Document 11212799
advertisement

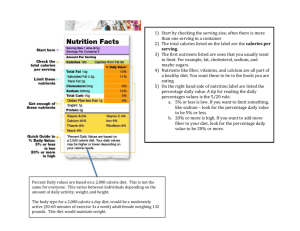
Journal Of Musculoskeletal Pain, Vol. 21(4): 365–370, 2013 ! 2013 Informa Healthcare USA, Inc. ISSN: 1058-2452 print / 1540-7012 online DOI: 10.3109/10582452.2013.852649 RESEARCH IDEA Allen Ernst, MS and John Shelley-Tremblay, PhD Department of Psychology, University of South Alabama, Mobile, AL, USA ABSTRACT Objectives: This study was conducted to assess the association between a non-ketogenic, low-carbohydrate diet [NKLCD] and symptoms of fibromyalgia syndrome [FMS], mood and energy levels, and confusion, as compared to controls reporting adherence to the Western Pattern Diet [WPD]. Methods: Participants were 33 middle-aged females with FMS who reported adherence to a NKLCD or the WPD. Respondents completed a questionnaire packet measuring state and trait mood and energy level as well as a measure of FMS symptoms and daily functioning. Results: The NKLCD sample reported less affective distress, less Confusion, less Fatigue and more Vigor than the WPD sample on the Profile of Mood States. Group scores for the Hospital Anxiety and Depression Scales showed lower Anxiety and Depression scores for the NKLCD sample. The NKLCD sample showed lowered symptom scores on the Fibromyalgia Impact Questionnaire. Morbidity was significantly reduced for all measures in the NKLCD sample. Conclusions: Results support hypotheses of less dysphoria, more energy, decreased FMS symptomatology in a NKLCD sample versus the WPD group. Results suggest the potential for development of a dietary intervention for managing affective and functional symptoms of this syndrome. KEYWORDS: Depression, diet, fibromyalgia, FIQ, HAD Scales, low-carbohydrate, POMS INTRODUCTION For three decades, the per capita and caloric proportional measures of the macronutrient carbohydrate [CHO] has increased in the American diet (1). At the same time an association between CHO intake and depressive affect has been empirically demonstrated in individuals presumed to be particularly sensitive to carbohydrate intake (2), as well as healthy females [Ernst and Shelley-Tremblay, unpublished observation]. Among the many laboratory abnormalities found in the fibromyalgia syndrome [FMS], an impairment of glycolysis, an oxidative stage in glucose metabolism within the Krebs metabolic cycle, has been observed. In one study, glycolysis was impaired such that the reaction products of this process, particularly adenosine triphosphate [ATP], the energy source for cell metabolism, was reduced in all FMS participants (3,4). Similar ATP energy deficits have also been observed in muscle biopsies of FMS patients (5). Both findings have been frequently cited to explain the profound anergy experienced in FMS. This metabolic dysfunction is pervasive and chronic, as digestible starches and most sugars are eventually rendered into glucose, which then goes on to partial conversion to ATP during the Krebs cycle (6). It has been suggested that the carbohydrate cravings observed in FMS (7) may arise out of a drive to self-medicate this anergic state. However, carbohydrate cravings have also been associated with 20 13 J Muscoskeletal Pain Downloaded from informahealthcare.com by University of South Alabama on 11/22/13 For personal use only. Non-Ketogenic, Low Carbohydrate Diet Predicts Lower Affective Distress, Higher Energy Levels and Decreased Fibromyalgia Symptoms in Middle-Aged Females with Fibromyalgia Syndrome as Compared to the Western Pattern Diet Correspondence: Allen Ernst, Department of Psychology, University of South Alabama, Mobile, AL 36688, USA. E-mail: ernsta@sanjuancollege.edu Submitted: 6 March 2013; Revisions Accepted 30 September 2013; published online 11 November 2013 J Muscoskeletal Pain Downloaded from informahealthcare.com by University of South Alabama on 11/22/13 For personal use only. 366 A. Ernst & J. Shelley-Tremblay depression (8,9), as well as other dysphoric mood and energy states (10) – both found in FMS in greater frequency than the American adult population. In an attempt to establish a direction of causality for this association, Christensen et al. (11) reported three case studies that showed improvement in depressive symptoms when participants restricted their