Direct Sick Leave Donation – RECIPIENT
advertisement

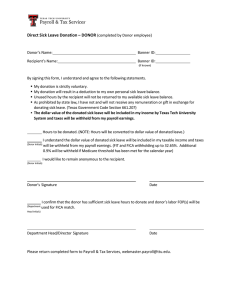
Direct Sick Leave Donation – RECIPIENT (completed by Recipient employee) You, , have been gifted with hours of sick leave . valued at $ from By signing this form, I understand and agree to the following statements. Donated sick leave hours will be available after I have exhausted my own personal sick and vacation leave. If my absence is Sick Leave Pool eligible, I have requested and exhausted the award. The hours stated above will be added to my sick leave donated balance. As prohibited by state law, I have not and will not give any remuneration or gift in exchange for donated sick leave. Recipient’s Signature and R# Date Please return completed form to Payroll & Tax Services, webmaster.payroll@ttu.edu.