Dennis P. Scanlon, Ph.D. Jeff Alexander, Ph.D. Laura Bodenschatz, M.S.W.
advertisement

Dennis P. Scanlon, Ph.D.
Jeff Alexander, Ph.D.
Laura Bodenschatz, M.S.W.
AcademyHealth, June 29, 2010
More information regarding AF4Q evaluation team at:
http://www.hhdev.psu.edu/CHCPR/activities/project_alignforce.html
Discuss the limitations, advantages, and utility of
traditional health services research approaches and
the value of mixed methods and realistic evaluation
approaches
Understand the choices and challenges
encountered when conducting rigorous evaluations
◦ We will only scratch the surface in 90 minutes
Provide examples from real evaluations to
emphasize key points
Workshop is pitched at an intermediate level
◦ Assumes graduate level training in research design,
statistics, and multivariate analysis
Training in qualitative research methods is not
assumed
Different approaches to measuring the impact
of a program or policy
◦ How research goals can/should influence research
design
Key Discussion Areas
◦ Program Definition
◦ Research Design Options
◦ Evaluation Implementation
Questions and Discussion
◦ Workshop is interactive – we will pause for
questions/discussion after each section
The Patient Protection and Affordable Care
Act (PPACA) of 2010, provides for several
complex systems changes that will challenge
traditional approaches to research
◦
◦
◦
◦
◦
◦
◦
Accountable Care Organizations (ACOs)
Health Insurance Exchanges
Individual and Employer Mandates
Medicaid Expansions
Meaningful Use of HIT and EHR
National Quality Strategy
Payment Reforms
“For example, the RCT is a powerful, perhaps
unequaled, research design to explore the
efficacy of conceptually neat components of
clinical practice – tests, drugs, and
procedures. For other crucially important
learning purposes, however, it serves less
well.”
Berwick (2008)
“Experimentalists have pursued too singlemindedly the question of whether a [social]
program works at the expense of knowing
why it works.”
Pawson and Tilley (1997)
“Thus, although the OXO model seeks
generalizable knowledge, in that pursuit it
relies on – it depends on – removing most of
the local details about “how” something
works and about the “what” of contexts.”
Berwick (2008)
Did ‘it’ (the program or policy) work?
◦ If so, what was the effect size?
◦ What mechanism(s) led to the effect?
◦ If not, why didn’t it work?
In which context and under what conditions
did it work?
Did the program happen?
◦ What was the dose?
◦ Did it vary across sites/markets and if so why?
Should any changes be made to the program?
Can it be spread? Under what conditions?
What do you want to know?
◦ What are the key outcomes of interest?
◦ How interested are you in the processes and
mechanisms that lead to change?
◦ How important is it to monitor the program or
policy implementation?
Regardless of mandatory or voluntary implementation
What is the theory of change?
◦ By what process or sequence of activities does one
expect the intervention to result in the outcome?
◦ What is the evidence base for the theory of change?
◦ What are the critical assumptions underlying this
theory of change?
Traditional “Difference-in-Difference-inDifference”
◦ Gruber’s study on the labor market incidence of
mandated maternity benefits
Difference-in-Difference analysis
supplemented with a survey
◦ Analysis of a “Hospital Safety Incentive” in an
employed population
Aligning Forces for Quality
◦ A program of the Robert Wood Johnson Foundation
The Incidence of Mandated Maternity
Benefits (Gruber, 1994): DDD Design
Wijt = log real hourly wage of individual i in state j (1 if
experimental and 0 if nonexperimental) in year t (1 if after the
law and 0 if before)
Xijt = vector of observable characteristics
δj = state fixed effect
τt = year fixed effect
TREATi = dummy for treatment group (1 if treatment, 0 if
control)
β2 = time‐series changes in wages
β3 = time‐invariant characteristics of the
experimental states
β4 = time‐invariant characteristics of the treatment
group
β5 = changes over time in the experimental states
β6 = changes over time for the treatment group
nationwide
β7 = time‐invariant characteristics of the treatment
group in the experiment states
β8 = all variation in wages specific to the treatments
(relative to controls) in the experimental states
(relative to the non‐experimentals) in the year
after the law (relative to before the law)
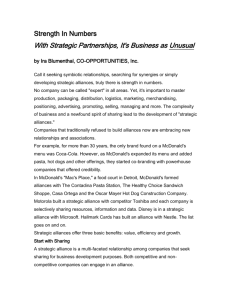
Who Chooses the Hospital?