carbohydrate intake, specifically sucrose. Following up these results, Christensen and Somers (8) reported greater CHO intake for depressed individuals. Some additional support for these findings comes from comparative animal studies that have shown antidepressant effects of an isoenergetic ketogenic diet on rats during the Porsolt test, an animal model of depression used in pharmaceutical research. Treated rats showed less ‘‘behavioral despair’’ than chow-fed subjects in response to this hopeless water tank escape dilemma (12). A ketogenic diet study with human subjects using the Profile of Mood States [POMS] assessments found no subscale score differences save for Confusion-Bewilderment, found to be higher in the American Dietetic Association diet group increasing over time, while the ketogenic, lowcarbohydrate diet [KLCD] group actually logged a decrease in Confusion scores over time (13). They also found group differences in cognitive performance tasks, with mixed results. A naturalistic study by Ernst and Shelley-Tremblay [2012, unpublished observations] has shown less affective distress in a sample of middle-aged females reporting adherence to a low-carbohydrate diet versus a second group that reported no diet or rather the Western pattern diet [WPD]. The WPD is characterized by a high consumption of red meat, refined grains, processed meat, high-fat dairy products, desserts, high-sugar drinks and eggs, as well as French fries and potatoes (14). In 1999, Hu et al. (15) reported on a study to test the validity of the construct WPD versus the Prudent Diet and found that from a factorial standpoint both constructs were stable over time and valid. In the laboratory Shelley-Tremblay et al. (16) reported a significant group interaction between FMS patients and healthy females in the high-alpha electroencephalogram [Alpha EEG] band, which the authors interpreted as associated with the ‘‘approach’’ emotion of anger, and correlated with the POMS Anger-Hostility subscale. These effects were in response to the intake of a 75-g sucrose challenge measured at five epochs over 3 h. In contrast to the aforementioned study, the present study was conducted in the same laboratory but sought to measure the association for females with FMS between KLCD and self-reported affect and symptoms. Numerous subjective reports indicate that low-CHO diets afford FMS patients more energy. Not only have these claims not been assessed systematically, but an empirically-based model of carbohydrate-mediated serotonin neurotransmitter production sometimes called the Wurtman Effect actually predicts a drop in tryptophan absorption across the blood–brain barrier and as a necessary precursor to serotonin production in the period following CHO consumption with subsequent depressive affect [for a review see (17)]. The present study was conducted to test the hypothesis that a low-carbohydrate diet is associated with a lower physiological and affective symptom profile in subjects diagnosed with FMS. MATERIALS AND METHODS Oversight The study was reviewed and approved by the Institutional Review Board of the University of South Alabama, which endorses the Helsinki Protocols of 1964. All subjects participated voluntarily in this study. Recruitment of subjects In this correlational study, 33 [4 non-ketogenic, lowcarbohydrate diet [NKLCD] and 29 Western Pattern Diet [WPD] adherents] age-equivalent groups with FMS were recruited from the student subject pool of a large southeastern university and the local community via newspaper. University subject pool participants received class credit, while locally recruited subjects were thanked for their participation. Group assignment Participants endorsed an informed consent form where potential respondents were informed, ‘‘The purposes of the study is to evaluate the difference(s), if any, in mood states. . .between two different meal types, on a population of women who have been diagnosed with FMS. You have been invited to this study because you are a woman with a history of FMS. You will be asked to fill out some questionnaires. One questionnaire will ask you some general questions about age and medical history. Another form will measure personality traits, while a third will inquire about how you have been feeling. . .’’ Respondents then completed the demographic questionnaire and self-report battery. All included J Muscoskeletal Pain Downloaded from informahealthcare.com by University of South Alabama on 11/22/13 For personal use only. Diet and Fibromyalgia Symptoms subjects reported treatment under the care of a physician and diagnosis of FMS according to the American College of Rheumatology criteria (18). Respondents were eliminated if they reported an eating disorder, other diet type, diabetes mellitus or severe clinical depression, as evidenced by reported history during telephone screening or Hospital Anxiety and Depression Scale [HADS] Depression score exceeding a clinical cutoff of 14. Those respondents reporting adherence to either a NKLCD or WPD were assigned to separate sample groups. Respondents were asked about their overall adherence to the low-carbohydrate diet to determine if their particular stage or level of adherence would be likely to produce ketosis. In addition, they were asked if they had recently been experiencing any of the recognized signs and symptoms of ketosis including headaches and distinctive breath odor. No participants were given instructions to modify their diet. Measurements Profile of Mood States Mood and energy levels were measured by the POMS (19). The POMS contains 65, five-response Likertscale adjective items [including 15 fillers] with scoring to yield six subscales to immediate or long-term somatic and affective states and one composite score, the Total Mood Disturbance Score. The subscales were factor-analytically derived to load on the constructs Tension-Anxiety, Depression-Dejection, Anger-Hostility, Vigor, Fatigue and ConfusionBewilderment. The Total Mood Disturbance Score was derived by the summation of the five ‘‘negative’’ subscales, then subtracting from this total the ‘‘positive’’ Vigor score. The POMS was administered with validated instructions to report subjective states ‘‘right now’’, within the last 3 min. Hospital Anxiety and Depression Scales The HAD Scales (20) were validated on a sample of hospital patients. Patients endorsed one of four statements for each of 16 items. In its development, all items were factor-derived such that any items loading strongly on somatization were eliminated, thus eliminating confounds from medical disorders. Another departure from the usual depression inventory is the factorization of depression-scale items to load on the anhedonic component of depressive states. Fibromyalgia Impact Questionnaire The Fibromyalgia Impact Questionnaire [FIQ] (21) is a self-report measure of physical functioning, 367 work status, depression, anxiety, sleep, pain, stiffness, fatigue and well-being. In its construction, some items were used from both the Health Assessment Questionnaire and the Arthritis Impact Measurement Scales. RESULTS Study subjects Recruitment efforts were successful in identifying a total of 87 females with FMS who were willing to participate in the study [see Figure 1]. Of those, 75 individuals had responded to a local newspaper advertisements and 12 individuals came from a University Subject Pool. Unfortunately, 45 of those recruited had to be excluded because they did not meet inclusion criteria, declined to participate or for other reasons. That left 42 subjects as study participants to be allocated to a study group, with five selfselecting to the NKLCD group and 37 self-selecting to the WPD group. Characteristics of groups The observed demographic characteristics of the two groups are shown in Table 1. Independent-samples t-tests were conducted to determine if a possible confound of age was different between the two groups. Group age difference was not significant. Independent samples non-parametric tests were conducted to determine if sample groups differed in their use of antidepressants, sleep meds, pain meds or guaifenisin, and no significant differences were found [Table 1] Further independent-samples t-tests were conducted with SPSS 20 to test the hypothesis that subjects reporting adherence to a NKLCD would report lower scores on measures of affective distress, fatigue and FMS symptoms. Table 2 shows significant group differences were evident for both HAD Scales Depression and