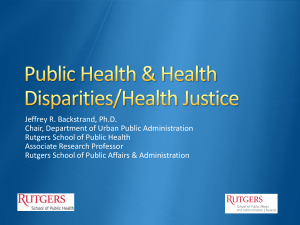
The Affordable Care Act (Part II): Section 4302 and Implications for
advertisement
: Section 4302 and Implications for")
The Affordable Care Act (Part II): Section 4302 and Implications for Data Collection David Meyers, M.D., Agency for Healthcare Research and Quality (AHRQ) José J. Escarce, M.D., University of California, Los Angeles School of Medicine; RAND November 18, 2010 AcademyHealth The professional society of health services research and health policy analysis. AcademyHealth represents a broad community of people with an interest in and passion for using health services research to improve health care. We promote interaction across the health research and policy arenas by bringing together a broad spectrum of players to share their perspectives, learn from each other, and strengthen their working relationships. www.academyhealth.org Aetna Foundation The Aetna Foundation is a national health foundation that promotes wellness, health, and access to high-quality health care for everyone. Our giving is focused on addressing the rising rates of adult and childhood obesity in the U.S.; promoting racial and ethnic equity in health and health care; and advancing integrated health care. Originally founded in 1972 as the independent charitable and philanthropic arm of Aetna Inc., Aetna and the Aetna Foundation have contributed over $379 million in grants and sponsorships since 1980. This work is enhanced by the time and commitment of Aetna employees, who have volunteered nearly 2 million hours since 2003. For more information, visit http://www.aetnafoundation.org. Learning Objectives The goals of this session are to: – Provide an overview of general provisions in the Affordable Care Act that address health disparities – Review the implications for data collection addressed in Section 4302 of the Affordable Care Act – Provide an overview of the next steps in implementation, and discuss steps that have been taken to encourage public engagement on data collection and reporting issues The audio and slide presentation will be delivered directly to your computer Speakers or headphones are required to hear the audio portion of the webinar. If you are having difficulties with the audio-stream, please dial (888)-632-5061 and enter the Conference ID number: 92065340 followed by the # sign. Technical Assistance If you require technical assistance, or are having difficulties with the audio portion of this webinar, please click on “Help” Submitting Questions Questions, both substantive & technical in nature, may be submitted at any time during the presentation. Click on “Ask a Question” below this presentation. Complete the form and click “Submit.” Responses will only be sent if related to a technical issue; otherwise you will not receive a confirmation that your question has been received. Welcome Anne C. Beal, M.D., M.P.H. President Aetna Foundation Faculty David Meyers, M.D. Director Center for Primary Care Agency for Healthcare Research and Quality Faculty José J. Escarce, M.D. PhD. Professor of Medicine, David Geffen school of Medicine at UCLA Senior Natural Scientist, RAND Health Implementing Affordable Care Act Section 4302: An overview of federal efforts David Meyers, M.D. Director, AHRQ Center for Primary Care AcademyHealth and Aetna Foundation Webinar November 18, 2010 Disclosure I have no financial interests to disclose Credibility I have no financial interests to disclose Credibility I have no financial interests to disclose Clinician – Practiced full-scope family medicine in a community health center in SE Washington, DC Credibility I have no financial interests to disclose Clinician Researcher – Focused on answering questions relevant to the care of the community I served Credibility I have no financial interests to disclose Clinician Researcher Policy advocate Credibility I have no financial interests to disclose Clinician Researcher Policy advocate Bureaucrat Disclosure The content of this presentation reflects the opinions of the presenter and does not necessarily represent the official positions of AHRQ or the US Department of Health and Human Services. Presentation Overview Setting the context: The ACA and health disparities Review of Affordable Care Act Section 4302: Data collection to understand health disparities Brief overview of federal implementation of Section 4302 Opportunity for feedback – Response from Dr. Escarce – Questions and comments from Webinar participants The Affordable Care Act and Health Disparities Expansion of insurance coverage Improved access to care Focus on quality Focus on prevention Focus on public health The Affordable Care Act and Health Disparities Expansion of insurance coverage Expansion in access to care Focus on quality Focus on prevention Focus on public health For more details, please listen to the first webinar in this series: The ACA: Impacts and Opportunities for Disparities Research on AcademyHealth’s website The Affordable Care Act and Health Disparities Expansion of insurance coverage Expansion in access to care Focus on quality Focus on prevention Focus on public health Attention to data collection and reporting – Section 4302 The Affordable Care Act Section 4302 Understanding Health Disparities: Data Collection and Analysis Overview Section 4302 has two main sections – (a) Federal national data collection efforts and the analysis and reporting of this data – (b) Medicaid and