Microbial Risk Assessment for Recreational Use of the
Kallang Basin, Singapore
By
Allison Park
B.S. Civil and Environmental Engineering, 2014
Massachusetts Institute of Technology
Submitted to the Department of Civil and Environmental Engineering
in Partial Fulfillment of the Requirements of the Degree of
Master of Engineering
in Civil and Environmental Engineering
at the
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
-
-
INIE
OF TECHNOLOGY
June 2014
JUN 13 2014
C 2014 Massachusetts Institute of Technology
All rights reserved
LIBRA RIE S
L.RA
Signature redacted
Signature of Author:
Allison Park
Department of Civil and Environmental Engineering
May 9 , 2014
Signature redacted
Certified by:
Peter Shanahan
Senior Lecturer of Civil and Environmental Engineering
(7Thesis
/
Adisor
Accepted by:
Signature redacted
Heidi Nepf
Chair, Departmental Committee for Graduate Students
Microbial Risk Assessment for Recreational Use of the
Kallang Basin, Singapore
By
Allison Park
Submitted to the Department of Civil and Environmental Engineering
on May 9th 2014
in Partial Fulfillment of the Requirements of the Degree of
Master of Engineering in Civil and Environmental Engineering
Abstract
The water quality in the Kallang Basin, Singapore, was analyzed in order to determine how safe
the waters are for recreational users, specifically focusing on dragon-boat racers. The Public
Utilities Board of Singapore has been managing reservoirs under the "Active, Beautiful, and
Clean Waters Programme" in order to help the public recognize the value of their scarce water
sources. Therefore, microbial risk assessments were conducted on locations along the Kallang
Basin to analyze any diurnal or spatial differences in probabilities of illness, and establish
guideline geometric mean concentrations.
Samples were collected at four different locations along the Kallang Basin every four hours
during a 48-hour period. Samples were then analyzed for Enterococci and E. coli using mostprobable-number methods. Adenovirus was analyzed by Liu (2014) using quantitative
polymerase chain reaction. Based on the Wiedenmann et al. (2006) statistics-based risk model,
no-observed-adverse-risk levels or guideline geometric-mean levels were established at 128
colony forming units (CFU) / 100 mL for Enterococci and 697 CFU/ 100 mL for E. coli.
Based on these guideline geometric-mean concentrations, all of the stations exceeded the
tolerable illness level for indicator bacteria at certain times, with peak concentrations at 7:00
A.M. and 11:00 A.M. However, for adenovirus, the probabilities of illness did not exceed the
tolerable level based on appropriate dragon-boat racer ingestion rates. Statistical analysis showed
that a high correlation existed between adenovirus concentrations and E. coli concentrations.
Future studies should analyze specific locations along the Kallang Basin that contribute to high
concentrations of indicator bacteria and viruses.
Thesis Supervisor: Peter Shanahan
Title: Senior Lecturer of Civil and Environmental Engineering
Acknowledgements
First, I would like to thank my thesis advisor, Dr. Peter Shanahan, for his support and
exceptional amount of technical advice. Without him, this thesis would not be in the shape it is
today. Next, I would like to thank my MIT group members who traveled to Singapore with me
for their enthusiasm, support, and passion throughout this process: Justin Angeles, Riana Kernan,
and Tina Liu.
Additionally, I would like to thank the extremely helpful and experienced members of the
National University of Singapore (NUS) for laboratory and field-work assistance. I would
especially like to thank Professor Karina Gin and Ginger Vergara for allowing us to work with
them.
Finally, I would like to thank my family and friends for their love and support throughout. They
provided me with optimism, and taught me the value of hard work and discipline.
Table of Contents
Table of Tables ..................................................................................................................
9
Table of Figures...............................................................................................................
10
1. Introduction.................................................................................................................
11
1.1 Singapore's W ater Sources............................................................................................
1.1.1 Imported W ater.............................................................................................................
1.1.2 Desalination..................................................................................................................
1.1.3 N EW ater.......................................................................................................................
1.1.4 Local Catchment W ater............................................................................................
1.2 ABC Program m e ...............................................................................................................
1.3 K allang River Basin Overview .....................................................................................
1.4 Current Study ....................................................................................................................
11
11
12
12
12
13
14
16
2. Quantitative Risk Assessment of Fecal Indicator Microbes for Recreational Use 18
2.1 Fecal Indicators and Viruses .........................................................................................
18
2.1.1 Coliphage and Adenovirus .......................................................................................
2.1.2 Epidem iological Studies............................................................................................
2.2 Recreational Risk Assessm ent.....................................................................................
2.2.1 Site Characterization ................................................................................................
2.2.2 Risk Quantification...................................................................................................
2.2.3 Risk Management and Communication ..................................................................
2.3 US Standards History...................................................................................................
2.3.1 W orld Health Organization and Singaporean Standards ..........................................
19
20
21
21
22
22
23
24
3. Models Assessing Risk Associated with Microbes ...............................................
3.1 No-O bserved-Adverse-Effect Levels (NOAELs) .......................................................
3.2 van Heerden et al. (2005) Exponential Dose-Response Risk Model...........................
3.2.1 Poisson-Distributed Dose-Response M odel ..............................................................
3.3 Dufour (1984) Risk M odel ............................................................................................
3.4 Fleisher (1991) Risk Equations......................................................................................
3.5 W iedenm ann (2007) Risk Model...................................................................................
3.6 Dufour vs. W iedenm ann M odel ...................................................................................
3.7 Single-Sam ple M axim um Allowable Densities................................................................
26
26
26
27
30
31
31
35
35
37
4. W ater Sam pling A nalyses and O verview .............................................................
37
4.1 Field Sam ple Collection ................................................................................................
37
4.2 Laboratory Analysis.....................................................................................................
37
4.2.1 Enterococci and E. coli Lab Analysis........................................................................
4.2.2 Indicator Bacteria NOAEL and Probability of Illness Derivation............................. 38
4.2.3 Quantitative Polymerase Chain Reaction (PCR) Preparation for Adenovirus Analysis
39
...............................................................................................................................................
40
4.3 W ater Ingestion Calculation..........................................................................................
5. R esults ..........................................................................................................................
7
42
5.1 Indicator Bacteria Results ............................................................................................
5.2 E. coli Results.....................................................................................................................
5.2.1 E. coli Results for Station 2.......................................................................................
5.2.2 . coli Results for Station 3 .......................................................................................
5.2.3 E. coli Results for Station 4.......................................................................................
5.2.4 E. coli Results for Station 5 .......................................................................................
5.2.5 Summary of E. coli Results .......................................................................................
5.3 Enterococci Results .......................................................................................................
5.3.1 Enterococci Results for Station 2 ..............................................................................
5.3.2 Enterococci Results for Station 3 ..............................................................................
5.3.3 Enterococci Results for Station 4 ..............................................................................
5.3.4 Enterococci Results for Station 5 ..............................................................................
5.3.5 Summary of Enterococci Results ..............................................................................
5.4 Adenovirus Results............................................................................................................
5.5 Comparison of Indicator Bacteria and Adenovirus ...................................................
5.5.1 Indicator Bacteria and Adenovirus Relationship.....................................................
5.5.2 Causes for High Indicator Bacteria Concentrations ................................................
6. Conclusion ...................................................................................................................
6.1 Guidelines...........................................................................................................................
6.2 Future Research ................................................................................................................
42
44
44
45
47
48
50
50
50
52
53
55
56
57
61
61
63
66
66
66
References........................................................................................................................
68
Appendix A......................................................................................................................
73
List of Adenovirus samples and concentrations in genomic copies/L.............................
73
Adenovirus quantitative PCR results in genomic copies/L (GC/L) for Station 2 at each time
...............................................................................................................................................
75
Adenovirus quantitative PCR results in genomic copies/L for Station 3 at each time.......... 76
Adenovirus quantitative PCR results in genomic copies/L for Station 4 at each time .......... 77
Adenovirus quantitative PCR results in genomic copies/L for Station 5 at each time .......... 78
Appendix B......................................................................................................................
Raw
Raw
Raw
Raw
Raw
Raw
79
E. coli data for samples collected on January 7 th 2014......................79
E. coli data for samples collected on January 8 th 2014......................80
E. coli data for samples collected on January 9 1h 2014......................81
Enterococci data for samples collected on January 7 th 2014
................. 82
Enterococci data for samples collected on January 8 th 2014
................. 83
Enterococci data for samples collected on January 9 th 2014
................. 84
8
Table of Tables
Table 1:
Table 2:
Table 3:
Table 4:
Table 5:
Table 6:
Table
Table
Table
Table
Table
7:
8:
9:
10:
11:
Table
Table
Table
Table
Table
12:
13:
14:
15:
16:
Table 17:
Table 18:
Table 19:
Table 20:
Indicator Bacteria Density Criteria (USEPA 1986) ............................................
24
WHO Bacterium Guidelines (WHO 2003)..............
..............
25
Findings from van Heerden et al. (2005) to determine concentration of
adenovirus (Eq. 4)...................................................................................................
29
Findings from van Heerden et al. (2005) to determine N (Eq. 3)......................29
Wiedenmann (2007) NOAEL risk equation variables ......................................
38
E. coli and Enterococci geometric mean concentrations of all locations for
each sam pling time ...............................................................................................
42
Station 2 E. coli concentration and probability of illness (%)..........................44
Station 3 E. coli concentration and probability of illness (%)...........................46
Station 4 E. coli concentration and probability of illness (%)..........................47
Station 5 E. coli concentration and probability of illness (%)..........................49
E. coli geometric mean concentrations averaged over all times and
probability of illness (%) at each station............................................................50
Station 2 Enterococci concentration and probability of illness (%).................52
Station 3 Enterococci concentration and probability of illness (%).................52
Station 4 Enterococci concentration and probability of illness (%).................54
Station 5 Enterococci concentration and probability of illness (%).................55
Enterococci geometric mean concentrations at all times and probability of illness
(% ) at each station................................................................................................
56
Adenovirus concentration calculation at each station........................................58
Calculation of N and daily and yearly probability of illness due to adenovirus
exposure for an ingestion rate of 6 mL per day, 156 days of the year..............59
Calculation of N and daily and yearly probability of illness due to adenovirus
exposure for an ingestion rate of 30 mL per day, 365 days of the year.............60
Daily and yearly probabilities of illness due to adenovirus exposure for each day
of sampling, representative of the whole Kallang Basin .....................................
60
9
Table of Figures
Figure 1:
Figure
Figure
Figure
Figure
2:
3:
4:
5:
Catchment Areas (light blue) and Reservoirs (dark blue) in Singapore
(Joshi et al. 2012)..................................................................................................
13
Map showing Entire Marina Basin, including the Kallang Basin (PUB 2013a) .15
Detailed View of Kallang Basin (PUB 2013a).....................................................15
Sampling Locations along the Kallang River Basin (Google Maps 2013).....17
Variations in vinJOOmLfrom Wiedenmann (2007) risk equations per Dixon
(2009)..........................................................................................................................34
Figure 6:
Figure
Figure
Figure
Figure
Figure
Figure
Figure
Figure
Figure
7:
8:
9:
10:
11:
12:
13:
14:
15:
Figure 16:
Figure 17:
Figure 18:
Figure 19:
Figure 20:
Figure 21:
E. coli and Enterococci geometric mean concentrations along the Kallang
Basin in MPN/100 mL versus date and time of day..........................................43
Station 2 E. coli concentration versus date and time .......................................
45
Station 3 E. coli concentration versus date and time ........................................
46
Station 4 E. coli concentration versus date and time ........................................
48
Station 5 E. coli concentration versus date and time ........................................
49
Station 2 Enterococci concentration versus date and time ..............................
51
Station 3 Enterococci concentration versus date and time ..............................
53
Station 4 Enterococci concentration versus date and time ..............................
54
Station 5 Enterococci concentration versus date and time ..............................
56
Probability of illness versus concentration of Enterococci curve at different
intake rates per day ..............................................................................................
57
Station 2 Probability of illness per day versus volume consumed (mL) due to
adenovirus exposure... .......................................................................................
59
Log Adenovirus concentration (viruses/L) versus Log E. coli Concentration
(MPN/ 100 mL) at each station............................................................................62
Log Adenovirus Concentration (viruses/L) versus Log Enterococci
Concentration (MPN/ 100 mL) at each station ................................................
62
Map view of Station 3, Kallang Riverside Park, and Station 4, Upper Boon Keng
Road, upstream of Station 3 (Google Maps 2014)............................................
64
Upstream of Station 4, Upper Boon Keng Road, along the Kallang River
(Google M aps 2014).............................................................................................
64
Upstream of Station 5, Crawford Street (Google Maps 2014)..........................65
10
1. Introduction
Singapore is a densely-populated island nation located in Southeast Asia. Since the 1970s
after the end of British military presence in 1971, Singapore began rapid economic
growth primarily based on manufacturing and trade. However, Singapore's rapid growth
also came with limitations. Because this island nation has no natural aquifers or lakes and
little land to collect rainwater, Singapore has been searching for methods to maximize
water as much as possible. Currently, Singapore's Public Utilities Board (PUB)
creatively manages water supplies and encourages conservation in order to provide the
needed 400 million gallons per day (MGD) to its 5.4 million residents (PUB 2013a).
Further, the needed water supply is expected to double by 2060. To address this growing
demand, Singapore has been increasing supply by tripling water reclamation and
increasing desalination capacity tenfold. The augmentation of these supply processes will
help meet up to 80% of the water demand in 2060. Due to limited water supplies, under
the Active, Beautiful, and Clean Waters Programme discussed in more detail in Section
1.2, the PUB wishes to open up the island's water bodies to recreational use. The PUB
hopes to help the public recognize how precious their water sources are in order to
conserve and protect their supplies for the future.
The current area of focus for this thesis, the Kallang River Basin (Figure and Figure ), is
used for a variety of recreational activities such as dragon- boat racing, water sports,
fishing, and picnicking. However, the PUB has concerns that the bacteriological levels in
the waters may pose health and safety risks for people coming in contact with it. Because
of its intended use for recreational activities, a team of Master of Engineering students
from the Massachusetts Institute of Technology visited Singapore in January 2014 in
order to evaluate the water quality of the basin.
Section 1 of this thesis was written in collaboration with Justin Angeles, Riana Kernan,
and Tina Liu.
1.1 Singapore's Water Sources
Singapore has four water sources: imported water, desalination, reclaimed "NEWater,"
and local catchment water.
1.1.1 Imported Water
Malaysia's Johor State Government and Singapore signed a water agreement in 1961, but
it expired on August 31, 2011. Under a separate water agreement created in 1962,
Singapore is still allowed to draw up to 250 MGD from the Johor River until 2061 (PUB
2013a). Due to the uncertainty of the future of this agreement and the desire to be water
independent, PUB hopes to provide all of its water internally by the expiration of this
agreement in 2061.
11
1.1.2 Desalination
Singapore's first desalination plant, built and operated since 2005, supplies about 30
MGD. The plant was designed to supply water to PUB for a period of 20 years. With
growing demand for water, a second and larger desalination plant, Tuaspring
Desalination Plant, opened in September 2013. This plant supplies an additional 70 MGD
to Singapore's water supply and together the two desalination plants have been able to
supply 25% of Singapore's water needs. However, desalination poses many challenges.
Desalination is energy-intensive and more costly than NEWater or conventional water
treatment, so PUB strives to develop technologies that will reduce this large energy
consumption and cost.
1.1.3 NEWater
Since its introduction in 2003, NEWater has been a source of raw water for potable use.
The process of NEWater uses advanced membrane technologies (microfiltration, reverse
osmosis, and ultraviolet disinfection) in further purifying treated used water. PUB
continuously monitors NEWater quality through water sampling and monitoring
programs. The National University of Singapore (NUS) discovered through extensive
tests that NEWater is of higher purity than PUB water (Soon et al. 2009). Therefore,
NEWater can substitute PUB tap water for use in certain manufacturing processes that
require ultra-clean water. In addition, PUB has incorporated NEWater into drinking water
systems where NEWater is injected into reservoirs, and then the mixed water is further
treated through water treatment plants. The largest NEWater plant located in Changi
supplies about 50 MGD of water. NEWater can currently meet 30% of Singapore's total
water demand with goals of meeting up to 55% by 2060 (PUB 2013a).
1.1.4 Local Catchment Water
Singapore's land area is 716 square kilometers, with two-thirds utilized as water
catchment. Surface water is collected and stored in 17 reservoirs located throughout the
island (Figure 1). Singapore is one of only a few cities around the world that applies
urban storm water harvesting on such a large scale. The extensive use of urban runoff
necessitates the reduction of non-point source pollution and careful management of
surface water quality. PUB's Active, Beautiful, and Clean Waters (ABC Waters)
Programme (Section 1.2) seeks to transform the city's concrete channels, drains, and
reservoirs into more natural looking and sustainably-managed waterways so that
Singapore becomes a "City of Gardens and Water" (PUB 2013a). PUB hopes that these
efforts will help increase water conservation and reduce pollution in Singapore's
waterways, creating a vitalized community.
12
/
r~%.
