Trust Board Meeting: Wednesday 12 November 2014 TB2014.125 Title
advertisement

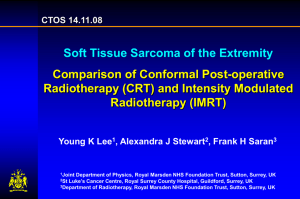
Trust Board Meeting: Wednesday 12 November 2014 TB2014.125 Title Review of Implementation of Expansion of Intensity Modulated Radiotherapy Status For information History Presented to the Trust Management Executive – 13/2/14 Re-presented to the Trust Management Executive with the addition of supplementary information – 9/10/14 Board Leads Key purpose Mr Paul Brennan, Director of Clinical Services Strategy Assurance TB2014.125 - Review of Implementation of Expansion - IMRT Policy Performance Page 1 of 15 Oxford University Hospitals TB2014.125 Executive Summary 1. An implementation review has been undertaken for the Full Business Case for the expansion of Intensity Modulated Radiotherapy. This development was approved by the Trust Board on the 5/7/12. 2. The implementation review confirms that implementation has been fully and successfully completed, delivering the benefits anticipated. A number of issues arose in the in the course of implementation which affected the timescales and approach for delivery e.g. delays in reaching agreement with PFI partners, and recruitment to certain staff groups. These present opportunities for organisational learning and will inform the future development and implementation of business cases. 3. Recommendation The Trust Board is asked to note the contents of this report. TB2014.125 Implementation Review - IMRT Page 2 of 15 Oxford University Hospitals TB2014.125 Implementation Review – Expansion of Intensity Modulated Radiotherapy 1. Purpose 1.1. The Trust undertakes implementation reviews of approved business cases to : • Provide an assessment of the extent to which the objectives and benefits of the case have been achieved within the agreed timescales and financial envelope • Audit the operation of the business case process to ensure that clear criterion for decision–making are explicit in the overall process • Provide assurance that decision making is underpinned by risk assessments which appropriately address clinical, non-clinical and financial risks at a strategic level 1.2. This paper presents an implementation review undertaken for the expansion in the provision of intensity modulated radiotherapy. The business case for this development was approved by the Trust Board on 5/7/12. 2. Expansion of Intensity Modulated Radiotherapy 2.1. Intensity modulated radiotherapy (IMRT) is a form of conformal radiotherapy that uses radiation beams of non-uniform intensity to conform dose to defined tumour volumes, which allows improved targeting of the radiation dose. 2.2. The business case proposed expansion in the provision of IMRT at OUH to ensure that all patients who would benefit from receiving this form of radiotherapy could receive it locally. This would increase access from a level of 30 patients during 2011/12 to 750 patients per annum by 2013/14. 2.3. A phased implementation was proposed, with the sequential development of protocols and implementation of IMRT by tumour site. 2.4. The expansion in the provision of IMRT would realise a number of benefits for the radiotherapy services, namely : • • • • • 3. Ensure the Trust is providing a comprehensive radiotherapy service for patients with cancer. The capacity to deliver IMRT including stereotactic radiotherapy is a measure of clinical excellence. Ensure that the treatment options available to patients minimise short and long term risks to healthy tissue and support the delivery of optimal outcomes. To support the development and delivery of an ambitious programme of cancer research. IMRT is a major focus of the NCRI Clinical and Translational Radiotherapy Research Working Group and the Gray Institute in Oxford. The delivery of key national targets of a minimum of 30% of patients treated with radical radiotherapy receiving inverse planned IMRT by end 2012. Ensure that the Trust continues to remain competitive as a Cancer Centre. Implementation Review 3.1. The implementation review (see Appendix 1) provides an assessment of delivery against : TB2014.125 - Review of Implementation of Expansion - IMRT Page 3 of 15 Oxford University Hospitals • Agreed timescales • The planned manpower requirements • Revenue and capital allocations • Additional income targets • The anticipated benefits that would be realised • Risk management TB2014.125 Any variances from plan are quantified and explained. 