- •
advertisement

•
FOURIER POvffiR SPECTRUM ANALYSES
OF
ELECTROCARDIOGR~M
TRACES
by
Martha Melinda Brown
Honors Paper
Ball State University
May 1976
Adviser:
Dr. David Ober
TABLE OF CONTENTS
i
Lis1: of Tables and Figures
:r.
II.
III.
INTRODUCTION. • • • •
1
THE ELECTROCARDIOGRA11
2
A.
Electrical Activity of the Heart •
2
B.
The Standard Electrocardiogram •
8
C.
ST Depression
8
ANALYSIS • • • • • •
· 11
A.
Fourier Analysis • .
B.
Criteria for the Diagnosis of
Depression . • • • .
11
<
C.
IV.
V.
S~
• • • • • • • • • •
Patient Data
RESULTS
.
13
• • 13
15
A.
Lead I Analyses
• • 15
B.
Twelve Lead Analyses •
• • 18
CONCLUSION .
• 20
REE'ERENCES
21
APPENDIX A
• 22
APPENDIX B
. • • 34
LIST OF TABLES AND FIGURES
FiH. 1.
Distribution of the body fluids in tissue
with concentrations of the major cations
in the extracellular and intracellular
compartments.
·······.
·
3
···
5
Fig. 3.
Electrical conduction system of the heart ••
6
Fig. 4.
Sequential electrical events of the cardiac
cycle.
7
Power spectrum determination of a truncated
triangular wave ••
12
Fi~J •
2.
Fig. 5.
· ·
Activation of the excitable cell.
.. . . . . · · · · · · ·
. · ··
· · · · · · · . . . · · ·
Table
I. Normal limits of S-T Segments . . . • .
Table
II. Results of the Fourier power spectrum
analyses for lead I data. . • • • . •
Table III. Averages and standard deviations for leads
one through twelve. . • • . . • . • . • . .
I
i
9
16
19
I. INTRODUCTION
The electrocardiogram is a valuable tool in
diagnosing heart abnormalities.
Cardiologists have mainly
used visual methods for the clinical analyses of electrocardioqrams (EKGs).
utilizE~d
Hore recently, computers have been
to perform these analyses.
In this investigation EKGs were analyzed utilizing
a computer.
Specifically, Fourier analyses were performed
on various EKGs.
In an earlier study at Ball State Uni-
versity, Larry McCutchan investigated a similar problem
by using Fourier analysis on lead I electrocardiograms
for patients with ST depression.
His results indicated
that certain harmonics can be associated \"i th a depressed
ST segment.
The present study utilized the HcCutchan
criteri.a for investigating more lead I data and for investigating all twelve leads for selected normal and ST
depression patients.
For more information concerning the utilization of
Fourier analyses and computer programming in the diagnosis
of heart abnormalities, refer to the study by Larry
McCutchan. 1
--
II.
THE ELECTROCARDIOGRAM
A. Electrical Activity of the Heart
The heart is a muscle which pumps blood.
Electrical
activity triggers coordinated contractions of different
parts of the heart.
The electrical activity is controlled
by the impulses received in the cells of the muscle.
Many
times the impulses are broken causing electrical abnormali tiE~s called cardiac arrythmias.
Living cells in the body are controlled by three
parts; intracellular fluid, extracellular fluid, and the
cell membrane.
The extracellular fluid is composed of
various gases, electrolytes, metabolites, and water.
cell
mE~mbrane
The
constantly expends energy as it pumps differ-
ent electrolytes into and out of the cell.
The
electro~
lytes distribute themselves inside and outside the cell
membrane such that negatively charged ions collect on
the inside surface of the cell ':membrane and positively
charged ions collect on the outer surface.
This produces
a potential of about -85 millivolts (see Fig. 1).
When
this potential reaches a maximum charged state it is
termed a resting cell.
I
,-
The cell is waiting for a stimulus
which will neutralize the membrane.
This process, called
depolarization, causes the ions on the inner and outer
3
THE
-1_ _ _ BODY
UIDS
EXTRACELLULAR 1
--------+----
INTERSTITIAL
•
&
I
~
•
J....
"' ..
.#"
J
~
..,
J
1
~
....
....
...... .
"
.J
..
,
.' I
"I
\
\
'II"
.. "
.... "
\~
..
"
,
..
,
11 ..
:
\1 ... ". . '\~ ,
•
.:
..
, , ' ..
\. ..... !' .. ", "
,., . """"T, _"
'"
•,.,\..... ~J....L.1J .....
," ; ....•... \
,.
