Establishment of a Healthy Human Range for
advertisement

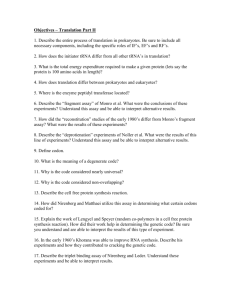
Cytometry Part B (Clinical Cytometry) 00:00–00 (2014) Original Article Establishment of a Healthy Human Range for the Whole Blood “OX40” Assay for the Detection of Antigen-Specific CD41 T Cells by Flow Cytometry Ross Sadler,1 Elizabeth A. L. Bateman,1 Victoria Heath,1 Smita Y. Patel,2 Phillip P. Schwingshackl,1 Alice C. Cullinane,1 Lisa Ayers,1 and Berne L. Ferry1* 1 Department of Immunology, Churchill Hospital, Oxford University Hospitals NHS Trust, Oxford, United Kingdom 2 Department of Clinical Immunology, John Radcliffe Hospital, Oxford University Hospitals NHS Trust, Oxford, United Kingdom Background: Clinical investigation of antigen-specific T cells in potentially immunodeficient patients is an important and often challenging aspect of patient diagnostic work up. Methods for detection of microbial exposure to the T-cell compartment exist but are laborious and time consuming. Recently, a whole blood technique involving flow cytometry and detection of CD25 and OX40 (CD134) expression on the surface of activated CD41 T cells was shown to be accurate and concordant when compared with more traditional methods of antigen-specific T-cell detection. Methods: Whole heparinized blood was collected from healthy donors and set up using the “OX40” assay to detect antigen-specific CD41 T-cell responses to Varicella Zoster Virus, Epstein-Barr Virus (EBV), Cytomegalovirus, Candida albicans, and Streptococcus pneumoniae. Results: The “OX40” assay technique was clinically validated for routine use in an NHS clinical immunology laboratory by analysis of incubation length (40–50 h), sample transport time (up to 24 h at room temperature), concordance with serology testing, proliferation and interferon-gamma production. In addition, 63 healthy controls (age range 21–78) were tested for responses to generate a healthy control reference range. Conclusions: The OX40 assay, as presented in this report, represents an economical, rapid, robust whole blood technique to detect antigen-specific T cells, which is suitable for clinical immunology diagC 2014 International Clinical Cytometry Society nostic laboratory use. V Key words: flow cytometry; costimulation/costimulatory; diagnostics; CD41 T cells How to cite this article: Sadler R, Bateman EAL, Heath V, Patel SY, Schwingshackl PP, Cullinane AC, Ayers L, Ferry BL Establishment of a Healthy Human Range for the Whole Blood “OX40” Assay for the Detection of Antigen-Specific CD41 T Cells by Flow Cytometry. Cytometry Part B 2014;00B: 000–000. Additional Supporting Information may be found in the online version of this article. This report is independent research arising from a Healthcare Scientist Research Fellowship. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute of Health Research or the Department of Health. Ross Sadler contributed to study design, data acquisition (all), and article writing/editing. Elizabeth Bateman contributed to study design, data acquisition (OX40 optimization), and article editing. Victoria Heath contributed to data acquisition (CFSE comparison). Smita Y. Patel contributed to clinical input regarding XIAP patients and article editing. Phillip Schwingshackl contributed to data acquisition (OX40 optimization). Alice Cullinane contributed to data acqusition (serologi- C 2014 International Clinical Cytometry Society V cal comparison). Lisa Ayers contributed to article writing/editing. Berne Ferry contributed to study design and article writing/editing. Correspondence to: Berne Ferry, Department of Immunology, Churchill Hospital, OUH Trust, Oxford, OX3 7LJ, United Kingdom. E-mail: Berne.Ferry@ouh.nhs.uk Grant sponsor: National Institute for Health Research and the Chief Scientific Officer. Received 12 August 2013; Revised 17 December 2013; Accepted 29 January 2014 Published online 00 Month 2014 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/ccc.21165 2 SADLER ET AL. Detection of previous exposure to a pathogen is an important aspect of clinical investigation (1). Traditionally this has been accomplished via two strategies. First, by detection of the pathogen in the subject, this can be carried out by culturing of patient fluid, or more recently by molecular techniques such as quantitative polymerase chain reaction (2). The second approach has been to analyze components of the immune system for their ability to specifically recognize the pathogen in question, this has most commonly been achieved in the clinical environment by serology testing (3) but now includes limited T-cell function detection methods, for example ELISpot assays, for pathogens such as tuberculosis (4). This second approach has the advantage of not only informing the clinician whether the patient has previously been exposed to the pathogen but also can indicate the degree of specific immune response the patient is capable of mounting. Serology has been and will continue to be useful in measuring antibody responses to pathogens (3). However, there is an urgent and increasing need for rapid, robust and accurate clincally validated assays capable of