A Systems View of the Smoking Problem: ... and Limitations of the Role of ... Decision-
advertisement

is
A Systems View of the Smoking Problem: Perspective
and Limitations of the Role of Science in DecisionMaking
by
Edward B. Roberts
with Jack Homer, Armen Kasabian and Michael Varrell
WP# 1030-78
October, 1978
Prepared for presentation and discussion
at the
M.I.T.- C.N.R.S. Conference on
Science and Decisinf. Making
Paris, France
February 1-3, 1979
:Wi.,
A Systems View of the Smoking Problem:
Perspective and Limitations of the Role of Science in Decision-Making
Abstract
The complex issues and relationships surrounding the smoking problem
indicate the desirability of a system dynamics computer simulation model
for policy development and analysis.
This paper describes an initial
model-building effort, including reports of initial policy and sensitivity
testing of the model.
The lack of scientific research on most of the
relationships and parameters required in such a model forced heavy reliance
upon intuition in the model development. The sensitivity of simulated
model outcomes to many of these assumptions demonstrates the need for a
more concentrated multi-disciplinary research effort if forecasting and
policy determination are to be carried out with confidence.
Introduction
In 1965, the U.S. Surgeon General released the now-famous report linking
smoking with lung cancer and other diseases.
continuous conflict in this "smoking problem".
Ever since, there has been a
Researchers continue to
find more hazards to smoking while the cigarette industry continues to deny
these reports; health officials lobby for more stringent cigarette standards
and more restrictions on smoking while the industry tries to counter this;
education has attempted to help smokers quit and prevent the initiation of
smoking while advertising has continued to exploit the "attractiveness" of
smoking.
These factors which affect the portion of the population that smokes
interact in a dynamic way. But certain proposals to solve or reduce the smoking problem may have results that are counterintuitive.
More stringent cigarette
III
-2standards may reduce tar and nicotine content in cigarettes which in turn
should reduce smoking related morbidity and mortality. However, this reduced
smoking-related morbidity and mortality in turn is likely to increase societal
approval of smoking which may in turn increase the smoking population.
The
complicated set of interactions in the smoking problem should be analyzed
carefully in trying to set public policy in an effective manner, even if we
begin by assuming an overall objective of reducing the prevalence and impact
of smoking.
This paper presents a simplified and preliminary system dynamics model
of the smoking problem and reports tests of certain policy alternatives as
to the efficacy in reducing the smoking population and smoking-related morbidity and mortality.
By its method of approach to analysis, the paper is
as much a statement of the inadequacy of focused social and policy-impacting
scientific research, as it is a presentation of a scientific methodology for
policy-seeking.
For lack of relevant evidence, most of the relationships and
parameters in the model had to be generated by intuition, rather than from
empirical analysis.
Two examples may help to illustrate the difficulty.
Significant re-
search has been done to determine differentiating characteristics between
smokers and nonsmokers. Saslow and Matarazzo list thirty-four such characteristics which have been statistically verified to differentiate smokers from
nonsmokers. These characteristics include such factors as age, sex, income,
residence, psychological tension level, emotional status and smoking habit
of parents.
But incorporating these variables into a dynamic causal model
is very difficult. What are the key factors that influence the initiation
of smoking and to what degree do they influence it?
Sparse scientific evidence
exists to answer these questions. As a second example, despite the theoretical
work of Harris, we know that it is impossible to find empirical evidences for
for relationships such as the effect of price on the initiation of smoking
in the United States.
We therefore developed the model with as many interactions as we
thought reasonable and incorporated relationships to the best of our
ability, guessing frequently but hopefully not arrogantly as to possible
effects.
The conclusions derivable from the model at its present stage of
development are therefore more presentations of hypotheses worth further
refinement and testing than guidance to current policy-makers.
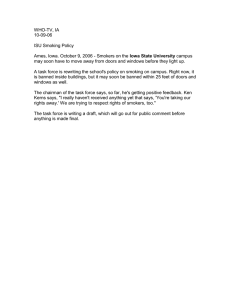
The Model
The model* focuses on the complex interactions which affect the initiation and quitting of smoking.
levels:
This divides the population into three
potential smokers, smokers, and ex-smokers.
Among the key varia-
bles that the model measures are the proportion of the population in these
three levels, and the mortality levels derived from the three population
levels.
(Fig. 1)
Figure 1. The Population Macro-System
ilation
19
Symbols:
[
--- Levels, Accumulations
"
--- Rates of Flow, Decisions
Cfr-- Sources or Sinks for Flows
C~,
-
* A more detailed discussion of the computer equations of the model is
available, as are complete listings of the DYNAMO-documentor output.
_
III
-4The initial model was developed in the following eleven interrelated
sectors:
1. Population -- the population is divided into three levels:
potential
smokers, smokers, and ex-smokers;
2. Contaminants and their effects -- representing the contaminants absorbed
by smokers and their effects on morbidity and mortality;
3. Factors affecting Initiation -- the factors affecting the initiation of
smoking, converting potential smokers into smokers;
4. Factors affecting Quits -- the factors affecting the quitting of smoking)
converting smokers into ex-smoKers;
5. Factors affecting Intensity -- factors affecting the intensity of smoking,
or the number of cigarettes smoked per smoking person per year;
6. Factors affecting Price -- examining the effect of various variables on
the price of cigarettes;
7. Restrictions on Smoking -- examining the factors that determine the general societal level of smoking restrictions;
8. Perceived Hazards -- examining the identified maladies and other factors
which affect the perceived level of hazards due to smoking;
9. Societal Approval of Smoking -- describing the effects of various factors
on society's attitudes of approval/disapproval towards smoking;
10.
