Chronic lower respiratory disease
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 35–44 years.
Cancer and unintentional injury were the leading causes of death among residents 35–44 years old,
each accounting for one-fifth of all deaths in this age group (20.9% and 20.3%, respectively). These
were followed by heart disease (13.3%), homicide (7.6%), suicide (7.2%) and other causes listed. The
top 10 leading causes of death accounted for 83.7% of all deaths in this age group.
57
LEADING CAUSES OF DEATH
25–34 years
Between 2005–2007, there were 317 deaths among Contra Costa residents 25–34 years of age. This
means that on average 106 county residents in this age group died each year. Deaths among residents
25–34 years of age accounted for 1.5% of all deaths in the county.
The death rate of residents 25–34 years old was 81.5 per 100,000.
Table 5 Leading causes of death for residents 25–34 years
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Unintentional injury
82
25.9%
21.1
Homicide
79
24.9%
20.3
Suicide
41
12.9%
10.5
Cancer
31
9.8%
8.0
Heart disease
19
6.0%
NA
HIV disease
8
2.5%
NA
Congenital malformations, deformations
and chromosomal abnormalities
Chronic liver disease and cirrhosis
6
5
1.9%
1.6%
NA
NA
317
100.0%
81.5
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 25-34 years.
Top 10 Leading Causes with fewer than five cases not shown.
Unintentional injury was the leading cause of death among residents 25-34 years old, accounting for
roughly one-quarter of all deaths in this age group (25.9%). Homicide ranked a close second, accounting
for 24.9% of deaths, followed by suicide (12.9%), cancer (9.8%), heart disease (6.0%) and other causes
listed. The top 10 leading causes of death, which also included stroke, and influenza and pneumonia,
accounted for 87.4% of all deaths in this age group.
58
LEADING CAUSES OF DEATH
15–24 years
Between 2005–2007, there were 313 deaths among Contra Costa residents 15–24 years of age. This
means that on average 104 county residents in this age group died each year. Deaths among residents
15–24 years of age accounted for 1.5% of all deaths among county residents.
The death rate for residents 15–24 years old was 76.5 per 100,000.
Table 6 Leading causes of death for residents 15–24 years
Contra Costa County, 2005 – 2007
Deaths
Percent
Rate
Unintentional injury
107
34.2%
26.2
Homicide
103
32.9%
25.2
Suicide
31
9.9%
7.6
Cancer
18
5.8%
NA
313
100.0%
76.5
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 15-24 years.
Top 10 Leading Causes with fewer than five cases not shown.
Unintentional injury and homicide were the leading causes of death among residents ages 15–24, each
accounting for 34.2% and 32.9%, respectively, of all deaths. These were followed by suicide (9.9%) and
cancer (5.8%). The top 10 leading causes of death which also included pregnancy/childbirth/puerperium,
congenital malformations/deformations/chromosomal abnormalities, heart disease, anemias, diabetes
and other tumors1 accounted for 87.9% of all deaths in this age group.
59
LEADING CAUSES OF DEATH
1–14 years
Between 2005–2007, there were 88 deaths among Contra Costa residents 1–14 years of age. This means
that on average, 29 county residents in this age group died each year. Deaths among residents 1–14
years of age accounted for 0.4% of all deaths among county residents.
Residents 1–14 years old had the lowest death rate (14.7 per 100,000) of all the age groups included
in this section.
Table 7 Leading causes of death for residents 1–14 years
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
Unintentional injury
26
29.5%
4.4
Cancer
14
15.9%
NA
Homicide
10
11.4%
NA
7
8.0%
NA
88
100.0%
14.7
Congenital malformations,
deformations and
chromosomal abnormalities
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents 1-14 years.
Top 10 Leading Causes with fewer than five cases not shown.
Unintentional injuries were the leading cause of death among residents ages 1–14, accounting for 29.5%
of all deaths in this age group. Cancer (15.9%) and homicide (11.4%) were the second and third leading
causes of death, respectively, followed by congenital anomalies (8.0%). The top 10 leading causes of
death, which also included anemias, influenza and pneumonia, heart disease, hernia, HIV and other
tumors1 accounted for 75.0% of all deaths in this age group.
60
LEADING CAUSES OF DEATH
<1 YEAR OLD
Between 2005–2007, there were 173 deaths among Contra Costa residents younger than 1 year old.
This means that on average, 58 Contra Costa infants in this age group died each year. Deaths among
residents younger than 1 year old accounted for 0.8% of all deaths among county residents.
The age-specific death rate of residents younger than 1 year was 441.4 per 100,000.
Table 8 Leading causes of death for residents younger
than 1 year old
Contra Costa County, 2005 –2007
Deaths
Percent
Congenital malformations, deformations and
chromosomal abnormalities
31
17.9%
79.1
Disorders related to short gestation/LBW-NEC
26
15.0%
66.3
Sudden infant death syndrome
17
9.8%
NA
Newborn affected by maternal complications
9
5.2%
NA
Neonatal hemorrhage
8
4.6%
NA
Unintentional injury
7
4.0%
NA
Respiratory distress of newborn
6
3.5%
NA
Intrauterine hypoxia and birth asphyxia
5
2.9%
NA
Newborn affected by complications of placenta,
cord and membranes
5
2.9%
NA
173
100.0%
Total
Rate
441.4
Total includes deaths from all causes, including but not limited to those listed above.
These are age-specific rates per 100,000 residents younger than 1 year old.
Top 10 Leading Causes with fewer than five cases not shown.
Congenital malformations, deformations and anomalies were the leading cause of death among infants in Contra Costa, accounting for 17.9% of all deaths in this age group. Disorders related to short
gestation (15.0%) ranked a close second, followed by sudden infant death syndrome (9.8%), maternal
complications (5.2%), neonatal hemorrhage (4.6%) and other causes listed. The top 10 leading causes
of death, which also included diseases of the circulatory system, accounted for 68.2% of all deaths in
this age group.
61
LEADING CAUSES OF DEATH
Data Sources: Leading Causes of Death, by Age
tables
Tables 1–8: These tables include total deaths and age-specific average annual death rates for 2005 through 2007. Mortality
data from the California Department of Public Health (CDPH), http://www.cdph.ca.gov/, Center for Health Statistics’
Death Statistical Master File, 2005-2007. Any analyses or interpretations of the data were reached by the Community
Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the CDPH. Counts
fewer than five are not shown in order to protect anonymity. Rates were not calculated for any group with fewer than 20
cases due to unstable estimates.
In this section, the number of deaths for unintentional injuries, homicide and suicide include late effects. In the Injury
sections of this report, late effects are not included so numbers, rates and conclusions may differ. A late effect is the
residual effect (condition produced) after the acute phase of an illness or injury has terminated.
Population estimates for Contra Costa rates for 2005–2007 were provided by the Urban Strategies Council, Oakland, CA.
January, 2010. Data sources used to create these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association
of Bay Area Governments (ABAG) 2009 Projections, and California Department of Finance Population Estimates for
Cities, Counties and the State 2001-2009, with 2000 Benchmark.
text
1. “Other tumors” refers to the ICD10 code for in situ neoplasm, benign neoplasm and neoplasm of uncertain behavior.
62
LEADING CAUSES OF DEATH
Leading Causes of Death, by Race & Ethnicity
African Americans had the highest rate of death.
• Heart disease, cancer and stroke were the top three leading causes of death for whites,
African Americans and Asians/Pacific Islanders.
• African Americans were more likely to die from heart disease, cancer, stroke, homicide,
unintentional injury, diabetes, essential hypertension and hypertensive renal disease,
and HIV, than county residents overall.
Editor’s note: See the Leading Causes Appendix for more complete numbers and
rates for leading causes of death.
Between 2005–2007, the greatest number of deaths in the county was among whites (15,042), followed
by African Americans (2,225) Hispanics (1,640) and Asians/Pacific Islanders (1,406).
Table 1 All-cause mortality by race/ethnicity
Contra Costa County, 2005 –2007
Deaths
White
Percent
Rate
15,042
73.3%
683.9*
African American
2,225
10.8%
1,002.7*
Hispanic
1,640
8.0%
460.2**
Asian/Pacific Islander
1,406
6.9%
443.9**
20,515
100.0%
651.2
Total
Total includes racial/ethnic groups not included above.
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The four racial/ethnic groups presented in this section had seven of 10 leading causes of death in common: cancer, heart disease, stroke, unintentional injury, diabetes, influenza/pneumonia and chronic
lower respiratory disease.
Heart disease, cancer and stroke were the top three leading causes of death for whites, African Americans
and Asians/Pacific Islanders. The top three causes of death for Hispanics were cancer, heart disease
and unintentional injury. Other leading causes of death varied by race/ethnicity, including: essential
hypertension and hypertensive renal disease (for African Americans, Asians/Pacific Islanders and
whites), Alzheimer’s disease (for Hispanics and whites), chronic liver disease and cirrhosis (for Asians/
63
LEADING CAUSES OF DEATH
Pacific Islanders and Hispanics), homicide (for African Americans and Hispanics), suicide (for Asians/
Pacific Islanders and whites) and HIV (for African Americans).
Whites
Between 2005–2007, there were 15,042 deaths among whites in Contra Costa. This means that on
average 5,014 white residents died each year.
Table 2 Leading causes of death among whites
Contra Costa County, 2005–2007
Deaths
Percent
Cancer
3,799
25.3%
175.6*
Heart disease
3,465
23.0%
151.9
Stroke
1,043
6.9%
45.6
Chronic lower respiratory disease
939
6.2%
42.7*
Alzheimer’s disease
771
5.1%
32.6*
Unintentional injury
520
3.5%
28.9
Influenza/pneumonia
439
2.9%
18.9
Diabetes
350
2.3%
16.0
Suicide
214
1.4%
12.3*
Essential hypertension/hypertensive
renal disease
210
1.4%
9.2
15,042
100.0%
Total
Rate
The unintentional
injury and suicide
rates shown here
differ slightly from
those in the Injury
section of this
report. See table
footnotes for further
explanation.
683.9*
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 white residents.
* Significantly higher rate than the county overall.
The age-adjusted all-cause death rate for whites (683.9 per 100,000) was higher than the age-adjusted
rate for Contra Costa residents overall (651.2 per 100,000).
Cancer was the leading cause of death among whites in the county, accounting for one-quarter (25.3%)
of all deaths in this group. Heart disease ranked a close second (23.0%), followed by stroke (6.9%),
chronic lower respiratory disease (6.2%), Alzheimer’s disease (5.1%) and other causes listed. The top
10 leading causes of death accounted for 78.1% of all deaths among whites.
Whites had higher death rates from cancer, chronic lower respiratory disease, Alzheimer’s disease and
suicide compared to county residents overall.
64
LEADING CAUSES OF DEATH
African Americans
Between 2005–2007, there were 2,225 deaths among African Americans in Contra Costa. This means
that on average 742 African American residents died each year.
Table 3 Leading causes of death among
African Americans
Contra Costa County, 2005 –2007
Deaths
Percent
Heart disease
538
24.2%
258.8*
Cancer
512
23.0%
228.0*
Stroke
161
7.2%
80.5*
Homicide
146
6.6%
54.5*
Unintentional injury
122
5.5%
43.8*
Diabetes
97
4.4%
46.5*
Chronic lower respiratory disease
71
3.2%
33.9
Essential hypertension/hypertensive
renal disease
53
2.4%
24.9*
HIV disease
45
2.0%
15.6*
Influenza/pneumonia
43
1.9%
20.7
Total
2,225
Rate
The homicide and
unintentional injury
rates shown here
differ slightly from
those in the Injury
section of this
report. See table
footnotes for further
explanation.
100.0% 1,002.7*
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 African American residents.
* Significantly higher rate than the county overall.
African American residents had the highest age-adjusted all-cause death rate in the county (1,002.7
per 100,000); higher than the age-adjusted rates for county residents overall and all other racial/ethnic
groups included in this section.
Heart disease was the leading cause of death among African Americans in the county, accounting for
roughly one-quarter (24.2%) of all deaths in this group. Cancer ranked a close second (23.0%), followed
by stroke (7.2%), homicide (6.6%), unintentional injury (5.5%) and other causes listed. The top 10
leading causes of death accounted for 80.4% of all deaths among African Americans.
African Americans had significantly higher death rates than county residents overall in each leading
cause listed above except for chronic lower respiratory disease and influenza/pneumonia; the African
American death rates from these two causes were similar to the county rates.
65
LEADING CAUSES OF DEATH
African Americans had the highest death rates of all of the racial/ethnic groups included in this section from each of the following leading causes: heart disease, cancer, stroke, unintentional injury, and
diabetes (see Appendix table for a full list of available rates).
Hispanics
Between 2005–2007, there were 1,640 deaths among Hispanics in Contra Costa. This means that on
average 547 Hispanic residents died each year.
Table 4 Leading causes of death among Hispanics
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
Cancer
360
22.0%
100.6**
Heart disease
321
19.6%
107.4**
Unintentional injury
130
7.9%
21.9
Stroke
107
6.5%
36.1**
Diabetes
77
4.7%
24.2
Homicide
75
4.6%
10.1
Influenza / pneumonia
46
2.8%
16.7
Alzheimer’s disease
44
2.7%
17.3**
Chronic lower respiratory disease
44
2.7%
15.7**
Chronic liver disease / cirrhosis
43
2.6%
10.2
1,640
100.0%
Total
The homicide and
unintentional
injury rates shown
here differ slightly
from those in the
Injury section of
this report. See
table footnotes
for further
explanation.
460.2**
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 Hispanic residents.
** Significantly lower rate than the county overall.
The age-adjusted all-cause death rate for Hispanics (460.2 per 100,000) was lower than the age-adjusted
rate for Contra Costa residents overall (651.2 per 100,000).
Cancer was the leading cause of death among Hispanics in the county, accounting for 22.0% of all deaths
in this group. Heart disease ranked a close second (19.6%), followed by unintentional injury (7.9%),
stroke (6.5%), diabetes (4.7%) and other causes listed. The top 10 leading causes of death accounted
for 76.0% of all deaths among Hispanics.
Hispanics had significantly lower death rates than county residents overall from the following leading
causes: cancer, heart disease, stroke, Alzheimer’s disease and chronic lower respiratory disease.
66
LEADING CAUSES OF DEATH
Asians/Pacific Islanders
Between 2005–2007, there were 1,406 deaths among Asians/Pacific Islanders in Contra Costa. This
means that there were on average 469 deaths each year among Asian/Pacific Islander residents.
Table 5 Leading causes of death among Asians/Pacific
Islanders
Contra Costa County, 2005–2007
Cancer
Heart disease
Stroke
Diabetes
Unintentional injury
Chronic lower respiratory disease
Influenza / pneumonia
Chronic liver disease/ cirrhosis
Essential hypertension/ hypertensive
renal disease
Suicide
Total
Deaths
Percent
Rate
404
299
141
64
54
52
43
25
24
28.7%
21.3%
10.0%
4.6%
3.8%
3.7%
3.1%
1.8%
1.7%
116.2**
99.5**
47.1
20.0
14.3**
18.1**
15.6
6.5
8.2
20
1,406
1.4%
100.0%
5.0**
443.9**
The suicide and
unintentional injury
rates shown here
differ slightly from
those in the Injury
section of this
report. See table
footnotes for further
explanation.
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 Asian/Pacific Islander residents.
** Significantly lower rate than the county overall.
The age-adjusted all-cause death rate for Asians/Pacific Islanders (443.2 per 100,000) was lower
compared to the age-adjusted rate for Contra Costa residents overall (651.2 per 100,000).
Cancer was the leading cause of death among Asians/Pacific Islanders in the county, accounting for
more than one-quarter (28.7%) of all deaths in this group. Heart disease ranked a close second (21.3%),
followed by stroke (10.0%), diabetes (4.6%) and unintentional injury (3.8%). The top 10 leading causes
of death accounted for 80.1% of all deaths among Asians/Pacific Islanders.
Asians/Pacific Islanders had significantly lower death rates than county residents overall from the following causes: cancer, heart disease, unintentional injury, chronic lower respiratory disease and suicide.
67
LEADING CAUSES OF DEATH
Data Sources: Leading causes of death, by race/ethnicity
Tables 1–5: These tables include total deaths and age-adjusted average annual death rates for 2005 through 2007. Mortality
data from the California Department of Public Health Services (CDPH), http://www.cdph.ca.gov/, Center for Health
Statistics’ Death Statistical Master File, 2005–2007. Any analyses or interpretations of the data were reached by the
Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the
CDPH. Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans include non-Hispanic residents. Not all races/ethnicities are shown but all are included
in total for the county.
In this section, the numbers of deaths due to unintentional injury, suicide and homicide include late effects. In the Injury
section of this report, late effects are not included and rates are not age-adjusted so numbers, rates and conclusions may
differ. A late effect is the residual effect (condition produced) after the acute phase of an illness or injury has terminated.
Population estimates for Contra Costa rates for 2005–2007 were provided by the Urban Strategies Council, Oakland, CA.
January, 2010. Data sources used to create these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association
of Bay Area Governments (ABAG) 2009 Projections, and California Department of Finance Population Estimates for
Cities, Counties and the State 2001–2009, with 2000 Benchmark.
68
LEADING CAUSES OF DEATH
Leading Causes of Death, by Gender
Males were more likely to die from most
leading causes than females.
• Cancer, heart disease and stroke were the top three causes of death for males and
females.
• Males and females shared eight top 10 leading causes of death.
• Females were more likely than males to die from Alzheimer’s disease.
Editor’s note: See the Leading Causes Appendix for more complete numbers and
rates for leading causes.
Between 2005–2007, there were more deaths among females (10,634) than males (9,881) in Contra
Costa. On average, 3,545 females and 3,294 males in the county died each year.
The age-adjusted all-cause death rate was higher for the county’s males (769.1 per 100,000) than females
(563.9 per 100,000).
Cancer, heart disease and stroke were the top three leading causes of death for both males and females,
accounting for more than half of all deaths for each group. Males and females shared eight top 10
leading causes of death.
Table 1 Leading causes of death among males
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Cancer
2,501
25.3%
188.5*
Heart disease
2,307
23.3%
185.1*
Stroke
552
5.6%
46.1
Unintentional injury
551
5.6%
38.1*
Chronic lower respiratory disease
495
5.0%
40.6*
Diabetes
304
3.1%
22.9*
Influenza/pneumonia
266
2.7%
23.1*
Alzheimer’s disease
254
2.6%
23.0**
Homicide
246
2.5%
16.8*
Suicide
198
2.0%
13.5*
9,881
100.0%
769.1*
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 male residents.
* Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
69
The unintentional
injury, homicide
and suicide rates
here differ slightly
from others in the
report. See this
section’s table
footnotes for
further explanation.
LEADING CAUSES OF DEATH
The three leading causes of death among Contra Costa males—cancer, heart disease and stroke—accounted for more than half (54.2%) of all male deaths. The top 10 leading causes of death accounted
for 77.7% of all deaths among males.
Males had higher death rates than females for cancer, heart disease, unintentional injury, chronic
lower respiratory disease, diabetes, influenza/pneumonia, homicide and suicide. Homicide and suicide
were the ninth and 10th (respectively) leading causes of death for males but were just the 19th and 14th
(respectively) leading causes of death for females. Males had a similar death rate from stroke and a
lower death rate from Alzheimer’s disease compared to females. (See Appendix table for a full list of
available rates).
Table 2 Leading causes of death among females
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Cancer
2,630
24.7%
146.0**
Heart disease
2,357
22.2%
120.0**
Stroke
910
8.6%
46.5
Chronic lower respiratory disease
617
5.8%
33.4**
Alzheimer’s disease
616
5.8%
30.1*
Influenza/pneumonia
309
2.9%
15.5**
Unintentional injury
290
2.7%
17.0**
Diabetes
288
2.7%
16.0**
Essential hypertension/hypertensive
renal disease
182
1.7%
9.2
Pneumonitis due to solids and liquids
112
1.1%
5.7**
10,634
100.0%
563.9**
Total
Total includes deaths from all causes, including but not limited to those listed above.
These are age-adjusted rates per 100,000 female residents.
* Significantly higher rate than county males overall.
** Significantly lower rate than county males overall.
The three leading causes of death among Contra Costa females —cancer, heart disease and stroke — accounted for 55.5% of female deaths. The top 10 leading causes of death accounted for 78.2% of all
deaths among females.
Females had a higher death rate for Alzheimer’s disease than men. Females had lower death rates than
men from cancer, heart disease, chronic lower respiratory disease, influenza/pneumonia, unintentional
injury, diabetes and pneumonitis due to solids and liquids.
70
LEADING CAUSES OF DEATH
Essential hypertension and hypertensive renal disease, and pneumonitis due to solids and liquids
were the ninth and 10th (respectively) causes of death for females and the 13th and 14th (respectively)
causes of death for males. Females had similar rates of death from stroke and essential hypertension/
hypertensive renal disease compared to males.
Sources: Leading Causes of Death for Contra Costa, by Gender
Tables 1, 2: These tables include total deaths and age-adjusted average annual death rates for 2005 through 2007. Mortality
data from the California Department of Public Health (CDPH), http://www.cdph.ca.gov/, Center for Health Statistics’
Death Statistical Master File, 2005-2007. Any analyses or interpretations of the data were reached by the Community
Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the CDPH.
In this section, the number of deaths for unintentional injury, homicide and suicide includes late effects. In the Injury
section of this report, late effects are not included and rates are not age-adjusted so numbers, rates and conclusions may
differ.
Population estimates for Contra Costa rates for 2005–2007 were provided by the Urban Strategies Council, Oakland, CA.
January, 2010. Data sources used to create these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association
of Bay Area Governments (ABAG) 2009 Projections, and California Department of Finance Population Estimates for
Cities, Counties and the State 2001–2009, with 2000 Benchmark.
71
LEADING CAUSES OF DEATH
Appendix: Age-Adjusted Rates for All Leading Causes of Death
This table is arrayed by Contra Costa County’s ranking of leading causes of death 1–10. Rankings that differ from
Contra Costa’s order are noted in parentheses ( ).
Contra Costa
County
All Causes
(#)
California
Male
Female
20,515
715,022
9,881
10,634
(rate per 100,000)
651.2
754.6
769.1
563.9
1. Cancers
5,131
(2) 165,284
2,501
2,630
162.0
168.6
188.5
146.0
4,664
(1) 194,082
2,307
2,357
147.5
212.9
185.1
120.0
1,462
44,802
552
910
46.7
49.5
46.1
46.5
1,112
38,791
(5) 495
617
36.0
42.0
40.6
33.4
870
(6) 24,473
(8) 254
616
27.8
28.9
23.0
30.1
841
(5) 34,673
(4) 551
(7) 290
26.8
32.4
38.1
17.0
592
22,591
(6) 304
(8) 288
18.9
23.4
22.9
16.0
575
21,588
(7) 266
(6) 309
18.2
24.5
23.1
15.5
308
(11) 9,472
(13) 126
182
9.7
10.6
10.1
9.2
292
(13) 7,580
(9) 246
(19) 46
10.0
6.8
16.8
3.0
286
(9) 11,835
(11) 177
(11) 109
8.5
10.8
11.2
6.1
270
(10) 10,263
(10) 198
(14) 72
8.6
9.4
13.5
4.3
233
(23) 2,621
(14) 121
(10) 112
7.5
3.0
10.8
5.7
79
(19) 3,606
(18) 60
(24) 19
2.4
3.2
3.7
NA
2. Heart disease
3. Stroke
4. Chronic lower respiratory disease
5. Alzheimer’s disease
6. Unintentional injury
7. Diabetes mellitus
8. Influenza/ pneumonia
9. Essential hypertension/
hypertensive renal disease
10. Homicide
11. Chronic liver disease/ cirrhosis
12. Suicide
13. Pneumonitis due to solids and liquids
21. Human Immunodeficiency
Virus (HIV) disease
72
continued next page
LEADING CAUSES OF DEATH
Appendix: Age-Adjusted Rates for All Leading Causes of Death
This table is arrayed by Contra Costa County’s ranking of leading causes of death 1–10. Rankings that differ
from Contra Costa’s order are noted in parentheses ( ).
White
African American
Hispanic
API
15,042
2,225
1,640
1,406
(rate per 100,000)
683.9
1002.7
460.2
443.9
1. Cancers
3,799
(2) 512
360
404
175.6
228.0
100.6
116.2
3,465
(1) 538
321
299
151.9
258.8
107.4
99.5
1,043
161
(4) 107
141
45.6
80.5
36.1
47.1
939
(7) 71
(9) 44
(6) 52
42.7
33.9
15.7
18.1
771
(11) 33
(8) 44
(11) 19
32.6
19.3
17.3
NA
520
(5) 122
(3) 130
(5) 54
28.9
43.8
21.9
14.3
(8) 350
(6) 97
(5) 77
(4) 64
16.0
46.5
24.2
20.0
(7) 439
(10) 43
(7) 46
(7) 43
18.9
20.7
16.7
15.6
210
(8) 53
(19) 19
(9) 24
9.2
24.9
NA
8.2
(19) 51
(4) 146
(6) 75
(12) 16
3.3
54.5
10.1
NA
(12) 193
(12) 22
(10) 43
(6) 25
8.9
8.0
10.2
6.5
(9) 214
(20) 11
(12) 22
(10) 20
12.3
NA
3.9
5.0
(12) 193
(15) 17
(18) 11
(15) 11
8.4
NA
NA
NA
(24) 27
(9) 45
(21) 7
0
1.5
15.6
NA
NA
All Causes
(#)
2. Heart disease
3. Stroke
4. Chronic lower respiratory disease
5. Alzheimer’s disease
6. Unintentional injury
7. Diabetes mellitus
8. Influenza/ pneumonia
9. Essential hypertension/
hypertensive renal disease
10. Homicide
11. Chronic liver disease/ cirrhosis
12. Suicide
13. Pneumonitis due to solids and liquids
21. Human Immunodeficiency
Virus (HIV) disease
73
FAMILY, MATERNAL & CHILD HEALTH
Overview of Local Births
Hispanic mothers had the greatest number of births.
• Hispanics had the highest crude birth rate.
• Residents of San Pablo had the highest birth rate.
• The birth rate of county residents did not change significantly between 2005–2007.
Between 2005 and 2007, there were 40,193 births to women residing in Contra Costa County, an
average of 13,398 births per year.
Hispanic women in the county had the largest number (14,485) and percentage (36.0%) of all births,
followed by white women (14,355, 35.7%), Asians/Pacific Islanders (5,931, 14.8%) and African
Americans (3,582, 8.9%).
Hispanics also had the highest crude birth rate (21.6 per 1,000)—higher than the county overall (13.0
per 1,000) and of any other racial/ethnic group listed. Asians/Pacific Islanders (15.3 per 1,000) and
African Americans (13.7 per 1,000) also had higher birth rates compared to the county overall. White
women had a relatively high number of births, but the lowest birth rate (8.5 per 1,000)—lower than
the county and of any other racial/ethnic group listed.
The county’s three largest cities had the largest number of births; Concord (5,415), Richmond (4,788)
and Antioch (4,738).
San Pablo residents had the highest crude birth rate (25.0 per 1,000)—higher than the county overall
and higher than any of the selected cities. Other cities had higher birth rates than the county rate
overall: Bay Point (18.2 per 1,000), Pittsburg (17.7 per 1,000), Antioch (15.9 per 1,000), Richmond and
Brentwood (15.5 per 1,000), Oakley (15.0 per 1,000), and Concord (14.6 per 1,000). Pinole (9.5 per
1,000), Walnut Creek (10.6 per 1,000), Pleasant Hill (11.5 per 1,000) and El Cerrito (11.6 per 1,000)
had lower birth rates than the county overall.
In Contra Costa, women 20-34 years had the greatest number of births (28,547) and the highest birth
rate (49.4 per 1,000) compared to other age groups. Less than 7% of births were to women 15-19 years,
while 22.3% of births were to women 35 years and older.
Seventy-nine percent (78.5%) of women who gave birth in the county had 12 years or more of education, and over a quarter of women who gave birth (26.3%) were covered by Medi-Cal.
74
FAMILY, MATERNAL & CHILD HEALTH
Select Characteristics of Live Births
Contra Costa, 2005–2007
Number of live % of total live
births
Birth rate by year
Race/ethnicity of mother
(2005–2007)
Selected cities
(2005–2007)
births
Crude birth
rate
2005
13,143
NA
12.8
2006
13,565
NA
13.1
2007
13,485
NA
12.9
Total
40,193
NA
13.0
Hispanic
14,485
36.0%
White
14,355
35.7%
Asian/Pacific
Islander
5,931
14.8%
15.3*
African
American
3,582
8.9%
13.7*
Concord
5,415
13.5%
14.6*
Richmond
4,788
11.9%
15.5*
Antioch
4,738
11.8%
15.9*
Pittsburg
3,324
8.3%
17.7*
San Pablo
2,319
5.8%
25.0*
Brentwood
2,175
5.4%
15.5*
Walnut Creek
2,081
5.2%
10.6**
Martinez
1,454
3.6%
13.4
Oakley
1,385
3.4%
15.0*
Bay Point
1,235
3.1%
18.2*
Pleasant Hill
1,147
2.9%
11.5**
Hercules
877
2.2%
12.3
El Cerrito
807
2.0%
11.6**
Pinole
548
1.4%
9.5**
75
21.6*
8.5**
continued next page
FAMILY, MATERNAL & CHILD HEALTH
Select Characteristics of Live Births
Contra Costa, 2005–2007
Age of mother (years)
(2005–2007)
Number of
% of total
Crude birth
live births
live births
rate
10–14 years
36
0.1%
0.2
**
15–19 years
2,657
6.6%
11.5
**
20–34 years
28,547
71.0%
49.4
*
35–44 years
8,809
21.9%
19.6
*
45–49 years
135
0.3%
0.5
**
31,558
78.5%
NA
10,560
26.3%
NA
Mother >= 12 years education
(2005-2007)
Medi-Cal delivery
(2005-2007)
These are crude rates per 1,000 residents.
*Significantly higher rate than county rate overall.
**Significantly lower rate than county rate overall.
Data Sources: Overview of Local Births
tables
Birth data from the California Department of Public Health (CDPH), Birth Statistical Master Files, 2005–2007. Any
analyses or interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation
(CHAPE) Unit of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include Hispanic
residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic
residents. Not all races/ethnicities shown but all are included in totals for the county and for each city, age group and
educational level. These tables include total live births to women who are residents of Contra Costa and average crude
birth rates for 2005 through 2007.
Population data for county total, race/ethnicity and age groups for 2005–2007
State of California, Department of Finance, Race/Ethnic Population with Age and Sex Detail, 2000–2050. Sacramento, CA,
July 2007.
Population data for selected cities for 2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January,
2010. Data sources used to create these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay
Area Governments (ABAG) 2009 Projections, and California Department of Finance Population Estimates for Cities,
Counties and the State 2001–2009, with 2000 Benchmark.
Crude birth rate is the number of births for a particular group of interest divided by the total population for that particular
group multiplied by 1,000.
Percent of Total Live Births is the number of births in a particular group divided by the number of total live births for
2005–2007 multiplied by 100.
76
FAMILY, MATERNAL & CHILD HEALTH
Births to Teens
Hispanic and African American women 15–19 years old
were more likely to give birth compared
to county teens as a whole.
• Contra Costa’s teen birth rate was lower than the California rate.
• More than half of all teen births were to Hispanic teens.
Editor’s note: This section presents data for births to women ages 15–19 in Contra
Costa. All rates presented are age-specific birth rates per 1,000 women ages 15–19
for the particular group, city or county.
Between 2005 and 2007, there were 2,657 births to women age 15–19 years residing in Contra Costa
County. This means that there were on average 886 births to women per year in the county. Contra
Costa’s teen birth rate (23.5 per 1,000) was lower than that of California (37.4 per 1,000).1
Table 1 Teen births by race/ethnicity
Contra Costa County 2005–2007
Births
Percent
1,544
58.1%
53.4*
African American
528
19.9%
42.5*
White
390
14.0%
7.2**
89
3.3%
6.6**
2,657
100.0%
Hispanic
Asian/Pacific Islander
Total
Rate
23.5
These are age-specific rates per 1,000 women ages 15–19.
Total includes some racial/ethnic groups not shown.
* Significantly higher rate compared to county.
** Significantly lower rate compared to county.
Hispanic women had the highest percentage (58.1%) and highest rate of teen births (53.4 per 1,000)—
higher than county teens overall (23.5 per 1,000) and teens of any other race/ethic group listed. African
American teen births represented almost one-fifth (19.9%) of the county’s teen births and the African
American teen birth rate (42.5 per 1,000) was higher than the rate of county teens overall. Whites and
Asians/Pacific Islanders had lower teen birth rates than county teens overall.
77
FAMILY, MATERNAL & CHILD HEALTH
Table 2 Teen births by selected communities
Contra Costa County 2005–2007
Cases
Percent
Rate
Richmond
554
20.9%
54.0*
Antioch
463
17.4%
39.0*
Concord
341
12.8%
28.8
Pittsburg
340
12.8%
47.2*
San Pablo
237
8.9%
67.4*
Bay Point
151
5.7%
60.2*
Brentwood
135
5.1%
24.9
Oakley
108
4.1%
29.2
Martinez
48
1.8%
14.0**
Hercules
39
1.5%
14.2**
Pinole
33
1.2%
16.8**
Walnut Creek
28
1.1%
6.3**
El Cerrito
21
0.8%
15.2**
Pleasant Hill
15
0.6%
NA
These are age-specific rates per 1,000 women ages 15–19.
Not all Contra Costa cities shown.
*Significantly higher rate compared to county.
** Significantly lower rate compared to county.
Four communities had more than 300 births to teens between 2005 and 2007. These were Richmond
(554), Antioch (463), Concord (341) and Pittsburg (340).
Five communities had significantly higher teen birth rates than county teens overall: San Pablo (67.4
per 1,000), Bay Point (60.2 per 1,000), Richmond (54.0 per 1,000), Pittsburg (47.2 per 1,000) and
Antioch (39.0 per 1,000).
Walnut Creek (6.3 per 1,000), Martinez (14.0 per 1,000), Hercules (14.2 per 1,000), El Cerrito (15.2 per
1,000) and Pinole (16.8 per 1,000) had rates of teen births that were lower than the county rate overall.
78
FAMILY, MATERNAL & CHILD HEALTH
What is it?
Teen birth is typically defined as births that occur to teenagers 15 to 19 years old, although sometimes
younger ages are included. The measure for teen births presented in this report is the teen birth rate,
which is the number of births to teens 15 to 19 years old per 1,000 female teens 15 to 19 years old.
Why is it important?
Most teen pregnancies are unintended,2 and teen childbearing can have negative consequences for the
mother, father and child. When teenagers become parents, they are less likely than teens without children to achieve educational goals, find sustainable and productive work, and become self sufficient.3,4
Infants born to teens are more likely to be born low birth weight and suffer from related health problems.5,6 In addition, compared to children of older mothers, children of teen mothers are more likely
to do poorly in or drop out of school and to become teen parents themselves.7 It is important to note
that some teen parents successfully face these challenges and meet their educational and career goals
and raise healthy children.
Who does it impact the most?
Teen births have been associated with a variety of factors including low income, low maternal education, lack of effective family planning practices, lack of education or counseling regarding family planning, previous teen pregnancy and initiation of sexual activity at a young age.3
In the United States, teen birth rates differ by race/ethnicity. In 2007, Hispanic teens had the highest
teen birth rate, and Hispanics, non-Hispanic blacks and American Indians all had teen birth rates higher
than the United States overall.8
What can we do about it?
Teen pregnancy is a complex issue. Preventing teen pregnancy requires a coordinated approach by
community programs and broad efforts to influence values and popular culture and engage parents
and schools.9 There are different types of programs that can reduce sexual risk-taking behaviors and/or
teen pregnancy, such as comprehensive sexuality education, youth development programs, and early
childhood programs.9,10,11
At a minimum, it is essential that youths have access to age-appropriate and medically accurate information about abstinence and contraception as well as confidential, affordable and accessible reproductive health services that include contraception. Interventions that affect nonsexual risk and protective
factors (e.g., school performance; positive plans for the future; connections to family, school and faith
community) that may reduce sexual risk-taking behaviors or pregnancy should also be considered when
addressing this pressing issue.
79
FAMILY, MATERNAL & CHILD HEALTH
Data Sources: Births to Teens
tables
Tables 1, 2: Birth data from the California Department of Public Health (CDPH), Birth Statistical Master Files, 2005-2007.
Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation
(CHAPE) Unit of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include Hispanic
residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic
residents. Not all race/ethnicities shown but all are included in totals for the county and for each city. Rates were not
calculated for any group with fewer than 20 cases due to unstable estimates. These tables include births to women ages
15-19 who are residents of Contra Costa and average crude teen birth rates for 2005 through 2007.
Teen birth rate is the number of infants born to teen girls 15–19 years old divided by the total population of teen girls
15–19 years for the particular group, city or county multiplied by 1,000.
Table 1: Population estimates for Contra Costa and its subpopulations (by age, gender and race/ethnicity) for 2005–2007
from State of California, Department of Finance, Race/Ethnic Population with Age and Sex Detail, 2000–2050. Sacramento,
CA, July 2007.
Table 2: Population estimates for Contra Costa and its subpopulations (by age, gender and city/census place) for 2005–
2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010.
text
1.
California Department of Public Health, Death and Birth Records. (2009) Vital Statistics Query System. Retrieved
from http://www.applications.dhs.ca.gov/vsq/ on January 8, 2010.
2. Finer, L.B., & Henshaw, S. (2006). Disparities in rates of unintended pregnancy in the United States. Perspectives on
Sexual and Reproductive Health, 38(2), 90–96.
3. National Campaign to Prevent Teen Pregnancy. Whatever happened to childhood? The problem of teen pregnancy in
the United States. Washington, DC; 1997.
4. Constantine NA, Nevarez CR. No time for complacency: teen births in California. Public Health Institute. Berkeley,
CA; 2003 Mar.
5. Maynard, RA, editor. Kids having kids: A Robin Hood Foundation special report on the costs of adolescent
childbearing. New York: Robin Hood Foundation; 1997.
6. National Campaign to Prevent Teen Pregnancy. Why it matters: Teen pregnancy and other health issues [Internet].
Washington, DC; 2007. Available from: http://www.thenationalcampaign.org/why-it-matters/wim_teens.aspx.
7. National Campaign to Prevent Teen Pregnancy. Why it matters: Teen pregnancy and education [Internet].
Washington, DC; 2007. Available from: http://www.thenationalcampaign.org/why-itmatters/wim_teens.aspx.
8. Child Trends. Teen births. 2010. Available from: http://www.childtrendsdatabank.org/?q=node/52
9. Kirby D, Emerging Answers: Research Findings on Programs to Reduce Teen Pregnancy and Sexually Transmitted
Diseases, Washington, DC: National Campaign to Prevent Teen Pregnancy, 2007
10. Ball, V, and Moore, K. A. What works for adolescent reproductive health: Lessons from experimental evaluations of
programs and interventions. Washington, DC: Child Trends. Publication #2008-20.May 2008.
11. Office of Adolescent Health, U.S. Department of Health and Human Services. Teen Pregnancy Prevention Research
Evidence Review. http://www.hhs.gov/ophs/oah/prevention/research/index.html
80
FAMILY, MATERNAL & CHILD HEALTH
Early Prenatal Care
Pregnant Hispanic and African American women
were less likely to receive first trimester
prenatal care compared to pregnant women
in the county overall.
• Contra Costa’s percentage of pregnant women who began prenatal care during the first
trimester did not meet the Healthy People 2010 objective.
• A greater percentage of women residing in Contra Costa received prenatal care in the
first trimester compared to California.
• Pregnant women residing in Bay Point, Pittsburg, Antioch and Concord had lower rates
of first trimester prenatal care than the county overall.
Between 2005 and 2007, 86.1% (34,588) of pregnant women residing in Contra Costa began prenatal
care during their first trimester of pregnancy. On average, 11,529 women residing in Contra Costa
began prenatal care during their first trimester (early prenatal care) each year. This means that 5,605
pregnant women, an average of 1,868 each year, did not receive prenatal care at all during their pregnancy, started prenatal care after the first trimester, or their care status was unknown.
Contra Costa’s percentage of pregnant women who received first-trimester prenatal care between 2005
and 2007 (86.1%) was higher than the percentage of women in the state who received early prenatal
care during the same period (84.0%) but did not meet the Healthy People 2010 objective (90%).1
Table 1 Women in early prenatal care by
race/ethnicity
Contra Costa 2005–2007
Cases
Percent
White
13,167
38.1%
91.7*
Hispanic
11,637
33.6%
80.3**
Asian/Pacific Islander
5,281
15.3%
89.0*
African American
2,914
8.4%
81.4**
34,588
100.0%
Total
These are unadjusted crude rates per 100 live births.
Total includes some racial/ethnic groups not listed.
* Significantly higher rate than the county.
** Significantly lower rate than the county.
81
Rate
86.1
In this section,
“pregnant
women” refers
to all women
who eventually
gave birth to a
live infant and
does not include
women whose
pregnancies ended
in miscarriage,
abortion or fetal
death.
FAMILY, MATERNAL & CHILD HEALTH
The highest number of women in the county who obtained early prenatal care were white (13,167),
followed by Hispanic (11,637), Asian/Pacific Islander (5,281) and African American (2,914). African
American (81.4 per 100 live births) and Hispanic women (80.3 per 100 live births) had lower rates of
early prenatal care compared to women in the county overall (86.1 per 100 live births).
The rate of early prenatal care for white women (91.7 per 100 live births) and Asian/Pacific Islander
women (89.0 per 100 live births) were higher than the county rate.
Table 2 Women in early prenatal care by city
Contra Costa County 2005–2007
Cases
Percent
Rate
Concord
4,358
12.6%
80.5**
Richmond
4,064
11.7%
84.9
Antioch
3,902
11.3%
82.4**
Pittsburg
2,630
7.6%
79.1**
San Pablo
1,954
5.6%
84.3
Brentwood
1,921
5.6%
88.3*
Walnut Creek
1,915
5.5%
92.0*
Martinez
1,284
3.7%
88.3*
Oakley
1,176
3.4%
84.9
Pleasant Hill
1,079
3.1%
94.1*
Bay Point
942
2.7%
76.3**
Hercules
791
2.3%
90.2*
El Cerrito
740
2.1%
91.7*
Pinole
471
1.4%
85.9
34,588
100.0%
86.1
Total
Prenatal care
initiated during the
first three months
of pregnancy —the
first trimester —is
considered “early
prenatal care” or
“early entry into
prenatal care.”
These are unadjusted crude rates per 100 live births.
Total includes cities and unincorporated areas not listed
* Significantly higher rate than the county.
** Significantly lower rate than the county.
The rate of early prenatal care also varied by community. Bay Point (76.3 per 100 live births), Pittsburg
(79.1 per 100 live births), Concord (80.5 per 100 live births) and Antioch (82.4 per 100 live births) women
had lower rates of early prenatal care than women in the county overall (86.1 per 100 live births). The
women of Pleasant Hill (94.1 per 100 live births), Walnut Creek (92.0 per 100 live births), El Cerrito
(91.7 per 100 live births), Hercules (90.2 per 100 live births), Brentwood (88.3 per 100 live births) and
Martinez (88.3 per 100 live births) had higher rates of early prenatal care than county women overall.
82
FAMILY, MATERNAL & CHILD HEALTH
What is early prenatal care?
Early entry into prenatal care occurs when a woman starts medical prenatal care within the first
trimester (or first 12 weeks) of pregnancy. Early entry into prenatal care is often called early prenatal care.
Why is it important?
Prenatal care is important for the health of both the mother and the baby. During prenatal care,
health care providers monitor the health of the mother and baby and identify and treat health conditions and issues that could impact the pregnancy. It is also an important time for providers to
educate mothers on a variety of health issues related to pregnancy, such as smoking, alcohol use,
exercise, nutrition, preparing for childbirth, and infant care and feeding.
Prenatal care is more likely to be effective if it is initiated early in pregnancy.2 Women who start
prenatal care in the last trimester are more likely to have babies with health problems. Women
who receive no prenatal care are more likely to have low birth weight babies, and these babies are
at greater risk of dying.3
Who does it impact the most?
Women may experience a variety of barriers to obtaining early prenatal care. In general, these barriers fall into four broad categories: (1) financial/economic issues (including problems with private
and public insurance programs and lack of insurance altogether), (2) inadequate capacity, primarily
within prenatal care systems relied upon by low-income women, (3) organization, practices and atmosphere of prenatal services (including policies and provider attitudes as well as issues such as
transportation and child care), and (4) cultural or personal factors that can limit prenatal care use.4
Rates of early prenatal care differ between racial/ethnic groups and by maternal age. In the United
States from 2000–2002, white women had the highest rates of early prenatal care (88.6%), followed
by Asians (84.4%), Hispanics (75.7%), Blacks (74.6%) and Native Americans (69.4%). In addition, teen
mothers have lower rates of early prenatal care (69.1%) compared to all women (83.4%).5
What Can We Do About It?
Early entry into prenatal care is a key factor in ensuring that pregnant women are healthy and have
healthy babies. Given that the goal of prenatal care is positive birth outcomes and healthy mothers,
strategies toward this end ideally include a focus on social determinants of health, health equity
and the Life Course Perspective. The Life Course Perspective suggests that perinatal outcomes are
determined by the entire life course of the woman prior to pregnancy, not just the nine months of
pregnancy. Efforts that focus more broadly on social determinants of health serve to address the
complex interplay of social, behavioral, biological and environmental factors that influence health
in a community. Medical care alone is not enough to address the cumulative risk factors that a
83
FAMILY, MATERNAL & CHILD HEALTH
woman may have encountered over her life’s course. The Life Course Perspective proposes that public
health efforts to reduce inequities in perinatal outcomes focus on:6
• Access to quality health care across the life span, including before, during and between pregnancies.
• Enhancing family and community systems that can have broad impacts on families and communities
(e.g., father involvement, integration of family support services, reproductive social capital,
community building).
• Addressing social and economic inequities that impact health (e.g., education, poverty, support
for working mothers, racism).
Data Sources: Early Prenatal Care
tables
Tables 1, 2: Birth data from the California Department of Public Health (CDPH), Birth Statistical Master Files, 2005-2007.
Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation
(CHAPE) Unit of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include Hispanic
residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic
residents. Not all races/ethnicities shown but all are included in totals for the county and for each city. These tables
include total number of women residing in Contra Costa who initiated prenatal care in the first trimester and average
crude early prenatal rates for 2005 through 2007. Early prenatal care rate is the number of mothers who began prenatal
care during the first trimester of pregnancy divided by the number of live births multiplied by 100.
text
1.
2.
3.
4.
5.
6.
California Department of Public Health, Death and Birth Records. (2009) Vital Statistics Query System. Retrieved
from http://www.applications.dhs.ca.gov/vsq/ on January 8, 2010.
National Center for Health Statistics. Healthy People 2010 final review. Hyattsville (MD): Public Health Service, 2001.
Available at http://www.healthypeople.gov/Document/HTML/Volume2/16MICH.htm#_Toc494699665
Maternal and Child Health Bureau, Health Resources and Services Administration, U.S. Department of Health and
Human Services. “A Healthy Start: Begin Before Baby’s Born.” Accessed September 27, 2005.
http://www.mchb.hrsa.gov/programs/womeninfants/prenatal.htm
Institute of Medicine. Prenatal Care: Reaching Mothers, Reaching Infants. Sarah Brown, editor. Division of Health
Promotion and Disease Prevention. National Academy Press, Washington, D.C. 1988.
March of Dimes. Peristats, Quick Facts, Prenatal Care. Available at http://www.marchofdimes.com/peristats/level1.as
px?reg=99&top=5&stop=24&lev=1&slev=1&obj=1
Lu M, Kotelchuck M, Hogan V, Jones L, Jones CP, Halfon N. Closing the Black-white gap in birth outcomes: A lifecourse approach. Accepted for publication in Ethnicity and Disease. 2010.
84
FAMILY, MATERNAL & CHILD HEALTH
Low Birth Weight Infants
African American mothers were most likely
to have a low birth weight baby.
• African Americans had the highest rate of low birth weight infants.
• Richmond mothers were more likely to have low birth weight infants than mothers in
the county overall.
• Contra Costa’s percentage of low birth weight babies did not meet the Healthy People
2010 objective.
From 2005 to 2007, there were 40,193 live births per year in the county; of these 2,712 (6.7%) were
low birth weight. This means that on average 904 low birth weight babies were born to residents of
Contra Costa each year. Contra Costa’s low birth weight percentage (6.7%) was similar to California’s
percentage (6.9%) for the same period but did not meet the Healthy People 2010 objective (5.0%).1
Table 1 Low birth weight by race/ethnicity
Contra Costa County 2005–2007
Cases
Rate
White
861
6.0 **
Hispanic
830
5.7 **
African American
444
12.4 *
Asian/Pacific Islander (API)
432
7.3
2,712
6.7
Total
Infants weighing
less than 2,500
grams (5 lbs.
8 oz.) are
considered low
birth weight.
These are unadjusted crude rates per 100 live births.
Total includes some racial/ethnic groups not shown.
* Significantly higher rate compared to county.
** Significantly lower rate compared to county.
In Contra Costa, the greatest numbers of low birth weight infants were white (861), followed by
Hispanic (830). Even though African American women had fewer low birth weight infants (444),
they had the highest rate of low birth weight infants (12.4 per 100 live births)—higher compared to
the county overall (6.7 per 100 live births), and any other race/ethnicity group listed. The rates of low
birth weight among Hispanics (5.7 per 100 live births) and whites (6.0 per 100 live births) were lower
than the county overall.
85
FAMILY, MATERNAL & CHILD HEALTH
Table 2 Low Birth Weight Births by Selected communities
Contra Costa County 2005–2007
Cases
Percent
Rate
Richmond
382
14.1%
8.0*
Concord
321
11.8%
5.9
Antioch
315
11.6%
6.6
Pittsburg
239
8.8%
7.2
San Pablo
173
6.4%
7.5
Brentwood
159
5.9%
7.3
Walnut Creek
147
5.4%
7.1
Pleasant Hill
90
3.3%
7.8
Oakley
84
3.1%
6.1
Martinez
79
2.9%
5.4
Bay Point
75
2.8%
6.1
Hercules
60
2.2%
6.8
El Cerrito
40
1.5%
5.0**
Pinole
36
1.3%
6.6
2,712
100.0%
6.7
Contra Costa
These are unadjusted crude rates per 100 live births.
Contra Costa total includes cities and unincorporated areas not shown.
* Significantly higher rate compared to county.
** Significantly lower rate compared to county.
Communities with the greatest number of low birth weight infants were Richmond (382), Concord
(321), Antioch (315) and Pittsburg (239).
Richmond had a rate of low birth weight (8.0 per 100 live births) that was significantly higher than
the county rate overall (6.7 per 100 live births). El Cerrito had a rate of low birth weight (5.0 per 100
live births) that was significantly lower than the county rate overall.
86
FAMILY, MATERNAL & CHILD HEALTH
Table 3 Low birth weight births in selected communities by race/ethnicity
Contra Costa County 2005–2007
White
Cases
Richmond
Cases
African American
Rate
Cases
Rate
API
Total
Cases
Rate
Cases
Rate
4.0 **
151
6.0
157
14.4 *
31
6.7
382
8.0*
Concord
117
6.0
122
5.0 **
20
12.3 *
49
7.7
321
5.9
Antioch
90
6.8
99
4.9 **
76
11.4 *
38
7.3
315
6.6
Pittsburg
29
6.1
100
5.5
62
12.8 *
35
7.9
239
7.2
San Pablo
12
NA
89
6.0
45
15.2 *
22
7.3
173
7.5
Brentwood
67
6.2
56
7.8
10
NA
18
NA
159
7.3
Walnut Creek
92
7.0
24
8.6
NA
NA
21
5.5
147
7.1
Pleasant Hill
51
7.0
12
NA
NA
NA
23
11.3
90
7.8
Oakley
22
4.0 **
47
7.2
7
NA
NA
NA
84
6.1
Martinez
46
5.2
21
6.6
NA
NA
7
NA
79
5.4
Bay Point
10
NA
42
5.3
9
NA
12
NA
75
6.1
Hercules
11
NA
10
NA
11
NA
27
6.7
60
6.8
El Cerrito
17
NA
NA
NA
NA
NA
15
NA
40
5.0**
12
NA
7
NA
11
NA
5
NA
36
6.6
861
6.0
830
5.7
444
12.4
432
7.3
2,712
6.7
Pinole
Contra Costa
21
Rate
Hispanic These are unadjusted crude rates per 100 live births.