Anxiety subscales and the HAD Scales Total Score such that subjects on NKLCD showed lower affective distress. In addition, mean score differences in seven of seven POMS scales did reach significance with the NKLCD sample showing less affective distress, confusion and fatigue. Finally, the NKLCD sample showed significantly lower FMS-related symptom scores than the WPD sample as reported on the FIQ. All measures showed large effect sizes as measured by Cohen’s d as calculated by G*Power 3. DISCUSSION This study has shown that individuals with FMS eating carbohydrate-restricted diets differed A. Ernst & J. Shelley-Tremblay 368 Assessed for eligibility (n=87) Recruited from local newspaper (n=75) From University Subject Pool (n=12) Enrollment Excluded (n=45) ♦ Not meeng inclusion criteria (n=16 ) ♦ Refused to parcipate (n=2) ♦ Other reasons (n=27 no packet) Assigned (n= 42) J Muscoskeletal Pain Downloaded from informahealthcare.com by University of South Alabama on 11/22/13 For personal use only. Allocaon Western Paern Diet Allocated to intervenon (n= 37) ♦Received allocated intervenon (n=37) ♦Did not receive allocated intervenon diabetes (n=3); depression (n=6) Non-Ketogenic Low-Carbohydrate Diet Allocated to intervenon (n=5) ♦Received allocated intervenon (n=5) Follow-Up Lost to follow-up Lost to follow-up Disconnued intervenon (incomplete packet) (n= 1) Disconnued intervenon (incomplete packet) n=3) Analysis Analysed (n= 4 ) Analysed (n= 29) FIGURE 1. Sampling and flow of participants for survey study. significantly from those on WPD with respect to all measures of affective state, energy levels and FMS symptoms. These findings support the hypothesis that the low carbohydrate diet sample would report less affective distress, fatigue and lower FMS symptom scores. Greater Vigor and lower Fatigue scores for the NKLCD group may be explained by a finding for healthy subjects by Piatti (22) that CHO intake actually reduced glucose oxidation or glycolysis, with the result that the system would have greater energy at its disposal at the cellular level. These results are of note in that the carbohydraterestricted diet appears to be associated with lessened affective distress and fatigue in a clinical population, supporting the results of Galletly et al. (23) who found that their low-CHO group showed a statistically-significant reduction in depression over time, as measured by the HAD Scales. It should be noted, however, that their subject group was comprised of female subjects diagnosed with a rare disorder. Interestingly, the prediction of greater affective distress as inferred from the model of brain serotonin augmentation by CHO intake (9) was not supported these or our results. The scope of this study and its conclusions were constrained by several limitations. Although the demographic variables seemed to support comparability between the study groups, there was a substantial disparity between study group sample sizes. In addition, the subject sample was restricted to females as this population may be more responsive to the modulation of CHO as a macronutrient in the diet (24). Therefore, the results from this study may not be applicable to males, even to males of a similar demographic. In the literature, non-ketogenic diets are often confounded with ketogenic diets. In general, it appears that most studies report potentially ketogenic diet samples, and that this type of diet should yield different metabolic effects than the nonketogenic type. To complicate matters, the descriptions of dietary manipulations in some studies have Diet and Fibromyalgia Symptoms 369 TABLE 1. Group sample characteristics. Group NKLCD Measure Age Education FMS Duration J Muscoskeletal Pain Downloaded from informahealthcare.com by University of South Alabama on 11/22/13 For personal use only. Binomial data Antidepressants Sleep meds. Pain meds. Compensation Hypoglyemia Counseling Guaifenisin WPD Statistic M SD N M SD N t p 53.75 13.25 13.00 8.62 1.50 8.72 4 4 4 45.97 14.00 10.29 7.98 1.54 7.32 29 29 29 1.814 .932 .679 0.079 0.404 0.502 % M rank N % M rank N U p 17.38 23.00 14.25 13.50 0.50 14.50 19.13 4 4 4 4 4 4 4 72 59 69 24 24 0.17 10 16.95 16.17 17.38 17.48 0.44 17.34 16.71 29 29 29 29 29 29 29 56.50 34.00 47.00 44.00 