Tobacco Industry Spending -- examining the industry income and its effects
on the industry's tools to maintain and/or increase smoking;
11.
Anti-Smoking Campaign -- examining the attempts of the anti-smokers to
reduce smoking.
An overview of the initial model, with the main interactions among the
various sectors, is included in Figure 2. The plus and minus signs on the
arrow-heads indicate the general direction of effect of one sector upon another.
For example, an increase in the Perceived Hazards of smoking will tend
to produce an increase in the Restrictions on Smoking. This is a reinforcing
-5or positive (+)relationship.
Whereas an increase in Restrictions is shown
as inducing a decrease in the Initiation Rate.
These forces thus move in
opposite directions and the relationship is shown as a negative (-)one.
Figure 2. Interactions AFcong Sectors of the Smoking Model
Each of the various sectors is composed ofa set of complicated interactions, and the sectors also interact with each other.
We can begin our more
detailed examination with our main interest in the model, which was the percentage of the population in the various categories and the death of smokers.
As was shown in Figure 1, the population is divided into three levels:
poten-
tial smokers, smokers, and ex-smokers.
The potential smokers consist of all individuals over 12 years of age
who were never smokers. This population level increases by the population
aging rate, i.e., those reaching 12 years of age each year, which is an
11
-6-
exogenous variable.
For this model, we have used a population aging rate
of 1% which has been the approximate average for the United States in the
last decade.
The potential smokers either die never having smoked, in accord with
'the "potential smoker death rate", or are converted to smokers by the
function describing the smoking initiation rate.
The level of smokers is the population that is currently smoking.
These smokers either die at the rate of the "smoker death rate", or quit
smoking, in accord with the "smoking quit rate" and become ex-smokers.
Ex-smokers are that part of the population that smoked for some time
but have quit the smoking habit permanently.
Once becoming an ex-smoker,
these people leave the level by dying at the
rate shown by the "ex-smoker
death rate".
We chose this representation of the population for several reasons.
First, the three levels can easily be distinguished by the two rates,
initiation and quits.
Second, it is clear that these three populations have
different death rates, which is a key variable in this model.
This is also
why smokers can become ex-smokers by quitting but ex-smokers (inthis model)
cannot become smokers again by reinitiating.
Ex-smokers are represented
here as individuals who have given up smoking permanently and are thus very
distinguishable from smokers.
For our initial model equilibrium conditions, we wanted the proportions
of the population in these three levels to be equivalent to proportions reported in Statistical Abstracts of the U.S. for the year 1970.
From the
statistics, we generated figures of 45% for potential smokers, 37% for smokers
and 18% for ex-smokers.
The various death rates were determined by estimating the number of
-7-
The
years an individual on the average spends in any one of the levels.
life expectancy of a potential smoker was taken as 74 years, an
73 years, and a smoker, 69 years.
ex-smoker,
From the data we also estimated that
smokers are on the average five years older than potential smokers and
ex-smokers are on the average eighteen years older than potential smokers.
The actual numbers used for life expectancy and average age did not
affect significantly the simulation results produced by the model.
The
normal Quit fraction and the normal Initiation fraction were calculated so
that the initial proportions of the three levels remained constant. The relative proportions of these three population levels during the simulated
time period are determined by the initiation rate and the quit rate.
Figure 3. Factors Affecting Initiation of Smoking
Tobacco
TrAl.
,
-,v/
Societal Approval
)fSmoking
Restrictions
on
'rice of
Cigarettes
Smoking
Perceived
Hazards
Anti-Smoking
Campaign
The initiation rate is decreased by increases in restrictions on smoking
(such as a restriction in sales), perceived hazards of smoking (individuals
are less likely to initiate if the perceived hazards of smoking are higher),
anti-smoking campaign activities and the price of cigarettes.
It is in
turn increased by increases in societal approval of smoking (people are more
likely to initiate when society has more positive attitudes towards smoking),
and the tobacco industry's lobbying and promotional expenditures.
III
-8The quit rate is in turn increased with an increase in perceived hazards
of smoking and anti-smoking campaign activities, while it is decreased by an
increase in societal approval of smoking and tobacco industry spending.
Figure 4. Factors Affecting Quitting Rate
Tobacco
Industry
Spending
Anti-Smoking
Campaign
Approval
of
Smoking
- -'
Perceived
Hazards
+
--
Societal approval of smoking is the society's acceptability of smoking.
The forces of the tobacco industry and the anti-smoking campaign act in opposite directions to each other in trying to sway public opinion about smoking.
Figure 5. Societal Approval of Smoking and its Consequences
Anti-Smoking
Campaign
Tobacco
Industry
Spending
on
Smoking
Rate
Rate
As societal approval goes up, the effort to impose more restrictions goes
down as does the tendency to or ability to quit.
If societal approval
rises, the likelihood and acceptability of initiation goes up.
The smokers' death rate is influenced by two factors, the intensity
of smoking and the level of contaminants in the cigarettes, in addition to
other non-smoking influences upon death rate.
-9Figure 6. Influer:es on Smokers' Death Rate
I -+ - Death
Intensity
Contaminants
Rate
Ideified
Maladies
As the death rate goes up, it becomes easier for maladies due to smoking to
become identified.
In the same way, as contaminants and intensity go up, it becomes easier
to identify maladies.