Contra Costa race/ethnicity totals includes some cities not shown.
Contra Costa and city totals includes some racial/ethnic groups not listed.
* Significantly higher rate compared to county.
** Significantly lower rate compared to county.
The number of low birth weight babies born to African American mothers was highest in Richmond
(157), Antioch (76), Pittsburg (62), San Pablo (45) and Concord (20). The rate of low birth weight infants
born to African American mothers in San Pablo (15.2 per 100 live births), Richmond (14.4 per 100 live
births), Pittsburg (12.8 per 100 live births), Concord (12.3 per 100 live births) and Antioch (11.4 births
per 100 live births) was higher than the low birth weight rate for the county and for each of the respective
cities overall.
The number of low birth weight babies born to Asian/Pacific Islander mothers was highest in Concord
(49), Antioch (38), Pittsburg (35), Richmond (31) and Hercules (27).
The number of low birth weight babies born to Hispanic mothers was highest in Richmond (151),
Concord (122), Pittsburg (100), Antioch (99) and San Pablo (89). Although these numbers were high,
the low birth weight rates for Hispanics in Antioch (4.9 per 100 live births) and Concord (5.0 per 100
live births) were lower than the county overall.
The number of low birth weight babies born to white mothers was highest in Concord (117), Walnut
Creek (92), Antioch (90), Brentwood (67) and Pleasant Hill (51). White mothers in Oakley and
Richmond (both 4.0 per 100 live births) had lower rates of low birth weight than the county overall.
87
FAMILY, MATERNAL & CHILD HEALTH
What is low birth weight?
Low birth weight is defined as less than 2,500 grams, or approximately 5.5 lbs. Often, low birth weight is
further broken down into moderately low birth weight (1,500 to 2,499 grams) and very low birth weight
(less than 1,500 grams, or 3.3 lbs.) An infant may be born with a low birth weight due to preterm birth
(birth before 37 weeks gestation) or fetal growth restriction (also known as small-for-gestational age).
Why is it important?
Infants who are born low birth weight often face serious health problems as newborns and are at greater
risk of dying compared to normal weight infants. Low birth weight infants are also at increased risk of
long-term disability and impaired or delayed development. The long-term effects of being born low birth
weight include increased risk of having a learning disability, being enrolled in special education classes, having a lower IQ and dropping out of high school.2 The risk for many of these problems is greater
for very low birth weight babies. Low birth weight may also contribute to chronic health problems in
adulthood, such as high blood pressure, type 2 diabetes and heart disease.3,4,5 Furthermore, females
who are born low birth weight are at increased risk of delivering a low birth weight baby, thereby perpetuating these risks across generations.4
Who does it impact the most?
Low birth weight is associated with various medical, socioeconomic, behavioral and environmental
risk factors such as smoking, low maternal weight gain or low pre-pregnancy weight, maternal or fetal
stress, infections and violence.2 Smoking is a significant contributor to low birth weight and accounts
for 20% to 30% of all low birth weight births in the United States.6
In the United States, there are significant inequities in rates of low birth weight between racial/ethnic
groups. Data from 2007 indicate that in the United States, non-Hispanic black women had the highest
rates of low birth weight (13.9%), almost two times that of other racial/ethnic groups.7 Traditionally,
inequities in birth outcomes have only been partially explained by pregnancy-related factors such as
smoking, maternal age, education, and quality and frequency of prenatal care. The Life Course Perspective suggests that these inequities result from a complex interplay of biological, behavioral, psychological and social protective and risk factors at play throughout women’s lives.8 One example supporting
this model is recent research that has shown chronic psychosocial stress, such as racial discrimination,
is associated with low birth weight.9,10
What can we do about it?
An important component of reducing low birth weight and other birth outcomes is reducing inequities
between racial/ethnic groups. Historically, efforts to address inequities in birth outcomes, such as low
birth weight, have focused on increasing access to prenatal care, however this has not reduced these
inequities.11 The Life Course Perspective suggests that birth outcomes are determined by the entire life
course of the woman prior to pregnancy, not just the nine months of pregnancy. As such, efforts to
improve birth outcomes should focus on factors at play throughout the life span. The Life Course Perspective proposes that public health efforts to reduce inequities in birth outcomes focus on:11
88
FAMILY, MATERNAL & CHILD HEALTH
• Access to quality health care across the life span, including before, during and between pregnancies.
• Enhancing family and community systems that can have broad impacts on families and communities
(e.g., father involvement, integration of family support services, reproductive social capital,
community building).
• Addressing social and economic inequities that impact health (e.g., education, poverty, support
for working mothers, racism).
Data Sources: Low Birth Weight Infants
tables
Tables 1, 2, 3: Birth data from the California Department of Public Health (CDPH), Birth Statistical Master Files,
2005-2007. Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning
and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include
Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include
non-Hispanic residents. Not all race/ethnicities shown but all are included in totals for the county and for each city. These
tables include total low birth weight births to females who are residents of Contra Costa and average crude low birth
weight rates for 2005 through 2007.
Crude low birth weight rate is the number of infants weighing less than 2,500 grams divided by the total number of live
births multiplied by 100.
text
1.
California Department of Public Health, Death and Birth Records. (2009) Vital Statistics Query System. Retrieved
from http://www.applications.dhs.ca.gov/vsq/ on January 8, 2010.
2. Child Trends. Low and Very Low Birthweight. 2010. Available at
www.childtrendsdatabank.org/?q=node/246.
3. March of Dimes. Fact Sheet: Low Birthweight. May 2008.
http://www.marchofdimes.com/professionals/14332_1153.asp
4. Collins JW, David, RJ, Pranchand NG, Pierce ML. Low birth weight across generations. Maternal and Child Health
Journal. December 2003; 7, 4; 229-237.
5. Rich-Edwards, JW, Colditz GA, Stampfer MJ, Willett WC, Gillman MW, Hennekens CH, Speizer FE, Manson
JE. Birthweight and the risk for type 2 diabetes mellitus in adult women. Annals of Internal Medicine. 1999;
130,4:278-284.
6. National Center for Health Statistics. Healthy People 2010 final review. Hyattsville (MD): Public Health Service, 2001.
Available at http://www.healthypeople.gov/Document/HTML/Volume2/16MICH.htm#_Toc494699665
7. NCHS: Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Mathews TJ, Kirmeyer S, Osterman MJ. (2010). “Births:
Final data for 2007.” National Vital Statistics Reports, 58(24). Hyattsville, MD: National Center for Health Statistics.
http://www.cdc.gov/nchs/data/nvsr/nvsr57/nvsr57_12.pdf
8. Contra Costa Health Services. Family, Maternal and Child Health Programs Life Course Initiative, An Overview.
October 2009.
9. Bryant Borders AR, Grobman WA, Amsden LB, Holl JL. Chronic stress and low birth weight neonates in a lowincome population of women. Obstetrics & Gynecology. February 2007; 109, 2: 331-338.
10. Mustillo S, Kieger H, Gunderson EP, Sidney S, McCreath H, Kiefe CI. Self-reported experiences of racial
discrimination and Black-white differences in preterm and low-birthweight deliveries: The CARDIA Study. American
Journal of Public Health. December 2004; 94,12: 2125-2131.
11. Lu M, Kotelchuck M, Hogan V, Jones L, Jones CP, Halfon N. Closeing the Black-white gap in birth outcomes: A lifecourse approach. Accepted for publication in Ethnicity and Disease. 2010.
89
FAMILY, MATERNAL & CHILD HEALTH
Fetal and Infant Death
Fetal and infant death was most likely to occur
among African American mothers.
• On average, there were 77 fetal deaths, and 58 infant deaths per year.
• Contra Costa’s fetal mortality rate did not meet the Healthy People 2010 objective.
• Contra Costa’s infant mortality rate was lower than the rate for California and met the
Healthy People 2010 objective.
Fetal Death
Between 2005 and 2007 there were 231 fetal deaths in Contra Costa —an average of 77 per year. The
fetal mortality rate for the county was 5.7 per 1,000 live births and fetal deaths. The county rate was
similar to that of California’s 2005–2007 rate (5.2 per 1,000 live births and fetal deaths) and did not
meet the Healthy People 2010 objective (4.1 per 1,000 live births and fetal deaths).
Table 1 Fetal Deaths by Race/Ethnicity
Contra Costa County 2005 –2007
Deaths
Percent
Total births
Rate
White
74
32.0%
14,429
5.1
Hispanic
71
30.7%
14,556
4.9
African American
43
18.6%
3,625
Asian/Pacific Islander
27
11.7%
5,958
4.5
231
100.0%
40,424
5.7
Total
The fetal death rate
includes deaths
occurring 20 weeks
after conception
but before birth.
11.9 *
These are unadjusted crude rates per 1,000 live births plus fetal deaths.
Total births includes live births plus fetal deaths.
Total includes some racial/ethnic groups not shown.
* Significantly higher rate than the county.
In Contra Costa County, the greatest number of fetal deaths occurred among whites (74), followed by
Hispanics (71), African Americans (43) and Asians/Pacific Islanders (27). Although African Americans
had a lower number of fetal deaths, African Americans had the highest rate of fetal deaths (11.9 per
1,000 live births and fetal deaths). This rate was higher than the county rate overall (5.7 per 1,000 live
births and fetal deaths) and higher than any other race/ethnic group listed.
90
FAMILY, MATERNAL & CHILD HEALTH
Infant Death
There were 173 infant deaths in Contra Costa between 2005 and 2007—an average of 58 per year. The
infant mortality rate for the county was 4.3 per 1,000 live births. The county rate was lower than the
California rate for 2005–2007 (5.2 per 1,000 live births) and met the Healthy People 2010 objective
(4.5 per 1,000 live births).1
Table 2 Infant Deaths by Race/Ethnicity
Contra Costa County 2005–2007
Deaths
Percent
Live births
Rate
Hispanic
57
32.9%
14,485
African American
41
23.7%
3,582
White
41
23.7%
14,355
2.9
Asian/Pacific Islander
13
7.5%
5,931
NA
173
100.0%
40,193
4.3
Total
3.9
11.4 *
Infant deaths are
deaths to live-born
babies younger than
1 year old.
These are unadjusted crude rates per 1,000 live births.
Total includes some racial/ethnic groups not shown.
* Significantly higher rate than the county.
In Contra Costa, the greatest number of infant deaths occurred among Hispanics (57), followed by
African Americans (41), whites (41), and Asians/Pacific Islanders (13). Although Hispanics had the
highest number of infant deaths, African Americans had the highest rate of infant death (11.4 per
1,000 live births). The African American rate was higher than the county rate overall (4.3 per 1,000
live births), more than three times the rate of whites (2.9 per 1,000 live births) and higher than any
other racial/ethnic group listed.
Infant deaths are divided into two groups—those that occur to infants younger than 28 days old
(neonatal deaths) and those that occur to infants 28 days to 1 year old (post-neonatal deaths). Of the
173 infant deaths that occurred in Contra Costa between 2005 and 2007, 115 (66.5%) occurred in the
first 27 days of life (neonatal).
Although Hispanics had the greatest number of neonatal deaths (41), African Americans had the highest
neonatal death rate (6.4 per 1,000 live births). This rate for African Americans was higher than the rate
for the county overall (2.9 per 1,000 live births) and higher than any other racial/ethnic group listed. The
neonatal death rate for whites (1.5 per 1,000 live births) was lower than the county rate.
91
FAMILY, MATERNAL & CHILD HEALTH
Table 3 Neonatal deaths by race/ethnicity
Contra Costa County 2005–2007
Deaths
Percent
Live births
Rate
Hispanic
41
35.7%
14,485
2.8
African American
23
20.0%
3,582
6.4*
White
22
19.1%
14,355
1.5**
Asian/Pacific Islander
12
10.4%
5,931
NA
115
100.0%
40,193
2.9
Total
These are unadjusted crude rates per 1,000 live births.
Total includes some racial/ethnic groups not shown
* Significantly higher rate than the county.
** Significantly lower rate than the county.
In Contra Costa, 58 infant deaths (33.5%) occurred between 28 days and one year of life (post-neonatal).
The overall county rate of post-neonatal deaths was 1.4 per 1,000 live births.
Table 4 Post-neonatal deaths by race/ethnicity
Contra Costa County 2005–2007
Deaths
Percent
Live births
Rate
White
19
32.8%
14,355
NA
African American
18
31.0%
3,582
NA
Hispanic
16
27.6%
14,485
NA
Total
58
100.0%
40,193
1.4
These are unadjusted crude rates per 1,000 live births.
Total includes some racial/ethnic groups not shown.
In Contra Costa, the most frequent categories for cause of infant death were:
• Congenital malformations, deformations and chromosomal abnormalities (31 deaths,
17.9% of total infant deaths 2005–2007)
• Disorders related to short gestation/low birth weight—necrotizing enterocolitis (26
deaths, 15% of total infant deaths 2005–2007)
• Sudden infant deaths syndrome (17 deaths, 9.8% of total infant deaths 2005–2007)
What is it?
A fetal death is a spontaneous intrauterine death that occurs prior to birth. In California, data on fetal
deaths are restricted to deaths that occur at 20 weeks gestation or older and do not include induced
terminations. An infant death is a death that occurs to a live-born baby younger than 1 year of age.
Infant deaths do not include fetal deaths.
92
FAMILY, MATERNAL & CHILD HEALTH
Why is it important?
Infant mortality is considered a critical measure of a community’s social and economic well-being, as
well as its health. It reflects a range of factors such as medical issues, the ability of health care systems to respond to the needs of women and infants, environmental factors, and social issues such as
poverty, education and culture. Furthermore, infant mortality tells us something about women’s lives—
their lifestyle and personal habits, their relationships and the stress they experience.2 Many of these
factors also impact fetal mortality, however fetal deaths are less understood than infant deaths. Since
infant deaths only include live-born infants, examining both fetal and infant mortality can provide a
more complete picture of perinatal health.
Who does it impact the most?
Low birth weight and prematurity accounted for almost 20% of all infant deaths in the United States in
2006.3 A variety of socioeconomic, behavioral and medical factors can increase a women’s risk of having
a premature birth or low birth weight baby. These include low income, maternal age (younger than 17
and older than 35 years), smoking, alcohol and drug use, carrying twin and higher-order pregnancies,
infection and chronic health problems.4,5 Many risk factors for infant mortality also apply to fetal mortality.
In the United States, there are significant disparities in fetal and infant mortality rates by race/ethnicity. In 2005, non-Hispanic black women had the highest fetal and infant mortality rates, more than two
times that of non-Hispanic whites.6,7 Traditionally these disparities have been partially explained by
factors such as quality and frequency of prenatal care. The Life Course Perspective suggests that these
disparities result from the differences in a complex interplay of biological, behavioral, psychological
and social protective and risk factors at play throughout women’s lives.8
What can we do about it?
An important component of reducing fetal and infant mortality is reducing inequities between racial/
ethnic groups. Historically, efforts to address inequities in birth outcomes, such as fetal and infant mortality, have focused on increasing access to prenatal care, however this has not reduced these inequities.9 The Life Course Perspective suggests that birth outcomes are determined by the entire life course
of the woman prior to pregnancy, not just the nine months of pregnancy. As such, efforts to improve
birth outcomes should focus on factors at play throughout the life span. The Life Course Perspective
proposes that public health efforts to reduce inequities in birth outcomes focus on:9
• Access to quality health care across the life span, including before, during and between pregnancies.
• Enhancing family and community systems that can have broad impacts on families and communities
(e.g., father involvement, integration of family support services, reproductive social capital,
community building).
• Addressing social and economic inequities that impact health (e.g., education, poverty, support
for working mothers, racism).
93
FAMILY, MATERNAL & CHILD HEALTH
Data Sources: Fetal and Infant Death
tables
Table 1-4: Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning and
Evaluation (CHAPE) Unit of Contra Costa Health Services and not the California Department of Public Health. Data
presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and
African Americans include non-Hispanic residents. Not all race/ethnicities shown but all are included in totals for the
county and for each city. Counts fewer than five are not shown in order to protect anonymity. Rates were not calculated for
any group with fewer than 20 cases due to unstable estimates. Data presented for Hispanics include Hispanic residents of
any race.
Table 1: Fetal death data from the California Department of Public Health (CDPH), Fetal Death Statistical Master Files,
2005–2007. This table includes fetal deaths to women who are residents of Contra Costa and average crude fetal mortality
rates for 2005 through 2007.
Fetal mortality rate is the fetal deaths occurring 20 weeks after conception but before birth divided by total births
multiplied by 1,000. The number of total births is the sum of live births and fetal deaths.
Table 2-4: Infant death data (including neonatal and post-neonatal) from the California Department of Public Health
(CDPH), Death Statistical Master Files, 2005–2007. These tables include infant, neonatal and post-natal deaths to women
who are residents of Contra Costa and average crude infant mortality, neonatal mortality and post-neonatal mortality
rates for 2005 through 2007.
Infant mortality rate is the deaths of infants younger than 1 year of age divided by live births multiplied by 1,000.
Neonatal mortality rate is the deaths of infants younger than than 28 days old divided by live births multiplied by 1,000.
Post-neonatal mortality rate is the deaths of infants 28 or more days old divided by live births multiplied by 1,000.
text
1.
2.
3.
4.
5.
6.
7.
8.
9.
California Department of Public Health, Death and Birth Records. (2009) Vital Statistics Query System. Retrieved
from http://www.applications.dhs.ca.gov/vsq/ on January 8, 2010.
Contra Costa Health Services. Contra Costa Fetal Infant Mortality Review Program. Findings and Accomplishments,
1998–2004. November 2005.
March of Dimes, Peristats. Available at
http://www.marchofdimes.com/peristats/level1.aspx?reg=99&top=6&stop=116&lev=1&slev=1&obj=1&dv=cr.
March of Dimes. Fact Sheet: Low Birthweight. May 2008. http://www.marchofdimes.com/professionals/14332_1153.
asp
March of Dimes. Fact Sheet: Premature Birth. April 2010. Available at
http://www.marchofdimes.com/professionals/14332_1157.asp
MacDorman M, Kirmeyer S. The challenge of fetal mortality. NCHS data brief, no 16. Hyattsville, MD: National
Center for Health Statistics. 2009. Available at http://www.cdc.gov/nchs/data/databriefs/db16.htm
MacDorman MF, Mathews TJ. Recent Trends in Infant Mortality in the United States. NCHS data brief, No 9.
Hyattsville, MD: National Center for Health Statistics. 2008. Available at
http://www.cdc.gov/nchs/data/databriefs/db09.htm#arethere.
Contra Costa Health Services. Family, Maternal & Child Health Programs Life Course Initiative, An Overview.
October 2009.
Lu M, Kotelchuck M, Hogan V, Jones L, Jones CP, Halfon N. Closeing the Black-white gap in birth outcomes: A lifecourse approach. Accepted for publication in Ethnicity and Disease. 2010.
94
FAMILY, MATERNAL & CHILD HEALTH
Breastfeeding
• African American babies were least likely to be breastfed in the hospital.
• In the San Francisco Bay Area, low-income mothers were less likely to breastfeed their
babies than higher-income mothers.
In 2006, 12,147 babies born in Contra Costa hospitals were breastfed, formula fed or some combination of the two before being discharged from the hospital. Of these, 11,318 were breastfed at least
once. The percentage of babies who were breastfed during this period (93.2%) was higher than the
California percentage (86.5%).1 Both the county and the state met the Healthy People 2010 objective
for breastfeeding in early postpartum (75%).2
While a high percentage of babies were breastfed, nearly one third of these were also formula fed before
being discharged from the hospital. Just 62.2% (7,556) of the 12,147 babies were breastfed exclusively
until they left the hospital.
Table 1 Breastfeeding in hospital by race/ethnicity
Contra Costa County hospitals, 2006
Any Breastfeeding
Number Prevalence
Hispanic
4,153
94.8%
White
3,877
Asian/Pacific Islander
African American
Total
*
Exclusive Breastfeeding
Number
Prevalence
2,650
60.5%
92.9%
2,755
66.0%
1,236
94.8%
792
60.7%
895
84.6%
566
53.5% **
11,318
93.2%
**
7,556
*
62.2%
Total includes some racial/ethnic groups not shown.
* Significantly higher rate compared to county.
** Significantly lower rate compared to county.
In Contra Costa, the greatest number of babies breastfed before discharge were Hispanic (4,153) followed
by white (3,877), Asian/Pacific Islander (1,236), and African American (895). A higher percentage of
Hispanic babies (94.8%) were breastfed before discharge compared with babies in the county overall
(93.2%). African American babies had the lowest percentage of breastfeeding before discharge (84.6%),
lower than the county and any other race/ethnicity group listed.
White babies had the highest percentage of exclusively breastfeeding before discharge (66.0%) higher
than babies in the county overall (62.2%) and any other race/ethnicity group listed. African American
babies had the lowest percentage of exclusive breastfeeding before discharge (53.5%), lower than the
county and any other race/ethnicity listed.
95
FAMILY, MATERNAL & CHILD HEALTH
Table 2 Breastfeeding in hospital by facility
Contra Costa County hospitals, 2006
Any Breastfeeding
Number Prevalence
Kaiser Permanente
Walnut Creek Medical
Center
John Muir Memorial
Hospital
Contra Costa Regional
Medical Center
Exclusive
Breastfeeding
Number Prevalence
3,974
2,442
96.0%*
92.3%
2,848
1,476
68.8%*
55.8%
1,803
93.2%
976
50.5%**
Sutter Delta Medical
Center
748
85.6%**
440
50.3%**
San Ramon Regional
Medical Center
747
94.3%
421
53.2%**
Doctors Medical Center—
San Pablo
372
84.4%**
174
39.5%**
Total
11,318
93.2%
7,556
62.2%
Total includes some cases not assigned to facilities listed.
* Significantly higher rate compared to county.
** Significantly lower rate compared to county.
Babies in the Kaiser Permanente Walnut Creek Medical Center had a higher percentage of breastfeeding
(96.0%) and exclusive breastfeeding (68.8%) before discharge than babies in the county overall (93.2%
and 62.2%, respectively).
They also had a higher percentage of exclusive breastfeeding than any other facility listed. Babies at Sutter
Delta Medical Center and Doctors Medical Center—San Pablo had a lower percentage of breastfeeding
and exclusive breastfeeding before discharge than babies in the county overall. Babies in Contra Costa
Regional Medical Center and San Ramon Regional Medical Center had breastfeeding percentages
similar to the county overall but exclusive breastfeeding rates that were lower than the county’s.
Editor’s note: Analyses of breastfeeding practices at 3, 6 and 12 months for Contra
Costa were not possible due to small sample size, but we can look at Northern
California percentages to get an idea of what is happening locally and make
comparisons to the state and nation.
96
FAMILY, MATERNAL & CHILD HEALTH
Table 3 Breastfeeding Percentages, 2006
6 months
12 months
Northern California
58.6%
33.4%
California
53.6%
31.9%
United States
43.5% **
22.7% **
Healthy People 2010 objective
50%
25%
** Significantly lower rate than Northern California.
In 2006, 58.6% of Northern California babies were still being breastfed at 6 months. This percentage
was similar to California’s percentage (53.6%) and higher than the nation’s (43.5%). Both Northern
California and California as a whole met the Healthy People 2010 objective of 50% of babies being
breastfed at 6 months; the United States did not.
At 12 months, the percentage of Northern California babies being breastfed (33.4%) was still similar
to California’s (31.9%) and higher than that of the United States (22.7%). Again, Northern California
and California as a whole met the Healthy People 2010 objective (25%), while the nation did not.
Table 4 Exclusive breastfeeding percentages, 2006
3 months
6 months
Northern California
48.8%
26.1%
California
42.5%
20.0%
United States
33.6% **
14.1% **
Healthy People 2010 objective
40%
17%
** Significantly lower rate than Northern California.
In 2006, 48.8% of Northern California babies were exclusively breastfed at 3 months and 26.1% were
exclusively breastfed at 6 months. These percentages were similar to those for all of California (42.5%
and 20.0%, respectively) and higher than the percentages for the United States (33.6% and 14.1%,
respectively). Both Northern California and California as a whole met the Healthy People 2010 objective
for exclusive breastfeeding at 3 months (40%) and 6 months (17%); the United States did not.
Editor’s note: Analysis of breastfeeding by race/ethnicity was not possible for
Contra Costa due to small sample size, but we can look to the San Francisco Bay
Area to learn more about how breastfeeding practices vary across our community.
97
FAMILY, MATERNAL & CHILD HEALTH
Table 5 Breastfeeding at 2 months by mother’s race/
ethnicity
San Francisco Bay Area, 2005–2006
Any
Exclusive
Asian/Pacific Islander
84.5%
52.4%
White
84.1%
64.2%
*
Latina
76.6%
46.2%
**
African American
62.9%
39.1%
**
Total
80.2%
**
54.1%
Total percentage includes some racial/ethnic groups not shown.
* Significantly higher rate than the San Francisco Bay Area.
** Significantly lower rate than the San Francisco Bay Area.
When their babies were 2 months old, African American mothers had the lowest percentage of
breastfeeding (62.9%), lower than the San Francisco Bay Area as a whole (80.2%) and every other
racial/ethnic group listed. The percentages of African American (39.1%) and Latina (46.2%) mothers
exclusively breastfeeding at 2 months were lower than the San Francisco Bay Area as a whole (54.1%),
while the percentage of white mothers exclusively breastfeeding at 2 months (64.2%) was higher than
the San Francisco Bay Area as a whole.
Table 6 Breastfeeding at 2 months by income
San Francisco Bay Area, 2005–2006
Any
Exclusive
0-100% of Federal Poverty Level
71.7% **
41.5%
**
101-200% of Federal Poverty Level
69.9% **
41.1%
**
201-300% of Federal Poverty Level
83.1%
59.0%
301-400% of Federal Poverty Level
82.5%
53.1%
Over 400% of Federal Poverty Level
88.0%
Total
80.2%
*
65.2%
*
54.1%
Total percentage includes cases with unknown income level.
* Significantly higher rate than the San Francisco Bay Area.
** Significantly lower rate than the San Francisco Bay Area.
Mothers who lived at 0–100% and 101–200% of the Federal Poverty Level had a lower percentage of
breastfeeding (71.7% and 69.9%) and exclusive breastfeeding (41.5% and 41.1%) than the San Francisco
Bay Area overall (80.2% and 54.1%, respectively). In contrast, mothers who lived at over 400% of the
98
FAMILY, MATERNAL & CHILD HEALTH
Federal Poverty Level had higher percentages of breastfeeding (88.0%) and exclusive breastfeeding
(65.2%) compared to the San Francisco Bay Area as a whole.
What is “any” and “exclusive” breastfeeding?
The percentage of women breastfeeding or “any breastfeeding” includes all women who have breastfed
exclusively or have combined breastfeeding with formula or other foods divided by the total number
who have only breastfed, only formula fed, or combined breastfeeding, formula feeding and/or other
foods. The percentage of women “exclusively breastfeeding” are those who have used only breast milk
to feed their infant since birth divided by the total number who have only breastfed, only formula fed,
or any combination breastfeeding, formula feeding, and/or other foods. The percentages for breastfeeding before discharge excluded cases with unknown method of feeding and those using total parenteral
nutrition/hyperalimentation (TPN/Hyperal).
Why is it important?
In addition to the Healthy People 2010 objectives already noted, the American Academy of Pediatrics
recommends exclusive breastfeeding for six months and continued breastfeeding with complementary
solid foods up to 12 months or longer.3
Breastfeeding reduces an infant’s risk for both acute and chronic disease, increases mother-infant
bonding, fosters appropriate growth and development and may increase learning ability and reduce
the risk for obesity. In addition to reduced health care costs, breastfeeding reduces social costs and is
less damaging to the environment than formula feeding.3
Breastfeeding mothers are half as likely to miss a day of work for a sick child compared to mothers of
formula-fed infants.4 So it is possible that increasing breastfeeding percentages may increase productivity. According to an article published in April 2010 in the journal Pediatrics, $13 billion and 911 infant
lives could be saved per year if 90% of U.S. families complied with the medical recommendations to
breastfeed exclusively for 6 months.5
Who does it impact most?
African American women are less likely than the population as a whole to breastfeed or exclusively
breastfeed in the hospital and at 2 months. While Latinas tend to be breastfeeding at similar rates to
the population at 2 months, Latinas are less likely to be exclusively breastfeeding.
Low-income women are less likely to be breastfeeding or exclusively breastfeeding than mothers as a
whole. Similarly, those who were covered through Medi-Cal only during pregnancy were less likely to
be breastfeeding or exclusively breastfeeding at 2 months than mothers who were covered exclusively
by private insurance alone during their pregnancies.6 Women, Infant and Children (WIC) participants
are less likely than non-WIC mothers to initiate breastfeeding or to continue breastfeeding for the recommended length of time.7
99
FAMILY, MATERNAL & CHILD HEALTH
Mothers younger than 24 are less likely to be breastfeeding or to be exclusively breastfeeding at 2 months
than mothers of all ages.6 Mothers with “some high school” or “high school/GED” were also less likely
to be breastfeeding or exclusively breastfeeding at 2 months than mothers in the total population.6
What can we do about it?
Exclusive breastfeeding during the hospital stay is critical to breastfeeding duration.8,9,10
Studies have shown that hospital practices affect breastfeeding duration and exclusivity throughout the
first year of life. Implementation of the 10 evidence-based steps of the Baby Friendly Hospital Initiative
(BFHI), developed by the World Health Organization in 1991, has been shown to increase initiation and
exclusivity of breastfeeding.11 Fewer that 3% of hospitals in the United States, and none in Contra Costa
County, have Baby Friendly Hospital Certification.12
Hospitals that have implemented “baby friendly” policies outlined in the World Health Organization’s
Ten Steps to Breastfeeding Success have higher exclusive breastfeeding rates among women of all races
and ethnicities.13,14
Peer Breastfeeding Counselors have been shown in several studies to improve exclusive breastfeeding rates.15,16
Data Sources: Breastfeeding
tables
Table 1, 2: Number and percentage of breastfeeding women from Newborn Screening Data, 2006, California Department
of Public Health, Center for Family Health, Genetic Disease Screening Program; retrieved 8/26/2010 from http://www.
cdph.ca.gov/data/statistics/Pages/BreastfeedingStatistics.aspx. All nonmilitary hospitals providing maternity services are
required to complete the Newborn Screening Test Form. Infant feeding data presented in this report include all feedings
from birth to time of specimen collection, usually 24 to 48 hours after birth. The table values exclude cases with unknown
method of feeding and cases marked as “TPN/Hyperal” or “Other”.
Table 1: Infant race/ethnicity is based upon mother and father race/ethnicity as reported on the birth certificate. Data
presented for Hispanics include Hispanic residents of any race. Data for county totals shown in this table include
information for all births occurring in that county, including cases in race/ethnicity groups not shown and with missing
race/ethnicity data.
Table 2: Facilities with fewer than 50 births with known type of feeding are not shown.
Table 3,4: Percentage of women breastfeeding from National Immunization Survey, Centers for Disease Control and
Prevention, Department of Health and Human Services; retrieved 8/26/2010 from http://www.cdc.gov/breastfeeding/
data/NIS_data/index.htm. The sample was limited to records with valid responses to the breastfeeding questions. Healthy
People 2010 objectives retrieved 8/26/2010 from http://www.healthypeople.gov/document/html/volume2/16mich.htm
100
FAMILY, MATERNAL & CHILD HEALTH
Table 5,6: Regional Tables from the 2005–2006 Maternal and Infant Health Assessment (MIHA) surveys; retrieved
8/26/2010 from http://www.cdph.ca.gov/data/surveys/Pages/SanFranciscoBayAreaRegion.aspx. San Francisco Bay Area
data includes data from Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano, and Sonoma
counties. Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans include non-Hispanic residents. Not all race/ethnicities shown but all are included in
totals for the region and each income level. The California Maternal and Infant Health Assessment (MIHA) is an annual,
statewide-representative survey of women who recently gave birth to a live infant. It is completed via the mail, with
telephone follow-up to non-respondents. MIHA is administered in English and Spanish only.
text
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
California Department of Public Health, Center for Family Health, Genetic Disease Screening Program, Newborn
Screening Data, 2006; retrieved 8/26/2010 from
http://www.cdph.ca.gov/data/statistics/Pages/BreastfeedingStatistics.aspx.
Centers for Disease Control and Prevention, Health Resources and Services Administration. Healthy People 2010
Maternal, Infant, and Child Health; retrieved 8/26/2010 from http://www.healthypeople.gov/document/html/
volume2/16mich.htm
Breastfeeding and the Use of Human Milk, Section on Breastfeeding, Pediatrics 2005; 115:496-506.
Cohen, Mrtek & Mrtek. Comparison of maternal absenteeism and infant illness rates among breastfeeding and
formula-feeding women in two corporations. American J of Health Promotion 1995; 1092: 148–153.
Bartick, M. Reinhold, A. The Burden of Suboptimal Breastfeeding in the United States: a Pediatric Cost Analysis,
Pediatrics, online April 5, 2010.
California Department of Public Health, Regional Tables from the 2005–2006 Maternal and Infant Health
Assessment (MIHA) surveys; retrieved 8/26/2010 from
http://www.cdph.ca.gov/data/surveys/Pages/SanFranciscoBayAreaRegion.aspx.
Ryan AS, Zhou W. Lower breastfeeding rates persist among supplemental nutrition program for women, infants, and
children participants: 1978–2003. Pediatrics. 2006;117 :1136–1146.
Murray EK, Ricketts S, Dellaport J. Hospital practices that increase breastfeeding duration: results from a populationbased study. Birth 2007; 34: 202–211
Semenic S, Loiselle C. Gottlieb L. Predictors of the duration of exclusive brestfeeding among first-time mothers.
Research in Nursing & Health (published online), March 6, 2008.
Szajewska H, Horvath A. Koletzko B. Kalisz M. Effects of brief exposure to water, breast-milk substitutes, or other
liquids on the success and duration of breasttfeeding: a systematic review. Acta Paediatr. 2006; 95: 145–152.
Braun M. Giugliani, E. Soares, MD et.al. Evaluation of the Impact of the Baby–Friendly Hospital Initiavive on Rates
of Breastfeeding, American Journal of Public Health, 2003;93(8): 12771279
U.S. Baby Friendly Hospitals and Birth Centers http://www.babyfriendlyusa.org/eng/03.html
Murray EK, Ricketts S, Dellaport J. Hospital practices that increase breastfeeding duration: results from a population
–based study. Birth 2007;34:202–211.
Merewood A, Mehta SD, Chamberlain LB et al. Breastfeeding rates in US Baby-Friendly hospitals: results of a
national survey Pediatrics, 2005;116:628–634.)
Sikorski J, Renfrew MJ, Pindoria S, Wade A. Support for breastfeeding mothers (Cochrane Review) The Cochrane
Library, Issue 3, 2004 ab001141
Bronner, Y, Barber T, Miele, L. Breastfeeding Peer Counseling: Rationale for the National WIC Study, J. Human
Lactation 2001; 17: 135–139
101
FAMILY, MATERNAL & CHILD HEALTH
Children’s Oral Health
• Dental disease is more common in U.S. children than any other chronic disease.
• Oral health problems can have negative effects on a child’s general health
and development.
• School absences from dental disease result in school funding losses.
In 2007, 74.6% of school-age children (5–17 years) in Contra Costa had seen a dentist in the previous
six months. This percentage is similar to the percentage for California (70.0%). A higher percentage
of children in the greater Bay Area (78.0%) had seen a dentist in the previous six months compared
to the state.
Table 1 Children visiting dentist in previous six months
Children ages 5 –17 years, 2007
Number
Prevalence
Contra Costa
140,000
74.6%
Greater Bay Area
929,000
78.0%*
California
5,065,000
70.0%
Estimates are not age-adjusted.
* Significantly higher rate than California.
In 2007, 7.7% of children ages 5–17 in the greater Bay Area (an estimated 93,000 children) missed at
least one day of school due to dental problems. This was similar to the percentage (7.0%, an estimated
504,000 children) that missed at least one day of school due to dental problems in the same year in
California.
Editor’s note: Analyses of missed school days was not possible for Contra Costa due
to small sample size, but data from the greater Bay Area and California illustrate
how dental problems affect school attendance.
Table 2 Missed school days due to dental problem
Children ages 5 –17 years, 2007
Greater Bay Area
Students Percentage
California
Students Percentage
No days missed
1,099,000
92.2%
6,736,000
93.0%
One day missed
57,000
4.7%
273,000
3.8%
Two or more days missed
36,000
3.0%
231,000
3.2%
Estimates are not age-adjusted.
102
FAMILY, MATERNAL & CHILD HEALTH
School-Based Oral Health Services
Contra Costa Health Services’ Children’s Oral Health Program is a primary source of free oral health
preventive services in Contra Costa. This program provides school-based services to children prekindergarten through sixth-grade in schools that are located in ZIP codes that have been prioritized
based on multiple poor health outcomes, high rates of poverty and low educational attainment and
have at least 75% of the student population eligible for the Free and Reduced Lunch Program. In the
2009-2010 school year, the Children’s Oral Health Program provided:1
• Classroom education to 10,608 school children on oral hygiene and nutrition.
• Oral health assessments and dental resources to 6,607 children in the county.
• Compilation of data collected during the oral health assessments revealed that:
• 78.5% needed routine dental care every six months
• 14.8% needed to see a dentist within two weeks for early dental problems
• 6.7% needed to see a dentist within 24 hours for urgent or chronic visible dental
problems (with pain or infection)
• 4,089 sealants were placed on 1,079 children’s teeth
• Fluoride varnish was applied to 1,784 children’s teeth
Twice the number of children received free fluoride and sealants from Contra Costa Health Services’
Children’s Oral Health Program in the 2009–2010 school year compared to the 2008–2009 school
year.1 This was accomplished by using limited resources to offer these services to new schools rather
than those who have been served in recent years.
What is oral health?
The World Health Organization defines oral health as “a state of being free from chronic mouth and facial pain, oral and throat cancer, oral sores, birth defects such as cleft lip and palate, periodontal (gum)
disease, tooth decay and tooth loss, and other diseases and disorders that affect the oral cavity”.2
The two leading dental diseases are caries (tooth decay) and the periodontal diseases (gum disease).3
Why is it important?
Dental disease, including untreated cavities, is more common in U.S. children than any other chronic
disease. It is five times more common than asthma and seven times more common than hay fever.4
Maintaining good oral health is important because untreated problems can result in painful infections
and eventually become serious threats to general health.5 Healthy teeth in childhood are vital for proper
nutrition and speech development and children who suffer from dental pain may have difficulty concentrating in school. Promotion of good oral health is also a cost effective use of scarce resources. Every
dollar spent on preventive care may save as much as $50 on emergency and restorative treatments.6
Between 2009 and 2018, annual spending for dental services in the United States is expected to increase 58%, from $101.9 billion to $161.4 billion. Approximately one-third of this money is expected to
be spent on dental services for children.7
103
FAMILY, MATERNAL & CHILD HEALTH
Missed school days due to dental disease have implications for California school children, their schools,
their parents and the economy. Children who are absent from class miss the opportunity to learn and
may fall behind academically. Schools receive funding from the state based on attendance, so when
a child misses school as a result of dental disease, the school district suffers financial consequences.
Statewide, these absences cost local school districts approximately $28.8 million.8 Often, missed school
days mean missed workdays for parents who take children for treatment or care for them at home.
These missed workdays may result in financial loss for the family and lost productivity for the economy
as a whole.
Who does it impact most?
National data indicates that Mexican-American and non-Hispanic Black children ages 2–11 have more
untreated decay and more dental caries in primary teeth compared to their non-Hispanic white counterparts.9 Similarly, the rate of untreated decay and dental caries in primary teeth is higher for children ages 2–11 living below 100% or between 100% and 200% of the federal poverty level than for their
counterparts living above 200% of federal poverty level.9
What can we do about it?
Placement of dental sealants and application of fluoride varnish have been found to be effective in
preventing dental decay and caries.10,11 School-based oral health services can target these services to
populations of greatest need and provide them at no cost to the child. One policy benchmark listed
the placement of sealants and fluoride in high-risk schools as a cost effective way to help prevent
problems from occurring.7
School-based programs can help clients increase access to care and apply for benefits. They may also
refer clients to community providers. In order for this referral system to be effective, however, there
must be an adequate number of community providers willing and able to treat low-income children.
Changes to Denti-Cal and Healthy Families that increase reimbursement rates and decrease administrative burdens would provide a needed incentive for more providers to offer services to this underserved population.
Data Sources: Children’s Oral Health
tables
Tables 1–2: California Health Interview Survey (CHIS) 2007; retrieved 8/20/2010 from http://www.chis.ucla.edu. Greater
Bay Area data includes the following counties: Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa
Clara, Solano and Sonoma.
text
1.
2.
3.
Internal Program Data. Children’s Oral Health Program, Contra Costa Health Services.
World Health Organization (WHO). Definition of oral health. Retrieved 8/20/2010 from
http://www.who.int/topics/oral_health/en/
National Institute of Dental and Craniofacial Research (NIDCR), National Institute of Health. Improving the Nation’s
Oral Health, retrieved 8/20/2010 from http://www.nidcr.nih.gov/DataStatistics/SurgeonGeneral/sgr/chap1.htm
104
FAMILY, MATERNAL & CHILD HEALTH
4.
U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research (NIDCR),
National Institute of Health. Oral Health in America: A report of the Surgeon General
5. U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child
Health Bureau. The National Survey of Children’s Health 2007. Rockville, Maryland: U.S. Department of Health And
Human Services, 2009.
6. Missouri Coalition for Oral Health, Oral Health white Paper (Columbia, MO: Missouri Coalition for Oral Health,
August 2008.
7. The Pew Center on the States (2010). The Cost of Delay: State Dental Policies Fail One in Five Children.
8. Pourat N and Nicholson G.University. Unaffordable Dental Care Is Linked to Frequent School Abscences. Los
Angeles, CA: UCLA Center for Health Policy Research, 2009.
9. Dye BA, Tan S, Smith V, Lewis BG, Barker LK, Thornton–Evans G, et al. Trends in oral health status: United States,
1988–1994 and 1999–2004. National Center for Health Statistics. Vital Health Stat 11(248). 2007.
10. Beauchamp et al., American Dental Association, Council on Scientific Affairs. 2008. Evidence-based clinical
recommendations for the use of pit-and-fissure sealants: A report of the American Dental Association, Council on
Scientific Affairs. Journal of the American Dental Association 139(3): 257–268.
11. Marinho VC et al., Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database of
Systematic Reviews (1): CD002279.
105
CHRONIC DISEASES
Cancers – All Types
Cancer was the leading cause of death
in Contra Costa.
• The most commonly diagnosed cancers in the county were
prostate, breast, lung and colorectal cancer.
• Lung, colorectal, breast and pancreatic cancers were
the most common causes of cancer death.
• Blacks and whites were more likely to be diagnosed with cancer than
county residents overall.
• African Americans were most likely to die from cancer.
• Males were more likely to be diagnosed with and die from cancer than females.
Deaths
Between 2005–2007, cancer was the leading cause of death in Contra Costa accounting for onequarter (25.0%) of all deaths (see Leading Causes of Death section). In Contra Costa, 5,131 residents
died from cancer. This means that an average of 1,710 Contra Costa residents died from cancer each
year. Contra Costa’s age-adjusted cancer death rate (162.0 per 100,000) was lower than California’s
age-adjusted rate (168.6 per 100,000) and was not significantly higher than the Healthy People 2010
objective (158.6 per 100,000).
Table 1 Cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths Percent
White
Rate
3,799
74.0%
175.6*
African American
512
10.0%
228.0*
Asian/Pacific Islander
404
7.9%
16.2**
Hispanic
360
7.0%
100.6**
5,131
100.0%
Total
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
162.0
In this report,
a cancer case
is defined as a
primary malignant
tumor that
originated in the
site or organ
where it was
identified rather
than having spread
from another
location.
The highest number of deaths from cancer in the county occurred among whites (3,799) followed by
African Americans (512), Asians/Pacific Islanders (404) and Hispanics (360).
African Americans had the highest cancer death rate (228.0 per 100,000); higher than the rates for the
county overall (162.0 per 100,000) and all other racial/ethnic groups listed. Whites (175.6 per 100,000)
had a higher cancer death rate than the county overall. Asians/Pacific Islanders (116.2 per 100,000)
and Hispanics (100.6 per 100,000) had lower cancer death rates than the county overall.
106
CHRONIC DISEASES
The number of cancer deaths was higher among females (2,630) than males (2,501) yet males (188.5
per 100,000) had a higher cancer death rate than females (146.0 per 100,000).
Among males, African Americans (258.7 per 100,000) had the highest cancer death rate; higher than
the rates for males in the county overall (188.5 per 100,000) and all other racial/ethnic groups listed.
White males (206.6 per 100,000) also had a higher cancer death rate than males in the county overall.
Hispanic (126.1 per 100,000) and Asian/Pacific Islander males (119.6 per 100,000) had lower cancer
death rates than county males overall.
Table 2 Male cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
1,864
74.5%
206.6*
African American
228
9.1%
258.7*
Asian/Pacific Islander
187
7.5%
119.6**
Hispanic
192
7.7%
126.1**
2,501
100.0%
White
Total
188.5
These are age-adjusted rates per 100,000 male residents.
Total includes males in racial/ethnic groups not listed above.
* Significantly higher rate than county males overall.
** Significantly lower rate than county males overall.
Among females, African Americans (216.5 per 100,000) had the highest cancer death rate; higher than
the rates for females in the county overall (146.0 per 100,000) and females of all other racial/ethnic
groups listed. Hispanic females (83.6 per 100,000) had the lowest cancer death rate; lower than females
in the county overall and than all other racial/ethnic groups listed. Asian/Pacific Islander females (114.6
per 100,000) also had a lower cancer death rate than county females overall.
Table 3 Female cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
1,935
73.6%
156.7
African American
284
10.8%
216.5*
Asian/Pacific Islander
217
8.3%
114.6**
Hispanic
168
6.4%
83.6**
2,630
100.0%
White
Total
These are age-adjusted rates per 100,000 female residents.
Total includes females in racial/ethnic groups not listed above.
* Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
107
146.0
CHRONIC DISEASES
The greatest number of deaths from cancer occurred among people living in Walnut Creek (746),
Concord (614), Richmond (486) and Antioch (430). These four cities accounted for 44.4% of all cancer
deaths in the county.
Four cities had significantly higher cancer death rates than the county overall (162.0 per 100,000):
San Pablo (269.6 per 100,000), Oakley (219.2 per 100,000), Martinez (207.0 per 100,000) and Antioch
(200.8 per 100,000).
Table 4 Cancer deaths by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Walnut Creek
746
14.5%
180.3
Concord
614
12.0%
172.4
Richmond
486
9.5%
177.7
Antioch
430
8.4%
200.8*
Pittsburg
268
5.2%
180.0
Martinez
234
4.6%
207.0*
San Pablo
190
3.7%
269.6*
Brentwood
190
3.7%
169.2
Pleasant Hill
190
3.7%
160.7
El Cerrito
160
3.1%
137.8
Oakley
122
2.4%
219.2*
Pinole
114
2.2%
169.9
Hercules
94
1.8%
149.1
Bay Point
60
1.2%
130.2
5,131
100.0%
162.0
Contra Costa
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
* Significantly higher rate than the county overall.
The leading causes of cancer deaths were lung, colorectal, breast, pancreas and prostate cancers. These
five cancer types accounted for more than half (53.8%) of all cancer deaths in the county. Note: The top
five cancers are covered in more detail in other cancer-specific sections of this report.
108
CHRONIC DISEASES
Table 5 Cancer deaths by cancer type
Contra Costa County, 2005–2007
Deaths
Lung
Percent
1,218
23.7%
Colorectal
517
10.1%
Breast
417
8.1%
Pancreas
341
6.6%
Prostate
270
5.3%
Non-Hodgkins lymphoma
212
4.1%
Leukemia
206
4.0%
Liver and intrahepatic bile ducts
187
3.6%
Bladder
159
3.1%
Ovary
145
2.8%
5,131
100.0%
Total
Total includes deaths from all cancers, including but not limited to those listed
above.
New Cases
To understand the impact of cancer on the community’s health it is important to assess both cancer
diagnoses and deaths. Information about cancer deaths indicates the ultimate toll this disease takes on
people’s lives, but many more people develop cancer than die from it. Information about new cancer
cases provides a sense of how much and among whom the disease is diagnosed and highlights the
need for prevention, screening and treatment programs.
Between 2003–2007, 23,065 new cases of invasive cancer were diagnosed in Contra Costa; an average
of 4,613 new cases per year. The age-adjusted rate of new invasive cancer cases was higher in Contra
Costa (454.2 per 100,000) than California (433.6 per 100,000). Both males and females in the county
had higher rates of new invasive cancer cases (519.3 and 409.0 per 100,000) than males and females
statewide (500.4 and 387.4 per 100,000).
Approximately half (50.5%) of all new invasive cancer cases in the county were among males. Males
in Contra Costa experienced a higher rate of new cancer cases compared to females (519.3 and 409.0
per 100,000, respectively).
109
CHRONIC DISEASES
Table 6 New invasive cancer cases by gender
Contra Costa County, 2003–2007
Cases
Percent
Rate
Males
11,651
50.5%
519.3 *
Females
11,414
49.5%
409.0
Total
23,065
100.0%
454.2
Invasive cancer is
cancer that has
spread beyond
the tissue where
it developed to
surrounding,
healthy tissue.
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than county females.
The greatest number of new invasive cancer cases in Contra Costa occurred among whites (16,676)
followed by Hispanics (2,015), Asians/Pacific Islanders (1,920) and blacks (1,914). Blacks (485.6 per
100,000) and whites (481.2 per 100,000) had higher rates of new invasive cancer cases than the county
overall (454.2 per 100,000). Asians/Pacific Islanders (298.3 per 100,000) had the lowest rate in the
county; lower than the county overall and the other groups listed. Hispanics (361.1 per 100,000) also
had a lower rate of new invasive cancer cases than the county overall.
Table 7 New invasive cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
White
Percent
Rate
16,676
72.3%
481.2 *
Hispanic
2,015
8.7%
361.1 **
Asian/Pacific Islander
1,920
8.3%
298.3 **
Black
1,914
8.3%
485.6 *
Total
23,065
100.0%
454.2
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of new invasive male cancer cases in Contra Costa occurred among white males
(8,454) followed by Hispanic (987), black (977) and Asian/Pacific Islander (869) males. Black (592.7 per
100,000) and white (542.8 per 100,000) men had higher rates of new invasive cancer cases than males
in the county overall (519.3 per 100,000). Asians/Pacific Islanders (317.7 per 100,000) had the lowest
rate of new cancer cases among males; lower than males in the county overall and all other groups
listed. The rate for Hispanic males (419.2 per 100,000) was also lower than males in the county overall.
110
CHRONIC DISEASES
Table 8 New invasive male cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
White
Percent
Rate
8,454
72.6%
542.8 *
Hispanic
987
8.5%
419.2 **
Black
977
8.4%
592.7 *
Asian/Pacific Islander
869
7.5%
317.7 **
11,651
100.0%
Total
519.3
These are age-adjusted rates per 100,000 male residents.
Total includes males in racial/ethnic groups not listed above.
* Significantly higher rate than county males overall.
** Significantly lower rate than county males overall.
The greatest number of new invasive female cancer cases in Contra Costa occurred among white
females (8,222) followed by Asian/Pacific Islander (1,051), Hispanic (1,028) and black (937) females.
Compared to the rate of new invasive cancer cases among females in the county overall (409.0 per
100,000), white females had a higher rate of new cancer cases (438.6 per 100,000). Asian/Pacific
Islander (287.3 per 100,000) and Hispanic (325.6 per 100,000) females had lower rates of new cases
than females in the county overall.
Table 9 New invasive female cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
Rate
White
8,222
72.0%
438.6 *
Asian/Pacific Islander
1,051
9.2%
287.3 **
Hispanic
1,028
9.0%
325.6 **
Black
937
8.2%
410.7
Total
11,414
100.0%
409.0
These are age-adjusted rates per 100,000 female residents.
Total includes females in racial/ethnic groups not listed above.
* Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
The most commonly diagnosed new invasive cancer cases in the county were prostate, breast, lung and
colorectal cancers, which accounted for more than half (55.4%) of all new invasive cancers in the county.
