Tumor Therapy
advertisement

A Novel Nanodelivery System for Combination
Tumor Therapy
By
David A. Eavarone
B.S. Biomedical Engineering
Case Western Reserve University, 2000
Submitted to the Biological Engineering Division
in partial fulfillment of the requirements for the degree of
MASTER OF SCIENCE IN BIOLOGICAL ENGINEERING
AT THE
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
February 2004
© 2004 Massachusetts Institute of Technology
All Rights Reserved
MASSACHUSETTS INSTImTTE
OF TECHNOLOGY
LIBRARIES
Signature of Author:
Biological Engineering Division
February 5th, 2004
.
v
Certified by:
Ram Sasisekharan
Professor of Biological Engineering
Thesis Supervisor
Accepted
Acceptedby: _
by:
I
/I
- /
TC
K. Dane Wittrup
JP Mares Professor of Chemical Engineering and Biological Engineering
Chairman of Thesis Committee
OF TECHNOLOGY
ARCHIVES
LIBRARIES
A Novel Nanodelivery System for Combination Tumor Therapy
By
David A. Eavarone
Submitted to the Division of Biological Engineering on February 5th, 2004
in Partial Fulfillment of the Requirements for the Degree
of Master of Science in Biological Engineering
Abstract
Anti-angiogenic therapy offers many benefits over traditional cytotoxic
chemotherapy including fewer toxic side effects and the reduced development of drug
resistance. Anti-angiogenics alone have not proven effective in inducing tumor
regression in the clinic due to both the cytostatic nature of anti-angiogenic therapy and
the potential formation of new regions of hypoxia within the tumor after therapy. The
new therapeutic paradigm is for combining both anti-angiogenics and traditional
cytotoxic agents for a synergistic effect. The efficacy of cytotoxic agents may be reduced
after anti-angiogenic therapy, however, due to limited access to tumor vasculature and
hypoxia-induced drug resistance. We propose that loading cytotoxic agents within the
tumor prior to blood vessel collapse will enable both greater drug accumulation within
the tumor as well as a reduction in the formation of therapy-induced regions of hypoxia.
We present here a novel nanodelivery vehicle termed a 'nanocell' for the spatio-temporal
recruitment of both anti-angiogenics and cytotoxic agents within the solid tumor to
achieve this goal. Nanocells consist of a polymeric nanocore encapsulating the cytostatic
agent doxorubicin surrounded by a lipid vesicle containing the anti-angiogenic agent
combretastatin A4. Nanocell treatment resulted in an 88% reduction in tumor size in
vivo, compared to a 66% reduction in tumor size after delivering combretastatin A4 lipid
vesicles and doxorubicin nanocores simultaneously but separately. Nanocell treatment
also resulted in a significant reduction in systemic toxicity, fewer metastases to the lung
and liver, and a greater degree of tumor apoptosis.
2
Acknowledgements
I would first and foremost like to thank my research advisor Ram Sasisekharan
who has been an outstanding mentor and an inspiration throughout my time here. I
would also like to thank my labmates and colleagues without whose assistance and
expertise this thesis would not have been possible. I would like to first thank Dr.
Shiladitya Sengupta, whose inspiring ideas and pharmacological expertise helped this
research to succeed like it did. I would also like to thank Dr. Ishan Capila for his
expertise and work on drug-polymer linkages and Dr. Ganlin Zhao for her expertise and
work on polymer formulations.
I would also like to thank Tanyel Kiziltipe for her work
preparing YFP-B 16F 10 cells, and Nikki Watson for her expertise on electron
microscopy. I would also like to thank the other members of Ram's lab who have all
made great contributions to my scientific and personal growth. I also owe many thanks
to my parents for their support over the years and to Lisa Haas who recently became my
wife. This thesis would not have been possible without her support and understanding.
would also like to thank the Whitaker Foundation for funding this study.
3
I
Table of Contents
Abstract...................................... .................
2..........
.................................................................................
Acknowledgements
Table of Contents......................................
...................
3
4.........
Chapter
1.
1.1.
1.2.