86.00 48.00 49.50 0.936 0.203 0.576 0.472 0.580 0.613 0.651 75 100 50 00 25 00 25 NKLCD, non-ketogenic, low-carbohydrate diet; WPD, Western pattern diet; FMS, fibromyalgia syndrome. TABLE 2. Sample group comparisons on measures of HAD Scales, POMS and FIQ. NKLCD Measure WPD Statistic M SD N M SD N t p d HADS HADSdep HADSanx HADStot 5.50 5.25 10.75 1.00 0.96 0.957 4 4 4 9.76 11.55 21.31 3.27 3.59 5.52 29 29 29 5.42 7.68 9.33 0.000 0.000 0.000 1.76 2.40 2.66 POMS TMDS Depression Tension Anger Vigor Fatigue Confusion 2.00 4.25 5.25 0.75 20.25 8.25 3.75 10.23 5.32 1.708 0.96 5.19 1.89 2.75 N 4 4 4 4 4 4 51.86 14.59 12.03 6.24 8.21 16.31 10.90 35.52 14.44 7.39 6.63 6.16 7.49 5.14 N 29 29 29 29 29 29 5.97 2.74 4.20 4.16 4.25 4.79 4.27 0.000 0.019 0.000 0.000 0.012 0.000 0.005 1.91 0.95 1.26 1.16 2.12 1.48 1.74 FIQ 52.58 8.26 4 66.86 15.41 29 2.84 0.027 1.91 HADS ¼ Hospital Anxiety and Depression Scale, POMS ¼ Profile of Mood States, TMDS ¼ Total Mood Disturbance Score, FIQ ¼ Fibromyaliga Impact Questionnaire, NKLCD ¼ non-ketogenic, low-carbohydrate diet, WPD ¼ Western Pattern Diet, FMS ¼ fibromyalgia syndrome not specified nor verified ketogenesis. Some studies that are unequivocally ketogenic have been reviewed here to fill in gaps in the literature that might have been filled by non-ketogenic studies, if they existed. The NKLC diets in general see greater adherence in the general public due to less dietary rigor coupled with a lack of signs and symptoms arising out of ketosis. Results of the study suggest that an efficacious dietary treatment may be developed through further applied studies. DIRECTIONS FOR FURTHER STUDY The ideal follow-up study would test the putative analgesic properties of a low-carbohydrate nonketogenic or ketogenic diet (25) through FMS-specific and general-research developed dolormetric and nociceptive measures throughout the life of the study using both objective and subjective measures. The use of tender points as a marker that is sensitive to change has come under question in recent years (26); therefore more responsive measures should be considered. The FIQR would be a good choice here, as well as the Modified Visual Analog Scale of the FIQ and measures of restorative sleep. Both NKLCD and KLCD groups should be studied with subjects randomly assigned to tease apart any discrete effects observed in each group. The ideal study would incorporate the use of diabetic reagent sticks for the in-stream assay of any ketone bodies in a mid-stream urine sample at A. Ernst & J. Shelley-Tremblay J Muscoskeletal Pain Downloaded from informahealthcare.com by University of South Alabama on 11/22/13 For personal use only. 370 regular intervals over the life of the study. This pilot study was able to attain to statistical significance and large effects sizes with small sample groups. However the population with FMS may contain a subgroup of dietary responders and therefore a larger sample group would enable the post hoc identification of any subject traits or patterns in the data that might be markers for responders or individuals refractory to response. A design employing repeated-measures ANOVA to follow before and after measures and Student’s t-test for group differences would capture time and group differences, along with measures of effect size. Despite an increase in acceptance of the construct of FMS within the rheumatology community there remains variance in the application of the American College of Rheumatology criteria and sparse use of algometry in the examination room. More progress needs to be realized in the area of differential diagnosis. Ideally subjects would be recruited directly from a rheumatology practice with physicians that are known to follow the most current ACR criteria. Any study lifetime should well exceed the standard 2-week period for carbohydrate washout and its commonly encountered malaise, fatigue and carbohydrate cravings. Therapeutic effects were shown in this present study with subjects despite no washout of prescribed antidepressants, pain meds, sleep medications or guaifenisin. As this pilot study showed significant group differences on all measures, it suggests that the observed effects were robust in the face of these concomitant treatments. DECLARATION OF INTEREST This study was funded entirely by the researchers using university facilities. REFERENCES 1. Centers for Disease Control and Prevention. Trends in Intake of Energy and Macronutrients – United States, 1971–2000 February 6, 2004/53(04): pp. 80–82. Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report. Retrieved March 2, 2013 from: www.cdc.gov/mmwr/ preview/mmwrhtml/mm5304a3.htm. 2. Christensen L, Burrows R: Dietary treatment of depression. Behav Ther 21: 183–193, 1990. 3. Eisinger J, Planatmura A, Ayavou, T: Glycolysis abnormalities in fibromyalgia. J Am Coll Nutr 13: 144–148, 1994. 4. Bazzichi L, Giannaccini G, Betti L, Fabbrini L, Schmid L, Palego L, Giacomelli C, et al: ATP, calcium and magnesium levels in platelets of patients with primary fibromyalgia. Clin Biochem 41: 1084–1090, 2008. 5. Bengtsson A, Henriksson KG, Larsson, J: Reduced high-energy phosphate levels in the painful muscles of patients with primary fibromyalgia. Arthritis Rheum 29: 817–821, 1986. 6. Somer E: Food and Mood, Henry Holt, New York, 1995. 7. Bell IR, Baldwin CM, Stoltz E, Walsh BT, Schwartz GE: EEG beta 1 oscillation and sucrose sensitization in fibromyalgia with chemical intolerance. Int J Neurosci 108: 31–42, 2001. 8. Christensen, L, Somers S: Comparison of nutrient intake among depressed and non-depressed individuals. Int J Eat Disorder 20: 105–109, 1996. 9. Wurtman, RJ, Wurtman, JJ: Carbohydrates and depression. Sci Am January: 68–75, 1989. 10. Bjorvell H, Ronnberg S, Rossner, S: Eating patterns described by a group of treatment seeking overweight women and normal weight women. Scand J Behav Ther 14: 147–156, 1985. 11. Christensen L, Krietsch K, White B, Stagner B: Impact of a dietary change on emotional distress. J Abnorm Psychol 94: 565–579, 1985. 12. Murphy P, Likhodii S, Nylen K, Burnham WM: The antidepressant properties of the ketogenic diet. Biol Psychiat 56: 981–983, 2004. 13. D’Anci KE, Watts KL, Kanarek, RB, Taylor HA: Low-carbohydrate weight-loss diets: Effects on cognition and mood. Appetite 52: 96–103, 2009. 14. Halton TL, Willett WC, Liu S, Manson JE, Stampfer MJ, Hu FB: Potato and French fry consumption and risk of type 2 diabetes in women. Am J Cin Nutr 83: 284–290, 2006. 15. Hu FB, Rimm E, Smith-Warner SA, Feskanich D, Stampfer MJ, Ascherio A, Sampson L, Willett WC: Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am J Clin Nutr 69: 243–249, 1999. 16. Shelley-Tremblay J, Ernst A, Kline J: The effects of sucrose consumption on left-frontal asymmetry and anger in persons with fibromyalgia syndrome. J Muscoloskelet Pain 17: 334–349, 2009. 17. Maher TJ: Effects of nutrients on brain function. Progress in Brain Research Vol. 122. Edited by EA Mayer, CB Saper, Elsevier Science BV, Amsterdam, 1999, pp. 187–194. 18. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, Tuqwell P, et al.: The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 33: 160–172, 1990. 19. Educational and Industrial Testing Service EdITS Manual for the Profile of Mood States (Rev. Ed.), EdITS, San Diego, 1992. 20. Zigmond, AS, Snaith, RP: The Hospital Anxiety and Depression Scale. Acta Psychiat Scand 67: 361–370, 1983. 21. Burkhardt CS, Clark SR, Bennett RM: The Fibromyalgia Impact Questionnaire: Development and validation. J Rheumatol 18: 728–733, 1991. 22. Piatti PM, Monti LD, Baruffaldi L, Magni F, Paroni R, Fermo I, Costa S, et al.: Hypocaloric high-protein diet improves glucose oxidation and spares lean body mass: Comparison to hypocaloric high carbohydrate diet. Metabolism 43: 1481–1487, 1995. 23. Galletly C, Moran L, Noakes M, Clifton P, Tomlinson L, Norman R: Psychological benefits of a low-protein, lowcarbohydrate diet in obese women with polycystic ovary syndrome – A pilot study. Appetite 49: 590–593, 2007. 24. Spring B, Maller O, Wurtman J, Digman L, Cozolino L: Effects of protein and carbohydrate meals on mood and performance: Interactions with sex and age. J Psychiat Res 17: 155–167, 1983. 25. Ruskin, DN, Masino, SA: The nervous system and metabolic dysregulation: emerging evidence converges on ketogenic diet therapy. Frontiers in Neuroscience 6: 1–12, 2012. 26. Harth, M: The fibromyalgia tender points: Use them or lose them? A brief review of the controversy. J Rheum 34: 914–922, 2007.