111
CHRONIC DISEASES
Table 10 Most commonly diagnosed new invasive cancers
Contra Costa County, 2003-2007
Cases
Percent
Rate
Prostate
3,908
16.9%
170.0
Breast
3,836
16.6%
73.5
Lung
2,704
11.7%
55.1
Colorectal
2,325
10.1%
46.1
Melanoma of the skin
1,050
4.6%
20.7
Urinary bladder
1,025
4.4%
20.8
Non-Hodgkin’s lymphoma
981
4.3%
19.3
Kidney and renal pelvis
657
2.8%
12.8
Corpus uteri
643
2.8%
22.6
Pancreas
575
2.5%
11.5
23,065
100.0%
454.2
Total
These are age-adjusted rates per 100,000 residents.
Total includes in situ bladder cancer and all new invasive cancers (except basal and squamous cell skin cancers) including but not limited to those listed above.
Table 11 Most commonly diagnosed new female invasive cancers
Contra Costa County, 2003 –2007
Cases
Percent
Rate
Breast
3,820
33.5%
136.1
Lung
1,436
12.6%
52.6
Colorectal
1,160
10.2%
41.0
Corpus uteri
643
5.6%
22.6
Non-Hodgkin’s lymphoma
447
3.9%
16.0
Melanoma of the skin
442
3.9%
16.1
Ovary
355
3.1%
12.7
Pancreas
310
2.7%
11.1
Thyroid
290
2.5%
10.8
Kidney and renal pelvis
247
2.2%
8.9
11,414
100.0%
409.0
Total
These are age-adjusted rates per 100,000 female residents.
Total includes in situ bladder cancer and all new invasive cancers (except basal and squamous cell skin cancers)
including but not limited to those listed above.
112
CHRONIC DISEASES
Table 12 Most commonly diagnosed new male
invasive cancers
Contra Costa County, 2003–2007
Cases
Percent
Rate
Prostate
3,908
33.5%
170.0
Lung
1,268
10.9%
59.7
Colorectal
1,165
10.0%
52.9
Urinary bladder
779
6.7%
37.0
Melanoma of the skin
608
5.2%
27.2
Non-Hodgkin’s lymphoma
534
4.6%
23.7
Kidney and renal pelvis
410
3.5%
17.5
Pancreas
265
2.3%
11.8
Liver and intrahepatic bile duct
232
2.0%
9.8
Stomach
199
1.7%
9.2
11,651
100.0%
519.3
Total
These are age-adjusted rates per 100,000 male residents.
Total includes in situ bladder cancer and all new invasive cancers (except basal and
squamous cell skin cancers) including but not limited to those listed above.
113
CHRONIC DISEASES
What is cancer?
Cancer includes more than 100 diseases, characterized by the uncontrolled growth and spread of abnormal cells. These cells typically form a lump or mass called a malignant tumor, although some cancers
such as leukemia, a cancer of the bone marrow and blood, do not involve tumors.1,2
Why is it important?
Cancer is the leading cause of death in Contra Costa and the second leading cause of death in California and the United States.1,3,4 Cancer accounts for approximately one in four deaths locally, statewide
and nationally.1,5,6
Despite declining rates of new cancer cases and cancer deaths in the state, cancer continues to impact
many people.1 More than 1.2 million Californians living today have survived or are living with cancer and it
is estimated that one in two Californians born today will be diagnosed with cancer at some point in life.1
In addition to the human toll there are tremendous financial costs associated with cancer. The National Institutes of Health estimates that the overall costs of cancer in 2010 will be $263.8 billion: direct
medical costs ($102.8 billion) and lost productivity due to illness ($20.9 billion) and premature death
($140.1 billion).5
Who does it impact most?
A number of factors can increase a person’s chance of developing cancer. However, the relationship between these factors and the disease is not straightforward. Some people with multiple risk factors for
cancer do not develop the disease; others develop cancer despite the absence of any known risk factors. 7
Cancer is a chronic disease that is heavily influenced by age.5,8 More than three-quarters (78%) of all
cancer diagnoses are among people 55 years of age and older.5
In Contra Costa, males are more likely to develop and die from cancer than females and African Americans are most likely to die from cancer.3,6 White females in Contra Costa are more likely to be diagnosed
with cancer than females in the county overall. Black and white males in Contra Costa are more likely
to be diagnosed with cancer than males in the county overall.3 Nationally, black males are more likely
to be diagnosed with cancer than males of other racial/ethnic groups, including whites.6,9
Obesity and several key health behaviors, including smoking, eating an unhealthy diet and being physically inactive, are considered the most significant avoidable causes of cancer.1,5,8,10 Approximately one in
three cancer deaths is caused by tobacco use; another one in three is caused by poor diet, obesity and
physical inactivity.1 Other factors that can increase the chance of developing cancer include: a family
history of cancer; excessive alcohol consumption; some viruses and bacteria; the use of certain hormones including estrogen; exposure to sunlight and other environmental toxins including secondhand
smoke, radiation and certain kinds of chemicals including asbestos and others.8
114
CHRONIC DISEASES
What can we do about it?
The following behaviors may help reduce the risk of developing cancer: refraining from smoking or using any tobacco products; being physically active; eating a healthy diet; maintaining a healthy weight,
avoiding unprotected sun exposure; and limiting alcohol consumption.1
Policies and programs that improve access to affordable healthy foods, increase opportunities for safe,
low- or no-cost physical activity, discourage smoking initiation, support smoking cessation and reduce
exposure to secondhand smoke are important cancer prevention strategies.
Screening can help prevent cancer by identifying precancerous tissue, which can then be removed before it develops into cancer.5 Screening can also help detect cancer early, when treatment options and
the chance of survival are greatest. For some of the most common cancers, including breast, prostate,
colorectal and cervical cancer, the five-year survival rate is at least 90% if the cancer is diagnosed before it spreads.1
Unfortunately, people without health insurance often postpone medical visits and cancer screenings due
to costs. Residents without health insurance are twice as likely to be diagnosed with late-stage cancer
compared to those who are insured.1 In addition, one in four cancer patients postpone or do not seek
treatment due to medical costs, which reduces their chance of survival.1 Access to health insurance
and affordable, culturally competent health care services is important to enable people to pursue appropriate cancer screenings and early treatment.
Data Sources: Cancers – All Types
tables
Tables 1-12: Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans (or blacks) include non-Hispanic residents. Not all races/ethnicities are shown but all
are included in totals for the county, by gender and by city.
Tables 1–5: These tables include total deaths due to all cancers and age-adjusted average annual death rates per 100,000
residents for 2005 through 2007. Mortality data from the California Department of Public Health (CDPH), http://www.
cdph.ca.gov/, Center for Health Statistics’ Death Statistical Master File, 2005–2007. Any analyses or interpretations of the
data were reached by the Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health
Services and not the CDPH.
ICD10 coding for malignant neoplasms (ICD C00–C97) from the Centers for Disease Control and Prevention National
Center for Health Statistics, available online at: http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001–2009,
with 2000 Benchmark.
115
CHRONIC DISEASES
California Population estimate for state level rate from the State of California, Department of Finance, E–4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services’ Office of Disease Prevention
and Health Promotion, available online at http://www.healthypeople.gov/.
Tables 6–12: These tables include five-year case counts and age-adjusted average annual new case rates for 2003 through
2007.New case data from the California Cancer Registry. (2009). Cancer Incidence Rates in California. Based on October
2009 Quarterly Extract (Released October 08, 2009). Retrieved (12/10/09 –12/24/09) from http://cancer-rates.info/ca.
Note: Veterans Health Administration hospitals did not report cancer cases to the California Cancer Registry (CCR) in
2005–2007. Therefore, case counts and rates for adult males for 2005-2007 are underestimates and should be interpreted
with caution. Although there is no way to know how many unreported cancer cases were diagnosed in these facilities,
historically VHA-reported cases have accounted for approximately 4% of all new male cancers reported to the California
Cancer Registry. (See www.ccrcal.org/publications/Vatechnotes).
New case data for this section include in situ bladder cancer and all invasive cancers excluding basal and squamous cell
skin cancers. For more information about the specific International Classification of Diseases for Oncology, Third Edition
(ICD-O-3) coding for new cancer cases, see the National Cancer Institute’s website: http://seer.cancer.gov/siterecode/
icdo3_d01272003. Note: In this report, the term “lung cancer” refers to lung and bronchus cancer and the term “colorectal
cancer” refers to colon and rectum cancer.
text
American Cancer Society, California Department Public Health, California Cancer Registry (2009). California
Cancer Facts and Figures 2010. Oakland, CA: American Cancer Society, California Division, September 2009.
2. National Cancer Institute, U.S. National Institutes of Health (2010). Cancer Topics: What is Cancer? Retrieved
September 27, 2010 from http://www.cancer.gov/cancertopics/what-is-cancer
3. California Cancer Registry, 2009. Incidence data for 2003–07, based on October 2009 Quarterly Extract, released
October 08, 2009.
4. Xu J., Kochanek K.D., Murphy S.L., Tejada-Vera B., Deaths: Final Data for 2007. U.S. Department of Health and
Human Services. National Vital Statistics Reports Volume 58, Number 19. May 2010.
5. American Cancer Society. Cancer Facts & Figures 2010. Atlanta: American Cancer Society; 2010.
6. California Department of Public Health, Center for Health Statistics’ Death Statistical Master File, 2005–2007.
7. Morris CR, Epstein J, Nassere K, Hofer BM, Rico J, Bates JH, Snipes KP. Trends in Cancer Incidence, Mortality,
Risk Factors and Health Behaviors in California. Sacramento, CA: California Department of Public Health, Cancer
Surveillance Section, January 2010.
8. National Cancer Institute, U.S. National Institutes of Health (2006). What You Need to Know AboutTM Cancer—Risk
factors? Retrieved September 27, 2010 from
http://www.cancer.gov/cancertopics/wyntk/cancer
9. U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2006 Incidence and Mortality Web-based
Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and
National Cancer Institute; 2010. Data for 2006 retrieved August 31, 2010 at: www.cdc.gov/uscs.
10. Cancer Trends Progress Report—2009/2010 Update, National Cancer Institute, NIH, DHHS, Bethesda, MD, April
2010, http://progressreport.cancer.gov.
1.
116
CHRONIC DISEASES
Female Breast Cancer
Breast cancer was the most commonly diagnosed cancer among females.
• Females in Contra Costa were more likely to be diagnosed with breast cancer
than females in California.
• White females were most likely to be diagnosed with invasive breast cancer.
• Most invasive breast cancer cases and deaths were among white females.
• African American females were more likely to die from breast cancer
than females in the county overall.
Deaths
Between 2005–2007, invasive breast cancer accounted for 15.8% of all cancer deaths among Contra
Costa females and 3.9% of all female deaths in the county. During this period in Contra Costa, 415
female residents died of breast cancer. This means that on average, 138 female residents died from
breast cancer each year.
The age-adjusted death rate from female breast cancer in Contra Costa (23.0 per 100,000) was similar
to the age-adjusted rate for California (22.8 per 100,000) and was not significantly higher than the
Healthy People 2010 objective (21.3 per 100,000).
Table 1 Female breast cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
303
73.0%
25.3
African American
50
12.0%
35.8*
Asian/Pacific Islander
35
8.4%
16.1
Hispanic
24
5.8%
12.0**
415
100.0%
White
Total
A breast cancer
case is defined
as a primary
malignant tumor
that originated in
the breast rather
than spread from
another location.
23.0
These are age-adjusted rates per 100,000 female residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
The greatest number of deaths from female breast cancer in the county occurred among whites (303),
followed by African Americans (50), Asians/Pacific Islanders (35) and Hispanics (24).
African American females had a significantly higher breast cancer death rate (35.8 per 100,000) than
county females overall (23.0 per 100,000). Hispanic females had a lower breast cancer death rate (12.0
per 100,000) compared to county females overall.
117
CHRONIC DISEASES
Table 2 Female breast cancer deaths by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Concord
49
11.8%
23.9
Walnut Creek
47
11.3%
24.6
Antioch
38
9.2%
29.8
Richmond
33
8.0%
21.4
Pittsburg
20
4.8%
24.8
Brentwood
20
4.8%
31.2
Martinez
17
4.1%
NA
San Pablo
15
3.6%
NA
Oakley
13
3.1%
NA
El Cerrito
13
3.1%
NA
Pleasant Hill
12
2.9%
NA
Hercules
8
1.9%
NA
Pinole
6
1.4%
NA
415
100.0%
Contra Costa
23.0
These are age-adjusted rates per 100,000 female residents.
Contra Costa total includes females in cities not listed above.
The greatest number of deaths from breast cancer occurred among females living in Concord (49),
Walnut Creek (47), Antioch (38) and Richmond (33). The available breast cancer death rates listed
were similar to the rate for county females overall (23.0 per 100,000). Rates were limited at the city
level due to small numbers of deaths.
New Cases
To understand the impact of breast cancer on the community’s health it is important to assess both
breast cancer diagnoses and deaths. Information about breast cancer deaths indicates the ultimate
toll this disease takes on people’s lives, but many more people develop breast cancer than die from
it. Information about new invasive and in situ breast cancer cases provides a sense of how much and
among whom the disease is being diagnosed and can highlight the need for prevention, screening and
treatment programs.
Between 2003–2007, 4,685 new breast cancer cases were diagnosed among Contra Costa females;
81.5% were invasive and 18.5% were in situ cancer. Breast cancer was the most commonly diagnosed
cancer among Contra Costa females, representing more than one-third (36.6%) of all new cancer cases
among females.
118
CHRONIC DISEASES
INVASIVE BREAST CANCER
During this five-year period, 3,820 new cases of invasive breast cancer were diagnosed among females
in Contra Costa—an average of 764 new cases per year. The age-adjusted rate of new female invasive
breast cancer cases for this period was significantly higher in Contra Costa (136.1 per 100,000 females)
than California (121.0 per 100,000 females).
The greatest number of new invasive female breast cancer cases in Contra Costa occurred among white
females (2,766) followed by Asian/Pacific Islander (360), Hispanic (359) and black (303) females. White
females also had the highest rate of new invasive breast cancer cases in the county (149.0 per 100,000);
significantly higher than females in the county overall (136.1 per 100,000) and all other racial/ethnic
groups listed in the table. Asian/Pacific Islander (92.3 per 100,000) and Hispanic females (110.6 per
100,000) experienced significantly lower rates compared to females in the county overall.
Table 3 New invasive female breast cancer cases
by race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
2,766
72.4%
Asian/Pacific Islander
360
9.4%
Hispanic
359
9.4%
110.6*
Black
303
7.9%
124.7
Total
3,820
100.0%
136.1
White
Rate
149.0*
92.3**
Invasive breast
cancer is cancer that
has spread beyond
the breast tissue
where it developed to
surrounding, healthy
tissues.
These rates are age-adjusted per 100,000 female residents.
Total includes females in racial/ethnic groups not listed above.
* Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
IN SITU BREAST CANCER
Between 2003–2007, 865 new cases of in situ breast cancer were diagnosed among females in Contra
Costa; 173 new cases per year. The age-adjusted rate of new in situ cases for this five-year period was
higher in Contra Costa (30.7 per 100,000) than California (27.5 per 100,000).
The greatest number of new in situ female breast cancer cases in Contra Costa occurred among white
females (601) followed by Asian/Pacific Islander (118), black (67) and Hispanic (63) females. Hispanic
females experienced a significantly lower rate (19.5 per 100,000) of new in situ breast cancer cases
compared to Contra Costa females overall (30.7 per 100,000).
119
CHRONIC DISEASES
Table 4 New in situ female breast cancer cases
by race/ethnicity
Contra Costa County, 2003 –2007
Cases
Percent
Rate
White
601
69.5%
32.6
Asian/Pacific Islander
118
13.6%
30.5
Black
67
7.7%
27.6
Hispanic
63
7.3%
19.5**
865
100.0%
Total
In situ breast
cancer is cancer
at its earliest
stage that has
not spread to
neighboring
tissue.
30.7
Total includes females in racial/ethnic groups not listed above.
These rates are age-adjusted per 100,000 female residents.
** Significantly lower rate than county females overall.
What is breast cancer?
The National Cancer Institute defines breast cancer as “cancer that forms in the tissues of the breast,
usually the ducts (tubes that carry milk to the nipple) and lobules (glands that make milk).”1 Although
both males and females develop breast cancer, male breast cancer is rare.1
Why is it important?
Breast cancer is the most commonly diagnosed cancer among females in Contra Costa,2 the greater Bay
Area,3 California2 and the United States.4 Breast cancer is also the second leading cause of cancer death
among females in the county,5 state6 and nation.7
Although the rate of new breast cancer cases declined in the greater Bay Area in the early 2000s, it remained stable in 2003–2007 for most racial/ethnic groups except Asian/Pacific Islander females among
whom the rate increased.3
Who does it impact most?
The exact causes of breast cancer are not known. However, several individual, familial and behavioral
factors have been identified that appear to increase the chances of developing breast cancer.
Females are more likely to develop breast cancer than males.7 The chance of being diagnosed with
breast cancer also increases with age.4,7 Most breast cancer cases develop after menopause and are
diagnosed in females older than 60 years of age.4,8 In Contra Costa, white females are most likely to
be diagnosed with invasive breast cancer, but African American females are more likely to die from the
disease than females in the county overall. Nationally, white females are most likely to be diagnosed
with both invasive and in situ breast cancer.9
Other individual and familial factors related to developing breast cancer include the following: personal or family history of breast cancer (i.e., mother, daughter, sister); abnormal breast cells and ge-
120
CHRONIC DISEASES
netic mutations related to breast cancer genes BRCA1 and BRCA2; long exposure to estrogen, including
menstruation over many years (i.e., starting before age 12 and ending after age 55) and having a first
child after age 30 or never having had a full-term pregnancy; use of hormone replacement therapy;
high doses of radiation to the chest; high breast tissue density;7 and other lifestyle/behavioral factors
including overweight or obesity, lack of exercise and too much alcohol consumption.4,7
What can we do about it?
The five-year survival rate for female breast cancer is high overall but best if diagnosed early: 98% if
the cancer is confined to the breast when diagnosed compared to 21% if it has spread to other parts
of the body.10 On average, mammograms detect 80%–90% of breast cancer cases in females without
symptoms.7 Although mammography rates among women 40 years of age and older declined nationally between 2000 and 2005 from 70.1% to 66.4%, early detection and better treatments have been
identified as an important factor in declining breast cancer mortality among females since 1990.7 More
recent declines are likely related to decreasing use of hormone replacement therapy after menopause.7
Breast cancer screening guidelines differ between various health organizations. In 2009, the U.S. Preventive Services Task Force began recommending that women receive mammograms every two years
between the ages of 50 and 74 years and that they not conduct breast self-exams.11 Some organizations adhere to older recommendations that suggest clinical breast exams every three years starting at
age 20, annual mammograms and clinical breast exams starting at age 40, and that breast self exams
be optional.10,11 Females should discuss screening options with their health care provider to make an
informed decision about when to be screened.
Being physically active, eating a healthy diet and maintaining a healthy weight may also help reduce the
risk of breast cancer.10 Policies and programs that improve access to affordable healthy foods and increase
opportunities for safe, low- or no-cost physical activity can support healthy behaviors to help prevent
breast cancer. Access to health insurance and affordable, culturally competent health care services is
also important to enable people to pursue appropriate screening and early treatment for breast cancer.
Data Sources: Female Breast Cancer
tables
Tables 1–4: The cases and deaths reported in these tables represent instances of female breast cancer. Data presented
for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and African
Americans/blacks include non-Hispanic residents. Not all race/ethnicities are shown but all are included in totals for
the county, by gender and by city. Counts fewer than five are not shown in order to protect anonymity. Rates were not
calculated for any group with fewer than 20 cases due to unstable estimates.
Tables 1–2: These tables include total deaths and age-adjusted average annual death rates per 100,000 female residents for
2005 through 2007. Mortality data from the California Department of Public Health (CDPH), http://www.cdph.ca.gov/,
Center for Health Statistics’ Death Statistical Master File, 2005–2007. Any analyses or interpretations of the data were
reached by the Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services
and not the CDPH. Data was not available for all Contra Costa communities.
121
CHRONIC DISEASES
ICD10 coding for malignant neoplasm of the breast (ICD C50) from the Centers for Disease Control and Prevention
National Center for Health Statistics, available online at: http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark
California Population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services’ Office of Disease Prevention
and Health Promotion, available online at http://www.healthypeople.gov/.
Table 3-4: These tables include five-year case counts and age-adjusted average annual new case rates per 100,000 female
residents for 2003 through 2007. New case data from the California Cancer Registry. (2009). Cancer Incidence/Mortality
Rates in California. Based on October 2009 Quarterly Extract (Released October 08, 2009). Retrieved (12/2/09) from
http://www.cancer-rates.info/ca. International Classification of Diseases for Oncology, Third Edition (ICD-O-3) coding
for new breast cancer cases: C500-509, excluding histology types 9590-9989, and sometimes 9050-9055, 9140+. (For
information on ICD-O-3 codes see: http://seer.cancer.gov/siterecode/icdo3_d01272003/)
text
National Cancer Institute. (n.d.) Cancer Topics: Breast Cancer. Retrieved on June 12, 2010 from: http://www.cancer.
gov/cancertopics/types/breast
2. California Cancer Registry, 2009. Incidence data for 2003–07, based on October 2009 Quarterly Extract released
October 08, 2009.
3. Cancer Prevention Institute of California. (2010) Cancer Incidence and Mortality in the Greater Bay Area, 1988–2007.
www.cpic.org
4. Morris CR, Epstein J, Nassere K, Hofer BM, Rico J, Bates JH, Snipes KP. (2010) Trends in Cancer Incidence, Mortality,
Risk Factors and Health Behaviors in California. Sacramento, CA: California Department of Public Health, Cancer
Surveillance Section, January 2010.
5. California Department of Public Health, Center for Health Statistics’ Death Statistical Master File, 2005–2007.
6. Hofer BM, Kwong SL, Allen M, Bates JH, Snipes KP. (2010) Cancer in California, 1988-2007. Sacramento, CA:
California Department of Public Health, Cancer Surveillance Section, March 2010.
7. American Cancer Society. (2010) Cancer Facts & Figures 2010. Atlanta: American Cancer Society, September 2010.
8. National Cancer Institute. (2009) What You Need To Know About™ Breast Cancer. U.S. National Institutes of Health.
NIH Publication # 09-1556. Retrieved June 25, 2010 from http://www.cancer.gov/cancertopics/wyntk/breast
9. U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2006 Incidence and Mortality Web-based
Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and
National Cancer Institute; 2010. Data for 2006 retrieved August 23, 2010 from www.cdc.gov/uscs.
10. American Cancer Society, California Department Public Health, California Cancer Registry. (2009) California
Cancer Facts and Figures 2010. Oakland, CA: American Cancer Society, California Division.
11. U.S. Preventive Services Task Force (2009). Screening for Breast Cancer: U.S. Preventive Services Task Force
Recommendation Statement. Annals of Internal Medicine. 151 (10); 716-726.
1.
122
CHRONIC DISEASES
Colorectal Cancer
Colorectal cancer was the second leading cause of cancer deaths.
• Colorectal cancer was the fourth most commonly diagnosed cancer in the county.
• Most new colorectal cancer cases in Contra Costa occurred among white residents.
• Black/African American residents were most likely to be diagnosed with
and die of colorectal cancer.
• People living in Antioch were more likely to die from colorectal cancer
than the county overall.
• Contra Costa’s colorectal cancer death rate did not meet the
Healthy People 2010 objective.
Colorectal Cancer Deaths
Between 2005–2007, colorectal cancer was responsible for 10.1% of all cancer deaths and 2.5% of all
deaths among Contra Costa residents. There were 517 Contra Costa residents who died of colorectal
cancer. This means that on average 172 residents died from colorectal cancer each year. Contra Costa’s
age-adjusted death rate (16.5 per 100,000) from colorectal cancer was similar to California’s age-adjusted
rate (16.1 per 100,000) and did not meet the Healthy People 2010 objective (13.7 per 100,000).
Table 1 Colorectal cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
370
71.6%
17.0
African American
65
12.6%
31.1 *
Asian/Pacific Islander
45
8.7%
Hispanic
29
5.6%
517
100.0%
White
Total
13.8
8.5 **
16.5
In this report a
colorectal cancer
case is defined
as a primary
malignant tumor
that orignated
in the colon or
rectum rather
than spread from
another location.
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of deaths from colorectal cancer in the county occurred among whites (370),
followed by African Americans (65), Asians/Pacific Islanders (45) and Hispanics (29).
Even though African Americans died in fewer numbers than whites, African Americans had the highest
colorectal cancer death rate (31.1 per 100,000); significantly higher than the county overall (16.5 per
100,000) and all other racial/ethnic groups listed. Hispanics (8.5 per 100,000) had a significantly lower
colorectal cancer death rate compared to the county overall.
123
CHRONIC DISEASES
Table 2 Colorectal cancer deaths by gender
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Females
276
53.4%
15.1
Males
241
46.6%
18.4
Total
517
100.0%
16.5
These are age-adjusted rates per 100,000 residents.
Females (276) experienced slightly more colorectal cancer deaths than males (241), yet the rates of
colorectal cancer death between females (15.1 per 100,000) and males were similar (18.4 per 100,000).
Table 3 Colorectal cancer deaths in selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Walnut Creek
69
13.3%
15.8
Concord
62
12.0%
18.0
Antioch
53
10.3%
25.5*
Richmond
41
7.9%
15.9
Pittsburg
30
5.8%
21.1
Martinez
27
5.2%
22.6
San Pablo
20
3.9%
28.3
Brentwood
20
3.9%
18.8
El Cerrito
17
3.3%
NA
Pleasant Hill
15
2.9%
NA
Hercules
12
2.3%
NA
Pinole
12
2.3%
NA
Bay Point
11
2.1%
NA
8
1.5%
NA
517
100.0%
Oakley
Contra Costa
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
*Significantly higher rate than the county overall.
124
16.5
CHRONIC DISEASES
The greatest number of deaths from colorectal cancer occurred among residents living in Walnut Creek
(69), Concord (62), Antioch (53) and Richmond (41). Antioch had a significantly higher colorectal
cancer death rate (25.5 per 100,000) than the county overall (16.5 per 100,000).
New Cases
To understand the impact of colorectal cancer on the community’s health it is important to assess both
colorectal cancer diagnoses and deaths. Information about colorectal cancer deaths indicates the ultimate
toll this disease takes on people’s lives. But many more people develop colorectal cancer than die from
it. Information about new colorectal cancer cases provides a sense of how much and among whom the
disease is diagnosed and can highlight the need for prevention, screening and treatment programs.
Between 2003–2007, 2,325 new cases of invasive colorectal cancer were diagnosed in Contra Costa;
an average of 465 new cases per year. Colorectal cancer was the fourth most commonly diagnosed
cancer in the county, representing 10.1% of all new invasive cancer cases. The age-adjusted rate of new
invasive colorectal cancer cases for this period was similar in Contra Costa (46.1 per 100,000) and
California (44.4 per 100,000).
New invasive colorectal cancer cases were evenly distributed between males (1,165) and females (1,160)
in the county, yet males experienced a significantly higher age-adjusted rate of new cases compared to
females (52.9 and 41.0 per 100,000 respectively).
Table 4 New invasive colorectal cancer cases by gender
Contra Costa County, 2003–2007
Cases
Percent
Rate
Males
1,165
50.1%
52.9 *
Females
1,160
49.9%
41.0
Total
2,325
100.0%
46.1
Invasive colorectal
cancer is cancer
that has spread
beyond the tissue
where it developed
to surrounding,
healthy tissue.
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than county females.
The greatest number of new invasive colorectal cancer cases in Contra Costa occurred among whites
(1,655), followed by Asians/Pacific Islanders (222), blacks (216) and Hispanics (182). Although whites
accounted for most new invasive colorectal cancer cases in the county, blacks had the highest rate of
new cases (58.9 per 100,000); significantly higher than the county overall (46.1 per 100,000) and the
other racial/ethnic groups listed in the table. Asians/Pacific Islanders (35.4 per 100,000) and Hispanics
(34.3 per 100,000) had significantly lower rates than the county overall.
125
CHRONIC DISEASES
Table 5 New invasive colorectal cancer cases by
race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
Rate
1,655
71.2%
46.8
Asian/Pacific Islander
222
9.5%
35.4 **
Black
216
9.3%
58.9 *
Hispanic
182
7.8%
34.3 **
2,325
100.0%
White
Total
46.1
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of new invasive male colorectal cancer cases in Contra Costa occurred among
whites (826) followed by Asians/Pacific Islanders (113), Hispanics (98) and blacks (97). Rates of new male
cases for all racial/ethnic groups listed in the table were similar to that of males in the county overall.
Table 6 New invasive male colorectal cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
Rate
White
826
70.9%
53.3
Asian/Pacific Islander
113
9.7%
41.5
Hispanic
98
8.4%
42.3
Black
97
8.3%
64.3
Total
1,165
100.0%
52.9
These are age-adjusted rates per 100,000 male residents.
Total includes males in racial/ethnic groups not listed above.
126
CHRONIC DISEASES
The greatest number of new invasive female colorectal cancer cases in Contra Costa occurred among
whites (829) followed by blacks (119), Asians/Pacific Islanders (109) and Hispanics (84). Although
white females accounted for most new invasive female colorectal cancer cases, rates were highest
among black females (54.8 per 100,000); significantly higher than females in the county overall (41.0
per 100,000) and all racial/ethnic groups listed in the table. Asian/Pacific Islander (30.9 per 100,000)
and Hispanic (28.2 per 100,000) females had significantly lower rates than females in the county overall.
Table 7 New invasive female colorectal cancer cases
By Race/Ethnicity
Contra Costa County, 2003–2007
Cases
Percent
Rate
White
829
71.5%
41.9
Black
119
10.3%
54.8*
Asian/Pacific Islander
109
9.4%
30.9**
84
7.2%
28.2**
1,160
100.0%
Hispanic
Total
41.0
These are age-adjusted rates per 100,000 female residents.
Total includes females in racial/ethnic groups not listed above.
* Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
What is colorectal cancer?
The National Cancer Institute defines colorectal cancer as “cancer that forms in the tissues of the c­olon
(the longest part of the large intestine) or ... the rectum (the last several inches of the large intestine
closest to the anus).”1
Why is it important?
Colorectal cancer is the fourth most commonly diagnosed invasive cancer in Contra Costa and California.2 It was also the second leading cause of cancer death in the county3 and the state.4
Although rates of new colorectal cancer cases have decreased throughout the past 20 years in California,
Korean males and females and Vietnamese and Filipina females in the state are experiencing increasing rates of new colorectal cancer cases.4
Who is most impacted?
In Contra Costa, males are more likely to be diagnosed with colorectal cancer than females. Locally,
blacks/African Americans are most likely to be diagnosed with and die from colorectal cancer.2,3 Black
females are also most likely to be diagnosed among females in the county.2 Although local data did not
detect differences among males, nationally black males are most likely to be diagnosed among males.5
127
CHRONIC DISEASES
Colorectal cancer is more likely to be diagnosed at older ages. More than 90% of people with colorectal cancer are diagnosed after age 50.6,7,8 Other factors that can increase the risk of developing colorectal cancer include: colorectal polyps, if not removed;6,7,8 family6,7,8 or personal history6,8 of colorectal
cancer; conditions that cause inflammation of the colon or bowels;6,7,8 several inhterited conditions;6,7,8
smoking;6,7 heavy alcohol consumption;6 and being physically inactive or obese.6 Diets low in fruits
and vegetables6.8 and those high in animal fat7,8 and red or processed meat6 may also contribute to
risk of developing colorectal cancer.
What can we do about it?
Colorectal cancer is less common than breast and prostate cancer but has a poorer prognosis partly
because it is often diagnosed at a late stage.9 In California in 2007, only 46% of new colorectal cancer
diagnoses were early stage compared to 82% for prostate cancer and 70% for breast cancer.9 Colorectal cancer survival is much better if the cancer is diagnosed early. The five-year survival rate is 64%
for all stages combined; 91% if diagnosed early before it has spread; 10% if diagnosed late after it has
spread to other parts of the body.9
Regular screening is critical to preventing and detecting colorectal cancer early.8 Screening can identify
polyps that can be removed before they develop into cancer.6 It can also detect early stage colorectal
cancer, when the prognosis is best.6 The American Cancer Society recommends that men and women
of average risk begin getting screened for colorectal cancer at age 50.9
Although colorectal screening has increased since the mid-1990s,7 in 2008 only 38% of California adults
50 years of age and older reported being screened for colorectal cancer (i.e., sigmoidoscopy or colonoscopy) within the prior five years.9
Being physically active, eating a healthy diet and maintaining a healthy weight may also help reduce
the risk of colorectal cancer.9 Policies and programs that improve access to affordable healthy foods,
increase opportunities for safe, low or no-cost physical activity and discourage smoking can support
healthy behaviors to help prevent colorectal cancer. Access to health insurance and affordable, culturally competent health care services is also important to enable people to pursue appropriate screening
and early treatment for colorectal cancer.
Data Sources: Colorectal Cancer
tables
Tables 1–7: Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans/blacks include non-Hispanic residents. Not all race/ethnicities are shown but all are
included in totals for the county, by gender and by city. Rates were not calculated for any group with fewer than 20 cases
due to unstable estimates.
Tables 1–3: These tables include total deaths due to colorectal cancer and age-adjusted average annual death rates per
100,000 residents for 2005 through 2007. Mortality data from the California Department of Public Health (CDPH),
http://www.cdph.ca.gov/, Center for Health Statistics’ Death Statistical Master File, 2005-2007. Any analyses or
128
CHRONIC DISEASES
interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation (CHAPE) Unit
of Contra Costa Health Services and not the CDPH.
ICD10 coding for malignant neoplasm of the colon, rectosigmoid junction, rectum and anus (ICD C18-C21) from the
Centers for Disease Control and Prevention National Center for Health Statistics, available online at:
http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001–2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services’ Office of Disease Prevention
and Health Promotion, available online at http://www.healthypeople.gov/.
Table 4–7: These tables include five-year case counts and age-adjusted average annual new case rates per 100,000 residents
for 2003 through 2007. New case data from the California Cancer Registry. (2009). Cancer Incidence Rates in California.
Based on October 2009 Quarterly Extract (Released October 08, 2009). Retrieved December 14, 2009 from http://www.
cancer-rates.info/ca. [Counts for black males and Asian/Pacific Islander females were not publicly available due to small
sample sizes but were provided by Mark Allen at the California Cancer Registry on January 5, 2010.]
Note: Veterans Health Administration hospitals did not report cancer cases to the California Cancer Registry (CCR) in
2005, 2006 and 2007. Therefore, new case counts and rates for adult males for 2005–2007 are underestimates and should
be interpreted with caution. Although there is no way to know how many unreported cancer cases were diagnosed in these
facilities, historically VHA-reported cases have accounted for approximately 4 percent of all new male cancers reported to
the CCR. (For information in the undercount see http://ccrcal.org/publications/Vatechnotes).
International Classification of Diseases for Oncology, Third Edition (ICD–O-3) coding for new colorectal cancer cases:
colon excluding rectum (C180–187, C260) and rectum and rectosigmoid junction (C199 and C209) excluding histology
types 9590–9989, and sometimes 9050-9055, 9140+. (For information on ICD–O-3 codes see:
http://seer.cancer.gov/siterecode/icdo3_d01272003/). This section includes data for invasive cancer only. All but 82
colorectal cancer cases (i.e., 97%) reported to the California Cancer Registry for this period were invasive.
text
1.
2.
3.
4.
5.
6.
National Cancer Institute, U.S. National Institutes of Health. (n.d.) Cancer Topics: Colon and Rectal Cancer.
Retrieved June 12, 2010 from: http://www.cancer.gov/cancertopics/types/colon-and-rectal
California Cancer Registry (2009). Incidence data for 2003–07, based on October 2009 Quarterly Extract, released
October 08, 2009.
California Department of Public Health, Center for Health Statistics’ Death Statistical Master File, 2005–2007.
California Cancer Registry, California Department of Public Health. (n.d.) Colorectal Cancer in California, 1988–
2007: Questions and Answers. Retrieved October 6, 2010 from www.ccrcal.org/Inside_CCR/CRC–FAQ.shtml
U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2006 Incidence and Mortality Webbased Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention
and National Cancer Institute; 2010. Data for 2006 retrieved August 23, 2010 from www.cdc.gov/uscs
American Cancer Society (2010). Cancer Facts & Figures 2010. Atlanta: American Cancer Society.
129
CHRONIC DISEASES
7.
8.
9.
Morris CR, Epstein J, Nassere K, Hofer BM, Rico J, Bates JH, Snipes KP. (2010) Trends in Cancer Incidence,
Mortality, Risk Factors and Health Behaviors in California. Sacramento, CA: California Department of Public Health,
Cancer Surveillance Section, January, 2010.
National Cancer Institute. (2006) What You Need To Know About™ Cancer of the Colon and Rectum. U.S. National
Institutes of Health. Retrieved June 20, 2010 from the NIH website:
http://www.cancer.gov/cancertopics/wyntk/colon-and-rectal/
American Cancer Society, California Department Public Health, California Cancer Registry (2009). California
Cancer Facts and Figures 2010. Oakland, CA: American Cancer Society, California Division, September 2009.
130
CHRONIC DISEASES
Lung Cancer
Lung cancer was the leading cause
of cancer deaths.
• Lung cancer was the third most commonly diagnosed cancer in the county.
• Blacks were most likely to be diagnosed with lung cancer.
• White females were more likely to be diagnosed with lung cancer
than county females overall.
• African Americans and whites were more likely to die of lung cancer
than county residents overall.
• Most new lung cancer cases and deaths were among whites.
Deaths
Between 2005–2007, lung cancer was the most common cause of cancer death in Contra Costa, accounting for 23.7% of all cancer deaths and 5.9% of all deaths in the county. During this time, 1,218
Contra Costa residents died of lung cancer. This means that on average 406 Contra Costa residents
died from lung cancer each year.
The age-adjusted death rate from lung cancer in Contra Costa (38.8 per 100,000) was similar to California’s
age-adjusted rate (41.1 per 100,000) and met the Healthy People 2010 objective (43.3 per 100,000).
Table 1 Lung cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
White
944
77.5%
43.9*
African American
120
9.9%
52.2*
Asian/Pacific Islander
93
7.6%
27.3**
Hispanic
45
3.7%
13.2**
1,218
100.0%
Total
38.8
In this report,
a lung cancer
case is defined
as a primary
malignant tumor
that originated in
the lung rather
than spread to the
lung from another
location.
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of lung cancer deaths in the county occurred among whites (944), followed by
African Americans (120), Asians/Pacific Islanders (93) and Hispanics (45).
African Americans (52.5 per 100,000) and whites (43.9 per 100,000) had significantly higher lung
cancer death rates than the county overall (38.8 per 100,000). Hispanics (13.2 per 100,000) had the
lowest rate of lung cancer death compared to the county overall and all other racial/ethnic groups
131
CHRONIC DISEASES
listed in the table. Asians/Pacific Islanders (27.3 per 100,000) had a significantly lower lung cancer
death rate than the county overall.
Table 2 Male lung cancer deaths
Contra Costa County, 2005–2007
Deaths
White
Percent
Rate
438
74.7%
48.2
African American
63
10.8%
64.3
Asian/Pacific Islander
49
8.4%
32.7
Hispanic
28
4.8%
18.6 **
586
100.0%
Total
43.8
These are age-adjusted rates per 100,000 male residents.
Total includes racial/ethnic groups not listed above.
** Significantly lower rate than county males overall.
Slightly more than half the number of the deaths from lung cancer (51.9%) occurred among females
(632), yet males (43.8 per 100,000) had a higher rate of lung cancer death than females (35.5 per 100,000).
Among males, Hispanics (18.6 per 100,000) had a lower lung cancer death rate than county males
overall (43.8 per 100,000). Among females, Asians/Pacific Islanders (23.3 per 100,000) had a lower
rate of lung cancer death than county females overall (35.5 per 100,000).
Table 3 Female lung cancer deaths
Contra Costa County, 2005–2007
Deaths
Percent
Rate
506
80.1%
41.5
African American
57
9.0%
43.4
Asian/Pacific Islander
44
7.0%
23.3**
Hispanic
17
2.7%
NA
632
100.0%
35.5
White
Total
These are age-adjusted rates per 100,000 female residents.
Total includes racial/ethnic groups not listed above.
** Significantly lower rate than county females overall.
The highest number of deaths from lung cancer occurred among residents of Walnut Creek (175),
Concord (156), Richmond (126)and Antioch (122).
132
CHRONIC DISEASES
Two cities had significantly higher lung cancer death rates than the county overall (38.8 per 100,000):
San Pablo (73.2 per 100,000) and Antioch (57.1 per 100,000). El Cerrito had a significantly lower lung
cancer death rate (25.1 per 100,000) than the county overall.
Table 4 Lung cancer deaths by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Walnut Creek
175
14.4%
42.6
Concord
156
12.8%
44.5
Richmond
126
10.3%
46.2
Antioch
122
10.0%
57.1*
Pittsburg
70
5.7%
49.1
Martinez
50
4.1%
43.7
San Pablo
49
4.0%
73.2*
Pleasant Hill
47
3.9%
40.6
Brentwood
39
3.2%
33.6
Oakley
34
2.8%
60.4
El Cerrito
29
2.4%
25.1**
Hercules
25
2.1%
39.3
Pinole
20
1.6%
28.8
Bay Point
13
1.1%
NA
1,218
100.0%
Contra Costa
38.8
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
New Cases
To understand the impact of lung cancer on the community’s health it is important to assess both lung
cancer diagnoses and deaths. Information about lung cancer deaths indicates the ultimate toll this
disease takes on people’s lives, but more people develop lung cancer than die from it. Information about
new lung cancer cases provides a sense of how much and among whom the disease is being diagnosed
and can highlight the need for prevention, screening and treatment programs.
Between 2003–2007, 2,704 new cases of invasive lung cancer were diagnosed in Contra Costa—an
average of 541 new cases per year. Lung cancer was the third most frequently diagnosed cancer in the
133
CHRONIC DISEASES
county, representing 11.7% of all new invasive cancer cases. The age-adjusted rate of new lung cancer
cases for this period was similar in Contra Costa (55.1 per 100,000) and California (53.7 per 100,000).
Slightly more than half of all new lung cancer cases in the county were among females (53.1%). Males
experienced a significantly higher rate (59.7 per 100,000) of new lung cancer cases compared to females
(52.6 per 100,000).
Table 5 New invasive lung cancer cases by gender
Invasive lung
cancer is cancer
that has spread
beyond the
tissue where it
developed to
surrounding,
healthy tissue.
Contra Costa County, 2003–2007
Cases
Percent
Rate
Females
1,436
53.1%
52.6
Males
1,268
46.9%
59.7*
Total
2,704
100.0%
55.1
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than females.
The greatest number of new invasive lung cancer cases in Contra Costa occurred among whites (2,045)
followed by blacks (269), Asians/Pacific Islanders (215) and Hispanics (152). Although whites accounted
for most new lung cancer cases, blacks had the highest rate of new cases (70.7 per 100,000); significantly
higher than the county overall (55.1 per 100,000) and the other racial/ethnic groups listed in the table.
Asians/Pacific Islanders (36.9 per 100,000) and Hispanics (32.3 per 100,000) had significantly lower
rates than the county overall.
Table 6 New invasive lung cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
White
Black
Asian/Pacific Islander
Hispanic
Total
2,045
269
215
152
2,704
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
134
Percent
75.6%
9.9%
8.0%
5.6%
100.0%
Rate
59.2
70.7*
36.9**
32.3**
55.1
CHRONIC DISEASES
The greatest number of new invasive male lung cancer cases in Contra Costa occurred among white
males (924), followed by black (135), Asian/Pacific Islander (110) and Hispanic (85) males. Although
white males accounted for most new male lung cancer cases, black males had the highest rate of new
male cases (83.9 per 100,000); significantly higher than men in the county overall (59.7 per 100,000) and
all other racial/ethnic groups listed in the table. Asian/Pacific Islander (45.7 per 100,000) and Hispanic
(43.4 per 100,000) males had lower rates of new lung cancer cases than males in the county overall.
Table 7 New invasive male lung cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
Rate
White
924
72.9%
61.0
Black
135
10.6%
83.9*
Asian/Pacific Islander
110
8.7%
45.7**
85
6.7%
43.4**
1,268
100.0%
Hispanic
Total
59.7
These are age-adjusted rates per 100,000 male residents.
Total includes males in racial/ethnic groups not listed above.
* Significantly higher rate than county males overall.
** Significantly lower rate than county males overall.
The greatest number of new invasive female lung cancer cases in Contra Costa occurred among white
females (1,121) followed by black (134), Asian/Pacific Islander (105) and Hispanic (67) females. White
females had a higher rate of new cases (58.9 per 100,000) than females in the county overall (52.6
per 100,000). Asian/Pacific Islander (31.1 per 100,000) and Hispanic (25.0 per 100,000) females had
lower rates of new lung cancer cases than females in the county overall. (Note: Although the rate for
black females appears higher than that for Contra Costa females overall, due to small numbers it was not
statistically significantly higher.)
Table 8 New invasive female lung cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
Rate
White
1,121
78.1%
58.9*
Black
134
9.3%
61.4
Asian/Pacific Islander
105
7.3%
31.1**
67
4.7%
25.0**
1,436
100.0%
Hispanic
Total
These are age-adjusted rates per 100,000 female residents.
Total includes females in racial/ethnic groups not listed above.
*Significantly higher rate than county females overall.
** Significantly lower rate than county females overall.
135
52.6
CHRONIC DISEASES
What is lung cancer?
According to the National Cancer Institute, lung cancer is “cancer that forms in the tissues of the lung,
usually in the cells lining the air passages. The two main types are small cell lung cancer and non-small
cell lung cancer. These types are diagnosed based on how cells look under a microscope.”1 In this report, the term “lung cancer” refers to cancer of the lung and bronchus.
Why is it important?
Lung cancer is the leading cause of cancer death for both males and females in Contra Costa2 and
California.3 It is also the second most commonly diagnosed cancer among males and females in the
county and the state.4
Who is most impacted?
In Contra Costa, males are more likely to be diagnosed with and die from lung cancer than females.2,4
Locally, black males are most likely to be diagnosed with the disease among males and white females
are more likely to be diagnosed than females overall.4 African American and white residents in the
county are more likely to die from lung cancer than county residents overall.2 Nationally black males
are most likely to die from lung cancer among males, and white females are most likely to die from
the disease among females.5
Smoking tobacco is the most important risk factor for lung cancer.6,7 Approximately 85% of lung cancer
deaths are caused by smoking.8 Compared to people who have never smoked, the risk of developing
lung cancer is 23 times higher in males smokers and 13 times higher in female smokers.7 Other factors
that can increase the likelihood of developing lung cancer include a history of tuberculosis and exposure to environmental hazards including secondhand smoke, air pollution, radon, radiation, asbestos
and some metals and organic chemicals.7 Genetics can also play a role in developing lung cancer, particularly among people who are diagnosed with the disease early in life.7
What can we do about it?
Although lung cancer survival has improved during the last 40 years, the five-year survival rate after
being diagnosed with lung cancer, all stages combined, is only 16%.8 Five-year survival increases to
52% if diagnosed early, before the cancer has spread beyond the lungs or bronchus.8 Unfortunately,
there are no generally accepted screening tests for lung cancer, so preventing lung cancer is critical.9
Quitting smoking can reduce the chance of developing lung cancer dramatically. Fifteen years after
quitting, former smokers are only slightly more likely to develop lung cancer compared to people who
have never smoked.8 Encouraging smokers to quit and discouraging others from starting to smoke are
important individual-level prevention strategies and can also reduce the risk of lung cancer for others
in the community by decreasing exposure to secondhand smoke.8
Since the 1988 passage of the California Tobacco Tax, rates of smoking and of new lung cancer cases
have declined in California.8,10 Much of this success is considered to be the result of California’s tobacco
control efforts, which focus on social norm change to create an environment in which tobacco is “less
desirable, less acceptable and less accessible.”8,10 Despite this progress, there were approximately 3.6
136
CHRONIC DISEASES
million adult smokers in California in 2008.11 In California, smoking is most common among African
Americans, men and young adults.11
Providing cessation services and developing and implementing policies and programs that attempt to
counter pro-tobacco influences in the community, limit exposure to secondhand smoke, and reduce
tobacco availability are important strategies to reduce smoking and prevent lung cancer.10 Changes to
the built environment can also limit the community’s exposure to other environmental risk factors for
lung cancer.
Data Sources: Lung Cancer
tables
Tables 1–8: Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans/blacks include non-Hispanic residents. Not all race/ethnicities are shown but all are
included in totals for the county, by gender and by city. Rates were not calculated for any group with fewer than 20 cases
due to unstable estimates.
Tables 1–4: These tables include total deaths and age-adjusted average annual death rates per 100,000 residents for 2005
through 2007. Mortality data from the California Department of Public Health (CDPH), http://www.cdph.ca.gov/, Center
for Health Statistics’ Death Statistical Master File, 2005–2007. Any analyses or interpretations of the data were reached by
the Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the
CDPH.
ICD10 coding for malignant neoplasm of trachea, bronchus and lung (ICD C33-C34) from the Centers for Disease
Control and Prevention National Center for Health Statistics, available online at:
http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California Population estimate for state level rate from the State of California, Department of Finance, E–4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the US Department of Health and Human Services’ Office of Disease Prevention and
Health Promotion, available online at http://www.healthypeople.gov/
Tables 5–8: These tables include five-year case counts and age-adjusted average annual new case rates per 100,000
residents for 2003 through 2007. New case data from the California Cancer Registry. (2009). Cancer Incidence Rates in
California. Based on October 2009 Quarterly Extract (Released October 08, 2009). Retrieved (12/5/09) from
http://www.cancer-rates.info/ca. [Note: The count for Hispanic males not publicly available due to small smple size, but
was obtained via email from Mark Allen at the California Cancer Registry on 1/5/10.] Veterans Health Administration
hospitals did not report cancer cases to the California Cancer Registry (CCR) in 2005, 2006 and 2007. Therefore, new case
counts and rates for adult males for 2005–2007 are underestimates and should be interpreted with caution. Although there
is no way to know how many unreported cancer cases were diagnosed in these facilities, historically VHA-reported cases
137
CHRONIC DISEASES
have accounted for approximately 4% of all new male cancers reported to the California Cancer Registry. (For information
in the undercount see www.ccrcal.org/publications/Vatechnotes). International Classification of Diseases for Oncology,
Third Edition (ICD–O-3) coding for new lung and bronchus cancer cases: C340–C349, excluding histology types 95909989, and sometimes 9050–9055, 9140+. (For information on ICD-O-3 codes see:
http://seer.cancer.gov/siterecode/icdo3_d01272003/). Note: This section includes data for invasive cancer only. All new
lung cancer cases reported by the California Cancer Registry for this period were invasive.
text
National Cancer Institute, U.S. National Institutes of Health. (n.d.) Cancer Topics: Lung Cancer. Retrieved June 12,
2010 from: http://www.cancer.gov/cancertopics/types/lung
2. California Department of Public Health, Center for Health Statistics’ Death Statistical Master File, 2005-2007.
3. Morris CR, Epstein J, Nassere K, Hofer BM, Rico J, Bates JH, Snipes KP. (2010) Trends in Cancer Incidence, Mortality,
Risk Factors and Health Behaviors in California. Sacramento, CA: California Department of Public Health, Cancer
Surveillance Section, January 2010.
4. California Cancer Registry. (2009) Incidence data for 2003-07, based on October 2009 Quarterly Extract, released
October 08, 2009.
5. U.S. Cancer Statistics Working Group.(2010) United States Cancer Statistics: 1999–2006 Incidence and Mortality Webbased Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention
and National Cancer Institute. Data for 2006 retrieved August 23, 2010 from www.cdc.gov/uscs.
6. Stewart, S., Cardinez, C., Richardson, L. (2008) Surveillance for Cancers Associated with Tobacco Use — United States,
1999–2004. MMWR. September 5, 2008 / 57(SS08);1-33. Department of Health and Human Services. Retrieved June
18, 2010 from the CDC website: http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5708a1.htm
7. American Cancer Society. (2010) Cancer Facts & Figures 2010. Atlanta: American Cancer Society.
8. American Cancer Society, California Department Public Health, California Cancer Registry (2009). California
Cancer Facts and Figures 2010. Oakland, CA: American Cancer Society, California Division, September 2009.