..
~
'"
,, ..
~
~
\.
,
..
\
.:
............
'"'
'.')
I
4
~
•
CONN"~CTIVE
TISSUE
sonIUr-r
POTASSIUM
Na+
K+
140
4 -
CALCIUK
ea++
5
I>1AGNESIUM
Mg++
2"-
Fig. 1.
10
150
1
40
Distribution of the body fluids in
tissue, with concentrations of the major cations in the
extracellular and intracellular compartments.
figure was taken from Ref. 2.
-
This
4
membrane surface to change positions.
This disturbance
of the :resting cell.is called an impulse.
Some cells do
not need any stimulation and depolarize automatically.
This impulse producer is known as automaticity and in the
heart is called the pacemaker.
Once depolarization
begins it spreads from cell to cell.
Following depolariza-
tion the cells begin to return to the resting state by the
process of repolarization (see Fig. 2).
']~he
betwee~
pacemaker of the heart lies in the right atrium
the superior and inferior vena cava (see Fig. 3).
This group of cells is known as the sinus node.
Impulses
begin here and travel through the heart in a depolariza-tion effect.
Since the impulse of the sinus node is weak,
the first measurable impulse is the depolarization of the
atrial muscle.
In the electrocardiogram this is labeled
the P wave (see Fig. 4).
The impulse spreads from the atria
to the ventricles by means of the A-V node.
These impulses
are not strong enough to be recorded by the electrocardiograph and thus are represented by the flat segment following the P wave.
The impulse travels to the common bundle
and splits into the right and left bundle branches.
The
impulse ·then moves from inside the ventricles to the outside.
The depolarization of the right and left ventricles
is recorded as the QRS complex.
The next segment is the
ST segment representing a period of electrical inactivity.
I
-
Repolarization of the ventricles is recorded as the T wave.
The T wa're is sometimes followed by a U wave which is the
5
STIMULATION
...;.-------
~1AXIMUM
-
--
NULL
Fig. 2.
Activation of the excitable cell.
This figure was taken from Ref. 2.
)
)
AORTA
SUPERIOR VENA CAVA
AURIClE OF RIGHT ATRIUM
PULMONARY VEoo
J
AURICLE OF LEFT ATRIUM
S .• A. NODE
LEFT ATRIUM (BACK OF HEART)
CORONARY SINUS
LEFT BUNDLE BRANCH
i
A.V. NODE
LEFT VENTRICLE
BUNDLE OF HIS
RIGHT BUNDLE BRANCH
RIGHT ATRMT
PURKINJE FIBERS
INFERIOR VENA CAVA
Fig. 3.
RIGHT VENTRICLE
Electrical conduction system of the heart.
was taken from Ref. 3.
This figure
'"
7
R
T.
1
SEQUENTIAL EIECTRICAL EVEN'IS
OF THE CARDIAC CYCLE
ELECTROCA?DICGRAPHIC
REPlBSSNTATICN
10
Impulse from the sinus node
not visible
2.
Depolarization of the atria
P wave
:3. Depolarization of the A-V node
4.
Repol~rlzation
of the atria
5. Depolarization of the ventricles
ao
b.
intraventricular septum
right and left ventricles
6. Activated state of the ventricles
IsoelectriC'
Usually ob3cured by the
Q,RS complex
QRS complex
a. initial portion
bo central and terminal
portions
St segment.
isoelectric
immediately after depolarization
7. Repolarization of the ventricles
8.
T wave
After-potentials following repolarization
of the ventricles
Fig. 4.
cardiac cycle.
U wave
Sequential electrical events of the
This figure was taken from Ref. 2.
8
sum of many repolarization events.
The electrocardiograph
records a flat signal on the baseline until the next beat
evolves. 2
B. The Standard Electrocardiogram
By placing electrodes at different points on the
body, electrocardiogram data for several leads can be
compared.
Different placements detect the same type of
information, but from different positions.
A standard
electrocardiogram utilizes twelve leads; six limb leads
(three bipolar and three unipolar) and six chest leads.
The difference in the ST segment for each lead can be
shown by comparing their normal limits of displacement
from the baseline.
These are shown in Table I.
c.
ST Depression
ST depression is a cornmon heart abnormality
appearing in electrocardiograms.
utilizing a stress test.
It often discovered by
Michael Ritota in Diagnostic
Electrocardiography defines ST depression as a ST segment
depression of one rom or more from the baseline. 3 ST
depression may be associated with many abnormalities
including ischemia, digitalis effects, right ventricular
hypertrophy, and complete bundle branch block,
The seg-
9
TABLE I. NOrn-~AL LD!ITS OF S-T SEc;r.~NTS
(This table was taken from Ref. 3.)