Introduction
..................................................................
Anti-angiogenics: Cutting off the Tumor Blood Supply.......................
Nanotechnology in Cancer Therapy ...............................................
5
5
9
Chapter 2. Materials/Methods ..................................................................
.............................
2.1. Synthesis/Characterization of Nanocells .........
2.1.a. Synthesis/Characterization of Nanocores .............................
2.1.b. Synthesis/Characterization of Lipid Vesicles........................
2.1.c. Encapsulation of Nanocores within Lipid Vesicles..................
12
12
12
14
14
2.2 In Vitro Evaluation in Co-culture Assay ..........................................
15
2.3. In Vivo Evaluation in Murine Melanoma Model .........
...................
2.3.a. Murine Melanoma Tumor Model ......................................
2.3.b. Immunohistocytochemistry of Tumor Vasculature ..................
.. .........
2.3.c. Quantifying Apoptosis in Tumor Sections.........
2.3.d. Analysis of Metastatic Nodes ...........................................
16
16
17
18
18
Chapter 3. Results .................................................................
3.1. Synthesis/Characterization of Nanocells .........................................
3.1 .a. Synthesis/Characterization of Nanocores ................................
3.1.b. Synthesis/Characterization of Lipid Vesicles...........................
3.1.c. Encapsulation of Nanocores within Lipid Vesicles....................
3.2. Evaluation of the Therapeutic Benefit of Nanocells ............................
19
19
19
20
21
23
Chapter 4. Discussion..................................................................
30
References
.....................................................
36
4
Chapter 1. Introduction
Current chemotherapeutic approaches are limited by the development of drug
resistance, palliative outcomes, and global systemic toxicity, leaving a niche for newer
strategies. Promising new molecules called anti-angiogenics are in advanced clinical
development stages as an alternative treatment for their inhibitory activity against tumor
vasculature. Anti-angiogenics are specific for dividing endothelial cells and are thus not
as likely to cause the toxic systemic side-effects characteristic of traditional
chemotherapeutic agents. Vascular endothelial cells are also far more genetically stable
than the tumors they inhabit, and are thus less likely to develop drug resistance even after
prolonged treatment.(1) We present here the development of a novel nanodelivery
system for the efficient delivery of anti-angiogenics in combination with traditional
cytotoxic agents for an enhanced therapeutic effect.
1.1. Anti-Angiogenics:
Cutting off the Tumor Blood Supply
The term angiogenesis describes the formation of new capillaries from existing
vasculature (for review see(2)). While the adult vasculature is primarily quiescent,
angiogenesis occurs physiologically during embryonic development, wound healing, and
the menstrual cycle. Angiogenesis is also implicated in certain pathological conditions
including cancer. As a tumor undergoes rapid growth, existing vasculature is co-opted to
ensure that cells maintain an adequate nutrient supply and are able to efficiently remove
waste(3, 4). Vascular cooption is confined to the tumor periphery and gradual tumor
expansion causes a progressive central hypoxia. In order for these hypoxic cells to
survive they must switch to an angiogenic phenotype(5, 6). Some tumor clones remain
5
dormant for many months and are thus confined within several millimeters in diameter
until they activate an angiogenic pathway(7). Hypoxia, through hypoxia inducible factora, induces the expression of pro-angiogenic factors and may result in an angiogenic
phenotype if proangiogenic factors are in excess of antiangiogenic factors(8). The
balance between proangiogenic and antiangiogenic conditions is affected by a variety of
factors including metabolic and mechanical stresses, hypoxia, and genetic mutations(9).
Once initiated, tumor angiogenesis is characterized by a regulated series of
sequential steps (for review see(9)). Angiogenic factors produced by tumor cells bind to
endothelial cell receptors and initiate angiogenesis. Matrix metalloproteinases (MMPs),
released by activated endothelial cells, degrade the basement membrane and extracellular
matrix (ECM) surrounding already existing capillaries near the tumor site. The break-up
of ECM releases additional pro-angiogenic factors further enabling the switch to an
angiogenic phenotype(10). Pro-angiogenic stimuli cause endothelial cell junctions to
become altered with newly formed cell projections growing towards the source of the
stimulus. Endothelial cells then migrate into the tumor ECM and proliferate. There,
newly formed endothelial cells organize into hollow tubes in a process called
canalization. The fusing of these newly formed vascular tubes with the creation of new
basement membrane enables blood flow within the tumor.