9. National Cancer Institute, U.S. National Institutes of Health. (2007) What You Need To Know About Lung Cancer.
Retrieved June 12, 2010 from: http://www.cancer.gov/cancertopics/wyntk/lung
10. California Department of Public Health, California Tobacco Control Program (2009) California Tobacco Control
Update 2009: 20 Years of Tobacco Control in California: Sacramento, CA. Retrieved December 14, 2010 from http://
www.cdph.ca.gov/programs/tobacco/Documents/CTCPUpdate2009.pdf.
11. California Department of Public Health Tobacco Control Program. (2010) Adult Smoking Prevalence Fact Sheet.
http://cdph.ca.gov/programs/Tobacco.
1.
138
CHRONIC DISEASES
Pancreatic Cancer
Pancreatic cancer was the fourth
leading cause of cancer deaths.
• Pancreatic cancer was the 10th most commonly diagnosed invasive cancer in the county.
• White residents accounted for the majority of new pancreatic cancer cases and deaths.
Deaths
Between 2005–2007, pancreatic cancer was the fourth most common cause of cancer death in Contra
Costa, accounting for 6.6% of all cancer deaths and 1.7% of all deaths in the county. During this time,
341 Contra Costa residents died of pancreatic cancer. This means that an average of 114 Contra Costa
residents died from pancreatic cancer each year.
The age-adjusted death rate from pancreatic cancer in Contra Costa (10.5 per 100,000) was similar to
the age-adjusted rate for California (10.7 per 100,000).
Table 1 Pancreatic cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
242
71.0%
11.0
African American
33
9.7%
14.1
Asian/Pacific Islander
33
9.7%
9.3
Hispanic
27
7.9%
7.4
341
100.0%
10.5
White
Total
In this report a
pancreatic cancer
case is defined as a
primary malignant
tumor that
originated in the
pancreas rather than
having spread from
another location.
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
The greatest number of deaths from pancreatic cancer in the county occurred among whites (242)
followed by African Americans (33), Asians/Pacific Islanders (33) and Hispanics (27).
All racial/ethnic groups listed had similar pancreatic cancer death rates to the county (10.5 per 100,000).
Males (11.6 per 100,000) and females (9.6 per 100,000) also had similar pancreatic death rates and
number of deaths (167 vs. 174, respectively). [Note: Although several rates in this section appear different
they are referred to as “similar” because they are not statistically significantly different.]
139
CHRONIC DISEASES
Table 2 Pancreatic cancer deaths by gender
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Females
174
51.0%
9.6
Males
167
49.0%
11.6
Total
341
100.0%
10.5
These are age-adjusted rates per 100,000 residents.
The greatest number of deaths from pancreatic cancer occurred among people living in Walnut Creek
(60), Richmond (39) and Concord (34). These three cities had similar pancreatic cancer death rates
to the county (10.5 per 100,000). Data was limited at the city level due to small numbers of deaths.
Table 3 Pancreatic cancer deaths by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Walnut Creek
60
17.6%
14.3
Richmond
39
11.4%
13.8
Concord
34
10.0%
9.2
Antioch
18
5.3%
NA
Pleasant Hill
18
5.3%
NA
Pittsburg
14
4.1%
NA
San Pablo
14
4.1%
NA
El Cerrito
11
3.2%
NA
Martinez
10
2.9%
NA
Brentwood
10
2.9%
NA
Pinole
9
2.6%
NA
Oakley
7
2.1%
NA
Hercules
6
1.8%
NA
341
100.0%
10.5
Contra Costa
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
140
Invasive pancreatic
cancer is cancer
that has spread
beyond the tissue
where it developed
to surrounding,
healthy tissue.
CHRONIC DISEASES
New Cases
To understand the impact of pancreatic cancer on the community’s health it is important to assess both
pancreatic cancer diagnoses and deaths. Information about new pancreatic cancer cases provides a sense
of how much and among whom the disease is being diagnosed and can highlight the need for prevention and treatment. Unfortunately, most people who develop pancreatic cancer die from the disease.
Between 2003–2007, 575 new cases of invasive pancreatic cancer were diagnosed in Contra Costa—an
average of 115 new cases per year. Pancreatic cancer was the 10th most commonly diagnosed cancer in
the county, representing 2.5% of all new invasive cancer cases. The age-adjusted rate of new pancreatic
cancer cases for this period was similar in Contra Costa (11.5 per 100,000) and California (11.2 per
100,000).
Slightly more than half (53.9%) of all new invasive pancreatic cancer cases in the county were among
females. Males and females experienced similar age-adjusted rates of new cases (11.8 and 11.1 per
100,000 respectively).
Table 4 New invasive pancreatic cancer cases by gender
Contra Costa County, 2003–2007
Cases
Percent
Rate
Females
310
53.9%
11.1
Males
265
46.1%
11.8
Total
575
100.0%
11.5
These are age-adjusted rates per 100,000 residents.
The greatest number of new invasive pancreatic cancer cases in Contra Costa occurred among whites
(428), followed by blacks (52), Hispanics (45) and Asians/Pacific Islanders (45).
Rates among blacks (14.2 per 100,000), whites (12.1 per 100,000), Hispanics (9.0 per 100,000) and
Asians/Pacific Islanders (7.8 per 100,000) were similar to the county overall (11.5 per 100,000).
Table 5 New invasive pancreatic cancer cases by race/ethnicity
Contra Costa County, 2003–2007
Cases
Percent
White
428
74.4%
12.1
Black
52
9.0%
14.2
Hispanic
45
7.8%
9.0
Asian/Pacific Islander
45
7.8%
7.8
575
100.0%
11.5
Total
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
141
Rate
CHRONIC DISEASES
What is pancreatic cancer?
Pancreatic cancer is the uncontrolled growth and spread of malignant cells from the tissues of the pancreas.1 Most pancreatic cancers start in the ducts that carry pancreatic juices but a rare form of the
disease begins in the cells that make insulin or other hormones.1
Why is it important?
Pancreatic cancer is the fourth leading cause of cancer death in Contra Costa2 and the United States.3
Nationally, rates of new pancreatic cancer cases and deaths increased from 2002–2006.3 In the greater
Bay Area, the rate of new pancreatic cancer cases increased among non-Hispanic white males from
2003–2007 and the pancreatic cancer death rate increased among Hispanic females from 1988–2007.4
The pancreatic cancer death rate among Hispanic females in the region was higher than in the rest of
the United States.4
Who does it impact most?
Although Contra Costa data do not detect differences by gender or race/ethnicity, males nationwide are
more likely to develop and die from pancreatic cancer than females.5 Blacks in the United States are
also more likely to be diagnosed with and die from the disease than whites, Hispanics, Asians/Pacific
Islanders and American Indian/Alaska Natives.5
The cause of pancreatic cancer is unknown. However, the following factors can increase a person’s
chances of developing the disease: older age; smoking tobacco;1,6 family history of pancreatic,1,6 colon,6
or ovarian cancer;6 diabetes;1,6 and chronic pancreatitis.1,6 Being overweight or obese may also increase
the likelihood of developing pancreatic cancer.1
What can we do about it?
The chance of surviving five years after a pancreatic cancer diagnosis is 5% for all stages of the cancer
combined.7 If diagnosed early (i.e., still confined to the pancreas) five-year survival increases to 19%.7
However, there are no routine screening tests for pancreatic cancer and people often do not exhibit
symptoms, so detecting it early is difficult.8 Only 7% of cases are detected early.8
To reduce the risk of developing pancreatic cancer the American Cancer Society recommends avoiding
tobacco use.7 Policies and programs that help smokers quit smoking and discourage non-smokers from
smoking are important strategies to support individual efforts to avoid tobacco use.
Maintaining a healthy weight, being physically active and eating a healthy diet may also help reduce
the chance of developing pancreatic cancer. Policies and programs that improve access to affordable
healthy foods and safe opportunities for physical activity can help support these behaviors.
142
CHRONIC DISEASES
Data Sources: Pancreatic Cancer
tables
Tables 1–5: Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/
Pacific Islanders and African Americans/blacks include non-Hispanic residents. Not all race/ethnicities are shown but
all are included in totals for the county, by gender and by city. Counts fewer than five are not shown in order to protect
anonymity. Rates were not calculated for any group with fewer than 20 cases due to unstable estimates.
Tables 1–3: These tables include total deaths and age-adjusted average annual death rates per 100,000 residents for 2005
through 2007. Mortality data from the California Department of Public Health (CDPH), http://www.cdph.ca.gov/, Center
for Health Statistics’ Death Statistical Master File, 2005-2007. Any analyses or interpretations of the data were reached by
the Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the
CDPH.
ICD10 coding for malignant neoplasm of pancreas (ICD C250-C259) from the Centers for Disease Control and
Prevention National Center for Health Statistics, available online at:
http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001–2009,
with 2000 Benchmark.
California Population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Tables 4-5: These tables include five-year case counts and age-adjusted average annual new case rates per 100,000 residents
for 2003 through 2007. New case data from the California Cancer Registry. (2009). Cancer Incidence Rates in California,
based on October 2009 Quarterly Extract (Released October 08, 2009). Retrieved April 1, 2010 from
http://www.cancer-rates.info/ca.
Note: Veterans Health Administration hospitals did not report cancer cases to the California Cancer Registry (CCR) in
2005, 2006 and 2007. Therefore, new case counts and rates for adult males for 2005-2007 are underestimates and should be
interpreted with caution. Although there is no way to know how many unreported cancer cases were diagnosed in these
facilities, historically VHA-reported cases have accounted for approximately 4% of all new male cancers reported to the
CCR. (For information about the undercount see
www.ccrcal.org/publications/Vatechnotes).
International Classification of Diseases for Oncology, Third Edition (ICD-O-3) coding for new pancreatic cancer cases:
C250-C259, excluding histology types 9590-9989, and sometimes 9050-9055, 9140+. (For information on ICD-O-3 codes
see: http://seer.cancer.gov/siterecode/icdo3_d01272003/).This section includes data for invasive cancer only. All but two
new pancreatic cancer cases reported to the California Cancer Registry for this period were invasive.
text
1.
2.
3.
National Cancer Institute. (2010) What You Need To Know About™ Cancer of the Pancreas. U.S. National Institutes of
Health. Retrieved October 6,2010 from: http://www.cancer.gov/cancertopics/wyntk/pancreas
California Department of Public Health, Center for Health Statistics’ Death Statistical Master File, 2005-2007.
Cancer Trends Progress Report—2009/2010 Update. (2010) National Cancer Institute, NIH, DHHS, Bethesda, MD.
Retrieved October 6, 2010 from: http://progressreport.cancer.gov.
143
CHRONIC DISEASES
4.
5.
6.
7.
8.
Cancer Prevention Institute of California (2010). Annual Cancer Incidence and Mortality in the Greater Bay Area,
1988-2007.
U.S. Cancer Statistics Working Group (2010). United States Cancer Statistics: 1999–2006 Incidence and Mortality Webbased Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention
and National Cancer Institute. Data for 2006 retrieved August 23, 2010 from www.cdc.gov/uscs
Morris CR, Epstein J, Nassere K, Hofer BM, Rico J, Bates JH, Snipes KP (2010). Trends in Cancer Incidence,
Mortality, Risk Factors and Health Behaviors in California. Sacramento, CA: California Department of Public Health,
Cancer Surveillance Section, January 2010.
American Cancer Society, California Department Public Health, California Cancer Registry (2009). California
Cancer Facts and Figures 2010. Oakland, CA: American Cancer Society, California Division, September 2009.
American Cancer Society (2010). Cancer Facts & Figures 2010. Atlanta: American Cancer Society.
144
CHRONIC DISEASES
Prostate Cancer
Prostate cancer was the most commonly diagnosed
cancer among males.
• Most new prostate cancer cases and deaths were among white males.
• Black males were most likely to be diagnosed with prostate cancer.
• African American males were more likely to die from prostate cancer than county men
overall.
Prostate Cancer Deaths
Between 2005–2007, prostate cancer was responsible for 2.7% of all deaths and 10.8% of all cancer
deaths among Contra Costa males. In Contra Costa, 270 males died of prostate cancer. This means
that an average of 90 males in the county died from prostate cancer each year.
Contra Costa’s age-adjusted death rate from prostate cancer was lower than California’s age-adjusted
rate (25.3 per 100,000) and met the Healthy People 2010 objective (28.2 per 100,000).
Table 1 Prostate cancer deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
201
74.4%
23.7
African American
38
14.1%
53.1*
Hispanic
18
6.7%
NA
Asian/Pacific Islander
11
4.1%
NA
270
100.0%
White
Total
22.7
In this report a
prostate cancer
case is defined
as a primary
malignant tumor
that originated in
the prostate rather
than having spread
from another
location.
These are age-adjusted rates per 100,000 male residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than county males overall.
The greatest number of deaths from prostate cancer in the county occurred among whites (201), followed by African Americans (38), Hispanics (18) and Asians/Pacific Islanders (11). Although African
American males died from prostate cancer in fewer numbers, they had a higher death rate (53.1 per
100,000) from prostate cancer than county males overall (22.7 per 100,000).
145
CHRONIC DISEASES
Table 2 Prostate cancer deaths by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Walnut Creek
50
18.5%
27.9
Richmond
36
13.3%
35.0
Concord
27
10.0%
23.0
Antioch
17
6.3%
NA
San Pablo
12
4.4%
NA
Pittsburg
12
4.4%
NA
Pleasant Hill
12
4.4%
NA
Martinez
10
3.7%
NA
El Cerrito
10
3.7%
NA
Oakley
9
3.3%
NA
Brentwood
7
2.6%
NA
270
100.0%
Contra Costa
Invasive prostate
cancer is cancer
that has spread
beyond the tissue
where it developed
to surrounding,
healthy tissue.
22.7
These are age-adjusted rates per 100,000 male residents.
Contra Costa total includes males from cities not listed above.
The greatest numbers of deaths from prostate cancer occurred among males living in Walnut Creek
(50), Richmond (36) and Concord (27). The prostate cancer death rates of these three cities were
similar to the county overall rate (22.7 per 100,000). Data at the city level was limited due to small
numbers of deaths.
New Cases
To understand the impact of prostate cancer on the community’s health it is important to assess both
prostate cancer diagnoses and deaths. Information about prostate cancer deaths indicates the ultimate
toll this disease takes on males lives, but many more males develop prostate cancer than die from it.
Information about new prostate cancer cases provides a sense of how much and among whom the
disease is diagnosed and can highlight the need for prevention, screening and treatment programs.
Between 2003–2007, 3,908 new cases of invasive prostate cancer were diagnosed in Contra Costa—an
average of 782 new cases per year. Prostate cancer was the most commonly diagnosed invasive cancer
among males in Contra Costa, accounting for approximately one-third (33.5%) of all new invasive
cancer cases among males. The age-adjusted rate of new invasive prostate cancer cases was higher in
Contra Costa (170.0 per 100,000) than California (146.6 per 100,000).
146
CHRONIC DISEASES
The greatest number of new invasive prostate cancer cases in Contra Costa occurred among white males
(2,727) followed by black (405), Hispanic (311) and Asian/Pacific Islander (253) males. Although white
males accounted for most new invasive prostate cancer cases, black males had the highest rate of new
cases (241.5 per 100,000); higher than males in the county overall (170.0 per 100,000) and the other
racial/ethnic groups listed in the table. Asian/Pacific Islander males (91.0 per 100,000) experienced
the lowest rate of new invasive prostate cancer cases in the county. Hispanic males (143.0 per 100,000)
also had a lower rate than males in the county overall.
Table 3 New invasive prostate cancer cases by race/ethnicity
Contra Costa 2003–2007
White
Cases
2,727
Percent
69.8%
Rate
168.3
Black
405
10.4%
241.5*
Hispanic
311
8.0%
143.0**
Asian/Pacific Islander
253
6.5%
91.0**
3,908
100.0%
Total
170.0
These are age-adjusted rates per 100,000 male residents.
Total includes males in racial/ethnic groups not listed above.
* Significantly higher rate than county males overall.
** Significantly lower rate than county males overall.
What is prostate cancer?
The National Cancer Institute defines prostate cancer as “cancer that forms in the tissues of the prostate (a gland in the male reproductive system found below the bladder and in front of the rectum).”1
Why is it important?
Prostate cancer is the most commonly diagnosed cancer and the second leading cause of cancer death
among males in Contra Costa2,3 and the United States.4
Who is most impacted?
In Contra Costa, black/African American males are most likely to be diagnosed with prostate cancer
and are more likely to die from the disease than males in the county overall.2,3 Similar patterns exist
at the national level.5 Although the exact causes of prostate cancer are not known, several factors can
increase the chance of developing prostate cancer: older age;4,6 family history of prostate cancer (i.e.,
brother or father);4,6 and some genetic factors.4 High levels of testosterone and diets high in fat (especially animal fat) may also increase the risk of prostate cancer.6
What can we do about it?
The survival rate for prostate cancer is quite high. The chance of surviving five years after a prostate
cancer diagnosis is 98% for all stages.7 However, five-year survival is 33% if the cancer has spread to
147
CHRONIC DISEASES
other parts of the body.7 Most prostate cancers are identified early through screening, using the prostate-specific antigen (PSA) test.4
Because many prostate cancers are slow-growing, they may never become life threatening. Screening
and treatment do provide benefits for some males who develop prostate cancer, but there is uncertainty
about the balance of risk and benefits for the population at large, particularly given the potential side
effects of treatment.4 The American Cancer Society suggests that males with at least a 10-year life expectancy who do not have symptoms of prostate cancer work with their health care provider to make
an informed decision about whether to be screened.4 The age at which males should begin receiving
information about screening varies depending on their level of risk for prostate cancer — age 40 for men
at very high risk; age 50 for men of average risk.4
Males living below the poverty level are less likely to get screened for prostate cancer than their wealthier
counterparts.7 Males without insurance or with Medicaid experience later-stage prostate cancer diagnoses compared to patients with private insurance.4 Access to affordable and equitable health insurance and health care services is important for early detection and appropriate treatment of this disease.
Data Sources: Prostate Cancer
tables
Tables 1-3: Data presented for Hispanics include Hispanic residents of any race. Data presented for whites, Asians/
Pacific Islanders and African Americans/blacks include non-Hispanic residents. Not all races/ethnicities are shown but
all are included in totals for the county, by gender and by city. Counts fewer than five are not shown in order to protect
anonymity. Rates were not calculated for any group with fewer than 20 cases due to unstable estimates.
Tables 1-2: These tables include total deaths and age-adjusted average annual death rates per 100,000 residents for 2005
through 2007. Mortality data from the California Department of Public Health (CDPH), www.cdph.ca.gov/, Center for
Health Statistics’ Death Statistical Master File, 2005-2007. Any analyses or interpretations of the data were reached by the
Community Health Assessment, Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the
CDPH.
ICD10 coding for malignant neoplasm of the prostate (ICD C61) from the Centers for Disease Control and Prevention
National Center for Health Statistics, available online at: http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the US Department of Health and Human Services’ Office of Disease Prevention and
Health Promotion, available online at http://www.healthypeople.gov/
148
CHRONIC DISEASES
Table 3: This table includes five-year case counts and age-adjusted average annual new case rates per 100,000 residents
for 2003 through 2007. New case data from the California Cancer Registry. (2009). Cancer Incidence Rates in California.
Based on October 2009 Quarterly Extract (Released October 08, 2009). Retrieved (12/14/09) from
http://www.cancer-rates.info/ca.
Note: Veterans Health Administration (VHA) hospitals did not report cancer cases to the California Cancer Registry
(CCR) in 2005, 2006 and 2007. Therefore, new case counts and rates for adult males for 2005–2007 are underestimates and
should be interpreted with caution. Although there is no way to know how many unreported cancer cases were diagnosed
in these facilities, historically VHA-reported cases have accounted for approximately 4% of all new male cancers reported
to the CCR. (For information in the undercount see www.ccrcal.org/publications/Vatechnotes).
International Classification of Diseases for Oncology, Third Edition (ICD-O-3) coding for new prostate cancer cases:
C619, excluding histology types excluding 9590-9989, and sometimes 9050-9055, 9140+; recode 28010. (For information
on ICD-O-3 codes see: http://seer.cancer.gov/siterecode/icdo3_d01272003/). Note: This section includes data for invasive
cancer only. All but two new prostate cancer cases reported to the California Cancer Registry for this period were invasive
cancer.
Text
1.
2.
3.
4.
5.
6.
7.
National Cancer Institute. (n.d.) Cancer Topics: Prostate Cancer. Retrieved on June 12, 2010 from:
http://www.cancer.gov/cancertopics/types/prostate
California Cancer Registry. (2009) Incidence data for 2003–07, based on October 2009 Quarterly Extract, released
October 08, 2009.
California Department of Public Health, Center for Health Statistics’ Death Statistical Master File, 2005–2007.
American Cancer Society. (2010) Cancer Facts & Figures 2010. Atlanta: American Cancer Society.
U.S. Cancer Statistics Working Group. (2010) United States Cancer Statistics: 1999–2006 Incidence and Mortality
Web-based Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and
Prevention and National Cancer Institute. Data for 2006 retrieved August 31, 2010 at: www.cdc.gov/uscs.
Morris CR, Epstein J, Nassere K, Hofer BM, Rico J, Bates JH, Snipes KP. (2010) Trends in Cancer Incidence,
Mortality, Risk Factors and Health Behaviors in California. Sacramento, CA: California Department of Public Health,
Cancer Surveillance Section, January 2010.
American Cancer Society, California Department Public Health, California Cancer Registry (2009). California
Cancer Facts and Figures 2010. Oakland, CA: American Cancer Society, California Division, September 2009.
149
CHRONIC DISEASES
Diabetes
African Americans were disproportionately impacted by diabetes.
•
•
•
African Americans were most likely to die of diabetes.
People living in San Pablo, Pittsburg, Antioch and Richmond were more likely to die
from diabetes compared to the county overall.
Males were more likely to die from diabetes than females.
Deaths
Between 2005–2007, diabetes was the seventh leading cause of death in Contra Costa, accounting for
2.9% of all deaths in the county (see Leading Causes of Death section). On average, 197 Contra Costa
residents died of diabetes each year. The age-adjusted death rate from diabetes was lower in Contra
Costa (18.9 per 100,000) than California (23.4 per 100,000) and met the Healthy People 2010 objective
(46 per 100,000).
In Contra Costa, the greatest number of diabetes deaths was among whites (350), followed by African
Americans (97), Hispanics (77) and Asians/Pacific Islanders (64).
Even though diabetes killed a greater number of whites, African Americans had the highest diabetes
death rate (46.5 per 100,000); higher than the rates for the county overall (18.9 per 100,000) and all
other racial/ethnic groups listed.
Table 1 Diabetes deaths by race/ethnicity
Contra Costa County, 2005–2007
Deaths
Percent
Rate
350
59.1%
16.0
African American
97
16.4%
46.5*
Hispanic
77
13.0%
24.2
Asian
64
10.8%
20.0
Total
592
100.0%
18.9
White
The statistics presented include
type 1 and 2 diabetes data.
They do not include pregnancyrelated diabetes data.
The number of diabetes deaths
from type 1 and 2 is likely
underestimated. Only 10%–15%
of decedents who had diabetes
have it listed as the underlying
cause of death.1
These are age-adjusted rates per 100,000 residents
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
In Contra Costa, slightly more males (304) died from diabetes than females (288). Males also had a
higher diabetes death rate (22.9 per 100,000) than females (16.0 per 100,000).
150
CHRONIC DISEASES
Table 2 Diabetes deaths by gender
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Males
304
51.4%
22.9*
Females
288
48.6%
16.0
Total
592
100.0%
18.9
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than county females overall.
The greatest number of diabetes deaths occurred among residents of Richmond (86), followed by
Concord (78), Antioch (70) and Pittsburg (53).
Four cities had significantly higher diabetes death rates than the county overall (18.9 per 100,000):
San Pablo (49.3 per 100,000), Pittsburg (37.0 per 100,000), Antioch (35.1 per 100,000) and Richmond
(32.4 per 100,000). Only Walnut Creek had a significantly lower diabetes death rate (10.1 per 100,000)
than the county overall.
Table 3 Diabetes deaths by selected cities
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
Richmond
86
14.5%
32.4*
Concord
78
13.2%
22.2
Antioch
70
11.8%
35.1*
Pittsburg
53
9.0%
37.0*
Walnut Creek
48
8.1%
10.1**
San Pablo
35
5.9%
49.3*
Martinez
27
4.6%
25.5
Pleasant Hill
24
4.1%
20.2
Brentwood
22
3.7%
22.0
El Cerrito
21
3.5%
16.5
Bay Point
14
2.4%
NA
Pinole
13
2.2%
NA
Hercules
9
1.5%
NA
Oakley
7
1.2%
NA
592
100.0%
Contra Costa
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
151
18.9
CHRONIC DISEASES
Estimated Cases
Information about diabetes deaths indicates the ultimate toll this disease takes on people’s lives. But
more people develop diabetes than die from it. To understand the full impact of diabetes on the community’s health it is also important to assess the diabetes burden on those living with the disease. In
this section, diabetes prevalence is defined as the number of people who reported ever being diagnosed
with diabetes. Since some people are never diagnosed, this data does not fully capture the total number
of people living with the disease. However, it provides some idea of how common diabetes is in our
community.
According to the 2007 California Health Interview Survey, approximately 51,000 adults 18 years and
older in Contra Costa had ever been diagnosed with diabetes, resulting in a diabetes prevalence of 6.5%.
Editor’s note: Analyses of diabetes prevalence by gender, race/ethnicity and city
was not possible for Contra Costa due to small sample size, but we can look to
the greater Bay Area to learn more about how diabetes affects our community
disproportionately.
In 2007, the diabetes prevalence among adults 18 years and older was similar for Contra Costa
(6.5%), the greater Bay Area (6.8%) and California (7.8%).
Table 4 Diabetes cases for adults 18 years and older
by gender
2007
Cases
California
Greater Bay Area
Contra Costa
Prevalence
2,099,000
7.8%
367,000
6.8%
51,000
6.5%
Estimates are not age-adjusted.
In the greater Bay Area, more males (190,000) than females (177,000) were diagnosed with diabetes.
The prevalence of diabetes between males (7.1%) and females (6.5%) however, was similar.
Table 5 Diabetes cases for adults 18 years and older by gender
Greater Bay Area, 2007
Cases
Prevalence
Males
190,000
7.1%
Females
177,000
6.5%
Total
367,000
6.8%
Estimates are not age-adjusted.
152
CHRONIC DISEASES
The greatest number of adult diabetes cases in the greater Bay Area was among whites (167,000), followed by Latinos (84,000), Asians/Pacific Islanders (80,000) and African Americans (30,000).
Table 6 Diabetes cases for adults 18 years and older by race/ethnicity
Greater Bay Area, 2007
Cases
White
Latino
Asian/Pacific Islander
African American
Total
167,000
84,000
80,000
30,000
367,000
Prevalence
6.1%
8.2%
6.8%
8.8%
6.8%
Estimates are not age-adjusted.
Total includes racial/ethnic groups not listed above.
Analysis of prevalence data at the California level revealed racial/ethnic disparities in diabetes prevalence. In 2007, American Indian/Alaska Native (14.2%) and African American adults 18 years and
older (11.5%) had higher prevalence of diabetes than California adults overall (7.8%). The prevalence
of diabetes among whites (6.7%) was lower than the state overall.
What is diabetes?
Diabetes is a chronic disease in which the body makes too little insulin or does not use it effectively.
Insulin helps the body absorb excess blood glucose from the bloodstream. Blood glucose levels are
normally kept within a normal range by insulin. People with diabetes have higher than normal blood
glucose levels.2 There are three types of diabetes: Type 1 diabetes, also known as insulin-dependent
diabetes, is an autoimmune disease and most typically occurs in children and young adults. Type 1
diabetes accounts for 5% to 10% of all diagnosed cases of diabetes.2 Type 2 diabetes, formerly known
as “adult onset” diabetes, accounts for 90–95% of diabetes cases. Although it typically occurs after the
age of 40, rates have been increasing among children and youths. Type 2 diabetes is linked to obesity and physical inactivity. Gestational diabetes is a type of diabetes that only pregnant females get. If
not treated, it can cause problems for mothers and babies. Gestational diabetes develops in 2% to 14%
of all pregnancies (depending on the race of the mother) but usually disappears when a pregnancy is
over. About half of women with gestational diabetes will develop type 2 diabetes later.1
Why is it important?
Diabetes is the seventh leading cause of death in Contra Costa overall and a top 10 cause of death for
Asian/Pacific Islander, Hispanic, African American and white residents of the county. It was also the
seventh leading cause of death in the United States in 2006, accounting for 72,507 deaths.2
More people live with diabetes than die from it. From 1980 through 2007, the number of U.S. adults
18–79 years with newly diagnosed diabetes almost tripled to more than 1.5 million in 2007. The number
153
CHRONIC DISEASES
of new cases of diabetes has increased sharply since the early 1990s.3 This is largely attributed to the
rise in type 2 diabetes, which is being increasingly diagnosed at younger ages.4
Diabetes is a major cause of disability. People with diabetes are more likely to experience leg and foot
amputations, heart disease and stroke.3 Diabetes is the leading cause of new cases of blindness in
adults 20-74 years, and kidney failure.2 Treating diabetes complications with medications, hospitalizations and dialysis is physically trying for patients and costly for society. Total health care and related
costs for the treatment of diabetes are roughly $174 billion annually.5
Who does it impact the most?
In Contra Costa, males are more likely to die from diabetes than females and African American residents
have the highest diabetes death rate. Although no differences by race/ethnicity could be detected in
local diabetes prevalence data, nationally African Americans, American Indians, Asian Americans, Pacific Islanders and people of Hispanic American/Latino heritage are at greater risk for being diagnosed
with diabetes than whites.6
Other factors that put people at increased risk for developing type 2 diabetes include: being overweight
or obese, which keeps the body from making and using insulin properly; family history of diabetes;
prior history of gestational diabetes or birth of a child weighing more than nine pounds; high blood
pressure; unhealthy cholesterol (i.e., low HDL or "good” cholesterol or high level of triglycerides); and
physical inactivity (i.e., exercising fewer than three times a week).6
What can we do about it?
There is currently no cure for diabetes, but there are ways to prevent it from occurring.1 The Diabetes
Prevention Program research indicated that people can delay and possibly prevent diabetes by losing
a small amount of weight (5 to 7 percent of total body weight) through 30 minutes of physical activity
five days a week and healthier eating.6 Increased physical activity and healthier diets are more likely
in communities where there are convenient, safe walking paths and accessible sources of fresh fruits
and vegetables.7
Preventing and treating diabetes complications involves routine medical examinations, tests and medications. Blood sugar, blood pressure and kidney functions must be monitored as well as any existing
sores or wounds. Access to quality preventive and outpatient medical care and education regarding
medications, healthy eating and exercise are crucial. To help reduce health disparities and improve
outcomes, efforts should be made to ensure that literacy and language are not barriers to receiving
effective diabetes care.3,8
Data Sources: Diabetes
tables
Tables 1-3: These tables include total deaths due to type 1 and type 2 diabetes and age-adjusted average annual death rates
per 100,000 residents for 2005 through 2007. Mortality data from the California Department of Public Health Services
(CDPH), http://www.cdph.ca.gov/, Center for Health Statistics' Death Statistical Master File, 2005-2007.
154
CHRONIC DISEASES
Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation
(CHAPE) Unit of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include Hispanic
residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic
residents. Not all race/ethnicities are shown but all are included in totals for the county and for each gender and city.
Counts fewer than five are not shown in order to protect anonymity. Rates were not calculated for any group with fewer
than 20 cases due to unstable estimates.
ICD10 coding for diabetes mellitus (ICDE10-E14) from the Centers for Disease Control and Prevention National Center
for Health Statistics, available online at: http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services’ Office of Disease Prevention
and Health Promotion, available online at: http://www.healthypeople.gov/
Tables 4-6: These tables include total estimated cases of diabetes among adults 18 years and older and crude prevalence
percentages for 2007. Local data about asthma from the California Health Interview Survey’s AskCHIS data query system,
copyright© 2007 the Regents of the University of California, all rights reserved, available online at:
http://www.chis.ucla.edu/. Data analysis performed March 17, 2010. Any analyses or interpretations of the data were
reached by the Community Health Assessment, Planning and Evaluation (CHAPE) unit of Contra Costa Health Services.
Data presented for Latinos include Latinos residents of any race. Data presented for whites, Asians/Pacific Islanders and
African Americans include non-Latino residents. Not all race/ethnicities are shown but all are included in totals for the
county, region, state and region by gender and by race/ethnicity. Greater Bay Area data includes the following counties:
Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano and Sonoma. Ask CHIS data are
generated from a telephone survey that asks questions to a randomly selected group of residents in Contra Costa and
other counties in California. Responses are then weighted to represent the county, region, and state as whole. The question
used for this data was "{Other than during pregnancy, has/Has} a doctor ever told you that you have diabetes or sugar
diabetes?" This question was only asked of adults 18 years or older.
text
1.
2.
3.
4.
5.
CDC, National Center for Chronic Disease Prevention and Health Promotion. (n.d.) National diabetes fact sheet:
general information and national estimates on diabetes in the United States, 2007. Atlanta, GA: U.S. Department of
Health and Human Services, Centers for Disease Control and Prevention, 2008.
CDC, National Center for Chronic Disease Prevention and Health Promotion Diabetes. (n.d.) Diabetes Public
Health Resource: Basics About Diabetes. Retrieved May 16, 2010 from the CDC website:http://www.cdc.gov/
diabetes/consumer/learn.htm
CDC, National Center for Chronic Disease Prevention and Health Promotion. (n.d.). Diabetes Data & Trends.
Retrieved May 16, 2010 from the CDC website:
http://www.cdc.gov/diabetes/statistics/incidence/fig1.htm
Gerberding J., CDC. (2005). Diabetes: Disabling, Deadly and On the Rise, 2005. At a Glance Report, May 2005.
Retrieved May 31, 2006 at the CDC website:
www.cdc.gov/nccdphp/ publications/aag/pdf/aag_ddt2005.pdf;
CDC, The Diabetic Epidemic among Older Adults. Adapted from the National Institute of Diabetes and Digestive
and Kidney Diseases. National Diabetes Statistics, 2007. Bethesda, MD: U.S. Department of Health and Human
155
CHRONIC DISEASES
6.
7.
8.
Services, National Institutes of Health, 2008. Updated December 2009. Retrieved August 29, 2010 at http://ndep.nih.
gov//media/FS_OlderAdult.pdf
CDC, National Center for Chronic Disease Prevention and Health Promotion Diabetes. (n.d.) Diabetes Public
Health Resource: Prevention. Retrieved May 16, 2010 from the CDC website:
http://www.cdc.gov/diabetes/consumer/prevent.htm#4
Aboelata MJ, Mikkelsen L, Cohen L, (2004) The Built Environment and Health: 11 Profiles of Neighborhood
Transformation. Prevention Institute, Oakland CA.
U.S. Department of Health & Human Services, Agency for Healthcare Research and Quality. (2001) Diabetes
Disparities Among Racial and Ethnic Minorities. AHRQ Publication No. 02-P007. Retrieved May 16, 2010 from the
AHRQ website: http://www.ahrq.gov/research/diabdisp.htm
156
CHRONIC DISEASES
Heart Disease
Heart disease was the second leading cause of death.
•
•
•
African Americans were most likely to die of heart disease.
People living in San Pablo were most likely to die of heart disease.
Males were more likely to die of heart disease than females.
Between 2005–2007, heart disease accounted for 22.7% of all deaths in Contra Costa, making it the
second leading cause of death in the county. There were 4,664 Contra Costa residents who died of heart
disease. This means that, on average, 1,555 residents of Contra Costa died from heart disease each year.
The age-adjusted death rate for Contra Costa (147.5 per 100,000) was lower than the age-adjusted rate
for California (212.9 per 100,000).
Table 1 Heart disease deaths by race/ethnicity
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
3,465
74.3%
151.9
African American
538
11.5%
258.8*
Hispanic
321
6.9%
107.4**
Asian/Pacific Islander
299
6.4%
99.5**
4,664
100.0%
White
Total
147.5
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of deaths from heart disease occurred among whites (3,465), followed by African
Americans (538), Hispanics (321) and Asians/Pacific Islanders (299).
Even though African Americans died in fewer numbers than whites, African Americans had the
highest death rate from heart disease (258.8 per 100,000); significantly higher than the county rate
overall (147.5 per 100,000) and all other racial/ethnic groups listed. Hispanics (107.4 per 100,000)
and Asians/Pacific Islanders (99.5 per 100,000) had significantly lower death rates from heart disease
compared to the county overall.
157
CHRONIC DISEASES
Table 2 Heart disease deaths by gender
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Females
2,357
50.5%
120.0
Males
2,307
49.5%
185.1*
Total
4,664
100.0%
147.5
These are age-adjusted rates per 100,000 residents.
* Significantly higher rate than county females overall.
The number of heart disease deaths was similar between females (2,357) and males (2,307). However,
males had a significantly higher death rate from heart disease (185.1 per 100,000) than females (120.0
per 100,000).
Table 3 Heart disease deaths by selected cities
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
Walnut Creek
627
13.4%
114.0**
Richmond
567
12.2%
210.2*
Concord
547
11.7%
153.8
Antioch
405
8.7%
211.1*
Pittsburg
254
5.4%
181.5*
San Pablo
249
5.3%
337.6*
Martinez
197
4.2%
188.5*
Pleasant Hill
197
4.2%
156.7*
El Cerrito
188
4.0%
145.9
Brentwood
130
2.8%
132.1
Oakley
100
2.1%
226.5*
Pinole
98
2.1%
142.5
Hercules
67
1.4%
135.7
Bay Point
48
1.0%
121.7
4,664
100.0%
147.5
Contra Costa
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
158
CHRONIC DISEASES
The greatest number of deaths from heart disease occurred among people living in Walnut Creek (627),
followed by Richmond (567), Concord (547) and Antioch (405).
San Pablo had the highest death rate from heart disease (337.6 per 100,000); higher than the county
overall (147.5 per 100,000) and all other selected cities listed. Five other cities had significantly higher
heart disease death rates than the county overall: Oakley (226.5 per 100,000), Antioch (211.1 per 100,000),
Richmond (210.2 per 100,000), Martinez (188.5 per 100,000) and Pittsburg (181.5 per 100,000). Walnut
Creek (114.0 per 100,000) had a significantly lower heart disease death rate than the county overall.
What is heart disease?
Heart disease includes a number of different diseases affecting the heart. The most common type of
heart disease in the United States is coronary artery disease (CAD), which occurs when cholesterol
d­eposits, or plaque, accumulate in the arteries, causing them to narrow.1 The build up of plaque can
cause a heart attack.1 Over time, CAD weakens heart muscle and may lead to heart failure.1
Why is it important?
Heart disease accounts for approximately one in four deaths locally, statewide and nationally.2 It is
the second leading cause of death in Contra Costa overall; first for African Americans, and second for
whites, Asians/Pacific Islanders and Hispanics in the county. It is also the leading cause of death in the
nation2 and state and a primary cause of premature and permanent disability.
The social and financial costs of heart disease are staggering. In 2010, it is estimated that heart disease will cost the United States $316.4 billion in the form of health care services, medications and lost
productivity.3
Who is most impacted?
In Contra Costa, African Americans are most likely to die from heart disease. Men in the county are
also more likely to die from heart disease than women. Nationally, African American adults are more
likely to die from heart disease than non-Hispanic whites.4 Although African American adults are more
likely to have high blood pressure, they are less likely than their white counterparts to have their blood
pressure under control.4
People are at greater risk for developing heart disease as they age. Other factors that can increase
risk for heart disease include: high low-density lipoprotein (LDL) cholesterol, high blood pressure; diabetes; cigarette smoking and exposure to secondhand smoke; and obesity.5,6 Physical inactivity, excessive alcohol use, and diets high in saturated fat, cholesterol and sodium are also linked to conditions related to heart disease (e.g., obesity, high LDL cholesterol, high blood pressure and diabetes).6
What can we do about it?
Many risk factors for heart disease can be modified through lifestyle changes or medication. People
can reduce their risk for heart disease by not smoking, adopting a healthy diet, being physically active,
159
CHRONIC DISEASES
maintaining a healthy weight, not drinking excessively, and managing other chronic conditions such as
diabetes, high blood pressure and high cholesterol.7
Although heart disease often has no symptoms, management and timely treatment for some risk factors, such as high blood pressure and cholesterol, can help reduce the risk of death and disability related to heart disease.2 National guidelines suggest that blood pressure be checked regularly and blood
cholesterol level be checked at least every five years.7
It is also important to recognize the symptoms of a heart attack (e.g., pain or discomfort in the chest,
back or neck; shortness of breath; and light-headedness) and to seek medical attention quickly if you
experience these symptoms.8 Access to health insurance, quality medical care and prescription medication is important in treating chronic illnesses, like heart disease.
Greater access to healthy foods and opportunities for low- or no-cost physical activity is important to
help foster health behaviors that can reduce the risk of heart disease. Policies and programs, including those that support neighborhood-level changes to the built environment, can help increase areas
for more physical activity such as convenient, safe walking paths and accessible sources of fresh fruits
and vegetables.9
Data Sources: Heart Disease
tables
Tables 1-3: These tables include total deaths due to heart disease and age-adjusted average annual death rates per 100,000
residents for 2005 through 2007. Mortality data from the California Department of Public Health (CDPH),
http://www.dph.ca.gov/, Center for Health Statistics' Death Statistical Master File, 2005-2007. Any analyses or
interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation (CHAPE) Unit
of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include Hispanic residents of any race.
Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic residents. Not all race/
ethnicities are shown but all are included in totals for the county and for each gender and city.
ICD10 coding for diseases of the heart (ICD I00-109, I11, I13, I20-I51) from the Centers for Disease Control and
Prevention National Center for Health Statistics, available online at:
http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California Population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
160
CHRONIC DISEASES
text
1.
2.
3.
4.
5.
6.
7.
8.
9.
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2009) About Heart Disease. Retrieved August 21, 2010 from the CDC website from
http://www.cdc.gov/heartdisease/about.htm
Centers for Disease Control and Preventions. Heart Disease Facts webpage. Retrieved August 21, 2010 from
http://www.cdc.gov/heartdisease/facts.htm
Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart Disease and Stroke Statistics—2010 Update. A Report from the
American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2010;121:e1-e170.
U.S. Department of Health & Human Services, Office of Minority Health. (n.d.) Heart Disease and African
Americans. Retrieved May 14, 2010 from the OMH website:
http://minorityhealth.hhs.gov/templates/content.aspx?lvl=3&lvlID=6&ID=3018
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2009) Heart Disease Conditions. Retrieved September 30, 2010 from the CDC website at
http://www.cdc.gov/heartdisease/conditions.htm
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2009) Heart Disease Behavior. Retrieved September 30, 2010 from the CDC website at
http://www.cdc.gov/heartdisease/behavior.htm
National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention
(2009). Prevention: What Can You Do? Retrieved September 30, 2010 from the CDC website:
http://www.cdc.gov/heartdisease/what_can_you_do.htm
National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention
(2009). http://www.cdc.gov/heartdisease/signs_symptoms.htm
Aboelata MJ, Mikkelsen L, Cohen L, (2004) The Built Environment and Health: 11 Profiles of Neighborhood
Transformation. Prevention Institute, Oakland CA.
161
CHRONIC DISEASES
Stroke
Stroke was the third leading cause of death.
• African Americans were most likely to die of stroke.
• People living in San Pablo, Pittsburg and Richmond were
more likely to die from stroke compared to the county overall.
From 2005–2007, 1,462 Contra Costa residents died of stroke, accounting for 7.1% of all deaths in
Contra Costa. This means that on average, 487 residents of Contra Costa died from stroke each year.
The age-adjusted death rate from stroke in Contra Costa (46.7 per 100,000) was lower than California’s
age-adjusted rate (49.5 per 100,000) and met the Healthy People 2010 objective (50 per 100,000).
Table 1 Stroke deaths by race/ethnicity
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
1,043
71.3%
45.6
African American
161
11.0%
80.5*
Asian/Pacific Islander
141
9.6%
47.1
Hispanic
107
7.3%
36.1**
1,462
100.0%
White
Total
46.7
These are age-adjusted rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
Editor’s note: In this report, stroke and heart disease are discussed as separate
topics. Some health reports group stroke and heart disease together under the
heading “cardiovascular disease.”
In Contra Costa, the greatest number of deaths from stroke occurred among whites (1,043), followed
by African Americans (161), Asians/Pacific Islanders (141) and Hispanics (107).
Although African Americans died in fewer numbers than whites, African Americans had the highest
death rate from stroke (80.5 per 100,000); higher than the county overall (46.7 per 100,000) and all
other racial/ethnic groups listed. Hispanics (36.1 per 100,000) had a lower death rate from stroke
than the county overall.
162
CHRONIC DISEASES
Table 2 Stroke deaths by gender
Contra Costa County, 2005 –2007
Deaths
Percent
Rate
Females
910
62.2%
46.5
Males
552
37.8%
46.1
1,462
100.0%
46.7
Total
These are age-adjusted rates per 100,000 residents.
More than half (62.2%) of all deaths from stroke occurred among females (910), yet the death rates
from stroke were similar for females (46.5 per 100,000) and males (46.1 per 100,000).
Table 3 Stroke deaths by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
Rate
Walnut Creek
Concord
Richmond
Antioch
Pittsburg
San Pablo
Pleasant Hill
Martinez
El Cerrito
Brentwood
Pinole
Hercules
238
180
162
109
97
71
51
50
49
44
31
25
16.3%
12.3%
11.1%
7.5%
6.6%
4.9%
3.5%
3.4%
3.4%
3.0%
2.1%
1.7%
43.1
51.9
61.5*
56.1
71.9*
99.9*
40.0
48.6
37.4
44.9
45.1
48.1
Oakley
Bay Point
Contra Costa
23
14
1,462
1.6%
1.0%
100.0%
51.5
NA
46.7
These are age-adjusted rates per 100,000 residents.
Contra Costa total includes cities not listed above.
* Significantly higher rate than the county overall.
The greatest number of deaths from stroke was in Walnut Creek (238), followed by Concord (180),
Richmond (162) and Antioch (109).
Three cities had significantly higher death rates from stroke than the county overall (46.7 per 100,000):
San Pablo (99.9 per 100,000), Pittsburg (71.9 per 100,000) and Richmond (61.5 per 100,000).
163
CHRONIC DISEASES
What is a stroke?
A stroke occurs when a blood vessel that carries oxygen and nutrients to the brain is either blocked by
a clot or bursts. Without oxygen brain cells begin to die, resulting in possible death or permanent disability. Ischemic strokes, which are caused by blood clots and plaque buildup in the arteries, are the
most common type of stroke, accounting for about 85% of all strokes.1
Why is it important?
In Contra Costa, stroke is the third leading cause of death for the county overall, men, women, African
Americans, whites and Asians/Pacific Islanders, and the fourth leading cause of death for Hispanics.
Stroke accounts for 7.1% of all deaths in the county.
Stroke is also a leading cause of serious, long-term disability.1 In the United States every year, about
610,000 people have a stroke for the first time and 185,000 stroke survivors have another stroke.2 Recovery from a stroke can take months or years and many survivors never fully recover.1
The social and financial costs from stroke take a toll on families and communities. In 2009, stroke episodes
cost the United States $68.9 billion in health care services costs, medications and missed days of work.2
Who is most impacted?
In Contra Costa, African Americans are most likely to die from a stroke. National data on the occurrence
of strokes indicate that males are more likely to have a stroke than females. Blacks, Hispanics and
American Indian/Alaska Natives are more likely to experience a stroke than whites or Asians.3 African
Americans are also more likely than whites to become disabled and have difficulty with activities of
daily living after surviving a stroke.4
The likelihood of having a stroke increases with age.3 Other factors that can increase the chance of having a stroke include: high blood pressure, high blood cholesterol, heart disease and diabetes.5 These
conditions are linked to cigarette smoking, exposure to secondhand smoke, a diet high in salt, lack of
exercise, overweight and obesity and consumption of too much alcohol.5,6 Personal and family history
of a stroke also increase the chance of having a stroke.3,5
What can we do about it?
It is important to recognize the symptoms of a stroke and respond quickly with medical attention. Stroke
symptoms include sudden numbness in the face and extremities, trouble seeing in one or both eyes,
trouble speaking and/or walking, severe headache with no known cause, loss of balance and sudden
confusion.7 If given shortly after the start of symptoms, modern medications can reduce the longterm disability for many patients. Educating high-risk families about the symptoms of a stroke and encouraging them, when needed, to seek immediate medical care could save lives and prevent disability.
Strategies to reduce the risk of having a stroke include the following: do not smoke; limit alcohol consumption; be physically active; maintain a healthy weight; and eat a healthy, low-cholesterol, low-
164
CHRONIC DISEASES
sodium, high-fiber diet that includes plenty of fruits and vegetables.8 Managing and treating chronic
conditions related to stroke including high blood pressure, high cholesterol and diabetes are also important stroke-prevention strategies.8
Programs and policies that improve access to healthy foods and opportunities for low- or no-cost physical activity, including those that support neighborhood-level changes to the built environment, can
foster healthy behaviors that reduce the risk of stroke.9
Data Sources: Stroke
tables
Tables 1-3: These tables include total deaths due to cerebrovascular disease and age-adjusted average annual death
rates per 100,000 residents for 2005 through 2007. Mortality data from the California Department of Public Health
(CDPH), http://www.cdph.ca.gov/, Center for Health Statistics' Death Statistical Master File, 2005-2007. Any analyses or
interpretations of the data were reached by the Community Health Assessment, Planning and Evaluation (CHAPE) Unit
of Contra Costa Health Services and not the CDPH. Data presented for Hispanics include Hispanic residents of any race.
Data presented for whites, Asians/Pacific Islanders and African Americans include non-Hispanic residents. Not all race/
ethnicities are shown but all are included in totals for the county and for each gender and city. Rates were not calculated
for any group with fewer than 20 cases due to unstable estimates.
ICD10 coding for cerebrovascular disease (ICD I60-169) from the Centers for Disease Control and Prevention National
Center for Health Statistics, available online at: http://www.cdc.gov/nchs/data/nvsr/nvsr50/nvsr50_16.pdf
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001–2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services’ Office of Disease Prevention
and Health Promotion, available online at: http://www.healthypeople.gov/
text
1.
2.
3.
4.
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2010) Stroke Facts. Retrieved April 15, 2010 from the CDC website at: http://www.cdc.gov/stroke/facts.
htm
Lloyd-Jones D, Adams R, Carnethon M, et al. Heart Disease and Stroke Statistics—2009 Update. A Report From the
American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:e21–e181.
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2010) Stroke Heredity. Retrieved September 30, 2010 from the CDC website at:
http://www.cdc.gov/stroke/heredity.htm
CDC 2005. Differences in Disability Among Black and white Stroke Survivors – United States, 2000-2001. MMWR
54(1): 3-6. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5401a2.htm
165
CHRONIC DISEASES
5.
6.
7.
8.
9.
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2010) Stroke Conditions. Retrieved September 30, 2010 from the CDC website at http://www.cdc.gov/
stroke/conditions
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2010) Stroke Behavior. Retrieved September 30, 2010 from the CDC website at http://www.cdc.gov/
stroke/behavior.htm
American Stroke Association, Division of American Heart Association (n.d.). Learn to Recognize a Stroke. Retrieved
on April 16, 2010 from the American Stroke Association website: http://www.strokeassociation.org/presenter.
jhtml?identifier=1020.
National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke
Prevention (2010) How to Prevent Stroke. Retrieved April 20, 2010 from the CDC website at: http://www.cdc.gov/
stroke/what_you_can_do.htm
Aboelata MJ, Mikkelsen L, Cohen L, (2004) The Built Environment and Health: 11 Profiles of Neighborhood
Transformation. Prevention Institute, Oakland CA.
166
CHRONIC DISEASES
Childhood Asthma
Asthma disproportionately affected African American children.
• African American children were most likely to be hospitalized for asthma.
• Boys were more likely to be hospitalized for asthma than girls.
• African American children in California were more likely to be diagnosed with asthma
than California children overall.
Hospitalizations
Between 2005–2007, there were 1,021 asthma hospitalizations among Contra Costa children 0-14 years
old. This means that, on average, there were 340 hospitalizations in Contra Costa due to childhood
asthma each year. Contra Costa’s age-adjusted asthma hospitalization rate for children (16.1 per 10,000)
was higher than California’s age-adjusted rate (13.2 per 10,000).