-
I
LEAD
S-T DISPLACEI:ENT
I
+1 to -1 mm.
II
+1 to -1 mm.
III
+1 to -1 mm.
aVR
+1 to -1 mm.
aVL
+1 to -1 mm.
aVF
+1 to -1 mm.
V1 ' V2
+2 to +4 TTun. to -1 TT'm.
V , V4 ' V ' V6
3
S
+2 to +4 mm. to -1 mm.
10
ment can be a horizontal, sagging, or angular depression •
-
.
-
III.
ANALYSIS
A. Fourier Analysis
A function which periodically repeats itself,
such as the electrocardiogram, can be represented by a
Fourier series.
The Fourier series for the function
f(x), over the interval (O,L), is given by the following
rela.tion: 4
~
f (x) = Ao/2
+y\~/0ncos (21inx/L)
+ Bnsin (Cfinx/LU
(1)
where
L
An
=
2/LJ f(x)cos(CfInx/L)dx
(2)
o
and
Bn
=
2/L
ro
l
f(x)sin(2finx/L)dx
(3)
and n is the number of the harmonic.
The coefficients, An and Bn' can be combined to form the
power spectrum coefficient, c n ' lV'hich is given by
(4)
When c n ' is plotted as a function of the frequency, a
power spectrum is obtained.
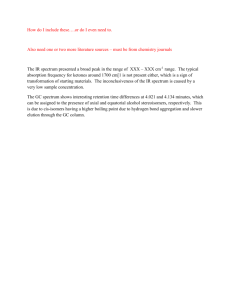
Shown in Figure 5 is the power spectrum for a
truncated triangular wave.
Since this function is an
even function, there are no sine terms and therefore, no
Bn
tE~rms.
12
r(x)
O.
-Y2 <x <-L/3
-t/3<x <
- 1 x,
o <'x
< 1/3
L/3 <x
< L/2
L
-it -1
2
o.
+lL +1-.
3
2L
t
3
0
A truncated triangle wave
.
10-1
..
10- 2
n
•
0
1
2
•
10-3
3
••
4
.5
10-4
6
7
10-5
.
o
'I
1
t
234
I
.5
,
t
6
7
Power spectrum for a truncated wave
Fig. 5.
Power spectrum determination of a
trun(:ated triangular wave.
Refer to reference 4.
cn0
.104
.007
.002
.0004
.0002
0
.00004
13
The computer program used in this investigation
to compute power spectra was developed in an earlier
study at Ball state University by McCutchan.
A listing
of t:he program and additional programming details are
givem in Ref. 1.
B. Criteria for the Diagnosis of ST DepresSion
Two criteria were developed for the diagnosis
of ST depression in an earlier study at Ball State
University performed by J'.lcCutchan. l
The first crlterion
to suggest ST depression was that the second power
spectrum coefficient (third harmonic), c2' be greater
than. nine per cent of the total power, Pt.
of all of the power spectrum coefficients.
P
is the sum
t
The second
criterion was that the ST score be less than three where
J...o
STscore =
«(Pt) ~ c n ) / (lOOOc2) •
n= 13
C; Patient Data
Digitized electrocardiogram data for 74
patients were obtained from the Public Health Service's
Ecan-E program.
A patient was defined as having ST
depression if two of the three ST segment voltage
readings were negative.
-
Of these 74 patients, 14 were
considered as having a depressed ST segment, 17 were
(5)
14
normal, and 43 had other abnormalities.
Lead I data were analyzed for all 74 patients.
All twelve lead EKGs for 13 normal patients, 10 ST
depressed patients, and 3 with other abnormalities were
also investigated.
Refer to Appendix A for the power
spectrum plots of twelve leads for a ST patient.
Details concerning the digitizing rate and stretching of the data for Fourier analysis has been given in
the previous study carried out by McCutchan. l
IV.
RESULTS
In the study conducted by McCutchan l , lead I
EKGs were investigated for 14 patients whose EKGs were
identified as normal and for 10 patients whose EKGs were
diagnosed as having ST depression.
Through these analyses
the t:wo criteria were developed (see Sec. III. B) to
identify ST depression.
These criteria were utilized
throughout the analyses of this investigation.
A. Lead I Analyses
The lead I EKGs were analyzed for 74 patients
whose EKG data were obtained from the Public Health
Service (see Sec. III. C).