Figure 7. Influences on Identified Maladies due to Smoking
mrL'erc
I
_
'JIIVICG
Death
Rate
Perceived
Hazards
Intens
Conta
As more maladies become identified or more unequivocally demonstrated, the
perceived hazards of smoking increase.
The increase in the level of perceived hazards affects the behavior of
smokers. More try to withdraw from smoking or at least to cut down on
Figure 8.
Consequences of Perceived Hazards
Identified
Maladies
--
__1_·_1___;_1___II_
_______
_·__
_____
ctio.ns on Smoking
ate
tion Rate
i ty
iinants
- --
11
-I U-
intensity and begin to smoke cigarettes with lower tar and nicotine content,
decreasing the contaminant content.
With a higher level of perceived
hazards also comes more public pressure to increase the restrictions on smoking.
Among additional elements included in the model are perceived impacts
of smoking on non-smokers, subsidies to the tobacco industry, support and
impacts of health research, social tension, tobacco industry lobbying, and
others.
Reference Mode Data and Computer Simulation
For Vital and Health Statistics the U.S. Public Health Service interviews approximately 50,000 families to determine the characteristics of the
population in terms of smoking.
The results (discounting for the section
"unknown if ever smoked") for several years are included below:
Year
Sex
Present
Smokers
Ex-Smokers %
Potential Smokers %
%
1965
M
F
avg.
51.1
33.3
42.2
19.3
7.9
13.6
29.6
58.8
44.2
1967
M
F
avg.
49.1
32.1
40.5
18.7
7.2
12.9
32.2
60.7
46.5
1968
M
F
avg.
47.0
31.2
39.1
19.7
8.1
13.9
33.4
60.7
47.1
1970
M
F
avg.
44.4
31.7
38.0
26.2
11.6
18.9
31.5
58.7
45.1
1974
M
F
avg.
42.5
31.9
37.2
27.2
12.5
19.8
30.2
55.7
42.9
Table 1. Data on U.S. Smoking Populations
The trends can be seen in the following graphs.
-11-
Figure 9.- Population by Smoking Status
I
___
I
m
1
__
.
3
.. .I . .
-t----
----
I-
·. F
.
....
j -.: .I .
tI .
. .i
I-
FI
.i. .. .. ..
: ..
I
-- I
I~": :
....
..
,,
.
7777
· ..., , f --
I
_
l
'------!
- -I -
.
..
I
.- .
.']
[.
-
.
I
.. I
II
iI-
'-ii-ii!:
; ;I;,,
.~
. :
.i
I
t.... . II
..
'' ..
· ,
i
:
1
f'·-·,··-I
·
.'i
,
':::[;:::i
t" POTENTIAL .
SMOKERS
. I·
.
i
-i
--I
..--
'.
.
iif!
...
i-.i
' 1
... I
.. ; --
I.. .. I
. .--.. : :
-1
t· ·
I
-- -1·-·1
·: i
·:11
·· ·-r ··- ·
----
i----
:::ii::·:
:t :
i
-
-
I
· · · ·· ·
··
------
r : :: :
1·---)-.·
l--·.L....
--r--.
. - t -- ·t-··
( .....
·I
i;
j..
··:·!.:.··
---1-- · f:
· I·
· ·-· · ··1-···i
f
-···r·-·
· ''''i
C:;;e
,···
`' i
-_i
:: i
··
---- e---: 1:: i : : I
- YEAR
I-.
~,i
-FROM VITAL AND HE)
r
...
-,,I'
:~ :
1
cii
-- ;:::ER
~:l
-17
....
.I-' ;!
: ' M·
f.-:
:
...·
·
·-' · I ·· ·L,·
: ' f '''··''
: .
: i :. 1'.:I
7 1
:,:::
--.-i : .I
·· · ·I
i · ··-
i :: t t ::::
.... I'.7 - !I. I ::
r. .~~~
~----;·
tiLL;L
... ... .' !. - . -.- -.. - .. 1I- . ' '
i
i
i
i
.....
i'·"i':- ·.. : .
:-:·'
.:..
I
·:
i
r · ·· ·
!::i.
..
--I :..
... 1....
· ·--
:_t
·
.
II
T-_
ir---·
': · '·-:-·--t-··
'
-- i ·· ·· C···-.:-·
t '···t····l-·;,-·
. j .. '
1- ' ·i · · · ·f · ··1-1
I il
'
.. -
.
1
.....
]:.~__:
i1
i
.~~~~~..
. I
:
: : .: i
.' i
I.
-
· '
t
·· · I
- -·
·- -:...
I--I- !
11'
... .'
i:i-ii:
···.··,·,i
I··-·
::··
I:!
..
-... ,....
i:I
'
I']
1.~i I .
I:
i
L-. -·i_
__·_)·
··- · ····
··.. · · · ·· t : i ·...1----·
------- t------l·- --.i··
· ··
·' ' ' ' '
`'''I..-..
i
....
··
~ . i--. .
. :I
,'..'
.. .
'
i
t1
: : ::
::
-
.'i·
I
Lc,--1
.
I
I
-o
.I,
. I
! - t --
ii
i~
.. . . .. . ..
· 'ij::::
' ' ' ''
.'.. . . ...
.....
.
.
. . . ..
.'.. . . ..
.....
. ..
: :: i
· ' ' ' ` ''
j::
`''''
'~
~~~~~~~~~~T~
~
~.r ...' ' I... .