Table 1 Childhood asthma hospitalization by race/ethnicity
Contra Costa County Children Age 0–14, 2005–2007
Boys
Girls
Total
African American
170
123
White
193
Hispanic
Asian/Pacific Islander
Total
Percent
Rate
293
28.7%
43.7*
96
289
28.3%
11.1**
167
83
250
24.5%
12.9**
39
28
67
6.6%
9.8**
657
364
1,021
100.0%
16.1
These are age-adjusted rates per 10,000 residents 0-14 years.
Total includes children in racial/ethnic groups not listed above.
* Significantly higher rate than county children overall.
** Significantly lower rate than county children overall.
In Contra Costa, the greatest number of hospitalizations for asthma was among African American
children (293), followed by white (289), Hispanic (250), and Asian/Pacific Islander children (67).
African American children had the highest age-adjusted rate of asthma hospitalizations (43.7 per 10,000);
significantly higher than the rates for county children overall (16.1 per 10,000) and all racial/ethnic
groups listed. White (11.1 per 10,000), Hispanic (12.9 per 10,000), and Asians/Pacific Islander (9.8 per
10,000) children had significantly lower rates of asthma hospitalization than county children overall.
Boys had a higher number (657) and age-adjusted rate (20.2 per 10,000) of asthma hospitalizations
than girls (364 and 11.7 per 10,000). Boys had higher numbers of asthma hospitalizations than girls
in every racial/ethnic group listed.
167
CHRONIC DISEASES
Table 2 Childhood asthma hospitalizations by gender
Contra Costa County Children Age 0–14, 2005–2007
Cases
Percent
Rate
Boys
657
64.3%
20.2*
Girls
364
35.7%
11.7
Total
1,021
100.0%
16.1
These are age-adjusted rates per 10,000 residents 0-14 years.
* Significantly higher rate than county girls age 0-14.
Twelve ZIP codes comprised more than two-thirds (68.3%) of the childhood asthma hospitalizations in
the county: 94565, 94509, 94806, 94804, 94801, 94513, 94531, 94520, 94547, 94572, 94803 and 94583.
Each of these ZIP codes accounted for more than 30 cases. Three ZIP codes had significantly higher
age-adjusted childhood asthma hospitalization rates than the county overall: 94804, 94547 and 94572.
These three ZIP codes were all located in the western part of the county.
Three ZIP code areas had significantly lower age-adjusted rates of childhood asthma hospitalizations
than the county overall: 94513, 94553 and 94521.
Because childhood asthma hospitalization is relatively rare, age-adjusted rates and confidence intervals
could not be calculated for many ZIP codes. In order to get a more complete picture of how asthma
hospitalization varies across the county, age-specific rates for age 0–14 were used for the map of rates
by ZIP code. A stable age-specific rate could not be calculated for ZIP codes with fewer than 20 cases.
If denominator data was available, statistical testing generated a confidence interval for these ZIP codes
to determine whether the age-specific rate range was lower, higher or similar to the county age-specific
rate and the area was shaded accordingly on the map.
168
CHRONIC DISEASES
Table 3 Childhood asthma hospitalizations by ZIP code
Contra Costa County children age 0–14, 2005–2007
Cases
Percent
94506
6
0.6%
94507
94509
94513
94514
94517
94518
94519
94520
94521
94523
94526
94530
94531
94547
94549
94553
94556
94561
94563
94564
94565
94572
94582
94583
94596
94597
94598
94801
94803
94804
94805
94806
Total
7
97
48
10
8
17
5
40
25
20
21
25
46
36
12
27
5
28
10
21
104
32
14
31
11
8
11
53
31
86
20
93
1,021
0.7%
9.5%
4.7%
1.0%
0.8%
1.7%
0.5%
3.9%
2.4%
2.0%
2.1%
2.4%
4.5%
3.5%
1.2%
2.6%
0.5%
2.7%
1.0%
2.1%
10.2%
3.1%
1.4%
3.0%
1.1%
0.8%
1.1%
5.2%
3.0%
8.4%
2.0%
9.1%
100.0%
These are age-adjusted rates per 10,000 children 0-14 years.
Total includes children in ZIP codes not listed above.
* Significantly higher rate than county children overall.
** Significantly lower rate than county children overall.
169
Rate
NA
NA
20.0
11.4**
NA
NA
NA
NA
13.9
10.0**
11.2
12.0
25.2
12.6
30.8*
NA
10.7**
NA
10.9
NA
21.2
15.7
56.1*
NA
14.1
NA
NA
NA
19.1
21.7
29.9*
23.7
21.5
16.1
CHRONIC DISEASES
170
CHRONIC DISEASES
Estimated Childhood Asthma Cases
To understand the impact of asthma on children’s health, it is important to assess both hospitalizations
and prevalence (estimated cases). Hospitalizations represent the most severe asthma cases. However,
for every child hospitalized, many others are treated at emergency rooms and outpatient clinics and
some children are not treated at all. Asthma diagnosis provides a more complete picture but it, too,
underestimates the number of children currently living with asthma since some people with asthma
are never diagnosed.
According to the 2007 California Health Interview Survey, approximately 39,000 children 1–14 years
in Contra Costa County had ever been diagnosed with asthma. The percentage of all children who
have been diagnosed with asthma in Contra Costa (19.0%) was similar to California (13.8%). (Note:
Although the percentage for Contra Costa appears higher than that for California, it was not statistically
significantly higher.)
Table 4 Asthma ever diagnosed
Children Ages 1–14, 2007
Children
California
Prevalence
1,051,000
13.8%
39,000
19.0%
Contra Costa
Estimates are not age-adjusted.
Editor’s note: Analyses of Contra Costa asthma cases for children 1–14 years by
gender and race/ethnicity were not possible due to small sample size, but we
can look to California data for an indication of how asthma affects our community
disproportionately.
Table 5 Asthma ever diagnosed by race/ethnicity
California Children Ages 1 –14, 2007
Children
Prevalence
Latino
479,000
12.8%
White
313,000
13.2%
Asian/Pacific Islander
109,000
14.5%
87,000
20.8%*
African American
Total
1,051,000
Estimates are not age-adjusted.
Total includes children in racial/ethnic groups not listed above.
* Significantly higher rate than state children overall.
171
13.8%
CHRONIC DISEASES
At the state level, the greatest number of children who had ever been diagnosed with asthma were
Latino (479,000), followed by white (313,000), Asian/Pacific Islander (109,000), African American
(87,000) and two or more races (56,000). Even though African American children had fewer diagnosed
cases of asthma, a significantly higher percentage were diagnosed with asthma (20.8%) than the state
overall (13.8%).
Table 6 Asthma ever diagnosed in children by gender
California Children Ages 1 –14, 2007
Children
Prevalence
Male
644,000
16.6%*
Female
407,000
10.9%
1,051,000
13.8%
Total
Estimates are not age-adjusted.
* Significantly higher rate than state females age 1-14.
Boys (644,000) accounted for more than half the number of asthma cases diagnosed in California
(1,051,000) and had a significantly higher percentage with diagnosed asthma (16.6%) than girls (10.9%).
What is asthma?
Asthma is a chronic respiratory disease caused by the inflammation and narrowing of small airways in
the lungs. A person diagnosed with asthma has it all the time, but an “episode” or “attack” comes on
when something bothers the lungs, and the airways become so swollen and clogged that the person
has trouble breathing.1 An asthma attack can range in severity from inconvenient to life-threatening,
and may include any of the following signs and symptoms: shortness of breath, wheezing, breathlessness, chest pain or tightness, and nighttime or early morning coughing.2,3
Why is it important?
Asthma is one of the leading chronic childhood diseases in the United States and a major cause of
childhood disability. The prevalence of childhood asthma more than doubled between 1980 to the mid1990s and remains at historically high levels.4 In 2008, 7 million U.S. children had asthma. 5 In 2005,
asthma was the third leading cause of hospitalizations in children younger than 15 years, accounting
for 200,000 hospital visits, and was responsible for 7 million doctors visits.6
Asthma limits a child’s ability to play, learn and develop to their full potential.7 Asthma is the leading cause
of school absenteeism, impairing the child’s education and, for some schools, attendance-based funding.8 Asthma places a burden on the affected child’s family because managing asthma requires potentially
complex treatments, constant monitoring and changes to the home environment.9
Who does it impact the most?
Asthma prevalence increases with age, but healthcare use is highest among the youngest children.
172
CHRONIC DISEASES
Boys have a higher prevalence of asthma and more asthma deaths throughout childhood than girls.9
Asthma disproportionately impacts some racial/ethnic groups more than others. African American children are more likely to ever have been diagnosed with asthma than Hispanic, white and Asian children.5
African American children are five times more likely to die from asthma and have three times higher
asthma-related hospitalization and emergency room visit rates than white children.3 Latino children
have higher rates of asthma-related emergency room visits and hospitalizations than whites.3
These differences may be explained by genetics, but other social inequities contribute to the disparity
as well. Factors such as exposure to traffic pollution, tobacco smoke, pollutants and environmental allergens (for example, house dust mites, cockroach particles, cat and dog dander, and possibly mold);
a lack of access to quality medical care; and a lack of financial resources to manage asthma effectively
on a long-term basis may contribute to the differences seen among racial/ethnic groups.10,11
What can we do about it?
While we still don’t know why some children acquire asthma and others do not, we do know what factors may “trigger” an asthma attack: allergens and irritants like “secondhand” tobacco smoke, dust
mites, outdoor air pollution, cockroaches and pets; exercise; changes in weather; and infections.12 Direct patient care and community strategies can help reduce triggers, prevent attacks or lessen their
severity and frequency.
Patient Care Children with asthma require regular doctor visits. Access to quality medical care and prescription medication is important in treating chronic illnesses, like asthma. Health insurance coverage
is crucial.13 An individual’s asthma-management plan should be developed with a physician, parents
and other caregivers. The plan should be guided by the severity of the child’s asthma, the benefits and
drawbacks of each treatment, and opportunities to reduce asthma triggers.2 Families also need to know
what actions to take if faced with an asthma emergency.
Community Prevention To improve outcomes for children with asthma and to help reduce health disparities, efforts should be made to ensure that literacy and language are not barriers to receiving effective
asthma care.14 Schools should be active partners in a family’s asthma-management plan. This includes
emergency plans in case of asthma attacks at school and efforts to improve classroom air quality.8
Asthma sufferers would also benefit from communitywide efforts to improve housing conditions and
lessen air pollution such as diesel exhaust emitted by trucks, buses and trains.10
Data Sources: Childhood Asthma
tables
Tables 1–3: These tables include total hospitalizations for asthma among children 0–14 years and age-adjusted average
annual hospitalization rates per 10,000 residents 0-14 years for 2005–2007. Childhood asthma hospitalization data from
the California Office of Statewide Health Planning and Development (OSHPD) Patient Discharge Data files 2005–2007,
http://www.oshpd.ca.gov/, Healthcare Quality and Analysis Division, Health Care Information Resource Center.
173
CHRONIC DISEASES
OSHPD data includes only those hospitalizations for which asthma was listed as the primary diagnoses (ICD-9 code 493).
They do not include treatment that takes place in a doctor’s office, health clinic or emergency room. A single child can be
counted multiple times for multiple asthma hospitalizations.
Tables 1, 2: Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning and
Evaluation (CHAPE) Unit of Contra Costa Health Services and not the California Department of Public Health (CDPH)
or California Office of Statewide Health Planning and Development (OSHPD). Data presented for Hispanics include
Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include nonHispanic residents. Not all race/ethnicities are shown but all are included in totals for the county and for each gender.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity) for 2005–2007 were
provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create these estimates
included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009 Projections,
and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009, with 2000
Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Table 3: Age-adjusted rates for asthma hospitalizations by Contra Costa ZIP codes were provided by the California
Environmental Health Investigations Branch (EHIB) using OSHPD data and the Environmental Systems Research
Institute (ESRI) Community Sourcebook of ZIP Code Demographics. Data was not available for all ZIP codes. ZIP codes
with fewer than five hospitalizations are not shown in order to protect anonymity. Rates were not calculated for any group
with fewer than 20 cases due to unstable estimates and are marked “NA” in the table.
Map: Age-specific rates for asthma hospitalization were calculated using OSHPD data and the Environmental Systems
Research Institute (ESRI) Community Sourcebook of ZIP Code Demographics. Although stable rates could not be
calculated for ZIP codes with fewer than 20 hospitalizations, statistical testing generated confidence intervals for these
ZIP codes to determine whether the rate range was lower, higher or similar to the county age-specific rate and the ZIP
codes were shaded accordingly. Neither rates nor shading were determined for ZIP codes that extended to areas outside of
Contra Costa (94551, 94707 and 94708) or for ZIP codes for which no denominator was available (94505). ZIP codes that
are assigned to P.O. boxes only, while included in the Table 3, could not be mapped. For several ZIP codes (94513, 94561
and 94806) the conclusions for the age-specific rates, represented by the shading in the map, are different from those for
the age-adjusted rates included in Table 3.
Tables 4-6: These tables include total estimated cases of asthma among children 1-14 years and crude prevalence
percentages for 2007. Local data about asthma from the California Health Interview Survey’s AskCHIS data query system,
copyright© 2007 the Regents of the University of California, all rights reserved, available online at:
http://www.chis.ucla.edu/. Data analysis performed March 17, 2010. Any analyses or interpretations of the data were
reached by the Community Health Assessment, Planning and Evaluation (CHAPE) unit of Contra Costa Health Services.
Data presented for Latinos include Latino residents of any race. Data presented for whites, Asians/Pacific Islanders and
African Americans include non-Latino residents. Not all race/ethnicities are shown but all are included in the gender, city,
county and state total. Ask CHIS data are generated from a telephone survey that asks questions to a randomly selected
group of residents in Contra Costa and other counties in California. Responses are then weighted to represent the county,
region and state as whole. The question used for analysis was “Has a doctor ever told you that you have asthma?” This
question was asked about all respondents 1 year of age and older.
text
1.
Center for Disease Control (2006) You Can Control Your Asthma: A guide to understanding asthma and its triggers.
Retrieved May 12, 2010 from the CDC website: http://www.cdc.gov/asthma/pdfs/asthma_brochure.pdf
174
CHRONIC DISEASES
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
California Breathing Asthma Media Center. “What is Asthma?” Asthma Education for Childcare and Preschool staff
companion guidebook. Retrieved August 25, 2010 at: http://www.californiabreathing.org/childcare_staff.php
Regional Asthma Management & Prevention. “Eliminating Inequities” Retrieved August 25, 2010 at http://www.
rampasthma.org/about-ramp/programs/inequities
Akinbami L.J. (2006). The State of Childhood Asthma, United States, 1980-2005. Advance Data from Vital and Health
Statistics (381), Hyattsville, MD: National Center for Health
Bloom B, Cohen RA, Freeman G. (2009) Summary health statistics for U.S. children: National Health Interview Survey,
2008. National Center for Health Statistics.
U.S. Environmental Protection Agency (EPA), Indoor Division, Office of Air and Radiation. (Feb 2010). Asthma
Facts. EPA 402-F-04-019 ). Retrieved May 12, 2010 from the EPA website: http://www.epa.gov/asthma/pdfs/
asthma_fact_sheet_en.pdf
Adams P.F., Herndershot G.E. (1996). Current estimates from the National Health Interview Survey. Vital Health Stat
10 (200) In Akinbami L.J. (2006). The State of Childhood Asthma, United States, 1980-2005. Advance Data from Vital
and Health Statistics (381), Hyattsville, MD: National Center for Health Statistics.
Regional Asthma Management & Prevention. Healthy Schools. Retrieved May 12, 2010 from the RAMP website:
http://www.rampasthma.org/about-ramp/programs/schools
Akinbami L. Asthma Prevelance, Health Care Use and Mortality: United States 2003-2005. Hyattsville, MD: National
Center for Health Statistics. Retrieved May 12, 2010 from the CDC website: http://www.cdc.gov/nchs/data/hestat/
asthma03-05/asthma03-05.htm
Regional Asthma Management & Prevention. Clean Environments. Retrieved May 14, 2010 from the RAMP website:
http://www.rampasthma.org/?page_id=614
Wade, S.; Weil, C.; Holden, G.; et al. Psycho social characteristics of inner-city children with asthma: A description of
the NCICAS psychosocial protocol. National Cooperative Inner-City Asthma Study. Pediatric Pulmonology 24:263276, 1997. PubMed; PMID 9368260; Retrieved August 25, 2010 from http://www.healthypeople.gov/Document/
HTML/Volume2/24Respiratory.htm#_Toc489704825
Newacheck P.W., Halfton N. (2006). Prevalence, impact, and trends in childhood disability due to asthma. Arch
Pediatr Adolesc Med 154 (3): 287-93 In Akinbami L.J. (2006). The State of Childhood Asthma, United States, 19802005. Advance Data from Vital and Health Statistics (381), Hyattsville, MD: National Center for Health Statistics.
Meng YY, Babey SH, Hastert TA, Lombardi C and Brown ER. (2008) Uncontrolled Asthma Means Missed Work and
School and Emergency Department Visits for Many Californians. Los Angeles, CA: UCLA Center for Health Policy
Research.
Babey SH, Meng YY, and Jones M. (2009) Many Californians with Asthma Have Problems Understanding Their
Doctor. Los Angeles, CA: UCLA Center for Health Policy Research.
175
CHRONIC DISEASES
Adult Overweight & Obesity
More than half of all adults in Contra Costa
were overweight or obese.
•
•
In Contra Costa, men were more likely to be overweight than women.
In the greater Bay Area, American Indian/Alaska Native, African American and Latino adults
were more likely to be overweight or obese than greater Bay Area adults overall.
According to estimates from the California Health Interview Survey, 407,000 Contra Costa adults 20
years and older were overweight or obese in 2007: overweight (253,000); obese (154,000).
In 2007, more than half (56.2%) of Contra Costa adults were either overweight or obese. This was similar
to the percent of overweight and obese adults in the greater Bay Area (53.3%) and California (58.4%).
Table 1 Prevalence of overweight & obese adults
Adults Ages 20 Years & Older, 2007
Overweight or Obese
(BMI 25+)
Overweight
(BMI 25-29.99)
Obese
(BMI 30+)
Contra Costa
56.2%
34.9%
21.3%
Greater Bay Area
53.3%
34.2%
19.1%
California
58.4%
35.2%
23.2%
Estimates are not age-adjusted.
The percentages of overweight (34.9%) and obese adults (21.3%) in the county were similar to those
in the greater Bay Area (34.2% and 19.1%, respectively) and the state (35.2% and 23.2%, respectively).
More men in the county were overweight or obese than women (239,000 and 168,000 respectively).
Men were also more likely to be overweight or obese than women. Approximately two-thirds (66.4%)
of men in the county were overweight or obese compared to less than half (46.2%) of women. The
percents of obese men and women were similar, but there was a greater percentage of overweight men
(44.3%) compared to women (25.8%).
Table 2 Prevalence of overweight & obese adults by gender
Contra Costa adults Ages 20 Years & Older, 2007
Overweight or Obese
(BMI 25+)
Overweight
(BMI 25-29.99)
Obese
(BMI 30+)
Men
66.4%*
44.3%*
22.1%
Women
46.2%
25.8%
20.4%
Total
56.2%
34.9%
21.3%
Estimates are not age-adjusted.
*Significantly higher than women.
176
CHRONIC DISEASES
At the county level, the percent of overweight and obese adults did not differ significantly by race/
ethnicity, based at least in part on small sample sizes. However, data for the greater Bay Area revealed
that some racial/ethnic groups were more likely to be overweight or obese than others. The percent of
overweight or obese American Indian/Alaska Native (77.2%), African American (69.0%) and Latino
(68.2%) adults in the greater Bay Area was significantly higher than the percent of overweight or
obese adults in the greater Bay Area overall (53.3%). A significantly lower percentage of Asian/Pacific
Islander adults were overweight or obese (35.6%) compared to adults in the greater Bay Area overall
and all other racial/ethnic groups listed.
These differences were due to obesity specifically. The percent of obese American Indian/Alaska Native
(46.4%), African American (32.7%) and Latino (30.7%) adults was higher than adults in the greater
Bay Area overall (19.1%). Asians/Pacific Islanders (6.2%) had the lowest percent of obese adults in
the Greater Bay Area; lower than adults in the region overall and all other racial/ethnic groups listed.
Table 3 Prevalence of overweight & obese adults
Greater Bay Area adults Ages 20 Years & Older, 2007
Overweight or
Overweight
Obese (BMI 25+) (BMI 25-29.99)
Obese
(BMI 30+)
American Indian/Alaska Native
77.2%*
30.8%
46.4%*
African American
69.0%*
36.3%
32.7%*
Latino
68.2%*
37.5%
30.7%*
White
52.7%
34.5%
18.2%
Asian/Pacific Islander
35.6%**
29.5%
Total
53.3%
34.2%
6.2%**
19.1%
Estimates are not age-adjusted.
Total includes racial/ethnic groups not listed above.
*Significantly higher than the greater Bay Area overall.
**Significantly lower than the greater Bay Area overall.
The greatest numbers of overweight and obese adults in the greater Bay Area were white residents
(1,395,000) followed by Latinos (677,000), Asians/Pacific Islanders (398,000), African Americans
(221,000) and American Indians/Alaska Natives (21,000).
Differences in obesity also existed based on income status. Lower-income adults in the greater Bay Area
were more likely to be obese than higher-income residents. In 2007, the percentage of obese adults
with household incomes less than 300% of the federal poverty level (26.0%) was higher than adults
with household incomes of 300% FPL and above (15.6%).
177
CHRONIC DISEASES
What is obesity?
Obesity is defined as excess body fat.1 Since body fat is difficult to measure, obesity is often identified
using body mass index (BMI), a number calculated from a person’s height and weight.1 Although it is
not a direct measure of fatness, BMI is a fairly good indicator of body fatness for most people and is
used to screen for weight categories that may lead to health problems.2 An adult is considered overweight but not obese with a BMI between 25.0 and 29.9 and obese with a BMI of 30.0 or higher.2 For
more information about BMI, see the Centers For Disease Control and Prevention’s website:
http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html
Why is it important?
In 2007, more than half of the adults ages 20 and older in Contra Costa were overweight or obese.
Nationally, more than two-thirds (68%) of adults were either overweight or obese in 2007–2008; 34.2%
were overweight and 33.8% were obese.3,4 The percent of obese adults in the United States has more
than doubled in the last 30 years.3
Being obese has serious health implications. Overweight and obese people are more likely than others
to develop a number of health issues, including high blood pressure, cholesterol problems (i.e., high
low-density lipoprotein (LDL) cholesterol, low high-density lipoprotein (HDL), high triglycerides), type
2 diabetes, coronary heart disease, stroke, gallbladder disease, joint problems, sleep apnea and other
respiratory problems and some cancers.2 People who are overweight or obese are also more likely to
die prematurely.5
Medical costs associated with obesity were estimated at $147 billion nationwide in 2006.5
Who does it impact most?
In the greater Bay Area in 2007, low-income adults and American Indian/Alaska Native, African American
and Latino adults were more likely to be obese than adults in the region overall. National data indicate
that racial/ethnic differences in adult obesity exist among women but not men. In 2007–2008 a greater
percentage of black women (49.6%) and Mexican-American women (45.1%) were obese compared to
white women (33.0%) in the United States.3
Typically, people gain weight if they consume more calories than they burn through physical activity
and other activities of daily living.6 Although genetic factors can make certain people more likely to
become overweight, individual eating and physical activity behaviors as well as the social and physical
environments that influence these behaviors play significant roles in the development of overweight
and obesity.6
What can we do about it?
Eating a healthy diet and getting adequate physical activity are important for maintaining a healthy
weight. Public health recommendations suggest that any amount of activity is better than being inactive.7 Ideally, adults should get at least 2.5 hours a week of moderate-intensity physical activity.7 Eating
a balanced diet that includes a variety of fruits and vegetables, whole grains, lean meats, low-fat dairy,
and limited sugar, salt and fat is also recommended for optimal health.8
178
CHRONIC DISEASES
Unfortunately, most Contra Costa adults do not get the physical activity they need. In 2008, almost
one-fifth (18.6%) of Contra Costa adults reported that they did not participate in any physical activity in the past month.9 Only 36.0% of Contra Costa adults engaged in a minimum amount of physical activity in 2007 (i.e., 30 minutes of moderate physical activity at least five days per week or 20
minutes of vigorous activity at least three days per week).10
Adults in the region also eat fast food often and do not get enough fruits and vegetables in their
diets. In 2007, more than half of Contra Costa adults (53.8%) ate fast food at least once in the past
week10 and approximately two-thirds (69.9%) of adults in the Bay Area (including the counties of
Alameda, Contra Costa, Marin, San Francisco and San Mateo) did not eat fruits and vegetables five
or more times per day.11
Environmental factors, including lack of access to affordable, healthy foods and safe places to be
active can make it difficult for people to eat healthy and be active.12 The Centers for Disease Control
and Prevention (CDC) suggests that communities create environments that foster healthy lifestyle
choices by implementing the following recommended strategies to increase healthy eating and physical activity:5,12,13
• Promote the availability of affordable healthy food and beverages: Make affordable, healthier
foods and beverages more available in public service venues (e.g., schools, after-school programs, child
care centers, community recreational facilities and government buildings); make supermarkets more
available and encourage food retailers to offer healthier food and beverages in underserved areas; and
make it easier for communities to purchase foods from farms through farmers markets and other avenues
• Support healthy food and beverage choices: Restrict availability of less healthy foods and
beverages and offer smaller portion size options in public service venues; limit advertising of
less healthy foods and beverages; and discourage consumption of sugar-sweetened beverages
• Create safe communities that support physical activity: Improve access to outdoor recreational
facilities such as parks and playgrounds; support bicycling and walking by creating bike lanes
and shared-use paths and improving or installing sidewalks, walking trails, pedestrian crossings,
etc.; locate schools within easy walking distance of residential areas; improve access to public
transportation; and locate different kinds of public land uses near one another to decrease the
distance and encourage people to walk between destinations such as home and shopping; and
enhance personal and traffic safety in areas where people are or could be physically active.
179
CHRONIC DISEASES
Data Sources: Adult Overweight & Obesity
tables:
Tables 1-4: Adult overweight and obesity data was taken from the California Health Interview Survey (CHIS) 2007;
retrieved 8/23/10 from http://www.chis.ucla.edu. Body mass index (BMI) data from CHIS is based on self-reported height
and weight and was calculated by CHIS by dividing weight (in kilograms) by height squared (in meters). Greater Bay Area
data include the following counties: Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano
and Sonoma.
Table 4: Data presented for Latinos include Latino residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans include non-Latino residents. Not all races/ethnicities are shown but all are included in
the greater Bay Area total.
text:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
White House Task Force on Childhood Obesity. (2010) Report to the President: Solving the Problem of Childhood
Obesity within a Generation. Retrieved September 9, 2010 from Let’s Move website:
http://www.letsmove.gov/pdf/TaskFroce_on_Childhood _Obesity_May2010_Full Report.pdf
Centers for Disease Control and Prevention (2010). About BMI for Adults. Retrieved 9/13/10 from
http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html
Ogden CL, Carroll MD. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults: United States,
Trends 1976–1980 Through 2007–2008. Health-E Stats, June 2010.
http://www.cdc.gov/NCHS/data/hestat/obesity_adult_07_08/obesity_adult_07_08.pdf. Accessed 8.11.10
Flegal KM, Carroll MD, Ogden CL; et al. (2010) Prevalence and Trends in Obesity Among US Adults, 1999–2008.
JAMA;303:235–241.
Centers for Disease Control and Prevention. (2010) Vital Signs: State-Specific Obesity Prevalence Among Adults –
United States, 2009. MMWR; 59 Early Release: 1-5. August 3, 2010.
Centers for Disease Control and Prevention (2009). Causes and Consequences of Obesity. Retrieved August 6, 2010
from http://www.cdc.gov/obesity/causes/index.html
Physical Activity Guidelines for Americans (2008). http://www.health.gov/paguidelines/guidelines/summary.aspx
Dietary Guidelines for Americans (2005) http://www.health.gov/dietaryguidelines/dga2005/document/html/
chapter3.htm
Centers for Disease Control and Prevention. (2008) Behavioral Risk Factor Surveillance Survey. Retrieved August 12,
2010 at http://apps.nccd.cdc.gov/BRFSS-SMART/index.asp
California Health Interview Survey (2007). Retrieved September 3, 2010.
Centers for Disease Control and Prevention. (2007) Behavioral Risk Factor Surveillance Survey. Retrieved August 12,
2010 at http://apps.nccd.cdc.gov/BRFSS-SMART/index.asp
Khan L.K., Sobush K., Keener D., Goodman K., Lowry A., Kakietek J., Zaro S. (2009) Recommended Community
Strategies and Measurements to Prevent Obesity in the United States, MMWR; 58(RR07);1-26. July 24, 2009
Keener, D., Goodman K., Lowry A., Zaro, S., Kettel Khan, L. (2009) Recommended Community Strategies and
Measurements to Prevent obesity in the United States: Implementation and Measurement Guide. Atlanta, GA: U.S.
Department of Health and Human Services, Center for Disease Control and Prevention.
180
CHRONIC DISEASES
Childhood Overweight & Obesity
More than one in four fifth-graders
in Contra Costa was overweight or obese.
• Among fifth-graders, boys were more likely to be overweight or obese than girls.
• Latino and African American fifth-graders were more likely to be overweight or obese
than fifth-graders in the county overall.
• Antioch, West Contra Costa and Pittsburg unified school districts had higher percents of
overweight or obese fifth-graders compared to the county overall.
In 2008–2009, an estimated 3,136 fifth-graders in Contra Costa were overweight or obese. Contra
Costa fifth-graders were less likely to be overweight or obese than their peers statewide. The percent of
overweight or obese fifth-graders was lower in Contra Costa (26.5%) than California as a whole (31.6%).
The following school districts had the greatest number of overweight or obese fifth-graders: West Contra
Costa Unified (826), Mt. Diablo Unified (658), Antioch Unified (531), Pittsburg Unified (270), San
Ramon Valley Unified (259) and Brentwood Union (249) school districts. Districts with a significantly
higher percent of overweight or obese fifth-graders than the county overall (26.5%) included: Antioch
Unified (36.6%), West Contra Costa Unified (36.5%) and Pittsburg Unified (36.2%).
Several districts had a significantly lower percent of overweight or obese fifth-graders than the county
overall: Walnut Creek Elementary (19.1%), Lafayette Elementary (16.3%), Moraga Elementary (13.0%),
San Ramon Valley Unified (12.6%) and Orinda Union Elementary (9.6%) school districts.
181
CHRONIC DISEASES
Table 1 Overweight or obese fifth-graders by school district
Contra Costa County, 2008–2009
Number Prevalence
West Contra Costa Unified
826
36.5%*
Mt. Diablo Unified
658
26.2%
Antioch Unified
531
36.6%*
Pittsburg Unified
270
36.2%*
San Ramon Valley Unified
259
12.6%**
Brentwood Union Elementary
249
27.3%
Martinez Unified
69
25.0%
Walnut Creek Elementary
65
19.1%**
Lafayette Elementary
58
16.3%**
Byron Union Elementary
46
25.0%
John Swett Unified
27
24.5%
Moraga Elementary
25
13.0%**
Orinda Union Elementary
24
9.6%**
Knightsen Elementary
15
NA
Total
3,136
In this report, data on
“overweight or obese”
children are based
on measurements
taken as part of the
California Department
of Education’s Physical
Fitness test. For more
information, see the
notes at the end of
this section.
26.5%
Total includes all fifth-graders for whom data was reported.
* Significantly higher percent than the county overall.
** Significantly lower percent than the county overall.
Students from low-income communities were more likely to be overweight or obese than those in the
county overall. All three Contra Costa school districts with a greater proportion of overweight fifthgraders had a higher percentage of students at schools with fifth-graders who were eligible for free
and reduced-priced meals compared to the county overall (40.0%): Pittsburg Unified (80.1%), West
Contra Costa Unified (70.0%) and Antioch Unified (56.9%).1
The greatest number of overweight or obese fifth-graders in Contra Costa was Hispanic/Latino (1,278)
followed by white (897), African American/black (464) and Asian (356). A significantly higher percentage of Hispanic/Latino (36.6%) and African American/black (34.2%) fifth-graders were overweight
or obese than fifth-graders in the county overall (26.5%). A significantly lower percentage of Asian
(20.7%) and white (18.6%) fifth-graders were overweight or obese than fifth-graders countywide. [Note:
Although the percent overweight or obese Native Hawaiian/Pacific Islander students appears higher than
the county, due to the small sample size the estimate is not very precise and therefore it is not statistically
significantly different from the county estimate.]
182
CHRONIC DISEASES
Table 2 Overweight or obese fifth-graders by race/ethnicity
Contra Costa County, 2008–2009
Number
Hispanic/Latino
1,278
Prevalence
36.6%*
White
897
18.6%**
African American/Black
464
34.2%*
Asian
356
20.7%**
Native Hawaiian/Pacific Islander
34
American Indian/Alaska Native
16
Total
3,136
35.5%
NA
26.5%
Total includes racial/ethnic groups not listed above.
* Significantly higher percent than fifth-graders in the county overall.
** Significantly lower percent than fifth-graders in the county overall.
In 2008–2009, there were almost twice as many overweight or obese fifth-grade boys as girls in Contra
Costa. Among fifth-graders in the county, boys were also more likely than girls to be overweight or
obese. More than one-third (34.0%) of fifth-grade boys were overweight or obese compared to less than
one-fifth (18.7%) of girls. However, at older ages, boys and girls were equally likely to be overweight or
obese. By ninth-grade the percent of overweight or obese boys (25.5%) and girls (26.4%) was similar.
What is childhood overweight & obesity?
Obesity is excess body fat.2 Body fat can be difficult to measure, so obesity is often identified using
body mass index (BMI), a number calculated from height and weight.3 Although BMI is a fairly good
indicator of body fatness, it is not a direct measure of fatness, so a health care provider should determine whether a child has an unhealthy amount of body fat.3
Typically, the terms “overweight” and “obese” for children refer to the Centers for Disease Control and
Prevention (CDC) definitions, which are based on BMI ranges for children that vary by gender and age:
children with a BMI between the 85th and 95th percentile for their age and gender are considered overweight; those with a BMI for age at or above the 95th percentile are considered obese.4
In this report, fifth-grade overweight and obesity data come from the body composition portion of the
State Physical Fitness Test. Fifth-graders were considered overweight or obese if their body composition
measurement on this test was higher than the “Healthy Fitness Zone” (HFZ). BMI ranges for the HFZ do
not exactly match the CDC’s ranges for child overweight and obesity mentioned earlier.5 However, all
children with a BMI higher than the HFZ would be considered overweight or obese based on the CDC’s
standards. Because the HFZ range is slightly more forgiving than the CDC’s criteria, the estimates of
183
CHRONIC DISEASES
the percent of overweight or obese fifth-graders in this report are lower than they would be if the
CDC’s standards were used.
Why is it important?
In Contra Costa, more than one in four fifth-graders (26.5%) was overweight or obese in 2008–2009
and more than one in seven low-income preschoolers participating in the Child Health & Disability
Prevention Program in the county (15.9%) was obese in 2008.6
In the United States, nearly one-third (31.7%) of U.S. children and adolescents (2–19 years old) were
overweight or obese in 2007–2008.7 An alarming 16.9% of 2-19 year olds were obese: 10.4% of 2–5 year
olds; 19.6% of 6–11 year olds and 18.1% of 12-19 year olds.7 Nationally, the percent of obese schoolaged children and youths in the United States has tripled since 1980.7
Obese young people are at risk for a number of health problems throughout their lives. Children who
are obese in their preschool years are more likely to be obese as adolescents and adults.8 Young
people who are obese are more likely than others to develop risk factors associated with cardiovascular disease, including high blood pressure and high cholesterol levels, as well as bone and joint
problems and sleep apnea.9 They are also more likely to become overweight or obese adults and
thus to develop related health problems including heart disease, type 2 diabetes, stroke and some
forms of cancer.9 Social pressures related to being too heavy can contribute to low self-esteem and
other social and psychological consequences among young people.9
In addition to the health and quality-of-life implications, the financial burden of this disease is tremendous. Childhood obesity is responsible for $14.1 billion in direct health care costs.10 Total costs
for obesity-related hospitalizations of children and adolescents nearly doubled from $125.9 million
in 2001 to $237.6 million in 2005.10
Who is most impacted?
Racial/ethnic differences in childhood overweight and obesity exist. Hispanic/Latino and African American/black fifth-graders were more likely to be overweight or obese than fifth-graders in Contra Costa
overall in 2008–2009. In the United States a higher percentage of Hispanic boys and black girls were
obese compared to their white peers in 2007–2008.7 These differences exist early on and also impact
young American Indian/Alaska Native children nationally. A recent study of 4 year olds in the United
States found that the highest percentage of obese children was among American Indian/Alaska Native children followed by Hispanic and black children.11
Income disparities also exist. School districts in Contra Costa with a higher percentage of overweight
or obese fifth-graders also had a greater percentage of low-income students than the county overall
in 2008–2009. Also at the county level, a higher percentage of adolescents in families with household
incomes below 200% of the federal poverty level (64.7%) were overweight or obese compared to those
in families with household incomes at or above 200% of the federal poverty level (18.2%) in 2007.12
184
CHRONIC DISEASES
There is no single cause of overweight and obesity.13 Children become overweight or obese when they
consume more calories than they expend through physical activity, and normal growth and development.13 Although some children may be more likely to gain excess weight as a result of their genetics, behaviors including not getting enough physical activity, spending too much time being sedentary,
and consuming too many calories (e.g., eating large food and drink portion sizes, calorie-dense foods
and sugar-sweetened beverages) play an important role in the development of obesity.13 Social and
physical environments at home, in child care settings, schools and communities can support or hinder
these behaviors.
What can we do about it?
To support healthy growth and development, public health recommendations suggest that children and
adolescents engage in at least 60 minutes of physical activity most, preferably all, days of the week;
limit time spent being sedentary (e.g., children’s total electronic media time, including television viewing time, should be no more than one to two hours a day); and eat a balanced, nutritious, age-appropriate diet that includes reasonable portion sizes, a variety of fruits and vegetables, whole grains, lean
meats, low fat dairy, and limited sugar, salt and fat.14, 15
Unfortunately, young people do not get adequate physical activity or eat enough fruits and vegetables.
In Contra Costa in 2007, only 35.4% of 5—11 year olds were physically active for at least one hour daily.16
More than half (57.7%) of 2—11 year olds consumed fewer than five servings of fruits and vegetables
daily and almost two-thirds (62.7%) ate fast food at least once a week.16
Healthy eating and physical activity behaviors can decrease the risk of becoming obese.1 It is particularly important for children to establish healthy habits for eating and active play early in life. Children
who are physically active are more likely to be active as adolescents and adults.13 Since home, school
and other community environments have the potential to influence children’s eating and physical activity behaviors, programs and policies that support healthy choices for children and their families in
these environments are critical to address this problem.8,13
The CDC’s Division of Nutrition, Physical Activity and Obesity recommends the following to address childhood obesity: increase breastfeeding (initiation, duration and exclusivity), physical activity and fruit and
vegetable consumption; decrease consumption of sugar-sweetened beverages, high energy-dense foods
(i.e., foods high in calories per gram weight), and television viewing.17 In May 2010, the U.S. Childhood
Obesity Task Force developed an action plan to reduce childhood obesity to 5% by 2030.1 The plan suggests that comprehensive approaches involving multiple sectors in society are needed to address the
behavioral risk factors associated with obesity.2 A summary of the Task Force’s recommendations follows:
• Start early with: good prenatal care for parents to ensure healthy weight at conception and during
pregnancy; support for breastfeeding; and quality child care environments that offer healthy foods
and beverages, and plenty of opportunities for young children to be physically active. Limiting
“screen time” (i.e., time spent in sedentary activities such as watching television or playing computer
games) is another important strategy to begin implementing early in life.
185
CHRONIC DISEASES
• Help parents and caregivers make healthy choices for children with simple, useful nutritional
information and better food package and menu labeling; less marketing of unhealthy products to
children, and improved health care services including BMI measurement for all children.
• Provide greater access to healthy foods by: improving the nutritional quality of federally-supported
school meal programs and other foods and beverages sold in schools and offered through afterschool programs; increasing access to affordable, healthy food in neighborhoods in underserved
communities through new supermarkets and grocery stores and farmers markets; and lowering
the price of healthy foods relative to unhealthy foods.
• Encourage children to be more physically active by: providing quality physical education, recess and
other physical activity opportunities during and after school; creating better access to safe parks,
playgrounds, and indoor and outdoor recreational facilities; and modifying the built environment
to make it easier for young people to walk or bike safely in their communities.
Data Sources: Childhood Overweight & Obesity
tables
Tables 1–2: Overweight and obesity data from the California Department of Education (CDE), Standards and Assessment
Division, 2008–2009 California Physical Fitness Report. Retrieved February 4, 2010 from http://dq.cde.ca.gov/dataquest/.
These analyses are based on data from the Body Composition portion of the CDE Physical Fitness Test, which uses several
methods to evaluate children’s body composition: (1) body mass index (BMI), calculated from measured height and
weight and (2) body fatness using triceps and calf skinfolds. Students were considered “overweight” or “obese” if their
body composition (i.e., BMI or body fatness) was higher than the “Healthy Fitness Zone (HFZ),” a range developed by The
Cooper Institute to indicate the minimum level of fitness thought to provide some protection from health risks associated
with inadequate fitness. The HFZ for the body composition test does not directly correspond to the Centers for Disease
Control and Prevention categories of “overweight” or “obese.” However, all children with a BMI higher than the HFZ
would be considered overweight or obese based on the CDC’s standards. Because the HFZ range is slightly more generous
than the CDC’s criteria, the estimates of the percent of overweight or obese 5th graders in this report are lower than they
would be if the CDC’s standards were used. For more information about calculating and interpreting BMI for children, go
to the CDC’s website: http://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html.
For more information about the Healthy Fitness Zone, see the CDE Physical Fitness Test—Report Definitions at
http://dq.cde.ca.gov/dataquest/PhysFitness/gls_pft_hfz.asp
Also seeThe Cooper Institute’s Fitness gram/Activitygram Reference Guide at
http://www.cooperinstitute.org/ourkidshealth/fitnessgram/documents/FITNESSGRAM_ReferenceGuide.pdf.
The CDE’s aggregate data for number of students tested and percent of students outside the HFZ on the body composition
test were used by Contra Costa Health Services’ Community Health Assessment Planning and Evaluation Unit (CHAPE)
to calculate the number of overweight or obese students. Because the CDE includes “partially tested students” in the total
number of students tested, the number of overweight or obese students calculated by CHAPE may be an overestimate.
Counts fewer than five are not shown in order to protect anonymity. Overweight and obesity statistics were not calculated
for any group with fewer than 20 cases due to unstable estimates.
Fifth-grade students from several school districts and schools were included in the county total but are not listed
separately. Data was not available for all schools. Oakley Unified School District did not provide fitness test data to
the state and is therefore not included in the county total. Data presented for Hispanics/Latinos include Hispanic/
Latino students of any race. Data presented for whites, Native Hawaiian/Pacific Islanders, Asian, American Indians/
186
CHRONIC DISEASES
Alaska Natives, and African Americans/blacks include non-Hispanic students. Not all race/ethnicities shown but all
are included in totals for the county. “Asian” includes: Asian Indian, Filipino, Cambodian, Chinese, Japanese, Korean,
Laotian Vietnamese and Other Asian. “Native Hawaiian/Other Pacific Islander” includes Native Hawaiian, Samoan and
Other Pacific Islander. County total included data for several groups of students for whom data is not available separately
including those who declined to state their race and Guamanian, Tahitian and Cambodian students.
text
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
California Department of Education School Fiscal Services Division. October 2008 School Level Free and Reduced
Priced Eligibility Data File from the 2008-09 Consolidated Application, Part II, Page 46 as of 4/1/10; retrieved 7/12/10
from: http://www.education.ca.gov/ds/sh/cw/documents/frpm2008.xls
White House Task Force on Childhood Obesity. (2010) Report to the President: Solving the Problem of Childhood
Obesity within a Generation. Retrieved September 9, 2010 from the Let’s Move website
http://www.letsmove.gov/pdf/TaskForce_on_Childhood_Obesity_May2010_FullReport.pdf
American Academy of Pediatrics (2003). American Academy of Pediatrics Policy Statement, Committee on Nutrition,
Prevention of Pediatric Overweight and Obesity. Pediatrics 112(2).
Centers for Disease Control and Prevention (2009). Defining Childhood Overweight and Obesity. Retrieved August 9,
2010 at http://www.cdc.gov/obesity/childhood/defining.html
California Department of Education (n.d.) Physical Fitness Test Glossary/Report Definitions: The “Healthy Fitness
Zone.” Retrieved October 18, 2010 at
http://dq.cde.ca.gov/dataquest/PhysFitness/gls_pft_hfz.asp
Pediatric Nutrition Surveillance System Growth Indicators by Race/Ethnicity and Age, Children Aged <5 years.
(2008) Retrieved August 10, 2010 at
http://www.dhcs.ca.gov/services/chdp/Documents/PedNSS/2008/16B0to5.pdf
Ogden CL, Carroll MD, Curtin LR, et al. (2010) Prevalence of High Body Mass Index in U.S. Children and
Adolescents, 2007-2008. Journal of the American Medical Association, 303(3): 242-9.
MMWR (2009) Obesity Prevalence Among Low-Income, Preschool-Aged Children – United States, 1998-2008;
58(28):769-773.
Centers for Disease Control and Prevention. (2010) Childhood Obesity. Retrieved September 7, 2010 from
http://www.cdc.gov/HealthyYouth/obesity/
Levi J, Vinter S, St Laurent R, Segal L. (2010) F as in Fat: How Obesity Threatens America’s Future.
Anderson S.E., Whitaker R.C. Prevalence of Obesity Among U.S. Preschool Children in Different Racial and Ethnic
Groups. Archives of Pediatrics and Adolescent Medicine (2009). 163 (4):344-348.
California Health Interview Survey (2007). Data retrieved from AskCHIS on October 15, 2010.
Centers for Disease Control and Prevention. (2009) Childhood Overweight and Obesity: Contributing Factors.
Retrieved July 23, 2010 from the CDC website: http://www.cdc.gov/obesity/childhood/causes.html
Centers for Disease Control and Prevention. (2010) Physical Activity Guidelines for Americans: Children and
Adolescents. Retrieved September 9, 2010 from http://www.cdc.gov/healthyyouth/physicalactivity/guidelines.htm
The U.S. Department of Health and Human Services and the U.S. Department of Agriculture. (2005). Dietary
Guidelines for Americans.
California Health Interview Survey (2007). Data retrieved from AskCHIS on August 6, 2010.
Polhamus B, Dalenius K, Mackentosh H, Smith B, Grummer-Strawn L.(2009) Pediatric Nutrition Surveillance 2008
Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention.
187
INJURIES
Fatal and Non-Fatal Unintentional Injury
Residents 65 years and older were most
at risk for unintentional injuries.
•
•
•
•
•
The most common cause of unintentional injury deaths was motor vehicle accidents.
The leading cause of unintentional injury hospitalizations was falls.
African Americans were most likely to die from unintentional injuries.
Whites were most likely to be hospitalized for unintentional injuries.
Residents 65 years and older were most likely to die from and be hospitalized
for unintentional injury.
Unintentional injuries are unplanned injuries that are not caused by a person’s intent to harm.1 They
include injuries from a wide assortment of causes including but not limited to: motor vehicle collisions,
poisonings, falls, drowning, burns, cutting/piercing, firearms, choking and suffocations. The leading
causes of unintentional injuries vary by age.
Unintentional Injury Deaths
There were 827 Contra Costa residents who died from unintentional injuries between 2005 and 2007,
which means that on average 276 residents died from unintentional injuries each year. During this
time, unintentional injuries accounted for 4.1% of all deaths, making it the sixth leading cause of death
in the county.
The crude death rate from unintentional injuries for Contra Costa (26.7 per 100,000) was lower than
the crude rate for California (29.5 per 100,000).
Table 1 Unintentional injury deaths by race/ethnicity
Contra Costa County, 2005 –2007
Deaths
White
Hispanic
African American
Asian/Pacific Islander
Total
509
129
121
53
827
Percent
61.5%
15.6%
14.6%
6.4%
100.0%
Rate
31.5*
19.6**
43.2*
13.3**
26.7
These are crude rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of deaths from unintentional injuries in Contra Costa occurred among whites
(509), followed by Hispanics (129), African Americans (121) and Asians/Pacific Islanders (53).
188
INJURIES
Even though African Americans died in fewer numbers from unintentional injuries, they had the highest
death rate from unintentional injuries (43.2 per 100,000); higher than the rates for the county overall
(26.7 per 100,000) and all other racial/ethnic groups listed. Whites (31.5 per 100,000) had a significantly
higher death rate from unintentional injuries compared to the county overall. Hispanic (19.6 per 100,000)
and Asians/Pacific Islanders (13.3 per 100,000) had significantly lower death rates from unintentional
injuries than the county overall.
Table 2 Unintentional injury deaths by gender
Contra Costa County, 2005-2007
Deaths
Men
Women
Contra Costa Total
540
287
827
Percent
Rate
65.30%
34.70%
100.00%
35.6*
18.2
26.7
These are crude rates per 100,000 residents.
*Significantly higher rate compared to county women overall.
Almost twice as many males (540) died from unintentional injuries as females (287). Males also had a
significantly higher unintentional injury death rate (35.6 per 100,000) than females (18.2 per 100,000).
Table 3 Unintentional injury deaths by selected cities
Contra Costa County, 2005-2007 Deaths
Concord
108
Richmond
95
Antioch
94
Walnut Creek
73
Pittsburg
62
Martinez 44
San Pablo
36
Brentwood
35
Pleasant Hill 25
Oakley 24
El Cerrito
23
Bay Point
22
Pinole
18
Hercules 13
Contra Costa Total
827
Percent
13.10%
11.50%
11.40%
8.80%
7.50%
5.30%
4.40%
4.20%
3.00%
2.90%
2.80%
2.70%
2.20%
1.60%
100.00%
These are crude rates per 100,000 residents.
Contra Costa Total includes cities not listed above.
*Significantly higher rate than the county overall.
189
Rate
29.2
30.8
31.5
37.2*
33
40.6*
38.8
24.9
25.2
26
33.1
32.4
NA
NA
26.7
INJURIES
The greatest number of unintentional injury deaths occurred among residents of Concord (108),
Richmond (95), Antioch (94) and Walnut Creek (73). The unintentional injury death rate for residents
of Martinez (40.6 per 100,000) and Walnut Creek (37.2 per 100,000) were significantly higher than the
county overall (26.7 per 100,000). In Walnut Creek, falls accounted for the greatest percentage (41%)
of unintentional injury deaths. In Martinez, poisonings accounted for the greatest percentage (34%)
of unintentional injury deaths.
Table 4 Unintentional injury deaths by cause
Contra Costa County, 2005 –2007
Cases
Percent
Rate
264
239
152
32
24
827
31.9%
28.9%
18.4%
3.9%
2.9%
100.0%
8.5
7.7
4.9
1.0
0.8
26.7
Motor vehicle traffic
Poisoning
Fall
Choking/suffocation
Drowning
Total
These are crude rates per 100,000 residents.
Total includes causes not listed above.
In Contra Costa, the leading cause of unintentional injury death was motor vehicle accidents (264),
followed by poisonings (239), falls (152), choking/suffocation (32) and drowning (24).
Table 5 Unintentional injury deaths by age
Contra Costa County, 2005 –2007
Cases
Percent
Rate
90
269
256
212
827
10.9%
32.5%
31.0%
25.6%
100.0%
10.1**
26.8
31.1
57.3*
26.7
0–20 years
21–44 years
45–64 years
65 years and older
Total
These are age-specific rates per 100,000 residents.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
The greatest number of unintentional injury deaths occurred among Contra Costa residents ages 21
to 44 years (269), followed by 45–64 years (256), 65 years and older (212) and 0-20 years (90).
Residents ages 65 years and older had the highest rate (57.3 per 100,000) of unintentional injury death
in the county; significantly higher than the rates for the county overall (26.7 per 100,000) and all other
age groups listed. Residents 0–20 years had the lowest rate (10.1 per 100,000); significantly lower than
the county overall and all other age groups.
190
INJURIES
The leading causes of unintentional injury death vary by age group. The exposure to injury risk changes
over a person’s lifetime, as does the body’s ability to recover from injury. Motor vehicle accidents are
the leading cause of unintentional injury death for younger age groups whereas falls are the leading
cause among the elderly.