measuring T-cell antigen-specific responses, especially in patients unable to produce antibody or who are on immunoglobulin replacement therapy. Previous work by Zaunders et al. (5) showed a flow cytometric technique for detecting antigen-specific CD41 T cells via upregulation of CD25 and OX40 (CD134) on the surface of the cell after approximately 48 h incubation with antigen. The “OX40” assay exhibited concordance with research methods of antigen-specific T-cell detection such as carboxyfluorescein succinimidyl ester (CFSE) proliferation studies and intracellular cytokine production (5). Further work showed the potential of this assay for the detection of latent TB infection in healthy control cohorts and HIV-infected cohorts and also in detection of Hepatitis C infection (6,7). The potential use for this assay in assessing T-cell functional responses in routine clinical laboratories is wideranging and significant. Currently, no healthy control ranges exist for pathogen-specific responses using this assay. In this study, we have optimized and validated the “OX40” assay for use in a routine clinical laboratory. This optimized assay was tested for its robustness and the effect of sample processing and incubation times with antigen and then used to generate healthy control ranges for pathogenspecific responses to an array of clinically relevant pathogens. This normal range was clinically validated against two patients with a characterized cellular immunodeficiency. METHODS AND MATERIALS Healthy Controls Subjects and X-Linked Inhibitor of Apoptosis Patients For all experiments, including the establishment of normal ranges, healthy controls (n 5 63, median age 5 40 years, range 5 21–78 years, M:F 5 27:36) were consented according to accepted ethics code 11/SC/0184 awarded by the South Berkshire research ethics committee. Heparinized blood of 7 ml and 3 ml of blood for serum collection was taken from each healthy control. Two male patients with X-linked inhibitor of apoptosis (XIAP) immunodeficiency, leading to recurrent severe EpsteinBarr Virus (EBV) infection were also consented according to the ethics code previously. Patients 1 and 2 have been described previously (8). At the time of the study, Patients 1 and 2 were 34 and 31 years of age respectably. Both patients were in good health at the time of sampling and were not suffering from symptomatic signs of EBV infection. All samples were processed within 6 h of venepuncture for all experiments except for the those used to investigation the effect of duration of blood storage. Reagents Phytohemagluttinin (PHA) was obtained from SigmaAldrich (Dorset, UK) and used at 15 mg/ml, Cytomegalovirus (CMV), Varicella Zoster Virus (VZV), EBV, Vero lysate, and human foreskin fibroblast (HFF) lysate were all supplied by Source Bioscience (Nottingham, UK) and used at 2 mg/ml. Candida albicans (Candida) lysate was supplied by Oxford Biosystems (Oxford, UK) and used at 2 mg/ml. Whole ethanol killed Streptococcus pneumoniae used at 1 3 105 cfu/tube was a kind gift from Richard Malley (Boston, Massachusetts). OX40 Assay Heparin blood from each subject was diluted 1:1 with Iscoves modified medium (Sigma-Aldrich) and aliquoted into 500 ml volumes in sterile capped 5 ml polystyrene flow cytometry tubes (BD Bioscience, Oxford, UK). To each relevant sample, 2 mg/ml of antigen or 15 mg/ml of PHA was added. Each assay was run with two negative control tubes which were media only and a cell lysate control (either Vero or HFF; Source Bioscience), run at 2 mg/ ml. After incubation at 37 C 5% CO2 for 42–44 h, samples were vortexed and 100 ml was aliquotted to a new tube. Blood was then stained with the following monoclonal fluorochromes; CD25–FITC, CD134-PE, CD14-PerCP, Viaprobe (7-AAD), CD4-APC, and CD3-PE-Cy7 (BD Bioscience). Samples were incubated for 15 minutes at room temperature before having 1 ml of FACSLyse (BD Bioscience) solution added for 5 minutes. Samples were washed twice with PBS before being fixed with 1% paraformaldehyde and run on a BD FACSCanto II (BD Bioscience). Analysis was carried out using BD FACSDiva software (version 6.1; BD Biosciences). Samples were gated to acquire 30,000 CD3 positive events, which were then negatively gated for CD14 and 7AAD. Quantification of CD31CD41CD251CD1341 events were calculated by setting gate coordinates on the media only sample to equal 0.1% CD31CD41CD251CD1341 events as a percentage of all CD31CD41 events. These coordinates were applied to subsequent antigen tubes to produce a percentage value of CD251CD1341 double positive events. CFSE Proliferation Assay Peripheral blood mononuclear cells (PBMC)s were purified using a lymphoprep gradient (Axis-Shield, Oslo, Norway). PBMCs were counted and diluted to 1 3 106/ ml in RPMI (Sigma-Aldrich) before being stained with Cytometry Part B: Clinical Cytometry CLINICAL VALIDATION OF THE “OX40” ASSAY FOR ANTIGEN-SPECIFC CD41 T CELLS 3 1 mM/ml of CFSE for 15 minutes at 37 C. After incubation, cells were quenched with 10 ml of ice cold RPMI (Sigma-Aldrich) before being spun at 350g for 5 min. This wash step was repeated before adding 200 ml of cells/well. Various