Factors Influencing Consumer’s Health Care Choices
Factors Influencing Hospital Choice
Quality
Rating
Prior
Experience
Out of
Pocket
Expenses
Physician
Privileges/
Recommendation
Amenities
Hospital
Choice
Reputation/
Recommend
-ation
Travel Time/
Distance
In Health
Plan
Network
Specialty
Services
Factors Influencing Physician Choice
Hospital
Choice
In Health
Plan
Network
Range of
Services
(lab, x-ray)
Reputation/
Recommendation
Physician
Choice
Credentials/
Board
Certification
Quality
Rating
Factors Influencing Health Plan Choice
Travel Time/
Distance
Prior
Experience
Physician Health Plan
Choice
Choice
Hospital
Network
Out of
Pocket
Expenses
Physician
Network
Health
Plan
Choice
Prior
Experience
Quality
Rating
Reputation/
Recommend
-ation
Covered
Benefits/
Services
20 minute phone interviews, pre/post with a random sample
of beneficiaries (employees or spouses)
◦ 4 groups pre and post July 1, 2004
The survey focused on the following areas:
◦ Awareness of enrollment materials and online decision support
tools
◦ Opinions regarding the quality and safety of health care
◦ Factors influencing hospital choice (for respondents with a recent
hospitalization)
◦ Factors important for future choice of hospital if inpatient care is
needed
◦ Factors related to health plan choice
◦ Demographic characteristics
Aligning Forces for Quality?
• An unprecedented commitment by the Robert
Wood Johnson Foundation to implement and
support resources to improve the quality of health
care, reduce disparities related to race and
ethnicity, and provide models for reform.
• Within the 17 different Alliances of AF4Q exist
local stakeholder groups charged with making
sense of the quality problem in America and
meeting it with local solutions.
19
The AF4Q Theory of Change
• Increased transparency
– Inpatient & ambulatory performance
measurement
– Cost & efficiency
– Patient Experience
• Information is being used by:
– Consumers to inform decision making
– Purchasers / employers / plans
– Providers to improve
20
17 Communities Across America
21
The Who – AF4Q Alliances
Albuquerque, NM: Aligning Forces for Quality in Albuquerque
Boston, MA: Greater Boston Aligning Forces for Quality
Central Indiana: Indiana Health Information Exchange
Cincinnati, OH: Health Improvement Collaborative of Greater Cincinnati
Cleveland, OH: Better Health Greater Cleveland
Detroit, MI: Greater Detroit Area Health Council
Humboldt County, CA: Community Health Alliance of Humboldt‐Del Norte
Kansas City, MO: Kansas City Quality Improvement Consortium
Maine: Maine Aligning Forces for Quality
Memphis, TN: Healthy Memphis Common Table
Minnesota: MN Community Measurement
Puget Sound: The Puget Sound Health Alliance
South Central Pennsylvania: Aligning Forces for Quality—South Central PA
West Michigan: Alliance for Health
Western New York: P2 Collaborative of Western New York
Willamette Valley, OR: Oregon Health Care Quality Corporation
Wisconsin: Wisconsin Collaborative for Healthcare Quality
22
The What – AF4Q Areas of Focus
Performance
Measurement
& Public
Reporting
Consumer
Engagement
Quality
Improvement
23
Equity
Targeted
alignment
AF4Q National Program Office:
George Washington University
• The National Program office works in concert
with the Robert Wood Johnson Foundation
• The NPO is responsible for the day-to-day
management and oversight of the AF4Q project.
• Coordinate and deploy technical assistance to
the Alliances for PM/PR, CE, QI, and Equity
24
For More Information
Visit www.rwjf.org/qualityequality/af4q.
25
The“why” of the program
◦ Program goals
◦ Theory of change
◦ Assumptions
◦ Evidence base
The “what” and “how” of the program
◦ Interventions
Degree of standardization
◦ Requirements
◦ Timing
◦ Implementation approach and context
The key actors and their roles
◦ Sponsors, implementers, intermediaries, others
Historical Context and External Environment
Alliance
Development
AF4Q
Community
Alliances
Employers
Labor
Public purchasers
Insurers
Providers
Hospital leadership
Nurse leaders
Publicly funded
healthcare
organizations
Public health experts
Consumers
representing
community
population
AF4Q
Interventions
Consumer
Engagement
Activities
Public Reporting
Initiatives
Quality
Improvement
Initiatives
Alliance
Sustainability
Intermediate
Outcomes
Patient experience
Patient activation
Price & quality
transparency
Provider quality
improvement
Patient safety
Care coordination
Care site transitions
Diffusion of best
practices
Nurse sensitive
outcomes
R/E/L Data Collection
{Performance Data}
Time
Rev 10_9_09
Longer Term
Outcomes
Quality
Improvement
Cost reductions
Improved Health
Status
Reductions in
Disparities
Tracking
◦ Systematic tracking of Alliance activities and relevant health
information and activities in the Alliances’ communities
e.g., availability of public reports, CE activities and state policy
proposals
Key Informant Interviews
◦ In person site visit interviews with multiple stakeholders
◦ Phone interviews
Surveys
◦ Consumer survey
◦ Physician survey
◦ Alliance Survey
Secondary Data
◦ Dartmouth Atlas
◦ H-CAHPS
◦ Area Resource File
Key Informant
Interviews
Key Informant
Interviews
Key Informant
Interviews
Alliance
Survey
Alliance
Survey