Fourteen of these patients
were classified as having ST depression, 17 were classified
as normal, and the remaining 43 were classified as
having various abnormalities.
(These classifications
resulted from Ecan-E computer analyses of the l2-lead
EKG analysis.)
Presented in Table II are the results of
the Fourier power spectrum analyses.
It is seen that 21% of the 43 "abnormals"
-
satisfied both of the ST criteria, 16% satisfied one
of the criteria, and the remaining 63% were found to
16
-
Table II.
Results of the Fourier power spectrum
ana.1yses for lead I data.
Pat.ient
Number
Per cent
c
2
ST score
Both
One
None
Abnormal Patients
2
3
4
6
7
8
9
11
14
15
16
17
21
22
23
26
29
30
31
32
33
35
36
38
40
45
47
48
49
51
53
54
57
58
I
-
.59
62
63
'70
'71
73
}4
41.1
12.4
1.2
2.7
18.5
6.9
5.9
3.2
1.8
15.1
2.5
7.2
12.1
4.6
8.7
12.6
.3
8.0
2.8
12.4
11.4
15.1
3.2
9.3
2.2
1.3
4.1
9.9
2.8
.5
4.9
6.1
4.2
1.2
.3
4.9
16.4
4.3
8.2
3.0
11.4
.1
1.4
22.3
11.3
1.6
7.3
9.0
8.0
21.6
1.2
18.7
3.1
5.3
4.5
2.1
4.4
120.6
3.4
7.3
5.0
.9
1.2
12.4
4.6
15.8
20.9
9.5
3.3
9.3
71.2
2.9
3.9
9.1
26.7
95.6
3.8
.5
12.4
5.4
9.2
1.2
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
17
-
Table II. cont.
Pa't:ient
Number
76
79
Per cent
c2
ST score
14.6
5.7
.9
4.2
Both
One
*
None
*
ST Depression Patients
1
19
25
28
37
39
41
42
55
64
67
69
72
77
22.6
10.0
9.5
15.5
16.6
12.6
13.4
11.7
8.0
10.4
25.2
6.0
14.9
2.9
.7
1.4
2.9
.9
3.1
1.4
.8
1.3
3.2
2.1
.2
4.7
1.4
11.4
*
*
*
*
*
*
*
*
*
*
*
*
*
*
Normal Patients
5
10
12
13
18
20
24
27
43
44
46
50
52
56
60
65
78
2.1
11.5
1.4
8.3
3.1
8.3
5.1
1.5
8.4
3.2
6.6
6.4
3.8
16.2
4.1
1.7
6.9
16.5
5.0
29.6
2.9
12.2
4.0
5.6
18.9
2.4
15.2
7.3
3.5
10.1
1.3
7.5
14.4
4.0
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
18
satisfy neither of the ST criteria.
Of the 14 "ST"
patients, ten, one and three of the patients satisfied
both, one, and none of the criteria, respectively.
Of
the 17 "normal" patients, one, three, and thirteen of the
patients satisfied both, one, and none of the criteria,
respectively.
B. Twelve Lead Analyses
For 24 patients (13 normal and 11 ST depression) ,
all 12 EKG leads were Fourier analyzed to determine if
the two criteria developed to identify ST depression
in lead I EKGs might also be valid for other EKG leads.
Presented in Table III are averages and standard deviations for leads one through twelve for the (a) c 2 per cent
and (b) ST score criteria for both the "normal" and
"ST\! patients.
Presented in Appendix B are the raw
data from which these results were derived.
Leads 1, 11, and 12 show significant differences
bet\'{een the criteria averages for the normal and ST
patients in that the standard deviations for the averages
do not overlap.
a
dE~finite
Leads two through six and ten show
difference between the normal and ST patient
averages, however, these averages with the associated
standard deviations do overlap.
Very little difference
is c)bserved between the normal and ST patient averages
for either criterion when using leads seven, eight, and nine.
)
)
PER CENT CRITERION
LEAD
NORMAL
PATIENT
ST SCORE CRITERION
ST
PATIENT
NORMAL
PATIENT
ST
PATIENT
1
r= 1'\ +
..J.v
.,.
~.':1
14.1 ±
5.1
9.6 ±
5.0
1.5 ±
1.0
2
6.4 ±
3.5
10.3
±
4.5
6.7 ±
4.5
4.5 ±
4.7
9.9 ±
5.8
5.8 ±
8.4
5.2 +
-
5.6
±
4.8
4.3 +
-
7.5
±
3:·2
3.