S
Figure 1 - Catchment Areas (light blue) and Reservoirs (dark blue) in Singapore (Joshi et
al. 2012)
Unfortunately, storm water runoff often contains high levels of bacteria and other
pathogens that may pose risk to human health. Increased public contact with the water
through recreational activities will require extensive monitoring of the water quality. The
goal of this study is to perform risk assessments on local catchment water, specifically
studying the Marina Reservoir watershed, to gain an understanding of the types of risk
posed to recreational users. With these results, the intention is to help PUB achieve their
goals of maintaining an active, beautiful, and clean water system for all to enjoy.
1.2 ABC Programme
In 2006, PUB developed the Active, Beautiful, and Clean Waters (ABC) Programme. As
mentioned, PUB is transforming Singapore's utilitarian drains, canals, and reservoirs into
streams, rivers, and lakes to be well integrated with the surrounding parks and spaces,
while also creating centers for recreational activity. The main intention of this
transformation is to allow Singaporeans to appreciate and cherish their limited natural
water resources.
13
The objectives of the ABC program are based on its acronyms (PUB 2013a):
Active: Bring people closer to the water through recreational activities. Through
these activities, the people will develop a connection with the water to value it and
recognize how precious their water sources are.
Beautiful: Make the reservoirs and waterways aesthetically pleasing and well
integrated with the local surroundings and residential areas.
Clean: Improve the water quality by incorporating retention ponds, aquatic plants,
and fountains to help remove nutrients. Minimize pollution in the waterways
through education and close people-water relationships.
1.3 Kallang River Basin Overview
The Kallang River Basin is located in the southeastern part of the country, just northeast
of downtown Singapore (Figure 3). The three major tributaries that drain into the basin
are the Rochor Canal, the Kallang River, and the Geylang River. Five main waterways
drain into the Marina Basin and include the Singapore River, Stanford Canal, Rochor
Canal, Kallang River, and Geylang River. The basin was created in 2008 by the damming
of the Marina channel by a 350-meter long barrage. The Marina Bay and Kallang Basin
were then converted into freshwater reservoirs. The barrage provides flood protection as
well as another source of drinking water for the people of Singapore (Nauta et al. n.d.).
14
Protected
Catchment
Jnprotectd
Seranloon
Cetchment?
Utban
4Sormwater
Collecfon
Basm
Figure 2 - Map showing Entire Marina Basin, including the Kallang Basin (PUB 2013a)
Figure 3 - Detailed View of Kallang Basin (PUB 2013a)
15
The Kallang River is the largest river in Singapore, spanning 10 kilometers, and the basin
is surrounded by Kampong Bugis to the north, Tanjong Rhu to the south, the Kallang
Stadium area to the east, and the Beach Road area to the west.
Due to extensive recreational usage of the Kallang Basin, the focus of this study is to
determine risk towards human health. From the results of this study, continuous
monitoring and management of runoff and bacterial concentrations from the basin should
be established to evaluate the microbial diversity and determine the risks associated.
1.4 Current Study
The Kallang Basin and the rivers that drain into it have become popular venues for
recreational activities such as dragon- boat racing where hundreds of teams race against
each other. Within the Kallang River, various dragon- boat racing clubs have practices
and competitive sessions during the weekends. It is also an area where leisurely dragonboat racing can occur for Singaporeans to practice and learn the sport. As mentioned, due
to great recreational activity within this basin, it is extremely important to determine
health risks associated with such use of the area. Further, analyzing viral pathogens using
traditional indicator risk models may pose a challenge, so this study translates extensive
field data of viral pathogens and indicator bacterial concentrations into various potential
risk models. In addition, spatial and diurnal risk differences may result depending on
sampling location and time. Based on the results from this study, the locations and times
along the Kallang Basin contributing the highest probabilities of illness could be
extremely valuable for regulatory agencies to protect recreational users.
The data collected during January 2014 will be used in this study with a statistics-based
risk model and exponential dose-response model to determine the probability of illness to
recreational users of the Kallang Basin. Additionally, the correlation between indicator
bacteria and adenovirus will be determined using linear regression.
16
F4
.
1
.|
-ml
U
7
Figure 4 - Sampling Locations along the Kallang River Basin (Google Maps 2013)
17
2. Quantitative Risk Assessment of Fecal Indicator Microbes
for Recreational Use
2.1 Fecal Indicators and Viruses
The current criteria for evaluating human risk due to recreational activity are based on
water quality measurements of fecal indicator bacterial concentration. Due to the
innumerable species of pathogens and the difficulty of detecting them easily, indicator
organisms are used as an alternative method for measuring environmental water quality.
An indicator organism provides evidence of the presence of a pathogen surviving under
similar environments, physically and chemically. According to Wade et al. (2003),
studies have shown that Enterococci and . coli are the most effective primary indicators
for predicting the presence of pathogens and specifically those causing gastrointestinal
illness.
The following characteristics are fundamental in establishing the reliability of an
indicator. Specifically for fecal contamination, indicator organisms should be able to do
the following (Sloat and Ziel 1992; Thomann and Mueller 1987):
*
*
*
*
Be easily detected using simple laboratory tests
Not be present in unpolluted waters
Be present in concentrations related to the extent of contamination
Have a die-off rate not faster than the die-off rate of the pathogens of interest
Unfortunately, many studies have shown that indicators may not accurately predict the
presence of waterborne human pathogenic viruses. For instance, preliminary evidence has
shown that F coli and Enterococci may be naturally detected in tropical regions without
a source of contamination based on a study conducted by researchers at the University of
Puerto Rico in 1991 (Hernandez-Delgado et al. 1991). Therefore, van Heerden et al.
(2005) evaluated the possibility of directly using human enteric viruses such as human
adenovirus as improved fecal contamination indicators. Many different types of
adenovirus (51) cause a wide range of infections involving gastrointestinal, respiratory,
and urinary tracts. The presence of these viruses in water used for drinking or recreational
use pose potential health risks. Adenoviruses also occur in large numbers in many water
environments, and these viruses are exceptionally resistant to purification and
disinfection processes (USEPA 1998).
Statistical tools have been established to assess the probability of illness constituted by
enteric viruses and other pathogens in water used for human consumption. The U.S.
Environmental Protection Agency (USEPA 1986) recommended a tolerable risk of one
18
infection per 10,000 consumers per year for drinking water. For recreational waters, the
agency has recommended a tolerable risk of one infection per 1000 bathers per day. For
fresh water Enterococci and E. coil, the acceptable level of risk or probability of illness is
8 cases of highly credible gastro-intestinal illness per 1000 swimmers. The guideline
level for Enterococci is 33 colony- forming units (CFU) per 100 mL, and 126 CFU per
100 mL for E. coli. The USEPA (1986) used the Dufour model discussed in detail in
Section 3.3 to establish guideline levels for recreational waters.
A study by Rose et al. (1987) found enteroviruses and rotaviruses in many samples that
had been considered acceptable by indicator bacteria standards. The main conclusions
from the study were that bacterial indicator occurrence did not correlate well with viral
occurrence and that in a majority of the studies that monitored marine waters for both
bacterial indicators and pathogenic viruses, viruses were detected when indicator levels
were below public health water quality threshold levels.
2.1.1 Coliphage and Adenovirus
As discussed in Section 2.1 above, E. coli bacteria and fecal Enterococci are the most
common indicators used in water quality testing. In 2006, coliphage, or bacteriophage in
the coliform group of bacteria, was considered an equivalent fecal indicator to E. coli
according to the Ground Water Rule (GWR) (US Federal Register, 2006). Coliphage
effectiveness as a fecal indicator was verified by 20 years of epidemiological data
showing that over 50% of waterborne illnesses in the United States were viral in origin
(USEPA 2006b). Further, due to the many challenges of using traditional indicators,
especially in tropical waters where bacterial indicators may occur naturally, researchers
have been searching for more accurate indicators to quantify risk from bacteria and
enteric viruses. One of the potential alternatives is coliphage, which are bacterial viruses
that attack E. coli. Male-specific coliphage are released through fecal matter and are
unable to replicate naturally in the water without the presence of coliform bacteria
(USEPA 2001 a). Therefore, coliphages can be useful indicators of water pollution.
Unfortunately, coliphage testing is more complicated than E. coli testing. For instance,
the official method of coliphage qualitative assessment, EPA Method 1601, uses many
steps and reagents. It also takes over 48 hours to complete and obtain results. Therefore,
due to the complexity and labor involved, it is very unlikely that regulators and
municipalities would perform coliphage tests. Now, with the recognition in the GWR that
viral indicators are an equivalent indicator to E. coli, there are now more efforts to
simplify processes.
Another alternative is to detect enteric viruses directly using molecular methods such as
quantitative polymerase chain reaction (PCR). This alternative is the preferred method
because it eliminates any uncertainties of using bacterial fecal indicators and can be used
to directly detect viruses, which do not replicate well in cell cultures (Pina et al. 1998). A
study conducted at the Nanyang Technological University in Singapore analyzed the
19
prevalence and genotypes of pathogenic viruses in wastewaters in tropical regions (Gin
and Aw 2010). Results showed that adenoviruses, astroviruses, and noroviruses were
detected in 100% of the sewage and secondary effluent. There was widespread
occurrence of tested enteric viruses in urban wastewaters in Singapore.
As mentioned in Section 2.1, adenoviruses occur in many water environments, and these
viruses are extremely resistant to disinfection processes (Eischeid et al. 2009 and
Nwachuku et al. 2005). Adenovirus types 40 and 41 cause most of adenovirus-associated
gastroenteritis and are quite resistant to conventional methods of disinfection, have a high
excretion rate in infected individuals, and are extremely persistent in the environment
(Enriquez et al. 1995, Kuo et al. 2010 and Rigotto et al. 2011). For these reasons, the
presence of adenovirus 40 and 41 in recreational waters poses a large health concern.
A study was conducted on coastal waters in Southern California that analyzed the
correlation between human adenovirus and coliphage in urban runoff (Jiang et al. 2001).
The results showed that a significant correlation did not exist between adenovirus and
somatic coliphage (r=0.32), but a significant correlation did in fact exist between
adenovirus and F-specific coliphage (r-0.99). Two types of coliphage, somatic coliphage
and male-specific (F+) coliphage, have a subtle difference. Male-specific coliphages are
viruses that infect through the F-pilus of male strain E. coli, and somatic coliphages are
viruses that infect the outer cell membrane of E. coli host cells (USEPA 2001b).
2.1.2 Epidemiological Studies
The primary purpose of conducting epidemiological studies is to determine the causes of
diseases and identify methods to prevent and manage them (Fosgate and Cohent 2008).
Dufour (1984) and Wiedenmann et al. (2006) sought to determine the relative
probabilities of illness associated with recreational use of waters based on chosen
indicator bacteria. Dufour (1984) developed a log-linear model analyzing fecal coliforms,
E. coli, and fecal streptococci or Enterococci. Wiedenmann et al. (2006) developed a
statistics-based risk model analyzing E.co/i, Enterococci, Clostridiumperfingens, and
coliphage. Both of these epidemiological studies tested for adverse health effects of
gastro-intestinal disease. Dufour's study was a freshwater, prospective-cohort study,
where he recruited participants who already used the water for recreational use.
Wiedenmann et al. (2006) conducted the first randomized-controlled-trial that looked at
freshwater recreational use risks. Measuring the risk associated with recreational water
depends on many factors. For instance, sampling locations are chosen based on complete
exposure pathways available to recreational users. The choice of indicator bacteria
depends on historical regulatory use as well as availability of epidemiological studies.
This availability provides a quantitative relationship between the indicator bacteria and
probability of illness. The studies by Wiedenmann et al. (2006) took place at five
freshwater beaches in Germany. A large group of participants (2,196) was recruited prior
to recreational contact, and participation and exposure to water were strictly controlled.
20
The participants were allowed to swim for ten minutes, and were instructed to completely
immerse their heads in the water at least three times. Every twenty minutes, samples were
taken to analyze the microbial activity within the waters (Wiedenmann et al. 2006). Nonswimmers were not allowed to have any contact with the water. Phone interviews were
conducted one week and three weeks after exposure to track illness rates. Wiedenmann et
al. (2006) found that E. coli and Enterococci were well correlated with rates of illness.
Section 3.3 and Section 3.5 discuss the Dufour (1984) and Wiedenmann et al. (2006)
recreational epidemiological studies in more detail and how risk models were derived
based on those studies.
2.2 Recreational Risk Assessment
Environmental risk assessment involves the three phases of site characterization, risk
quantification, and risk management and communication. Site characterization describes
how users are exposed to pathogens within a specific site. Risk quantification, which
includes a newer field of quantitative microbial health risk assessment, focuses on the
concentration of particular pathogens that humans may become exposed to from
recreational activity (USEPA 1998). Quantitative microbial health risk assessment
follows the four-step process of hazard identification, exposure assessment, doseresponse analysis (probability of illness), and risk characterization (determining how
much infection would arise in a population exposed to a distribution of pathogens in the
water). Risk management and communication require the participation of a relevant
regulatory agency in order to develop any necessary rules or regulations (Dixon 2009).
Dose-response analyses use the terminology "risk of illness" and "probability of illness"
interchangeably. Their difference is quite subtle, but should be clarified. Risk is closely
related to the probability of illness, except risk incorporates this probability in addition to
any consequence of the event (Holton 2004). For instance, the probability of contracting
gastrointestinal illness from a certain water body may be slim, but the consequences for
the user may be quite severe and harmful to his/her health.
2.2.1 Site Characterization
Site characterization involves the development of an exposure model for current or
anticipated use of a site. In the exposure model for microbial contamination, the three
primary sources are water, sediment, and surficial soil. For each of those sources, three
possible exposure routes for pathogens involve dermal contact, inhalation, and ingestion
(Haas et al. 1999). There is a fundamental difference between future primary contact
(e.g., swimming) and future secondary contact (e.g., boating) for recreational users.
Secondary-contact recreational users are exposed to the water and sediment for a shorter
duration, so they are exposed to fewer pathogens (Dixon 2009). A complete exposure
pathway would include a potential user exposed to pathogenic bacteria through an
21
established exposure route. Specifically for this study along the Kallang Basin, a potential
exposure pathway for dragon-boat racers is exposure to pathogens in the water via
ingestion.
2.2.2 Risk Quantification
Risk quantification involves calculating the dose to which the potential users are exposed.
Dose is calculated by analyzing the concentration of pathogens. Since concentrations may
differ based on location and time, the geometric mean value of samples must be taken. In
addition, dose calculation requires the amount of source medium that the potential user
has been exposed to and the concentration of pathogens in the medium. Taking a single
event exposure and multiplying by the number of likely exposures can calculate dose
over multiple exposures (Dixon 2009).
A relationship exists between the dose of the contaminant and the response of the user
through a set of equations. Microbial risk relationships assume that risk increases with
increased dose of microbial pathogens that users are exposed to. However, the
relationship between the dose and response for indicator bacteria is often not known and
has been assumed to follow a log-linear relationship (Dufour 1984), a logistic
relationship (Fleisher 1991; Wymer & Dufour 2002), and a statistics-based model
(Wiedenmann 2007).
2.2.3 Risk Management and Communication
The final step after determining the amount of risk posed to users is risk management and
communication. In order to manage the risk and communicate that risk to future users,
guidelines and standards of acceptable bacterial concentration must be established. If
guidelines are exceeded for certain water bodies, the area must be closed and the risk
must be communicated to potential users.
Two types of regulatory criteria exist to assess the water quality within recreational areas.
The first is the guideline based on geometric mean concentration. The USEPA uses the
geometric mean concentrations and single-sample maximums method (Dixon 2009). The
regulation is that if the geometric mean of the last five water sample concentrations
exceeds the geometric mean guideline, or if a single-sample concentration exceeds the
single-sample maximum, then that body of water should be closed to recreation. The
geometric mean guideline indicates the level of bacteria that provides an acceptable level
of risk to the public. The second type of criterion is used by the World Health
Organization (WHO), which uses a 95th percentile value. A water body is considered safe
for recreational use if the 95th percentile value of all samples is below guideline levels
(WHO 2003). Singapore currently uses the 95 th percentile value method in evaluating
water quality safety for recreational users (SGNEA 2008).
22
This study in Singapore focuses on quantifying risk from waterborne pathogens to
recreational users by specifically analyzing traditional indicator bacteria and
nontraditional human adenovirus along the Kallang Basin. Indicator bacteria will be
analyzed using the relationships found in previous epidemiological studies. Adenovirus
concentration will be gathered via quantitative polymerase chain reaction (PCR), and
probability of illness will be quantified via an exponential dose-response model. Studies
have quantified inhalation adenovirus risk by an exponential dose-response relationship,
and inhalation dose-response appears to be a conservative estimator for ingestion (Couch
et al. 1969). The primary exposure route to dragon boat racers for this study is ingestion
of the water. Section 4.3 explains how this exposure route for these racers was
determined.
2.3 US Standards History
Determining guidelines for proper management of the Kallang Basin requires
understanding current and historical standards. The American Public Health Association
on Bathing Places established the first standard for total coliform counts in the mid- 193 Os
with a concentration of 1000 total coliform forming units (CFU) per 100 mL, even
without conducting epidemiological studies to support that concentration (APHA 1936).