Residents 0–20 years
The death rate due to unintentional injuries was lowest among residents 0–20 years (10.1 per 100,000).
More than half (53.3%) of the unintentional deaths within this age group were due to motor vehicle
accidents.
Residents 21–44 years
The unintentional injury death rate for residents 21–44 years (26.8 per 100,000) was similar to the
county rate. Motor vehicle accidents (108) and poisonings (107) were the leading causes of unintentional
injury death for this age group.
Residents 45–64 years
The unintentional injury death rate for residents 45–64 years (31.1 per 100,000) was similar to the county
rate. Almost half (45.7%) of the unintentional injury deaths among residents of this age group were
due to poisonings. Residents of this age had a higher death rate from poisonings (14.2 per 100,000)
than the county overall (7.7 per 100,000).
Residents 65 years and older
Residents 65 years and older had the highest unintentional injury death rate (57.3 per 100,000) in the
county. More than half (56.1%) of all unintentional injury deaths in this age group were due to falls,
and almost one-fifth (18.4%) were due to motor vehicle accidents. Residents of this age group had
the highest death rate due to falls (32.1 per 100,000); significantly higher than the rates for the county
overall (4.9 per 100,000) and all other age groups.
Unintentional Injury Hospitalizations
To understand the impact of unintentional injury it is important to assess hospitalizations in addition
to deaths. Death data indicate the ultimate toll that unintentional injury takes on people’s lives, but
more people experience unintentional injuries than die from them. Non-fatal unintentional injuries,
though not severe enough to cause death, can have lasting consequences in terms of physical, mental,
and emotional health. Those that result in hospitalization are the most severe. Other less-severe
unintentional injuries are treated at home, in emergency departments and/or outpatient clinics.
Between 2005–2007, there were 16,613 unintentional injury hospitalizations among Contra Costa
residents. This means that on average, there were 5,538 hospitalizations in Contra Costa due to unintentional injuries each year. The crude hospitalization rate from unintentional injuries for Contra
Costa (537.1 per 100,000) was lower than California’s crude rate (552.1 per 100,000).
191
INJURIES
Table 6 Unintentional injury hospitalizations
By Race/Ethnicity Contra Costa County, 2005 – 2007
White
Hispanic
African American
Asian/Pacific Islander
Total
Cases
Percent
Rate
11,708
1,636
1,441
791
16,613
70.5%
9.8%
8.7%
4.8%
100.0%
723.7*
248.5**
514.0
199.0**
537.1
These are crude rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
**Significantly lower rate than the county overall.
The greatest number of unintentional injury hospitalizations was among whites (11,708), followed by
Hispanics (1,636), African Americans (1,441) and Asians/Pacific Islanders (791).
Whites had the highest rate of hospitalizations due to unintentional injuries (723.7 per 100,000); significantly higher than the rates for the county overall (537.1 per 100,000) and all other racial/ethnic groups
listed. More than half (59.2%) of all unintentional injury hospitalizations among whites were caused
by falls. Hispanics (248.5 per 100,000) had a significantly lower unintentional injury hospitalization
rate compared to the county overall. Asians/Pacific Islanders (199.0 per 100,000) had the lowest rate,
significantly lower than the county overall and all other racial/ethnic groups listed.
Table 7 Unintentional injury hospitalizations by gender
Contra Costa County, 2005 – 2007
Females
Males
Total
Cases
Percent
8,685
7,928
16,613
52.3%
47.7%
100.0%
Rate
550.9*
522.7
537.1
These are crude rates per 100,000 residents.
*Significantly higher rate than county males overall.
The number of unintentional injury hospitalizations was significantly higher among females (8,685)
than males (7,928). Females had a higher unintentional injury hospitalization rate (550.9 per 100,000)
than males (522.7 per 100,000).
192
INJURIES
Table 8 Unintentional injury hospitalizations by age
Contra Costa County, 2005 – 2007
0-14 years
15-24 years
25-34 years
35-44 years
45-54 years
55-64 years
65 years and older
Total
Cases
Percent
Rate
1,097
1,204
1,012
6.6%
7.2%
6.1%
172.3**
294.4**
260.2**
1,382
1,875
1,845
8,198
16,613
8.3%
11.3%
11.1%
49.3%
100.0%
297.1**
394.6**
530.4
2,214.7*
537.1
These are age-specific rates per 100,000 residents.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
Almost half (49.3%) of the county’s unintentional injury hospitalizations occurred among residents
65 years and older and more than three-quarters (75.9%) of these hospitalizations were due to falls.
Residents 65 years and older had the highest unintentional injury hospitalization rate (2,214.7 per
100,000); significantly higher than the rates for the county overall (537.1 per 100,000) and all other age
groups listed. Residents 0-14 years (172.3 per 100,000) had the lowest unintentional injury hospitalization rate; significantly lower than the county overall and all other age groups.
Table 9 Unintentional injury hospitalizations by cause
Contra Costa County, 2005–2007
Cases
Fall
Motor vehicle traffic
Poisoning
Natural/environmental
Struck by object
Overexertion
Total
8,880
2,244
1,245
436
404
351
16,613
Percent
53.5%
13.5%
7.5%
2.6%
2.4%
2.1%
100.0%
Rate
287.1
72.5
40.3
14.1
13.1
11.3
537.1
These are crude rates per 100,000 residents.
Total includes causes not listed above.
More than half (53.5%) of unintentional injury hospitalizations were due to falls, followed by motor
vehicle traffic accidents (13.5%) and poisonings (7.5%). Falls were the leading cause of unintentional
injury hospitalizations for all racial/ethnic groups included in this section.
193
INJURIES
Twelve ZIP codes comprised more than half (56.7%) of the unintentional injury hospitalizations in
the county: 94565, 94509, 94595, 94553, 94806, 94520, 94521, 94513, 94523, 94598, 94804 and 94549.
Each of these ZIP codes accounted for more than 500 cases. (See Table 10)
Ten ZIP codes had significantly higher unintentional injury hospitalization rates than the county
overall: 94509, 94595, 94520, 94523, 94598, 94549, 94548, 94596, 94563 and 94525. Falls among white
residents 65 years and older were the predominant cause of unintentional injury hospitalizations in
the red-shaded ZIP codes in Central County. Sixteen ZIP codes had significantly lower unintentional
injury hospitalization rates than the county overall (see table and map of rates by ZIP code).
A stable rate could not be calculated for ZIP codes with fewer than 20 cases. If denominator data was
available, statistical testing generated a confidence interval for these ZIP codes to determine whether
the rate range was lower, higher or similar to the county rate.
Table 10 Unintentional injury hospitalizations by ZIP codes
Contra Costa County, 2005 –2007
Cases
94505ª+
94506
94507
94509
94511ª+
94513
94514
94517
94518
94519
94520
94521
94522+
94523
94524+
94525
94526
94528
94530
94531
94547
94548
94549
94553
94556
22
211
241
1263
82
653
185
212
487
297
687
670
7
649
7
72
493
20
414
383
204
21
524
831
265
194
Percent
0.1%
1.3%
1.5%
7.6%
0.5%
3.9%
1.1%
1.3%
2.9%
1.8%
4.1%
4.0%
0.0%
3.9%
0.0%
0.4%
3.0%
0.1%
2.5%
2.3%
1.2%
0.1%
3.2%
5.0%
1.6%
Rate
NA
240.8**
519.6
640.4*
NA
471.0**
461.8**
483.0
574.8
502.7
597.9*
517.0
NA
632.7*
NA
719.6*
540.4
848.9
576.7
315.1**
302.7**
3818.2*
618.7*
562.9
528.7
INJURIES
Cases
94561
94563
94564
94565
94569
94572
94575+
94582
94583
94595
94596
94597
94598
94801
94802+
94803
94804
94805
94806
94807+
Total
455
349
258
1265
6
149
6
122
449
983
465
263
600
441
10
374
549
184
753
11
16,613
These are crude rates per 100,000 residents.
Total includes ZIP codes not listed above.
*Significantly higher rate compared to the county overall.
**Significantly lower rate compared to the county overall.
ª Rate unavailable due to lack of denominator.
+ ZIP code not mapped.
195
Percent
2.7%
2.1%
1.6%
7.6%
0.0%
0.9%
0.0%
0.7%
2.7%
5.9%
2.8%
1.6%
3.6%
2.7%
0.1%
2.3%
3.3%
1.1%
4.5%
0.1%
100.0%
Rate
448.3**
634.2*
466.0**
493.3**
NA
584.1
NA
231.4**
443.5**
1913.7*
774.0*
387.4**
754.5*
468.2**
NA
460.0**
453.8**
434.3**
415.0**
NA
537.1
INJURIES
196
INJURIES
What is unintentional injury?
Injuries are characterized as intentional or unintentional. Unintentional injuries are unplanned injuries
that are not caused by a person’s intent to harm.1 Although often labeled as “accidents”, unintentional
injuries are preventable and sometimes predictable.2 They include motor vehicle crashes, poisonings,
falls, drowning, burns, cuts, choking and suffocations.
Intentional injuries including homicides, assaults, suicides and self-inflicted injuries are presented in
other sections of this report.
Why is it important?
Between 2005–2007, unintentional injuries accounted for 4.1% of all deaths, making it the 6th leading
cause of death in the county. Unintentional injury was the number one cause of death among residents
1–34 years old, accounting for approximately 30% of all deaths among this age group.
Injury deaths represent only a small portion of the people affected by unintentional injury. For each of
the 179,065 U.S. deaths due to injuries (both intentional and unintentional) in 2006, there were nearly
11 times as many hospitalizations and 179 times as many emergency department visits.3 There were
34 million outpatient visits in the United States due to unintentional injuries3 and an undetermined
number of people never seek treatment for their injuries.
Injuries that occurred in 2000 will ultimately cause an estimated $326 billion in productivity losses, as
those injured often lose part or all of their productivity potential.4
Who does it impact the most?
In Contra Costa, African Americans were most likely to die from and whites were most likely to be
hospitalized for unintentional injuries. Men were more likely to die from unintentional injuries and
women were more likely to be hospitalized from them. Adults 65 years and older had the highest
rates of death and hospitalizations from unintentional injuries, most of which were caused by falls.
Although the number of unintentional injuries to American Indian and Alaska Native people in Contra
Costa were too small to calculate a stable rate, these groups have some of the highest injury rates of
any racial group nationwide. Unintentional injuries are the leading cause of death for American Indians
and Alaska Natives 1– 44 years old.5
What can we do about it?
Although unintentional injuries are not intended, they may be prevented. Knowing where injuries take
place and what people are doing when they are injured is important for designing prevention programs.
Almost half (47%) of non-fatal injuries took place at home, and more than one-third occurred while a
person was engaged in leisure activities, including sports.3 It is also important to know the most frequent causes of injury in order to guide prevention efforts. Motor vehicle collisions, falls and increasingly, poisonings/overdoses, are responsible for most injury deaths and hospitalizations.6, 7
Prevention efforts include traditional forms of health education around these and other causes of un-
197
INJURIES
intentional injuries. Programs and campaigns can encourage people to adopt and maintain behaviors
that may reduce unintentional injuries like turning their cell phone off while driving, wearing seat
belts and bike helmets, enrolling in safe-driving programs, putting up fences around pools and labeling medications.6
Some of the most effective injury prevention strategies are the result of public health policy change
at the local, state and national level. For example, seat belt laws help to reinforce public health safety
messages and the laws that led to the beeping seat belt warnings and airbags, now standard in all
new cars, have saved many lives.
Recent Contra Costa efforts to prevent injuries have turned their focus to transportation and land-use
interventions. For example, redesigning a neighborhood’s roadways to slow traffic (“traffic calming”)
has been proven to reduce motor vehicle-related bicycle and pedestrian injuries because it changes
the environment in which people travel.8
Data Sources: Unintentional Injury
tables and map
Tables 1-10: Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning
and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the California Department of Public Health
(CDPH) or California Office of Statewide Health Planning and Development (OSHPD). Data presented for Hispanics
include Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include
non-Hispanic residents. Not all race/ethnicities are shown but all are included in totals for the county and for each gender,
age, cause and city. Rates were not calculated for any group with fewer than 20 cases due to unstable estimates.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Tables 1–5: These tables include total deaths due to unintentional injury and crude or age-specific average annual death
rates per 100,000 residents for 2005 through 2007. Unintentional injury mortality data from the California Department
of Public Health (CDPH), http://www.cdph.ca.gov/, Center for Health Statistics' Death Statistical Master File, 2005-2007.
ICD10 coding for unintentional injuries (ICD V01-X59) found at the CDHS Brand EPICenter California Injury Data
Online at http://www.applications.dhs.ca.gov/epicdata/default.htm, modified from the Centers for Disease Control
and Prevention National Center for Health Statistics, available online at: http://www.cdc.gov/nchs/data/nvsr/nvsr50/
nvsr50_16.pdf. Poisonings includes drug overdose. Late effects are not included.
Tables 6–10: These tables include total hospitalizations due to non-fatal unintentional injury and crude or age-specific
average annual hospitalization rates per 100,000 residents for 2005 through 2007. Non-fatal unintentional hospitalization
data from the California Office of Statewide Health Planning and Development (OSHPD) Patient Discharge Data files
198
INJURIES
2005-2007, http://www.oshpd.ca.gov/, Healthcare Quality and Analysis Division, Health Care Information Resource
Center.
OSHPD data includes only those hospitalizations for which an unintentional injury was listed as the primary diagnoses
(ICD E800-E928.9). They do not include treatment that takes place in a doctor’s office, health clinic or emergency room. A
single person can be counted multiple times for multiple injury hospitalizations. Poisonings includes overdose.
Table 10:
The rates for several ZIP codes are marked “NA” in the table. This is due to any one of the following reasons:
• The ZIP code has fewer than 20 cases
• A denominator for the ZIP code is not available (including P.O. box only ZIP codes)
• ZIP codes marked “+” indicate that the ZIP code is not mapped. This is due to one of the following reasons:
• The ZIP code has no denominator available: 94505
• The ZIP code is PO box only: 94511, 94522, 94524, 94575, 94802, 94807
ZIP codes with fewer than five cases and those that are shared with another county are not shown in the table.
Non-fatal Unintentional Injury Hospitalization map:
The shading for some ZIP codes indicates that the rate is not available. This is due to the following reasons:
• A denominator for the ZIP code is not available: 94505
• The ZIP code extends to areas outside of Contra Costa county: 94551, 94707, 94708
Although rates were not calculated for ZIP codes with fewer than 20 cases, statistical testing generated a confidence
interval for the ZIP code 94569 to determine that the rate range was similar to the county rate and it was shaded
appropriately on the map.
ZIP codes that are assigned to P.O. boxes only could not be shown on the map.
ZIP code population estimates for ZIP code level rates provided by the Environmental Health Investigations Branch
(EHIB) from the Environmental Systems Research Institute (ESRI) Community Sourcebook of ZIP Code Demographics.
Data was not available for all ZIP codes.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services' Office of Disease Prevention
and Health Promotion, available online at http://www.healthypeople.gov/
text
1.
2.
3.
4.
5.
6.
California Injury Prevention Network (CIPN) “Intentional Injury Prevention” webpage. Retrieved August 12, 2010
from the CIPN website:
http://www.injurypreventionnetwork.org/injury-prevention-info/intentional
Prevention Institute “Reducing Injury” webpage. Retrieved August 12, 2010 from the Prevention Institute website:
http://www.preventioninstitute.org/focus-areas/preventing-violence-and-reducing-injury/reducing-injury.html
National Center for Injury Prevention and Control, Centers for Disease Control. (2009)NCHS Data on Injuries:
Information Sheet. Retrieved April 10, 2010 at the CDC website:
http://www.cdc.gov/nchs/data/infosheets/infosheet_injury.htm
Finkelstein E.A., Corso, P.S. and Miller, T.R. (2006). The Incidence and Economic Burden of Injury in the United
States: Fact Sheet. Retrieved April 10, 2010 at the CDC website: http://www.cdc.gov/NCIPC/factsheets/Economic_
Burden_of_Injury.htm
Centers of Disease Control and Prevention. “Injuries among Native Americans: Fact Sheet”. Retrieved August 19,
2010 from http://www.cdc.gov/ncipc/factsheets/nativeamerican
Society for Public Health Education (n.d.). Injury 101. Retrieved May 21, 2007 at
http://www.sophe.org/ui/injury.shtml.
199
INJURIES
7.
8.
Paulozzi, L. Centers for Disease Control and Prevention. “Trends in Unintentional Drug Overdose Deaths” March 12,
2008. Retrieved August 20, 2010 from
http://www.hhs.gov/asl/testify/2008/03/t20080312b.html
Baer, N., Rattray, T. (2007). Planning Communities: What Health Has to Do With It. Contra Costa Health Services,
Community Wellness & Prevention Program. Retrieved April 10, 2010 at the CCHS website: http://cchealth.org/
groups/injury_prevention/pdf/planning_healthy_communities.pdf
200
INJURIES
Homicide and Non-Fatal Assault
Homicide was the fourth leading cause of death
among African Americans.
• The leading cause of homicide and hospitalized assaults was firearms.
• African American males were most likely to die from homicide.
• Residents of Richmond and San Pablo were more likely to die
from homicide than county residents overall.
• Residents 21-44 years were most likely to die from homicide.
• Males were more likely to die from homicide than females.
Homicide
There were 287 homicides among Contra Costa residents between 2005–2007. This means that on
average 96 Contra Costa residents died from homicide each year. The crude death rate from homicide
for Contra Costa (9.3 per 100,000) was higher than California’s crude rate (6.6 per 100,000).
Half (50.5%) of all homicides in Contra Costa occurred among African Americans, followed by
Hispanics (24.5%), whites (17.4%) and Asians/Pacific Islanders (5.2%).
African Americans had the highest homicide rate (51.7 per 100,000) in the county; significantly higher
than the rates for the county overall (9.3 per 100,000) and all other racial/ethnic groups listed. Whites
(3.1 per 100,000) had a significantly lower homicide rate than the county overall.
Table 1 Homicide by race/ethnicity
Contra Costa County, 2005 –2007
Deaths
African-American
Hispanic
White
Asian/Pacific Islander
Total
145
73
50
15
287
Percent
50.5%
24.5%
17.4%
5.2%
100.0%
Rate
51.7*
11.1
3.1**
NA
9.3
Homicide is any
intentionally
inflicted fatal injury
to another person.
These are crude rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
**Significantly lower rate than the county overall.
Males (84.3%) accounted for the majority of deaths from homicide and had a higher homicide rate
(16.0 per 100,000) than females (2.9 per 100,000).
201
INJURIES
Table 2 Homicide by gender
Contra Costa County, 2005 – 2007
Males
Females
Total
Deaths
Percent
Rate
242
45
287
84.3%
15.7%
100.0%
16.0*
2.9
9.3
These are crude rates per 100,000 residents.
*Significantly higher rate than county females overall.
African American males, in particular, were disproportionately affected by homicide. African American
males comprised 4.3% of the county population yet represented 43.9% of all homicides that occurred
in the county. They had the highest homicide rate (95.6 per 100,000); significantly higher than the rates
for county males overall (16.0 per 100,000) and males of any other racial/ethnic groups listed. White
males (4.3 per 100,000) had a significantly lower homicide rate than county males overall.
The greatest number of homicide deaths in Contra Costa occurred among residents ages 21–44 years
(180), and in particular among males of this age group. Residents 21–44 years had the highest homicide
rate (17.9 per 100,000); significantly higher than the rates for the county overall (9.3 per 100,000) and
all other age groups listed. Residents 45-64 years (4.1 per 100,000) had a significantly lower homicide
rate than county residents overall.
Table 3 Homicide by Age
Contra Costa County, 2005 – 2007
0-20 years
21-44 years
45-64 years
65 and older
Total
Deaths
Percent
Rate
64
180
34
9
287
22.3%
62.7%
11.8%
3.1%
100.0%
7.2
17.9*
4.1**
NA
9.3
These are age-specific rates per 100,000 residents.
*Significantly higher rate than the county overall.
**Significantly lower rate than the county overall.
The greatest number of homicides occurred among residents of Richmond (119), Antioch (35) and
San Pablo (23). Richmond (38.6 per 100,000) and San Pablo (24.8 per 100,000) had significantly higher
rates of homicide than the county overall (9.3 per 100,000).
202
INJURIES
Table 4 Homicide by selected cities
Contra Costa County, 2005–2007
Cases
Richmond
Antioch
San Pablo
Pittsburg
Concord
Walnut Creek
Pinole
Bay Point
Brentwood
Oakley
El Cerrito
Contra Costa
119
35
23
22
13
9
8
7
7
7
5
287
Percent
Rate
41.5%
12.2%
8.0%
7.7%
4.5%
3.1%
2.8%
2.4%
2.4%
2.4%
1.7%
100.0%
38.6*
11.7
24.8*
11.7
NA
NA
NA
NA
NA
NA
NA
9.3
These are crude rates per 100,000 residents.
Contra Costa total includes cities not listed above.
*Significantly higher rate than the county overall.
More than three-quarters (78.7%) of all homicide deaths in Contra Costa involved firearms.
Table 5 Homicide by cause
Contra Costa County, 2005–2007
Firearm
Other
Cut/Pierce
Total
Cases
Percent
226
34
21
287
78.7%
11.8%
7.3%
100.0%
Rate
7.3
1.1
0.7
9.3
These are crude rates per 100,000 residents.
Total includes causes not listed above.
Non-Fatal Assault Hospitalizations
To understand the impact of assault it is important to assess hospitalizations in addition to deaths.
Information about homicides indicates the ultimate toll that assault takes on people’s lives, but more
people experience assault than die from it. Assaults that are serious enough to result in hospitalization
greatly affect one’s health and well-being. Other less-severe assault injuries are treated at home, in
emergency departments or outpatient clinics.
Between 2005-2007, there were 1,144 hospitalizations due to non-fatal assaults among Contra Costa
residents. This means that on average, there were 381 hospitalizations due to assaults each year. The
crude hospitalization rate from assaults for Contra Costa (37.0 per 100,000) was lower than the crude
rate for California (39.6 per 100,000).
203
INJURIES
Table 6 Non-fatal assault hospitalizations
By Race/Ethnicity
Contra Costa County, 2005–2007
Cases
African American
White
Hispanic
Asian/Pacific Islander
Total
373
356
244
38
1,144
Percent
32.6%
31.1%
21.3%
3.3%
100.0%
Rate
133.0*
22.0**
37.1
9.6**
37.0
Non-fatal assault
is intentionally
inflicted injury to
another person
that may or
may not involve
intent to kill. In
this section we
look at non-fatal
assaults that led to
hospitalization.
These are crude rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
**Significantly lower rate than the county overall.
The greatest number of assault hospitalizations in the county was among African Americans (373),
followed by whites (356), Hispanics (244) and Asian/Pacific Islander residents (38).
African Americans had the highest assault hospitalization rate (133.0 per 100,000); significantly higher
than the rates for the county overall (37.0 per 100,000) and all other racial/ethnic groups listed. Whites
(22.0 per 100,000) had a significantly lower assault hospitalization rate than the county overall. Asians/
Pacific Islanders (9.6 per 100,000) had the lowest rate, significantly lower than the county overall and
all other racial/ethnic groups listed.
Table 7 Non-fatal assault hospitalizations by gender
Contra Costa County, 2005–2007
Cases
Males
Females
Total
959
185
1,144
Percent
83.8%
16.2%
100.0%
Rate
63.2*
11.7
37.0
These are crude rates per 100,000 residents.
*Significantly higher rate than county females overall.
Males (83.8%) experienced the majority of assault hospitalizations and had a higher rate of assault
hospitalization (63.2 per 100,000) than females (11.7 per 100,000).
African American males had the highest assault hospitalization rate (235.2 per 100,000); higher than
the rates for county males overall (63.2 per 100,000) and males of all other racial/ethnic groups listed.
White males (35.5 per 100,000) had a lower assault hospitalization rate than county males overall.
Asian/Pacific Islander males (16.2 per 100,000) had the lowest rate, lower than county males overall
and all other racial/ethnic groups listed.
204
INJURIES
Table 8 Non-fatal assault hospitalizations by age
Contra Costa County, 2005–2007
0–14 years
15–24 years
25–34 years
35–44 years
45–54 years
55–64 years
65 years and older
Total
Cases
Percent
Rate
33
453
254
180
131
54
39
1,144
2.9%
39.6%
22.2%
15.7%
11.5%
4.7%
3.4%
100.0%
5.2**
110.8*
65.3*
38.7
27.6**
15.5**
10.5**
37.0
These are age-specific rates per 100,000 residents.
*Significantly higher rate than the county overall.
**Significantly lower rate than the county overall.
More than half (61.8%) of all assault hospitalizations occurred among residents 15–34 years. Within
this age group, residents 15–24 years had the highest assault hospitalization rate (110.8 per 100,000);
significantly higher than the rates for the county overall (37.0 per 100,000) and all other age groups
listed. Residents 25–34 years old (65.3 per 100,000) had a significantly higher rate of assault hospitalizations than the county overall. Residents 0–14 years, and 45 years and older had significantly lower
rates than the county overall.
Table 9 Non-fatal assault hospitalizations by cause
Contra Costa County, 2002–2004
Firearm
Unarmed fight
Cut/pierce
Other
Blunt object
Abuse and neglect
Total
Cases
Percent
Rate
422
209
197
164
106
46
1,144
36.9%
18.3%
17.2%
14.3%
9.3%
4.0%
100.0%
13.6
6.8
6.4
5.3
3.4
1.5
37.0
These are crude rates per 100,000 residents.
Total includes causes not listed above.
The largest percentage of all assault hospitalizations involved firearms (36.9%), followed by unarmed
fights (18.3%), and cutting/piercing (17.2%).
Six ZIP codes had higher assault hospitalization rates than the county overall: 94565, 94804, 94806,
94801, 94509 and 94520. These ZIP codes comprised almost two-thirds (64.8%) of the assault hospitalizations in the county and accounted for at least 70 cases each. A stable rate could not be calculated
205
INJURIES
for ZIP codes with fewer than 20 cases. If denominator data was available, statistical testing generated
a confidence interval for these ZIP codes to determine whether the rate range was lower, higher or
similar to the county rate. One ZIP code (94548) was shown to have a rate range higher than the
county rate and is represented accordingly on the map, but because there are fewer than five cases it
is excluded from the table.
Seventeen ZIP codes had assault hospitalization rates or rate ranges lower than the overall county rate.
These ZIP codes are shaded accordingly on the map and those that had at least five cases are included
and identified in the table.
Table 10 Non-fatal assault hospitalizations by ZIP code
Contra Costa County, 2005–2007
Cases
Percent
Rate
54.8*
NA**
94509
94513
108
18
9.4%
1.6%
94518
94519
94520
94521
94523
94526
94530
94531
94547
94549
94553
94561
94564
94565
94572
94583
94595
94596
94598
94801
94803
94804
94805
94806
Total
20
11
74
18
15
5
16
37
21
13
48
26
16
158
10
11
10
10
20
128
29
144
11
129
1,144
1.7%
1.0%
6.5%
1.6%
1.3%
0.4%
1.4%
3.2%
1.8%
1.1%
4.2%
2.3%
1.4%
13.8%
0.9%
1.0%
0.9%
0.9%
1.7%
11.2%
2.5%
12.6%
1.0%
11.3%
100.0%
23.6**
NA**
64.4*
NA**
NA**
NA**
NA
30.4
31.2
NA**
32.5
25.6
NA
61.6*
NA
NA**
NA
NA**
25.2
135.9*
35.7
119.0*
NA
71.1*
37.0
These are crude rates per 100,000 residents. Total includes ZIP codes not listed above.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
206
INJURIES
207
INJURIES
What are homicides and non-fatal assaults?
Homicides and non-fatal assaults are violent injuries intentionally inflicted by one person on another.1
They result from the use of physical force or power, threatened or actual, and can involve firearms,
blunt objects, cutting/piercing, unarmed fights and abuse and neglect. Injuries caused by law enforcement officers in the line of duty, and combat deaths or acts of war are excluded from this category.
Why is it important?
Between 2005-2007, homicide was the second leading cause of death among Contra Costa residents 1534 years, accounting for more than one-quarter (28.9%) of the deaths in this age group. Homicide was
the fourth leading cause of death among African American residents.
Though there is an alarming number of homicide deaths, many more people survive this kind of violence than are killed by it. The Bureau of Justice 2003 statistics showed that for each homicide, there
were approximately 1,000 nonfatal assaults.2 In 2006, there were 1.8 million emergency department
visits for assault in the United States.3
Violence affects people in all stages of life.4 Victims of violence and those exposed to it are often left
with permanent physical injuries, chronic pain, emotional scars, disability, post-traumatic stress disorder, depression, substance abuse tendencies and sometimes profound changes in lifestyle.4,5 Violence
erodes the health of communities by reducing productivity, decreasing property values, and disrupting
public education and social services.4 Neighborhoods that offer no safe places to play put urban children and adolescents at greater risk for obesity and later cardiovascular disease.6
Who does it impact the most?
Homicide represents a troubling health disparity, disproportionately affecting young people and people
of color. Nationwide in 2007, homicide was the second leading cause of death for young people ages
10–24 years, accounting for 5,764 deaths. Of these homicides, 86% of victims were male.7
In Contra Costa, African American males had the highest rate of homicide. In the county, homicide
was the fourth leading cause of death for African Americans and the sixth leading cause of death for
Hispanics. Among U.S. youths 10–24 years, homicide was the leading cause of death for African Americans, the second leading cause for Hispanics and third leading cause for Asians/Pacific Islanders and
American Indians and Alaska Natives.7
Poverty is a risk factor associated with becoming victims or perpetrators of violence.8
What can we do about it?
Violence prevention efforts should include a continuum of strategies aimed at the individual, community and societal levels.8
Individual: Promote attitudes and beliefs that prevent violence through peer programs or mentorship.
Provide young people with crucial conflict-resolution and problem-solving skills.
208
INJURIES
Community: Build social connections within neighborhood institutions. Provide after-school programs.
Respond swiftly to reports of family violence. Limit adolescents’ access to firearms and substances often involved in violent episodes such as alcohol and other drugs.
Societal: Develop and implement legislation limiting the availability of firearms since weapons are
commonly obtained and used to commit violent acts and law regulating firearms are getting weaker.
Data Sources: Homicide and Non-Fatal Assault
tables and map
Tables 1-10: Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning and
Evaluation (CHAPE) Unit of Contra Costa Health Services and not the California Department of Public Health (CDPH)
nor the California Office of Statewide Health Planning and Development (OSHPD). Data presented for Hispanics
include Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include
non-Hispanic residents. Not all race/ethnicities are shown but all are included in totals for the county and for each gender,
age, cause and city. Counts fewer than five are not shown in order to protect anonymity. Rates were not calculated for any
group with fewer than 20 cases due to unstable estimates.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Tables 1-5: These tables include total deaths due to homicide and crude or age-specific average annual death rates per
100,000 residents for 2005 through 2007. Homicide mortality data from the California Department of Public Health
(CDPH), http://www.dhs.ca.gov/, Center for Health Statistics' Death Statistical Master File, 2005-2007.
ICD10 coding for homicide (ICD X85-Y05, Y06-Y07 (.0-.9), Y08-Y09) found at the CDHS Brand EPICenter California
Injury Data Online at http://www.applications.dhs.ca.gov/epicdata/default.htm, modified from the Centers of Disease
Control and Prevention National Center for Health Statistics available online at
http://www.cdc.gov/nchs/about/otheract/ice/matrix10.htm.
Late effects are not included. Table 5’s ICD10 coding for “other” may include homicides due to the following causes; drugs
and other biological, corrosive, and noxious substances, explosives, arson, hanging, suffocation, strangulation, drowning,
pushing from high place, rape, motor vehicle involvement
Tables 6-10: These tables include total hospitalizations due to non-fatal assault and crude or age-specific average annual
hospitalization rates for 2005 through 2007. Non-fatal assault hospitalization data from the California Office of Statewide
Health Planning and Development (OSHPD) Patient Discharge Data files 2005-2007, http://www.oshpd.ca.gov/,
Healthcare Quality and Analysis Division, Health Care Information Resource Center.
209
INJURIES
OSHPD data includes only those hospitalizations for which assault was listed as the primary diagnoses (ICD9 EE960-E968.9 and E979.0--979.9). They do not include treatment that takes place in a doctor’s office, health clinic or
emergency room. A single resident can be counted multiple times for multiple times for multiple assault hospitalizations.
Table 9’s “other” category includes non-fatal assault injuries from the following causes: rape, antipersonnel bombs,
unspecified explosives pushing from a high place, motor vehicle involvement, air gun, human bite, and other unspecified
means.
Table 10: The rates for several ZIP codes are marked “NA” in the table. This is because the ZIP code has fewer than 20
cases. ZIP codes with fewer than five cases and those that are shared with another county are not shown in the table.
Non-fatal Assault Injury Hospitalization map: The shading for some ZIP codes indicates that the rate is not available. This
is due to the following reasons:
• A denominator for the ZIP code is not available: 94505
• The ZIP code extends to areas outside of Contra Costa county: 94551, 94707, 94708
Although rates were not calculated for ZIP codes with fewer than 20 cases, statistical testing generated a confidence
interval for these ZIP codes to determine whether the rate range was similar to the county rate and it was shaded
appropriately on the map.
ZIP code population estimates for ZIP code level rates provided by the Environmental Health Investigations Branch from
the Environmental Systems Research Institute (ESRI) Community Sourcebook of ZIP Code Demographics. Data was not
available for all ZIP codes.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services' Office of Disease Prevention
and Health Promotion, available online at
http://www.healthypeople.gov/.
text
1.
2.
3.
4.
5.
6.
7.
8.
California Injury Prevention Network (CIPN) “Intentional Injury Prevention” webpage. Retrieved August 12, 2010
from the CIPN website:
http://www.injurypreventionnetwork.org/injury-prevention-info/intentional
Bureau of Justice Statistics, Criminal Victimization in the United States, 2003: Statistical Tables. Available at:
www.oip.usdoj.gov/bjs/pub/pdf/cvus03.pdf.
National Center for Health Statistics Centers for Disease Control and Prevention (2009). Fast Stats A-Z, Assault or
Homicide. Retrieved August 10, 2010 at the NCHS/CDC website: http://www.cdc.gov/nchs/fastats/homicide.htm
Centers for Disease Control and Prevention (CDC), Injury Prevention and Control: Violence Prevention website.
Retrieved August 20, 2010 from the CDC website:
http://www.cdc.gov/ViolencePrevention/
Lynch M. Consequences of children’s exposure to community violence. Clinical Child and Family Psychology
Review 2003; 6(4): 265-74.
Molnar BE, Gortmaker SL, Bull FC, Buka SL. (2004). Unsafe to play? Neighborhood disorder and lack of safety
predict reduced physical activity among urban children and adolescents. American Journal of Health Promotion.
May-Jun; 18(5): 378-86.
Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting system (WISQARS)
[online]. (2007). National Center for Injury Prevention and Control, Centers for Disease Control and Prevention
(producer). Available at: www.cdc.gov/ncipc/wisqars/default.htm
Dahlberg LL, Krug EG. (2002) Violence-a global public health problem. In: Krug E, Dahlberg LL, Mercy JA, Zwi
AB, Lozano R, eds. World Report on Violence and Health. Geneva, Switzerland: World Health Organization; 1–56.
Retrieved April 10, 2010 at the NCIPC/CDC website:
http://www.cdc.gov/ViolencePrevention/overview/social-ecologicalmodel.html
210
INJURIES
Suicide and Non-Fatal
Self-Inflicted Injury
Residents ages 15–24 years were most likely to be hospitalized
for self-inflicted injury.
• Whites were more likely to commit suicide and be hospitalized
for self-inflicted injuries than county residents overall.
• Suicide is the third leading cause of death among residents 15–34 years old.
• Females were more likely to be hospitalized for self-inflicted injury than males.
• Males were more likely to commit suicide than females.
Suicide
Between 2005–2007, 269 Contra Costa residents committed suicide. This means that on average 90
Contra Costa residents committed suicide each year. Suicide was the third leading cause of death
among Contra Costa residents 15–34 years (see Leading Causes of Death section).
The crude suicide rate for Contra Costa (8.7 per 100,000) was similar to California’s crude rate (9.0
per 100,000).
The greatest number of suicides occurred among whites (213), nearly three-fourths of these (152) were
males. Whites had the highest suicide rate (13.2 per 100,000); significantly higher than the rates for
the county overall (8.7 per 100,000) and other racial/ethnic groups listed. Hispanics (3.3 per 100,000)
and Asians/Pacific Islanders (5.0 per 100,000) had significantly lower suicide rates compared to the
county overall.
Table 1 Suicide by race/ethnicity
Contra Costa County, 2005–2007
Deaths
White
Hispanic
Asian/Pacific Islander
African American
Total
Percent
213
22
20
11
269
79.2%
8.2%
7.4%
4.1%
100.0%
Rate
13.2*
3.3**
5.0**
NA
8.7
Suicide is any
intentionally selfinflicted injury
that is fatal. Fatal
injuries due to
reckless behavior,
such as driving
while intoxicated,
are not categorized
as suicide.
These are crude rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
**Significantly lower rate than the county overall.
Males had a higher number (197) and rate (13.0 per 100,000) of suicide than females (72 and 4.6 per
100,000).
211
INJURIES
Table 2 Suicide by gender
Contra Costa County, 2005–2007
Deaths
Males
Females
Total
197
72
269
Percent
73.2%
26.8%
100.0%
Rate
13.0*
4.6
8.7
These are crude rates per 100,000 residents.
*Significantly higher rate than county females overall.
Most suicides in Contra Costa occurred among residents 21-64 years (76.2%).
Table 3 Suicide by age
Contra Costa County, 2005-2007
Deaths
0–20 years
21–44 years
45–64 years
65 years and older
Total
Percent
Rate
15
5.6%
NA
108
97
49
269
40.1%
36.1%
18.2%
100.0%
10.7
11.8
13.2
8.7
These are age-specific rates per 100,000 residents.
The highest number of suicides occurred among residents of Concord (35), followed by Walnut Creek
(30), Richmond (26) and Martinez (21). Suicide rates among residents of Martinez (19.4 per 100,000)
and Walnut Creek (15.3 per 100,000) were significantly higher than the county overall (8.7 per 100,000).
Table 4 Suicide by selected cities
Contra Costa County, 2005–2007
Deaths
Percent
35
30
26
21
18
13
12
11
8
8
5
5
269
13.0%
11.2%
9.7%
7.8%
6.7%
4.8%
4.5%
4.1%
3.0%
3.0%
1.9%
1.9%
100.0%
Concord
Walnut Creek
Richmond
Martinez
Antioch
Pittsburg
El Cerrito
Brentwood
Pleasant Hill
San Pablo
Oakley
Pinole
Contra Costa
These are crude rates per 100,000 residents.
Contra Costa total includes cities not listed above.
212
Rate
9.4
15.3*
8.4
19.4*
NA
NA
NA
NA
NA
NA
NA
NA
8.7
INJURIES
More than one-third (39.0%) of all suicides were committed with a firearm. Poisoning (23.4%) and
hanging/suffocation (22.3%) were other common means of committing suicide.
Table 5 Suicide by cause
Contra Costa County, 2005–2007
Deaths
Firearm
Poisoning
Hanging/suffocation
Other
Jump
Total
Percent
105
63
60
25
10
269
39.0%
23.4%
22.3%
9.3%
3.7%
100.0%
Rate
3.4
2.0
1.9
0.8
NA
8.7
These are crude rates per 100,000 residents.
Total includes causes not listed above.
Non-Fatal Self-Inflicted Injury Hospitalizations
To understand the impact of self-inflicted injuries, it is important to assess hospitalizations in addition
to deaths. Information about suicide indicates the ultimate toll that self-injurious behaviors take on
people’s lives, but more people harm themselves than kill themselves. The most serious self-inflicted
injuries, including suicide attempts, may result in hospitalization. Other less-severe self-inflicted injuries
are treated in emergency departments, outpatient clinics or not at all.
Between 2005–2007, there were 995 hospitalizations due to non-fatal self-inflicted injuries among
Contra Costa residents. This means that on average, there were 332 hospitalizations in Contra Costa
due to self-inflicted injury each year. The crude hospitalization rate from self-inflicted injuries for
Contra Costa (32.2 per 100,000) was lower than the crude rate for California (43.8 per 100,000).
Table 6 Self-inflicted injury hospitalizations by race/ethnicity
Contra Costa County, 2005-2007
White
African American
Hispanic
Asian/Pacific Islander
Total
Cases
Percent
Rate
649
122
102
46
995
65.2%
12.3%
10.3%
4.6%
100.0%
40.1*
43.5*
15.5**
11.6**
32.2
These are crude rates per 100,000 residents.
Total includes racial/ethnic groups not listed above.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
213
Non-fatal selfinflicted injury is
most often the
result of a failed
suicide attempt.
In this section we
look at self-inflicted
injuries that led to
hospitalization.
INJURIES
In Contra Costa, the greatest number of self-inflicted injury hospitalizations was among whites (649),
followed by African Americans (122), Hispanics (102) and Asians/Pacific Islanders (46).
African Americans (43.5 per 100,000) and whites (40.1 per 100,000) had significantly higher rates of selfinflicted injury hospitalizations than the county overall (32.2 per 100,000). Hispanics (15.5 per 100,000) and
Asians/Pacific Islanders (11.6 per 100,000) had significantly lower rates of self-inflicted injury hospitalizations
compared to the county overall.
Females accounted for more than half (60.3%) of the county’s self-inflicted injury hospitalizations and
had a significantly higher self-inflicted injury hospitalization rate (38.1 per 100,000) than males (26.0
per 100,000).
Table 7 Non-fatal self-inflicted injury hospitalizations By Gender Contra Costa County, 2005–2007
Cases
Percent
Rate
Females
600
60.3%
38.1*
Males
395
39.7%
26.0
Total
995
100.0%
32.2
These are crude rates per 100,000 residents.
*Significantly higher rate than county males overall.
White females had a higher hospitalization rate for self-inflicted injury (49.3 per 100,000) compared
to county females overall (38.1 per 100,000). Hispanic (13.2 per 100,000) and Asian/Pacific Islander
females (16.0 per 100,000) had lower rates than county females overall.
African American males had a higher rate of self-inflicted hospitalization (44.0 per 100,000) than
county males overall (26.0 per 100,000). Hispanic males (17.7 per 100,000) had a lower rate than
county males overall.
Table 8 Non-fatal self-inflicted injury hospitalizations by age
Contra Costa County, 2005–2007
Cases
Percent
Rate
0–14 years
15–24 years
37
262
3.7%
26.3%
5.8**
64.1*
25–34 years
35–44 years
45–54 years
55–64 years
65 years and older
Total
160
189
197
83
67
995
16.1%
19.0%
19.8%
8.3%
6.7%
100.0%
41.1*
40.6*
41.5*
23.9**
18.1**
32.2
These are age-specific rates per 100,000 residents.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
214
INJURIES
Residents 15–24 years old accounted for more than one-quarter (26.3%) of all self-inflicted injury
hospitalizations and had the highest self-inflicted injury hospitalization rate (64.1 per 100,000); significantly higher than the rates for the county overall (32.2 per 100,000) and all other age groups. Residents
25–54 years also had significantly higher rates of self-inflicted injury hospitalizations than the county
overall. Residents 0–14 and 55 years and older had significantly lower rates than the county overall.
Table 9 Non-fatal self-inflicted injury hospitalizations by cause
Contra Costa County, 2005–2007
Cases
Poisoning
Cut/pierce
Other
Jump
Hanging/Suffocation
Firearm
Total
807
117
42
16
8
5
995
Percent
81.1%
11.8%
4.2%
1.6%
0.8%
0.5%
100.0%
Rate
26.1
3.8
1.4
NA
NA
NA
32.2
These are crude rates per 100,000 residents.
Total includes causes not listed above.
The majority (81.1%) of all self-inflicted injury hospitalizations involved poisonings, followed by
cutting/piercing (11.8%).
Three ZIP codes had significantly higher self-inflicted injury hospitalization rates than the county
overall: 94553, 94520 and 94509. These were located in East and Central counties. A stable rate could
not be calculated for ZIP codes with fewer than 20 cases. If denominator data was available, statistical
testing generated a confidence interval for these ZIP codes to determine whether the rate range was
lower, higher or similar to the county rate. Results from this test are reflected in the ZIP code table
and map. Four of these ZIP codes had a rate range significantly lower than the county rate: 94507,
94517, 94531 and 94595.
215
INJURIES
Table 10 Non-fatal self inflicted injury hospitalizations by ZIP code
Contra Costa County, 2005–2007
Cases
Percent
Rate
94506
94507
94509
94513
94514
94517
94518
94519
94520
94521
94523
94526
94530
94531
94547
94549
19
5
88
40
8
5
23
19
59
36
32
23
18
18
19
21
1.9%
0.5%
8.8%
4.0%
0.8%
0.5%
2.3%
1.9%
5.9%
3.6%
3.2%
2.3%
1.8%
1.8%
1.9%
2.1%
NA
NA**
44.6*
28.9
NA
NA**
27.1
32.2
51.4*
27.8
31.2
25.2
NA
NA**
NA
24.8
94553
94556
94561
94563
94564
94565
94572
94582
94583
94595
94596
94597
94598
94801
94803
94804
94805
94806
Total
79
13
38
11
11
88
12
13
48
6
30
21
29
26
20
44
16
44
995
7.9%
1.3%
3.8%
1.1%
1.1%
8.8%
1.2%
1.3%
4.8%
0.6%
3.0%
2.1%
2.9%
2.6%
2.0%
4.4%
1.6%
4.4%
100.0%
Total includes ZIP codes not listed above.
*Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
216
53.5*
NA
37.4
NA
NA
34.3
NA
NA
47.4
NA**
49.9
30.9
36.5
27.6
24.6
36.4
NA
24.2
32.2
INJURIES
217
INJURIES
What are suicides and self-inflicted injuries?
Suicide is a death resulting from the intentional use of force against oneself.1 There are many more suicide attempts than successful suicides. Self-inflicted injuries are often the result of a suicide attempt,
but not always. Other self-injurious behaviors such as cutting or burning oneself are also included in
self-inflicted injuries.
Why are they important?
Suicide was the 12th leading cause of death in the county overall and the third leading cause for county
residents age 15 to 34.
Considering only suicide deaths and hospitalized attempts would underestimate the problem. For each
suicide, there are an estimated 25 unsuccessful attempts. Among adults 15–24 years, there are estimated 100–200 attempts for every suicide completed.2 Unsuccessful suicide attempts and other selfinjurious behavior can lead to serious injuries, such as broken bones, brain damage or organ failure,
that require medical care.4,5
Suicide accounts for $25 billion each year in direct costs, including health care services, autopsies, investigations and funeral services, and indirect costs like productivity loss.3 The social costs, including
the life potential lost due to an early death, can burden schools, neighborhoods and communities.4
Who does it impact the most?
In the United States, much like in Contra Costa, men are more likely to die from suicide than females,
and account for a greater portion of suicides.5 County data show females are more likely to be hospitalized for self-inflicted injuries and U.S. females report failed suicide attempts during their lifetime
more often than males.1 Although suicide death rates are highest in U.S. adults 65 years and older,6 the
proportion of deaths attributable to suicide is larger in younger age groups.
The number of suicides committed by American Indian/Alaska Native residents of Contra Costa was
too small to calculate stable rates, but the national suicide rate for American Indian/Alaska Native
residents 15–34 years (19.7 per 100,000) was higher than the national average for that age group (11.1
per 100,000).5 In Contra Costa, whites were more likely to commit suicide and be hospitalized for selfinflicted injuries than county residents overall.
Risk factors for committing or attempting suicide include a previous suicide attempt, history of mental
disorders—particularly depression, history of alcohol and substance abuse, family history of suicide or
violence, feelings of hopelessness, isolation and loss, impulsive or aggressive tendencies, physical illness, and barriers to mental health treatment.4
What can we do about it?
Strengthening an individual’s bond to their families, friends and peers, and to community organizations such as schools, universities, places of employment, community centers, and churches or other
religious or spiritual organizations may have the potential to decrease risk for suicidal behavior. Bonds
formed by adolescents to their schools, for example, have been shown to protect teens against suicidal
218
INJURIES
thoughts and behaviors in several national studies.6
Also, close family members, friends and teachers may be able to pick up on warning signs such as
changes in mood, diet or sleeping pattern of someone who may be already contemplating suicide.4 A
strong public information campaign and readily available counseling may enable people to recognize
warning signs and seek help.
Victims of interpersonal violence (e.g., child abuse, youth violence, community violence, sexual assault,
and domestic violence) have a higher risk of suicide than nonvictims. Preventing these “profound life
stresses” may prevent subsequent suicidal behaviors and additional instances of interpersonal violence. 7
Environmental risk factors for attempting suicide can also be addressed by limiting the availability of
prescription and illegal drugs, firearms, and alcohol to underage youths.
Data Sources: Suicide and Non-Fatal Self-Inflicted Injury
tables and map
Tables 1-10: Any analyses or interpretations of the data were reached by the Community Health Assessment, Planning
and Evaluation (CHAPE) Unit of Contra Costa Health Services and not the California Department of Public Health
(CDPH) or California Office of Statewide Health Planning and Development (OSHPD). Data presented for Hispanics
include Hispanic residents of any race. Data presented for whites, Asians/Pacific Islanders and African Americans include
non-Hispanic residents. Not all race/ethnicities are shown but all are included in totals for the county and for each gender,
age, cause and city. Counts fewer than five are not shown in order to protect anonymity. Rates were not calculated for any
group with fewer than 20 cases due to unstable estimates.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005-2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: U.S. Census 2000, Neilsen Claritas 2009, Association of Bay Area Governments (ABAG) 2009
Projections, and California Department of Finance Population Estimates for Cities, Counties and the State 2001-2009,
with 2000 Benchmark.
California population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
Tables 1-5: These tables include total deaths due to suicide and crude or age-specific average annual death rates per
100,000 residents for 2005 through 2007. Suicide mortality data from the California Department of Public Health
(CDPH), http://www.cdph.ca.gov/, Center for Health Statistics’ Death Statistical Master File, 2005-2007.
ICD10 coding for suicide (ICD X60-X84) found at the CDHS Brand EPICenter California Injury Data Online at
http://www.applications.dhs.ca.gov/epicdata/default.htm, modified from the Centers of Disease Control and Prevention
National Center for Health Statistics available online at http://www.cdc.gov/nchs/about/otheract/ice/matrix10.htm.
Poisonings includes drug overdose. Late effects are not included. Table 5’s ICD10 coding for “other” may include suicides
due to the following causes; drowning, explosives, fire, hot vapors or objects, blunt object, motor vehicle involvement and
other specified and unspecified means.
219
INJURIES
Tables 6-10: These tables include total hospitalizations due to self-inflicted injury and crude or age-specific average annual
hospitalization rates per 100,000 residents for 2005 through 2007. Non-fatal self-inflicted hospitalization data from the
California Office of Statewide Health Planning and Development (OSHPD) Patient Discharge Data files 2005-2007, http://
www.oshpd.ca.gov/, Healthcare Quality and Analysis Division, Health Care Information Resource Center.
ICD9 E-coding for non-fatal self-inflicted injury found at the CDHS Brand EPICenter California Injury Data Online at
http://www.applications.dhs.ca.gov/epicdata/default.htm, modified from the Centers of Disease Control and Prevention
National Center for Health Statistics available online at http://www.cdc.gov/nchs/about/otheract/ice/matrix10.htm.
OSHPD data includes only those hospitalizations for which assault was listed as the primary diagnoses (ICD E950-958.9).
They do not include treatment that takes place in a doctor’s office, health clinic or emergency room. A single resident can
be counted multiple times for multiple times for multiple self-inflicted injury hospitalizations. Table 9’s “other” category
includes non-fatal self-inflicted injuries from the following causes: burns, fire, scalding, motor vehicle crash and other
specified and unspecified means.
Table 10:
The rates for several ZIP codes are marked “NA” in the table. This is because the ZIP code has fewer than 20 cases
ZIP codes with fewer than five cases and those that are shared with another county are not shown in the table.
Non-fatal Self-inflicted Injury Hospitalization map:
The shading for some ZIP codes indicates that the rate is not available. This is due to the following reasons:
• A denominator for the ZIP code is not available: 94505
• The ZIP code extends to areas outside of Contra Costa county: 94551, 94707, 94708
Although rates were not calculated for ZIP codes with fewer than 20 cases, statistical testing generated a confidence
interval for these ZIP codes to determine whether the rate range was similar to the county rate and it was shaded
appropriately on the map.
