Informing a Business Case to Prevent g Infections Acquired in Acute Care Hospitals
advertisement

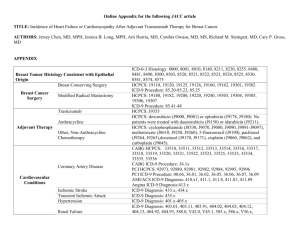
Informing g a Business Case to Prevent Infections Acquired in Acute Care Hospitals Yaozhu ((Juliette)) Chen,, MPA Covance Market Access Services Inc. Acknowledgement • Co-authors – Timothy Dall, MS, The Lewin Group – Erica Moen, BS • Special thanks to – Vestagen Technical Textiles LLC 2 Introduction • Hospital-acquired infections (HAIs) impose a significant health and economic burden – Higher medical costs, reduced quality of life, lost productivity and premature mortality productivity, • A business case model to inform the cost impact of HAIs to hospitals – Perspective: acute-care hospital in the U.S. – Purpose: to estimate HAI HAI-attributed, attributed annual increases in mortality, LOS, and medical costs for both overall inpatient population and selected subsets of sicker patients 3 Model Components • Most prevalent and costly HAIs to be modeled – Device related • Catheter-associated urinary tract infections (CAUTI) • Ventilator-associated pneumonia (VAP) • Bloodstream infections (BLS) – Procedure related • Surgical site infections (SSI) – Pathogen related • Methicillin-resistant Staphylococcus p y aureus ((MRSA)) • Vancomycin-resistant Enterococci (VRE) • Discharges to be included – Of patients who were treated in acute-care hospitals and a few patient subsets who had service experience in several selected ICUs during their hospital stays 4 Model Components Oncology VRE Or al Ca re Ca i rd Catheter Site Care ac o Ne al t a n l PATIENT CAUTI 5 a ic rg re Ca VAP Su in Sk M ed l a ic MRSA SSI BSI Methods – Data Sources & Definitions • Data sources – 2007 Nationwide Inpatient Sample (NIS) linked to the American Hospital Association (AHA) Annual Survey to yield a nationally representative sample of about 5.7 million discharges from nonfederal, acute care hospitals – HAI incidence data ((number of cases p per 1,000 , inpatient p days) y ) from 2006-2007 National Healthcare Safety Network (NHSN) – Apply incidence risks to discharges to generate estimated # of HAI cases • Then, use NIS to estimate HAI attributed increases • Claims data define HAIs and proxies for discharges by care unit – HAIs: apply ICD-9-CM codes to the secondary diagnosis fields and all procedure fields – Discharge proxies by care unit: a combination of diagnoses diagnoses, procedures, and a few other criteria (e.g., age, admission reason, LOS, discharge DRG, etc.) to identify higher-risk patients that were likely received care from ICU 6 Diagnoses and Procedures to Define HAIs Description Code Type Details/Exclusions Source Notes Urinary tract infection (UTI) UTI - related to urinary catheter 996.64 ICD-9 UTI - unspecified 599 ICD-9 Urinary tract infection V13.02 ICD-9 Urinary tract infection of newborn 771.82 ICD-9 Ventilator-associated V til t i t d pneumonia 481 - 486 ICD 9 ICD-9 Mustt have M h procedure d code d 96.72 96 72 (i (i.e., Buczko k W ((2007))97 continuous ventilation for 96 hours) Ventilator-associated pneumonia 997.31 ICD-9 ICD-9 search; Apply codes to secondary fields. Needleman et al Exclude: any primary diagnosis of pneumonia (ICD 480-487, 507.0, 514, (2001) 96; PSI V4.0 997.3); any secondary diagnosis of ICD 480, 481, 483, 484, or 487; MDC4 (respiratory system); AIDS; immunocompromised Needleman et al (2001) 96; PSI V4.0 Apply codes to secondary fields. Exclude: primary diagnosis, MDC 11 (kidney and urinary tract), MDC 12 (male reproductive system), MDC 13 (female reproductive system) MDC Same exclusion criteria as above, except include MDC=15 and exclude age>0. Needleman et al (2001)96 ICD-9 search ICD-9 search Needleman listed sepsis as exclusion criteria; sepsis diagnosis codes were identified through independent ICD-9 search. These two UTI code were not included in the Needleman study - identified through independent ICD9 search (http://icd9cm.chrisendres.com/) Pneumonia Post-operative pneumonia 997.3 ICD-9 Bacterial pneumonia 482 ICD-9 Bronchopneumonia 485 ICD-9 Unspecified pneumonia 486 ICD-9 998.5 ICD-9 Surgical Site Infection (SSI) Postoperative infection Denominator includes patients who had inpatient surgical procedures. Codes apply to secondary diagnosis fields. Exclude: any primary diagnosis of 998.5 and 996.6. Lissovoy 200946; Needleman et al (2001)96; National Hospital Discharge Survey98 997.31 identified through an independent ICD-9 search using icd9cm.chrisendres.com. The code was added to the ICD-9 in FY 2009. Since NIS