,.,
n
16.1 +
- 11.5
4
4.4
±
2.0
10.8
±
4.1
8.9
5
6.7 +
-
4.8
13.7 +
-
6.7
10.9
6
12.1 +
-
9.3
9.1 +
-
6.6
5.3 -
7~1
7
12.4:!:
4/2
8.5
2.2 +
-
1.8
1.0 +
-
.6
8
18.2 +
-
7.0
16.7 +
17.1 +
-
6.8
·.2.3
±
2.2
2.5 +
-
3.1
9
11.5 +
-
7.6
11. 5 +
-
9.1
11.5 +
-
7.8
9.6 - 12.0
± 11.6
+
2.8
12.9 +
- 22.4
'"
10
4.3 +
-
3.7
11. 2 +
-
6.8
11
3.1 +
-
46.0 ""- 64.0
2.0
11. 8 f
5.4
22.6 +
- 27.4
+
5.0 2.4 +
-
12
2.8 +
-
1.8
12.1 +
-
5.9
17.1 +
- 13.4
2.3 +
- (·2.0
Table III.
5.1
1.7
Averages and standard deviations for leads one through twelve
I-'
\0
v.
CONCLUSION
A"primary purpose of this investigation was to
detE~rmine
whether the Fourier analysis of digitized EKG
data could be used to identify EKG abnormalities.
From
the results of this study, there does appear to be a
correlation between power spectrum coefficients and certain
heart abnormalities such as ST depression.
The criteria
used in this study for the diagnosis of ST depression
were affective with certain leads (namely one, eleven,
-
and twelve), however, several other leads (such as seven,
eight, and nine) showed no difference between normal and
ST patients.
In these cases additional studies may show
that different criteria for the diagnosis of ST depression
needs to be established which would utilize other harmonics
and/or combinations of harmonics •
-
.
21
-
-
.
REFERENCES
1:
Larry J. McCutchan, Identification of Abnormal ST
Segments in Electrocardiograms Using Fast Fourier
Transform Analysis, M.S. Thesis, Ball State University, November (1975).
2.
R. E. Phillips and M._ K. Feeney, The Cardiac
Rythms (W. B. Saunders Co., Philadelphia, PA, 1973).
3.
M. C. Ritota, Diagnostic Electrocardiography (J. B.
Lippincott Co., Philadelphia, PA, 1969).
4.
F. R. Merrill, Using Computers in Physics (Houghton
Mifflin Co., Boston, 1976) •
22
APPENDIX A
P\
1.0
~-
L \
'-
~
~
~
ir'"""'
""---
"'"'"
~
-
-1.0
100
10
(\J
w
0
::J
r--
~
i\
1
I
,
--1
CL
I
::t::
IT.
I
O. 1
0.01
0.001
10Fa
SOFa
PClWER SPECTRUM
120FO
23
1.0
,
w
o
::J
0
r-.I
0...
V
V
"
:c
a: .
V
"'"'-
/
r-----
----
/
/'
~
'-
~
...,....,.
N--
-
-
-1.0
1000
100
~I~
~
10
N
W
0
::J
r-
1
I
-.J
a...
:i:
a:
I
O. 1
\~
I
~
I
~
lVvl
0.01
I
I
I
!
I
I
~~
()
0.001
\
lOFa
60Fa
PClWER SPECTRUM
\
1\ 1\
I~
120f1J
24
-
1.0
lJ...J
o
~ 0 ~,
I~
::l
-1
CL
:s:::
a: .
\
~
~
~
-1.0
V
I--'
N
1000
--
100
10
Iv
~
I
\w-
I
I
I
I
N
I
lJ...J
0
::l
~
.......
I
-.J
(L
,
I
:L
a:
~~~
O. 1
I
I
(
~ ~~ A1//\
,
0.01
,
\
--
0.001
10Fo
60 Fi0
!
I 'IV
A
~.
l)
PClWEA SPECTRUM
!
~.
fV\
~fl ~
N1V
12( FU
V
25
-.
P I l..1...\
1.0
-
w
-
-
o
:::l
'-
:: 0
~
-'
CL
:s:::
~ ~~ ~
~V
/""
'\
(\ r '
~
-
a:
Iv
-1.0
1000
I~,
100
[\
~
I
I
I
10
I
N
r
W
0
I
:::l
r-
.........
I
1
-'
CL
II
~
:s:::
a:
-
I,
I
I
I
,I
I
!
I
I
,!
i
i
i
I
I
I
I.
I
,I
I
r
I
i
i
i
I
!
