Request for Medical Leave of Absence
advertisement

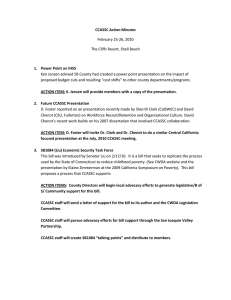
Request for Medical Leave of Absence Name Date Title I hereby request a medical leave of absence as follows: Beginning Date Ending Date Purpose of Leave: Birth of child and to care for new-born child. Employee's serious health condition which makes employee unable to perform the functions of employee's job. Placement of child for adoption or foster care, and to care for adopted child or child in foster care. The care of spouse, child or parent with a serious health condition. Relationship: I understand upon receipt of this request the Human Resource Office will provide me with additional information and the additional required forms that will need completed. Print Form Employee's Signature Date: Human Resource Office Use Only Approved Human Resource Director's Signature Denied Date