Implementation Science and Quality Improvement Research:
advertisement

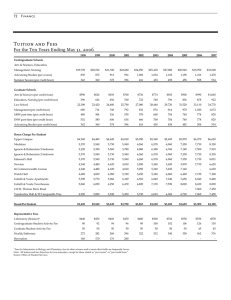
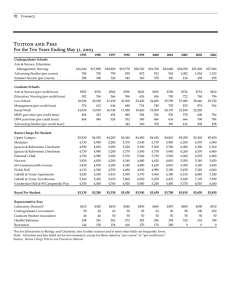
Center for the Study of Healthcare Provider Behavior Implementation Science and Quality Improvement Research: Methods for Translating Research into Practice Approaches to Evaluating QI Interventions Elizabeth M. Yano,, PhD,, MSPH VA Greater Los Angeles HSR&D Center of Excellence UCLA School of Public Health AcademyHealth Chicago, IL June 2009 Overview Approaches to evaluating implementation of QI interventions – Evaluation methods for different stages – Moving from understanding the evidence to national rollout studies Case examples – VA primary i care – Depression collaborative care models (TIDES) Designs for Developing Evidence Base D t t work k under d optimal ti l Does a new ttreatment conditions? Hypothesis-generating, safety studies HypothesisRandomized efficacy trials vs vs. placebo or vs. best available treatment – Patients randomized to studyy arms within each site, provider or clinical practice – Patients selected to reduce complexity – Aim to factor out patient, provider and contextual variables (organizational and area) – Study St d ensures adherence dh to t the th protocol t l Adapted from Rubenstein LV et al. Provider behavior design methods Designs for Developing Evidence Base Randomized Efficacy/Effectiveness Trials Randomized at the patient level – Complex or unselected patient populations – Usual care or unselected providers – Diverse clinical practices or organizations – Treatment is discrete Aim is still to factor out patient and provider variables p Organizational or area context typically not factored in ((or designed g for)) Adapted from Rubenstein LV et al. Provider behavior design methods Methods on the Path to Implementation: B ildi IImplementation l t ti E id Building Evidence Identify the Target Problem – Epidemiological studies – Literature synthesis – Expert panels D fi B Define Bestt P Practices ti – Literature synthesis, meta meta--analysis – Expert panels Adapted from Rubenstein LV et al. Provider behavior design methods Methods on the Path to Implementation: Id tif i T t tP bl &C Identifying Treatment Problems Causes Assess care variations – Epidemiologic designs (e.g., cohort studies) – Quality measurement Assess determinants of care variations – Qualitative Q hypothesis generating – Epidemiologic designs (e.g., cross cross--sectional) – Literature synthesis Adapted from Rubenstein LV et al. Provider behavior design methods Improving Delivery of Efficacious Treatments D Develop l and d ttestt prototype t t interventions i t ti – Literature review regarding variations and d t determinants i t – Literature review on human behavior theories ( ti t & providers), (patient id ) organizational i ti l th theories i Implementation interventions include – Efficacious treatments AND – Improved methods of treatment delivery Adapted from Rubenstein LV et al. Provider behavior design methods Approaches to Early Interventions Aim to test in favorable environments Aim for either the strongest intervention (multi--component black box) or the most (multi feasible E Ensure adherence dh tto protocol t l – Personnel paid for by the study are involved i carrying in i outt th the iintervention t ti att the th local l l level Adapted from Rubenstein LV et al. Provider behavior design methods Formative Evaluations for Early IInterventions t ti Assess ways to improve safety safety, acceptability, feasibility – Qualitative Q lit ti d data t on iimplementation l t ti – Qualitative improvement (e.g. industrial QI), demonstration project design – Monitoring outcomes, possible adverse effects for each patient Adapted from Rubenstein LV et al. Provider behavior design methods Effectiveness Evaluations for Early IInterventions t ti Assess program effects on process and outcomes – Randomized quasi quasi--experiments or rigorous pre--post designs pre Randomize patients within providers if possible Qualitative data – Measure intervention fidelity Quantitative data – Outcome, O t process, subgroups, b costs t Adapted from Rubenstein LV et al. Provider behavior design methods Develop Intervention Implementation St t i Strategies Are there still quality deficits/need for QI? What are the best interventions? – Meta Meta--analysis, metameta-regression – Expert panels – Marketing approaches What groups can be approached for implementation? – Diverse clinical practices within similar types of organizations ideal Adapted from Rubenstein LV et al. Provider behavior design methods Evaluate Effectiveness of Intervention IImplementation l t ti Policy evaluation – Pre Pre--post – Natural experiments – Large Large--scale