11/20/2014 Psychotherapeutic or Psychotropic Antidepressants
advertisement

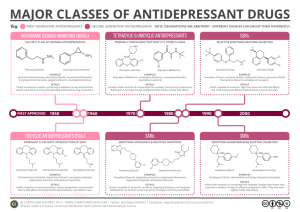
11/20/2014 Psychotherapeutic or Psychotropic Medications Antidepressants Many varieties Antianxiety drugs Antidepressants Mood Stabilizers Major Depression is the 3rd most disabling disease worldwide. It currently affects 30 million Americans (only about 21% get treatment) & accounts for ~70% of psychiatric hospitalizations and ~40% of suicides. 10% of males and 25% of females will suffer clinical depression in their lifetimes. Antipsychotics (all these category names should be viewed as indicating just 1 of the prominent uses of the drugs) Over 230 million prescriptions/yr in US At least 10-15% of the population receiving psychotherapeutics Symptoms of Major Depressive Disorder • At least 5 of the following almost every day weeks: • Persistent depressed or irritable mood • Decreased interest or pleasure • Significant change in appetite/weight • Insomnia or hypersomnia • May move & talk slowly, or may be restless • Fatigue, loss of energy or motivation, apathetic • Feel worthless; inappropriate guilt • Can’t make decisions, concentrate • Suicidal thoughts or actions for at least 2 • This family of transmitters is known as the monoamines. • Symptoms of psychosis in severe cases Original Monoamine Theory of Mood • Normal mood depends on appropriate levels of monoamine activity in brain. • Levels too low depression • Levels too high euphoria, mania • All current antidepressants have actions which would help normalize these deficiencies. Monoamine Theory Updated Based on New Research • Antidep drugs all increase monoamine activity immediately, but aren’t clinically effective for weeks. It appears that slower, long term effects of these drugs are key to the clinical improvement. • Formation of new neurons (neurogenesis) & repair of damaged neurons are normal processes in certain brain areas (hippocampus, frontal cortex) • Psychological stress as well as many physiological stresses decrease neurogenesis and neuron repair. • All with depression probably don’t experience exactly the same monoamine imbalance. 1 11/20/2014 Neurogenic Theory of Depression • Depression (stress-related & stressful itself) is associated with loss of neurons & decreased neurogenesis. It is a neurodegenerative disease like Alzheimer’s or Parkinson’s, but affecting different regions. • The increased monoamine activity caused by antideps stimulates intracellular production of substances which promote neuron repair and neurogenesis necessary to replace the neurons lost in depression. Growth of new neurons takes time. Tricyclics Categories of Antidepressants • First Generation Antidepressants (‘50’s-’60’s): • Tricyclic antidepressants (TCAs) • Monoamine oxidase inhibitors (MAOIs) • Second Generation Antidepressants (‘89 ) • Selective serotonin reuptake inhibitors (SSRIs) • Dual action antidepressants (2000) • Miscellaneous group Tricyclic Antidepressants (TCAs) • Best known: • • • • *imipramine (Tofranil) Classic examples of this group *amitriptyline (Elavil) *desipramine (Norpramin) Newer & fewer side effects, so *nortriptyline (Pamelor, Aventil) preferred among the TCAs today • Significantly more effective than placebo in providing relief for severe depression & sustained prevention of depressive episodes. Not as effective for psychotic or atypical forms of depression. • Usually taken once a day at bedtime • Very inexpensive Tricyclics Block Reuptake of 5HT & NE so transmitter activates receptors longer • Even though these are old drugs they have a useful combination of effects: • Antidepressant • Anti-anxiety • Analgesic • Sedating 2 11/20/2014 Tricyclic Problems • Delayed effectiveness (3-6 weeks); therapeutic window for effectiveness • Also block ACh & histamine receptors- may cause annoying side effects before benefits are felt: • Anticholinergic: Dry mouth, dizzy, blurred vision, constipation, urinary hesitance, tachycardia, *possible cognitive problems (not recommended for young or old) • Antihistamine: sedation • Have a low safety margin & are lethal in overdose (cardiac arrhythmia & heart failure, coma, respiratory distress10,000 ER, 800 deaths); interact with a wide variety of drugs. Had been #1 cause of prescription drug overdose death in US in past (before opioids) Table 12.1 Claire D. Advokat, Joseph E. Comaty, Robert M. Julien: Julien’s Primer of Drug Action, Thirteenth Edition Copyright © 2014 by Worth Publishers Monoamine Oxidase Inhibitors (MAOIs) Other Uses for Tricyclics • dysthymia (milder but persistent depression) or the depression of bipolar disorder • OCD (clomipramine is a favorite) • panic disorder/agoraphobia & other anxiety disorders • treatment of chronic pain conditions, migraine, chronic fatigue • treatment of enuresis (bed-wetting) • some cases of ADHD* • * Caution necessary: have been 12 deaths in kids using TCAs MAOI Problems • Foods with high levels of tyramine must be avoided • Drugs with sympathomimetic or NE/5HT effects must be avoided, including other antidepressants • Neglecting restrictions can result in life-threatening hypertensive crisis (severe headache, skyrocketing blood pressure, heart palpitations); must continue restrictions 2 weeks after stopping drug as well • Clinical improvement delayed • selegiline (Ensam) patch – slow transdermal absorption seems to avoid food/drug interactions while still being effective. While expensive this may result in more frequent prescribing for the conditions for which MAOIs are particularly effective (e.g. atypical depressions, depression in elderly, anorexia, bulimia) or in those patients who do not respond to other antidepressants. • *phenelzine (Nardil), tranylcypromine (Parnate), isocarboxazid (Marplan, Enerzer) • Inhibit action of MAO, an enzyme which breaks down 5HT, DA and NE, allowing more transmitter release/action • Problem : enzyme is inhibited not only in brain but also in body where it serves an important protective function Low Tyramine Diet • Foods to Avoid • Medications to Avoid • Aged cheeses (including cheddar, American, mozzarella as on pizza; cream cheese, farmer cheese, cottage cheese are considered safe) • (ask your physician about any other prescribed medications for safety) • Yeast extract (may be a component of certain canned soups; baked products raised with yeast are acceptable) • Red wine (especially Chianti; white wine in moderation will not cause a hypertensive reaction) • Beer or ale (tyramine content varies from lot to lot) • Pickled herring, canned sardines, anchovies, caviar • Any meat or fish which is not fresh, freshly canned, or freshly frozen (including lox, salami, sausage, corned beef, liver pate) • • Broad beans or fava beans Canned figs, stewed or overripe bananas, overripe avocados • • • Decongestants Nasal drops or sprays Pain relievers* (NB: meperidine is very dangerous) • General and local anesthetics* • Stimulants* • L-Dopa* • Propranolol* • Caffeine* • • Soy sauce* • • Raisins* • Liver (dangerous when not fresh) • * = considered safe in limited amounts Other antidepressants* Some herbal preparations, e.g., those containing ginseng or ma huang 3 11/20/2014 Selective Serotonin Reuptake Inhibitors (SSRIs) (1989) Action of SSRIs • fluoxetine* (Prozac, Serafem)*, paroxetine (Paxil), sertraline (Zoloft), fluvoxamine (Luvox), citalopram (Celexa) & escitalopram (Lexepro) + 2 new • same effectiveness but more acceptable side effects and fewer overdose risks • side effects more like stimulant drugs in most ( 1 in 5 users might feel anxious, hyper, restless, suffer insomnia, stomach upset, diarrhea) early in treatment • too high dose in kids may be mistaken for bipolar disorder; only fluoxetine shown to be effective in kids Other Uses for SSRIs • *Treatment of dysthymia,pre-menstrual dysphoria, postpartum depression, bipolar depression • *Used for social phobias, panic disorder, PTSD, generalized anxiety disorder, OCD • Treatment of some eating disorders & addictions and some chronic headaches SSRI Problems SSRI-Induced Sexual Dysfunction Significant proportion (up to 80%) will have sexual side effects (loss of desire, impotence, difficulty achieving orgasm) • Can be serious enough to affect marriages, relationships Serotonin Syndrome High Dose or Combining 5HT Drugs Produces an Exaggerated Response l Altered cognition (disorientation, confusion, hypomania, delusions, “losing-it”) l Behavioral alterations (agitation, restless) l Autonomic (fever, chills, sweat, diarrhea, hypertension, tachycardia) l Neuromuscular impairment (ataxia, hyperreflexia) l Surprisingly, an SSRI + an opioid