Alliance
Survey
Consumer
Survey
Physician
Survey
Secondary Data
Sources
Secondary Data
Sources
Alliance
Tracking
Alliance
Tracking
Alliance
Tracking
Alliance
Tracking
Questions/Discussion
Research Design in Realistic
Evaluation Research
Thinking Outside the O-X-O Box
Focus on “proving” internal validity of
intervention
RCT and QED best suited for discrete
interventions (e.g. drugs, tests, procedures)
Rely on sufficient statistical power to reject
null
Do not tell us much about the mechanism
or process by which change occurs
Controls away (holds constant) the context
of the intervention
•
•
•
•
Things change- traditional designs not
adaptive
Context as intervention- traditional designs
ignore context
The end of the story is not the storytraditional designs not suited to providing
timely results to intervention sites, funders,
and evaluators
Politics of evaluation- traditional designs not
suited to needs and expectations of multiple
stakeholders
Interventions as complex social systemstracking and incorporating change in
evaluation design (intentional and
unintended)
Anticipating change and making appropriate
adjustments
Assessing change to evaluate implementation
Context as a condition for intervention
success or failure
Interaction of context and intervention
Context as a component of the intervention
Separating long term, short term, and
intermediate effects
Being realistic about time required for social
change
Not all research questions require power
calculations
Alternatives when faced with limited power
Compromising understanding of complex
interventions and their effects for the sake of
statistical power
Research Design as Balancing Act
Funders
Intervention sites
National Program office
Other agencies and external groups
Evaluators themselves
Data Collection Decisions
what- outcomes, process, structure, context
when- frequency
level- market/community, intervention site,
individual stakeholder
type- qualitative, survey, secondary
mixin what combination
How will the data be used?
How much will the data cost to collect and
analyze?
How do the data relate to other data
(complimentarity)
How useful/interesting will the data be to
various evaluation stakeholders?
Scaling evaluation
Allocating scarce evaluation resources
Doing realistic evaluation on a limited budget
◦ How much?
◦ How deep?
◦ How often?
Questions/Discussion
Implementing a
Realistic Evaluation of a
Complex Program
Balancing Process and Product
Methods decisions drive team composition
The double whammy
◦ Realistic evaluation often requires specialized skills
across multiple disciplines
◦ Complex programs typically involve various types of
data and points of data collection
Significant time devoted to process with large
and varied teams
The Balancing Act continues
Expect to devote time to developing and
maintaining relationships with multiple
entities and individuals
◦ The Funder and their partners
◦ The intervention sites
◦ The National Program Office and their consultants
The “Are you evaluating…?” question
Expect it
Create a team culture of adaptability
Plan to devote time to
◦
◦
◦
◦
Discussing it
Reviewing research design in light of it
Adapting to it
Documenting it
Mixed methods require collection of both
quantitative & qualitative data
Qualitative methods are resource- and timeintensive
Many team members may be new to
qualitative and mixed methods
Research design provides framework
Understanding context and tracking change
may require more
Many day-to-day decisions
Multiple types of data
◦ Key Informant Interview (KII)
◦ Observations
◦ Project documentation
Challenges of qualitative data in evaluation
◦ Need to move the data quickly
◦ Many people working with the data
Look at existing tools and strategies
◦ Coding
◦ CAQDAS (computer assisted qualitative data
analysis software)
Build or adapt other tools and strategies
Start with the end in mind…what do you need
to know in order to answer your research
questions?
Determine whom (by role, characteristics,
etc.) to interview and when
Communicate with intervention sites early
about interviews; set target dates
Identify specific topics and questions
Develop interview protocol(s) and determine
level of interview structure needed
Make data creation decisions (record and
transcribe interviews, write field notes, etc.)
Create recruitment materials
Gain IRB approval of protocols and
recruitment materials
Test protocols and train interviewers
Work with intervention sites to identify and
schedule specific people who fit your
identified need categories
Conduct interviews
Transcribe interviews and/or write field notes
Develop codebook(s) for the data
Train coders and establish inter-coder
reliability processes
Code data and enter into software program (if
using)
Begin work on first paper/products by
identifying relevant codes and pulling data
KII Data Preparation
Screen Shots
Codebook, coded page
& software output
Multiple Audiences
◦ the Balancing Act continues
◦ Evaluation team itself is the first audience
Multiple or “Layered” findings
◦ Overarching question
◦ Interim results
All in ‘Real Time’
A project supported by the Robert Wood Johnson Foundation
May 12, 2009
Questions/Discussion