':T:'t"[·:'i-·
-
POPULATION
i
i~~~~~~~~
:i
ii!l
i! !i
~:~i!:
I1'i ,~~~~~~~~~~~~~~·
t3~
t '~i:::;I':!L~t
I~i
-77
~~: .i...'
~;.....
.. '~~~~
;,'::I
~~~~~I.·i
i':!'' '
I!! !i~-:l:...... Y EAR'
._.(
...... .... .. I ...
I
I
.·
R.QM
I
I
'1···(
"
'
.
'
-
-
!1
1;·-· .,.,..1.....
:~
..
·-,..:.:.~...
I
· ~~~~~~~~~
IT____
.b~~~~~~~L
~~~·
'~
-- r
. ,....)
.·t'::'
iI
--------
.,,_.________._____
-12For our reference mode it would have been difficult to duplicate these
results.
First of all, the statistics themselves are not reliable.
Secondly,
there have been various "impulses" in the system, such as the 1965 Surgeon
General's report.
We were able to have the model duplicate the trends in the smoker and
ex-smoker populations; however, we find the trend in the potential smoker
population puzzling.
The statistics provided were for the population aged
17 years and older, whereas our model is formulated to include all over 12
years.
The dip in the potential smoker percent may be due to population
age fluctuations or to the difference in bases used.
In our model base
run, the potential smoker percent continues to rise.
In the base simulation run of our computer model, the following results
are obtained.
Year
1970
1975
1980
1985
1990
Present Smokers %
Ex-Smokers %
Potential Smokers %
37.00
18.00
45.00
36.37
18.15
45.48
34.45
18.66
46.88
31.53
19.57
48.90
27.74
20.78
51.48
Table 2. Simulated Data on Smoking Populations (Base Run)
The base run has the smoking population decreasing in proportion
while the potential smoker and ex-smoker populations increase in proportion.
Because of the continuing increase in population, the actual number of smokers
does not decrease immediately.
Year
Smokers
1970
1975
1980
1985
1990
74.00
76.40
76.01
73.03
67.48Table 3. Base-Line
Ex-Smokers
Potential Smokers
(populations
in millions)
36.00
90.00
38.12
95,54
41.15
103.41
45.34
113.26
50.54
125.22
Model Projection of Smoking PoDulations
-13Fiqure 10,
PopbTation by Smoking Status,(:iodel
Dase Run)
. 1·· I_ Ji :
L_
!: _.1..
jii L.
__
--
: .: .
i
I'
I
I _ .
i.. · -
i ·· ·
I
I' :
---
i
I
r---tts--
I
. .i '
.. . I -. .
.
',
.
II
: i:. I
.
...
....
i ,i
1-
I.
..
· !
-:!'
,
. ' : I I
t
.
f
r
''!'
____
·i
'- ii
I
:o POTENTIAL
--
cc--r
"
ul-·L
CI--"(
I
: .': :
.
j. SMOKERS
I'.i:.;I .I. I
I
I -
I
.
:. .
':
!I^!
h:--i ....
I
¥-4
-.i .: .
% OF
:
QPULATION .
..
..
. .; :
. ..
· ··r
·
I · -t
·: :: I
---+----i
----· ·-
r--.--;
::-
I
,..
i
.
I i17 i:
.I ,
:
-- L
i ·· .
~':
_.,i_
i .
· ·
.
:;:':,.
ii'
iIj'
'
t-·
Ij
i.]:
;.['
.::
---
i
I.. .
!:
·, ·-
..
.
-A--I--',.'
..;-: LL
i
':;··
.;'
' .',
"ii!SMOKERs'
.. tJ
....
i''~~~~
·'
·'
I '' '
':
'' i
j
ill
ii
I :
1'
:: · r·
I.-
:'
· ""
-'-i
i;;;;
i:
:
: . /:
·' '
:
Iii i
'
i I
"'
)
r
·· · I ·-·
f '·'..
·
%OF~~~~
;: 7-;~ ;!i;
LI!,·*
; t·
:ii!~ii~:1i !
!!;
-:.. ; t:. :
!i i
:
.::;;:
i ii:' tI
·'·· `··'( ' ' ' ' ` 1
II I
--i
: t:: i
;-
·': '
!!::::i i! i li !
':I~~~
ii:~i:~ii:':!
~~
·f · ·I
:
·i
-- I
·: I '
· I:'
__I
·' '
iiii: ...
I :
:
I
·
·:
o..
.. r.;
;
··
·· ·
771
r Ii
;;f
: Ii : :
1:
....
,..
·- ·
:,.~.· . i
::::::.. :I.:
~·...;'.":::
;~!: ,: :' !.-
, :.:i·--
'' ' ' .
.
i :;
~.,1~ ·\ E=SMOKERS'
----
· 1.
i
"-ie
·· I
I ..
-- +--.. ...
: : 11 : i ;
... 1..-.
I .
... ;...
. ....
· [:i fi 1 :
--
:: t.
' ' :'' ':
:
: :
... i
: ...
9
-- ----
::· ::;
:
· t
i I
·t -··
I ·-
1
I r r:1
::
::i- --"Z, ' .... -!-·,
....
'
: II :
:..1. i;.
POPULATION '
- · ··i
·i ·- I
-t
LL!'
: : I -: : : : .I : !. :_i___
"--"-i'T-'"--,,,~""~
"T--`1
i ' :-
I:
'.:
I .. 'I .t
- I -1 -1,
.
f
III
-14The model was run repeatedly for a 40 years simulated duration, beginning in 1970, but we will not attempt to argue in support of the model's
results for more than 20 years because of the many extraneous factors that
may influence the real-world situation beyond the 20 year point.