antigens were added to wells at concentrations ranging from 0.2 to 1 mg/ml, cells were then incubated for 5 days at 37 C 5% CO2. After this time, cells were washed in 1 ml of PBS at 350g for 5 min before being incubated for 15 minutes at room temperature with CD3-PE-CY7 and CD4-APC (BD Bioscience). After a final wash, cells were acquired on a BD FACScanto II and analyzed. Cells were first gated using CD3 and then by forward/side scatter to capture T cells that showed “blast-like” appearance. Proliferating cells were measured by a decrease in CFSE fluorescence intensity compared to unstimulated control. Concordance was calculated as the percentage of the true positives and true negatives generated by the assay compared to the total number of results generated (true positives 1 true negatives 1 false positives 1 false negatives). Sensitivity values were calculated as the percentage of the true positive results generated by the assay when compared to the total number of true positives 1 false negatives. Specificity values were calculated as the percentage of the true negatives generated by the assay when compared to the total number of true negatives 1 false positives. Serological ELISAs for CMV/EBV/VZV Initial development of the “OX40” assay (5) used a fourcolor system that gated on lymphocytes using forward and side scatter, followed by identification of CD31CD41 cells before measuring CD25 and CD134 expression (Fig. 1Ai). A concern with this original strategy was that using an initial forward/side scatter gate when examining activated cells could lead to some cells that showed increased granularity from their activation being overlooked from analysis. This is highlighted in Figure 1Aii with analysis of a PHA stimulated sample that has been shown with an overly expanded initial gate to show potentially missed events. The importance of using an expanded gate is further shown in Figure 1B where the same sample stimulated with CMV lysate was analyzed with a “compact” lymphocyte gate and an “expanded” lymphocyte gate. Figure 1Bii demonstrates CD251CD1341 CMV-specific T cells were present in the forward/side scatter plot outside the “compact” lymphocyte gate (Fig. 1Bi), leading to different CD251CD1341 T-cell percentages (4.6 vs 5.3%). A concern with using an “expanded” gating strategy was the potential inclusion of either dying cells that would be aberrantly upregulating cell markers or CD14 monocytes that possess large amounts of FC receptors on their surface, leading to nonspecific monoclonal antibody binding. To confront these two potential issues, it was decided that initial gating with a comprehensive CD31 gate should be sufficiently inclusive to include all true T cells followed by an additional negative selection gate using CD14 and the viability marker 7-AAD to help minimize nonspecific cell contamination (Fig. 2A). Detection and quantification of antigen-specific T cells was measured against viral (VZV, EBV, and CMV), fungal (Candida), and bacterial (S. pneumoniae) antigens. These encompassed both pathogens that inhabit perenially and those that are associated with an isolated infection (Fig. 2B). As a further control measure to test the specificity of the response, individuals were tested against lysates of two established cell lines used to propagate the VZV and CMV antigen used in the experiments (Fig. 2B). No individual tested showed a response to either cell line that was >0.1% above the unstimulated control, in addition, increasing concentrations of cell Patient serology to EBV, CMV, VZV, and Candida [immunuglobulin G (IgG)] were measured according to manufacturers instructions (Diasorin, Vercelli, Italy). S. pneumoniae Serotype Testing The quantification of specific IgG to 12 S. pneumoniae serotypes was performed using a multiplex assay. Conjugation of pneumococcal polysaccharide to beads and performing the multiplex assay follows techniques described previously (9–11). Briefly, serotypes 1, 3, 4, 5, 7F, 9V, 18C, 19A, 6B, 14, 19F, and 23F (Statens Serum Institut, Copenhagen, Denmark) were conjugated and coupled onto activated carboxylated beads (Bio-Rad, Hemel Hempstead, UK). Samples were acquired and analyzed on a Bio-Plex-200 machine using Bio-Plex Manager 6.0 software (Bio-Rad) and the quantity of serotypespecific IgG in lg/ml was determined by comparing the mean fluorescent intensity (FI) to a Log-5PL standard curve generated from FI against expected IgG concentration for 89-sf (Food and Drug Administration, MD). Interferon-Gamma Production From Whole Blood Cultures Whole blood stimulated by the OX40 assay (as described previsouly) was removed from the incubator after 42–44 hrs incubation. 