Then, epidemiological studies were conducted in the late 1940s. The United States Public
Health Service (USPHS) conducted them with the goals of establishing safe bacterial
levels, but the USPHS did not have enough data to accurately predict probabilities of
illness from the concentrations of total coliforms (Dufour 1984). In 1968, the National
Technical Advisory Committee on Water Quality Criteria (NTAC 1968) recommended
using fecal coliforms as opposed to total coliforms as bacterial indicators. The Federal
Water Pollution Control Administration then recommended a level of 200 fecal coliforms
per 100 mL. In 1972, the USEPA made this standard official based on research that
showed reduced numbers of Salmonella infections below that level (USEPA 1972).
Due to the lack of studies relating the risk of illness to the concentration of indicator
bacteria in the water, epidemiological studies were conducted at fresh and marine water
swimming areas starting in 1973. The results of these studies produced regression
equations relating swimming-associated gastrointestinal symptom rates with the
geometric mean E. coli and Enterococci density per 100 mL of freshwater (Dufour 1984).
In 1986, the USEPA recommended a probability of illness of 8 illnesses per 1000
swimmers, which means that there is an additional 0.8 percent chance above normal
environmental infection rates that a swimmer will contract gastroenteritis from a single
swimming event (USEPA 1986).
The USEPA standards summarized in the table below were based on full contact
immersion swimming, which is also known as primary-contact recreation (USEPA 1986).
23
Secondary contact activities refer to boating, wading, and fishing. Many US states apply
the single-sample maximum allowable density for Moderate Full-Body-Contact
Recreation as the standard for secondary recreation. Moderate Full-Body-Contact
Recreation refers to recreational waters that are not designated beach waters, but during
recreation season are used by about half of the people as a designated beach area
(USEPA 2004a). The Designated Beach Area single-sample maximum is commonly
used as the standard for primary recreation (Dixon 2009).
Table 1: Indicator Bacteria Density Criteria (USEPA 1986)
Single-sample Maximum Allowable Density
(Enterococci/1 00 mL)
Steady State
Geometric
Mean
Indicator
Density
(Enterococci/
100 mL)
Designated
Beach Area
(upper 75%
C.L.)
Moderate
Full-BodyContact
Recreation
(upper 82%
C.L.)
Lightly Used
Full-BodyContact
Recreation
(upper 90%
C.L.)
Infrequently
Used FullBody-Contact
Recreation
(upper 95%
C.L.)
Enterococci
33
61
78
107
151
E. coli
126
235
298
409
575
C.L. = Confidence Limit
Dixon (2009) expressed that the current standards do not adequately account for different
usages of recreational waters. However, it is possible to test for many more microbial
agents directly instead of relying on indicator bacteria using techniques such as
quantitative polymerase chain reaction (PCR).
2.3.1 World Health Organization and Singaporean Standards
The World Health Organization (WHO 2003) proposed guidelines dealing with many
factors that affect recreational waters, including drowning, bacterial water quality, and
dangerous aquatic organisms. The WHO recommendations included guideline indicator
bacteria, but instead of using a geometric mean guideline, the WHO used a 9 5 th percentile
method for measuring bacterial concentrations (WHO 2003). Under this
recommendation, 95% of the water samples taken should fall below the guideline values
in order for the waters to be considered safe. Current Singaporean standards for marine
and freshwaters are organized based on class levels, which depend on estimated
gastrointestinal probability per exposure, respiratory disease, and 9 5 th percentile value of
indicator bacteria. Singapore standards follow the WHO recommended guidelines, with
goals of achieving at least Class B level for their recreational waters (SGNEA 2008).
Following Table 2 below, this goal corresponds to a guideline 9 5 th percentile level of 200
Enterococci per 100 mL or less.
24
Table 2: WHO Bacterium Guidelines (WHO 2003)
Class
95th percentile value of
Enterococci/100 mL
Estimated Probability per Exposure
Gastrointestinal illnessdies
Acute febrile respiratory
disease
A
<40
<1%
<0.3%
B
41-200
1-5%
0.3-1.9%
C
201-500
5-10%
1.9-3.9%
D
>500
>10%
>3.9%
25
3. Models Assessing Risk Associated with Microbes
Dose-response models are mathematical functions that yield a probability of an adverse
health effect as a function of dose. USEPA (2011) described dose-response models for
waterborne pathogens. The most common practice of dose-response modeling has been
through fitting experimental data to statistical models. The models are almost exclusively
focused on the ingestion route of exposure.
3.1 No-Observed-Adverse-Effect Levels (NOAELs)
A no-observed-adverse-effect level (NOAEL) is the bacterial concentration below which
probabilities of illness for recreational users are no different than the environmental rate
of illness (Dixon 2009). Wiedenmann et al. (2006) determined a NOAEL of 25
Enterococci colony-forming units (CFU) per 100 mL for swimming, and a NOAEL of
100 E. coli CFU per 100 mL. Wade et al. (2003) determined the probability of
gastrointestinal (GI) illness in relation to water quality indicator density in various types
of water bodies. The results of their fresh water study showed that concentrations below
the guideline value or NOAEL for E. coli and Enterococci were not associated with
illness. However, exposures to concentrations above the guideline level were. There was
evidence that the probability of contracting a GI illness was considerably lower in studies
with indicator densities below guidelines proposed by the USEPA. Dufour (1984)
recommended a NOAEL of 33 Enterococci CFU per 100 mL and 126 E. coli CFU per
100 mL, which is the current geometric mean concentration guideline used by the
USEPA today (Table 1). Section 3.3 and Section 3.5 discuss the Dufour and
Wiedenmann models in more detail, with descriptions of how their NOAELs were
determined.
The following models utilize various equations that include parameters and constants to
describe factors known to influence relations between fecal indicator bacterial organisms
and incidence rates of infectious diseases. The dose-response relationships for bacterial
indicators are often not known and have been modeled based on the Dufour (1984) and
Wiedenmann (2007) models. The dose-response relationship for adenoviruses is known
and has been modeled based on studies conducted by van Heerden et al. (2005).
3.2 van Heerden et al. (2005) Exponential Dose-Response Risk Model
Van Heerden et al. (2005) used an exponential dose-response model to assess the risk of
infection caused by human adenovirus detected in a river and impoundment used for
recreational purposes.
26
3.2.1 Poisson-Distributed Dose-Response Model
When the probability of ingesting a dose of pathogens is Poisson-distributed and all of
the ingested pathogens have an equal probability of causing illness, the result is an
exponential dose-response model of the form:
P (d, r) = 1 - erd
(1)
Where:
P, = probability of illness
d= dose or number of pathogens
r = probability that an individual pathogen initiates infection
When the probability of ingesting a dose of pathogens is Poisson-distributed and the
probability that the individual pathogens initiate infection is beta-distributed, a betaPoisson model is appropriate:
Pi(d,1a,
)
,if#>> land#>> a
=
For risk characterization of E. coil, a beta-Poisson model is commonly used with a and
values of 0.178 and 1.78 x 106 (Haas et al. 1999). The exponential and beta-Poisson
models both assume that the number of organisms is Poisson-distributed with a fixed
mean (USEPA 2011).
(2)
p
An exponential dose-response model is most commonly used to evaluate the risk
associated with exposure to viruses (USEPA 2011). For the exponential model, r is a
constant for the interaction between the pathogen and the host. Despite the unrealistic
assumption that all individuals within a population have the same probability of illness,
the exponential model provides a good fit for a number of human-pathogen data sets
(Haas et al. 1999). Once the pathogen is identified in the recreational water, exposure
analyses can be completed. An exposure analysis consists of four terms, the average
concentration of viruses in the water, the efficiency of the recovery procedure, the
viability of the viruses, and the average volume of water consumed per individual. The
efficiency of the recovery procedure refers to the efficiency of the method used for the
recovery of human adenovirus from water samples. This value was estimated at 40%
based on the findings by Grabow and Taylor (1993), Vilagines et al. (1993) and Vilaginds
et al. (1997). Viability of the viruses refers to infectivity. For instance, in van Heerden et
al. (2005), all of the adenoviruses were considered viable and infectious because they
were able to infect their cell culture and at least replicate their nucleic acid. Daily
exposure is determined using the following equation (van Heerden et al. 2005):
N = C * R1 *1* V *
27
1 0 DR
(3)
Where:
C= average concentration of the human adenovirus in the recreational
water (viruses
L
R = efficiency of the recovery method (%)
I= fraction of detected human adenovirus that is capable of infection
DR = removal efficiency
V= volume consumed (L)day
van Heerden et al. (2005) assumed that the daily volume of water consumed during
swimming in recreational water was 30 mL for healthy adults as supported by Crabtree et
al. (1997). The concentration of viruses was determined using PCR, using detected and
undetected methods (van Heerden et al. 2005).
The average concentration of human adenovirus was characterized by:
C=
A(4)
mean volume of water analyzed
Where:
X = -ln[P(0)]
P(0) = 1-fraction of positives detected by PCR.
Parameters used by van Heerden et al. (2005) are summarized in Table 3 for drinking
water, river water, and impoundments from locations in South Africa.
The exponential dose- response model used to assess the risk of human adenovirus is as
follows:
Pi = I - e-rN(3
Where:
P,= the probability of illness
N= number of viruses ingested using (Eq.3) above
r = dose-response parameter as seen in (Table 4)
28
Table 3 - Findings from van Heerden et al. (2005) to determine concentration of adenovirus
(Eq. 4)
Drinking water supplies
Equation or
_______
_______
Supply B
Supply A
Units
______
River water
Impoundment
_____
Poisson parameter (2)
X = -ln[P(O)]
0.03
0.06
0.15
0.19
Mean volume (V)
(L)
212.7
247.8
27.0
194.7
5.46 x 10-3
9.97 x 10~4
C= X)V
Human adenovirus
1.40 x 10-4
2.45
x
10- 4
viruses
concentration (C)
L
Table 4 - Findings from van Heerden et al. (2005) to determine N (Eq. 3)
Mean value of drinking
supplies
Model
parameters
Mean value
(river
water)
Mean value
(impoundment)
Supply A
Supply B
Human
adenovirus
1.40 x 10-4
2.45 x 10-4
5.46 x 10-3
concentration
(C)
Recovery (R)
0.4
0.4
0.4
Infectivity (1)
1
1
1
reduction
(DR)
NA
NA
NA
NA
Volume
2
2
0.03
0.03
9.97
x
10-4
Units
Viruses/L
0.4
Decimal
consumed (1/)
Dose-response
parameter (r)
0.4172
_
0.4172
I
0.4172
I
A
L/day
0.4172
_I
The exponential dose-response model can be modified to determine the probability of
illness per year (Haas et al. 1999):
P
Pi
year
day)
365
(6)
A drawback to this exponential dose-response model is that the probabilities of illness
calculated may overestimate the actual risk due to unknown inaccuracies in assumed
29
values for variables. For instance, the 30 mL of recreational water ingested per day may
be too high for recreational dragon-boat racing, as the racers are not physically swimming
in the water while rowing. Ingestion would occur with a volume much less than 30 mL.
3.3 Dufour (1984) Risk Model
The USEPA currently uses the Dufour (1984) risk model to estimate risk for freshwater
recreation. Dufour (1984) conducted an epidemiological study at fresh water beaches in
Lake Erie, Pennsylvania and Keystone Lake, Oklahoma in order to develop a set of risk
equations that linked the concentrations of E. coli or Enterococci in the water to the
probability of contracting gastrointestinal illness. The study measured rates of illness
among both swimmers and non-swimmers through the use of follow-up surveys
conducted by phone eight to ten days after the beach visit. Swimmers were defined as
those having complete exposure of the head to the water and non-swimmers were defined
as those who did not immerse their heads in the water. Dufour graphed probability of
illness per 1,000 people (P) versus Enterococci concentration (CEN in CFU/1 00 mL) and
he was able to develop the following relationship between illness rate and bacteria
indicator density:
Pi = -4.5 + 14.3
HCGI Pi = -
6 .3
*
log(CEN)
+ 9 .4 *log10(CEN)
(7
(8)
Gastrointestinal illness (GI) refers to symptoms such as vomiting, diarrhea, stomachache,
or nausea, whereas highly-credible gastrointestinal illness (HCGI) refers to symptoms
such as vomiting, diarrhea with a fever, stomach ache, or nausea occurring together with
abdominal cramps. For example, a HCGI symptom is diarrhea and abdominal cramps
occurring together or nausea and abdominal cramps occurring together (USEPA 2006).
3.3.1 Criticisms of the Dufour Model
Dixon (2009) summarized problems with the Dufour risk equations and the USEPA
guidelines derived from them. For instance, the risk equations may not have been
accurate due to the calculation of the geometric means of the bacterial concentrations
over the span of a whole year. Using yearly geometric mean eliminates many data points
that may have influenced the risk equations. Further, the standard deviation was not
included in the original analysis and non-swimmer illness rates were taken from many
locations.
Additionally, the Dufour studies were prospective-cohort studies, where participants were
recruited from people who had already been exposed to recreational waters. These
swimmers and non-swimmers were interviewed at specific recreational locations and a
30
follow up survey was conducted 8 to 10 days later to determine illness rates. There were
no attempts to control the amount of exposure. However, in a randomized trial conducted
by Wiedenmann et al. (2006), participants were recruited before they had any contact
with the recreational waters. The locations, the amount of time in the water, and the type
of exposure were strictly controlled. Randomized trials are a more accurate way to
determine dose-response relationships. Unfortunately, prospective-cohort studies are
often used due to the expense and difficulty in controlling and designing randomized
trials (Dixon 2009).
3.4 Fleisher (1991) Risk Equations
Fleisher (1991) criticized the Dufour risk equations and developed a logistic regression
model that reanalyzed Dufour's 1984 data from studies conducted on marine water. The
criticism was that the log-linear model of Dufour's epidemiological data was incorrect.
The logistic regression model specifies the probability of illness directly and is generally
found to follow an s-shaped curve, with response increasing slowly at low doses, then
more quickly at medium doses, and then again more slowly at higher doses. The general
formula follows Eq 9 below (Wymer & Dufour 2002):
(1+e-(a+Px))()
Where:
P = probability of contracting gastrointestinal illness from recreational
water use
a and 3 = terms that describe the shape of the risk curve and can be
found by fitting the risk curve to data from the epidemiological study
x = logio of indicator bacterial concentration
When Fleisher constructed his series of risk models, he came to the conclusion that
Dufour's general risk equations were inaccurate and needed to be reevaluated. Fleisher
constructed his model by separating the data from the three locations used in Dufour's
marine studies. The risk varied quite significantly between each location, so Fleisher
concluded that the Dufour risk equations were not useful and should be reevaluated
(Fleisher 1991).
3.5 Wiedenmann (2007) Risk Model
The Wiedenmann (2007) model will be used in this thesis to assess the probability of
illness associated with fecal indicator bacterial organisms. Based on epidemiological
studies, this specific model developed by Wiedenmann (2007) describes the probability
of acquiring infectious diseases from bathing in recreational waters with increasing levels
of fecal indicator organisms. Wiedenmann et al. (2006) conducted the first randomized
31
controlled trial for recreational exposure. Swimmers were allowed to swim for ten
minutes and each dunked their heads in the water at least three times. Microbial samples
were analyzed every twenty minutes and Wiedenmann found that E. coli and Enterococci
were well correlated with rates of illness.
In Wiedenmann's derived risk model, these components were included: (1) a baseline
risk, or the risk of acquiring the same kind of disease in an unexposed control group, (2)
an attributable risk, or the risk due to exposure, (3) a dose risk, or a risk level that is
reached when all susceptible individuals have been infected, (4) a functional form
describing the dose-response relationship, (5) a pathogen-indicator ratio, (6) an estimate
of the accidental volume intake of water, and (7) an estimate of the probability of illness.
The pathogen-indicator ratio multiplied by the concentration of fecal indicator organisms
describes the conversion of direct pathogen measurement to fecal indicator bacteria
concentrations (Wiedenmann 2007).
The following equations describe risk in terms of the probability of becoming ill:
MR (Maximum Risk Level) = BR + AR
(10)
Where:
BR = baseline risk (%)
AR = attributable risk (%)
For gastroenteritis, BR ranges from 0.01 to 0.03 or I to 3% (Pruss 1998).
AR = ARwr + ARdr
(11)
Where:
AR.,= risk attributable to the exposure to water, but is independent of the
dose or concentration of the pathogen or fecal indicator organisms
ARdr= dose-related attributable risk
ARr is risk that does not depend on the dose or concentration of the pathogenic
organisms (POs) or fecal indicator organisms (FIOs). For instance, swallowing water
with high salinity content may also cause negative gastrointestinal symptoms. Ardr is the
risk dependent on the dose of the POs or FIOs in the water (Wiedenmann 2007).
The probability of illness, Y, is:
Y = BR + ARwr + ARdrmax
* f(x)DRR
Where:
Y= probability of illness
x = dose or the intake of a certain number of pathogens
ARdrax = dose-related maximal attributable risk
32
(12)
f(x)DRR
is based on a binomial distribution. If x is the concentration of pathogens per 100
mL of water, then the dose is the concentration, x, multiplied by the average volume
intake of water in 100-mL units (vinbooiL). That is, for a swimmer who ingests 30 mL of
water, the value of vinOOm,.L = 30 mL/100 mL = 0.3. ARd,,ax is the risk level reached when
all susceptible individuals have been infected (Wiedenmann 2007).