I
I
I
I,
,I
I
,I
I
O. 1
I
I
Ir
I
-
i
i
.~~
0.01
--
0.001
N
lOFo
~
~
60Fo
1J1 I
~
PClWER SPECTRUM
t
))
I
~i ~~
I
::r
120FO
26
1.0
~
-
r---.-
~
~
..-
II
.-,.
f"--
'-
~
l-
-1.0 I-
1000
100
10
~l,
I
I
1\
I
I
i
C\I
\
I..Ll
0
:::l
l-
I
-..J
(L
:s::
a:
f\
I
\11
O. 1
0.01
0.001
lOFa
\
I
Ii
I
I
I
I
I
I
II
I
I
I
II
II
r 1\
f\1~
SOFa
II
!
I
I
I
I
I
!i
I
I
I
I
I
I
II
J1'
\ ~t
~
PClWER SPECTRUM
II
~:
~
,
~\
j
!~
~
120fu
/
27
-
1.0
w
o
:::l
r- 0
~,
~
-1
(L.
~
a:
~
I,-r-"
~
~
~
-'"""
V
-
-
~
I-
-1.0
./\
I-
-
-
1000
I
I
-
100
niJfr
10
I
C\I
W
0
:::l
l-
I
I
I
I
I
-1
I
(1...
s::
I
IT.
V~!
O. 1
I
I
!'vi
I
I
I
I
" VI
~IJ
II
N
0.01
-
0.001
10Fo
I
60Fo
PClWEA SPECTRUM
I
I
J
I
-
I
I
!
iI
I
I
I
I
~
I
~
~
~U rf
120fo
lr
28
-
1.0
w
o
::J
0
r-l
CL.
s::
cr: .
-1.0
1000
-
v
-
"
l-
I
I
I
Ir
100'
~
~
I
II
I
10
N
W
0
:::J
r-
--<
1
1
-l
CL
I
s::
IT:
O. 1
0.01
-
0.001
i OFo
60Fo
P~WEA
SPECTRUM
120ft,
29
-
1.0
t-
-1.0
I
-
r---...
I
I
I
I
I
...;
I
I
i
I
10
l
I
N
w
0
::J
l-
I
-.J
0..
~
IT
O. 1
0.01
o. 0 0 1
'----1O+-Fi-o-+--+-----Ir-----t
60Fa
PClWER SPECTRUM
120fll
30
-1 .0
I
-
I
I
.,
-
r-
V
--
--
~
""'---
1
-1. Or-
-
!
1000
100
l
I
J
10
N
w
I
0
=:J
r-
1
I
I
.-J
CL
:c
a::
I
I
O. 1
0.001
I
I
II
I
I
0.01
I
I
-
1 CiFo
SOFo
P~WEA
SPECTRUM
I
I!
31
-
1.0
)
w
o
::)
.~
~ 0
.....J
(L.
:::E
a: .
-
t--
.,..~
-
-1.0
-
I
1000
ft'
100
I
I
I
I
I
10
(\J
w
I
I
I
I
II
0
::)
t>-1
i
--1
I
I
0..
:i:
I
IT.
I
I
I
I
O. 1
I
I
1\ \ n
0.01
-
0.001
10Fo
~
~ ~ VvAIjlll J
V
60Fo
PllWEA SPECTRUM
lA
120Fo
II
32
..-
r'\
1.0
w
o
:::J
I-
0
-.J
CL
:i:
0:.
-1.0
~v
-
,I
I
",,-
I...I
.........-- v
r
r
r
1000
100
10
~~
-
~
-
I
C\J
W
0
:::J
l-
I
-
-.J
CL.
:i:
IT.
I
O. 1
/:
~01
0.01
0.001
lOFo
(\
hJ\
60Fo
Pl:lWEA
IL.
SPECTRUM
I
.~ ~ A
1\
120Fo
33
1 .0
~
.--r- ~
~
r-
-
-1.0 r-
-
r-
1000
~
100
-
!
I
10
N
-
I
W
0
::J
t-
I
-1
I
........
u..
,i
J
I
I
I
s::
a:
I
I
I
I
I
O. 1
~I~
0.01
0.001
-
I
,
I
I
I
I
i
-
h
-
If
l)Fo
~
SOFe
P~WEA
~
N ~ bA Jl\ ~f\f 11
SPECTRUM
~
120FU
34
APPENDIX B
Table III.
Results of the Fourier power spectrum
analyses for leads one through twelve.
