Bridges to Excellence Engaged Purchaser Beliefs From the Employer – Purchaser Perspective
advertisement

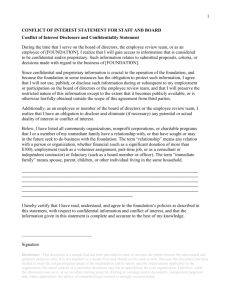
Bridges to Excellence From the Employer – Purchaser Perspective National Health Policy Conference Dale Whitney UPS Health & Welfare Manager Bridges to Excellence Executive Committee A RWJ Foundation Grantee Engaged Purchaser Beliefs 1. Effectiveness and efficiency must improve dramatically 2. We must transform the health care supply chain into a consumer driven market 3. Health care efficiency and effectiveness can be improved using the same tools (IT & continuous process improvement) we use to improve quality and productivity in our businesses. 4. Purchasers and consumers will reward providers demonstrating the greatest effectiveness and efficiency 5. Purchaser, consumer, provider and health plan incentives must be aligned. Bridges To Excellence, Proprietary & Confidential 1 6. Buying Effectiveness and Efficiency Costs Less LOW Efficiency • No standardization in measures • No business case for quality Provider universe today Provider universe tomorrow HIGH LOW Effectiveness of Care HIGH To move the market, we need to find and reward the most effective, highest quality providers while engaging consumers. Bridges To Excellence, Proprietary & Confidential Program Fundamentals Pay rewards AFTER physicians have demonstrated high performance Encourage employees to seek better performers; create incentives for better self-care Pick performance measures that change practice patterns and yield better, safer care Keep pushing for tougher standards Keep demanding complete accountability for use of resources and delivery of outcomes Bridges To Excellence, Proprietary & Confidential 2 BTE: Initial Markets and Programs Cincinnati, OH / Louisville, KY Boston Albany / Schenectady Launch Date June 2003 January 2004 March 2004 Program(s) Diabetes Care Link Diabetes Care Link Cardiac Care Link Diabetes Care Link Cardiac Care Link Physician Office Link # of Employers 6: GE, Ford, UPS, P&G, Humana, CCHMC 4: GE, Raytheon, Verizon, Fidelity, IBM 3: GE, Hannaford Bros, Verizon # of Plans 6: Humana, Aetna, UHC, Anthem, BCBS(2) 5: Tufts, Harvard, BCBS (2), UHC 5: Anthem, MVP, CDPHP, BCBS, UHC # of Covered Lives 180,000 (7,000 Diabetes) 100,000 (3,000 Diabetes) 50,000 (1,500 Diabetes; 2,000 Cardiac) Bridges To Excellence, Proprietary & Confidential We’ve Made Great Progress in Our Pilot Markets Jan 2004 Recognized Physicians Dec 2004 PPC 30 465 DPRP 60 335 DPRP 1,655 PPC 8,041 Employees going to recognized Physicians Rewards paid to-date $964K Available Rewards $8MM Bridges To Excellence, Proprietary & Confidential 3 Lessons Learned in each market will help us in all future markets Louisville – small independent practices need the most hand holding…even when they have a lot of rewards available. Cincinnati – using third party chart extractors is a powerful way to reduce barriers to reporting. Boston – engaging large groups and “train the trainer” approach led to rapid program uptake. Albany – most IPAs welcome the business case and rewards that this program brings them to help their members needed investments. Bridges To Excellence, Proprietary & Confidential Louisville market presents the most opportunity to learn At launch: 4 recognized physicians, today 11 The Challenge: Physician Philosophy – driven regionally Outside of Norton Healthcare, physicians are not organized into large practices/systems, limited resources Single product market – 63k lives = 3500 diabetics The Lessons: Need both a push and pull approach Basic outreach & follow up doubled patient percentage (4% to 8.4%) Extraction services supported by grants has increased pipeline to 20-30 physicians for DPRP Public support from multiple sources – all pushing for the same thing Physicians are learning what constitutes guideline care and receiving the tools to support it in lieu of EMR to get them there Patients need to get in the game through incentives Bridges To Excellence, Proprietary & Confidential 4 Creating The Push By Engaging Employees PCP switch incentives Physician Report Card demo 2005: Launch Quality Ratings tool company-wide Our Challenge: how to integrate w/ other sources of information that exists, including plan-based. Targeted and expected patient redemption of 5% to 10% Primary impact could be to move docs not yet recognized off fence through potential market share loss (Prospect theory) Incentives are measurable Patient incentive use evaluated by market Bridges To Excellence, Proprietary & Confidential Our Efforts Have Been Incorporated in Other National Initiatives CMS – we’re working with CMS on three of its demos: CMP, DOQ, DOQ-IT to make sure that our performance measures are synched up BTE and CMS will be jointly implementing incentives in MA and Arkansas (through a local NBCH coalition), and possibly Utah National Business Coalition – four sites in 2005 with more to follow Health Plans UHC has licensed BTE and will offer it in select markets to its customers. CIGNA and Aetna have agreed to incorporate BTE measures in their High Performance Network products CareFirst BCBS has just announced a BTE rollout BCBS Association and several local plans have shown interest Bridges To Excellence, Proprietary & Confidential 5 Additional Interest In Nearly 30 Markets Market Programs Peoria, IL Quincy, IL Denver, CO Fort Smith, AK Baltimore/ DC/ VA Minnesota New York North Carolina South Carolina Utah Iowa