200 ml of cell free supernatant was removed from the cultures and immediately stored at 280 C until required. Interferon-gamma (IFNg) concentrations were measured by Luminex assay using a Bio-Plex-200 machine and a human IFN-g kit supplied by Bio-Rad. Analysis was carried out using BioPlex Manager 6.0 software (Bio-Rad). Statistics Statistical analysis was performed using Microsoft Excel and Prism GraphPad version 5 Software (GraphPad Prism, San Diego, CA). Reference ranges were generated by calculating the median, 5th and 95th percentile for each pathogen. For 2 group comparisons, nonparametric Mann-Whitney tests were carried out. Correlation analysis was made using a Spearman Rank test. For all analyses, P < 005 was considered to be statistically significant. Cytometry Part B: Clinical Cytometry RESULTS A CD31 Gate Followed by a Negative Gate to Remove Dying/Dead Cells and CD141 Cells Is Essential to Capture All Relevant Cells While Eliminating Contaminants 4 SADLER ET AL. FIG. 1. (A) Original gating strategy from Zaunder et al. (5) on healthy control blood that has been unstimulated or stimulated with PHA. Initial gating of cells made by gating lymphocyte population using forward and side scatter, PHA stimulated lymphocytes show increased granularity and size requiring a bigger gate to capture lymphocyte population. Black events within gates are CD31CD41CD251OX401 cells. (B) Comparison of different sized initial lymphocyte gates using forward/side scatter on collection of CD31CD41CD251OX401 cells. The gating strategy on a healthy control sample stimulated with CMV was analyzed, first using a compact lymphocyte gate (i) and second using an expanded lymphocyte gate (ii). Black events within gates are CD31CD41CD251OX401 cells. Percentage CD251OX401 cells as a proportion of all CD31 CD41 cells is marked in the quadrant. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] Cytometry Part B: Clinical Cytometry CLINICAL VALIDATION OF THE “OX40” ASSAY FOR ANTIGEN-SPECIFC CD41 T CELLS 5 FIG. 2. New proposed gating strategy for the detection of CD14-7AAD-CD41CD251OX401 T cells. (A) A healthy control sample was left unstimulated or stimulated with PHA. Cells were first gated as CD31 before being gated as CD142 and 7AAD2. These cells were then selected according to CD4 expression and then analyzed for CD25 and OX40 expression. Black cells within gates are CD31CD14-7AAD-CD41CD251OX401 cells. (B) Representative plots of healthy control whole blood stimulated with various pathogens using the strategy outlined in (A). Percentage CD251OX401 cells as a proportion of all CD31 CD41 cells is marked in the quadrant. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] Cytometry Part B: Clinical Cytometry 6 SADLER ET AL. FIG. 3. Concordance of OX40 assay results with CD41 T-cell proliferation by CFSE staining. Representative plots of both OX40 assay responses and CFSE proliferation assay responses in the same individual after stimulation with PHA, VZV, EBV, CMV, or Candida. Values given as percentage CD251OX401 cells in stimulated culture minus value obtained from the same quadrant in the relevant unstimulated control. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] line lysate did not increase the level of CD251CD1341 T cells (n 5 63, data not shown). OX40 Assay Results Are Concordant With Antigen-Specific T-Cell Proliferation Assays To determine the accuracy of the “OX40” assay, parallel assays were setup on the same healthy controls to measure VZV, EBV, CMV, and Candida status (n 5 15) by both the OX40 assay and an antigen-specific CD41 Tcell proliferation assay using CFSE. Although this assay is measuring proliferation rather than activation of CD41 T cells in response to the antigen ie like the OX40 assay, it was preferred to other techniques such as intracellular cytokine staining or ELispot since it captures the entire antigen-specific population rather than one particular cohort such as IFN-g 1 CD41 T cells for example. There was 100% concordance between results generated by the two different assays with all antigens measured, in all individuals both in either detecting the serologically confirmed presence or absence of a particular pathogen. Correlative analysis of levels of proliferating antigenspecific CD41 T cells vs OX401CD251 CD41 T cells for each individual against the selected pathogens showed variable results with significant correlations seen in CMV, EBV, and VZV responses (r 5 0.93, 0.82, and 0.68, respectively, P < 0.001 for all results, data not shown) but not candida (r 5 0.04, data not shown). Figures 3A–3E show the representative OX40 and CFSE proliferation plots of a healthy control that had confirmed VZV1EBV1 CMV2 serology. The 40–50 h Incubation Is Suitable for Consistant Measurements For use in a clinical environment, incubation times must be pragmatic and reproducible with regard to results. To assess incubation timing on individual response variation, time course experiments were performed, measuring PHA and CMV responses in five CMV positive individuals with stimulation times between 40 and 50 h (Fig. 4). The highest variance seen between a 40-h and a 50-h incubation sample in any one individual was 8.5 and 0.9% for PHA and CMV, respectively (Figs. 4A and 4B). Variance for all samples between 40 and 50 h incubation in each individual gave a mean coefficient of variation (CV%) of 9.1 and 12.9% for PHA and CMV, respectively. These CV% values are within an acceptable Cytometry Part B: Clinical Cytometry CLINICAL VALIDATION OF THE “OX40” ASSAY FOR ANTIGEN-SPECIFC CD41 T CELLS 7 FIG. 4. Differences in antigen-specific CD41 T-cell responses