Y = BR + ARwr + ARdrmax
*
f(xpo
* vinl1OmL)
(13)
If x is not the dose of a certain number of pathogens, but the dose of a certain number of
fecal indicator organisms, then the dose is the concentration of the fecal indicator
organism per 100 mL, multiplied by the pathogenic organism ratio, multiplied by the
volume intake of water in 1 00-mL units.
Y = BR + ARwr + ARdrmax
*
f (XFIO
*
PIR * vin100mL)
(14)
We can simplify this equation by assuming that the cumulative probability of infection,
P(X < x), resulting from the ingestion of x number of pathogenic organisms can be
described by the cumulative distribution function of a binomial distribution with:
F(x) = 1 - [1 - P(1)]x
(15)
Where:
P(1) = the probability of illness associated with the single intake of a
pathogenic organism
Based on experimental observations between the concentrations of E coli and intestinal
Enterococci in fresh and marine water conducted by Borrego et al. (1990), Dizer et al.
(2005), WHO (2003), and Wiedenmann et al. (2004), the following equations show the
relationship between the number of pathogenic organisms (xpo), the number of fecal
indicator organisms (xFIO), and the pathogen-indicator ratio (PIR):
PIR =
q
= log 1 0 (
)
XFIO
= -0.67 + 0.98 * log 1 0 (')
(16)
(17)
Ward et al. (1986) modeled experimental dose-response data in human volunteers for
rotavirus and suggested a P(1) of 0.17. Wiedenmann (2007) set parameters at baseline
risk (BR) = 0.03; maximum risk level (MR) = 0.09; pathogen-indicator ratio (PIR) = 0.1;
and ingestion rate per 100 mL (vintoo,, = 0.3. With these values, risk is calculated as:
33
Risk = (MR - BR) * {1 - [1 - P(1)]z}
(18)
in which z is the number of pathogens ingested defined as:
z = PIR * XFIO
*
v
1
(19)
OOmL
Where:
MR = 0.09 = maximum risk level
BR = 0.03 = baseline risk level
PIR = 0.1 = pathogen-indicator ratio
VinlOOmL = 0.3 = water ingestion rate as fraction of 100 mL
P(J) = 0.17
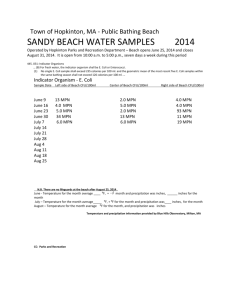
Dixon found that adjusting the value of PIR by some factor resulted in an approximately
proportional inverse change in the NOAEL, Figure 5. Multiplying PIR by 10 decreased
the NOAEL by 10 while multiplying the PIR by 1/10 increased the NOAEL by 10.
Therefore, due to the lower ingestion rate for dragon-boat racers by a factor of 5 (Section
4.3), a proportional increase in the NOAEL resulted.
I
Vl
-
5%-
S
I
I
0
2k -
I
-
-NOAEL
__
2%
Ow' Maa
*0
V~
1225
1
10
51
100
CRU Enteoccoc/unit of ingstion
1,000
Figure 5: Variations in vinllooL (defined as v in Figure 5) from Wiedenmann (2007) risk
equations per Dixon (2009). Additional Risk of Gastroenteritis is equivalent to the
Probability of Illness evaluated in this study.
34
Fecal indicator organism (XFIO) concentrations were measured along the Kallang Basin,
and an appropriate value of viniooml was determined based on dragon- boat racing
ingestion rates per event for adults.
Several problems exist with the Wiedenmann model; however, the derivation of the PIR
term is the main problem. Wiedenmann (2007) assumed a non-constant pathogenindicator ratio (PIR) that varies with XFIO. In this derivation, Wiedenmann assumed an
ingestion rate of 30 mL for the 10-minute swimming period. The assumed 30-mL
ingestion rate seems to be highly conservative because research by Dufour (1984)
showed that adult swimmers ingested about 4 mL in a 10-minute period. Therefore, the
actual PIR is most likely to be higher than the one calculated by Wiedenmann.
3.6 Dufour vs. Wiedenmann Model
Major differences exist between the Dufour and Wiedenmann models. First, the Dufour
model was based on a prospective-cohort epidemiological study, whereas Wiedenmann
used a randomized trial. These fundamental differences are significant because Dufour
did not strictly control how his users interacted with the water. For instance, Dufour did
not control the amount of water ingested by his recruits or the amount of time spent
swimming. He also did not control the age of the participant. The Dufour model also did
not model the pathogen-indicator ratio. The data collected were averaged, and only two
variables were used to model the different factors that influence risk to recreational users.
On the other hand, since Wiedenmann controlled for many of the variables that influence
users, the values of PIR= 0.1, MR= 0.09, and BR = 0.03 were derived through his
epidemiological study (Eq. 18 and Eq. 19). There is variability in the PIR since it may be
significantly lower in tropical climates than in temperate climates (Hernandez-Delgado et
al. 1991).
Overall, the Wiedenmann model provides a more accurate quantification of the amount
of risk to recreational users than the Dufour model. The data used to generate the
Wiedenmann model are much more controlled and account for more variables that
Dufour ignores. Also, since the Wiedenmann model accounts for different ingestion rates
and PIRs, it is much more flexible. Therefore, the Wiedenmann model will be used in this
study of the Kallang Basin to analyze indicator bacteria and probabilities of illness to
dragon- boat racers.
35
3.7 Single-Sample Maximum Allowable Densities
In addition to determining exposure risk due to recreational activity, single-sample
maximum allowable densities can also be constructed for a given water body. Exceeding
the value of a single-sample maximum (SSM) will indicate that the mean indicator
density is higher than the acceptable risk level (Dixon 2009). The SSM should be
customized for the water body of interest, so the statistical distribution of the indicator
bacteria or virus must be determined. According to the USEPA (1986), the SSM for a
specific water body is the one-sided upper confidence level. USEPA (2002) recommends
two methods for calculating the SSM of a given log-normal distribution. While it is
recommended that an SSM be calculated for each water body, this is not always done.
According to Dixon (2009), none of the states have adopted SSMs that have been
adjusted for the different characteristics of each water body due to the large number of
recreational water bodies that are regulated. This large number of water bodies makes it
difficult to customize regulations for each one.
36
4. Water Sampling Analyses and Overview
4.1 Field Sample Collection
The field sampling process was completed in collaboration with a large team from the
National University of Singapore. Water samples were collected from four separate
stations along the Kallang Basin and tested for adenoviruses and indicator bacteria. These
four stations were Jalan Benaan Kapal, Kallang Riverside Park, Upper Boon Keng Road,
and Crawford Street. Water samples were collected over a 48-hour period, at 4-hour
intervals starting on January 7 th, 2014 at 11 A.M., and ending January 9 th 2014 at 7 A.M.
Concentrations of indicator bacteria were analyzed using IDEXX (IDEXX Laboratories,
Inc., Westbrook, Maine, USA) MPN trays. The most probable number of colony forming
units or CFUs was read from IDEXX-supplied MPN tables. Human adenovirus was
identified using quantitative PCR, which was conducted in a separate laboratory setting.
Samples were collected at the four locations by using a bucket and rope to pull up the
water. Twenty liters of water were collected at each station during each sampling session.
Once the water was gathered, samples were taken into the lab to concentrate further.
4.2 Laboratory Analysis
From each 20-L sample collected at the four sites along the Kallang Basin, a final volume
was concentrated to 100 mL via a peristaltic pump and hollow fiber Hemoflow F HF80
hollow-fiber filters (Fresenius Medical Care, Hochtaunuskreis, Hesse, Germany). The
100-mL concentrated sample was eluted using 300 mL of 0.05-M glycine at pH 7. The
final volume including the elution was 400 mL, of which 200 mL was used for secondary
precipitation for the adenovirus analysis. The remaining 200 mL was used to prepare the
Enterococci and E. coli samples.
4.2.1 Enterococci and E. coli Lab Analysis
Enterococci and E. coli samples were analyzed using IDEXX Enterolert and Colilert
media and Quanti-Tray/2000 MPN trays. Aliquots of concentrated reservoir water
samples were diluted with deionized water into 1 00-mL samples. These samples were
combined with the Enterolert and Colilert packets and mixed in sterile whirl packs. The
samples were poured into a Quanti-Tray/2000 MPN tray, sealed, and labeled with the
location, time, and type of microbe. The sealed trays were then placed in an incubator set
at 37'C. After 24 hours, the samples were removed and read using a light-box with a
365-nm UV light. The numbers of positives and negatives counted were recorded and
then the most probable number of colony forming units (CFU) per 100 mL was read from
the IDEXX-provided MPN table (IDEXX Laboratories, Inc., Westbrook, Maine, USA).
37
4.2.2 Indicator Bacteria NOAEL and Probability of Illness Derivation
The NOAEL or guideline level for Enterococci concentrations in the basin was calculated
using the Wiedenmann (2007) risk equation (Eqs. 18 and 19) and the values of the
variables shown in Table 5. These guideline levels will predict whether recreational areas
are safe for dragon-boat racers.
Table 5: Wiedenmann (2007) NOAEL risk equation variables:
CEN-NOAEI
MR
0.091
BR
0.028
a
-0.67
b
0.98
25
(MPN/1OO mL)
0.3
Vlf1OOmL
In Table 5, a and b are constants that were found by curve-fitting the risk data from the
epidemiological study conducted by Wiedenmann et al. (2006). The number of pathogens
ingested, represented by the variable z in Eqs. 18 and 19, is the tolerable number
associated with the NOAEL found by Wiedenmann et al. (2006). Wiedenmann (2007)
solved for z in Eq. 19 by substituting the risk equation variable values from Table 5 into
the following modified form of Eq. 19. This modified form was derived by substituting
Eq. 16 and Eq. 17 into Eq. 19. xFIO in Eq. 17 is equal to CEN-NOAEL in Eq. 20 and Eq. 21.
Z
=
vin1 OOmL
* j
(20)
ga+b*lo1O(CEN-NAEL)
Substituting the values of the risk equation variables from Table 5, including the
ingestion rate (vinlfomL) of 0.3 and the NOAEL concentration (CEN-NOAEL) of 25 MPN/100
mL as given by Wiedenmann (2007), z was calculated as 1.5. However, these values are
based on Wiedenmann's presumed ingestion rate of 30 mL by swimmers, while for
dragon-boat racers an ingestion rate of 6 mL is more appropriate as discussed in Section
4.3. The NOAEL for dragon-boat racers was calculated assuming a constant pathogen
ingestion volume, z, but for a different water ingestion rate than that presumed by
Wiedenmann. Therefore, keeping the z value constant at 1.5, a NOAEL was calculated by
using the new ingestion rate of 0.06. Rearranging Eq. 20 to solve for the NOAEL
concentration CEN-NOAEL for dragon-boat racers, we arrive at the equation below:
log1(CEN-NOAEL)
=
1-02
38
*
09
10
(15
+ 0.68
()
Eq. 21 includes the a and b constants from Table 5. Then, Eq. 18 was used to calculate
the probability of becoming ill based on the observed geometric mean concentrations.
Eq. 18 is repeated below.
Pi = (MR - BR) * {1 - [1 - P(1)]z}
(18)
Substituting the values from Table 5, we arrive at the following equation:
Pi = (0. 063) * {1 - (0. 8 3 )1(-0.67098*o10 (CEN
(22)
*vin00mL}
In summary, the NOAEL for Enterococci was calculated using an estimated ingestion
rate of 6 mL for dragon-boat racers. The value of the variable vin00L, which represents
water ingestion per day as a fraction of 100 mL, was set at 6 mL/1 00 mL or 0.06 and Eq.
21 was solved for CEN-NOAEL. Based on those calculations, the guideline concentration of
Enterococci is 128 CFU/100 mL.
Instead of producing new risk equation variables, Wiedenmann (2007) determined the
correlation between microbial parameters using linear regression in order to establish the
NOAEL for E. coli. The following relationship relates the concentration of Enterococci
with the concentration of . coli:
log10(CEN) = 0.836
*
lo10(CE.Coli)
-
0.270
Solving Eq. 23 for CE. coli-NOAEL using 128 CFU/100 mL for CEN-NOAEL, CE. coli-NOAEL
determined to be 697 CFU/100 mL.
(23)
is
4.2.3 Quantitative Polymerase Chain Reaction (PCR) Preparation for
Adenovirus Analysis
Liu (2014) summarized the procedures for quantitative PCR conducted during the
January 2014 sampling and microbial analysis period at the National University of
Singapore (NUS). The quantitative TaqMan PCR assay developed by Jothikumar et al.
(2005) was used to detect adenoviruses in the water samples. After initial RNA
extraction, a real-time TaqMan PCR assay was performed using the QuantiTech Probe
PCR kit (QIAGEN GmbH, Hilden, Germany) in a R.A.P.I.D. real-time PCR system
(BioFire Diagnostics, Inc., Salt Lake City, Utah, USA). Template DNA, forward and
reverse primers, and a fluorogenic probe were used to complete the amplification
reaction. The complete amplification process took approximately 90 minutes, beginning
with a denaturation step at 95'C for 15 minutes. After this initial denaturation step, 45
cycles of a 95'C denaturation step for 10 seconds, a 55 0 C annealing step for 30 seconds,
and a 72'C elongation step for 15 seconds completed the amplification procedure
(Jothikumar et al. 2005).
Initial RNA extraction required the following steps. Samples of 200- mL created from the
original 20 L of bucket water were each transferred to two 50-mL tubes for centrifuging
39
using sterile pipettes. The samples were centrifuged for thirty minutes in order to separate
the liquids from the particulate matter, which included the adenovirus as well as other
bacteria and pathogens. The liquids were discarded. Polyethylene glycol (PEG) was
added to the solids and then mixed thoroughly. Next, chloroform was added in order to
kill any bacteria or pathogens remaining in the sample. The goals were to concentrate the
sample as much as possible in order to isolate the viral RNA because adenoviruses are
resistant to chloroform. The liquids, which contained the adenoviruses, were further
filtered using an Amicon Ultra filter unit (EMD Millipore Corporation, Billerica, MA,
USA). A QIAmp RNA kit (QIAGEN GmbH, Hilden, Germany) was used to isolate the
RNA. Once the samples were concentrated and the RNA isolated, the TaqMan PCR
assay process began in order to determine the number of genomic copies/L of
adenoviruses based on detected and undetected samples.
4.3 Water Ingestion Calculation
Exposure rates for dragon boat racers were estimated using the ingestion rates for
swimming and then adjusted for the relative amounts of water these racers came in
contact with. Two dragon- boat racers of the German Dragons in Singapore were
interviewed on January 17, 2014 about their dragon-boat racing experiences. The
information gathered from these racers was vital towards estimating a water ingestion
rate.
Dragon-boat practice sessions last for about two hours and are conducted twice a week.
Races are generally once a month and can vary in times from 90 seconds to as long as 50
minutes depending on the race distance. Twenty-two crew members race on each boat.
The people in the front keep the pace, while the people in the back are responsible for
maintaining the proper direction of the boat. While the boat rarely capsizes, the most
common mode of exposure is through splashing from the paddles to the face. Due to rare
immersion of their heads during the races or practice sessions, I assumed an average
ingestion rate of approximately one-fifth of that for swimming. This approximation
results in a per-event ingestion rate of about 6 mL for adults. These numbers are averages
because the front rower experiences more splashing to the face than the other members
rowing in different parts of the boat. These numbers are also rough estimates, and any
guidelines or recommendations derived from these numbers should be confirmed from
actual studies conducted on dragon-boat racer exposure.
According to the USEPA Risk Assessment Guidance for Superfund (RAGS) last updated
in 2012, an exposure pathway is complete if there is a source or chemical release from a
source, an exposure area where contact can occur, and an exposure route where contact
can occur (USEPA 2012). Most complete pathways are determined by getting evidence
from monitoring human data indicating chemical effects in the site area. RAGS created a
population/exposure route matrix that could be used to determine potential exposure
40
pathways at a specific site. For instance, for surface waters and recreational usage, the
most common exposure would be through incidental ingestion or dermal contact.
Lifetime contact would occur, and exposure in children may be significantly higher than
in adults. Because most children do not participate in dragon-boat racing, adult exposure
was the focus of this current study.
The rate of water ingestion highly impacts estimating health risks of water recreation.
Two studies were conducted in the summer of 2009 that estimated water ingestion during
limited-contact recreational activities such as canoeing, fishing, kayaking, motor boating,
and rowing, as well as during full-contact activities such as swimming in outdoor pools
(Dorevitch et al. 2010). In the first study conducted in Chicago area surface waters,
survey research methods were used to estimate water ingestion during those activities
among 2705 people. In the other survey, conducted on outdoor swimming pools, a tracer
was used to estimate water ingestion among 662 people participating in full-contact and
limited-contact recreational activities. Results showed that fewer than 2% of canoers and
kayakers ingested 5 mL or more. Swimmers in a pool were 25-50 times more likely to
report swallowing 5 mL of water than those participating in limited-contact exposure.
Dorevitch et al. (2010) found that the mean and upper confidence estimates of water
ingestion during limited-contact recreational activities on surface waters were 3-4 mL
and 10-15 mL. Therefore, the 6 mL conservative estimation of swimming ingestion rates
for dragon- boat racers, taking into account the front-man who ingests more water than
those rowing in the middle or back, appears to be a good approximation for this study.