4. Conclusions 4.1. The review has confirmed that the expansion in IMRT provision has been successfully implemented, fully delivering the anticipated benefits. 4.2. In the course of implementation, a number of issues did impact more adversely than had been anticipated, namely the timeliness of agreeing the variation with PFI partners and difficulties in recruiting to particular staff groups. The review highlights the importance of early engagement with PFI partners where there is a need to progress building works/equipment installation. Collaboration with the university proved effective with some appointments proceeding on a joint basis e.g. some medical appointments. Similarly appointments in “hard to appoint” staff groups were addressed by making appointments at a lower grade than originally planned and providing training. These issues will be used to inform the future planning and implementation of schemes. 5. Recommendation 5.1. The Trust Board is asked to note the contents of this report. Mr Paul Brennan, Director of Clinical Services October 2014 TB2014.125 Implementation Review - IMRT Page 4 of 15 Oxford University Hospitals TB2014.125 Appendix 1 Implementation Review – Expansion of Intensity Modulated Radiotherapy Business Case Reference TB2012.079 Full Business Case for expansion of Intensity Modulated Radiotherapy Date of Trust Board Approval 5/7/12 Implementation Plan The business case proposed the following timescales for implementation. Please comment on the delivery of these timelines. Business Case approval SOC approved by SPC 9/2/12 Achieved Present Full Business Case to Oncology Directorate/Clinical Director Business case to Surgery and Oncology Division Business case to Strategic Planning Committee Business case to Trust Board Request formal variation enquiry through INC (company overseeing equipment management in PFI), following discussion with suppliers on cost (suppliers have indicated room for negotiation on price) IMRT roll out Pilot prostate intensity modulated radiotherapy (IMRT) completed and breast forward planned IMRT routine Prostate IMRT on-going planning 2 patients per week Gynae IMRT protocol development. Work with Ipswich Start first treatments May 2012 Achieved 13/6/12 Achieved 14/6/12 Achieved 28/6/12 No date set in business case Achieved on 5/7/12. Variation enquiry request completed by directorate Sept 2012. Submitted to INC Jan 2013. Delay due to negotiation on price and submission of variation enquiry by OUH team. October 2011 Pilot prostate IMRT Oct 2010 achieved. Breast forward planned IMRT – Oct 2011 achieved. Achieved April 2012. Increased to ALL prostate cancer Oct 2013. Achieved. Jan 2012 October 2011 – March 2012 June 2012 Head and neck IMRT protocol development. Work with Ipswich Oct 2011 – July 2012 Start first treatment July 2012 TB2014.125 Implementation Review - IMRT Achieved June 2012 – endometrial cancer. More protracted – completed Jan 2013. IMRT lead (RM) appointed Nov 2012 had big effect on roll out thereafter. Delayed - first patient treated Jan Page 5 of 15 Oxford University Hospitals TB2014.125 Implement pancreas IMRT protocol Staff recruitment process following business case approval Start programme for protocol development for other tumour sites. (sarcoma, CNS multiple fraction, lymphoma, oesophagus, paeds) June 2012 Staff appointed, increase to 4 patients per week Programme to install RapidArc on linac 4 (add OBI) then linac 2 (existing OBI) October 2012 Oct 2012 Increase to 6 patients per week Jan 2013 July – Sept 2012 September 2012 TB2014.125 Implementation Review - IMRT 2013. ALL H+N patients treated from April 2013. Delayed due to focus on H+N IMRT – first pancreas patient April 2013 See below. Recruitment extended through to 2013. Programme started and implementation continues. New new tumour sites started as below with protocols in progress: Oesophagus due Feb 