depending on incubation time with antigen. Five healthy control whole blood samples were either stimulated with PHA (A) or CMV (B). Samples were stained and processed for detection of CD251OX401 CD41 T cells at 2-h intervals from 40 to 50 h poststimulation. (C) IFN-gamma production from whole blood samples after stimulation with either EBV or CMV. Whole blood from healthy controls was incubated for 42–44 h with either CMV or EBV lysate. Samples were grouped as either both serologically and OX40 assay negative or both positive. Correlations between the amount of IFN-gamma released after each stimulation and OX40 assay result generated in that same individual were also carried out. Identical results (individuals producing 0% OX40 result and 0 pg/ml) are overlaid on the graph. Cytometry Part B: Clinical Cytometry 8 SADLER ET AL. Table 1 Concordance, Sensitivity, and Specificity of OX40 Assay Antigen-Specific CD41 T-Cell Responses With Serology in Healthy Controls Pathogen tested VZV CMV EBV Number of samples False Positives/ true Positives False negatives/ true negatives Concordance (%) Sensitivity (%)/ specificity (%) OX40 assay cutoff determined for positivity 51 55 53 0/48 0/24 1/43 1/2 0/31 2/7 98.0 100.0 94.3 98/100 100/100 96/88 0.4% 0.5% 0.2% CV% for flow cytometric assays on live blood cells indicating that clinical testing using this assay could allow for some flexibility in the incubation times of samples without fear of producing significantly different results. For the remainder of the work in this study, all samples were incubated for between 42 and 44 h as this suited the work flow of the clinical laboratory. Concordance of OX40 Assay Response in Healthy Individuals With Serological Analysis To further confirm the validity of the “OX40” assay for detecting previous antigen exposure, serological analysis in a group of healthy controls was compared with their response against the same pathogens on the “OX40” assay. A cohort of healthy controls was used to test antigen-specific T-cell responses to VZV, EBV, and CMV. Table 1 shows the amount of true positives, false positives, true negatives, false negatives, overall concordance and sensitivity and specificity in the OX40 assay compared with serology using set cutoff percentage values for positivity within each antigen test, using the serological result as the gold standard. CMV was most concordant with 100% concordance to serology, this included both seronegative and seropositive individuals. VZV testing produced 1 discordant result, which was found in a 22 year old female who had contracted chicken pox at the age of 18 months. While serology for VZV was negative, the “OX40” assay response was 0.4%. The median level of VZV response for all healthy controls tested below the age of 25 was 1.3% (n 5 6, data not shown), indicating that this individual produced a relatively low VZV-specific response. EBV concordance was 94.3% with 1 false positive and 2 false negatives. No specific data regarding the infection of these patients could give a reason for these discrepancies. Using these results, OX40 assay cutoffs for positivity could be determined using the lowest recorded responses seen for each antigen (Table 1). As expected, sensitivity and specificity values for each antigen test gave similar results to the concordance values within each antigen, CMV producing the highest values (100% sensitivity and specificity) and EBV the lowest (96% sensitivity and 88% specificity) (Table 1). Serology testing against Candida and S. pneumoniae was also carried out. Since these are organisms that inhabit the human body consistently from a young age, every individual tested produced a serological response. These data were used for all subsequent OX40 assays in new individuals to determine pathogen exposure positivity without carrying out serology. OX40 Assay Responses to CMV and EBV Correlate With Production of IFN-c in Whole Blood Samples To further validate the accuracy of the OX40 assay, a comparison of IFN-g production was made in CMV1 vs CMV2 individuals and EBV1 vs EBV2 individuals as determined by both the OX40 assay and serology. A significant difference in IFN-g production was seen between both CMV1 vs CMV2 and EBV1 vs EBV2 individuals (Fig. 4C). Correlation analysis of the relative frequency of OX401CD251 T cells and the amount of IFN-g produced for each individual showed significant correlation for both EBV and CMV (CMV r 5 0.97, P < 0.0001, EBV r 5 0.8, P < 0.0001 Fig. 4C). These data confirm that OX401 CD251 CD41 T cells can be considered to be activated antigen-specific T cells responding to the specific antigen stimulus. Establishment of a Healthy Human Range for OX40 Responses to PHA, VZV, EBV, CMV, Candida, and S. pneumoniae A total of 63 healthy controls with an age range of 21–78 (median 40 years) were recruited and T-cell antigen specificity to a range of commonly encountered pathogens determined. Data for each respective pathogen response were only included for individuals that showed an OX40 response that was higher than the cutoffs as determined by serological analysis and stated in Table 1. Reference ranges