demonstrations E g Medicare E.g., Adapted from Rubenstein LV et al. Provider behavior design methods Features of Encouragement Designs Randomized encouragement designs – Randomized at the provider or organizational levels – Intervention is implemented p by y organizations g or providers themselves, without direct action by study – Minimal study dollars to support the intervention – Qualitative Q lit ti data d t on fidelity, fid lit organizational i ti l variables i bl Encouragement approaches have variation in implementation by design Adapted from Rubenstein LV et al. Provider behavior design methods Desirable Features for Encouragement D i Designs Maximize the number of intervention vs. control sites Evaluate the effect of the program on random i di id l entering individuals i the h practice i – Weighting and imputation – ? Identify program patients to the practice Document training, materials, intervention adherence Propensity score approaches Source: Yano, et al. The evolution of changes in primary care delivery underlying transformation. Am J Public Health, 2007;97(12):2151-2159. Adapted VA’s from quality Rubenstein LV et al. Provider behavior design methods After Encouragement, IInstitutionalization tit ti li ti Ability to involve all relevant stakeholders – Informatics – Human resources management – Ongoing education and training resources – Provider Pro ider behavior beha ior ssupport pport Ability to sustain intervention financially – Reimbursement policy Ability to ensure ongoing QI/adaptation – Performance measures, changing evidence Adapted from Rubenstein LV et al. Provider behavior design methods Evolving ResearchResearch-Clinical Partnership From researcherresearcher-control to control of others – Need for tools to support pp their control and “ownership” in ways that support fidelity – Need for processes/procedures for ongoing adaptation d t ti (but (b t within ithi view i off evidence id b base)) – Need for tools/materials to orient new team members new leaders members, Need for ongoing consultation as evidence changes new challenges emerge changes, Case Example: VA Primary Care VA historically hospitalhospitalbased specialty oriented Reputation p for p poor care Institute of Medicine panel – What to do with the VA… Clinton health care reform – VA “wake“wake-up p call” Case Example: VA Primary Care Identify the target problem – Surveyed VA outpatient/primary care programs Virtuallyy no primary p y care Walk--in clinics, charts rarely available, very long Walk waits, limited generalist staffing, no teams D fi b Define bestt practices ti – Literature synthesis showing primary care models features associated with quality models, – Policy directive to implement primary care based on evidence ((e.g., g , teams)) Sources: Rubenstein et al., VA Survey of Outpatient Services (1993); Yano et al., Arch Internal Med (1995); VA Primary Care Directive (1994). Case Example: VA Primary Care Assess care variations – Measured adoption of primary care models and features via organizational survey – VA primary care quality measures collected through chart review and patient surveys Chronic disease quality, preventive practice Patient ratings of access, continuity, coordination Sources: Soban & Yano J Ambul Care Manage (2005); Jackson et al., Am J Managed Care (2002); Yano et al., HSR (2008). Case Example: VA Primary Care Assess determinants of care variations – Site visits of early adopters – Cross Cross--sectional studies of differences by urban/rural, academic vs. not, by gender Develop and test prototype interventions – Consensus development conference to identify optimal primary care model – Pilot model demonstration project Sources: Weeks et al., J Rural Health, 2002; Yano et al., Women’s Health Issues, 2003; Goldzweig et al., Am J Manage Care (2004); Rubenstein et al., Acad Med 1995. Case Example: VA Primary Care Identify successful model characteristics – Cross Cross--sectional analyses of effectiveness of different primary care models and features Monitor implementation (“fidelity”) – Ongoing organizational surveys assessing changes in primary care delivery over time Sources: VA Survey of Primary Care Practices (1999-2000); VA Clinical Practice Organizational Survey (2007), VA Primary Care Survey (2009). Case Example: VA Primary Care Patient--centered medical homes (PCMH) Patient – Consensus development meetings – Demonstration project(s) – Literature synthesis A Assess care variations i ti and dd determinants t i t – Assess level of PCMH implementation – Area and organizational factors related to PCMH implementation Evolution of VA Primary Care Delivery Percent of VAs w/PC Program 100 90 80 PC budget PC-based QI Pt-PCP assignment PC teams PC Teams Pt