2014. CNS stereotactic due to start August 2014. Started 4 pts per week Oct 2012. April 2013 start. Delayed from 201213 due to delay in variation with PFI being agreed. So all installation moved to 2013-14 year. Installation completed Oct 2013. RapidArc commissioning substantially complete (Dec 2013). RapidArc treatment rolled out during Jan – March 2014 to head and neck and prostate cancer. Other tumour sites to follow. The delay in installation of RapidArc by 9 months, has meant that we have had to implement fixed beam IMRT to achieve the national target of 24% of all radical patients (including all H+N cancer patients) by April 2013 which was later adjusted to July 2013. We did achieve this target in June 2013. However have had to implement 16 hours weekend working (Sat and sun am on 2 linacs) to achieve this during the period of equipment upgrade where 1 machine has been constantly out of action for 2013-14 year. RapidArc roll out on Varian 2 and 4 started Feb 2014. Achieved. 29 patients started IMRT in Jan 2013. See graph below. Page 6 of 15 Oxford University Hospitals Start rollout of other tumour sites treatment gradual increase in new starters TB2014.125 April 2013 Install ExacTrac/RapidArc/On April 2013 board imaging (OBI) on linac 6 – installation was completed on linac 5 Roll out all additional tumour sites (anus, stereotactic single fraction CNS, rectum) May 2013 – April 2014 14 patients per week, all tumour sites implemented April 2014 New tumour sites started Inverse IMRT: Breast ca Dec 2012. Lymphoma included in H+N protocol Feb 2013. Unusual sites Sept 13. In addition. We started stereotactic ablative radiotherapy (SABR) stereotactic lung RT (Dec 2012) and stereotactic liver RT (Feb 2013). This was not included in the IMRT business case, but involved considerable technical input. Delay due to moving all of RapidArc and cone beam computed tomography (CBCT) installation into 2013-14. So this machine was put later in programme. OBI and RapidArc installed August 2013. ExacTrac installation completed Feb 2014. But not accepted until 22 May 2014 due to issues around whether OBI link to ExacTrac was included in order or not. (The link was not available when the equipment was ordered). Varian 5 RapidArc commissioning was completed 1 July 2014. Go live for RapidArc on Varian 5 - 7 July 2014. Achieved early: Anal cancer Feb 2013 Rectal ca protocol approved Oct 2013. To start clinical in 2014 with RapidArc. Stereotactic radiosurgery (SRS) August 2014 as outlined above. 140 patients started IMRT treatments Aug – Oct 2013. A rate of 11-12 per week. See graph below. Approximately 50 patients per month are now starting IMRT. (35% of all radical patients) Recruitment The business case described the requirement for the additional staff listed below to support IMRT activity and service growth respectively. The case proposed that TB2014.125 Implementation Review - IMRT Page 7 of 15 Oxford University Hospitals TB2014.125 appointments to the IMRT posts would start in 2012/13 and for growth in 2013/14. Please explain any variances from this plan. Note that the project benefited a lot from the support of university employed staff including Dr Tim Maughan, (Clinical Director) who supported and contributed to the business case and Dr Maria Hawkins (started Nov 2012 as Technical Radiotherapy lead) who contributed to the protocol and technique development within the GI tumour sites. IMRT 10PA Consultant Clinical Oncologist 5PA in 2012-13: sessions 3PA from Nov 2012 : part funded University appointment: RM LGI cancer Oxford 2PA from Nov 2012 : part funded University appointment: SM UGI Oxford 5PA in 2013-14: 1PA from Jan 13 IMRT Lead, RM – early start due to RT Innovation funding. 1PA from Apr13 : Prostate cancer, AS 0.5PA from Apr13 : UGI Cancer: SM 0.5PA from Apr 13 : Lung cancer: NP 1PA from July 13 : Lung and urology: RS new post. 0.5PA to CB (CNS SRT) start August 2014 0.5PA to NW(CNS SRT) start August 2014 1PA Consultant radiology sessions 0.5PA started Jan 2013 (NT) Head and Neck cancer radiology. 0.5PA to start in August 2014 with the Stereotactic Cranial RT service (PP). 