Omaha, NE New Jersey DCL CCL DCL Physician POL Physician Physician Physician Physician Physician Physician Physician TBD All All All All All All All All Dallas Northern CA TBD TBD Market RPs RPs RPs RPs RPs RPs RPs RPs Milwaukee, WI Chicago, Il Maine Seattle, WA Kansas City, MO Memphis, TN Las Vegas Madison, WI Hawaii Tampa, FL Miami, FL St. Louis, MO Dayton, OH Houston Programs All Physician RPs All Physician RPs All Physician RPs LHRP All Physician RPs LHRP All Physician RPs All Physician RPs TBD TBD TBD TBD TBD TBD Bridges To Excellence, Proprietary & Confidential Program Success Factors Critical mass re: employer participation (covered lives) in specific markets – nearly 10,000 participating patients Active employer and health plan participation in each market – 11 large employers in 4 markets, 5+ new markets in 2005, United Health Group first BTE managed care licensee. Buy-in by physician community – from 90 to over 800 new participating physicians in 2004 Bridges To Excellence, Proprietary & Confidential 6 We’re Continuing A Rigorous Evaluation What we know: DPRP docs are more efficient, by 15% when looking at diabetes costs alone, by 5% when looking at overall costs The first year gross diabetic care cost savings per patient is about $250 Additional savings in disabiliity reduction and productivity gains What we don’t know: Are POL docs more efficient? We’re getting the answer from two sources: • • Ingenix – working with Tufts CFP - aggregated data in MA Are DPRP docs more efficient over time? We’re also getting the answer from two sources: • Ingenix & CFP data Bridges To Excellence, Proprietary & Confidential Preliminary Data Confirm Savings for Recognized Physicians Diabetes Costs Only All Costs $7,500 $1,650 $1,600 $7,300 $1,550 $1,500 $7,100 $1,450 $6,900 $1,400 $1,350 $6,700 $1,300 $6,500 $1,250 Diabetes Costs Only Non-recognized Physicians Recognized Physicians All Costs Non-recognized Physicians Recognized Physicians Bridges To Excellence, Proprietary & Confidential 7 Our Future Focus 2005 All Docs 2006 2007 PPC version 2.0 + Patient Experience of Care PCPs (IM, FP, Gyn, Ped, etc.) PCP Recognition Program Ortho & Rheum MSK RP Oncologists Cancer RP Bridges To Excellence, Proprietary & Confidential Contacts and Additional Information Additional program information: www.bridgestoexcellence.org Bridges To Excellence, Proprietary & Confidential 8 Appendix Bridges To Excellence, Proprietary & Confidential Summary Of Rewards For Related Programs Program Measures Business Case Reward CMS – Physician Group Practice demonstration Selected HEDIS measures (A1c, LVEF & ECG for CHF, etc) Reduction in ACSC admissions /1000 compared to baseline (33.3 total for CHF, Pneumonia, COPD/Asthma) Jencks 2% to 15% of Physician income, or $76 pppy to $500pppy CMS – Disease Management Demo DPRP HEDIS measures for CHF and CAD MPR study of CC/DM programs Fixed fee pmpm for DM services CMS – Coordinated Care Demo Chronic Illness management using criteria id’d in MPR’s study MPR study of CC/DM programs Fixed fee pmpm for services Plans – Aetna, CIGNA, Highmark, Anthem, BCBS IL, BC CA, Ind. Health HEDIS-based, utilization, patient sat. Reduced ER/Hospitalizations Jencks Varies, from $24 to $96 pmpy IHA HEDIS IT – “Ambulatory Patient Safety Leap” Patient Experience Bates, Middleton Varies, from $24 pmpy to 10% of physician fees Wu and Pope McCall Davies Safran, Colton Bridges To Excellence, Proprietary & Confidential 9 Summary of Evidence on Cost Impact of Interventions PGP Demonstration Design Report Confirms findings from Kane et al on overuse of hospitalizations among patients with ambulatory sensitive conditions Estimates that savings can be significant for Medicare, which sets up the bonus system for participating docs Care Coordination, Case Management and Disease Management Demo Reports Programs with certain characteristics have been proven effective (ID patients, establish plan, measure, improve) Increased compliance by patients and physicians leads to better outcomes and lower costs IOM’s Crossing the Quality Chasm Report Reengineering physician offices is needed to systematize the reduction of defects (misuse, overuse, underuse) Defects for all types of care, not simply chronic care, are prevalent in all aspects of the delivery system Can’t expect reengineering towards efficiency/effectiveness if we don’t offset some of the costs through incentives Bridges To Excellence, Proprietary & Confidential Estimated Overall Impact & Available Incentive Pool for POL Better Management of Chronic Conditions: Hewitt analysis identifies 5% gross potential opportunity • • Reduce by 1/3 to take into account current impact of good care (diabetes defect rate at 67%) Reduce by 1/3 to take into account that we’re only focusing on the physicianfaced interventions, not patient faced interventions Net opportunity of 1.7% of total spend Better Pharmacy Management: PWC/Allscripts analysis yields gross opportunity of 5% of Rx spend • • Reduce by 25% to take into account current impact of Pharma mgmt Rx is 22% of total spend Net opportunity of about 1% of total spend Reduce ADEs, Lab & Radiology Overuse: Bates et al. estimate opportunity to be about 1% to 2% of total spend Net opportunity at 1.5% of total spend • UHC confirms overuse of Imaging at 25%, 1.1% of total spend Total conservative review yields a 4.2% gross spend opportunity of $110 pmpy, and our max incentives are $55 pmpy Bridges To Excellence, Proprietary & Confidential 10