CHIP Overview Section 4302 has two main sections – (a) Federal national data collection efforts and the analysis and reporting of this data – (b) Medicaid and CHIP Part (a) of Section 4302 Requires the DHHS Secretary to establish data collection standards Calls for the use of the standards in federal data collection Instructs that the data be used for analyses and that the results be reported Contains some important language about funding Part (a) of Section 4302 Requires the DHHS Secretary to establish data collection standards Calls for the use of the standards in federal data collection Instructs that the data be used for analyses and that the results be reported Contains some important language about funding Disclaimer: During today’s overview, I will not be covering all of the details and nuances of this complex piece of legislation. Establishing Standards Requires the DHHS Secretary to establish data collection standards for five specific demographic categories: – – – – – Race Ethnicity Sex Primary language Disability status Data Standards Must be for self-reported measures – Or for parents to report for children and guardians to report for legally incapacitated adults Must comply with OMB standards – The law states current OMB standards for race and ethnicity must be used at a minimum Implications of Self Report The creation of standards for self reported demographic measures may suggest that the intent of the law is: – to guide data collection from surveys of individuals, – possibly to apply to data collected at program enrollment, – not focused on administrative data. Use of the Data Standards Affordable Care Act Section 4302 begins: The Secretary shall ensure that, by not later than 2 years after the date of enactment of this title, any federally conducted or supported health care or public health program, activity or survey collects and reports, to the extent practicable data on race, ethnicity, sex, primary language, and disability status Use of the Data Standards: Which Standards Affordable Care Act Section 4302 begins: The Secretary shall ensure that, by not later than 2 years after the date of enactment of this title, any federally conducted or supported health care or public health program, activity or survey collects and reports, to the extent practicable data on race, ethnicity, sex, primary language, and disability status Use of the Data Standards: By When Affordable Care Act Section 4302 begins: The Secretary shall ensure that, by not later than 2 years after the date of enactment of this title, any federally conducted or supported health care or public health program, activity or survey collects and reports, to the extent practicable data on race, ethnicity, sex, primary language, and disability status Use of the Data Standards: Applies to What Affordable Care Act Section 4302 begins: The Secretary shall ensure that, by not later than 2 years after the date of enactment of this title, any federally conducted or supported health care or public health program, activity or survey collects and reports, to the extent practicable data on race, ethnicity, sex, primary language, and disability status Use of the Data Standards: An Important Guide Affordable Care Act Section 4302 begins: The Secretary shall ensure that, by not later than 2 years after the date of enactment of this title, any federally conducted or supported health care or public health program, activity or survey collects and reports, to the extent practicable data on race, ethnicity, sex, primary language, and disability status An Additional Focus on People with Disabilities Section 4302 calls for specific new data collection activities around the care of people with disabilities [(a) 2 D i-iii] – locations where individuals with disabilities access primary, acute, and long term care – the number of providers with accessible facilities and equipment to meet the needs of the individuals with disabilities – the number of employees of health care providers trained in disability awareness and patient care of individuals with disabilities Expanded Demographic Categories Section 4302 gives the DHHS Secretary discretionary authority to require standard data collection around demographic categories related to health care disparities in addition to the five already required categories (race, ethnicity, sex, primary language, and disability status). Analysis and Reporting Requires that any federal reporting requirements related to health care quality be reported (to the extent practicable) by race, ethnicity, sex, primary language, and disability status. Analysis and Reporting Calls for the incorporation of demographic data collection standards into national health IT efforts Requires all federal programs that collect demographic data related to health disparities to use the data to detect health disparities, monitor for trends, and to widely report results Calls for the DHHS Secretary to make data available for research, additional analysis, and dissemination Requires use of privacy protections and data security standards Funding Part (a) concludes with two statements related to funding: – Authorizes ‘such funds as necessary’ for 2010-2014 to conduct these activities Does not include a specific appropriation – Concludes with a statement that no data collection activities as described under this Section may be conducted “unless funds are directly appropriated for such purpose in an appropriations