Case Report: Glidewear Patch on a unilateral left below the knee amputee... from shear forces

Case Report:
Glidewear Patch on a unilateral left below the knee amputee with ulcer on his distal tibia from shear forces
Charles Kuffel CPO, FAAOP
Kevin L Hines CPO
Patient Demographics:
Age/sex: 69 yrs/male
Primary diagnosis: Left below knee amputee from complications from type 2 diabetes and right charcot neuropathy.
Case Overview:
The referenced patient is a unilateral transtibial amputee.
He presents with type II diabetes with complications resulting in his transtibial amputation on the left side approximately 7 years ago.
Patient has been a full time prosthetic user since shortly after the amputation with a K3 functional level.
He also wears depth inlay diabetic shoes with custom diabetic inserts on the right lower extremity to provide total a total contact protective environment for his remaining at ‐ risk lower extremity.
Patient was fit with transtibial prosthetic socket with gel locking liners.
Patient has returned to normal activities of daily living after fitting and break ‐ in period in his transtibial prosthesis.
Patient has functioned as a full ‐ time wearer at an upper K2/lower K3 functional level since his amputation.
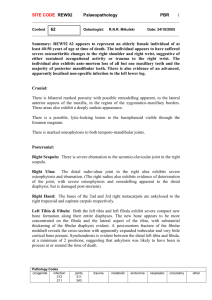
Patients only issue since being fit was consistent skin breakdown over his distal tibia from pressure and shear forces between
patients skin and the gel locking liner.
Treatment Protocol:
Patient’s socket has been fit within the last six months and is total contact with an additional soft pad placed in the area of the anterior tibia due to previous issues with distal tibial skin breakdown.
Normal prosthetic techniques such as pretibial pads and pads built into the socket over the area of pressure were used to try and address the area of concern.
Padding the socket and relieving the area were helpful, but did not provide adequate relief from shear to keep patient from having skin breakdown.
A patch of a shear reducing material was placed between patient’s distal tibia and the locking gel liner.
The material was used to spot reduce the shear forces over patients distal tibia that was causing him to have skin breakdown.
Interface liners are fabricated in a linear fashion but undergo multiple plane disfiguration during dynamic prosthetic use.
This pushing and pulling between the skin, liner, and socket can created areas of shear leading to skin disruption .
The use of the patches has allowed patient to spot reduce shear over his distal tibia.
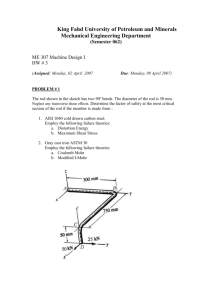
Patient used the distal patches in conjunction with wound application of Medihoney
dressings to speed the healing of the wounds.
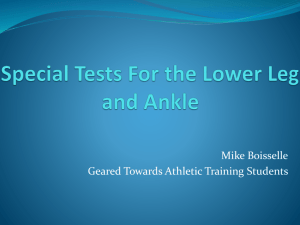
Patient healed his large open area in 6 weeks while continuing use of his prosthesis and has maintained healed status since being fit with the patches.
Ongoing Management:
Mr.
X continues to function as an upper K2/ lower K3 ambulator wearing his prosthesis 12 ‐ 14 hours a day to maintain his activities of daily living.
He uses shear reducing fabric over his distal tibia and underneath his gel liner at all times for shear reduction.
The use of these patches has allowed patient to function at his highest possible level without the incidence of reccurring skin disruption.
Images:
3/22/2013
3/28/2013
4/23/2013