0.5WTE Band 8C Physicist – FvdH appointed in 2013. Started Feb Development Lead (plus 0.5WTE 2014. Joint post with university. University of Oxford) 2.0WTE Band 8A Physicist (1.0 2012/13: HW and CH appointed to posts appointed in 2012/13 and 1.0 in conjunction with 0.5 brachytherapy appointed in 2013/14) post. total 1.5 WTE. Started Jan 2013. 2013/14: SP appointed initially to band 7 May 2013 while gaining experience he moved to the full SRT Band 8A post 1st Dec 2013 2.0WTE Band 7 Physicists Unable to recruit registered clinical scientists due to national shortage. JL in post Nov 2013 as Band 6 and moved to registration and Band 7 post in April 2014. EI in post March 2013 as Band 6 and should move to registration and Band 7 post in Dec 2014 1.0WTE Band 6 Dosimetrist A O’N in post Jan 2013 1.0WTE Band 7 Radiographer (CNS Divided into 2 posts jointly with band 7 TB2014.125 Implementation Review - IMRT Page 8 of 15 Oxford University Hospitals SRT and H and N specialist) TB2014.125 existing post funding. SD appointed H+N specialist radiographer – started June 2013. CNS SRT specialist radiographer RW started April 2014. 1.0WTE Band 1.0WTE Band Growth 1.0WTE Band 2.0WTE Band 3 Radiographer helper 4 Clinical Secretary GB started May 2013 CC appointed Sept 2012. 7 Radiographer 6 Radiographer Recruited. During 2013-14 Recruited. During 2013-14 Finance (IMRT and Growth) Revenue The business case proposed additional pay costs of £165k in 2012/13, increasing to £623k for 2013/14 and annually thereafter. Please confirm the additional pay costs for 2012/13 and the additional pay costs for 2013/14. Please comment on any variance from plan. Please confirm budgets for 2014/15. The business case proposed additional non-pay costs of £69k (capital charges) in 2012/13, increasing to £347k in 2013/14. Please confirm the non-pay costs incurred in 2012/13 and the nonpay costs for 2013/14. Please explain any variance from plan. Please confirm the budget for 2014/15. The business case anticipated additional income, over and above the 2011/12 baseline of £31k, of £675k in 2012/13, increasing to £1,649k in 2013/14. Please confirm the additional income delivered in 2012/13 and the additional income for 2013/14. TB2014.125 Implementation Review - IMRT 2012/13 – £115k - £50k lower than planned due to some delays in appointments 2013/14 - £523k - £100k lower than planned due to some delays in appointments. In particular the band 8C physics joint university post started Feb 2014. Budget for 2014/15 is £623k. 2012/13 – no capital charges as equipment installation occurred 2013/14 2013/14 non pay costs: £413k capital charge and depreciation. Mistake in business case. Capital charges on expenditure of £1,555k were included rather than £2,600k. Budget for 2014/15: £413k capital charge. 2012:13 additional income. We planned to deliver 196 courses, and actually delivered 147 courses of IMRT. 2013:14 We planned to deliver 485 courses of IMRT during 2013/14. In fact 463 were delivered. Page 9 of 15 Oxford University Hospitals Please explain any variance from plan. Please confirm budgets for 2014/15. TB2014.125 The additional income was £1,887k. (cf £1,649k in business case) This is related to the higher than expected income for IMRT planning. (£864k due to growth and £1,023k due to delivery of IMRT). Budget for 2014/15 £2,600k looks achievable. Other Revenue Cost Consequences Have any other costs been incurred No as a result of this business case? Capital and Space Requirements Additional capital expenditure of No non-pay expenditure was incurred in £2,651k was approved, with 2012/13. The £69k purchase of QA expenditure of £1,096k planned for equipment was delayed (agreed with Paul 2012/13 and £1,555k expenditure Brennan) from 2012/2013 to match the planned for 2013/14. What delay of the linac upgrades, (more delays expenditure was incurred in than anticipated occurred in the 2012/13 and 2013/14 respectively? procurement process). Please explain any variances from plan. Non-pay Expenditure : 2013-14 £2,134 k to OCHRE. (NO VAT paid) £84.3k for QA equipment – includes VAT. Total: £2,218k The variation from the total expected expenditure of £2,651k is due to the fact that 20% VAT was assumed in the business case, but was not in fact payable. Saving approx. £450k cf business case Have any other capital costs been incurred as a result of this business case? The non-pay upgrade of the linacs has now been completed. No Activity The case anticipated the delivery of the total levels of activity for 2012/13 and 2013/14. Demand for treatment is expected to increase year on year. Please comment on its achievement in 2012/13 and the position for 2013/14. Please confirm the plan for 2014/15. 