assignment i t 70 60 PC-based QI 50 40 Separate PC budget 30 20 10 0 1993 1996 1999 Source: Yano, et al. The evolution of changes in primary care delivery underlying VA’s quality transformation. Am J Public Health, 2007;97(12):2151-2159. Primary Care Features Associated with Diff lit Differences iin Q Quality Colorectal cancer screening rates – Sufficiency of resources for clinical support arrangements, practice autonomy, size Breast and cervical cancer screening rates – Better in VAs with stronger PCPC-subspecialist coordination di ti (timely (ti l consultlt results) lt ) – Worse in VAs with strict PC assignment – Better in VAs with women’s women s health clinics Diabetic control (HbA1c) – Better in VAs with chronic care model components Sources: Yano, et al. (2006); Jackson, Yano, et al (2004); Goldzweig, Yano, et al. (2004). Case Example: Depression Identify target problem – Epidemiologic studies on prevalence, impact of depression and location in primary care Define best practices (guidelines) – Literature synthesis/meta synthesis/meta--analysis showing CBT and antidepressants equally effective – Expert panel methods to develop guidelines Adapted from Rubenstein LV et al. Application of QUERI evaluation methods. Case Example: Depression Assess care variations – Quality measures based on medical record and survey – Worse care for minorities, managed care identified in large studies Develop intervention models and evaluate effectiveness – Provider behavior and QI theory for design – Randomized trials of collaborative care Adapted from Rubenstein LV et al. Application of QUERI evaluation methods. Case Example: Depression C Collaborative C Care Identify successful model characteristics and develop implementation models – Qualitative research on models models, organizations organizations, predictors of success and barriers – Quasi Quasi--experiments based on diffusion diffusion, provider behavior change, and QI theory – Literature synthesis and metameta-analysis Adapted from Rubenstein LV et al. Application of QUERI evaluation methods. Case Example: Depression C Collaborative C Care Identify successful implementation models, implement as routine policies/procedures – Quality improvement theories used to engage organizations and their leaders – Quality Qua ty improvement p o e e t type measurement easu e e t – Qualitative research on organizations/models – Policy analysis and theory to understand/foster policy uptake, incentive changes for spread Evaluate system performance measures Adapted from Rubenstein LV et al. Application of QUERI evaluation methods. VA ResearchResearch-to to--Practice Implementation: Trajectory j y Toward National Rollout Depression Collaborative Care Model TIDES WAVES Process Evaluation Outcomes Evaluation 20+ year evidence base (efficacy/effectiveness) Single and multi-component interventions Multiple settings COVES Cost Assessment Stakeholder Analysis Formative Evaluation ReTIDES Impact evaluation Cost-effectiveness National “bridge” interviews Process tools DESIGN PROGRESSION Building a Clinical-Research Partnership National Rollout Ongoing Performance Monitoring PHQ--9 Score Baseline to 24 PHQ Weeks 14 12 10 8 6 4 2 0 Baseline 4-6 wk 8-12 wk 16 wk 20 wk 24 wk Q lit ti E l ti Qualitative Evaluation Semi--structured interviews during field visits Semi – Regional (VISN) and medical center managers – Providers, Providers administrators administrators, and consumers – Focused on perspectives on the care model and the implementation process Documentation of process, timeline, and costs associated with adaptation and implementation Source: Kirchner J, Liu C-F, Parker LE, Ritchie M, Fickel JJ, Yano EM. Cost and value evaluation (COVES). Costs of Implementation Broad range of involvement for both researcher consultants and participating VISNs/sites – 128 persons contributed 3,764 hours with a total cost of $296,346 over 4 years Partner p People Hours Cost VISNs/Sites 86 1,190 $83,581 Researchers 42 2,573 $212,765 Data sources: Project records, ~20,000 project emails, personnel survey. Source: Liu, Rubenstein, et al. HSR 2009. PC C Provider o de Penetration e e a o % PCPs Started 1st 6 Months Referrals/PCP FTEs 100 30 % PCPs Started Consults/FTE 90 25 80 70 20 60 50 15 40 10 30 20 5 10 0 0 A1 A2 Network #1 B1 B2 Network #2 B3 C1 C2 Network #3 Evaluating Variable Implementation Study designs need to account for variable implementation (designed & unintentional) Be cognizant of SQUIRE guidelines Data sources include patients, providers, managers and d the th iintervention t ti tteam Track organizational outputs (time, costs) Analysis needs to be at multiple levels – Implementation measures should map to them Triangulation across data sources key