ZIP codes that are assigned to P.O. boxes only could not be shown on the map.
ZIP code population estimates for ZIP code level hospitalization rates provided by the Environmental Health
Investigations Branch from the Environmental Systems Research Institute (ESRI) Community Sourcebook of ZIP Code
Demographics. Data was not available for all ZIP codes.
Healthy People 2010 objectives from the U.S. Department of Health and Human Services’ Office of Disease Prevention
and Health Promotion, available online at http://www.healthypeople.gov/.
text
1.
2.
3.
4.
5.
Karch D, Dahlberg L, Patel N, (2010). Surveillance for Violent Deaths–National Violent Death Reporting System, 16
states, 2006. MMWR; 59(ss04); 1-50.
Goldsmith SK, Pellmar TC, Kleinman AM, Bunney WE, editors. Reducing suicide: a national imperative.
Washington (DC): National Academy Press 2002.
Centers for Disease Control and Prevention (CDC) National Center for Injury Prevention and Control. “Preventing
Suicide Program Activities Guide”. Available at: http://www.cdc.gov/violenceprevention/pub/PreventingSuicide.html
National Center for Injury Prevention and Control, Center Disease Control and Prevention, (2006). Suicide: Fact
Sheet. Retrieved February 12, 2007 from the CDC website: www.cdc.gov/ncipc/factsheets/suifacts.htm
Centers for Disease Control and Prevention (CDC). Web-based Injury Statistics Query and Reporting System
(WISQARS) [Online]. (2007). National Center for Injury Prevention and Control, CDC (producer). Available from
URL:
www.cdc.gov/injury/wisqars/index.html
220
INJURIES
6.
Centers for Disease Control and Prevention. (2008). Strategic Direction for the Prevention of Suicidal Behavior:
Promoting Individual, Family, and Community Connectedness to Prevent Suicidal Behavior. Retrieved April 2, 2010
from the CDC website at: http://www.cdc.gov/violenceprevention/pdf/Suicide_Strategic_Direction_Full_Version-a.
pdf
221
INJURIES
Domestic Violence
Domestic violence is an important
public health issue.
• A higher percentage of women reported intimate partner violence compared to men.
• Antioch, Concord, Martinez, Pittsburg, Richmond and San Pablo had higher rates of
domestic violence calls compared to the county overall.
• Antioch, Concord, Martinez, Oakley and the unincorporated areas of the county had
higher rates of domestic violence arrests than the county overall.
Domestic violence, or intimate partner violence (IPV), describes physical, sexual or psychological
harm that occurs between two people in a close relationship. This includes but is not limited to physical violence, sexual violence, threats and emotional abuse. This section presents information on three
indicators of domestic violence: experience with intimate partner violence, domestic violence calls
and domestic violence arrests. These indicators move from the broad to more specific dimensions of
this issue.
Domestic violence is underreported in every community. The indicators included below come from
anonymous telephone surveys, calls to a community-based domestic violence service provider, police
reports and arrests. They do not provide a complete picture of domestic violence in Contra Costa.
Each of these indicators reflects different community norms in understanding domestic violence,
willingness to report it and the response of the authorities. As community norms change and domestic
violence is more effectively addressed, some of these indicators—reports of violence and arrests—may
paradoxically increase before eventually declining over time.
According to 2007 estimates from the California Health Interview Survey, 103,000 Contra Costa adults
between the ages of 18 and 65 have ever experienced physical or sexual violence by an intimate partner.
The prevalence of IPV in Contra Costa County (15.4%) was similar to the prevalence for the greater
Bay Area (17.0%) and California overall (17.2%). It is estimated that 790,000 people in the greater Bay
Area have experienced IPV since age 18.
Table 1 Experienced intimate partner violence since age 18
Adults 18–65 Years, 2007
Cases
California
Greater Bay Area
Contra Costa
3,993,000
790,000
103,000
These estimates are not age-adjusted.
222
Prevalence
17.2%
17.0%
15.4%
INJURIES
Women experienced more than two-thirds (68.5%) of all the IPV cases in the greater Bay Area and
reported a significantly higher prevalence (23.2%) of intimate partner violence compared to men (10.8%).
Table 2 Experienced intimate partner violence since age 18
Greater Bay Area Adults 18–65 Years, 2007
Cases
Women
Men
Total
Percent
541,000
249,000
790,000
68.5%
31.5%
100.0%
Prevalence
23.2%*
10.8%
17.0%
These estimates are not age-adjusted.
* Statistically higher rates compared to men.
Editor’s note: Analyses of Contra Costa intimate partner violence by gender, age
or race/ethnicity were not possible due to small sample size, but we can look at
the Greater Bay Area overall for an indication of the prevalence of intimate partner
violence in these subgroups.
Young adults (aged 18–24) reported a lower prevalence of intimate partner violence (10.0%) than
the greater Bay Area overall (17.0%). It is important to note that this may be the result of the survey
question, which asks about experience after age 18.
Table 3 Experienced intimate partner violence since age 18
Greater Bay Area Adults 18–65 Years, 2007
Cases
18–24 years
25–39 years
40–65 years
Total
Percent
62,000
247,000
481,00
790,000
7.8%
31.2%
60.9%
100.0%
Prevalence
10.0%**
16.2%
19.3%
17.0%
These estimates are not age-adjusted.
** Significantly lower rate compared to the greater Bay Area overall.
The highest number of IPV cases was reported by whites (469,000) followed by Latinos (110,000),
Asians/Pacific Islanders (96,000), African Americans (71,000), people of two or more races (33,000)
and American Indian/Alaska Native (12,000). Whites (20.6%) and American Indian/Alaska Natives
(52.3%) had significantly higher prevalence of intimate partner violence compared to the greater Bay
Area overall (17.0%). Latinos (11.6%) and Asians/Pacific Islanders (9.6%) reported significantly lower
prevalence than the greater Bay Area overall.
223
INJURIES
Table 4 Experienced intimate partner violence since age 18
Greater Bay Area Adults 18–65 Years, 2007
Cases
Percent
Prevalence
White
Latino
Asian/Pacific Islander
469,000
110,000
96,000
59.4%
13.9%
12.2%
20.6%*
11.6%**
9.6%**
African American
American Indian/Alaska Native
Total
71,000
12,000
790,000
9.0%
1.5%
100.0%
23.0%
52.3%*
17.0%
These estimates are not age-adjusted.
* Significantly higher rate compared to the greater Bay Area overall.
** Significantly lower rate compared to the greater Bay Area overall.
Another measure of domestic violence in Contra Costa County is the number of calls for domestic
violence that come into STAND! For Families Free of Violence, a community-based organization that
works with residents affected by domestic violence. Calls to STAND! demonstrate the distribution of
calls in cities across the county.
Between 2006 and 2008, there were 17,797 calls from the county’s 19 major cities and its unincorporated
areas. Residents of Antioch, Concord and Richmond each made more than 500 calls per year. These
three cities also had significantly higher rates of domestic violence calls than the county overall, as did
Pittsburg (9.2 per 1,000), Martinez (8.8 per 1,000) and San Pablo (8.6 per 1,000).
Antioch had the highest rate (10.3 per 1,000), significantly higher than the county overall (5.7 per
1,000) and all other cities. Several cities had significantly lower rates than the county: Brentwood (4.8
per 1,000), Pleasant Hill (4.6 per 1,000), Walnut Creek (4.6 per 1,000), Oakley (4.1 per 1,000), Hercules
(3.0 per 1,000), El Cerrito (2.5 per 1,000), Lafayette (2.3 per 1,000), Clayton (1.5 per 1,000), Danville
(1.0 per 1,000), San Ramon (1.0 per 1,000) and Orinda (0.6 per 1,000). The unincorporated areas of
the county also had a significantly lower rate of calls (3.1 per 1,000).
224
INJURIES
Table 5 Domestic violence calls to STAND! by selected
communities
Contra Costa County, 2006–2008
Number
Antioch
Concord
Richmond
Pittsburg
Unincorporated
Martinez
Walnut Creek
San Pablo
Brentwood
Pleasant Hill
Oakley
Pinole
Hercules
San Ramon
El Cerrito
Lafayette
Danville
Clayton
Orinda
Moraga
Contra Costa
3,098
3,083
2,763
1,754
1,547
956
910
803
725
463
411
312
220
183
177
162
133
49
31
17
17,797
Percent
17.4%
17.3%
15.5%
9.9%
8.7%
5.4%
5.1%
4.5%
4.1%
2.6%
2.3%
1.8%
1.2%
1.0%
1.0%
0.9%
0.7%
0.3%
0.2%
0.1%
100.0%
Rate
10.3*
8.3*
8.9*
9.2*
3.1**
8.8*
4.6**
8.6*
4.8**
4.6**
4.1**
5.4
3.0**
1.0**
2.5**
2.3**
1.0**
1.5**
0.6**
NA
5.7
These are rates per 1,000 population.
* Significantly higher rate when compared to the county overall.
** Significantly lower rate when compared to the county overall.
An indicator that points out the severity of domestic violence is the number of domestic violence calls
for assistance involving weapons. Between 2006 and 2008, there were 2,535 of these calls in Contra
Costa County. Residents of Concord, Richmond, Antioch and the unincorporated areas of the county
averaged more than 100 domestic violence calls that involved weapons each year. Pinole (2.8 per 1,000),
Hercules (2.0 per 1,000), Concord (1.6 per 1,000), Richmond (1.1 per 1,000), Antioch (1.1 per 1,000)
and Pleasant Hill (1.1 per 1,000) all had rates significantly higher than the county overall (0.8 per 1,000).
San Ramon (0.2 per 1,000), Brentwood (0.3 per 1,000), Danville (0.3 per 1,000), the unincorporated
areas of the county (0.7 per 1,000), Martinez (0.6 per 1,000) and Pittsburg (0.4 per 1,000) all had rates
significantly lower than the county overall.
225
INJURIES
Table 6 Domestic violence related calls to law enforcement
involving weapons by selected communities
Contra Costa County, 2006-2008
Number
Concord
Richmond
Unincorporated
Antioch
Pinole
Hercules
Pleasant Hill
Oakley
Martinez
Pittsburg
San Pablo
El Cerrito
Brentwood
San Ramon
Danville
Moraga
Walnut Creek
Clayton
Lafayette
Orinda
Contra Costa
607
339
337
323
160
147
105
82
67
67
61
52
41
40
33
18
18
17
12
9
2,535
Percent
23.9%
13.4%
13.3%
12.7%
6.3%
5.8%
4.1%
3.2%
2.6%
2.6%
2.4%
2.1%
1.6%
1.6%
1.3%
0.7%
0.7%
0.7%
0.5%
0.4%
100.0%
Rate
1.6*
1.1*
0.7**
1.1*
2.8*
2.0*
1.1*
0.8
0.6**
0.4**
0.7
0.7
0.3**
0.2**
0.3**
NA
NA
NA
NA
NA
0.8
These are rates per 1,000 population.
* Significantly higher rate when compared to the county overall.
** Significantly lower rate when compared to the county overall.
The number of arrests for domestic violence can also be an indicator of the distribution of domestic
violence. Between 2005-2006, there were 6,826 arrests for domestic violence in Contra Costa County.
These arrests were made across the county, but Concord (1,893) had the highest number of arrests,
followed by Antioch (1,476) and the unincorporated areas as a whole (1,242). Almost half of all domestic
violence arrests (49.3%) occurred in Antioch and Concord.
Antioch (7.4 per 1,000), Concord (7.7 per 1,000), Martinez (7.4 per 1,000), Oakley (4.7 per 1,000)
and the unincorporated areas of the county (3.8 per 1,000) had significantly higher rates of domestic
violence arrests than the county overall (3.3 per 1,000). Several cities had significantly lower rates:
Pittsburg (2.4 per 1,000), Orinda (2.3 per 1,000) Danville (2.2 per 1,000), Brentwood (2.2 per 1,000),
San Ramon (1.9 per 1,000), Pleasant Hill (1.7 per 1,000), Lafayette (1.6 per 1,000) and Walnut Creek
(0.9 per 1,000). The aggregate domestic violence arrest rate for Richmond, El Cerrito, Hercules, Pinole
and San Pablo combined (0.2 per 1,000) was also significantly lower than the county overall.
226
INJURIES
Table 7 Domestic violence arrests by selected communities
Contra Costa County, 2005-2006
Concord
Antioch
Unincorporated
Martinez
Pittsburg
Oakley
San Ramon
Brentwood
Danville
Walnut Creek
Pleasant Hill
Orinda
Lafayette
Richmond +
Moraga
Contra Costa
Number
Percent
1,893
1,476
1,242
535
298
289
224
206
189
123
111
82
75
74
9
6,826
27.7%
21.6%
18.2%
7.8%
4.4%
4.2%
3.3%
3.0%
2.8%
1.8%
1.6%
1.2%
1.1%
1.1%
0.1%
99.9%
Rate
7.7*
7.4*
3.8*
7.4*
2.4**
4.7*
1.9**
2.2**
2.2**
0.9**
1.7**
2.3**
1.6**
0.2**
NA
3.3
These are rates per 1,000 population.
These estimates are not age-adjusted.
* Significantly higher rate when compared to the county overall.
** Significantly lower rate when compared to the county overall.
(+) Richmond statistics includes data for El Cerrito, Hercules, Pinole and San Pablo.
What is domestic violence?
Domestic violence (sometimes called “intimate partner violence” or IPV) is a serious, preventable public
health problem that affects millions of Americans. Domestic violence occurs between two people in a
close relationship. This includes current and former spouses and dating partners. This type of violence
can occur among heterosexual or same-sex couples and does not require sexual intimacy.1 Domestic
violence can vary in frequency and severity. It occurs on a continuum, ranging from one punch or hit
to chronic, severe battering. Domestic violence includes four types of behavior:
• Physical violence is when a person hurts or tries to hurt a partner by hitting, kicking, strangling
or other type of physical force.
• Sexual violence is forcing a partner to take part in a sex act when the partner does not consent.
• Threats of physical or sexual violence include the use of words, gestures, weapons or other means
to communicate the intent to cause harm.
• Emotional abuse is threatening a partner or his or her possessions or loved ones, or harming a
partner’s sense of self-worth. Examples are stalking, name-calling, intimidation, or not letting a
partner see friends and family. Often, domestic violence starts with emotional abuse. This behavior
can progress to physical or sexual assault. Several types of domestic violence may occur together.1
227
INJURIES
Why is domestic violence important?
Domestic violence can affect health in many ways. The longer the violence goes on, the more serious
the effects. Many victims suffer physical injuries. Some are minor, like cuts and bruises. Others are
more serious and can cause lasting disabilities or death. These include broken bones, internal bleeding and head trauma.2
Not all injuries are physical. Domestic violence can also cause emotional harm. The anger and stress
that victims feel may lead to eating disorders, depression and loss of self-esteem. Some victims even
think about or commit suicide. Witnessing domestic violence, usually involving caretakers, can have a
dramatic negative effect on children, impacting health throughout the child’s life course and into the
next generation.
Domestic violence is linked to harmful health behaviors as well. Victims are more likely to smoke, abuse
alcohol, use drugs and engage in risky sexual activity.2
Who is at the greatest risk for domestic violence?
Some risk factors for domestic violence victimization and perpetration are the same.3
A combination of individual, relational, community and societal factors contribute to the risk of becoming a victim or perpetrator of domestic violence. Understanding these risk factors can help identify
various opportunities for prevention.
Individual Risk Factors
•
•
•
•
•
•
•
•
Low self-esteem
Emotional dependence and insecurity
Low academic achievement
Young age
Heavy alcohol and drug use
Depression
Anger and hostility
Prior history of being physically abusive
Relationship Factors
•
•
•
•
•
Marital conflict (e.g., fights, tension and other struggles)
Marital instability, divorces or separations
Dominance and control of the relationship by one partner over the other
Economic stress
Unhealthy family relationships and interactions
228
INJURIES
Community Factors
• Poverty and associated factors (e.g., unemployment, overcrowding)
• Lack of strong institutions, relationships and norms that shape a community's social interactions
• Weak community sanctions against domestic violence (e.g., unwillingness of neighbors to intervene
in situations where they witness violence)
• Traditional gender norms (e.g., women should stay at home, not enter work force and be submissive;
men support the family and make the decisions)3
What can we do about domestic violence?
Early identification of domestic or intimate partner violence (IPV) is key to early and effective intervention. Identification requires community awareness, an understanding that IPV is not a norm and is not
acceptable. Just as sexual harassment or date rape existed for years without identification, recognition,
or appropriate response until these behaviors were given language and named, organizations, systems
and communities must learn to identify IPV and call it by name. Only then can we learn its prevalence,
confront its perpetrators, support its victims, and intervene in the cycle of violence that impacts adults
and children. The data reported above is incomplete largely because of the failure of all our agencies
and communities to fully identify, name, respond to and report episodes of IPV.
Community organizations, churches, agencies and civic groups need to own the issue of IPV, and see
it as part of their core mission. At a minimum, agencies and their staff can develop competence in
three areas:
• Understanding the concept of IPV and its importance to their core mission
• Identifying clients involved with IPV
• Counseling IPV victims in basic, immediate safety planning.
Health care systems are some of the most important institutions that should own the issue of IPV as
core to their mission, as IPV has a devastating impact on the health of individuals, families and children.
Health care staff need to be trained to identify IPV. Basic questions about IPV should be asked in every
time a patient interacts with the health care system. Health care staff especially should be trained in
the three competencies described above.
As identification, naming and reporting of IPV improves, we will see an initial increase in IPV rates.
However, early identification, coupled with community and institutional resources for intervention,
should lead to a decrease in homicide, suicide and serious injury associated with IPV. We can measure
our initial success in addressing this issue by the increase in reporting and the decrease in morbidity
from IPV. Later progress will show as a decrease in real rates of IPV, and a wider community norm of
naming and condemning IPV.
229
INJURIES
Data Sources: Domestic Violence
tables
Tables 1–4: Local data about intimate partner violence comes from the California Health Interview Survey’s AskCHIS
data query system, copyright© 2007 the Regents of the University of California, all rights reserved, available online at:
http://askchis.com/main/default.asp Respondents (adults aged 18–65) were asked: "Since you turned 18, has a current or
past intimate partner ever hit, slapped, pushed, kicked or physically hurt you in any way?" and "Since you turned 18, has a
current or past intimate partner ever forced you into unwanted sexual intercourse, oral or anal sex, or sex with an object
by using force or threatening to harm you?" Data analysis performed in May 2010. AskCHIS data are generated from a
telephone survey that asks questions to a randomly selected group of residents in Contra Costa and other counties in
California. Responses are then weighted to represent the county, region and state as whole. The Greater Bay Area includes
the counties of Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano and Sonoma.
Tables 5-7: Data from Zero Tolerance report for Contra Costa County, 2009. Population denominators were included in
these reports and were based on California Department of Finance estimates. Any analyses, interpretations or conclusions
of the data have been reached by Community Health Assessment, Planning and Evaluation (CHAPE).
Rates were not calculated for any group with fewer than 20 cases due to unstable estimates.
text
1.
2.
3.
National Center for Injury Prevention and Control, Centers for Disease Control. (2008) Intimate Partner Violence:
Definitions. Retrieved July 10, 2010 at the CDC website:
http://cdc.gov/ViolencePrevention/intimatepartnerviolence/definitions.html
National Center for Injury Prevention and Control, Centers for Disease Control. (2009). Understanding Intimate
Partner Violence: Fact Sheet. Retrieved July 9, 2010 at the CDC website:
http://www.cdc.gov/violenceprevention/pdf/IPV_factsheet-a.pdf
National Center for Injury Prevention and Control, Centers for Disease Control. (2009) Intimate Partner Violence:
Risk Factors and Protective Factors. Retrieved July 10, 2010 at the CDC website:
http://cdc.gov/ViolencePrevention/intimatepartnerviolence/riskprotectivefactors.html
230
MENTAL HEALTH & SUBSTANCE ABUSE
Mental Health
Whites were more likely to report taking prescription medicines
for emotional/mental health issues than the county as a whole.
There are many possible indicators for mental health and mental illness. For this report two recent
indicators of mental health were selected: 1) adults likely to have had psychological distress in the past
year, 2) adults taking prescription medication for emotional or mental health issues.
Psychological Distress
In 2007 the prevalence of psychological distress in the past year among adults 18 years of age and older
was similar in the greater Bay Area (7.3%) and California (8.5%).
Editor’s note: In order to obtain stable estimates, greater Bay Area rather than
county-level data on psychological distress was included in these analyses. “Cases”
represent an estimate of the number people with psychological distress based on
a sample of respondents who answered “yes” to questions in the California Health
Interview Survey regarding this issue. This data does not identify all residents
who have emotional and mental health problems or who actually need or receive
services due to such problems.
Table 1 Likely has had psychological distress in past year
Adults 18 years and older, 2007
Cases
California
Greater Bay Area
2,287,000
393,000
Prevalence
8.5%
7.3%
These estimates are not age-adjusted.
In the greater Bay Area, the number of women who were likely to have had psychological distress
(217,000) was greater than the number of men (175,000). A similar percentage of women (8.0%) and
men (6.6%) were likely to have suffered from psychological distress.
Table 2 Likely has had psychological distress in past year
Greater Bay Area adults 18 years and older, 2007
Cases
Women
Men
Total
217,000
175,000
393,000
These estimates are not age-adjusted.
231
Percent
55.2%
44.5%
100.0%
Prevalence
8.0%
6.6%
7.3%
MENTAL HEALTH & SUBSTANCE ABUSE
Adults 65–79 had the lowest prevalence (2.2%) of reported psychological distress; significantly lower
than the greater Bay Area (7.3%) and all other age groups. (Note: Data for residents ages 80 and older
were unavailable due to unstable rates.)
Table 3 Likely has had psychological distress in past year
Greater Bay Area adults 18 years and older, 2007
Cases
Percent
18–24 years
25–39 years
76,000
131,000
19.3%
33.3%
40–64 years
65–79 years
Total
168,000
13,000
393,000
42.7%
3.3%
100.0%
Prevalence
12.3%
8.6%
6.9%
2.2%**
7.3%
These estimates are not age-adjusted.
** Significantly lower than the greater Bay Area overall.
Total includes age groups not shown.
The highest number of residents who were likely to have had psychological distress were whites
(183,000), followed by Asians/Pacific Islanders (79,000) and Latinos (78,000). (Note: Data for African
Americans and American Indians/Alaska Natives were unavailable due to unstable rates.)
Table 4 Likely has had psychological distress in past year
Greater Bay Area adults 18 years and older, 2007
Cases
White
Asian/Pacific Islander
Latino
Total
183,000
79,000
78,000
393,000
Percent
46.6%
20.1%
19.8%
100.0%
Prevalence
6.7%
6.7%
7.6%
7.3%
These estimates are not age-adjusted.
Total includes racial/ethnic groups not shown.
Taking Prescription Medicine for Emotional/Mental Health
In 2007, some 76,000 Contra Costa adults 18 years and older reported they had taken prescription
medicines for emotional/mental health issues for at least two weeks in the past year. The prevalence
of prescription medication use for emotional/mental health in Contra Costa (9.8%) was similar to
California (10.0%) and the greater Bay Area (10.4%).
232
MENTAL HEALTH & SUBSTANCE ABUSE
Table 5 Taken prescription medicine for emotional/mental
health issue for at least two weeks in past year
Adults 18 and older, 2007
California
Greater Bay Area
Contra Costa
Cases
Prevalence
2,676,000
557,000
76,000
10.0%
10.4%
9.8%
These estimates are not age-adjusted.
Editor’s note: In order to obtain stable estimates, we look to greater Bay Area data
for further analysis of prescription medication use for emotional/mental health by
gender, age and race/ethnicity.
In the greater Bay Area, 557,000 people reported they had taken prescription medicine for an emotional/
mental health issue for at least two weeks in the past year.
More women (349,000) reported taking prescription medicine for emotional/mental health issues
than men (208,000). Women were more likely (12.8%) than men (7.8%) to have taken prescription
medicines for these purposes.
Table 6 Taken prescription medicine for emotional/mental
health issue for at least two weeks in past year
Greater Bay Area adults 18 and older, 2007
Women
Men
Total
Cases
Percent
Prevalence
349,000
208,000
557,000
62.7%
37.3%
100.0%
12.8%*
7.8%
10.4%
These estimates are not age-adjusted.
* Significantly higher rate than men.
There were no significant differences in the age groups with respect to the prevalence of taking these
prescription medicines.
233
MENTAL HEALTH & SUBSTANCE ABUSE
Table 7 Taken prescription medicine for emotional/mental health issue
for at least two weeks in past year
Greater Bay Area adults 18 and older, 2007
Cases
Percent Prevalence
18–24 years
25–39 years
41,000
129,000
7.4%
23.2%
6.6%
8.4%
40–64 years
65–79 years
80 years and older
Total
320,000
53,000
15,000
557,000
57.5%
9.5%
2.7%
100.0%
13.1%
9.0%
7.1%
10.4%
These estimates are not age-adjusted.
More whites (364,000) reported taking prescription medicines for emotional/mental health issues for
at least two weeks in the past year than Latinos (74,000) and Asians/Pacific Islanders (65,000). (Note:
Data for African Americans and American Indians/Alaska Natives were unavailable due to unstable rates.)
Whites reported a significantly higher prevalence (13.4%) of taking prescription medicines for emotional/
mental health issues than the greater Bay Area as a whole (10.4%). Asians/Pacific Islanders (5.5%) had
a significantly lower prevalence compared to the greater Bay Area overall.
Table 8 Taken prescription medicine for emotional/mental health
issue for at least two weeks in past year
Greater Bay Area adults 18 and older, 2007
White
Latino
Asian/Pacific Islander
Total
Cases
Percent
Prevalence
364,000
74,000
65,000
557,000
65.4%
13.3%
11.7%
100.0%
13.4%*
7.3%
5.5%**
10.4%
These estimates are not age-adjusted. Total includes racial/ethnic groups not shown.
* Significantly higher than the greater Bay Area overall.
** Significantly lower than the greater Bay Area overall.
234
MENTAL HEALTH & SUBSTANCE ABUSE
What are mental health disorders?
Mental health is defined as "a state of well-being in which the individual realizes his or her own
abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able
to make a contribution to his or her community." Cultural differences, subjective assessments and
competing professional theories all affect how "mental health" is defined.1
Mental illness is the term that refers collectively to all diagnosable mental disorders.
Mental disorders are health conditions characterized by alterations in thinking, mood or behavior
(or some combination thereof) associated with distress or impaired functioning. Alzheimer’s disease
is an example of a mental disorder largely marked by alterations in thinking (especially forgetting).
These alterations in thinking, mood or behavior contribute to a host of problems—patient distress,
impaired functioning, heightened risk of death, pain, disability or loss of freedom.2
Why are they important?
Mental health is critical for personal well-being at every stage of life. Mental disorders are real, disabling health conditions that have an immense impact on individuals and families. Mental disorders
vary widely in type and severity. About one in four U.S. adults suffer from a diagnosable mental
disorder in a given year. Depression is the leading cause of disability in the United States for individuals ages 15–44.3
Two-thirds of people with diagnosable mental disorders do not seek treatment. Many people suffer
from more than one mental disorder at a given time—nearly half (45%) of those with any mental
disorder meet the criteria for two or more disorders.4
Nationally in 2004, adults surveyed as part of the Centers for Disease Control and Prevention’s Behavioral Risk Factor Surveillance System reported experiencing an average of 3.5 days of poor mental health in the past 30 days. Ten-percent of adults reported 14 or more mentally unhealthy days.5
Who is impacted most?
Mental disorders occur in all racial, ethnic and socioeconomic groups. Although the specific causes
of most mental disorders are not known, many risk factors have been identified or suggested. These
include biological factors (e.g., brain trauma), psychological factors (e.g., stressful events), and sociocultural factors (e.g., poverty). Genetics and a family history of mental and addictive disorders
also can increase risk.3
Scientists believe that many mental disorders result from the complex interplay of multiple genes with
diverse environmental factors. Family studies, often with identical twins who share the same genes,
have provided evidence of genetic contributions to depression, bipolar disorder, schizophrenia, autism and other mental disorders. Even for those with genetic risk, however, environmental factors can
play a significant role in whether or not a person develops a disorder, or the severity of an illness.3
235
MENTAL HEALTH & SUBSTANCE ABUSE
What can we do about it?
Community-wide strategies can be effective in preventing and reducing severity of some mental health
conditions, such as depression and post-traumatic stress disorder. Also, prevention strategies can delay
onset and support treatment outcomes for those with mental health conditions.
Effective community strategies to prevent mental illness include:6
Build the resilience of local communities: Stress is an inevitable part of life that everyone — adults,
teens and children — experiences at times. Healthy and resilient communities provide people with physical safety and strong supportive social networks.
Build the research base: Neuroscience and genetics present important research opportunities. Research that explores approaches for reducing risk factors and strengthening protective factors for the
prevention of mental illness should be encouraged.
Overcome stigma: Powerful and pervasive, stigma prevents people from acknowledging their own mental health problems and ever disclosing them to others. We can help reduce stigma by dispelling myths
about mental illness, and by encouraging individuals experiencing mental health problems to seek help.6
Improve public awareness of effective treatment: Americans are often unaware of the choices
they have for effective mental health treatments. Treatments fall mainly under several broad categories — counseling, psychotherapy, medication therapy, rehabilitation. All human services professionals,
not just health professionals, have an obligation to be better informed about mental health treatment
resources in their communities and should encourage individuals to seek help.
Ensure the supply of mental health services and providers: Efforts should be made to expand
mental health services, which now exist in short supply. For adults and children with less-severe conditions, primary health care, the schools and other human services must be prepared to assess and,
at times, to treat individuals who come seeking help.
Ensure delivery of state-of-the-art treatments: A wide variety of effective, community-based services
exist for even the most-severe mental illnesses, yet often these best practices are not being translated
into community settings. To be effective, the diagnosis and treatment of mental illness must be culturally competent and tailored to all characteristics that shape a person’s image and identity.
Facilitate entry into treatment: Public and private agencies have an obligation to facilitate entry into
mental health care and treatment through the multiple “portals of entry” that exist: primary health
care, schools and the child welfare system.
Reduce financial barriers to treatment: Concerns about the cost of care and the disparity in insurance coverage (for mental disorders in contrast to other illnesses) are among the most common reasons why people do not seek needed mental health care.
236
MENTAL HEALTH & SUBSTANCE ABUSE
The Mental Health Division of Contra Costa Health Services currently serves approximately 18,000 individuals, roughly 7,000 children and 11,000 adults annually. The Mental Health Division is the publicly
funded safety net for the county with a mission to provide services to low-income individuals with
severe mental illness who are either on Medi-Cal or uninsured. [The estimated prevalence of severe
mental illness among people living in households with an income below 200% of the federal poverty
level is 8.9%.7] The Mental Health Division’s services are provided through a system of care that includes
Mental Health staff, community-based organizations and a network of private therapists.
The
•
•
•
•
Mental Health Division serves:
Adults who have serious mental disabilities
Children and adolescents who are seriously and emotionally disturbed
Anyone in acute psychiatric crisis
Anyone who lives in the county who has Medi-Cal or no insurance and asks for services
Data Sources: Mental Health
tables
All data for the Mental Health section are from the California Health Interview Survey’s AskCHIS data query system,
copyright © 2007 the Regents of the University of California, all rights reserved, available online at: http://www.chis.ucla.
edu/. Data analysis performed in June 2010. AskCHIS data are generated from a telephone survey that asks questions to
a randomly selected group of residents in Contra Costa and other counties in California. Responses are then weighted to
represent the county, region and state as whole. Total numbers are estimates calculated by CHIS using rates so some totals
may not exactly match the sum of subgroups.
Percent is the number of likely psychological distress cases for a group divided by the total number of likely psychological
distress cases multiplied by 100. The prevalence is the number of likely psychological distress cases for a group divided by
the number of residents within each group multiplied by 100.
Data presented for Latinos include Latino residents of any race. Data presented for Whites, Asians/Pacific Islanders and
African Americans include non-Latino residents. Not all race/ethnicities shown but all are included in totals for Contra
Costa, greater Bay Area and California. The greater Bay Area includes the counties of Santa Clara, Alameda, Contra Costa,
San Francisco, San Mateo, Sonoma, Solano, Marin and Napa.
Tables 1-4: The variable used for these tables is a dichotomous measure of psychological distress in the past year using the
Kessler 6 series. The Kessler 6 series is a commonly used scale of nonspecific psychological distress and is used to describe
the characteristics of adults with and without serious psychological distress. Distress in the past year was assigned to those
indicating a month worse than the current month. If the respondent did not indicate a worse month, the current month's
distress levels are assigned.
Tables 5-8: For these tables respondents were asked: "During the past 12 months, did you take any prescription
medications, such as an antidepressant or sedative, almost daily for two weeks or more, for an emotional or personal
problem?"
237
MENTAL HEALTH & SUBSTANCE ABUSE
text
1.
2.
3.
4.
5.
6.
7.
World Health Organization (2005). Promoting Mental Health: Concepts, Emerging Evidence, Practice. A report of the
World Health Organization, Department of Mental Health and Substance Abuse in collaboration with the Victorian
Health Promotion Foundation and the University of Melbourne. World Health Organization. Geneva.
U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General. Chapter 1:
Introduction. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental
Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute
of Mental Health, 1999. Retrieved July 16, 2010 from the DHS website: http://www.surgeongeneral.gov/library/
mentalhealth/chapter1/sec1.html#approach
National Center for Chronic Disease Prevention and Health Promotion, Public Health Genomics (2010) Genomics
and Health: Mental Health Awareness. Retrieved July 16, 2010 from the CDC website:
http://www.cdc.gov/genomics/resources/diseases/mental.htm
Kessler R.C., Chiu W.T., Demler O., Walters E.E. (2005). Prevalence, severity, and comorbidity of twelve-month
DSM-IV disorders in the National Comorbidity Survey Replication (NCS-R). Archives of General Psychiatry, 2005
June; 62(6): 617–27.
Centers for Disease Control and Prevention (2005). Mental Health Prevalence Data. Retrieved June 11, 2007 from
the CDC website at http://www.cdc.gov/mentalhealth/prevelance_data.htm The BRFSS question used was “Now
thinking about your mental health, which includes stress, depression, and problems with emotions, for how many
days during the past 30 days was your mental health not good?”
U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General. Executive
Summary. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health
Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of
Mental Health, 1999. Retrieved July 16, 2010 from the DHS website:
http://www.surgeongeneral.gov/library/mentalhealth/home.html
Holzer Estimates for Contra Costa County, based on 2004 Census data.
http://www.dmh.cahwnet.gov/Statistics_and_Data_Analysis/Prevalence_Rates_Mental_Disorders.asp
238
MENTAL HEALTH & SUBSTANCE ABUSE
Substance Abuse
Young people, whites and males had higher rates of binge drinking compared
to the county overall.
• Nearly 11% of Contra Costa adults were current smokers
• Among illicit drugs, marijuana was the most commonly used
Substance abuse has been defined as “the overindulgence in and dependence on an addictive substance,
especially alcohol or a narcotic drug”.1 While there is a wide variety of addictive substances, this section
is a brief summary of three key forms of substance abuse: smoking tobacco, binge drinking and use
of illicit drugs.
Smoking Tobacco
In 2007, there were an estimated 83,000 current adult smokers in Contra Costa. This amounted to
10.7% of the county population 18 years and older. Contra Costa’s adult smoking prevalence (10.7%)
was not significantly different from that of the greater Bay Area (12.4%) or California (14.4%).
Table 1 Current smoking
Adults 18 and older, 2007
Smokers Prevalence
California
Greater Bay Area
Contra Costa
3,869,000
671,000
83,000
14.4%
12.4%
10.7%
These estimates are not age-adjusted.
Editor’s note: Analyses of Contra Costa current smoking data by race/ethnicity,
gender and age were not possible due to small sample size, but we can look at
the greater Bay Area overall for an indication of the prevalence of smoking in these
subgroups.
Whites had the greatest number of adult smokers (321,000) in the greater Bay Area followed by Latinos
(141,000), Asians/Pacific Islanders (118,000) and African Americans (58,000).
239
MENTAL HEALTH & SUBSTANCE ABUSE
Table 2 Current smoking by race/ethnicity
Greater Bay Area adults 18 and older, 2007
Smokers
White
Latino
Asian/Pacific Islander
African American
Total
321,000
141,000
118,000
58,000
671,000
Percent
Prevalence
47.8%
21.0%
17.6%
8.6%
100.0%
11.8%
13.7%
10.0%
17.1%
12.4%
These estimates are not age-adjusted.
Total includes racial/ethnic groups not listed above.
More men (408,000) were current smokers than women (263,000) in the greater Bay Area. Men also
had a significantly higher current smoking prevalence (15.3%) compared to women (9.6%).
Table 3 Current smoking by gender
Greater Bay Area adults 18 and older, 2007
Smokers
Men
Women
Total
408,000
263,000
671,000
Percent
60.8%
39.2%
100.0%
Prevalence
15.3%*
9.6%
12.4%
These estimates are not age-adjusted.
* Significantly higher than women.
People 80 years and older had the lowest smoking prevalence (2.4%), lower than adults in the greater Bay
Area (12.4%) overall and all other age groups. Adults ages 65-79 also had a lower smoking prevalence
(6.9%) than adults in the greater Bay Area overall.
Table 4 Current smoking by age group
Greater Bay Area adults 18 and older, 2007
Smokers
18-24 years
25-39 years
40-64 years
65-79 years
80 years and older
Total
101,000
209,000
315,000
41,000
5,000
671,000
These estimates are age-specific.
** Significantly lower rate compared to the greater Bay Area overall
240
Percent
15.1%
31.1%
46.9%
6.1%
0.7%
100.0%
Prevalence
16.3%
13.7%
12.9%
6.9%**
2.4%**
12.4%
MENTAL HEALTH & SUBSTANCE ABUSE
Youth smoking is also an important indicator of this problem. According to data from the California
Health Interview Survey, 14.5% of 15 to 17 year olds in the greater Bay Area were current smokers in
2007. Sample sizes were too small to develop a stable estimate of smoking prevalence among 12–14
year olds in the greater Bay Area.
Why is tobacco use important?
Cigarette smoking remains the leading preventable cause of death in the United States, accounting for
approximately one of every five deaths each year.2
Smoking is the strongest environmental risk factor for lung cancer and pancreatic cancer.3 Exposure to
tobacco smoke is also closely associated with several other diseases including cancer of the larynx,
chronic bronchitis, emphysema, coronary artery disease and hypertensive heart disease.
Tobacco smoke contains respiratory irritants, poisons (including nicotine) and cancer-causing compounds
(carcinogens).4 It can worsen the health effects of air pollution and other inhaled irritants. Half of all
smokers who keep smoking will end up dying from a smoking-related illness.
The adult smoking rate in California in 2006 was 13.3%.5
Who is more likely to smoke?
Educational attainment is closely linked to cigarette use. National surveys have found that adults with
less than a high school education were three times as likely to smoke as those with a bachelor’s degree or more education. Cigarette smoking also varied by race, ethnicity and gender, with the highest
prevalence found among African American men and American Indian and Alaska Native men.6
In 2006, the smoking rate was 6.1% among California middle school students and 15.4% among California high school students. Despite an increase in California's youth smoking rate, the percentage of
California youths who smoke is still far below the national average.5
Preventing smoking among teenagers and young adults is essential because smoking usually begins
in adolescence.6
What can we do about smoking?
Smoking cessation
No matter how old someone is or how long they have smoked, quitting can help them live longer and
be healthier. People who stop smoking before age 50 cut their risk of dying in the next 15 years in half
compared with those who continue smoking.7 Quitting smoking also reduces the risk of lung cancer for
other residents by decreasing secondhand smoke. Every year in the United States, 3,400 non-smoking
adults die of lung cancer as a result of breathing smoke from other people’s cigarettes.8
241
MENTAL HEALTH & SUBSTANCE ABUSE
Nationally, an estimated 69.5% of current adult smokers want to quit smoking. An estimated 70.7% of
African American adults who are current smokers want to quit, as do 70.3% of white, 68.8% of Asian
American and 61.5% of Hispanic current adult smokers.9
Tobacco dependence is a chronic condition that often requires repeated interventions, but effective
treatments and helpful resources exist. Smokers can and do quit smoking. Today, in the United States
there are more former smokers than current smokers.2
Tobacco prevention
The goal of the California Tobacco Control Program is to change the broad social norms around the use
of tobacco by “indirectly influencing current and potential future tobacco users by creating a social milieu and legal climate in which tobacco becomes less desirable, less acceptable and less accessible.”10
State and local tobacco-control policies have proven to be very effective in reducing smoking. Since the
1988 passage of the California Tobacco Tax, per capita cigarette consumption in California declined by
59.0%. During the same period, per capita cigarette consumption in the rest of the nation declined by
only 35.0%. The greater decline in California is a result of activities of the California Tobacco Control
Program along with the higher price of cigarettes in California.11
Unfortunately, there are still approximately 4 million smokers in California (3.6 million adults and
300,000 youths).12
Binge Drinking
In 2007, an estimated 224,000 adults 18 and older in Contra Costa reported binge drinking in the past
year. This amounted to 28.8% of the adult population. This overall prevalence was not different from
that of the greater Bay Area (29.5%) or California (29.7%).
Table 5 Binge drinking
Adults 18 and older, 2007
Cases
California
Greater Bay Area
Contra Costa
7,973,000
1,592,000
224,000
Prevalence
29.7%
29.5%
28.8%
Binge drinking involves
consuming more drinks on
the same occasion than is
considered healthy or safe by
experts. In this section, binge
drinking is defined for males
as having five or more drinks
on a single occasion and for
females as having four or more
drinks on a single occasion.
These estimates are not age-adjusted.
Editor’s note: Analyses of Contra Costa binge drinking by race/ethnicity, gender
or age were not possible due to small numbers, but we can look at the greater
Bay Area overall for an indication of the prevalence of binge drinking in these
subgroups.
242
MENTAL HEALTH & SUBSTANCE ABUSE
The greatest number of binge drinking reports in the greater Bay Area was among whites (935,000)
followed by Latinos (343,000), Asians/Pacific Islanders (207,000), African Americans (56,000) and
American Indian/Alaska Natives (12,000). In the greater Bay Area, 1,592,000 adults reported binge
drinking in the past year.
Whites (34.3%) had a binge drinking prevalence that was significantly higher than the rate of the greater
Bay Area overall (29.5%). Asians/Pacific Islanders (17.5%) and African Americans (16.4%) had lower
prevalence than the greater Bay Area as a whole.
Table 6 Binge drinking by race/ethnicity
Greater Bay Area adults 18 and older, 2007
White
Latino
Asian/Pacific Islander
African American
American Indian/Alaska Native
Total
Cases
Percent
Prevalence
935,000
343,000
207,000
56,000
12,000
58.7%
21.5%
12.5%
3.5%
0.8%
34.3%*
33.4%
17.5%**
16.4%**
43.8%
1,592,000
100.0%
29.5%
These estimates are not age-adjusted.
Total includes racial/ethnic groups not listed above.
* Significantly higher rate compared to the greater Bay Area overall.
** Significantly lower rate compared to the greater Bay Area overall.
Men and women were different when it came to binge drinking. More men (941,000) than women
(652,000) had engaged in binge drinking in the past year. Men (35.4%) also had a significantly higher
prevalence of binge drinking compared to women (23.8%).
Table 7 Binge drinking by gender
Greater Bay Area adults 18 and older, 2007
Cases
Men
Women
Total
941,000
652,000
1,592,000
Percent Prevalence
59.1%
41.0%
100.0%
35.4%*
23.8%
29.5%
These estimates are not age-adjusted.
* Significantly higher rate compared to women
Most Bay Area adults (95.0%) who engaged in binge drinking were younger than 65 years.
Young adults had higher prevalence of binge drinking. Adults aged 18–24 (45.5%) and 25–39 (39.1%)
years had significantly higher prevalence of binge drinking than the greater Bay Area overall (29.5%).
Adults 65–79 years had a significantly lower prevalence (11.5%) of binge drinking compared to the
243
MENTAL HEALTH & SUBSTANCE ABUSE
greater Bay Area (29.5%). Adults 80 years and older had the lowest prevalence (5.4%); significantly
lower than the greater Bay Area and all other age groups.
Table 8 Binge drinking by age group
Greater Bay Area adults 18 And older, 2007
18–24 years
25–39 years
40–64 years
65–79 years
80 years and older
Total
Cases
Percent
Prevalence
282,000
596,000
635,000
68,000
12,000
1,592,000
17.7%
37.4%
39.9%
4.3%
0.8%
100.0%
45.5%*
39.1%*
26.0%
11.5%**
5.4%**
29.5%
These estimates are age-specific.
* Significantly higher rate compared to the greater Bay Area overall.
** Significantly lower rate compared to the greater Bay Area overall.
What is binge drinking?
Binge drinking involves consuming more drinks on the same occasion than is considered healthy or
safe by experts. In this section, binge drinking is defined for males as having five or more drinks on a
single occasion and for females as having four or more drinks on a single occasion.
Binge drinking is considered "alcohol abuse," a pattern of problematic drinking that continues despite
recurrent adverse consequences, such as harm to one’s health, interpersonal relationships or the ability to work.13 Binge drinking differs from alcoholism, also known as “alcohol dependence,” which is
recognized as a chronic disease that includes the following four symptoms: craving, loss of control,
physical dependence and tolerance (i.e., the need to drink greater amounts of alcohol to get "high.")13
Most people who binge drink are not alcohol dependent.14
Why is binge drinking important?
Alcohol use is very common in our society. Drinking alcohol has immediate effects that can increase the
risk of many harmful health conditions. Alcohol use poses additional problems for underage drinkers.
Alcohol use is the third leading lifestyle-related cause of death for people in the United States each year. 15
About 75% of the alcohol consumed by adults in the United States is in the form of binge drinks.16 Approximately 92% of U.S. adults who drink excessively report binge drinking in the past 30 days.17
Binge drinking is associated with risk-taking behaviors that can lead to a number of health issues, including unintentional injuries (e.g., car crashes, falls, burns, drowning), intentional injuries (e.g., firearm
injuries, sexual assault, domestic violence), alcohol poisoning, sexually transmitted diseases (e.g. HIV/
AIDS, hepatitis C), and unintended pregnancy. Over-consumption of alcohol can also result in children
born with fetal alcohol spectrum disorders.13
244
MENTAL HEALTH & SUBSTANCE ABUSE
Who is risk of developing alcohol problems?
Although men are more likely to drink alcohol and drink in larger amounts, gender differences in body
structure and chemistry cause women to absorb more alcohol, and take longer to break it down and
remove it from their bodies (i.e., to metabolize it). In other words, upon drinking equal amounts, women have higher alcohol levels in their blood than men, and the immediate effects occur more quickly
and last longer. These differences also make women more vulnerable to alcohol’s long-term effects on
their health.18
Nationally, alcohol abuse is more prevalent among whites than among Hispanics, blacks and Asians. Alcohol dependence is more prevalent among Native Americans, Hispanics and whites than among Asians.19
Research also shows that people who start drinking at an early age — for example, at age 14 or younger —are at much higher risk of developing alcohol problems at some point in their lives compared to
someone who starts drinking at age 21 or after. 13 About 90% of the alcohol consumed by youths younger
than 21 years in the United States is in the form of binge drinks.16
Drinking alcohol can be especially harmful to adolescents whose growing bodies and brain are in a
critical stage of development. Drinking under the age of 21 is against the law and is typically called
underage drinking. Adolescents are more vulnerable to the harmful effects of alcohol than adults, and
underage drinking puts them at a higher risk of becoming alcoholics at a later age. Because drinking is
part of our culture, teenagers receive messages leading them to believe that drinking is acceptable. In
Contra Costa County, 41% of 11th-grade students reported drinking alcohol in the past 30 days. This is
twice the reported use for marijuana (18%) or any other drug, and higher than the state rate (37%).20
In Contra Costa County, 22% of 11th-graders report binge drinking in the past 30 days and 10% report
binge drinking three or more days in the past month, suggesting a pattern of risky behavior.20
What can we do about binge drinking?
Beer accounted for most alcohol consumed by binge drinkers and most alcohol consumed by those at
greatest risk of causing or incurring alcohol-related harm. Lower excise taxes and relatively permissive
sales and marketing practices for beer as compared with other beverage types may account for some
of these research findings. Establishing alcohol-control policies/taxes at more stringent levels would be
an effective way to prevent excessive drinking.21
Evidence-based prevention efforts include interventions aimed at the general public (all drinkers) and
those that prioritize underage drinkers:
• Limit the number of retail alcohol outlets in a given area and limit the days and hours of alcohol sale.
• Increase alcoholic beverage costs and alcohol taxes.
• Consistently enforce laws and policies intended to prohibit adults from furnishing alcohol to minors.
• Join a local coalition and support community efforts to limit the availability of alcohol to young people.
• Work toward shifting community norms regarding underage drinking and creating a new attitude
for unsafe and unhealthy alcohol promotion
245
MENTAL HEALTH & SUBSTANCE ABUSE
Illicit Drug Use
Current illicit drug use refers to the use of illegal drugs (including marijuana or hashish, cocaine,
inhalants, hallucinogens, lysergic acid diethylamide (LSD), Ecstasy (MDMA), heroin and prescriptiontype psychotherapeutics used non-medically) in the last month.
Nationally, 20.1 million people (8.0%) of the population ages 12 years or older reported being current
(within the past month) illicit drug users in 2008. Of those who used illicit drugs, most used marijuana
or marijuana in combination with other drugs (15.2 million).22
Table 9 Current illicit drug use
U.S. residents 12 and older, 2008
Prevalence
Marijuana
Prescription-type psychotherapeutics
used nonmedically
Cocaine
Hallucinogens
Total
Estimated
number of users
(in millions)
6.1%
2.5%
15.2
6.2
0.7%
0.4%
8.0%
1.9
1.1
20.1
Total includes drugs not listed above.
Drug groups are not mutually exclusive.
The following were the key findings of the 2008 National Survey on Drug Use and Health produced
by the U.S. Department of Health and Human Services.22
•
•
•
•
•
•
•
•
•
The rate of illicit drug use in 2008 (8.0%) was the same as the rate in 2007 (8.0%)
The rate of past month marijuana use in 2008 (6.1%) was similar to the rate in 2007 (5.8%)
There were an estimated 1.9 million cocaine users nationwide (0.7% of the population aged
12 and above) and 1.1 million hallucinogen users (0.4% of the population), including 555,000
who had used Ecstasy.
There were an estimated 6.2 million people aged 12 and over who used prescription-type
psychotherapeutic drugs non-medically. These drugs include pain-relievers, tranquilizers,
stimulants and sedatives.
There were an estimated 10 million people (4.0% of those 12 and older) who reported driving
under the influence of illicit drugs in the past year.
An estimated 22. 2 million people were classified with substance dependence or abuse in the
past year. Of these:
3.1 million were dependent or abused both alcohol and illicit drugs
3.9 million were dependent or abused illicit drugs but not alcohol
15.2 million abused alcohol but not illicit drugs
246
MENTAL HEALTH & SUBSTANCE ABUSE
If the national pattern of illicit drug use in 2008 were applied to Contra Costa County, there would
have been more than 71,000 users of these drugs.
Table 10 Estimated illicit drug use
Contra Costa County Residents 12 and Older, 2008
Marijuana
Prescription-type psychotherapeutics
used nonmedically
Cocaine
Hallucinogens
Total
Estimated number of users
54,377
22,286
6,240
3,566
71,314
Total includes drugs not listed above
Drug groups are not mutually exclusive
Substance-abuse treatment admissions suggest that methamphetamine use may be particularly
important within Contra Costa County. In 2009, there were 4,201 admissions to licensed or publicly
funded facilities for substance-abuse treatment in Contra Costa. More people were admitted for
methamphetamine-abuse treatment (1,297) than any other drug group. Alcohol was the second most
common reason for admission (1,046), followed by marijuana (659).23
What is drug addiction?
Drug addiction is a chronic, often relapsing condition that causes compulsive drug seeking and use despite harmful consequences to the individual who is addicted and to those around them.
Although the initial decision to take drugs is often voluntary, over time drug abuse can lead to structural and functional changes in the brain that can affect self-control, hinder sound decision-making and
result in intense impulses to take drugs.24
Why is drug addiction important?