2012/13 Plan Actual 2013/14 Variance TB2014.125 Implementation Review - IMRT Plan Actual Variance 2014/15 Plan Page 10 of 15 Oxford University Hospitals Fractions SC22,23, SC41Z 1,500 (69005400) ?? IMRT Planning SC40Z, SC41Z Growth Fractions 196 151 44,934 IMRT and Non IMRT Planning 3,715 TB2014.125 6,456 (16056 -9600) Unable to estimate This figure was overestimated 13880 (2488011000) 45 485 490 +5 750 45,270 -336 49,440 48,298 -1,142 50,000 3049 666 3,805 3427 -378 3700 Benefits Realisation The business case proposed the realisation of the following benefits, please comment on their delivery. Benefit Target Timeline Delivery Value Increase portfolio 30% of Due End Oct 2013 – 38.6% of patients of treatment patients to 2012. starting radical RT started inverse options to include receive IMRT Likely to planned IMRT treatments. See IMRT, thus achieve graph demonstrating that this meeting NRAG end 2013. delivery has been sustained target Reduce irradiation 26% End 2013 This is a long term aim. We have of healthy tissues reduction in audited our outcomes in anal and long-term late toxicity cancer pre IMRT and will morbidity as shown in compare post IMRT. clinical trials Increase number 4 End 2013 4 Trials open using IMRT: Arc 2, of IMRT clinical (more in Import High, Neoscope, BR14. trials later years) Financial and Margin of 2014-2015 Stereotactic RT to be Operational 43% in financial implemented in 2014-15. Will viability in the 2013/14 and year increase numbers further 50 SRS long-term 57% in and 35 multiple fraction SRT. 2014/15 Risks The case identified a number of risks to implementation namely : • Downtime in 2012 and 2013 to allow installation and commissioning of additional equipment for RapidArc and ExacTrac hardware/software • Additional staffing not approved • Additional staffing not available to recruit • Forward projection of patient and fraction numbers are too low. Hit capacity TB2014.125 Implementation Review - IMRT Page 11 of 15 Oxford University Hospitals TB2014.125 earlier than envisaged • Forward projection of patient and fraction numbers are too high or commissioners do not commission the actual numbers delivered Of the risks identified, Yes, the delay in installation of RA by 6 months, against did any of them impact our plan. Firstly, the department was unable to start any more significantly than work on RapidArc until the anaesthetic gas pipe work had been anticipated? had been completed in Dec 2012 and then there was a delay in submitting and agreeing variation with INC until Jan 2013 with a start date put back from Oct 2012 to April 213. This has meant that we have had to implement fixed beam IMRT to try and achieve the national target of 24% of all radical patients (including all H+N cancer patients) by April 2013. We did achieve this target in June 2013 and have done since. However have had to implement 16 hours weekend working (Sat and Sun AM on 2 linacs) to achieve this during the period of equipment upgrade where 1 machine has been constantly out of action for 2013-14 year. Additional staffing were approved in a timely manner. Delay in recruiting both physicist and radiographer staff. This is due to nationally recognised shortages in these staff groups. Necessitating appointing 3 of the physics posts below grade and providing training. Clinician appointment did not present any issues due to University joint appointments. Commissioners have funded our planned and actual numbers because RT is now specialist commissioned and funded by case based tariff. Were there any National target 24% to receive IMRT by April 2013 was unanticipated issues introduced in Dec 2012. We met this by June 2013 and