The vascular density of tumors is highly heterogeneous, and tumor blood vessels
exhibit many abnormalities when compared to normal vessels including a high
percentage of proliferating endothelial cells, an increased tortuosity, and aberrant
basement membrane formation(1 , 12). As a result, tumor blood vessels exhibit marked
extravasation or vessel wall hyperpermeability. Molecular transport across tumor vessels
6
may occurr via a number of pathways including interendothelial junctions and
transendothelial channels, vesicular vacuole organelles, and fenestrations(13). The pore
cutoff size of the tumor vasculature varies depending upon tumor model, however it is
most commonly reported to range between 400 and 800nm(13, 14).
The first convincing evidence that tumor growth may be angiogenesis dependent
came in 1968 with an experiment demonstrating that implanted tumor tissue in nonvascularized rabbit cornea did not grow until newly formed vessels from the limbus
reached the implant(15).
Since then, a large body of work has gone into uncovering the
factors responsible for promoting tumor angiogenesis as potential targets for new therapy.
Such factors currently include vascular endothelial growth factor (VEGF), basic
fibroblast growth factor (bFGF), platelet-derived endothelial growth factor (PDGF),
fibronectin, scatter factor (SF), and others (for review see(16)). Currently explored antiangiogenic agents are of at least three classes: agents that are directly cytotoxic or static
against endothelial cells, agents that inhibit growth factor release, and agents that block
growth factor signaling (for review see(1)).
Several angiogenic inhibitors are currently under study in Phase I, II, and III
clinical trials (see http://www.cancer.gov/clinicaltrials
for current trials). Contrary to a
promising body of successful work using anti-angiogenics in animal tumor models, the
best outcomes from these clinical studies have been, with few exceptions, stabilization of
tumor growth over a defined period(17). An explanation for these relatively
disappointing findings has been offered on several rationales(l7).
Most animal studies
on which the success of anti-angiogenics are based are performed with ectopically
growing subcutaneously implanted tumors. Due to the relative sparseness of vasculature
7
within the subcutis, tumors in these studies are then expected to be more dependent on
new vessel formation than tumors that grow orthotopically(18). Also, tumor cells used in
animal studies are highly selected compared to the heterogeneous mixture of cells found
in patients. Tumor cells expressing specific genetic markers have demonstrated marked
susceptibility or resistance to anti-angiogenic treatments(19). Further difficulty in
analyzing the effect of anti-angiogenics comes from finding clinical parameters for
measuring their success(20). With current cytotoxic therapies, tumor reduction is the
major parameter for measuring treatment success. With anti-angiogenics, however, the
lack of tumor regression may not always indicate a failure, as the mechanism of action of
anti-angiogenics is often cytostatic in nature(1).
While there is compelling experimental evidence that at least certain types of
tumors are angiogenesis dependent, recent clinical trials have demonstrated that purely
anti-angiogenic treatments are not as effective for achieving tumor regression as was
originally hoped. The growing consensus is towards combination therapy(1, 5, 17), using
anti-angiogenics as well as traditional chemotherapy for a synergistic effect. This,
however, has been more difficult than was originally anticipated. While combination
therapy has been shown in many cases to be beneficial(21, 22), recent evidence has
demonstrated that interactions between anti-angiogenic and cytotoxic agents may in fact
be antagonistic in certain tumor models. Anti-angiogenics, by cutting off the tumor
blood supply, may in turn induce new regions of tumor hypoxia(23, 24). Tumor hypoxia
not only contributes to the induction of angiogenesis through the release of hypoxia
inducible factor-a, but it also has been correlated with an increase in tumor invasion and
metastasis(23). Of particular concern is the effect of hypoxia on the efficacy of
8
traditional chemotherapeutic agents. While it can be expected that reduced blood flow
within the tumor will reduce the access of an intravenously administered drug, hypoxia
has also been shown to contribute directly to cytotoxic drug resistance over a range of
tumor models(25). While this resistance is likely due in part to reduced cell proliferation
within hypoxia regions of tumor(25), upregulation of hypoxia inducible factor-a has also
been correlated with the upregulation of the anti-apoptotic protein Bcl-2 and the multidrug resistance product P-glycoprotein(26, 27). We propose that this antagonistic effect
may be minimized by the controlled loading of cytotoxic agents within vascularized
regions of tumor prior to blood vessel collapse. Blood vessel collapse at the site of
cytotoxic agent delivery may provide the added benefit of trapping the drug within the
tumor thus reducing systemic toxicity while promoting drug action. We relied upon
extensions to the existing art of nanoscale drug delivery to approach this goal.