41
5. Results
5.1 Indicator Bacteria Results
Measured concentrations of . coli and Enterococci (Table 6 and Figure 6) were
compiled in collaboration with Justin Angeles (Angeles 2014). The numbers for the
stations correspond to the order in which samples were taken:
Samples
2
3
4
5
(Jalan Benaan Kapal)
(Kallang Riverside Park)
(Upper Boon Keng Road)
(Crawford Street)
Table 6 and Figure 6 show the geometric mean concentrations at each sampling time
averaged over all sampling locations. This data set is representative of the whole Kallang
Basin, since geometric mean concentrations were taken for all stations at each time of
day. The highest geometric mean concentrations for E coli and Enterococci consistently
occurred during mornings: on January 7th at 11:00 A.M., January 8th at 7:00 A.M., and
January 9th at 7:00 A.M.
Table 6: E. coli and Enterococci geometric mean concentrations of all locations for each
sampling time
E. coli MPN Geometric Mean
(MPN/100 mL)
3504
Enterococci MPN Geometric Mean
(MPN/100 mL)
562
Date
7/1/14
Time
11:00 A.M.
7/1/14
7/1/14
7/1/14
8/1/14
8/1/14
3:00 P.M.
7:00 P.M.
11:00 P.M.
3:00 A.M.
7:00 A.M.
1720
1052
1205
863
1182
51
180
88
403
1112
8/1/14
11:00 A.M.
1165
69
8/1/14
8/1/14
8/1/14
3:00 P.M.
7:00 P.M.
11:00 P.M.
935
234
352
28
287
32
9/1/14
3:00 A.M.
154
24
9/1/14
7:00 A.M.
1298
210
42
7000
6000
50C0
040( 0
Z 30(
0
E. coli
Concentration
S-- Eneooc
Enterococci
20( 10
Concentration
10( 0
0
1/7 6:00 1/7 12:001/7 18:00 1/8 0:00 1/8 6:00 1/8 12:001/8 18:00 1/9 0:00 1/9 6:00 1/9 12:00
Date - Time
Figure 6: E. coli and Enterococci geometric mean concentrations along the Kallang Basin in
MPN/100 mL versus date and time of day
The corresponding probabilities of illness were calculated using the Wiedenmann (2007)
risk equations. All of the E. coli geometric mean concentrations measured in the field
except those at 7:00 P.M. on January 8t, 11:00 P.M. on January 8 th, and 3:00 A.M. on
January 9th exceeded the calculated NOAEL of 697 CFU/100 mL. Enterococci geometric
mean concentrations exceeded the NOAEL of 128 CFU/100 mL on January 7'h at 11:00
A.M. and 7:00 P.M., January 8th at 3:00 A.M., 7:00 A.M., and 7:00 P.M., and on January
9th at 7:00 A.M. For Enterococci concentrations, the geometric mean concentrations
measured at the times of 7 A.M., 11 A.M., and 7 P.M. consistently exceeded this
guideline level, with peak concentrations occurring in the mornings at 7 A.M. and 11
A.M. This result for Enterococci shows that time of day does impact the probability of
illness to recreational users. For instance, 11 A.M., 7 A.M., and 7 P.M. tend to be the
times when the most fecal contamination occurs. However, more in-depth studies should
be conducted over a longer timescale in order to confirm these findings. For E. coli, most
of the concentrations measured exceeded the NOAEL of 697 CFU/100 mL. However,
this NOAEL may be inaccurate because it was calculated via a linear regression of
Enterococci concentrations, with a correlation of 0.79.
43
5.2 E. coli Results
In order to dissect particular stations that may contribute to high geometric mean
concentrations in the Kallang Basin, the probability of illness for each station was
analyzed. The probability of illness was calculated using Eq. 22; however, Eq. 22 was
determined using variables unique to the concentration of Enterococci. Therefore, in
order to calculate the probability of illness for E. coli, the E. coli concentrations were
translated to equivalent Enterococci concentrations using Eq. 23. The probability of
illness was then calculated and is summarized in the sections below.
5.2.1 E. coli Results for Station 2
Results for Station 2 on the Geylang River are shown in Table 7 and Figure 7. Station 2
showed a peak E. coli concentration of 14,300 CFU/l 00 mL and corresponding
probability of illness of 6.1% at 11:00 A.M. on January 8th. Further, all of the
concentrations exceeded the NOAEL of 697 CFU/100 mL except on January 7th at 7:00
P.M., and on January 9th at 3:00 A.M. A NOAEL of 697 CFU/100 mL corresponds to a
probability of illness of 1.5% each time the racers take to the river. This 1.5% was
calculated using Eq. 22, solving for the probability of illness by using the concentration
of Enterococci associated with the NOAEL of the concentration of E. coli , Eq. 23.
Station 2 should be investigated further in order to manage these high probabilities of
illness to dragon-boat racers.
Table 7: Station 2 E. coli concentration and probability of illness (%)
Station 2
E. coi
Date - Time
MPN/100 mL
1/7/14 11:00 A.M.
Enterococci
Computed
Probability
of Illness
MPN/100 mL
(%)
2098
321
3.1%
1/7/14 3:00 P.M.
985
171
1.9%
1/7/14 7:00 P.M.
465
91
1.1%
1/7/14 11:00 P.M.
2224
337
3.2%
1/8/14 3:00 A.M.
1842
288
2.9%
1/8/14 7:00 A.M.
2723
400
3.6%
1/8/14 11:00 A.M.
14300
1601
6.1%
1/8/14 3:00 P.M.
3441
486
4.0%
1/8/14 7:00 P.M.
1133
192
2.1%
1/8/14 11:00 P.M.
1726
273
2.8%
1/9/14 3:00 A.M.
314
66
0.9%
1/9/14 7:00 A.M.
1160
196
2.2%
44
100000
10000
0
1000
697
100
1/7 6:00
1/7 12:00
1/7 18:00
1/8 0:00
1/8 6:00
1/8 12:00
1/8 18:00
1/9 0:00
1/9 6:00
1/9 12:00
Date - Time
Figure 7: Station 2 E. coli concentration versus date and time
5.2.2 E coli Results for Station 3
Results for Station 3, the Kallang River at Kallang Riverside Park just upstream of the
Kallang Basin, are shown in Table 8 and Figure 8. Station 3 showed much lower
concentrations of E. coli compared to those at Station 2. Peak concentrations occurred at
11:00 A.M. on January 7 1h with declining concentrations after this peak. Probabilities of
illness equivalent to the NOAEL were also exceeded on January 7t at 3 P.M. and 7 P.M.
Therefore, because the tolerable illness level was exceeded at Station 3 at certain times of
the day, this location should be investigated further. For instance, high concentrations
seen on January 7th may have resulted from storm events prior to sampling, or weekend
activities that may have impacted the water quality of the basin. In order to properly
manage these high probabilities of illness, activity should be analyzed upstream of
Station 3. Because dragon-boat racers race during these times of peak concentration, the
Kallang Basin should be highly monitored or even closed off to recreation.
45
Table 8: Station 3 E. coli concentration and probability of illness (%)
Station 3
E. coli
Computed
Enterococci
Probability
of Illness
Date - Time
MPN / 100 mL
MPN/ 100 mL
1/7/14 11:00 A.M.
1127
191
(%)
2.1%
1/7/14 3:00 P.M.
863
153
1.8%
1/7/14 7:00 P.M.
862.5
153
1.8%
1/7/14 11:00 P.M.
572.5
109
1.3%
1/8/14 3:00 A.M.
280.5
60
0.8%
1/8/14 7:00 A.M.
371.5
76
1.0%
226
50
0.7%
1/8/14 3:00 P.M.
281.5
60
0.8%
1/8/14 7:00 P.M.
41.4
12
0.2%
1/8/14 11:00 P.M.
55.6
15
0.2%
1/9/14 3:00 A.M.
103
26
0.4%
1/9/14 7:00 A.M.
443
88
1.1%
1/8/14 11:00 A.M.
10000
1000
0 0100
10
1/7 6:00
1/7 12:00
1/7 18:00
1/8 0:00
1/8 6:00
1/8 12:00
1/8 18:00
Date - Time
Figure 8: Station 3 E. coli concentration versus date and time
46
1/9 0:00
1/9 6:00
1/9 12:00
5.2.3 E. coli Results for Station 4
Results for Station 4, upstream in the Kallang River at Upper Boon Keng Road, are
shown in Table 9 and Figure 9. The highest concentrations at Station 4 occurred at 11:00
A.M. and 3:00 P.M. on January 7 th and 7 A.M. on January 8 th. Station 4 showed a similar
trend in E. coli concentration as at Station 3, with declining concentrations after the peak
at 11:00 A.M. Because most of the highest probabilities of illness occurred on January
7 th, storm events or weekend activities may have impacted the water quality of Station 4
as well. Studies should be conducted at this location to determine causes of such high
concentration, and monitoring programs should be put in place to protect dragon-boat
racers during those times.
Table 9: Station 4 E. coli concentration and probability of illness (%)
Station 4
Computed ,
Enterococci
E. coli
Probability
of Illness
Date - Time
MPN / 100 mL
MPN / 100 mL
(%)
1/7/14 11:00 A.M.
4106
563
4.4%
1/7/14 3:00 P.M.
1050
180
2.0%
1/7/14 7:00 P.M.
836
149
1.7%
1/7/14 11:00 P.M.
717
131
1.6%
1/8/14 3:00 A.M.
906
159
1.8%
1/8/14 7:00 A.M.
1046
180
2.0%
1/8/14 11:00 A.M.
420
84
1.1%
1/8/14 3:00 P.M.
591
111
1.4%
1/8/14 7:00 P.M.
269
58
0.8%
1/8/14 11:00 P.M.
233
51
0.7%
1/9/14 3:00 A.M.
134
32
0.4%
1/9/14 7:00 A.M.
278
59
0.8%
47
1
10000
1000
697
100
1/7 6:00
1/7 12:00
1/7 18:00
1/8 0:00
1/8 6:00
1/8 12:00
1/8 18:00
1/9 0:00
1/9 6:00
1/9 12:00
Date - Time
Figure 9: Station 4 E. coli concentration versus date and time
5.2.4 E. coli Results for Station 5
Results for Station 5, the Rochor River at Crawford Street, are shown in Table 10 and
Figure 10. Station 5 showed the highest concentrations of E. coli out of all four stations,
with similar trends as those of Stations 3 and 4. The highest concentrations at Station 5
occurred on January 71h at 11:00 A.M., 3:00 P.M., and 7:00 P.M., with declining
concentrations on January 8th until a sharp peak in concentration at 7:00 A.M. on January
9 th. Since Station 5 showed the highest concentrations out of all the other stations
analyzed along the Kallang Basin, this location may significantly contribute high
probabilities of illness. In order to determine causes of high concentrations, the areas
surrounding Crawford Street are analyzed in greater detail in Section 5.5.2.
48
..............................
"" 1111" I'll-------------....
..
..
.....
.........
..........
..
..........
............
................
.................
.....
..
........
.....
....
-.
.............
Table 10: Station 5 E. coli concentration and probability of illness (%)
Station 5
E. colR
Computed
Enterococci
Probability
Date - Time
MPN / 100 mL
MPN /100 mL
(%)
of Illness
16000
1710
6.1%
1/7/14 3:00 P.M.
9800
1170
5.7%
1/7/14 7:00 P.M.
3650
511
4.2%
1/7/14 11:00 P.M.
2310
348
3.3%
1/8/14 3:00 A.M.
1190
200
2.2%
1/8/14 7:00 A.M.
1840
289
2.9%
1/8/14 11:00 A.M.
1350
223
2.4%
1/8/14 3:00 P.M.
1330
220
2.4%
1/8/14 7:00 P.M.
240
52
0.7%
1/8/14 11:00 P.M.
690
127
1.5%'
1/9/14 3:00 A.M.
128
31
0.4%
1/9/14 7:00 A.M.
20000
2100
6.2%
1/7/14 11:00 A.M.
100000
10000
0
1000
100
1/7 6:00
1/7 12:00
1/7 18:00
1/8 0:00
1/8 6:00
1/8 12:00
1/8 18:00
Date - Time
Figure 10: Station 5 E. coli concentration versus date and time
49
1/9 0:00
1/9 6:00
1/9 12:00
5.2.5 Summary of E. coli Results
Overall, all of the stations showed high concentrations of E. coli, with certain times
experiencing particularly high concentrations that exceeded the tolerable illness level for
dragon-boat racers. All of the stations except Station 2 showed similar trends with peak
concentrations at 11:00 A.M. on January 7 th and declining concentrations on January 8 th
to January 9 th. Station 2 showed a peak concentration at 11:00 A.M. on January 8 th
Overall, 11:00 A.M. seems to be a significant time in the Kallang Basin where
particularly high concentrations occur for E. coli. Because these stations all exceeded the
tolerable illness level at certain times, they should be investigated further in order to
ensure the safety of dragon-boat racers. The locations upstream of these stations are
analyzed in greater detail in Section 5.5.2.
Table 11 shows that Station 2 and Station 5 exceeded the tolerable level for E. coli based
on the geometric mean concentration averaged over all times sampled. The probability of
illness corresponding to the NOAEL for E. coli is 1.5%.
Table 11: E. coli geometric mean concentrations averaged over all times and probability of
illness (%) at each station
E. coli
Computed
Enterococci
Probability
of Illness (%)
Station 2
1600
260
2.7%
Station 3
290
60
0.8%
Station 4
580
110
1.3%
Station 5
1900
290
2.9%
5.3 Enterococci Results
The Enterococci concentrations at each station are similarly analyzed below in order to
determine correlations between E. coli and Enterococci concentrations and assess
whether consistencies in probabilities of illness exist diurnally and spatially.
5.3.1 Enterococci Results for Station 2
Table 11 and Figure 11 show high concentrations at Station 2 on the Geylang River
exceeding the NOAEL of 128 CFU/ 100 mL on January 7th at 11:00 A.M., with a peak
concentration on January 8th at 7:00 A.M. Overall, probabilities of illness due to
Enterococci did not exceed the tolerable level as frequently as probabilities of illness due
to E. coli at Station 2, and the peak Enterococci probability of illness (6.1% at 7 A.M. on
January 8 th) was about the same as the peak E. coli probability of illness (6.1% at 11
A.M. on January 8th in Table 7).
50
......
..
"I'll.."
11,11,11
11",
...............................
........
1 1111
...
.
. ...
..........
..............
- --.................
I..........
1.1
1--- 11111111-..........................
Table 12: Station 2 Enterococci concentration and probability of illness
Station 2
Enterococci
Date - Time
MPN / 100 mL
Probability
of Illness
(%)
1120
5.7%
1/7/14 3:00 P.M.
22
0.3%
1/7/14 7:00 P.M.
54
0.7%
1/7/14 11:00 P.M.
60
0.8%
1/8/14 3:00 A.M.
1010
5.5%
1/8/14 7:00 A.M.
1730
6.1%
20
0.2%
1/8/14 3:00 P.M.
5
0.1%
1/8/14 7:00 P.M.
70
0.9%
1/8/14 11:00 P.M.
22
0.3%
1/9/14 3:00 A.M.
12
0.2%
1/9/14 7:00 A.M.
60
0.8%
1/7/14 11:00 A.M.
1/8/14 11:00 A.M.
(%)
110000
1000
128
100
\VIA
0
r
VV
1
1/7 6:00 1/7 12:001/7 18:00 1/8 0:00 1/8 6:00 1/8 12:001/8 18:00 1/9 0:00 1/9 6:00 1/9 12:00
Date - Time
Figure 11: Station 2 Enterococci concentration versus date and time
51
5.3.2 Enterococci Results for Station 3
Table 13 and Figure 12 show concentrations at Station 3 on the Kallang River exceeding
the tolerable level of 128 MPN/100 mL at 7:00 A.M. on January 8 th and January 9 th, at
3:00 A.M. on January 8 th, and at 11:00 A.M. on January 7 th. These trends are very
similar to the high concentrations of Enterococci at Station 2 as well as the peak
Enterococci geometric mean concentrations in the Kallang Basin, Figure 6. The times at
which concentrations exceeded the tolerable illness level for E. coli at Station 2
correlated well with the times at which concentrations exceeded the tolerable illness level
for Enterococci concentrations at Station 2 and Station 3, 11:00 A.M. on January 7 th and
7:00 A.M. on January 8th
Table 13: Station 3 Enterococci concentration and probability of illness (%)
Station 3
Enterococci
Probability
of Illness
Date - Time
MPN /100 mL
(%)
280
2.8%
1/7/14 3:00 P.M.
30
0.4%
1/7/14 7:00 P.M.
60
0.8%
1/7/14 11:00 P.M.
43
0.6%
1/8/14 3:00 A.M.
88
1.1%
1/8/14 7:00 A.M.
210
2.3%
1/8/14 11:00 A.M.
10
0.2%
1/8/14 3:00 P.M.
17
0.3%
1/8/14 7:00 P.M.
139
1.6%
1/8/14 11:00 P.M.
14
0.2%
1/9/14 3:00 A.M.
12
0.2%
1/9/14 7:00 A.M.
124
1.5%
1/7/14 11:00 A.M.
52
......
...
............
-- . - ----....
..
.......
-- -...........
- ---................
......
.....
.......
.......
.........................