data is from FY 2007, it does not include this code. Exclusion criteria from Needleman (2001) and the Patient Safety Indicator 4.0 documentation. The pneumonia diagnosis code and exclusion criteria were based on the information provided by the Needleman study. We used the diagnosis codes listed in h P Patient i S Safety f Indicator I di V4.0 V4 0 to id identify if the immunocompromised patients Diagnosis code and exclusion criteria were taken from the Lissovoy and Needleman studies. Analysis was further restricted to only those patients who underwent a surgical procedure. Surgical procedures were flagged using the ICD-9 procedure codes listed in Table 8 of the National Hospital Discharge Survey (Inpatient surgeries). Infection and inflammatory 996.6 reaction due to internal prosthetic device device, implant implant, and graft ICD-9 Denominator includes patients who had inpatient surgical procedures. Exclude: Same as above RTOP-CMS HACPOA Request for Proposals RTOP-CMS HAC-POA RFP included both a diagnosis code and procedure code to identify infection related only to orthopedic surgical procedures. procedures Since we are interested in infection from any surgery, we only included the diagnosis code and did not apply any additional procedure restrictions. Re-admission for postoperative 418 infection DRG Denominator includes patients who had inpatient surgical procedures. Also, 998.5 must be included in diagnoses (any position, including primary code) Lissovoy 200946 The 418 DRG flags for patients who are "Readmitted for Post-Operative and Post-traumatic Infection". With DRG 418, a primary diagnosis of surgical site infection could indicate a hospital-acquired infection. Surgical site infection, mediastinitis, following CABG ICD-9 Denominator includes patients who had inpatient surgical procedures. Al Also, mustt include i l d one off the th following procedure codes: 36.1036.19 RTOP-CMS HACPOA Request for P Proposals l This set of codes only flags for the mediastinitis infection following coronary artery bypass graft. Secondary diagnosis field. Exclude: AHRQ Patient records with a primary diagnosis of Safety Indicator (PSI) V4.0 venous-catheter-related codes (996.63, 999.3, 999.3) and any diagnosis codes for immunocompromised state or cancer Inclusion and exclusion criteria were based on the documentation for the Patient Safety Indicator documentation Version 4.0. Immunocompromised states and cancer were identified using code in the PSI V4.0 Exclude: primary diagnosis of Clodium difficile Schmiedeskamp The ICD-9 code is estimated to have a sensitivity of 78% and specificity of 99.7%. (http://www.cdc.gov/ncidod/Eid/vol12no10/060016.htm) 519.2 (MCC) Bloodstream infections (BSI) Discharge prior to Oct 1, 2007 Due to other vascular device, implant, and graft 996.63 ICD-9 Other infection 999.3 ICD-9 Discharges on or after Oct 1, 2007 Infection due to central venous 999.31 catheter ICD-9 Clostridium difficile difficile-associated associated disease (CDI) Clostridium difficile-associated 8.45 disease ICD-9 200999 Vancomycin Resistant Enterococcus (VRE) Infection with microorganisms resistant to other specified drugs V09.8 ICD-9 Exclude: primary diagnosis of VRE ICD-9 search We identified the VRE code by performing an independent online search at icd9cm.chrisendres.com. Enterococcal infection (not exclusive to resistant strains) 41.04 ICD-9 Exclude: primary diagnosis of VRE Reik 2008100 http://www.princeton.edu/~eklein/pubs/Reik.et.al.20 08.TheBurdenOfVancomycinResistantEnterococcalInfec tions.pdf Methicillin-resistant staphylococcus aureus (MRSA) S. aureus septicemias 7 38.11 S. aureus pneumonias 482.41 Other S. aureus infections 41.11 Infection with microorganisms resistant to penicillins V09.0 ICD-9 Exclude: primary diagnosis of 038.11, Kuehnert 2005101 482.41, and 041.11 ICD-9 Exclude: primary diagnosis of V09.0, Jhung 2009102 038.11, 482.41, and 041.11 Proxy Strategy to Group Discharges by Unit Unit Type Neonatal Cardiac ICD-9 Diagnosis and Procedure Codes Extreme immaturity: ‘765.0'; Gestational age<35 weeks: '765.21' - '765.27'; Birth weight <1,750 g: '764.01' '764.06', '764.11' - '764.16', '764.21' - '764.26', '764.91' '764.96', '765.01' - '765.06', '765.11' - '765.16'; Other conditions requiring NICU admission: '749' '772.1' '772.2' '767.0' '769' '770.6' '770.1' '770.0' 777.5' '756.6' 756.77' '741' 741 '750 750.33' '745 745.22' '770 770.88' '756 Common cardiac conditions requiring CICU admission: 410-417, 420-428, 746; Additional Criteria Median of ICU days