Act.” Implementing Section 4302 Establishing data standards Considering additional categories Special surveys related to the care of people with disabilities Preparing to incorporate standards Data analysis and reporting Seeking Guidance and Clarification “To the extent practicable” Application to the direct provision of health care services What is considered a direct appropriation in relation to the provision that no data collection may take place ‘unless funds are directly appropriated’ Seeking Guidance and Clarification “To the extent practicable” Application to the direct provision of health care services What is considered a direct appropriation in relation to the provision that no data collection may take place ‘unless funds are directly appropriated’ On going Transparency and Public Engagement DHHS is committed to making Affordable Care Act implementation a transparent process and seeking public input throughout the process. Initial Data Standards Long-standing and well-established DHHS interagency Data Council has taken the lead on drafting initial data standards for race, ethnicity, sex, primary language, and disability status Initial Data Standards Long-standing and well-established DHHS interagency Data Council has taken the lead on drafting initial data standards for race, ethnicity, sex, primary language, and disability status – – – – – Guided by OMB standards for race and ethnicity Consultations with OMB, Dept of Labor, Bureau of Census and other federal partners Informed by recent IOM reports on data granularity Decision made to narrowly define sex so as not to include sexual orientation Primary focus is on self reported data collection standards for surveys, but using the opportunity to explore data collection standards for administrative data Next Steps Data Council to complete draft standards Conduct DHHS and Secretarial review Solicit and incorporate public comment on proposed draft standards Issue final five data collection standards Additional Categories DHHS is hosting listening sessions to elicit ideas for additional demographic categories related to health disparities – Desire for additional data must be tempered by consideration that these standards will apply to all federal health data collection activities Consideration of public data collection burden Consideration of cost Additional Categories DHHS is hosting listening sessions to elicit ideas for additional demographic categories related to health disparities – Desire for additional data must be tempered by consideration that these standards will apply to all federal health data collection activities Consideration of public data collection burden Consideration of cost More about this in a few moments… Next Steps Incorporate public input Prepare DHHS recommendation to the Secretary Secretary may choose not to create additional categories at this time, may call for standard development for one or more additional categories, or may request additional public input New Surveys on Health Care for People with Disabilities Small working group led by DHHS Office on Disability leading this effort Without specific appropriation, this effort may not progress quickly Preparing for Use of Data Standards Despite standards not being ready, DHHS is conducting a review of the major federal health care surveys and considering how to incorporate inclusion of all five data standards. Data Analysis and Reporting Prior to the Affordable Care Act, DHHS had a commitment to creating health care equity. Many efforts were already underway to improve data collection, analysis, and reporting, and these continue in parallel with implementation of Section 4302. Inviting Input on Additional Demographic Categories In the near future, DHHS staff involved in implementing Section 4302 will be conducting listening sessions to gather input on what, if any, additional demographic categories related to health disparities, the DHHS Secretary should require be collected in all federal data collection activities. Specific Questions What characteristic(s) do you think should be added to the current list of race, ethnicity, sex, primary language and disability status to further address health disparities? How many individuals would be affected if data addressing this topic is collected? Is there evidence that a health disparity exists for this characteristic? Have any instruments been developed and tested to measure this demographic characteristic? If so, please provide a brief summary of the measures and evaluation results. If not, do you have recommendations as to the questions that should be asked or how the measures should be developed? Specific Questions (cont.) Has information on this characteristic ever been collected, presented, published, or televised? If so, where has this been done? Recognizing that demographic data, especially data related to disparities, may be sensitive, elicit prejudices, and affect individual’s willingness to provide information, do you have information about how collecting information on this category may affect overall data collection activities and how to maximize data quality? Do you have any recommendations as to how the Secretary should decide (i.e., what criteria should be used) whether the potential for burden of adding your proposed characteristics would outweigh the need to gather additional information to address health disparities? Do you have any other recommendations with respect to any