that impacted adversely have exceeded this month on month. While the year on on implementation? year increase in demand for radiotherapy was anticipated and planned for, the Milton Keynes patient transfer to OUH during 2013-14, and completely from April 2014 could not have been anticipated. This has meant the requirement for an increase in capacity of an additional 8000 fractions per year more. This has had a significant impact on the delivery of cancer targets. As IMRT ultimately enables patients to be treated more quickly, its implementation has played a key role in the plans to return performance to the required standards (this is especially so for the 31 day target for radiotherapy). Separate business case approved TME 25 June 2014 to expand staff to continue to open 2 machines weekends and run 6th linac full time. Steps have been made to minimise the downtime due to maintenance and QA e.g. maintenance largely TB2014.125 Implementation Review - IMRT Page 12 of 15 Oxford University Hospitals TB2014.125 supported in-house with QA taking place at week-ends. This allows optimal use to be made of all machines within the limitations of the PFI MES contract (linac hours/year). Learning points Please describe any learning points from the implementation of your business case which can be shared with others. Once the business case has been approved. Ensure that the OUH estates team engage with the PFI partners rapidly to ensure that the variation enquiry is approved rapidly so that work can be undertaken. Our project was 7 months behind schedule due to this and the delay in completing anaesthetic gas pipes repair work, and had to employ staff to work weekend overtime for 9 months to compensate for this. But still met the national target of 24% IMRT treatments by June 2013 (target was imposed in December 2012 to start April 2013). With regard to the MES, it is very important to ensure that the clinical teams are rigorous in their evaluation of equipment, particularly where the technology is new to the department. This will ensure that the needs of the service are optimally met. Author: Date: Claire Blesing – Clinical Director Oncology and Haematology 1 December 2013, updated 4 September 2014 following ExacTrac acceptance. Implementation of IMRT The following graph and table demonstrates the increasing levels of cancer treatment that have been delivered by IMRT : % IMRT/ radical for treatments started each month 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Note: National target from April 2013: 24% of radical cases to receive IMRT TB2014.125 Implementation Review - IMRT Page 13 of 15 Oxford University Hospitals Actual IMRT % IMRT/ Radical TB2014.125 Number of Radical Cases New Tumour Sites Jan-12 2 1% 148 Feb-12 7 6% 127 Mar-12 8 6% 130 Apr-12 7 5% 149 May-12 5 4% 139 Jun-12 2 2% 126 Jul-12 10 7% 148 Aug-12 2 2% 136 Sep-12 7 6% 118 Oct-12 18 11% 172 Nov-12 15 10% 147 Dec-12 14 11% 125 Jan-13 29 15% 188 Head and neck cancer Feb-13 19 15% 123 Anal cancer Mar-13 23 17% 134 Apr-13 28 21% 135 May-13 29 22% 131 Jun-13 33 25% 134 Jul-13 50 29% 171 Aug-13 35 22% 157 Sep-13 44 28% 159 Oct-13 61 39% 158 Nov-13 47 33% 141 Dec-13 41 137 Jan-14 Feb-14 Mar-14 Apr-14 May-14 45 55 64 40 30% 28% 33% 35% 39% 26% Jun-14 63 40% 50 Prostate cancer (started as pilot 2010) Endometrial cancer (post op) All prostate cancers Pancreas cancer Rapid Arc signed off V2 and V 4 160 Rapid Arc started for prostate cancer 155 Rapid Arc started for Head and Neck ca 163 151 Rapid Arc go live Varian 5 machine , 159 ExacTrac signed off 153 Acronyms and Abbreviations CNS - Central nervous system CBCT – Cone beam computed tomography IGRT - Image guided radiotherapy, use of on board imaging or portal imaging to verify patient position and guide treatment. IMRT - Intensity modulated radiotherapy Linac - linear accelerator – used to deliver external beam radiotherapy treatment TB2014.125 Implementation Review - IMRT Page 14 of 15 Oxford University Hospitals TB2014.125 OBI - On Board Imaging (kilovoltage and cone beam CT imaging integrated with treatment unit) SABR – Stereotactic ablative radiotherapy TB2014.125 Implementation Review - IMRT Page 15 of 15