Nationwide Children's Hospitals Age=0, Admission type McMaster M M University, U i i Division Di i i off Neonatology 19 days Rhode Island Department of Human Services Embry M. Howell et al. 2002 Apisarnthanarak et al. 2003 Diwas KC, Christian Terwiesch 2007 2 days Common heart surgery procedure codes: 35-37 Legacy Health Flagged if DRG *Range too large: equals 082, 203, 172, Sude KJ, Motl SE, Kuth JC 2006 0-81 days 274, 346, or 010 Oncology Cancer diagnosis codes: '140.00' - '209.29', V10.00 V10.99; Surgical Ope at o s on Operations o various va ous systems: syste s: ‘01.00-16.00’, 0 .00 6.00 , ‘18.008.00 86.00’; Other diagnostic and supporting procedures related to surgery: "00.50", "0051", "0053", "0054", "0055", "0061", "0062", "0063", "0064", "0065", "0066" "0070", "0071", "0072", "0073", "0080", "0081", "0082","0083", "0084" 5 days Critical care procedures: ‘96' '96.7', '99.0', '89.6', '11.0', '96.0', '31.1' ,'99.62','99.15', '36.10' - '36.19' 5 days Medical Source Ri h d ett al. Richards l 2000 The Children's Hospital Al-Rawajfah et al. 2009 Richards et al. 2000 8 Methods – Regression Approach • A series of multivariate regressions to isolate the change in patient outcomes associated with the presence of each HAI – Logistic regression for mortality → increased inpatient death rates associated with each type of HAIs – Generalized Generali ed linear model [GLM] with ith Poisson distrib distribution tion for LOS → increased LOS associated with each type of HAIs – GLM with gamma distribution for medical cost → increased medical costs associated with each type of HAIs • Cost-to-charge ratios were employed, and use CPI medical component to convert cost into 2009 $. • Separate regressions employed – By HAI type – By setting (all inpatient settings together, each selected ICU) • Hierarchical Hi hi l vs. regular l regression i modeling d li – Estimate the impact of explanatory variables at both hospital and discharge level 9 Methods - Controlling Variables • Patient demographics (e.g., age, sex) • Admission type – Elective, newborn, trauma center, urgent, emergency, and other • Payer type – Medicare Medicare, Medicaid Medicaid, private insurer insurer, self pay pay, no charge charge, and other) • Hospital characteristics – Ownership/control Ownership/control, bed size, size urban/rural urban/rural, teaching status status, and Census Region) • A series of indicator variables reflecting if each HAI type is present during the stay (1=present (1=present, 0=absent) • Risk-adjustment variables created based on patient’s primary diagnosis (Dx1) – Average LOS for discharges with the same Dx1 – Average mortality risk for discharges with the same Dx1 – Average e age medical ed ca cost for o d discharges sc a ges with t tthe e sa same e Dx1 10 Estimated Risk for HAI, Medical Cost, LOS, and per HAI Case Death Risk p HAI CAUTI Measure Neonatal Care Unit Surgical Medical All Hospital Settings Risk for HAI 0.40% 0.80% 0.80% $ 83 959 $ 83,959 Medical cost 12 294 12,294 $ 1,846 1 846 $ 1.1 15.0 4.4 Length of stay 0.28% 0.30% 1.58% Mortality risk VAP Risk for HAI 0.20% 0.80% 0.40% $ 64,703 $ 59,686 $ 3,058 $ Medical cost 0.5 18.9 6.3 Length of stay 3.16% 2.85% 5.47% Mortality risk SSI Risk for HAI 0.20% 0.10% NA $ 170,989 $ Medical cost 33,436 NA $ NA 15 6 15.6 86 8.6 L Length h off stay NA 3.49% 2.18% Mortality risk CLABSI Risk for HAI 0.40% 0.70% 0.70% $ 270,840 $ 80,690 $ 6,429 $ Medical cost 32 3.2 19 8 19.8 11 2 11.2 Length of stay <0.01% 2.88% 1.89% Mortality risk VRE Risk for HAI <0.1% 0.10% 0.10% NA $ 225,028 Medical cost $ 4,882 $ 1.3 NA 4.4 Length g of stay y 0.15% NA <0.01% Mortality risk MRSA Risk for HAI 0.10% 0.10% 0.10% $ 129,053 $ 10,075 $ 2,380 $ Medical cost 1.2 33.0 3.3 Length of stay 0 0.40% 40% 2 27% 2.27% 0 76% 0.76% Mortality risk Note: Risk for HAI is the average patient risk for HAI during a stay. Medical cost (in 2009 $), LOS, and mortality risk represent additional burden per case if HAI is present. 