were calculated as the 5th and 95th percentiles (Fig. 5). The data showed that PHA stimulation produced the widest normal range (3.8– 54.1%) and EBV the narrowest (0.2–3.9%). Gender difference analysis of all antigen reference ranges showed no significant differences (data not shown). Correlation analysis of age with specific antigen responses showed a weak positive trend for increased CMV responses with increasing age (r2 5 0.29, P 5 0.006). No other antigen showed a correlation with age. For these reasons, agespecific reference ranges were not calculated at this point in time. OX40 Assay EBV-Specific Responses in Patients With an XIAP Mutation Are Elevated Compared to the Reference Range In order to test the potential clinical utility of having a healthy control reference range for specific pathogens, a pathogen-specific response was measured in patients Cytometry Part B: Clinical Cytometry CLINICAL VALIDATION OF THE “OX40” ASSAY FOR ANTIGEN-SPECIFC CD41 T CELLS 9 FIG. 5. Establishment of healthy control normal ranges for antigen-specific CD41 T cell responses to common pathogens using the OX40 assay. A cohort of 63 health controls was used to generate a normal response range. Samples were all incubated for 42–44 h and data was only used for individuals that showed a positive response to the pathogen as determined by serology (Table 1). Median values and normal range high and low cut-off values, defined as the 5th and 95th percentiles are shown for each plot. with a diagnosed immunodeficiency. Mutations in XIAP result in affected individuals suffering from recurrent EBV infection (12). EBV-specific responses were investigated in two siblings (Patients 1 and 2) with a characterized XIAP mutation (8). The amount of OX401CD251 CD41 T cells generated in both siblings in response to EBV was dramatically raised (23.3 and 20.6% Fig. 6A) compared with the reference range (95th percentile for EBV 5 3.9%) whilst PHA responses and candida responses were within the reference range generated (95th percentile for PHA 5 54.1%, 95th percentile for Candida 5 5.0%; Fig. 6B). Specific comparisons of the patient data with age/sex-matched individuals data from the reference range cohort also showed no distinct differences in PHA and candida responses (Fig. 6B). Further confirmation of a large EBV-specific response in Patient 1 was carried out using a CFSE proliferation assay again showing a raised response of 38.2% [mean EBV response by CFSE proliferation in healthy cohort 5 6.3% (data not shown); Fig. 6A]. Effects of Length of Blood Storage Prior to Assay Setup To determine the optimum time between venepuncture and “setting up” of the OX40 assay, five CMV and EBV seropositive healthy controls were analyzed for their antigen-specific T-cell responses to PHA, CMV and EBV. Blood was used at 6 h of venepuncture, 24 h postvenepuncture or 48 h postvenepuncture. In all experiments blood was incubated with antigen for 42–44 h. Analysis of antigen-specific responses showed that all responses against all antigens (except for one control against EBV) were above/on the lower limit of the reference range after 24 h (Supporting Information Fig. 1). Cytometry Part B: Clinical Cytometry However, the mean CV% produced over the three time points measured for each individual, in all 3 antigen stimulations used, was increased compared to typical interassay variation for flow cytometric data, with EBV responses showing the highest variance (PHA 5 33.5 CV%, CMV 5 34.3 CV%, and EBV 5 84.2 CV%; Supporting Information Fig. 1). This could also in part be due to EBV responses showing the smallest numerical values which can skew CVs to higher values. One control who showed a consistently low PHA response during the generation of the PHA normal range was also tested and this proved to be consistently low, staying below the normal range cutoff (Supporting Information Fig. 1). These results suggest that samples can be left for up to 24 h at room temperature before assay set up if assessing antigen specificity only but not for accurate quantification of antigen-specific response. DISCUSSION Clinical investigations into the presence and extent of antigen-specific T-cell immunity are becoming more important and the need for antigen-specific functional CD4 T-cell assays that can be performed in routine diagnostic clinical laboratories is clear (1). In this report, the OX40 antigen-specific functional CD41 T-cell assay was clinically validated for use in a routine clinical immunology laboratory and the validated assay was used to establish a healthy control normal response range for antigenspecific T-cell responses to five common pathogens. OX40 is a member of the TNF superfamily and is considered a later costimulatory marker, important in the activation and survival of T cells as they under go differentiation from na€ıve to effector memory status from 1 FIG. 6. Investigations into EBV-specific CD41 T cell responses in patients with XIAP defects. (A) Whole blood from two patients with a characterized XIAP defect was stimulated with either PHA, EBV, or Candida for 42–44 h before being run on the OX40 assay. Patient 1 was also tested for CD41 proliferation in response to PHA or EBV. (B) Comparison of % CD251CD1341 CD41T cells generated in response to PHA, EBV or Candida in XIAP patients and in age/sex-matched healthy controls. Dotted line indicates the 95th percentile value from the reference range generated. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] CLINICAL VALIDATION OF THE “OX40” ASSAY FOR ANTIGEN-SPECIFC CD41 T CELLS to 2 days after antigen recognition (13). There is a concern that this assay could be detecting na€ıve CD41 T cells in individuals that are specific for the stimulating antigen rather than pre-existing CD41 T-cell memory. However, this is unlikely for two reasons. First, strong concordance data with serology from this report support the idea that only memory cells are recognising antigen and reacting with upregulation of OX40. Second, incubation of CMV seronegative individuals blood with CMV antigen does not induce OX40 upregulation for at least 8 days (R. Sadler, unpublished observations), suggesting that T-cell antigen-specific responses described in this report were due to pre-existing effector memory T cells. Another potential issue is that the assay quantifies proliferated antigen-specific T cells— exaggerating the true memory compartment of the individual to that antigen. Previous work reported that proliferation of memory T cells began 48 h post second antigen exposure (5), indicating that incubations of approximately 48 h or below were suitable for detecting baseline CD41 T-cell memory levels. Additional optimization and clinical validation of the OX40 assay in the study has shown that a different gating strategy increases confidence in the results generated by the assay. This is particularly important since the level of detection of this assay appeared to be 60.5% in some cases ((5) and this study). Comparisons with a CFSE proliferation assay, an already established Tcell function assay used in clinical immunology laboratories, showed 100% qualitative concordance between the assays in all antigens measured but did not show quantitative correlation when candida responses were analyzed. This was the only antigen measured that did not quantitatively correlate between the two assays and interestingly it was also the only pathogen that can be considered a commensal of humans. This universal exposure of the body to candida could explain the differences seen in proliferation and activation of exposed CD41 T cells. Crucially, for the purposes of logistics of sample processing in the laboratory, studies show that an antigen incubation window can be used between 40 and 50 h, allowing some flexibility when performing the assay. Sample transportation analysis revealed that by delaying assay setup, an accurate qualitative result of exposure to pathogen could still be obtained as long as samples were processed within 24 h. However, quantifiable levels of antigen-specific response were not concordant between stored blood and blood that was <6 h old, indicating that comparison with this healthy control range can only be made when blood is processed within 6 h of venepuncture. In addition, only CMV and EBV responses were analyzed and investigations into the other pathogens chosen here should be carried out. Antigen-specific T-cell responses are currently investigated in a number of ways. MHC-tetramer staining is considered the gold standard for detecting antigenspecific T cells. This technique is predominantly used in CD81 T-cell work and while highly specific and informative, paradoxically the MHC restrictive nature of this Cytometry Part B: Clinical Cytometry 11 technique severely limits who can be measured. In addition, the complex labor required and high consumable costs, together with the paucity of available MHC tetramers makes it difficult to use the technique in routine NHS laboratories. Measurement by antigen-specific CFSE or ELIspot are both possible but require PBMC sorting and extensive optimization to become interpretable. The OX40 assay is a whole blood assay with a minimal setup time before incubation, it allows for both qualitative and quantitative analysis of antigen-specific T cells. Qualitative analysis can be useful in patients with dysgammaglobulinemia or who are on IVIG and therefore are not able to be measured by more established serological methods. Investigations into EBV-specific CD41 T-cell responses in two patients with a mutation in XIAP revealed grossly abnormal levels of antigen-specific OX401CD251CD41 T cells. These raised levels could be a result of the T-cell compartment having to dedicate greater levels of resource to a particular pathogen to compensate for a functional failing in another component of the immune system such as the NK cells or CD81 T cells. These data support the notion that quantifying levels of antigen-specific CD41 T cells using the OX40 assay against particular pathogens can be useful in investigating patients with suspected immunodeficiency. The OX40 assay can only be used to detect antigenspecific CD41 T-cell responses, not CD81 T cells. Analysis of CD81 T cells does not show the same kinetics or accuracy with regards to CD25 