The following five computer-generated graphics show the trends in
some of the key variables in the base simulation run of the model.
From Graph number 2 we see that the initiation fraction continuously
decreases and the quit fraction increases, which explain the trends in the
population variables.
In the same graph we see that peer pressure, which
is formulated as a function of the smokers/not-smokers ratio, drops also.
This results in a system of four interconnected positive feedback loops
(indicated in Figure 11) which further increases the quit fraction and
decreases the initiation fraction after the first 20 years of the model.
Figure 11. Positive Feedback Loops Involving Peer Pressure
Peer
PresrCcII
%M
MA
-'~
/
-
Quit
Rate
on-Smokers
vCmnrL, n rc
LA-
..l
.II-IV
J
l
+
Societal approval of smoking (Graph 2), which is partly a function
of perceived hazards of smoking, drops.
This is a result of the increase
in perceived hazards of smoking (Graph 3), which is a result of the in-
-15crease in the identified maladies due to the increase in health research
(all in Graph 3).
The decrease in societal approval of smoking eventually leads to an
increase in restrictions on smoking (Graph 4).
The perceived hazards of smoking affect the behavior of smokers as
well by decreasing the intensity of their smoking and the contaminants per
cigarette (by shifts toward lower tar and nicotine cigarettes) (Graph 1).
This decrease results in the decrease in the number of smoking-related maladies per smoker (Graph 1).
This decrease is not enough to overcome the
other factors, such as health research (Graph 3), which continue to increase
the perceived hazards of smoking.
The model, if carried out to 2010, results in potential smokers % = 64.93,
smokers % = 11.97, ex-smokers = 23.1.
This is due to the positive feedback
loops in the system which drive the smoker % to such a low figure.
This is
basically due to the assumption that health research will continue to find
hazards due to smoking.
III
-16-
_II
___
SMOKING-RELATED
MALADIES PER
coU)
X C.()Z
*OC
if,
nr . ALr
lIr
X
C C
"
t
0I
II
i
!
z
I
s,
< - *
·
<
0 * 0 o f.
· '
*
t .
i
I
ce
i
I
r;
I
V-1
0
',
0
-0C
.
.
4
.
C.i
'. o c ,'
",.-*
C..
i
0
*
.0'
.0
*
Ic
NANT
'ION
)KER
I
LI
I'
Z
H
<'*
* C 0 C N
V7H
_
.
.
4o
.
+
·
-
I
I
I
r
J 'PRICE OF
t CIGARETTES
E
X
-3
Lz
X
r
0
C 0
*0
C
C
q
Ls.
CCj
:".
:iiI
E
O
0
,
r
CONTAMINANTS
RELEASED PER
1LIMRL I IL
' C
0
G
IG
''<.0 I
+
*
*
*
*
*
-
'
I
I5
.
4
r
4
*
4
.
4
+
I
4
0
-I
0
0-
0
O~4
0
f.
Graph 1 ( Base Simulation Run)
1-4
N,
-77__
-"
PEER
t~
~
i
"t
i
q~ ¢
i
i
___·_
0~
t~~c
co
0tr!
C.
C
4
.
H
0i
'
-
C
H
*
.
-
*
.
C1.4
.
.
.
I
4.
rC\m
*
.
·
4
4
4
I
I
. z
t
C
<,
*
Li
;
*N
$
*
+
SOCIETAl
I APPROVA
OF SMOK
OMI.
.S&.
•^
I
i N
,-
.-
MP
. .
f\
T-4
t. N
'-i
I
INITIATION
!o
-'
FRACTION
N
N
Ar
'-
*
0
*
*
I
0 0
N, IT
QUIT
_RACTION
*
4
4
*
4
I
IE
I
I
C
I
0
I
I
1
I
I
II
0
CC <I
* *
0O0
-4 C.
I tIEr
V)
I
I
I
I
*
I
*
*
*
.
aC;
3
I
1i4
C3
!i
to
I
I
I
I
I
I
I
ILi
II
H
II
Ci
ii.
*
I,
If
Li
I
I
!
I
I
-0000~
,I
1
*
4
.
4
*
.
i-!
· I
*
*
.
.
*
.
*
i
.
0
-4
0
C..j
I-j
C
I
i
r'-4
ii
L
_r-
__
_---IC-
Graph 2
(Base Simulation Run)
l
III
-18-
TOBACCO
HEALTH
SUBSIDIES
i-I
. <
.
..0 C
.I
O O
Ic
+
IDENTIFIED HAZARDS
OF SMOKING
Z'
, ,
1
C - N ,
* .0
,*N
N 0
Im
r;
7t
IDENTIFIED
SMOKING-RELATED
MALADIES PER
SMOKER
-
N
1-.
*4
N
ICO
b.
%-I
'11
It
*
-i
*
O0
-
04
rq
Ic
U
1:
tt
I
i
t' ,_
0
' Z
!.o
ii
Z
CL
* *·
i
C
*N
IOKE EXPOSURE
O
Z NON SMOKER
.1
C.
I
II
.-
fI
it
g'r
I
I
I
i
Lt
I
I I..
I-f
I!-
! .
to
I
!N
i 3
: <c
i
CL
I
t
0
IT
O-
..
*
*
*.*
I
i
.
- ..
*
4
-
-
4.........................