1.2. Nanotechnology in Cancer Therapy
Nanoscience has been described as one of the most important research and
development frontiers in modem science(28). Nanoscale particles are of an interest
fundamentally because nearly all physical properties of a material change when the size
of the particles making up the material are nanoscopic. One prominent use of nanoscale
particles in medicine involves the use of gold nanoparticles in medical diagnostic kits.
The small size and shape of these particles enables gold to show virtually all colors of the
rainbow while macroscopic quantities of gold may only show one color(29). Other uses
of nanoparticles in medicine include their use as vehicles for DNA transfection, enzyme
encapsulation, biosensors, and drug delivery(28). The use of nanoparticles in drug
9
delivery has offered considerable promise for the enhanced delivery of chemotherapeutic
agents. Encapsulation within or binding to small colloidal particles enables drugs in
many cases to circulate longer, accumulate preferentially within tumor tissue, have
reduced systemic toxicity, undergo controlled release, and even bypass certain cellular
mechanisms of drug resistance (for review see(30)).
Recently, the design of multichamber nanoparticle devices has been of benefit for
improving the utility of nanotechnology in biomedical applications. The encapsulation of
fluorescent semiconductor nanocrystals (quantum dots) within block-copolymer micelles
has enabled enhanced biocompatibility for both in vitro and in vivo imaging(3 1).
Micellar nanocontainers consisting of a core containing an active therapeutic agent
surrounded by a block-copolymer micelle has assisted in water dispersability of the agent
and efficient delivery to specific cytoplasmic organelles(32). Drug-loaded polymeric
chitosan vesicles encapsulated within lipid have been demonstrated to enable controlled
release of a single agent altered by the presence of the outer lipid chamber(33).
The
advantages and pitfalls of current combination therapy have established a potential
benefit for single vehicles able to deliver multiple drugs having different modes of action
with controlled and distinct release properties. The use of multi-chambered nanodelivery
vehicles has logical extensions to this application.
We demonstrate here a novel nanodelivery system for the spatio-temporal
recruitment of anti-angiogenics and traditional cytotoxic agents at the site of tumor for a
more optimal anti-tumor effect than standard co-administration of the two therapies. This
delivery system consists of a small (<100nm) polymeric nano-core surrounded by a larger
(-200nm) spherical lipid bilayer shell. Both the nano-core and the surrounding lipid shell
10
are able to encapsulate separate chemotherapeutic agents with different release
characteristics.
In this case, the cytoxic drug doxorubicin is covalently encapsulated
within the nano-core, while the anti-angiogenic agent combretastatin A4 is preferentially
partitioned within the lipid bilayer. These drug-loaded 'nanocells' are passively taken up
by the tumor's leaky vasculature through extravasation, though they may also be targeted
to tumor by means of ligand or antibody binding. We demonstrate here that this system
enables a substantially greater anti-tumor effect than traditional co-administration of the
two agents, as well as less systemic toxicity and tumor metastasis.