and CD134 expression as CD41 T cells (R. Sadler unpublished observations). Further work needs to be carried out to identify a similar technique to the OX40 assay that can work for CD81 T cells. Previous studies phenotypically analysing vaccinia tetramer positive CD8 T cells in vaccinated individuals reveal many candidate markers such as CD38 and HLA-DR (14,15). In summary, this study shows clinical validation and establishment of a healthy human range for the detection of antigen-specific CD41 T-cell responses to a number of common pathogens using the OX40 assay. This allows quick, cheap, whole blood analysis of patient Tcell immunity to aid in immune profiling of patients. ACKNOWLEDGMENTS The authors would like to thank Richard Malley, Department of Epidemiology and Department of Immunology & Infectious Diseases, Harvard School of Public Health, Boston, Massachusetts, for the gift of whole ethanol killed Streptococcus pneumoniae. The authors would also like to acknowledge the staff at the Department of Immunology, Churchill Hospital, Oxford, UK. LITERATURE CITED 1. Abraham RS. Relevance of laboratory testing for the diagnosis of primary immunodeficiencies: A review of case-based examples of selected immunodeficiencies. Clin Mol Allergy 2011;9:6. 2. Mackay IM, Arden KE, Nitsche A. Real-time PCR in virology. Nucleic Acids Res 2002;30:1292–12305. 3. Orange J, Ballow M, Stiehm ER. Use and interpretation of diagnostic vaccination in primary immunodeficiency: A working group report 12 4. 5. 6. 7. 8. 9. SADLER ET AL. of the basic and clinical immunology interest section of the american academy of allergy, asthma and immunology. J Allergy Clin Immunol 2012;130:S1–S24. Lalvani A, Nagvenkar P, Udwadia Z, Pathan AA, Wilkinson KA, Shastri JS, Ewer K, Hill AV, Mehta A, Rodrigues C. Enumeration of T cells specific for RD1-encoded antigens suggests a high prevalence of latent Mycobacterium tuberculosis infection in healthy urban Indians. J Infect Dis 2001;183:469–477. Zaunders JJ, Munier ML, Seddiki N, Pett S, Ip S, Bailey M, Xu Y, Brown K, Dyer WB, Kim M, de Rose R, Kent SJ, Jiang L, Breit SN, Emery S, Cunningham AL, Cooper DA, Kelleher AD. High levels of human antigen-specific CD41 T cells in peripheral blood revealed by stimulated coexpression of CD25 and CD134 (OX40). J Immunol 2009;183:2827–2836. Hsu DC, Zaunders JJ, Plit M, Leeman C, Ip S, Iampornsin T, Pett SL, Bailey M, Amin J, Ubolyam S, Avihingsanon A, Ananworanich J, Ruxrungtham K, Cooper DA, Kelleher AD. A novel assay detecting recall response to Mycobacterium tuberculosis: Comparison with existing assays. Tuberculosis (Edinb) 2012;92:321–327. Keoshkerian E, Helbig K, Beard M, Zaunders J, Seddiki N, Kelleher A, Hampartzoumian T, Zekry A, Lloyd AR. A novel assay for detection of hepatitis C virus-specific effector CD4(1) T cells via co-expression of CD25 and CD134. J Immunol Methods 2012;375:148–158. Rigaud S, Lopez-Granados E, Siberil S, Gloire G, Lambert N, Lenoir C, Synaeve C, Stacey M, Fugger L, Stephan JL, Fischer A, Picard C, Durandy A, Chapel H, Latour S. Human X-linked variable immunodeficiency caused by a hypomorphic mutation in XIAP in association with a rare polymorphism in CD40LG. Blood 2011;118:252–261. Lal G, Balmer P, Stanford E, Martin S, Warrington R, Borrow R. Development and validation of a nonaplex assay for the simultane- 10. 11. 12. 13. 14. 15. ous quantitation of antibodies to nine Streptococcus pneumoniae serotypes. J Immunol Methods 2005; 296:135–147. Whitelegg AM, Birtwistle J, Richter A, Campbell JP, Turner JE, Ahmed TM, Giles LJ, Fellows M, Plant T, Ferraro AJ, Cobbold M, Drayson MT, MacLennan CA. Measurement of antibodies to pneumococcal, meningococcal and haemophilus polysaccharides, and tetanus and diphtheria toxoids using a 19-plexed assay. J Immunol Methods 2012;377:37–46. Pickering JW, Martins TB, Greer RW, Schroder MC, Astill ME, Litwin CM, Hildreth SW, Hill HR. A multiplexed fluorescent microsphere immunoassay for antibodies to pneumococcal capsular polysaccharides. Am J Clin Pathol 2002;117:589–596. Rigaud S, Fondaneche MC, Lambert N, Pasquier B, Mateo V, Soulas P, Galicier L, Le Deist F, Rieux-Laucat F, Revy P, Fischer A, de Saint Basile G, Latour S. XIAP deficiency in humans causes an X-linked lymphoproliferative syndrome. Nature 2006;444:110–114. Gramaglia I, Jember A, Pippig SD, Weinberg AD, Killeen N, Croft M. The OX40 costimulatory receptor determines the development of CD4 memory by regulating primary clonal expansion. J Immunol 2000;165:3043–3050. Precopio ML, Betts MR, Parrino J, Price DA, Gostick E, Ambrozak DR, Asher TE, Douek DC, Harari A, Pantaleo G, Bailer R, Graham BS, Roederer M, Koup RA. Immunization with vaccinia virus induces polyfunctional and phenotypically distinctive CD8(1) T cell responses. J Exp Med 2007;204:1405–1416. Miller JD, van der Most RG, Akondy RS, Glidewell JT, Albott S, Masopust D, Murali-Krishna K, Mahar PL, Edupuganti S, Lalor S, Germon S, Del Rio C, Mulligan MJ, Staprans SI, Altman JD, Feinberg MB, Ahmed R. Human effector and memory CD81 T cell responses to smallpox and yellow fever vaccines. Immunity 2008;28:710–722. Cytometry Part B: Clinical Cytometry