With continued drug use, there is a danger of a fatal or non-fatal overdose. In health statistics, intentional drug overdoses are counted as suicides and unintentional (accidental) overdoses are documented
as drug “poisonings.” (See this report's Injury sections for statistics.)
Beyond the harmful consequences for the addicted person, drug abuse can cause serious health problems for others. Drug abuse can contribute to the spread of serious infectious diseases in several ways.
247
MENTAL HEALTH & SUBSTANCE ABUSE
Injection of drugs such as heroin, cocaine and methamphetamine can facilitate the spread of HIV/AIDS
and hepatitis C.25
Drug use can also interfere with a person’s judgment, increasing the likelihood of engaging in risky
sexual behaviors that can contribute to the spread of HIV/AIDS, hepatitis B, and other sexually transmitted diseases. (See this report's HIV/AIDS and STD sections for more information.)
Who is at risk for drug addiction?
No single factor can predict whether or not a person will become addicted to drugs. Risk for addiction
is influenced by a person’s biology, social environment, and age or stage of development. The more risk
factors an individual has, the greater the chance that taking drugs can lead to addiction.
For example:
Biology. The genes that people are born with—in combination with environmental influences—account
for about half of their addiction vulnerability. Additionally, gender, ethnicity and the presence of other
mental disorders may influence risk for drug abuse and addiction.
Environment. Peer pressure, physical and sexual abuse, stress, poverty and limited parental involvement can greatly influence the course of drug abuse and addiction in a person’s life.
Development. Genetic and environmental factors interact at critical developmental stages in a person’s
life to affect addiction vulnerability. Although taking drugs at any age can lead to addiction, the earlier
drug use begins, the more likely it is to progress to more serious abuse. And because adolescents’
brains are still developing in the areas that govern decision-making, judgment and self-control, they
are especially prone to risk-taking behaviors, including trying drugs.24
What can we do about drug addiction?
Drug addiction is a preventable disease. Results from NIDA-funded research have shown that prevention programs families, schools, communities and the media are effective in reducing drug abuse. Although many events and cultural factors affect drug-abuse trends, when youths perceive drug abuse
as harmful, they reduce their drug use. It is necessary, therefore, to help youth and the general public
understand the risks of drug abuse.24
Research has shown the key risk periods for drug abuse in youths are during major transitions in children’s lives. Prevention programs aimed at general populations at key transition points, such as the
transition to middle school, can produce beneficial effects even among high-risk families and children.
Such interventions do not single out risk populations and, therefore, reduce labeling and promote bonding to school and community.26
The impact of specific risk and protective factors changes with age. For example, risk factors within the
family have greater impact on a younger child, while association with drug-abusing peers may be a
more significant risk factor for an adolescent. Because risks appear at every life transition, prevention
248
MENTAL HEALTH & SUBSTANCE ABUSE
planners need to choose prevention programs that strengthen protective factors across the life course.
Parents can use information on risk and protection to help them develop positive preventive actions
(e.g., talking about family rules) before problems occur.
Educators can strengthen learning and bonding to school by addressing aggressive behaviors and poor
concentration — associated with later onset of drug abuse and related problems.
Community Leaders can assess community risks and protective factors associated with drug problems
to best target prevention services.25
Research has shown programs that reach youths through multiple settings can strongly impact community norms.
Data Sources: Substance Abuse
text
Houghton Mifflin Company. (2000) The American Heritage Dictionary of the English Language, Fourth Edition.
Centers for Disease Control and Prevention. (2010) Smoking & Tobacco Use- CDC Fact Sheet. Retrieved July 24, 2010
from
http://www.cdc.gov/tobacco/data_statistics/fact_sheets/cessation/quitting/index.htm
3. Stewart, S., Cardinez, C., Richardson, L. (2008) Surveillance for Cancers Associated with Tobacco Use—United States,
1999–2004. MMWR. September 5, 2008 / 57(SS08);1-33. Department of Health and Human Services. Retrieved June
18, 2010 from the CDC website: http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5708a1.htm
4. Centers for Disease Control and Prevention. (2005) National Center for Health Statistics; Health, United Sates, 2004
With Chartbook on Trends in the Health of Americans. (PDF-116KB) Hyattsville, MD: U.S. Department of Health
and Human Services. Available from the CDC website: http://www.cdc.gov/nchs/data/hus/hus04.pdf
5. California Department of Public Health, CDIC/Tobacco Control Section. (2010) CA Success. Retrieved July 24, 2010
from http://www.tobaccofreeca.com/ca_success.html
6. National Center for Health Statistics (2010). Health, United States, 2009 with Chartbook with Special Feature on
Meidcal Technology. US Dept of Health & Human Services. DHHS Publication No. 2010-1232. Retrieved May 17,
2007 at the CDC website: http://www.cdc.gov/nchs/data/hus/hus09.pdf
7. American Cancer Society (2009) Guide to Quitting Smoking. Retrieved June 19, 2010 from the ACS website: http://
www.cancer.org/docroot/PED/content/PED_10_13X_Guide_for_Quitting_Smoking.asp
8. American Cancer Society, California Division and Public Health Institute, California Cancer Registry (2006).
California Cancer Facts and Figures 2007. Oakland, CA: American Cancer Society, California Division.
9. National Center for Health Statistics. Data File Documentation, National Health Interview Survey, 2005 (machinereadable data file and documentation). Hyattsville, MD: National Center for Health Statistics, Centers for Disease
Control and Prevention, 2006 [accessed 2007 May 10].
10. California Department of Health Services. (1998) A Model for Change: The California Experience in Tobacco Control.
Sacramento, CA: California Department of Health Services.
11. Hu T-W, Sung HY, Keeler TE. Reducing cigarette consumption in California: tobacco taxes vs an anti-smoking media
campaign. Am J Public Health. 1995; 85:1218–22.
12. California Department of Public Health, California Tobacco Control Program. (2009) California Tobacco Control
Update 2009: 20 Years of Tobacco Control in California. Retrieved June 5, 2010 from the CA DPH website: http://www.
cdph.ca.gov/programs/tobacco/Documents/CTCPUpdate2009.pdf
1.
2.
249
MENTAL HEALTH & SUBSTANCE ABUSE
13. National Institute on Alcohol Abuse and Alcoholism. FAQ for the General Public. Retrieved July 23, 2010 from the
NIH website: http://www.niaaa.nih.gov/FAQs/General-English/default.htm - groups
14. Centers for Disease Control and Prevention (2010) CDC Fact Sheet: Binge Drinking. Retrieved July 24, 2010 from the
CDC website: http://www.cdc.gov/alcohol/fact-sheets/binge-drinking.htm
15. Centers for Disease Control and Prevention. (2010) Alcohol and Public Health. Retrieved July 24, 2010 from the CDC
website: http://www.cdc.gov/Alcohol/|
16. Office of Juvenile Justice and Delinquency Prevention. Drinking in America: Myths, Realities, and Prevention Policy.
Washington, DC: U.S. Department of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency
Prevention, 2005. Available at http://www.udetc.org/documents/Drinking_in_America.pdf. Accessed July 24, 2010.
17. Town M, Naimi TS, Mokdad AH, Brewer RD. Health care access among U.S. adults who drink alcohol excessively:
missed opportunities for prevention. Prev Chronic Dis [serial online] April 2006. Accessed July 24, 2010. http://www.
cdc.gov/pcd/issues/2006/apr/05_0182.htm
18. Centers for Disease Control and Prevention. (2010) Excessive Alcohol Use and Risks to Women’s Health- CDC Fact
Sheet. Retrieved July 24, 2010 from the CDC website: http://www.cdc.gov/alcohol/fact-sheets/womens-health.htm
19. National Institute on Alcohol Abuse and Alcoholism. (2004) Alcohol Abuse Increases, Dependence Declines Across
Decade: Young Adult Minorities Emerge As High-Risk Subgroups. Retrieved July 24, 2010 from the NIAAA website:
http://www.niaaa.nih.gov/NewsEvents/NewsReleases/NESARCNews.htm
20. Binge drinking rates from California Healthy Kids Survey (2007)
21. Naimi TS, Brewer RD, Miller JW, Okoro C, Mehrotra C. (2007) What do binge drinkers drink? Implications for alcohol
control policy. Am J Prev Med. Sep;33(3):188-93. PubMed PMID: 17826577.
22. Results from the 2008 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, NSDUH
Series H-36, HHS Publication No. SMA 09-4434). Rockville, MD. Available from:http://www.oas.samhsa.gov/
nsduh/2k8nsduh/2k8Results.cfm
23. Information from the Alcohol and Other Drugs (AODS) Program (Substance Abuse Prevention Program), Contra
Costa Health Services, August 2010, from 2009 CalOMS treatment admission data
24. National Institute on Drug Abuse. NIDA InfoFacts: Understanding Drug Abuse and Addiction. Retrieved July 24, 2010
from the NIH website: http://www.nida.nih.gov/Infofacts/understand.html
25. National Institute on Drug Abuse. (2010) NIDA InfoFacts: Addiction and Health. Retrieved July 24, 2010 from the
NIH website: http://www.nida.nih.gov/scienceofaddiction/health.html
26. US Dept of Health and Human Services, National Institutes of Health, National Institute on Drug Abuse (2003)
Preventing Drug Use among Children and Adolescents: A Research-Based Guide. Retrieved July 24, 2010 from the NIH
website: http://www.drugabuse.gov/pdf/prevention/InBrief.pdf
tables
Tables 1-8: Data presented for Latinos include Latino residents of any race. Data presented for whites, Asians/Pacific
Islanders and African Americans include non-Latino residents. Not all race/ethnicities are shown but all are included in
Contra Costa, greater Bay Area and California totals.
Tables 1-4: Local data about tobacco use comes from the California Health Interview Survey’s AskCHIS data query
system, copyright© 2007 the Regents of the University of California, all rights reserved, available online at:
http://askchis.com/main/default.asp. Data analysis performed in April 2010. Current smoking prevalence refers to the
percent of respondents who report that they now smoke based on a series of smoking related questions. In Table 4, data
for American Indians/Alaska Natives was excluded due to small numbers. AskCHIS data are generated from a telephone
survey that asks questions to a randomly selected group of residents in Contra Costa and other counties in California.
Responses are then weighted to represent the county, region and state as whole. The Greater Bay Area includes the
counties of Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano and Sonoma.
Tables 5-8: Local data about binge drinking from the California Health Interview Survey’s AskCHIS data query system,
copyright© 2007 the Regents of the University of California, all rights reserved, available online at:
http://askchis.com/main/default.asp. Data analysis performed in April 2010. Respondents were asked a series of questions
250
MENTAL HEALTH & SUBSTANCE ABUSE
concerning their alcohol consumption in the past year to determine binge drinking. AskCHIS data are generated from
a telephone survey that asks questions to a randomly selected group of residents in Contra Costa and other counties in
California. Responses are then weighted to represent the county, region, and state as whole. The greater Bay Area includes
the counties of Alameda, Contra Costa, Marin, Napa, San Francisco, San Mateo, Santa Clara, Solano and Sonoma.
Table 9: National data from the Results from the 2008 National Survey on Drug Use and Health: National Findings (Office of
Applied Studies, NSDUH Series H-36, HHS Publication No. SMA 09-4434). Rockville, MD. Available at:
http://www.oas.samhsa.gov/nsduh/2k8nsduh/2k8Results.cfm
Table 10: Local estimates for illicit drug use among Contra Costa residents ages 12 years and older were created by the
Community Health Assessment Planning and Evaluation (CHAPE) Unit of Contra Costa Health Services by applying
national estimates of the percent of people 12 years and older using illicit drugs from the 2008 National Survey on Drug
Use and Health to 2008 population projections for Contra Costa County residents ages 12 years and older from the State
of California, Department of Finance, Race/Ethnic Population with Age and Sex Detail, 2000–2050. Sacramento, CA, July
2007.
251
COMMUNICABLE DISEASES
Childhood Immunization
and Vaccine-Preventable Diseases
Contra Costa did not meet the Healthy People 2010 objective for immunization for 2 year olds.
Immunization is a critical public health prevention activity. In 2008 among all children in Contra Costa
2 years of age, 80.0% had been fully immunized. However, Contra Costa did not meet the Healthy
People 2010 objective of having at least 90% of all 2 year olds fully immunized.
Table 1 Percent fully immunized at 24 months, 2008
Percent
Contra Costa
80.0%
California
76.7%
Healthy People 2010 objective
90.0%
Fully immunized means four doses of DTaP, three doses of polio vaccine and one dose
of MMR by 24 months.
Table 2 Percent fully immunized at 24 months, 2003-2008
2003
2004
2005
2006
2007
2008
Contra
Costa
76.6%
81.6%
73.9%
75.5%
81.0%
80.0%
California
71.4%
71.8%
76.3%
77.7%
75.7%
76.7%
Fully immunized means four doses of DTaP, three doses of polio vaccine and one dose of MMR by 24
months.
Between 2003 and 2008, the percentage of fully immunized 2-year -old children in Contra Costa has
fluctuated from a high of 81.6% in 2004 to a low of 75.5% in 2006.
252
COMMUNICABLE DISEASES
Table 3 Percent fully immunized at 24 months
By Race/Ethnicity, 2008
Contra Costa
White
Hispanic
African American
Total
85.0%
80.0%
67.0%
80.0%
California
75.6%
77.3%
66.0%
76.7%
Fully immunized means four doses of DTaP, three doses of polio vaccine and
one dose of MMR by 24 months.
The rate of immunizations by race/ethnicity in both Contra Costa and California are below 90%, the
Healthy People 2010 objective.
What is immunization?
Immunization is the process by which an individual’s immune system becomes fortified against an infection or disease, most often through vaccines.
A vaccine is an injection, oral dose or nasal spray that typically contains an agent that resembles a
disease-causing microorganism, and is often made from weakened or killed forms of the microbe or its
toxins. Vaccines can prepare the body’s immune system, thus helping to fight or prevent an infection.
Why is it important?
Vaccination is a highly effective method of preventing certain infectious diseases.
For the individual, and for society in terms of public health, prevention is better and more cost-effective
than cure. Vaccines are generally very safe and serious adverse reactions are uncommon.1
California law requires that children be up-to-date on their immunizations before entering kindergarten
and seventh grade, and before enrolling in licensed child care programs.
Brief summary of some vaccine-preventable diseases:
Diphtheria
Bacterial infection that produces a toxin that interferes with
normal heart, nerve and organ function. It has a 20% case
fatality rate
Tetanus (lockjaw)
Bacterial infection that can cause muscle spasms and
interferes with breathing
Pertussis
Bacterial infection that can cause severe respiratory
(whooping cough)
complications, pneumonia and death in infants
Polio
Viral infection that attacks the motor neurons and causes a
crippling paralysis
253
COMMUNICABLE DISEASES
Vaccines are responsible for the control of many deadly infectious diseases that were once common in
this country, including polio, measles, diphtheria, pertussis (whooping cough), rubella (German measles), mumps, tetanus and Haemophilus influenzae type b (Hib).
For some vaccine-preventable diseases, there are now only a small number of cases reported in the
county each year. Still, immunization remains an important part of the strategy to maintain the reduction in cases. Because a rise in disease is always possible, it is important to be vigilant. The success
of an immunization program depends on high rates of acceptance and coverage.
Who does it impact most?
People who cannot be immunized include those who are too young to be vaccinated (e.g., children
younger than 1 year old cannot receive the measles vaccine but can be infected by the measles virus),
those who cannot be vaccinated for medical reasons (e.g., children with leukemia), and those who
cannot make an adequate response to vaccination.2
Others choose not to be immunized. Some parents refuse to get their children vaccinated, believing
that the vaccine is unnecessary or may harm their child. In Contra Costa, the percent of personal belief exemptions (PBEs) have been on the rise, increasing from 0.75% among kindergarten entrants in
1998 to 2.18% in 2008.3 Public health officials are concerned about this rise in PBEs because there will
be less “community immunity” as fewer people are vaccinated and protected. This is particularly important for those who can’t be vaccinated including the very young and immunocompromised people.
What can we do about it?
In the United States, policy interventions, such as immunization requirements for school entry, have
contributed to high vaccine coverage and record or near-record lows in the levels of vaccine-preventable diseases.
Parents view doctors as respected sources of information. There is a renewed need for doctors to discuss the hazards of refusing vaccination for both the individual, their family members and the community as a whole. There is no scientific evidence that links autism to vaccines, and numerous large
studies have failed to find any connection.4
By law, California managed care organizations (such as the Contra Costa Health Plan and Kaiser Permanente) must cover recommended immunizations for children.
Children without health insurance may be able to get free immunizations through one of these programs:
Healthy Families: Children enrolled in California’s Healthy Families plan receive free immunizations
with no copayment.
Medi-Cal: Medi-Cal covers preventive care services for eligible low-income children and adults.
Vaccines for Children: Many private-practice California doctors participate in the Vaccines for Children
(VFC) program, which gives free vaccines to eligible children up to age 18.
254
COMMUNICABLE DISEASES
CHDP: Children eligible for California’s Child Health and Disability Prevention (CHDP) program may also
be eligible for free or low-cost shots.5
Preschool-age children who remain under-vaccinated are likely to have missed some vaccinations because of interruptions in the family’s health care coverage or socio-demographic characteristics, such
as poverty or limited English proficiency.3
Data Sources: Immunizations
tables
Tables 1–3: Local data about immunization levels is analyzed by the California Department of Public Health (CDPH),
Immunization Branch and the Contra Costa Health Services Immunizations Program. A random survey of schools is used
to assess the immunization levels of students in kindergarten. CDPH uses these immunization records to estimate the
percentage of children who were up-to-date when they were 2 years old. Not all race/ethnicity groups were available due
to small sample size.
“Fully immunized” in this survey means receiving four DTaP (diphtheria, tetanus, pertussis) vaccine, three doses of Polio
vaccine and one dose of MMR (measles, mumps, rubella) vaccines before 24 months of age.
text
1.
2.
3.
4.
5.
World Health Organization International Travel and Health 2010. Retrieved July 16, 2010 from the WHO website:
http://www.who.int/topics/immunization/en/
Department of Health & Human Services. (2009) Vaccines & Immunizations: How Vaccines Prevent Disease.
Retrieved July 16, 2010 from the CDC website:
http://www.cdc.gov/vaccines/vac-gen/howvpd.htm
Contra Costa Health Services, Public Health Division, Communicable Disease Program, Immunization Coordinator,
December 2009
Omer SB, Salmon DA, et al. (2009) Vaccine Refusal, Mandatory Immunization, and the Risks of VaccinePreventable Diseases. The New England Journal of Medicine. 360;19 May 7, 2009. Available:
http://content.nejm.org/cgi/reprint/360/19/1981.pdf
California Immunization Coalition (2008) Vaccine Basics. Retrieved July 16, 2010 from
http://www.whyichoose.org/vaccinebasics.html
255
COMMUNICABLE DISEASES
HIV/AIDS
African Americans had the highest rate
of AIDS diagnoses.
•
•
•
•
Whites had the highest number of HIV infections.
Males had a higher rate of AIDS diagnoses than females.
Among males with AIDS, sex with other males was the major mode of HIV transmission.
More than half of AIDS diagnoses in the county were among residents of Richmond,
Concord, Antioch and Pittsburg.
Human immunodeficiency virus, or HIV, is the virus that causes acquired immunodeficiency syndrome
or AIDS. AIDS refers to the most advanced stage of HIV disease. This report presents information
about both HIV infection and AIDS.
HIV Infection
The reporting of HIV infections by name began in California in April 2006. From 2006 to 2008 there
were 599 HIV infections reported by name in Contra Costa County. Almost half (49.6%) of the infections were among whites, followed by African Americans (30.1%), Latinos (17.7%) and Asians/Pacific
Islanders (2.0%). The time these people were infected is not known.
Table 1 HIV cases by race/ethnicity
Contra Costa County, April 2006–December 2008
Cases
White
African American
Latino
Asian/Pacific Islander
Total
297
180
106
12
599
Percent
49.6%
30.1%
17.7%
2.0%
100.0%
Rate
21.2
69.3*
15.4**
3.0
20.9
These are unadjusted crude rates per 100,000 residents.
Total includes racial/ethnic groups not shown.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
African Americans had the highest rate of reported HIV infections (69.3 per 100,000); significantly
higher than the county (20.9 per 100,000) and all other racial/ethnic groups listed. Latinos had a
significantly lower reported infection rate (15.4 per 100,000) than the county overall.
The vast majority of HIV cases reported were among males (486), and males had a significantly higher
reported infection rate (34.7 per 100,000) than females (7.7 per 100,000). Fewer than one in five cases
(18.9%) were among females.
256
COMMUNICABLE DISEASES
Table 2 HIV cases by gender
Contra Costa County, April 2006–December 2008
Cases
Males
Females
Total
Percent
486
113
599
81.1%
18.9%
100.0%
Rate
34.7*
7.7
20.9
These are unadjusted crude rates per 100,000 residents.
* Significantly higher rate than females.
More than half (59.6%) of all HIV cases were among those aged 25–44 years. This age group had
the highest reported infection rate (44.5 per 100,000); significantly higher than the county (20.9 per
100,000) and all other age groups listed. The infection rate for those ages 0–24 (7.5 per 100,000) was
significantly lower than the county rate. The 73 cases in this age group included nine people under
age 5 and 12 people aged 13 to 19.
Table 3 HIV cases by age at first positive test
Contra Costa County, April 2006–December 2008
Cases
Percent
Rate
73
357
165
599
12.2%
59.6%
27.5%
100.0%
7.5**
44.5*
21.7
20.9
0–24 years
25–44 years
45–64 years
Total
These are unadjusted crude rates per 100,000 residents.
Total includes age groups not shown.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
AIDS
AIDS is the most severe form of HIV infection and is diagnosed when one of a number of specific
opportunistic infections or cancers develops or the CD4+T cell count drops below 200. Contra Costa’s
rate of reported AIDS cases among residents was lower (6.9 per 100,000) than the rate for California
(10.9 per 100,000), but it did not meet the Healthy People 2010 objective (1.0 per 100,000.)
Between 2005 and 2007, there were 213 AIDS cases diagnosed in Contra Costa County. African
Americans had the highest number of cases (86) followed by whites (71), Latinos (44) and Asians/
Pacific Islanders (12).
Although African Americans accounted for only 9.1% of the population of Contra Costa County in
2005–2007, they accounted for 40.4% of all new AIDS diagnoses. They had a significantly higher rate
(30.7 per 100,000) of AIDS diagnoses than whites (4.4 per 100,000), Latinos (6.7 per 100,000) and
the county overall (6.9 per 100,000). The rate among whites was significantly lower than the overall
county rate.
257
COMMUNICABLE DISEASES
Table 4 Residents diagnosed with AIDS by race/ethnicity
Contra Costa County, 2005 – 2007
Cases
86
71
44
12
213
African American
White
Latino
Asian/Pacific Islander
Total
Percent
40.4%
33.3%
20.7%
5.6%
100.0%
Rate
30.7*
4.4**
6.7
NA
6.9
These are crude rates per 100,000 residents.
* Significantly higher than the county overall.
** Significantly lower than the county overall.
More than three-quarters (79.8%) of AIDS diagnoses were among males. Males also had a significantly
higher rate of AIDS diagnoses (11.2 per 100,000) compared to females (2.7 per 100,000).
Table 5 Residents diagnosed with AIDS by gender
Contra Costa County, 2005 – 2007
Cases
Males
Females
Total
170
43
213
Percent
79.8%
20.2%
100.0%
Rate
11.2*
2.7
6.9
These are crude rates per 100,000 residents.
* Significantly higher than females.
More than half (57.7%) of new AIDS diagnoses were among adults 25-44 years of age. Almost one-third
(31.0%) of the cases were among adults 45-64 years of age. Adults 25-44 years had the highest rate (14.4
per 100,000); significantly higher than the county (6.9 per 100,000) and the other age groups. Residents
aged 0–24 had a rate of AIDS diagnoses significantly lower than the county overall.
Table 6 Residents diagnosed with aids by age
Contra Costa County, 2005 – 2007
Cases
0–24 years
25–44 years
45–64 years
65 years and older
Total
20
123
66
NA
213
These are age-specific rates per 100,000 residents.
Total includes all ages.
* Significantly higher than the county overall.
** Significantly lower than the county overall.
258
Percent
Rate
9.4%
57.7%
31.0%
1.9%
100.0%
1.9**
14.4*
8.0
NA
6.9
COMMUNICABLE DISEASES
More than half (54.5%) of AIDS diagnoses in the county were among residents of four cities: Richmond
(19.2%), Concord (13.6%), Antioch (11.3%) and Walnut Creek (10.3%).
Richmond had a higher rate (13.3 per 100,000) of AIDS diagnoses compared to the county as a whole
(6.9 per 100,000).
Table 7 Residents diagnosed with AIDS by selected cities
Contra Costa County, 2005 – 2007
Cases
Richmond
Concord
Antioch
Walnut Creek
Pittsburg
San Pablo
Total
Percent
Rate
41
19.2%
13.3*
29
24
22
20
14
213
13.6%
11.3%
10.3%
9.4%
6.6%
100.0%
7.8
8.0
11.2
10.7
NA
6.9
These are crude rates per 100,000 residents.
Total includes cities not shown.
* Significantly higher than the county.
Men having sex with other men (MSM) was a major mode of HIV transmission among men diagnosed
with AIDS from 2005-2007. Men having sex with men accounted for 73.5% of AIDS cases diagnosed
among males during this period. For females, injection drug use and heterosexual contact accounted
for a majority (81.4%) of cases. Almost half (48.8%) of the AIDS cases diagnosed among females from
2005-2007 were transmitted via heterosexual contact. Injection drug use was the mode of transmission
for 32.6% of AIDS cases diagnosed among females during this same period.
Table 8 AIDS Cases by Probable Mode of Infection & Gender
Contra Costa County, 2005 – 2007
Male Percent
Men who have sex with men
(MSM)
Injection drug use (IDU)
Heterosexual contact
MSM injection drug use
Unknown or not reported
Total
Female
125
73.5%
NA
15
7
5
18
170
8.8%
4.1%
2.9%
10.6%
100.0%
14
21
NA
8
43
259
Percent
NA
32.6%
48.8%
NA
18.6%
100.0%
Total
125
29
28
5
26
213
COMMUNICABLE DISEASES
The number of Contra Costa County residents dying from AIDS has dramatically declined since
1996 when antiretrovirals became widely accessible. Improved medications, earlier diagnosis of HIV,
earlier access to treatment and care, and better-trained physicians have contributed to the decline in
the number of AIDS-related deaths.
Figure 1 Deaths among people diagnosed with AIDS in Contra Costa
by year of death 1982-2008
(N=1,716)
185
135
151 150
161
111
39
62
73
66
44
20
39
45
42
29
42
38
38
30
22
19
82
19
83
19
84
19
85
19
86
19
87
19
88
19
89
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
1
3
12
51
108
What are HIV & AIDS?
HIV, or human immunodeficiency virus, is the virus that can lead to acquired immune deficiency syndrome, or AIDS. HIV damages a person’s body by destroying specific blood cells, called CD4+ T cells,
which are crucial to helping the body fight diseases.1
AIDS is the late stage of HIV disease, when a person’s immune system is severely damaged and has
difficulty fighting opportunistic infections and certain cancers.
Why is it important?
HIV/AIDS is a worldwide health problem and a global pandemic. In 2007, it was estimated that 33.2
million people lived with the disease worldwide, and that AIDS killed an estimated 2.1 million people,
including 330,000 children.2
More than 25 years after the initial onset of the AIDS epidemic, the crisis of HIV/AIDS infection continues
to represent a serious health emergency for the Contra Costa County health and social service system,
and has had tragic consequences for people living with and impacted by HIV and AIDS.3
Currently, HIV/AIDS disproportionally burdens the African American community. Significant stigma exists in regard to many HIV risk behaviors and populations, and in regard to the HIV disease itself—this
stigma has in turn limited both the availability of funding and public support for more extensive HIV
interventions.3
260
19
COMMUNICABLE DISEASES
Who is most impacted?
Anyone of any age, race, sex or sexual orientation can be infected with HIV, but these behavioral and
social risk factors place a person at greater risk of HIV/AIDS:
• Having sex with multiple partners without a condom. A person is at risk whether he/she is
heterosexual, homosexual or bisexual.
• Having unprotected sex with someone who is HIV-positive.
• Having another sexually transmitted disease, such as syphilis, herpes, chlamydia, gonorrhea or
bacterial vaginosis.
• Sharing needles during intravenous drug use.
• Received a blood transfusion or blood products before 1985.
• Having fewer copies of a gene called CCL3L1 that helps fight HIV infection.
• Newborns or nursing infants whose mothers tested positive for HIV but did not receive treatment
also are at high risk.4
Of all racial and ethnic groups, HIV and AIDS have hit African Americans the hardest. Nationally, African
Americans represent 13% of the U.S. population, but account for nearly half (49%) of the people with
HIV and AIDS. The reasons for this disparity are related to some of the social conditions and barriers
faced by many African Americans. These barriers can include poverty, sexually transmitted diseases
and stigma (negative attitudes, beliefs, and actions directed at people living with HIV/AIDS or directed
at people who do things that might put them at risk for HIV).5
In Contra Costa, three priority populations have been identified as being hardest-hit by HIV/AIDS and in
greatest need of HIV prevention support and intervention. These priority populations are African Americans, men who have sex with men (MSM), and injection drug users and persons who share needles.3
What can we do about it?
Prevention of HIV infection remains the key to controlling AIDS in the community. Vital education about
safe sex and the use of condoms in the heterosexual as well as the lesbian, gay, bisexual and transgender (LGBT) communities, and the importance of clean needles, needle exchange and harm reduction
for intravenous drug users, all confront strong cultural and religious barriers that must be addressed
with understanding and persistence. Notification of partners of HIV infected individuals, either directly
or anonymously, helps slow transmission and facilitates early treatment. HIV testing should become
part of routine medical care in private providers offices, in emergency departments of hospitals and
in prenatal visits.
Early identification and evidence-based medical treatment slows the progression of HIV to AIDS, and
helps reduce transmission risk. A variety of care services are available for people with HIV or AIDS. In
addition to nurse case management services for eligible individuals, the Contra Costa Health Services
AIDS Program coordinates and offers referrals to a network of support services including: access to
clinic-based social workers and HIV early intervention services; certification for enrollment in the AIDS
Drug Assistance Program; referrals to community-based (medical) case management services; access
to mental health or substance abuse services; help with accessing housing services; non-criminal legal
261
COMMUNICABLE DISEASES
services; and other practical support such as food and transportation assistance, and other emergency
assistance. Anonymous partner notification services as well as enhanced risk reduction services for HIV
positive individuals are also available.6
The AIDS Program also coordinates a network of HIV prevention services geared to help HIV-negative
individuals remain negative. These services include targeted prevention outreach services, one-to-one
prevention case management services, support groups and workshops, and access to HIV testing. Services
are designed to support individuals in making healthy choices to reduce the risk for transmission of HIV.6
Data Sources: HIV & AIDS
text
1.
2.
3.
4.
5.
6.
Divisions of HIV/AIDS Prevention. (March 22, 2010) Basic Information about HIV and AIDS. National Center for
HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Retrieved July 9, 2010 from the CDC website:
http://www.cdc.gov/hiv/topics/basic/
UNAIDS, WHO (December 2007) 2007 AIDS epidemic update. Retrieved July 9, 2010.
http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf
Contra Costa Health Services, AIDS Program. (2008) Contra Costa County, California Comprehensive HIV
Prevention Plan 2008–2013. Retrieved July 9, 2010 from the CCHS website:
http://cchealth.org/groups/aids/pdf/hiv_plan_2008.pdf
Mayo Foundation for Medical Education and Research. (2010) HIV & AIDS: Risk factors. Retrieved July 9, 2010
from http://www.mayoclinic.com/health/hiv-aids/DS00005/DSECTION=risk-factors
The Centers for Disease Control and Prevention (2007). HIV/AIDS and African Americans. Retrieved July 9, 2010
from http://www.cdc.gov/hiv/topics/aa/index.htm
Contra Costa Health Services (ND) HIV & AIDS. Retrieved July 9, 2010 from the CCHS website:
http://cchealth.org/services/hiv_aids/
Tables 1–8
The Contra Costa data about AIDS diagnoses and deaths and HIV are from the Contra Costa Health Services
Epidemiology, Surveillance and Health Data unit. Any analyses, interpretations or conclusions of the data have been
reached by Community Health Assessment, Planning and Evaluation (CHAPE). Counts fewer than five are not shown in
order to protect anonymity. Rates were not calculated for any group with fewer than 20 cases due to unstable estimates.
Population estimates for Contra Costa and its subpopulations (by age, gender, race/ethnicity, city/census place) for
2005–2007 were provided by the Urban Strategies Council, Oakland, CA. January, 2010. Data sources used to create
these estimates included: Census 2000, Claritas 2009, Association of Bay Area Governments (ABAG) 2009 Projections,
and California Department of Finance Population Estimates for Cities and Counties 2001–2009, with 2000 Benchmark.
California Population estimate for state level rate from the State of California, Department of Finance, E-4 Population
Estimates for Cities, Counties and the State, 2001–2009, with 2000 Benchmark. Sacramento, California, May 2009.
HIV cases reported by name only. An additional 241 non-name code HIV cases are reported in HARS, but are not
included as they have not had HIV testing since April 2006 (when names reporting became law) that would allow them to
be re-ascertained as a named HIV case report.
Figure 1: Data about cumulative AIDS deaths through 2008 are from the Contra Costa Health Services HIV/AIDS
Epidemiology Report, August 2009.
262
COMMUNICABLE DISEASES
additional resources
Many thanks to Contra Costa’s Epidemiology and Surveillance Unit for providing data and select graphics included in this
section.
For more information about HIV and AIDS in Contra Costa, please contact Juan Reardon, MD, MPH, juan.reardon­@­hsd.
cccounty.us, Director, Epidemiology, Surveillance and Health Data Unit, or Martin Lynch by phone at 925-313-6323.
“Contra Costa County HIV/AIDS Epidemiology Report”- August 2009 is available from their website at
http://www.cchealth.org/groups/epidemiology/aids/pdf/2009_hiv_aids_epi_report.pdf
The Centers for Disease Control and Prevention HIV/AIDS information website: http://www.cdc.gov/hiv/
The California Department of Health Services Office of AIDS homepage: http://www.dhs.ca.gov/aids/
263
COMMUNICABLE DISEASES
Sexually Transmitted Diseases (STDs)
Most sexually transmitted diseases occur
among teenagers and young adults.
• Young adults had the highest rates of chlamydia and gonorrhea.
• All the primary and secondary syphilis cases were reported among men.
Chlamydia
From 2005–2007, there were 9,323 cases of chlamydia reported in Contra Costa County. The county
had a lower rate of chlamydia (300.3 per 100,000) than the state (365.2 per 100,000).
In Contra Costa, more than two-thirds of the cases (67.8%) occurred among those 15–24. The greatest
percentage of chlamydia cases was among those 15–19 (35.3%), followed by 20–24 (32.5%), 25–29
(15.6%), 30–34 (6.0%), 35–44 (5.0%), 45 and older (2.3%), 10–14 (1.0%) and 0–9 (0.1%).
The rates of chlamydia followed a similar age pattern to the cases. The rates were significantly higher
among young adults between the ages 15–19 (1,386.6 per 100,000), 20–24 (1,469.5 per 100,000) and
25–29 (862.0 per 100,000) compared to the county overall. The rates were significantly lower than the
county overall among those ages 10–14 (39.6 per 100,000), 35–44 (95.7 per 100,000) and 45 and older
(17.8 per 100,000).
Table 1 Chlamydia cases by age
Contra Costa, 2005–2007
Cases
0–9 years
10–14 years
15–19 years
20–24 years
25–29 years
30–34 years
35–44 years
45 years and older
Total
11
92
3,293
3,026
1,454
557
466
213
9,323
Percent
0.1%
1.0%
35.3%
32.5%
15.6%
6.0%
5.0%
2.3%
100.0%
Rate
NA
39.6**
1,386.6*
1,469.5*
862.0*
293.7
95.7**
17.8**
300.3
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
These are age-specific rates per 100,000 residents.
Total includes cases in which age was not reported.
There were more cases among females (6,977) than males (2,276). Females had a significantly higher
rate of chlamydia (436.6 per 100,000) compared to males (148.7 per 100,000).
264
COMMUNICABLE DISEASES
Table 2 Chlamydia cases by gender
Contra Costa, 2005 –2007
Cases
Females
Males
Total
6,977
2,276
9,323
Percent
74.8%
24.4%
100.0%
Rate
436.6*
148.7
300.3
Total includes cases with gender not reported.
* Significantly higher rate than males.
These are crude rates per 100,000 residents.
Gonorrhea
Rates of gonorrhea were lower than chlamydia. Contra Costa County had a similar rate of gonorrhea
(84.0 per 100,000) compared to the state (88.5 per 100,000). There were 2,607 cases of gonorrhea
reported in Contra Costa from 2005 to 2007.
The largest percentage of cases of gonorrhea in Contra Costa occurred among those 20–24 years of
age (28.5%) and those 15-19 (27.1%), followed by those 25-29 (16.3%), 35–44 (10.2%), 30–34 (8.8%),
45 and above (5.8%) and 10–14 (1.1%).
Young adults also had higher rates of gonorrhea. Those aged 15–19 (297.3 per 100,000), 20–24 (360.8
per 100,000), 25–29 (252.6 per 100,000) and 30–34 (120.7 per 100,000) had significantly higher rates of
gonorrhea than the county overall (84.0 per 100,000). Residents ages 10–14 (12.5 per 100,000), 35–44
(54.4 per 100,000) and 45 and above (12.7 per 100,000) had significantly lower rates than the county.
Table 3 Gonorrhea cases by age
Contra Costa, 2005–2007
Cases
10–14 years
15–19 years
20–24 years
25–29 years
30–34 years
35–44 years
45 years and older
Total
29
706
743
426
229
265
152
2,607
Percent
1.1%
27.1%
28.5%
16.3%
8.8%
10.2%
5.8%
100.0%
Total includes cases with age not reported and for age groups not listed.
* Significantly higher rate than the county overall.
** Significantly lower rate than the county overall.
These are age-specific rates per 100,000 residents.
265
Rate
12.5**
297.3*
360.8*
252.6*
120.7*
54.4**
12.7**
84.0
COMMUNICABLE DISEASES
Between 2005–2007, 1,521 cases of gonorrhea were reported among females and 1,077 cases among
males. The rate among females (95.2 per 100,000) was significantly higher than that of males (70.4
per 100,000).
Table 4 Gonorrhea cases by gender
Contra Costa, 2005 –2007
Cases
Females
Males
Total
1,521
1,077
2,607
Percent
58.3%
41.3%
100.0%
Rate
95.2*
70.4
84.0
Total includes cases with gender not reported.
* Significantly higher rate than males.
These are crude rates per 100,000 residents.
Syphilis
There were 58 cases of primary and secondary syphilis reported in Contra Costa County from 2005–2007.
The rate for Contra Costa County (1.9 per 100,000) was lower than the state’s rate (4.9 per 100,000).
Most of the cases of syphilis (69.0%) occurred among those age 35 and older. All of the syphilis cases
reported during this period occurred among males. Data for 2007 cases indicate that two-thirds of all
syphilis cases occurred among men who have sex with men (MSM), many of whom were co-infected
with HIV.
Table 5 Syphilis cases by age
Contra Costa, 2005 –2007
Cases
20-24 years
25-29 years
30-34 years
35-44 years
45 years and older
Total
5
8
NA
20
20
58
Percent
8.6%
13.8%
NA
34.5%
34.5%
100.0%
Total includes cases for unlisted age groups and age groups with cases not listed.
* Significantly higher rate than the county overall.
These are crude rates per 100,000 residents.
266
Rate
NA
NA
NA
4.1*
1.7
1.9
COMMUNICABLE DISEASES
What are sexually transmitted diseases?
The term sexually transmitted disease (STD) refers to the more than 25 bacterial, parasitic and viral infections acquired by sexual contact. A person can contract sexually transmitted diseases any time he/she has
unprotected sex with a partner who is already infected. The organisms that cause sexually transmitted
diseases may pass from person to person in blood, semen or vaginal fluids or through mucosal contact.1,2
Why are they important?
Sexually transmitted diseases, such as gonorrhea or chlamydia, can often have no symptoms. The
symptoms of several other STDs can be easily mistaken for those of other illnesses delaying a correct
diagnosis. Serious health consequences can result from STDs if left untreated.
If women are infected while pregnant this may harm the health of their unborn children. If left untreated, these diseases can cause debilitating pain, or irreversible damage, destroying a woman’s ability to have children.
There is growing evidence that the presence of other STDs increases the likelihood of both transmitting
and acquiring HIV. Individuals who are infected with STDs are at least two to five times more likely than
uninfected individuals to acquire HIV infection if they are exposed to the virus through sexual contact.
If an HIV-infected individual is also infected with another STD, that person is more likely to transmit HIV
through sexual contact than an HIV-infected individual without another STD. Strong STD prevention, testing
and treatment can play a vital role in comprehensive programs to prevent sexual transmission of HIV.3
Some stds can be cured with a single dose of antibiotics, but some, such as acquired immunodeficiency syndrome (aids) or herpes, are incurable. People with these diseases remain infectious for the
rest of their lives.
Who do they impact most?
A person’s risk of contracting an STD depends on his/her sex, age and sexual practices, as well as on
the sexual practices and lifestyles of potential partners. It’s possible to contract sexually transmitted
diseases from people who seem perfectly healthy and people who aren’t aware of being infected.2
Factors that increase the risk of being infected with a sexually transmitted disease include:
• Having unprotected sex. Vaginal or anal penetration by an infected partner who is not wearing
a latex condom increases the risk of contracting an STD.4
• Having sex while infected with an STD. Being infected with one std makes it much easier to contract
another one.4
• Having multiple sex partners.4
• Other factors that can lead to increased risk of acquiring an STD include using alcohol or recreational
drugs and casual or anonymous sex.4 Alcohol and recreational drug use can make sexual risk-taking
more likely, and casual or anonymous sex can put people at higher risk for exposure to STDs.4
267
COMMUNICABLE DISEASES
Groups that appear to be at higher risk of infection include:
• Almost half of all new STD cases each year are in people between the ages of 15 and 24 years.
In teenage girls and young adult women, the cervix is more vulnerable to trauma and infection.4
• When exposed, women are more likely to get an STD from men than vice versa4 due to differences
in male/female anatomy.
• Men who have sex with men4
• STDs, particularly gonorrhea and syphilis, are reported in a disproportionate number of African
Americans. This may be partly because African Americans are more likely to receive care at clinics that report STD statistics, including breakdowns of cases by age, sex and race. Missing race/
ethnicity information may skew this number.4
• If a person has had one STD, he/she is at increased risk of contracting another one.4 This is partly
because the person may be more likely to engage in behaviors that result in a STD or have sex
with people in social networks in which STDs are more prevalent.4
What can we do about them?
Latex condoms, when used consistently and correctly, are highly effective in preventing sexually transmitted infections, including HIV.5
Individuals at risk for STDs should be offered counseling regarding methods to eliminate or reduce their
risk and testing and treatment so that they can be aware of their status and take steps to protect their
own health and that of their partners.
Partner notification, including partner counseling and referral services (PCRS) with strong linkages to
prevention and treatment/care services is important.
Prevention efforts for high-risk populations, including teens and young adults, are also critical to reducing the spread of STDs.6
Data Sources: Sexually Transmitted Diseases
text
1.
2.
3.
4.
5.
Sexually Transmitted Diseases in California, 2008. California Department of Public Health, std Control Branch,
November 2009.
Mayo Foundation for Medical Education and Research. (2010) Sexually Transmitted Diseases: Definition Retrieved
July 14, 2010 from
http://www.mayoclinic.com/health/sexually-transmitted-diseases-stds/DS01123
Division of std Prevention, National Center for hiv/aids, Viral Hepatitis, std, and tb Prevention. (2010) hiv/aids &
stds. Retrieved July 14, 2010 from the cdc website:
http://www.cdc.gov/std/hiv/default.htm
Mayo Foundation for Medical Education and Research. (2010) Sexually Transmitted Diseases: Risk Factors. Retrieved
July 14, 2010 from
http://www.mayoclinic.com/health/sexually-transmitted-diseases-stds/DS01123/DSECTION=risk-factors
Centers for Disease Control and Prevention. (2008) stds and Pregnancy — cdc Fact Sheet. Retrieved July 14, 2010
from http://www.cdc.gov/std/STDFact-stds&Pregnancy.htm - protect
268
COMMUNICABLE DISEASES
6.
National Center for hiv/aids, Viral Hepatitis, std and tb Prevention. (2006) Components of Comprehensive hiv
Prevention. Retrieved July 16, 2010 from the cdc website: http://www.cdc.gov/hiv/resources/reports/comp_hiv_prev/
components.htm - identifying
Tables 1-5
Source: California Local Health Jurisdiction std Data Summaries for 2005–2007 from the California Department of Public
Health, std Control Branch. Any analyses, interpretations or conclusions of the data have been reached by Community
Health Assessment, Planning and Evaluation (chape).
Counts fewer than five are not shown in order to protect anonymity. Rates were not calculated for any group with fewer
than 20 cases due to unstable estimates.
The data were not presented by race/ethnicity in this report due to missing race/ethnicity data for a large percentage of
reported std cases.
269
Understanding the Data
To get the most out of this report, it is important to understand the measures used and what each can
tell you about the health issues it describes. This report uses totals, percents, prevalence and several
different kinds of rates.
Totals
Totals provide us with numbers and counts. Depending on the topic, the totals might be labeled deaths,
cases, number or children. Totals refer to the number of people experiencing the health issue and give
us an idea about the scope of the problem. Knowing the total number affected can help with decisions
about how to allocate appropriate resources for treatment and prevention. Looking at the totals for
different groups tells us which group has the most cases but not which group is at greatest risk. We
expect to get larger totals for bigger groups but that doesn’t mean they are at greatest risk.
Example: There were 3,465 heart disease deaths among whites in Contra Costa from 2005–2007. There
were 538 heart disease deaths among African Americans during the same period. Even though there
were more deaths among whites, it does not mean they were at greater risk.
Percents
Percents tell us how the totals are distributed across groups. They are a familiar way to compare proportions and they tell us what part of the total number of cases is attributed to each group. Percents
tell us which group has the greatest share of cases but not which group is at greatest risk. We expect
groups that make up a larger part of the total population to have a larger percent of cases but that does
not mean they are at greatest risk.
Example: There were a total of 1,218 lung cancer deaths in Contra Costa between 2005 and 2007.
Whites accounted for 944 of these deaths while African Americans accounted for 120 of the deaths.
The percent of deaths among whites was 77.5% = (944/1,218)*100% and the percent of deaths among
African Americans was 9.9% = (120/1,218)*100%. Since there are more whites in the county we would
expect that more of the county’s lung cancer deaths were among whites but this does not mean whites
are at greatest risk.
Prevalence
Prevalence tells us what percentage of the population is affected by the health problem. Prevalence is
a measure of risk and can be used to compare one group to another. If a higher percentage of people
in one group are affected by a problem compared to another the group, the group with the higher
percentage is said to have a higher prevalence and be at greater risk. Although percent and prevalence
are both reported as a percentage in this report, the percent is the number of cases in a group divided
by the number of cases in the total population while the prevalence is the total cases in a group divided
by the population of that group. In order to calculate prevalence, we must know the total population.
In many cases prevalence is calculated using the number of people surveyed as the total population
and the number who reported they had experienced the health problem or been diagnosed with the
disease as the number affected.
270
Example: The California Health Interview surveyed 1,157 Contra Costa adults in 2007 about various
health outcomes. Of those surveyed 75 reported ever being diagnosed with diabetes. The prevalence for
Contra Costa was calculated to be 6.5% = (75/1,157)*100%. Because they made a similar calculation
for everyone surveyed in California we can compare the prevalence in California (7.8%) to Contra
Costa’s prevalence even though the number of people living in California (and the number of people
surveyed in California) is much larger than those living (and surveyed) in Contra Costa.
Rates
Rates are the best way to compare risk between groups. The most basic rate is calculated by dividing
the number of deaths or cases by the total population at risk. The result is then multiplied by a number
that is standardized by topic area for reporting (typically 1,000 or 100,000 depending on the rarity of
the outcome). Because the rate takes into account the total population at risk, it is a legitimate way to
compare groups of different size.
Example: There were 129 unintentional injury deaths among Hispanics in Contra Costa from 2005 to
2007 and 121 unintentional injury deaths among African Americans in the same period. Although the
total number of deaths is very similar, the number of Hispanics in the county during that period (their
population at risk) is much higher (658,438) than the total number of African Americans in the county
during that period (280,355), so the Hispanic rate of 19.6 per 100,000 residents = (129/658,438)*100,000
is lower than the African American rate of 43.2 per 100,000 residents = (121/280,355)*100,000.
The rate calculated above is the most basic kind of rate and is called a crude rate. It is the easiest to
calculate and does not take into consideration differences in the age distribution of each population.
Crude rates are used for things like injuries and infectious diseases where there is not consistent
relationship between age and risk.
Age-specific rates are crude rates calculated for particular age groups. In this case we divide the
number of cases that occur in a particular age group by the total number of people in that age group.
Sometimes we use these rates to show how risk of a particular outcome changes throughout the life
course by comparing one age group’s age-specific rate to that of another age group. Other times the
health outcome we are measuring only makes sense for a particular age group and we use age-specific
rates to compare that outcome across multiple groups.
Example 1: There were 229 cases of gonorrhea among Contra Costa residents aged 30-34 years and 265
cases among residents aged 35-44 years old. Although the older group had more cases it also covered
more ages. There were just 189,660 residents aged 30-34 years and 486,802 residents aged 35-44 years, so
the age specific rate for 30-34 year olds120.7 per 100,000 population = (229/189,660)*100,000 was higher
than the age-specific rate for 35–44 year olds 54.4 per 100,000 population = (265/486,802)*100,000.
Example 2: There were 1,544 births to Hispanic girls aged 15-19 years old from 2005 to 2007 and 390
births to white girls aged 15-19 years old in the same period. This shows that there were almost four
times as many births to Hispanic teens as white teens, but when you consider that there were just
28,913 Hispanic girls aged 15-19 years and 54,432 white girls the same age you see that the teen birth
271
rate for Hispanics 53.4 per 1,000 teen girls = (1,544/28,913)*1,000 is more than seven times the teen
birth rate for whites 7.2 per 1,000 teen girls = (390/54,432)*1,000.
Age-adjusted rates are used to compare rates of health outcomes that vary consistently with age between
groups that might have a different age distribution. We use age-adjusted rates when comparing rates
for chronic diseases because the risk of these diseases increases strictly with age. If we did not adjust
for age, a group that had a greater number of older people would look like they were at greater risk
than a group with more young people. Age-adjusted rates require a complex calculation that combines
multiple age-specific rates for a group, weighing each age group according to its proportion in another
population chosen as the standard. The resulting rate does not reflect an actual risk in any group but
it does allow us to make a meaningful comparison between groups.
In our county, the Hispanic population tends to be younger than the white population and the male
population tends to be younger than the female population. We can see these effects when we compare
certain age-adjusted rates.
Example: There were 1,436 cases of lung cancer among Contra Costa women from 2003 to 2007 and
1,268 cases of among men in the same period. Although there were more cases in women, the ageadjusted rate was higher for men 59.7 per 100,000 residents than women 52.6 per 100,000 cases because
women are an older population in Contra Costa.
272
Acknowledgements
The Community Health Assessment, Planning and Evaluation (CHAPE) Unit of the Contra Costa
Health Services Public Health Division wished to thank the following individuals for their support
and contribution to this report.
CONTRA COSTA HEALTH SERVICES
Nancy Baer
Andi Bivens
Wendel Brunner, MD
Diane Dooley, MD
Shawn Eyer
Kate Fowlie
Steve Hahn-Smith
Nancy Busby Hill
Erika Jenssen
Michael Kent
Kristina Kutter
Christine Leivermann
Martin Lynch
Fatima Matal Sol
Lorena Martinez-Ochoa
Andrea Menefee
Padmini Parthasarathy
Cheri Pies
Juan Reardon, MD
Tracey Rattray
Oliver Symonds
William Walker, MD
CONTRA COSTA COUNTY
Jennifer June Balogh
Devorah Levine
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH
Lily Chaput
Meredith Milet
Caroline A. Peck, MD
CALIFORNIA CANCER REGISTRY
Mark E. Allen
U.S. CENSUS BUREAU
David Raglin
273