Pat:ient
Number
°2
Per cent
ST score
Both
One
None
Normal Patients
Lead 1
.-
10
18
27
5
46
50
60
13
20
43
44
52
65
11.5
3.2
1.5
2.1
6.6
6.4
4.1
8.3
4.2
8.4
3.2
3.8
1.7
5.0
12.2
18.9
16.5
7.3
3.5
7.5
2.9
8.5
2.4
15.2
10.1
14.4
*
*
*
*
*
*
*
*
*
*
*
*
*
Lead 2
10
18
27
5
46
50
60
13
20
43
44
52
65
3.0
.2
10.6
1.1
5.8
7.4
16.9
6.4
4.5
1.3
7.9
7.4
4.0
5.7
146.9
2.8
20.0
6.1
4.7
2.5
3.8
4.6
13.5
6.4
3.4
7.0
*
*
*
*
*
*
*
*
*
*
*
*
*
35
-.-"
.
Table III cont •
Lead 3
10
18
27
5.
46
50
60
13
20
43
44
52
65
20.8
1.6
31.0
2.4
3.1
25.4
21.9
32.6
4.2
11.5
9.9
11.3
33.2
1.3
19.5
3.6
28.9
9.8
1.3
.5
.6
3.6
•8
3.81.5
.6
*
*
*
*
*
*
*
*
*
*
*
*
*
Lead 4
10
18
27
5
46
50
60
13
20
43
44
52
65
2.8
1.8
5.7
4.1
3.5
2.9
7.2
6.1
4.1
6.4
7.3
4.4
1.4
13.4
16.5
5.6
6.8
12.5
9.8
5.2
3.5
5.7
3.9
7.2
7.2
18.9
*
*
*
*
*
*
*
*
*
*
*
*
*
Lead 5
.-
10
18
27
5
46
50
60
13
20
43
44
52
65
17.8
9.0
11.Q
.9
1.1
7.6
5.0
12.1
8.6
3.9
3.7
1.6
4.6
5.1
7.3
3.0
40.3
28.7
3.1
5.6
2.0
1.1
5.3
14.7
21.0
5.0
*
*
*
*
*
*
*
*
*
*
*
*
*
36
,-
Table III cont.
Lead 6
10
18.
2'2.
5
46
50
60
13
20
43
4~
52
65
10.9
1.0
12.1
10.7
3.2
19.2
37.0
6.1
4.5
21.7
·13 .. 0
6.2
11.4
.7
27.8
3.2
1.6
12.0
3.4
.9
3.6
4.2
1.7
3.0
4.1
3.0
*
*
*
*
*
*
*
*
*
*
*
*
*
Lead 7
10
18
27
5
46
50
60
13
20
43
44
52
65. ~
19.8
8.0
11.9
16.4
11.0
11.4
13.3
10.6
15.1
17.6
3.8
7.9
14.4
.5
1.9
2.3
1.2
2.7
1.8
1.6
1.7
2.0
10.4
7.2
4.3
1.4
*
*
*
*
*
*
*
*
*
*
*
*
*
Lead 8
10
18
27
5
46
50
60
13
20
43
44
52
65
(-
25.5
16.1
5.8
19.7
21.9
22.6
20.5
19.1
17.1
11.4
12.2
11.6
33.5
.9
.9
9.2
1.2
1.0
.8
.9
1.3
2.4
4.2
3.1
3.0
.5
*
*
*
*
*
*
*
*
*
*
*
*
*
37
-.
Table III. cont.
Lead 9
10
18
27
5
46
50
60
13
20
43
44
52
65
19.7
23.9
2.4
1.9
22.4
10.9
15.0
19.9
3.7
7.2
10.1
7.4
5.3
2.1
.7
14.0
29.9
1.5
6.3
2.7
1.9
15.2
6.5
5.1
9.0
6.8
*
*
*
*
*
*
*
*
*
*
*
*
*
Lead 10
10
18
27
5
46
50
60
13
20
43
44
.52
65
6.4
.3
3.3
1.1
11.7
6.1
7.5
7.3
.3
8.6
1.9
1.6
.1
11.8
106.2
8.4
32.5
5.5
8.0
8.3
7.9
134.4
3.2
27.8
23.0
220.7
*
*
*
*
*
*
*
*
*
*
-#:
'*
*
Lead 11
10
18
27
5
46
50
60
13
20
43
44
52
65
.4
.9
3.7
2.2
2.9
6.1
4.0
6.7
1.8
4.6
2.0
4.5
.8
110.9
32.3
7.3
13.9
15.3
6.1
8.9
5.5
21.1
4.7
24.8
6.9
36.3
*
*
*
*
*
*
*
*
*
*
*
*
*
38
.-.