*
I
I
I
4
0
0
.V-4
NiiI
*
i
V*4
0·
~~~~~~~~~~~~~~~~~
O~~~~~~~~
CD
LGraph 3
(Base Simulation Run)
-19-
'C4L Z'iH
t
:j4
.
.
iO
MT I
.
.
.
.
.
.
.
RF'TMrrTMNI
1-.
DESIRED FRACTION! AL DECREASE IN
i RESTRICTIONS
z
LL
7-1
.
.
U;;
C.
.
.
V.
.
,
.
.
4
*
t
.\
i
:,
I
IN
- *
*
T U` L*N
H.
.rr
.
1,r
.
i
II
im
W
0
I
I
C'L
1-
7-i
I-
t
*T C N M
0
.
!
I.:W
i.
,
.-,
tL
.
S-MOKING DONE
DESIRED IN PUBLIC
DESIRED FRACT-
CC'0 0 i
.
;
.
.
.
.
.
o
! iti
C
1
t
i
IONAL INCREASE I;
RESTRICTIONS
W6
.
FRACTION OF
k
,POLITICAL BI
, TO INCREASE
RESTRICTIONS
s£
0,
oo oo o
o o o
o
.o
i~~~~~~~~~~t
1-4
I_
__
Graph 4 (Base Simulation Run)
III
-20-
CIGARETTE
.RTISING
H
L
<
U LL
*
t
00
O C
·*
O
LL
LLL
·*
*
I
t i
I
INDUSTRY
INCOME
ANTI-SMOKINGFUNDS
Z
i
·
O
*
I
.
4.
ANTI-SMOKING
_LOBBY ING
, .w
£U
.N
.
-SMOKING
YING
TION
,-,
4
0
'0
~-I0
0 -4
C'.J
O0
I /ANTI-SMOKINI
,r f
ADVERTISING
I
_
I
I
I!
·"L
I-4
i<L
N
i
I
II
I
.
0
i-I
i
I
I
I
i
I
i
r.
!
c00000
.
.
1
+
4
II
i
*
4
*
.
0
..
+
..
.
*
...
+
I
0
,.
0
v-4
4
0
N
~c
4
I
I
z
COE.
: CO
C-)
*
*
*
INDUSTRY
I LOBBYING
h.3
0
0
*
n
_q
c~~~~~~~~~~~~~~~
o
0
~~~~~~~r~~.
c .f
z
I-f,
_
Graph 5
(Base Simulation Run)
______
-21Simulated Policy Tests'
We have tested the effects of four possible public policies on the
output of the computer simulation model. These policy alternatives are:
1. Federal contribution to anti-smoking funds;
2. An increase in the price of cigarettes (an effective tax);
3. A reduction in the contaminants in cigarettes;
4. A ban on all pro and con cigarette advertising.
The simulated outcomes of these policies are discussed below.
1. There has been some pressure for the government to spend additional
funds on anti-smoking campaigns.
In this model, when public funds are appro-
priated to an anti-smoking campaign we see a minor impact on the relative
proportions of the population levels and subsequently on the total number
of deaths.
In this model run, by the year 1990 the relative proportions of the
population groups are smokers = 27.44%, potential smokers = 51.77%, exsmokers = 20.79%, compared to the base run results of smokers = 27.-74%,
potential smokers = 51.48%, ex-smokers = 20.78%.
The major changes can be seen in Graph 7, in the way the increase
in anti-smoking funds in 1980 affects advertising and lobbying.
This
results in a minor change in the perceived hazards of smoking (Graph 6)
which causes the minor changes in the population outcomes.
2. The impact of a tripling of price (an effective tax) of cigarettes
was tested on the model.
The increase in price was imposed in 1980.
The
immediate effect on the smoking population was not great (smoker % = 24.31
vs. 27.74 in the base run) but was meaningful.
The increase in price
affected mostly the initiation fraction (Graph 9) and the intensity of
smoking (Graph 8).
-22-
H
*W==
I
i"r_
Ct
C'
* C f
*
* OC.'
I
0'
4
'
°
* -
I
I.. I
-
I
i
i *
i
I
*
I
}
!
-4
i
Ht
0
*
LL
11
4
4
jI
I
-4
±
W
4x
i
0
4
4
c
Lt_
I
*
*
-
,-4 .U' 0
W
*
*
0
.
.
,-41
00
M
I
*
!
W --
I--i
i
-
0
.rq
0
I
I
I-LLI
I-
'-5
I
I
i
~ --t
1
4
*
a
*
i
-
*
H
co
4
I
c3
t
*
1
I
· 3~j
I
*
4
!
*--4
.
I
- I
W
1-4
i
1
I
-
*
4
4
4
4
0
Co0
::
II
1)
WL
~
I
F
i-
*
SMOKING
I
I
*
*L
U')<
I-
·
3 0O
in 0
I·
I
i
0
3Z
L_
i"
L
W
,e
*
+
*
*
-
4$
W
1
L
I
zz
z
W
to
I-I
1.
i
-0
4
*
'* 4
in0
I-r
_
LW
W i
I
:
I-
0
Co
UJ
O0
;D
¢~
W
I
xC)
e4
W
*
1-I
b
4
*
4
.
4
4
0
mI-
i.
c,
I
__
__~-
0
-4
0
..!
I
*
w
Graph 6 (Policy-Test #1: Federal Contribution
to Anti-Smoking Campaign)
(\,
-23-
.Nt
0o
Zr
o4
'
'
=-C,
.
CO.
0
*
<C
<CCC
4'
*
4
4
*I
C
i4. 4.