1000
100
10
1/7 6:00 1/7 12:001/7 18:00 1/8 0:00 1/8 6:00 1/8 12:001/8 18:00 1/9 0:00 1/9 6:00 1/9 12:00
Date - Time
Figure 12: Station 3 Enterococci concentration versus date and time
5.3.3 Enterococci Results for Station 4
Table 14 and Figure 13 depict Station 4 upstream on the Kallang River showing similar
trends as those at Station 2 and Station 3, with particularly high concentrations
corresponding to a probability of illness exceeding the tolerable illness level on January
7t at 11:00 A.M. and January 8t" at 7:00 A.M. and 7:00 P.M. The highest concentrations
occurred on January 7th at 11:00 A.M. and January 8t at 7:00 A.M. The times of peak
concentration are consistent throughout Stations 2, 3, and 4. This consistency confirms
the need to investigate those stations further, particularly focusing on activities occurring
upstream of those locations during the mornings around 7:00 A.M. and 11:00 A.M.
53
....
....................
Table 14: Station 4 Enterococci concentration and probability of illness
(%)
Probability
of Illness
(%)
4.9%
Station 4
Enterococci
Date - Time
1/7/14 11:00 A.M.
MPN /100 mL
727
1/7/14 3:00 P.M.
101
1.2%
1/7/14 7:00 P.M.
132
1.6%
1/7/14 11:00 P.M.
87
1.1%
1/8/14 3:00 A.M.
122
1.5%
1/8/14 7:00 A.M.
1732
6.1%
1/8/14 11:00 A.M.
52
0.7%
1/8/14 3:00 P.M.
50
0.7%
1/8/14 7:00 P.M.
403
3.6%
1/8/14 11:00 P.M.
29
0.4%
1/9/14 3:00 A.M.
36
0.5%
1/9/14 7:00 A.M.
107
1.3%
10000
1000
1
128
100
r
-
LI
A
=mud
10
1/7 6:00 1/7 12:001/7 18:00 1/8 0:00 1/8 6:001/8 12:001/8 18:00 1/9 0:00 1/9 6:00 1/9 12:00
Date - Time
Figure 13: Station 4 Enterococci concentration versus date and time
54
5.3.4 Enterococci Results for Station 5
Finally, Table 15 and Figure 14 show the results for Station 5 on the Rochor River.
Station 5 had the highest concentrations out of all four stations analyzed. All of the times
sampled showed concentrations and corresponding probabilities of illness exceeding the
tolerable illness level except for those measured on January 7th at 3:00 P.M., January 8 th
at 11:00 P.M., and January 9 th at 3:00 A.M.. The highest concentrations corresponding to
a probability of illness of 6.3% occurred on January 81h at times 7:00 A.M., 11:00 A.M.,
7:00 P.M., and 3:00 A.M.. The concentrations marked as >2420 represent levels that
were too high to be measured without further dilution on the IDEXX table used to
translate the fraction of positive wells into a concentration of indicator bacteria.
Therefore, the probability of illness for these wells is even higher than those shown in
Table 15.
Table 15: Station 5 Enterococci concentration and probability of illness (%)
Station 5
Enterococci
Date - Time
MPN /100 mL
Probability
of Illness
(%)
1/7/14 11:00 A.M.
435
3.8%
1/7/14 3:00 P.M.
106
1.3%
1/7/14 7:00 P.M.
>2420
6.3%
263
2.7%
1/8/14 3:00 A.M.
>2420
6.3%
1/8/14 7:00 A.M.
>2420
6.3%
1/8/14 11:00 A.M.
>2420
6.3%
1/8/14 3:00 P.M.
126
1.5%
1/8/14 7:00 P.M.
1733
6.1%
1/8/14 11:00 P.M.
1/7/14 11:00 P.M.
110
1.3%
1/9/14 3:00 A.M.
62
0.8%
1/9/14 7:00 A.M.
2420
6.3%
55
10000
1000
0
128
100
10
1/7 6:00 1/7 12:001/7 18:00 1/8 0:00 1/8 6:00 1/8 12:001/8 18:00 1/9 0:00 1/9 6:00 1/9 12:00
Date - Time
Figure 14: Station 5 Enterococci concentration versus date and time
5.3.5 Summary of Enterococci Results
Overall, the times of 7 A.M., 11 A.M., and 7 P.M. consistently had high concentrations of
Enterococci exceeding the tolerable illness level. Table 16 shows that geometric mean
concentrations at all sampling times exceeded the tolerable level at Stations 4 and 5. All
of the stations that exceeded the tolerable probability of illness should be investigated
further in order to develop appropriate regulations to manage these high concentrations.
However, because Stations 2, 3, 4, and 5 all showed high probabilities of illness due to E
coli and Enterococci at certain times that exceeded the tolerable level, these locations are
analyzed in greater detail in Section 5.5.2.
Table 16: Enterococci geometric mean concentrations at all times and probability of illness
(%) at each station
Enterococci
Probability
of Illness (%)
0.9%
Station 2
70
Station 3
50
0.7%
Station 4
130
1.6%
Station 5
580
4.4%
56
Figure 15 shows the probability of illness associated with concentrations of Enterococci
measured at Station 2 with different curves corresponding to different ingestion rates. As
the ingestion rate increases, the probability curve shifts to the left, which suggests that a
higher ingestion rate corresponds to a lower NOAEL. This figure shows that at the 6-mL
dragon-boat-racer ingestion rate (blue line in Figure 15), the probability of illness of
0.015 or 1.5% is at a concentration of 128 MPN/100 mL or the NOAEL for Enterococci.
mL
Probability of Illness vs. Enterococci MPN/100
0.07
0.06
An'5
V_intake= 6 mL
0.04
"1_intake =10 mL
0.03
LV_intake = 20 mL
0.02
------ -
0.01
1
-
--
X V intake = 30 mL
-
-
--
10
100
1000
Enterococci MPN/ 100 mL
10000
Figure 15: Station 2 probability of illness versus concentration of Enterococci curve at
different intake rates per day. The NOAEL (128 CFU/ 100 mL) is associated with a
probability of illness of 1.5% at an intake rate of 6 mL.
5.4 Adenovirus Results
The data presented in this section was compiled in collaboration with Liu (2014) and is
presented in Appendix A. The probability of illness associated with exposure to the
measured concentrations of adenovirus was compared to the Enterococci and E. coli
probabilities of illness in order to determine any diurnal or spatial relationships in the
Kallang Basin. Further, linear regression was conducted to determine whether
correlations exist between indicator bacteria and adenovirus concentrations.
The following discussion suggests that based on the concentrations of adenovirus at each
station for each time sampled, the times of peak concentration were quite inconsistent
compared to the times of peak indicator bacteria peak concentration. There do not seem
57
to be specific times of adenovirus concentration that contribute to high probabilities of
illness from water in the Kallang Basin.
In order to determine the probability of illness associated with adenovirus exposure, the
viral concentrations in terms of genomic copies/L were analyzed. However, since van
Heerden et al. (2005) utilized the number of positives detected by PCR in his exponential
dose-response model, the genomic copies/L had to be translated into number of positives
in order to apply Van Heerden et al.'s model. Following Viau et al. (2011), if one of the
two viral replicates was negative, it was assigned a number of 5 genomic copies/L. If
both of the replicates were negative, the target was considered "not detected." Therefore,
for this current analysis, if one of the replicates produced a negative result, the geometric
mean was taken of the two concentrations, assuming that the negative replicate was
equivalent to 5 genomic copies/L. Based on van Heerden et al. (2005), the number of
"detected" and "not detected" samples was compiled and the fraction of detected samples
was calculated in order to compute the concentration in viruses/L. The concentration in
viruses/L was calculated using Eq. 4, repeated below, using the original mean sample
volume of 20 L:
mean volume of water analyzed
Where:
A=
-ln[P(O)]
P(O) = 1-fraction of positives detected by PCR.
Results of this calculation are shown in Table 17.
Table 17: Adenovirus concentration calculation at each station
Number of
non-positive
adenovirus
detections,
P(O)
i
Concentration
of adenovirus,
C
(viruses /L)
Station 2
0.33
1.1
0.06
Station 3
0.92
0.09
0.004
Station 4
0.68
0.39
0.02
Station 5
0.33
1.1
0.06
N in the exponential dose-response model was calculated using Eq. 3. The probability of
illness was then calculated using Eq. 5, repeated below, with the results shown in Table
18.
Pi = 1 -e -rN
58
(5)
Table 18: Calculation of N and daily and yearly probabilities of illness due to adenovirus
exposure for an ingestion rate of 6 mL per day, 156 days of the year
N
P (%)
Station 2
0.00083
0.034
5
Station 3
0.000065
0.0027
0.4
Station 4
0.00029
0.012
2
Station 5
0.00083
0.034
5
_year (%)
The probability results in Table 18 show that there is a 3/10,000 probability of illness per
day due to adenovirus exposure at Station 2 and Station 5, 1/10,0000 probability at
Station 4, and 3/100,000 probability at Station 3. The acceptable or tolerable risk of
illness for drinking water is one illness per 10,000 consumers per year with an ingestion
rate of 2 L per day. The tolerable risk for recreational waters is one illness per 1000
bathers per day (USEPA 1986) for users consuming 30 mL of water per day of
recreation. This adenovirus tolerable illness level is much lower than the indicator
bacteria tolerable illness level because adenoviruses are pathogens and pose direct
adverse health effects. In contrast, indicator bacteria measure the potential presence of
fecal pathogens, and often do not cause illnesses directly (USEPA 1986). The dragonboat racers are presumed to consume only 6 mL of water per day based on the analysis
presented in Section 4.3. Van Heerden et al. (2005) showed that as the volume of water
consumed or the exposure to water decreased, the probability of illness also decreased, as
shown in Figure 16.
0.002
Cu 0.0018
E.g
0.0016
0.0014
0.0012
0.001
0
0.0008
0.0006
Cu 0.0004
0 0.0002
T4.g
0
1mo
0
5
10
20
15
Volume Consumed (mL)
25
30
Figure 16: Station 2 Probability of illness per day versus volume consumed (mL) due to
adenovirus exposure (van Heerden et al. 2005)
59
The probability of contracting a GI illness increases linearly as the volume of
consumption increases. At 30 mL, which is the assumed volume of consumption for a
swimmer in recreational waters, the probability of contracting an illness due to swimming
in the Kallang Basin tributaries (Table 19) exceeds the tolerable level of 0.01%.
Adenovirus concentrations at Stations 2 and 5 exceed the tolerable risk when normalized
to an ingestion rate of 30 mL per day.
Table 19: Calculation of N and daily and yearly probability of illness due to adenovirus
exposure for an ingestion rate of 30 mL per day, 365 days of the year
Station 2
Station 3
Station 4
Station 5
N
P, (%)
P, year
0.0041
0.00033
0.0015
0.0041
0.17
0.014
0.061
0.17
46
5
20
46
(%)
The tolerable probability of infection of 1 per 1000 bathers per day (0.1%) translates to a
tolerable probability of illness per year of 31% if the users are exposed for 365 days of
the year, or 14% for dragon-boat ingestion if ingesting 3 days per week, for a total of 156
days per year, calculated using Eq. 6 repeated below.
Pi
_
3 65
-
-
year
(6)
day)
For an equivalent ingestion rate of 30 mL per day, Table 19 shows the results. Table 18
shows the yearly probability of illness for an ingestion rate of 6 mL per day for 156 days
per year at each station. Finally, Table 20 shows daily and yearly probabilities of illness
for each day of sampling, representative of the whole Kallang Basin.
Table 20: Daily and yearly probabilities of illness due to adenovirus exposure for each day
of sampling, representative of the whole Kallang Basin
1/7/14
1/8/14
1/9/14
0.58
0.61
0.69
C (viruses/L)
0.029
0.03
0.034
N (viruses)
0.0004
0.00046
0.0005
0.018
0.019
0.022
2.8
2.9
3.0
0.22
0.23
0.26
57
61
Pi(6 mL
)0
Pvear(6 mL)
P
(%)
(30 mL) (%)
P year(30 mL)_/0
55
60
5.5 Comparison of Indicator Bacteria and Adenovirus
5.5.1 Indicator Bacteria and Adenovirus Relationship
Kundu et al. (2013) analyzed the probability of adenovirus illness for primary contact by
adults, primary contact by children, and secondary contact regardless of age in a multiuse coastal watershed. Results showed that seven of eight virus detections occurred when
E. coli concentrations were below the single sample maximum water quality criterion for
recreational activity, and five of eight viral detections occurred when fecal coliforms
were below the corresponding criterion. However, quantitative microbial risk assessment
(QMRA) on adenoviruses showed similar levels of protection to recreational users as risk
assessments conducted on fecal indicator bacteria. In contrast, Viau et al. (2011) found
that there were no associations between occurrence of viruses and fecal indicator
bacterial concentrations. Gastrointestinal risks from viral exposure were generally orders
of magnitude greater than those from bacterial exposures. Their conclusions suggested
that pathogens could have come from both human and nonhuman nonpoint sources,
contributing to the high probabilities of illness.
Results from this study showed that the probability of contracting a gastrointestinal
illness from adenovirus exposure was less than the risk associated with indicator bacteria
exposure (Table 11 and Table 16 versus Table 18 probabilities of illness at each station).
Comparing the probability of illness at each station based on the geometric mean of
concentrations at each time for fecal indicator bacteria (Table 11 and Table 16), Stations
2 and 5 for E. coli exceeded the tolerable probability of illness of 1.5%, and Stations 4
and 5 exceeded this tolerable probability for Enterococci. Based on yearly probability of
illness for swimmer ingestion rates of adenovirus, Stations 2 and 5 exceeded the tolerable
level (Table 19). However, tolerable probabilities of illness were not exceeded when
analyzing dragon-boat racer ingestion rates for adenovirus (Table 18). High probabilities
of illness for indicator bacteria for dragon-boat racers suggest that all of the stations pose
risks to recreational users and thus require proper management.
Further analysis was conducted to determine if there was any correlation between the
probability of illness posed by bacteria and that posed by viruses. Figure 17 shows the
results of a linear regression of the logarithm of the adenovirus concentration at each
station (data from Table 18) with the logarithm of the E coli concentration at each
station (Table 11). The concentration of adenovirus correlated well with the
concentration of E. coli with an R2 value of 0.95 for each station. However, the
concentration of adenovirus did not correlate well with the concentration of Enterococci
(Table 16) with an R2 value of 0.36 (Figure 18). The equation relating the concentration
of adenovirus with the concentration of F. coli is repeated below:
log1(Cdenovirus) =
1.32 *
61
log1(CE.coli) -
5.52
(24)
Log Adenovirus Concentration (viruses/L) vs. Log E. coli
Concentration (MPN/100 mL)
-0.5
-0.7
:
2.2
2.4
2.6
2.8
3.2
3
3.4
-0.9
0"I
-1.1
- 5.5177
y = 1.3221x
2
_-___
__________
-1.3
R
=0
___
-1.5
W
-1.7
-1.9
-2.1
-2.3
-2.5
E. coli Concentration (MPN/100 mL)
Figure 17: Log Adenovirus concentration (viruses/L) versus Log E. coli Concentration
(MPN/ 100 mL) at each station
Log Adenovirus Concentration (viruses/L) vs. Log Enterococci
Concentration (MPN/ 100 mL)
-0.5
1.5
-0.7
2
2.5
U,
-0.9
i
-
-1.1
y = U.6665x - 3.U5P
2
SR
=
-1.3
0.36
-1.5
0
-1.7
-1.9
-2.1
I
-2.3
-2.5
Enterococci Concentration (MPN/ 100 mL)
Figure 18: Log Adenovirus Concentration (viruses/L) versus Log Enterococci
Concentration (MPN/ 100 mL) at each station
62
3
5.5.2 Causes for High Indicator Bacteria Concentrations
Potential causes for high indicator bacteria concentration are analyzed in this section. The
Kallang Basin drains into Station 2, the Geylang River at Jalan Benaan Kapal, seen in
Figure 4. The basin contributes nonpoint source runoff and high concentrations of
bacterial pollution to this station. In addition, many roads run adjacent to Jalan Benaan
Kapal, which may contribute further contamination. Station 3, Kallang Riverside Park is
on the Kallang River, which is downstream of Station 4, Upper Boon Keng Road (Figure
19). Table 11, Table 16, and Table 18 all suggest that Station 4 is more contaminated
than Station 3. Major sources of contamination may exist upstream of Station 4, and
dilution or microbial inactivation during transport downstream to the basin, either
through photolysis or bacterial die-off, may explain the lower concentrations at Station 3.
Upstream of Station 4 is Bishan Park (Figure 20), which may contribute to additional
high concentrations of microbes. This park is 62 hectares and is one of the largest and
most popular parks in Singapore. The Kallang River stretches through the park, and the
Ang Mo Kio housing estates border it, which may produce high concentrations of fecal
bacteria and pathogens during peak activity times.
Rochor Canal leads to the Rochor River, Station 5, which then empties into the Kallang
Basin (Figure 21). The Rochor River is integrated with surrounding developments to
allow the people to enjoy the waterway. Rain gardens are also incorporated into the
Rochor Canal. Station 5 contributed the highest concentrations, but Angeles (2014)
showed that the Rochor River had the lowest flow rate out of the rivers tributary to the
Kallang Basin. Therefore, the high microbial concentration seen at Station 5 may not be
due to any single source, but may more result from the relatively stagnant conditions
associated with this low flow rate. Upstream of the Kallang River, Station 4 had the
largest flow rate, which may also explain high microbial contamination at Station 4.