Table III.
cont •
Lead 12
10
18
27
5
46
50
60
13
20
43
44
52.
65
.9
1.7
1.4
2.5
.7
7.0
4.4
2.3
1.3
3.5
1.8
5.6
2.6
31.8
17.4
18.1
10.2
53.9
4.6
6.2
12.1
20.9
5.3
25.5
5.5
10.7
*
*
*
*
*
*
*
*
*
*
*
*
*
ST Patients
Lead 1
25
28
1
39
19
41
42
64
67
72
79
9.5
15.5
22.6
12.6
10.0
13.4
11.7
10.4
25.2
14.9
9.7
25
28
1
39
19
41
·42
64
67
72
'79
6.2
7.3
7.8
14.0
18.1
2.6
8.8
8.6
14.0
10.3
16.0
2.9
.9
.7
1.4
1.4
.8
1.3
2.1
.2
1.4
3.5
Lead 2
7.5
1.9
14.8
.6
.7
12.6
1.6
2.2
1.2
2.6
3.2
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
*
39
,-.,
Table III. cont.
Lead 3
25
28
1
39
19
41
42
64
67
72
79
6.9
6.6
14.0
11.4
16.1
2.5
2.5
5.0
22.3
12.1
9.2
4.4
5.5
.9
1.2
.8
19.9
9.1
10.0
.05
2.8
2.6
*
*
*
*
*
*
*
*
*
*
*
Lead 4
25
28
1
39
19
41
42
64
87
72
79
11.1
13.2
12.3
13.2
.8
6.7
10.1
10.0
17.2
14.1
9.9
.9
1.0
2.9
1.0
27.7
3.9
1.7
1.7
.8
1.7
4.4
*
*
*
*
*
*
*
*
*
*
*
Lead 5
25
28
1
39
19
41
42
64
67
72
79
7.1
14.4
27.5
8.7
13.4
16.9
3.7
11.2
23.3
15.7
8.2
3.8
1.5
.2
4.1
.8
.7
12.0
2.1
.04
1.4
3.9
*
*
*
*
*
*
*
*
'*
*
*
40
-
Table III. cont.
Lead 6
25
28
1
39
19
41
42
64
67
72
79
4.6
1.7
10.9
13.2
17.8
.7
5.3
.8
19.6
8.4
16.6
4.3
5.9
3.4
.7
.5
73.2
.~ 3.8
43.8
.3
4.4
1.4
*
*
*
*
*
*
*
*
*
*
*
Lead 7.
,-
25
28
1
39
19
41
42
64
67
72
79
15.3
16.9
11.3
21.4
23.8
15.9
15.5
14.7
19.9
27.2
1.4
1.3
1.0
.8
.2
.6
1.2
2.3
.5
1.0
X
X
*
*
*
*
*
*
*
*
*
*
*
Lead 8
25
28
1
39
19
41
42
64
67
72
79
16.1
15.1
5.4
20.8
27.9
21.6
16.9
8.3
19.2
26.7
9.6
1.8
2.3
2.8
1.6
.2
.3
.6
9.8
.4
.4
7.6
*
*
*
*
*
*
*
*
*
*
*
41
-,
Table III. cont.
Lead 9
25
28
1
39
19
41
42
64
67
72
79
4.9
1.6
5.9
11.0
24.8
27.2
17.8
4.9
20.7
.6
7.5
11.6
30.8
3.7
1.6
.4
.3
.2
13.8
*
*
*
*
*
*
*
.5
35.6
6.8
*
*
*
*
Lead 10
25
28
1
39
19
41
42
64
67
72
79
1.8
4.3
16.5
19.4
21.7
17.9
7.5
2.4
.4
.4
X
X
10.7
4.5
18.4
7.7
6.5
3.4
7.9
.2
2.9
7.0
*
*
*
*
*
*
*
*
*
*
Lead 11
25
28
1
39
19
41
42
64
67
72
79
8.2
15.2
20.5
19.2
7.1
3.7
12.3
8.2
15.0
12.1
7.8
2.6
1.1
1.3
.4
2.0
6.0
1.9
2.3
.6
1.9
5.7
*
*
*
*
*
*
*
*
*
*
*
42
Table III. cont.
,.-,
Lead 12
25
28
1
39
19
41
42
64
67
72
79
-
15.2
16.8
23.7
17.6
3.0
6.4
12.3
9.9
9.4
13.5
5.7
1.8
.7
.8
.4
3.7
3.2
1.4
1.6
2.4
1.7
7.8
*
*
*
*
*
*
*
*
*
*
*