4
svo f '3 _Y r '
4*
*
e . i
*
" *
*
*
*
1{
;IGARETTE
0C
I
NDUSTRY
!
3
!
I
i
0i
!
LL
*
*
*. ¢1
ANTI-SMOKING
V-
"FUNDS
i
(
ANTI-SMOKING
LOBBYING
FRACTTIN
4.
N-
1!
If
.
_i
-
ZZ
*
4
0
*
C
0
*
.
('*
.
.
4
la
0OC
O
'.4
3
C
0
-SMOKING
!
<Z
Zr
4
0
4
*
.
LO
-i
.
*
0
.
ij
*
4
.
4
4
4
I
ADVERTI
0
0O
'-I
I
j
LOBBYING
Li
(3
(
C
N
t
.I
LL
C
i
000000
0
'
*
+
*
* I
r4
C
*
4
0
0*
N
0-
0Li
*
V-4
.
*
V-4
Z
!-I
Graph 7 (Policy Test #1: Federal Contribution
to Anti-Smoking Campaign)
_
11
__111_1___·_1_··1___
---1___--
0
i
I
~~~~~~~~~~~~~~~~~~~~~~
-24-
z
-
<.
.
*..
n
*ooo
.
O',
N
CL
C.
X
+
C-
'*,M
C',
i
Ti
NN
co
If5
Z
Q3
I
L.3 <: r
* t3
0
* .00
*000
C-~(i 0
I
I
C)
i
Z
W-ioX
Z
)C
+'-
'-
·
· 0
.,i
!. C
'14
LI
_J0
t
AbSUKP IUN
zi,
*j
H
FtK
SMOKER
C
.-
I
*
I
I
I
-
*0
* 0
·
CONTAMINANTS
'RELEASED PER
CIGARETTE
X
OCO
/
0
*
*
"
I
*
4
+
0
0
:
0
0
0
Cl
C
-
11-1 - -
Graph 8 (Policy Test #2:
- -~~~~~~~~~~._
__liF
Effective Tax)
_
_
-
.
~ ~
I-
-25-
* to
<: <
*
.
.
.
.
.
4
I
0CO
,PEER
PRESSURE
I
i
i
(r*: * t3t *
3
30
3,
.*
*
I
i
I
QUIT
FRACTION
I
i
i
00
.
4
.
.
·
.
4
..
aC
.
.
i
.
_
o C
n.
If,
W
0
i)
li
.
.
4.
.~
.
4
00
1-4
ca
-
w
I
I
o
C
I
W
Ii
coco
- I
i
FRACTION
I
-
t
-
Wf
i-U
0
C
fl.
ii
I
I
* g
··
· !
*
*
.....
__
!
*
*
-
4
*
4-
-
I
0
0
01-
~0
N4
i.
__
Graph 9 (Policy Test #2:
.__
I
t-
_·_
.
*
4
·.·_ -L·C--
Effective Tax)
*-·--
--- V-
-263. The third policy evaluated in the model was a reduction in the
contaminant content of cigarettes by 75% in the year 1980.
The "contam-
inants" in cigarettes are here defined to be the causes (admittedly not
yet fully known) of smoking-related maladies and mortality.
This policy
is intended to decrease the direct health risks of smoking.
However,
such a policy has interesting consequences.
In the model run, the smoker
% = 27.00 compared to 27.74 in the base run in the year 1990.
But by the
year 2010 the population by smoking status has the following characteristics:
smoker % - 13.97, potential smokers %
64.96, ex-smoker % = 21.07 compared
to the following results in the base run:
% = 64.38, ex-smoker % = 22.65.
smoker % = 12.97, potential smoker
This policy results in a slight increase in
the long-term projected smoking population!
The total number of deaths in
the 40 year period are 176.80 million in the policy run whereas they are
177.39 for the base run.
Thus, although the smoking population is larger,
the death rate is slightly lower because of the decrease in the contaminant
level.
The initial result of the decrease in contaminants per cigarette is an
increase in intensity (smokers may increase smoking to compensate for the
lower levels of "contaminants" per cigarette).
But this diminishes rapidly
because of the decrease in contaminant absorption per smoker (Graph 10).
The quit rate goes up rapidly at first but levels off (Graph 11) because of the decrease in identified smoking-related maladies per smoker and
the slower rise in perceived hazards (Graph 12), which is all due to the
lower contaminant level.
These results have interesting implications.
If such a policy were
instituted it may reduce maladies and mortality due to smoking but may
-27-
I
.,
.I-
cc
,-
00
.
.
0
Wn
z
.
C:
C-
S9
.0
0 N
i-.
0
0
.-
<
L
- <
-
·i
i
?
.
N *
0 0 0 1
3
£f
,-I
LO
0 X ;r;·
V)C
C'J
i-
O
,q
z
0
0o
I
i
CL
o
O O, t C 0j
.C.fN .ri
z Tq3
,
:
ii
z!
i
I
+ * *
J
. i
0 Vi
*z0
T-4
CO
1,--
RELEASED PER
)(
X
LLJt,
CO
0000
,
.
9
.
-
-
*
C0
XU
1
*
9
.
CIGARETTE
.
+
.
0
.
.
9
9
.
9
ABSORPTION
PER SMOKER
o
0
0O-
t!
0
N.
-- -- -·
I------
-··-- ---
Graph 10 (Policy Test #3:
-------
er·LP·I.-
----91OP·-·ll--
Reduced Contaminants)
111
-28-
r.