Overall, regulators should analyze the quality of the water, primarily focusing on the
Kallang River, before allowing further recreational use of the basin, especially during
these peak activity times.
63
VL
Ka
Kalang
A
Fr
Fragrance Hotel
- Lavender
Honig Aik Properiy Pite
Sr Manmatha
Karuneshverar
(Sivan) Temple
der W.
K
Kaang
Lavender
River
KaHang Riverside Park
00004.
oKilo
Rochor River
Figure 19: Map view of Station 3, Kallang Riverside Park, and Station 4, Upper Boon Keng
Road, upstream of Station 3 (Google Maps 2014)
Yahoo 8usiness
AnU
Mefben Seafood 11
Family Health
Wn 6
sEr
0BATM -Ang $ MedicalCentrePte
,
Mo Kio Ave I
UPg
00
W*
ng
Kish
lon
Meg
P
KaIk
M7atr
as~~n
Two Ch6f Eating Place T#~
Md
Ave
The Canopy C ra
SKong Meng San Phortum
~'
r
Kant See Monastery
CU
A.
Figure 20: Upstream of Station 4 - Upper Boon Keng Road, along the Kallang River.
(Google Maps 2014)
64
7
VHoteliidend
The Music Cbinic Pie
/
x\1A~tdIUep
Lif B1s Foundalv
MyDrumscpo 't
Sgfnaloan Neia
~r~aIRc.
Kong PeN Chang
le
BNock HDB
NI uChang Se'oodI
NOrth dge
MuSImcemeler
SantaGrd HotelBugis
A
r,,Mh( n il
SPORTS CT
Figure 21: Upstream of Station 5, Crawford Street (Google Maps 2014)
65
Bar On 0oe
Mectcal Store Pie
I1
6. Conclusion
In order to ensure the safety of recreational users of the Kallang Basin, the PUB must
determine appropriate guidelines. Therefore, microbial risk assessments of indicator
bacteria and adenovirus were conducted on locations along the Kallang Basin. Because
probabilities of illness may vary diurnally and spatially, the risk assessments were based
on concentrations measured at locations along the Kallang Basin during a 48-hour time
period, with samples taken every four hours. Based on guidelines calculated from
statistics-based and exponential dose-response models using appropriate ingestion rates
for dragon-boat racers, Station 2 on the Geylang River; Station 3 on the Kallang River;
Station 4 on the Kallang River upstream; and Station 5 on the Rochor River all exceeded
the tolerable levels of illness for indicator bacteria, especially at 7:00 A.M. and 11:00
A.M. The probabilities of illness for dragon-boat racers did not exceed the tolerable
illness level for exposure to adenoviruses. However, tolerable illness levels were
exceeded when considering swimmer exposure to adenovirus at ingestion rates of 30 mL.
While probabilities of illness were inconsistent among indicator bacteria and adenovirus,
because the stations all exceeded the tolerable levels of illness at certain times of the day,
the PUB should investigate those locations further.
6.1 Guidelines
Based on the statistics-based risk model by Wiedenmann (2007), the guideline geometric
mean concentration for Enterococci is 128 CFU/100 mL and for E. coli, 697 CFU/ 100
mL, corresponding to a probability of illness of 1.5% per recreational day for dragon-boat
racers. Based on the van Heerden et al. (2005) exponential dose-response model for
adenovirus, the tolerable probability of illness per day of 0.1% was not exceeded for
dragon-boat racer ingestion rates of 6 mL per day. However, for swimmer ingestion rates
of 30 mL per day, probabilities of illness exceeded this level at Station 2 and Station 5.
Analyzing the probabilities of illness for each day within the Kallang Basin, the basin is
safe for dragon-boat racers ingesting adenovirus, but not for indicator bacteria, especially
during peak bacterial concentrations at 7:00 A.M. and 11:00 A.M.
6.2 Future Research
Liu (2014) determined the correlation between human adenovirus and coliphage (malespecific and somatic). She analyzed whether viral indicators were effective at specific
sampling locations in the Kallang River Basin, focusing on the detection of coliphages
and adenovirus. Because microbial risk assessments have not been conducted on
coliphages, a future study should investigate potential models based on the correlation
between adenovirus and coliphage. The results of derived risk equations based on the
66
prevalence of coliphage would be vital towards calculating a more accurate risk level for
recreational users of the Kallang Basin.
Also, the locations that exceeded the tolerable levels of illness along the Kallang Basin
should be explored more deeply to determine causes for such high concentrations.
Studies could explore public activities during peak times of high bacterial concentration
in order to determine specific times and locations when the Kallang Basin should be
closely monitored or even closed to recreational use.
Dixon (2009) recommended sampling at various locations along the Kranji Reservoir
during storm events. Dragon-boat racers still race during storms, so a study of the water
quality after a storm event should be conducted to ensure that particularly high microbial
concentrations do not exist during this time in the Kallang Basin. A study conducted by
the Nanyang Technological University (2008) showed that the Kranji Reservoir
experienced significantly higher bacteria densities after storm events than during dry
periods. Further, if probabilities of illness are significantly higher during storms, a study
should be conducted analyzing when dragon-boat racers can safely use the Kallang Basin
after the storms have cleared.
67
References
Angeles, J.V.V. (2014). Water Quality Modelling for Recreational Use in the Kallang River
Basin, Singapore. Master of Engineering thesis. Department of Civil and Environmental
Engineering, Massachusetts Institute of Technology, Cambridge, Massachusetts.
Aw, T.G. and Gin, K.Y.H. "Prevalence and genetic diversity of waterborne pathogenic viruses in
surface waters of tropical urban catchments." JournalofApplied Microbiology, 110(4): 903914 (2010).
Borrego, J. J., Cornax, R., Moriffigo, M. A., Martinez-Manzanares, E., and Romero, P. (1990).
"Coliphages as an indicator of a faecal pollution in water. Their survivial and productive
infectivity in natural aquatic environments." Water Research, 24(1), 111-116.
Couch, R.B. and Knight V. (1969). "The minimal infectious dose of adenovirus type 4; the case
for natural transmission by viral aerosol." Transactions of the American and Climatological
Assocation. 80: 205-211.
Crabtree, K. D., Gerba, C. P., Rose, J. B., and Haas, C. N. (1997). "Waterborne adenoviruses: a
risk assessment." Water Science and Technology, 35, 1-6.
Dixon, C. C. (2009). "Microbial Risk Assessment for Recreational Use of the Kranji Reservoir,
Singapore." Master of Engineering thesis. Department of Civil and Environmental
Engineering, Massachusetts Institute of Technology, Cambridge, Massachusetts.
Dizer, H., Wolf, S., Fischer, M., Lopez-Pila, J. M., Roske, I., and Schmidt, R. (2005). "Die
Novelle der EU-Badegewasserrichtlinie - Aspekte der Risikobewertung bei der
Grenzwertsetzung." BundesgesundheitsblattGesundheitsforschGesundheitsschutz. 48,
607-614.
Dorevitch, S., Panthi, S., Huang, Y., Li, H., Michalek, A.M., Pratap, P., Wroblewski, M., Liu, L.,
Scheff, P.A., Li, A. (2010). "Water Ingestion during Water Recreation." Water Research,
45(5), 2020-2028.
Dufour, A. P. (1984). Health Effects CriteriaforFresh Recreational Waters. No. EPA-600/1-84004. United States Environmental Protection Agency, Research Triangle Park, NC.
Eischeid, A.C., Meyer, J.N., and Linden, K.G. (2009) "UV disinfection of adenovirus: Molecular
indications of DNA damage efficiency." Applied and EnvironmentalMicrobiology.
75(1):23-28.
Enriquez, E.C., Hurst, C.H., Gerba, C.P., 1995. "Survival of enteric adenoviruses 40 and 41 in
tap, sea and wastewater." Water Research 29, 2548-2553.
Fleisher, J. M. (1991). "A Reanalysis of Data Supporting U.S. Federal Bacteriological Water
Quality Criteria Governing Marine Recreational Waters." Research Hournal of the Water
PollutionControl Federation,63(3 ), 259.
68
Fosgate, G.T. and Cohent, N.D., (2008). "Epidemiological study design and the advancement of
equine health." Equine Veterinary Journal,40(7): 693-700.
Grabow, W. 0. K., and Taylor, M. B. (1993). "New methods for the virological analysis of
drinking water supplies." Biennial Conference and Exhibition of the Water Institute of
Southern Africa, 259-264.
Haas, C. N., Rose, J. B., and Gerba, C. P. (1999). Quantitative MicrobialRisk Assessment. John
Wiley & Sons Inc., New York, N.Y.
Hernandez-Delgado, E. A., Sierra, M. L., & Toranzos, G.A. (1991). "Coliphages as Alternate
Indicators of Fecal Contamination in Tropical Waters." Environmental Toxicology and
Water Quality, 6(2), 131-143.
Holton, Glyn A. (2004). "Defining Risk." FinancialAnalysts Journal,60(6), 19-25.
IDEXX Laboratory Inc. (2013b). "Water Testing Solutions: Product Catalog."
Jiang, S., Noble, R. and Chu, W. (200 1). "Human adenoviruses and coliphages in urban runoffimpacted coastal waters of Southern California." Applied and Environmental Microbiology,
67, 179-184.
Joshi, Y. K., Tortajada, C., and Biswas, A. K. (2012). "Cleaning of the Singapore River and
Kallang Basin in Singapore: Economic, Social, and Environmental Dimensions."
InternationalJournal of Water Resources Development, 28(4), 647-658.
Jothikumar, N., Cromeans, T. L., Hill, V. R., Lu, X., Sobsey, M. D., and Erdman, D. D. (2005).
"Quantitative Real-Time PCR Assays for Detection of Human Adenoviruses and
Identification of Serotypes 40 and 4 1." Applied and EnvironmentalMicrobiology, 71(6),
3 13 1-3 136.
Kundu, A., McBride, G., Wuertz, S. (2013). "Adenovirus-associated health risks for recreational
activities in multi-use coastal watershed based on site-specific quantitative microbial risk
assessment." Water Research, 47(16):6309-25.
Kuo, D. H. W., Simmons, F.J., Blair, S., Hart, E., Rose, J.B. & Zagoraraki, 1. (2010).
"Assessment of human adenovirus removal in a full-scale membrane bioreactor treating
municipal wastewater." Water Research, 44, 1520-1530.
Liu, T.Y. (2014). Enteric Adenovirus and Coliphage as Microbial Indicators in Singapore's
Kallang Basin. Master of Engineering thesis. Department of Civil and Environmental
Engineering, Massachusetts Institute of Technology, Cambridge, Massachusetts.
Nauta, T., Wui, C. C., Smits, J., and Lee, E. (n.d.). OperationalWater Quality Managementjor
MarinaReservoir, Singapore.
<http://www.who.int/watersanitation-health/bathing/srwe2full.pdf>.
69
Nwachuku, N., Gerba C.P., Oswald, A, and Mashadi, F.D. (2005). "Comparative Inactivation of
Adenovirus Serotypes by UV Light Disinfection." Applied and Environmental
Microbiology, 71(9): 5633-5636.
Pina, S., Puig, M., Lucena, F., Jofre, J., and Girones, R. (1998). "Viral pollution in the
environment and in shellfish: human adenovirus detection by PCR as an index of human
viruses." Applied and EnvironmentalMicrobiology, 64(9), 3 3 76-82.
PUB. (2013). "Our Water, Our Future." Public Utilities Board,Singapore.
<http://www.pub.gov.sg/mpublications/OurWaterOurFuture/Pages/default.aspx>.
Rigotto, C., Hanley, K., Rochelle, P.A., De Leon, R., Barardi, C.R.M, Yates M.V. (2011).
"Survival of Adenovirus Types 2 and 41 in Surface and Ground Waters Measured by a
Plaque Assay." EnvironmentalScience Technology, 45, 4145-4150.
Rose, J. B., Mullinax, R. L., Singh, S. N., Yates, M. V., and Gerba, C. P. (1987). "Occurrence of
rotaviruses and enteroviruses in recreational waters of Oak Creek, Arizona." Water
Research, I I, 1375-1381.
SGNEA (2008). "Recreational Water Quality Guidelines for Recreational Beaches and Fresh
Water Bodies." Singapore National EnvironmentAgency.
<http://app.nea.gov.sg/cms/htdocs/article.asp?pid=3039>, (Jan. 4, 2014)
Sloat, S., and Ziel, C. (1992). The Use ofIndicator Organisms to Assess Public Water Safety.
Hach Company, Loveland, CO.
Soon, T.Y., Jean, L.T., Tan, K. (2009). Clean, green and blue. Singapore'sjounreytowards
environmentaland water sustainabilitv. ISEAS Publishing, Singapore.
Thomann, R. V., and Mueller, J. A. (1987). Principlesof Surface Water Quality Modeling and
Control. Harper and Row, New York.
USEPA. (1986). Ambient Water Quality Criteriafor Bacteria.No. EPA440/5-84-002, United
States Environmental Protection Agency, Office of Water Regulations and Standards,
Washington, DC.
USEPA. (1998). Guidelinesfor EcologicalRisk Assessment. No. EPA/630/R-95/002F. Risk
Assessment Forum, U.S. Environmental Protection Agency, Washington, D.C.
USEPA. (200 1 a). "Manual of Methods for Virology: Chapter 16." Report Number EPA 600/484/013 (N 16). Office of Research and Development, U.S. Environmental Protection
Agency, Washington, D.C.
USEPA. (2001 b). "Method 1601 : Male-specific ( F + ) and Somatic Coliphage in Water by Twostep Enrichment Procedure." Report Number EPA 821-R-01-030. Office of Water, U.S.
Environmental Protection Agency, Washington, D.C.
70
USEPA. (2002). "Calculating Upper Confidence Limits for Exposure Point Concentrations at
Hazardous Waste Sites." United States EnvironmentalProtectionAgency,
<http://www.orp.doe.gov/dqo/training/ucl.pdf> (Jan, 2014)
USEPA. (2006b). "National Primary Drinking Water Regulations: Ground Water Rule; Final
Rule. 40 CFR Parts 9, 141, and 142. FederalRegister, 71:216:65574.
<http://www.epa.gov/fedrgstr/EPA-WATER/2006/November/Day-08/w8763.pdf>. (Jan,
2014)
USEPA. (2011). "Revisions to the Unregulated Contaminant Monitoring Regulation (UCMR 3)
for public water systems." FederalRegister, 76(42):11713-11737.
van Heerden, J., Ehlers, M.M., Heim, A. and Grabow, W.O. (2005) "Prevalence, quantification
and typing of adenoviruses detected in river and treated drinking water in South Africa."
JournalofApplied Microbiology,99, 234-242.
Vilagines, P., Sarrette, B., Champsaur, H., Hugues, B., Dubrou, S., Joret, J.-C., Laveran, H., J.,
L., Paquin, J. L., Delattre, J. M., Oger, C. Alame, J., Grateloup, I. Perrollet, H., Serceau, R.
Sinegre, F., and Vilagines, R. (1997). "Round robin investigation of glass wool method for
poliovirus recovery from drinking water and sea water." Water Science and Technology, 35,
445-449.
Viau, E.J., Lee, D., and Boehm, A.B. (2011). "Swimmer Risk of Gastrointestinal Illness from
Exposure to Tropical Coastal Waters Impacted by Terrestrial Dry-Weather Runoff."
EnvironmentalScience Technology, 45(17) 7158-7165.
Vilagines, P., Sarrette, B., Husson, G., and Vilagines, R. (1993). "Glass wool for virus
concentration at ambient water pH level." Water Science and Technology, 27, 299-306.
Wade, T.J., Pai, N., Eisenberg, J. N. S., & Colford, J.M. (2003). "Do US Environmental
Protection Agency water quality guidelines for recreational waters prevent gastrointestinal
illness? A systematic review and meta-analysis." EnvironmentalHealth Perspectives,
111(8), 1102-1 109.
Ward, R. L., Bernstein, D. I., Young, E. C., Sherwood, J. R., Knowlton, D. R., and Schiff, G. M.
(1986). "Human rotavirus studies in volunteers: determination of infectious dose and
serological response to infection." Journal of Infections Diseases, 154, 871-880.
WHO. (2003). "Guidelines for safe recreational waters: Volume 1 - Coastal and fresh waters.
Water Sanitation Health." World Health Organization, Geneva, Switzerland.
http://www.who.int/watersanitationhealth/bathing/srwg 1.pdf
Wiedenmann, A. (2007). "A plausible model to explain concentration-response relationships in
randomized controlled trials assessing infectious disease risks from exposure to recreational
waters." In: StatisticalFrameworkfor Recreational Water Quality Criteriaand
Monitoring,L. Wymer (ed.), John Wiley and Sons Ltd., West Sussex, 153-179.
Wiedenmann, A., Kruger, P., Dietz, K., Lopez-Pila, J.M., Szewzyk, R., & Botzenhart, K. (2006).