11 2.60% 5 347 5,347 2.8 0.96% 1.50% 47,487 4.0 4.62% 0.70% 36,025 89 8.9 2.10% 1.00% 79,960 12 1 12.1 1.70% 0.20% 19,760 3.8 <0.01% 0.30% 10,071 3.5 0 70% 0.70% Strategy to Compare with An Average Hospital • Baseline set-up in the business model – Of an average, average acute acute-care care hospital in 2007 • With work volume of 30,000 inpatient days and 4,700 discharges • Model users can generate estimates – If use default values • For this average-risked hospital, what are the HAI-associated outcomes in form of attributed medical costs, inpatient days, and d premature t d deaths th ffor allll iinpatient ti t settings tti as a whole h l and d by selected ICUs separately – If use customized entries in admission volume and inpatient days • Can get customized results on HAI-attributed outcomes 12 Selected Outcomes from Business Model Outcomes by Type Discharge Outcomes Average discharge volume An Average, Average inpatient days Acute-Care # of HAI Cases per acute-care Hospital hospital with average risk National discharge volume Inpatient days National Total # of HAI Cases of all acute-care hospitals HAI-Attributed Discharge Outcomes Attributed medical costs An Average, Att ib t d iinpatient Attributed ti t d days Acute-Care Hospital Attributed premature mortality Attributed medical costs National Total Attributed inpatient days Attributed premature mortality Discharge by ICU Experience Neonatal Surgical Medical All Hospital Settings 140 1,260 2 170 2,950 8 200 2,530 5 4,700 30,100 181 703,000 6,130,000 8,000 811,000 14,321,000 36,900 972,000 12,295,000 26,500 22,682,000 146,010,000 879,000 $315,000 36 $692,000 126 $45,000 16 $6,782,000 1 134 1,134 0.04 0.6 0.2 4.7 $1 53 billion $3.36 $1.53 $3 36 billion $0 22 billion $0.22 $32 94 billion $32.94 177,000 609,000 80,000 5,506,000 200 2,800 800 23,000 Note: The color highlighted areas are the outcomes relevant to the average, acute-care hospital; in particular, light green areas allow model users to do customized data entry. 13 HAI Prevention • Implementing p g prevention can lead to up to a 70% reduction in HAIs • Challenges HAI Infection H n Rate High Hospital P f Performance Low Higher potential for HAI reduction Average Lo ow Lower potential for HAI reduction High 0% 14 HAI Prevention Potential 100% – As HAIs are reduced,, the cost of detecting each event will become increasingly gyg great – Implementation of interventions designed to move towards the target will require more resources HAI Severity by Acute-Care Hospital 350 Num mber of US A Acute Care H Hospitals 300 250 200 150 100 50 0 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 Hospital Acquired Infections per 1000 Inpatient Days Note: Measured by # of hospitals at different HAI risk level. Source: NIS 2007. 15 39 41 43 Use of This Business Model • Offer hospitals with an easy-to-apply approach to estimate the potential benefits from implementing prevention & control approaches against HAIs • It is a benchmark natured exercise exercise, may not be specific to the unique risks of each hospital • Can be used to estimate potential medical savings • But may under-represent total hospital benefits – Hospital reputation and avoidable litigation costs – Hospital management: bed turnaround time, revenue from reimbursement, isolation cost – Hospital staff: increased work load for hospital staff, i increased d chances h off staff t ff burn-out b t 16 Business Model: Current and Future Versions • Our analysis indicates that opportunities exist for substantial improvements in patient outcomes and h hospital it l performance f th through h effective ff ti HAI prevention ti and control • Based on this model, model hospitals may compare alternative approaches to reduce HAI cases – Compare costs of each prevention approach vs. potential benefits to help reduce red ce the HAI b burden rden • Next steps in model development: continue to build more dynamic y evaluation tools – Budget-impact analysis: to estimate the financial consequences of adopting one or a series of intervention approaches, and measure hospital’s hospital s resource reallocation – Cost-effectiveness analysis: to compare the relative costs and effects of two or more interventions, and can accommodate outcomes like life years gained and QALY 17 Relevance to Hospital Management • Establish greater consistency of HAI-related estimates – Increase reliable estimates of HAIs as economic base for prevention and feasibility assessment • Relate model to hospital Value-Based Purchasing (VBP) plan methodology – Help hospitals implement CMS performance-based payment for hospitals, which include measures of HAI prevention and outcomes as a basis for payment • Multi-modal infection control program needed – – – – Surveillance or monitoring g of incidence Limiting use of invasive procedures and devices Staff training and education Limiting the risk of disease transmission through appropriate hygiene and environmental decontamination – Improve antimicrobial use 18 F further For f th information, i f ti please l contact: t t Yaozhu (Juliette) Chen, yaozhu.chen@covance.come