C
a:
C
*
·
*··
4
.
4
.·
4
.
.
.·
I
C
R
SSIIRE
a-
a
c
I
I
V-1
0
U
a5
.\QUIT
FRACTION
t
i
i
3
En
Ar
4
II
4
(N
'-4
to
-
-
*
I
.
L
I
I
I
a
I
I
I
I
I
I
i
N
SOCIETAL
0 I
C1.4
'-4
I
V.
In
-p
<r V)01,
C i
W
'-4
0
z(P
I
INITIATION
FRACTION
I
I
I
I
I
I
T-i
*
0
I
I
-iG
*
I
I
I
!
CO
0
I
I
I
f'A*
(N-
CL
a.
LD
<Z
00
0
0-
*
*
*
4
I
4
· 4· ·
I
0
N
0-
0,
IC?
b-
__
Graph 11 (Policy Test #3:
Reduced Contaminants)
0.*4
I
-29-
- 1I
FQ FH
CL
*
.
0C
-
.
NO
I
4
.
.
.
.
.
.
.
.
.
.
.
I
{
I
"r'
.-4
I
-1
0
*
* N
*
*
*
4
!
$4
j
e.
I
i
ER
'-4
t--
-q
i
1-I
i
4
*
-
4
00 O
W
.
i
I
0
W
I
W
(.
W
U.
.
.
:r
I
Wl
i
LJ
I
*- i lV i
*
*
i
.
W
4
}U
C
o3
4
4
4
i
II
I
II
*
C).
}
!
!
I
I
i
W
W
LLt W
CrC
r
*
i;
5c
I
W
I
zi
4
!
tOi
A.
o
.-
!
+
_
I-
I
I
4
.
Fnl
i
CI
00
.
W
I
) C
.
O C
* CO 'i.t
0
0*
*
.0
CJ I
W
W
LLf
i
i
4,
4
4
4
4
. -W
4
.,
I
4
4
4
4
4
0
O'-4
.frl
Graph 12 (Policy Test #3:
Reduced Contaminants)
*
I
0
'
0
N,
i
III
-30increase the number of smokers.
4. The fourth policy tested is to ban all advertising (pro and con)
for cigarettes in 1980.
The results show a faster decrease in the smoker
population than in the base run, smoker % for 1990 = 27.14. This is due
to the fact that the model assumes that the cigarette advertising is a
more powerful influence on smoking than the anti-smoking advertising is
against smoking.
Sensitivity Testing
The model was further tested by performing the following sensitivity
analyses:
1. Tension stepped up by factor of three in 1980;
2. Fraction of smoking permitted in public set equal to zero in 1980;
3. Tension stepped up initially;
4. Effect of societal approval of smoking removed from influencing
health education;
5. Effect of societal approval of smoking removed from influencing
health research;
6. Social learning time increased to fifteen years from ten years;
7. Total identifiable smoking-related maladies decreased to seven
from ten;
8. Tail effect of restrictions on initiation changed;
9. Population growth set equal to zero in 1980;
10.
Smoking-related maladies prevented set equal to 4 instead of 0;
11.
10% noise level in societal approval of smoking.
The results from these sensitivity tests indicate that the model is
as sensitive (or even more so) to these parameter changes as to some of
the policy tests shown previously.
Since most of the relationships in the
.
model were chosen thoughtfully but in fact arbitrarily, this indicates that
the variables in the model must be more accurately determined for the results to be taken seriously.
-31-
*
Limitations of Science in Decision-Making
The smoking model and the experiments conducted with it,as presented
in this paper, provide a case illustration of the limits of science's role
in public policy-oriented decisions.
Beginning with a central concern for
the smoking process and its impact upon morbidity and mortality, the model's
scope includes the forces perceived as important in the development and implementation of policies intended to control and reduce the smoking problem.
Those forces can be acknowledged to include medical, behavioral, economic,
sociological, and political relationships.
Despite the controversy surrounding the Surgeon General's and related
reports, the medical linkages between cigarette smoking and morbidity and
mortality are among the least uncertain of the model formulations. Other
aspects of the model representation, such as the impacts upon health research
funding of society's attitudes towards smoking, are much more speculative in
both structure and parameter values.
The biomedical relationships are better
understood and more reliably measured than are the socio-economic-political
variables.
But to what extent is the methodological approach taken here--of feedback systems representation, quantification and computer simulation analyses-affected by data inadequacies?
Surely the causal loop diagrams themselves
and the logical and/or intuitive conceptualization based on those diagrams,
are not affected by the data limitations described. To the extent public
policy insights into smoking issues can be gained from the process of diagramming or the resulting visual representations, constraints on information
availability are not material.
Ill
-32However, in regard to the computer simulation results the consequences
are different.
For many modelled parameters policy implications are unchanged
over a fairly wide range of numerical values.
Surprisingly, for example,
different mortality assumptions made little impact upon model projections.
But for far too many socio-economic-political relationships, model outcomes
turned out to be very sensitive to assumed changes of relationships that were
well within the bounds of data uncertainty.
In the smoking problem the limits of utility of scientific decisionaiding approaches are set by the limited social science knowledge available.
The authors suspect that the same constraint may dominate many other areas of
public policy formation. The model presented in this paper is only a preliminary representation of the issues and relationships that must critically
affect the development and effectiveness of public policy on the smoking
problem. A serious commitment to coping with the consequences of cigarette
smoking warrants a dedicated multi-disciplinary research effort to elaborate
and provide data support for the approach taken here.