"A Randomized controlled trial assessing infectious disease risks from bathing in fresh
recreational waters in relation to the concentration of Escherichia coli, intestinal
71
enterococci, Clostridium perfringens, and somatic coliphages." Environmental Health
Perspectives, 114(2), 228-236.
Wiedenmann, A., Kruger, P., Gommel, S., Eissler, M., Hirlinger, M., Paul, A., Junst, K., Sieben,
E., and Dietz, K. (2004). Epidemiologicaldeterminationof disease risksfrom bathing.
Report No. UFOPLAN 298 61 503. Federal Environmental Agency (UBA), Berlin.
Wymer, L.J., & Dufour, A.P. (2002). "A model for estimating the incidence of swimming-related
gastrointestinal illness as a function of water quality indicators." Environmetrics, 13(5-6),
669-678.
72
Appendix A
List of Adenovirus samples and concentrations in genomic copies/L
Well
Sample Name
Al
A2
A3
AIO
4-4
4-8
4-12
5-4
All
A12
B1
5-8
5-12
B2
B3
BlO
B1I1
B12
C1
C2
C3
4-4
4-8
4-12
5-4
5-8
5-12
CT Mean
CT
GC/L dilutions
Undetermined
Undetermined
Undetermined
Undetermined
34.38
36.20
89.67
28.12
389.91
122.2
3899
1222
103.99
452.1
4521
36.68
36.85
27.22
18.52
118.38
80.51
1183
805.
38.30
7.36
32.01
320
36.68
33.86
15.70
125.51
68.29
545.7
682
5457
38.95
4.85
21.10
211.06
39.44
35.92
3.54
33.58
15.43
146
154.34
1460
39.65
172.4
1724
35.66
27.36
118.9
1189
36.49
23.33
101.4
1014
34.38
35.17
Undetermined
Undetermined
Undetermined
Undetermined
Undetermined
34.38
35.17
34.15
CII
4-3
4-7
4-11
5-3
5-7
C12
D1
5-11
4-3
D2
D3
4-7
4-11
D1O
5-3
DII
5-7
D12
El
5-11
4-2
E2
E3
El0
4-6
4-10
5-2
Undetermined
Undetermined
Undetermined
38.95
Eli
5-6
Undetermined
39.44
E12
F1
5-10
4-2
Undetermined
Undetermined
35.92
33.86
F2
4-6
F3
FIO
4-10
5-2
F1
F12
5-6
5-10
Gl
G2
G3
4-1
4-5
4-9
GIO
5-1
G1
5-5
G12
5-9
H1
4-1
H2
4-5
CIO
GC/L
GC
Undetermined
Undetermined
Undetermined
Undetermined
Undetermined
36.85
38.30
36.25
36.85
Undetermined
Undetermined
38.30
Undetermined
37.11
33.86
38.95
Undetermined
Undetermined
39.44
35.92
Undetermined
Undetermined
Undetermined
36.49
35.23
35.66
38.13
Undetermined
36.24
Undetermined
36.49
73
Well
Sample Name
H3
4-9
H7
HlO
HII
H12
Pos
5-1
5-5
5-9
CT Mean
CT
GC
GC/L
GC/L*dilutions
Undetermined
29.54
34.81
38.13
35.08
29.54
35.23
38.13
35.66
74
1980
68.37
8.19
57.48
8610
297
35.61
249
86110
2972
356
2499
Adenovirus quantitative PCR results in genomic copies/L (GC/L) for Station 2 at
each time
Geometric
Mean
GC/L
Station 2
1
2
Date - Time
GC/L
GC/L
1/7/14 11:00 A.M.
2500
1780
2100
1/7/14 3:00 P.M.
940
X
690
1/7/14 7:00 P.M.
520
1500
890
X
X
X
1/8/14 3:00 A.M.
790
1210
980
1/8/14 7:00 A.M.
690
X
60
1/8/14 11:00 A.M.
450
X
50
1/8/14 3:00 P.M.
910
X
70
1/8/14 7:00 P.M.
2420
X
110
1/8/14 11:00 P.M.
X
X
X
1/9/14 3:00 A.M.
X
X
X
1/9/14 7:00 A.M.
X
X
X
1/7/14 11:00 P.M.
2500
2000
8 1500
1000
500
0
1/7/14 0:00
1/7/14 12:00
1/8/14 12:00
1/8/14 0:00
Date-Time
75
1/9/14 0:00
1/9/14 12:00
Adenovirus quantitative PCR results in genomic copies/L for Station 3 at each time
2
Station 3
Date - Time
Geometric
Mean
GC/L
GC/L
GC/L
1/7/14 11:00 A.M.
X
X
X
1/7/14 3:00 P.M.
X
X
X
1/7/14 7:00 P.M.
X
X
X
1/7/14 11:00 P.M.
X
X
X
1/8/14 3:00 A.M.
X
X
X
1/8/14 7:00 A.M.
X
X
X
1/8/14 11:00 A.M.
X
X
X
1/8/14 3:00 P.M.
X
X
X
1/8/14 7:00 P.M.
X
X
X
1/8/14 11:00 P.M.
X
X
X
1/9/14 3:00 A.M.
190
X
30
1/9/14 7:00 A.M.
1200
X
80
90
80
70
,60
S50
o40
o30
20
1/7/14 0:00
I
10
10
1/7/14 12:00
1/8/14 0:00
1/8/14 12:00
Date-Time
76
1/9/14 0:00
1/9/14 12:00
Adenovirus quantitative PCR results in genomic copies/L for Station 4 at each time
Station 4
1
2
Date - Time
GC/L
GC/L
Geometric
Mean
GC/L
X
X
X
1/7/14 3:00 P.M.
5460
X
165
1/7/14 7:00 P.M.
X
805
60
1/7/14 11:00 P.M.
X
X
X
1/8/14 3:00 A.M.
X
1000
70
1/8/14 7:00 A.M.
X
210
30
1/8/14 11:00 A.M.
X
X
X
1/8/14 3:00 P.M.
X
X
X
1/8/14 7:00 P.M.
X
X
X
1/8/14 11:00 P.M.
X
X
X
1/9/14 3:00 A.M.
X
X
X
1/9/14 7:00 A.M.
X
X
X
1/7/14 11:00 A.M.
180
9
160 140
120
100
80
I----
-
+-
60
40 20
0 II
I
1/7/14 0:00
I
I
1/7/14 12:00
I
1/8/14 0:00 1/8/14 12:00
Date-Time
77
1/9/14 0:00
1/9/14 12:00
Adenovirus quantitative PCR results in genomic copies/L for Station 5 at each time
Station 5
1
2
Date - Time
GC/L
GC/L
Geometric
Mean
GC/L
1720
3000
2260
1/7/14 3:00 P.M.
X
X
X
1/7/14 7:00 P.M.
X
320
40
1/7/14 11:00 P.M.
X
X
X
1/8/14 3:00 A.M.
X
360
40
1/8/14 7:00 A.M.
X
150
30
1/8/14 11:00 A.M.
X
X
X
1/8/14 3:00 P.M.
X
X
X
1/8/14 7:00 P.M.
1190
2500
1700
X
1460
85
1/7/14 11:00 A.M.
1/8/14 11:00 P.M.
1/9/14 3:00 A.M.
1180
680
900
1/9/14 7:00 A.M.
X
4520
150
2500
2000
U,
0
1500 4
2
1000 +---
-
500
A
L
- --
1/7/14 0:00
I
-.
1/7/14 12:00
~---
1/8/14 0:00
1/8/14 12:00
Date-Time
78
1/9/14 0:00
1/9/14 12:00
Appendix B
Raw E. coli data for samples collected on January 7th, 2014
Date
Time
7/l/
11:00
A.M.
14
Samples I Dilution
2
MPN
LOWER
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
145.5
209.8
301.1
1455
2098
3011
10
MPN
__
__________________
_______
3
5
169.5
225.4
296.2
847.5
1127
1481
4
10
260.6
410.6
618.9
2606
4106
6189
5
10
1016.2
1553.1
2353.1
10162
15531
23531
3504.18
Average
Date
Time
Samples
7/1/1
3:00
2
4
P.M.
MPN
LOWER
Dilution
10
_
_
MPN
ACTUAL
72.2
_
_
_
_
_
98.5
_
_
_
_
132.1
_
_
_
_
722
_
_
_
_
MPN
UPPER
MPN
ACTUAL
MPN
LOWER
MPN
UPPER
985
_
_
_
_
_
1321
_
_
_
_
1142.5
3
5
126.4
172.6
228.5
632
863
4
10
74.8
105
143.9
748
1050
1439
5
10
660.6
980.4
1410.2
6606
9804
14102
1719.92
Average
Date
Time
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
7/1/1
4
7:00
P.M.
2
10
32.3
46.5
64.7
323
465
647
3
5
123
172.5
235.5
615
862.5
1177.5
4
10
59.6
83.6
113.8
596
836
1138
5
10
231.9
365.4
555.5
2319
3654
5555
1052.07
Average
Date
Time
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
7/1/1
11:00
2
10
158.5
222.4
303.3
1585
2224
3033
3
5
81.6
114.5
155.5
408
572.5
777.5
4
10
51.1
71.7
97.5
511
717
975
5
10
169.2
231
315.5
1692
2310
3155
4
P.M.
Average
79
1205.06
Raw E. coli data for samples collected on January 8th 2014
Dat
e
Time
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
8/1
A:.
2
10
134.9
184.2
251.4
1349
1842
2514
3
5
40
56.1
75.9
200
280.5
379.5
4
10
64.6
90.6
124.1
646
906
1241
5
10
84.7
118.7
162.7
847
1187
1627
Average
DatT
e
rime
8/1
Samples
A..
863.38
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
e
T
rime
8/1
11:00
/14
A.M.
10
183.5
272.3
382.9
1835
2723
3829
3
5
53
74.3
98.8
265
371.5
494
4
10
74.6
104.6
142.1
746
1046
1421
5
10
134.9
184.2
251.4
1349
1842
2514
Samples
1181.5
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
10
924.9
1431.6
2101.6
9249
14316
21016
3
5
31.3
45.2
62.5
156.5
226
312.5
4
10
28.3
42
59.7
283
420
597
5
10
96.5
135.4
184
965
1354
1840
_______
Average
Dat
e
8/1
/14
Time
rime
Samples
Dilution
1164.6
MPN
LOWER
MPN
ACTUAL
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
3:00
P.M.
10
245.3
344.1
472.5
2453
3441
4725
3
5
39.1
56.3
77.6
195.5
281.5
388
4
10
42.1
59.1
81.2
421
591
812
5
10
95.1
133.4
177.9
951
1334
1779
Dat
8/1
7:00
/14
P.M.
MPN
UPPER
2
Average
Time
MPN
UPPER
2
Average
Dat
MPN
UPPER
934.81
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
2
10
87.4
113.3
144.2
874
1133
80
MPN
UPPER
1442
I
I
I
3
1
1
27.9
41.4
58.6
27.9
41.4
58.6
4
10
17.1
26.9
39.8
171
269
398
5
10
15.5
23.7
35
155
237
350
233.85
Average
MPN
Dat
e
8/1
/14
11:00
.P.
Samples
Dilution
LOWER
2
10
126.4
M.
MPN
ACTUAL
MPN
UPPER
172.6
228.5
MPN
LOWER
1264
___
____
MPN
ACTUAL
1726
MPN
UPPER
2285
__
3
1
38.5
55.6
77.2
38.5
55.6
77.2
4
10
14.4
23.3
36.1
144
233
361
5
10
50.5
68.9
93.8
505
689
938
352.31
Average
Raw E. coli data for samples collected on January 91, 2014
MPN
UPPER
Date
Time
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWE
MPN
ACTUAL
9/1/
14
3:00
2
10
21.8
31.4
44.2
A. M.
218
314
442
3
5
12.7
20.6
31.8
63.5
103
159
4
10
7.4
13.4
22.3
74
134
223
5
10
6.9
12.8
21.7
69
128
217
153.47
Average
MPN
UPPER
Date
Time
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUA
L
9/1/
14
7:00
A.M.
2
10
87.2
116
152.6
872
1160
1526
3
5
64.9
88.6
118.3
324.5
443
591.5
4
10
18.2
27.8
40.6
182
278
406
5
10
1222
1986.6
3300.2
12220
19866
Average
81
1297.9
33002
Raw Enterococci data for samples collected on January 7 t, 2014
Date
Time
Samples
7/l/
11:00
2
14
A.M.
Dilution
1
_______
MPN
MPN
LOWER
ACTUAL
754.6
1119.9
______
MPN
MPN
UPPER
LOWE
MPN
ACTUAL
MPN
UPPER
1614
754.6
1119.9
1614
R
_________
3
1
205.8
280.9
378.3
205.8
280.9
378.3
4
1
475.7
727
1048.9
475.7
727
1048.9
5
1
276.2
435.2
650
276.2
435.2
650
Average
Date
14l/
Time
561.67
Samples
.
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
1
12.9
21.6
33.7
12.9
21.6
33.7
3
1
19.7
30.1
44.2
19.7
30.1
44.2
4
1
74
101
133.7
74
101
133.7
5
1
79.7
105.9
137
79.7
105.9
137
P.
Average
Date
14l/
Time
51.35
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
1
39.7
54.3
72.4
39.7
54.3
72.4
3
1
43.4
60.9
83.3
43.4
60.9
83.3
4
1
102
132.2
168
102
132.2
168
5
1
1439.5
2419.6
lx^OA7
1439.5
2419.6
lx^OA7
P.
Average
Date
Time
7/1/
11:00
14
P.M.
Samples
Dilution
2
_
_
_
MPN
LOWER
1
_
_
_
MPN
ACTUAL
44.1
_
_
_
MPN
UPPER
60.2
_
_
_
180.3
MPN
LOWER
80
_
_
_
MPN
ACTUAL
MPN
UPPER
60.2
80
44.1
_
_
_
_
_
_
_
3
1
29.9
43.1
59.8
29.9
43.1
59.8
4
1
65.5
87.1
112.8
65.5
87.1
112.8
5
1
218.4
263.1
314.5
218.4
263.1
314.5
Average
82
87.81
Raw Enterococci data for samples collected on January 8
Date
8/1/
14
Time
3:00
A.M.
h
2014
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
1
740.6
1011.2
1323.5
740.6
1011.2
1323.5
3
1
62.9
88.2
120.2
62.9
88.2
120.2
4
1
91.9
122.2
159.8
91.9
122.2
159.8
5
1
1439.5
2419.6
108
1439.5
2419.6
108
Average
Date
8/1/
14
Time
7:00
A.M.
402.97
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
1
1167.7
1732.9
2709.5
1167.7
1732.9
2709.5
3
1
154.2
210.5
281
154.2
210.5
281
4
1
1167.7
1732.9
2709.5
1167.7
1732.9
2709.5
5
1
1439.5
2419.6
108
1439.5
2419.6
108
Average
Date
Time
8/1/
11:00
14
A.M.
1112.07
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
1
9.7
16.8
26.8
9.7
16.8
26.8
3
1
5.1
10.7
18.5
5.1
10.7
18.5
4
1
37.1
52
71
37.1
52
71
5
1
1439.5
2419.6
108
1439.5
2419.6
108
Average
Date
Time
8/1/
3:00
14
P.M.
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
68.96
MPN
LOWER
Time
8/1/
7:00
14
P.M.
MPN
UPPER
Samples
Dilution
2
1
2.3
5.2
11.9
2.3
5.2
11.9
3
1
10.7
17.9
28.2
10.7
17.9
28.2
4
1
35.4
49.6
67.8
35.4
49.6
67.8
5
1
104.2
125.6
149.8
104.2
125.6
149.8
Average
Date
MPN
ACTUAL
27.59
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
2
1
49.7
69.7
95.3
49.7
69.7
95.3
3
1
101.9
139.1
182
101.9
139.1
182
4
1
295.5
403.4
526.2
295.5
403.4
526.2
5
1
1167.7
1732.9
2709.5
1167.7
1732.9
2709.5
83
Average
286.92
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
UPPER
MPN
LOWER
MPN
ACTUAL
UPPER
8/1/
Time
11:00
14
P.M.
2
1
13.4
21.8
33.1
13.4
21.8
33.1
3
1
7.6
14.2
23.4
7.6
14.2
23.4
4
1
18.8
28.7
41.6
18.8
28.7
41.6
5
1
82
109
142.2
82
109
142.2
Date
MPN
Average
Raw Enterococci data for samples collected on January
Date
MPN
31.36
9 th,
2014
Time
Samples
Dilution
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
3:00 A.M.
2
1
6
11.6
20.1
6
11.6
20.1
3
1
6.5
12.1
21.1
6.5
12.1
21.1
4
1
24.2
35.9
51
24.2
35.9
51
5
1
43.9
61.6
83.3
43.9
61.6
83.3
9/1/
14
23.60
Average
Date
Time
9/1/14
A.M.
Samples
Dilution
MPN
LOWER
2
1
42.9
3
1
91.2
4
1
78.2
5
1
1630.4
MPN
ACTUAL
MPN
UPPER
MPN
LOWER
MPN
ACTUAL
MPN
UPPER
60.2
83
42.9
60.2
124.6
167.8
91.2
124.6
167.8
106.7
140.4
78.2
106.7
140.4
2419.6
4716.1
1630.4
2419.6
4716.1
7:00
Average
84
209.78
83