other demographic data regarding health disparities that you would like the Secretary to consider? Responses Lead response from Dr. José Escarce Followed by questions and answers and responses regarding additional demographic categories – Please remember, that at this time, feedback must focus on additional categories and not the five required categories (race, ethnicity, sex, primary language, and disability status) Submitting Questions Questions, both substantive & technical in nature, may be submitted at any time during the presentation. Click on “Ask a Question” below this presentation. Complete the form and click “Submit.” Responses will only be sent if related to a technical issue; otherwise you will not receive a confirmation that your question has been received. Commentary José J. Escarce, M.D. Associate Director Robert Wood Johnson Clinical Scholars Program UCLA School of Medicine/RAND Comments on: The Affordable Care Act: Section 4302 and Implications for Data Collection José J. Escarce, M.D., Ph.D. UCLA and RAND AcademyHealth and Aetna Foundation Disparities Research Webinar Series November 18, 2010 Outline of comments • Types of disparities • Reasons for collecting data • Scope of data collection – Private health insurance – Socioeconomic position Types of disparities • Health care disparities – Social justice – Effect on health status Types of disparities • Health care disparities – Social justice – Effect on health status • Health disparities – Role of health care – Social determinants of health Reasons for collecting data • Identify and measure disparities • Design and implement interventions to address them • Monitor progress in reducing disparities and refine interventions Scope of data collection • Most Americans receive their health insurance coverage through private insurers Scope of data collection • Most Americans receive their health insurance coverage through private insurers • Therefore, to describe and address health care disparities, we must understand patterns of care by race, ethnicity, and other relevant characteristics among persons with private coverage Scope of data collection • Who could collect these data? – Health plans – Health care providers – Purchasers • Challenges to data collection – Member concerns and perceptions – Inadequate information systems – Resource limitations • NCQA Multicultural Health Care standards Scope of data collection • Socioeconomic position affects the health care that Americans receive Scope of data collection • Socioeconomic position affects the health care that Americans receive • Socioeconomic position also has a profound effect on the health of Americans through a variety of mechanisms Scope of data collection • Socioeconomic position affects the health care that Americans receive • Socioeconomic position also has a profound effect on the health of Americans through a variety of mechanisms • Therefore, to describe and address health and health care disparities, ideally we would understand patterns of care and health status by SEP Summary of research on SEP and health • Gradient between SEP and mortality is continuous – there is no threshold • Gradient is seen with multiple indicators of SEP • In most studies using U. S. data, income and education exert independent effects • Mortality has declined over time, but the gradient has persisted Explaining the effects of SEP on health Materialistic Behavioral Type of Explanation Source of Inequality Life span Health care Housing quality, sanitation, transportation, occupational hazards, environmental hazards, neighborhood quality, nutrition Ability to buy insurance, medical care, medications Diet, smoking, exercise, leisure activities, alcohol and substance abuse, risk taking Medical information, awareness of health problems, navigating the system, self-management, adherence Feinstein JS. Milbank Q 1993; 71(2):279-322. Medical care spending for U.S. adults, by family income Medical care spending (jn $) 3,500 3,000 2,500 2,000 1,500 1,000 500 0 <1.0 1.0-1.99 2.00-2.99 3.00-3.99 4.00-4.99 Income, multiple of poverty level Unadjusted >5.0 Medical care spending for U.S. adults, by family income Medical care spending (in $) 3,500 3,000 2,500 2,000 1,500 1,000 500 0 <1.0 1.0-1.99 2.00-2.99 3.00-3.99 4.00-4.99 Income, multiple of poverty level Unadjusted Adjusted >5.0 Conclusions • Identifying and addressing health and health care disparities requires collecting relevant data on relevant populations • Efforts to collect data on persons with private health insurance coverage should be encouraged and expanded • Ideally, data collection would include measures of socioeconomic position Discussion Questions for our speakers can be submitted now. Click on “Ask a Question” below this presentation. Complete the form and click “Submit.” Methods Sessions: Register Today! Analytic Considerations for Collecting Data on Race, Ethnicity, and Language Date: Tuesday, November 30, 2010 - 1:00-2:30 pm (Eastern) Faculty: Romana Hasnain-Wynia, Ph.D., Northwestern University Community Based Participatory Research: Strategies for Reducing Health Disparities Date: Wednesday, December 8, 2010 - 1:00 - 2:30pm (Eastern) Faculty: Nina Wallerstein, Dr.P.H. and Lorenda Belone, Ph.D., Robert Wood Johnson Foundation Center for Health Policy at the University of New Mexico Visit www.academyhealth.org/training for more information. Thank You! Please take a moment to fill out the online evaluation.