analgesic or a benzodiazepine sometimes triggers serotonin syndrome 4 11/20/2014 Serotonin Withdrawal Syndrome or “Discontinuation Syndrome” • ~ 60% who abruptly stop their SSRI will experience some of these: Note “FINISH” mnemonic) • • • • • • • Flu-like symptoms (fatigue, aches, chills, diarrhea) Insomnia or disturbed sleep Nausea Imbalance (dizziness, incoordination) Sensory abnormalities (electric shock sensations, visual) Hyperarousal (agitation, anxiety) & Headache Dose should be slowly tapered Paxil “Termination” Symptoms • http://www.youtube.com/watch?v=hfQUTHrWnRk&mode=related&s earch= • http://www.youtube.com/watch?v=T5X01wvJWPs • Discontinuation syndrome can also occur after lengthy use of other antideps Drugs Not Fitting Above Categories • Fewer effects on sexual functioning: • *Wellbutrin (buproprion) (DA/NE reuptake inhibitor somewhat like cocaine/amphetamine). As a “stimulating” antidep it treats depression & the fatigue it produces but also has some seizure risk & can worsen anxiety disorders, OCD, panic. • Serotonin AND NE reuptake inhibitors– newer “dual action” • Effexor (venlafaxine) & Pristiq (desvenlafaxine) – fewer sex effects than SSRIs but not as good as bupropion. • Watch for “funny stuff” (agitation, aggression, manic flips, homicidality (new warnings added), not for adolescents • Cymbalta (duloxetine) (analgesic too) • Remeron (mirtazapine) (may work somewhat faster; sedative & increases appetite too) New Warnings • Adult and Pediatrics: • There are clinical trial and post-marketing reports with SSRIs and other newer antidepressants, in both pediatrics and adults, of severe agitation-type adverse events coupled with self-harm or harm to others. The agitation-type events include: akathisia, agitation, disinhibition, emotional lability, hostility, aggression, depersonalization. In some cases, the events occurred within several weeks of starting treatment. • Rigorous clinical monitoring for suicidal ideation or other indicators of potential for suicidal behaviour is advised in patients of all ages. This includes monitoring for agitation-type emotional and behavioral changes. • http://www.antidepressantsfacts.com/2004-05-26-HC-suicid-self-harm-effexor.htm (see next slide) Beware of Re-Packaged or Slightly Altered Old Drugs to Get a New Patent & More $$$ • Doxepin Silenor 50x as expensive • Celexa Lexepro • Effexor Pristiq Increased Suicidality in Pediatric and Adolescents on Antidepressants? • Metanalysis of 24 small studies revealed an increased risk, particularly when starting the drug or changing dose • Risk in untreated group: 2/100 • Risk in treated group: 4/100 • So in 2004 FDA require “Black Box” Warnings * NOTE: New genetic research looks promising for being able to identify antidep “nonresponders” and also antidep users prone to suicidal ideation! 5 11/20/2014 Required “Black Box” Warning Controversy Has a Cascade Effect http://www.youtube.com/watch?v=k-BT8nxO8Pg • But reactionary decrease in antidep use 14-49% increase in suicides – largest increase since suicide data began to be collected!! • http://www.youtube.com/watch?v=bLpuIezmf-w • Psychotherapy along with meds decreases the suicide risk. • http://www.uchospitals.edu/news/2012/20120206 -depression.html SSRIs and Suicide Antidepressant Limitations • Response to antidep may take up to 12 weeks to occur • Antidepressants only partially effective in many • Even if first antidep does not work, switching to another may be successful • All antideps are effective for some – no single best antidep – need to match drug with patient • May be necessary to “augment” treatment – various add-ons: • • • • A second antidepressant (e.g. SSRI+buproprion) Provigil (modafanil); BuSpar (buspirone) A mood stabilizer/anticonvulsant like Lamictal (lamotrigine) An atypical antipsychotic like Abilify (aripiprazole) or Seroquel (quetiapine) or antipsych/antidep mix (olanzapine+ fluoxetine) Symbyax • Cognitive-behavioral therapy New Drug Research • Several distinctively different antideps are under investigation. • One surprising new finding: • Low dose intravenous ketamine can produce immediate relief of depressive or serious anxiety symptoms in some individuals. Typically lasts 1-3 weeks, sometimes longer. Looking for a non-hallucinogenic drug that might have the same action. 6