11
Chapter 2. Materials/Methods
2.1. Synthesis/Characterization
2.1.a. Synthesis/Characterization
of Nanocells
of Nanocores
Polylactic glycolic acid (PLGA) (Medisorb® 5050 DL 4A), having a lactide /
glycolide molar ratio of 50/50, was obtained from Alkermes (Wilmington, OH). The
average molecular weight of this polymer is reported to be 61 kDa and it has free
hydroxyl and carboxylic groups at its terminal ends. Doxorubicin hydrochloride, p-
nitrophenyl chloroformate, polyvinyl alcohol (PVA) (Av. Mol. Wt. 30,000-70,000), and
triethylamine were obtained from Sigma-Aldrich (St. Louis, MO). All other reagents and
solvents were analytical grade.
The conjugation of doxorubicin to PLGA was performed as described
previously(34). Briefly, 1.5 g of PLGA 5050 DL 4A was dissolved in 15 ml of methylene
chloride and activated by the addition of 14 mg of p-nitrophenyl chloroformate and 9.4
mg (- 9.6 ptL) of pyridine to the solution, kept in an ice bath at 0 °C (stoichiometric
molar ratio of PLGA: p-nitrophenyl chloroformate: pyridine = 1:2.8:4.7). The reaction
was carried out for 3 hours at room temperature under nitrogen atmosphere. The
resulting solution was diluted with methylene chloride and washed with 0.1 % HCl and
brine solution. The organic phase was separated, dried on anhydrous magnesium sulfate,
filtered, and then rotary-evaporated to yield activated PLGA polymer. Activated PLGA
(0.4g) was dissolved in 3 mL of dimethylformamide (DMF) and reacted with 4 mg of
doxorubicin and 2.7 mg (- 4 ptL)of triethylamine for 24 hours at room temperature under
nitrogen atmosphere (stoichiometric molar ratio of activated PLGA: doxorubicin:
12
triethylamine = 1:1:4). The final conjugated product was precipitated by the addition of
cold ether then washed with ether, filtered, and dried under vacuum.
Nanocores were formulated using an emulsion-solvent evaporation technique
similar to that described previously(34).
Briefly, 50mg PLGA-DOX was allowed to
dissolve completely in 2.5mL acetone for one hour at room temperature. At this time,
0.5mL methanol was added and the entire solution was emulsified into an aqueous
solution of PVA (0.5 g / 25 mL) by slow injection with constant homogenization using a
tissue homogenizer followed by one minute of sonication (Misonix, Farmingdale, NY).
The emulsion was added to a dilute aqueous solution of PVA (0.2 g / 100 mL) with rapid
mixing for 3 hours at room temperature to evaporate any residual acetone or methanol.
Nanocore size fractions were recovered by ultracentrifugation
at 8,000, 15,000, 20,000,
and 22,000 RPMs. Nanocores from the smallest size fractions were extruded through a
100nm membrane using a hand-held extruder (Avestin, Ottawa, ONT) to obtain
nanocores for encapsulation within nanocells. The nanocores were sized by dynamic
light scattering (Brookhaven Instruments Corp, Holtsville, NY) as well as by SEM. For
SEM preparation, nanocores were lyophilized for 72 hours following which a small
quantity was dusted onto a carbon grid and coated with gold. Particles were analyzed
using a Philips EM at a magnification of 65000X. All nanocores were used within 2
hours of synthesis to minimize aggregation.
13
2.1.b. Synthesis/Characterization of Lipid Vesicles
Cholesterol (CHOL), egg-phosphatidylcholine
(PC), and
distearoylphosphatidylcholine - polyethylene glycol (m.w. 2000) (DSPE-PEG) were
obtained from Avanti Polar Lipids (Birmingham, AL). Combretastatin A4 was obtained
from Tocris Cookson (Ellisville, MO). All other reagents and solvents were of analytical
grade.
Lipid vesicles consisting of PC:CHOL:DSPE-PEG (2:1:0.2 molar) were prepared
by dissolving 27.5mg lipid in 2mL chloroform in a round bottom flask. 12.5mg of
combretastatin A4 was co-dissolved in the choloroform mixture at a 0.9:1 drug:lipid
molar ratio. Chloroform was evaporated using a roto-evaporator to create a monolayer
lipid/drug film. This drug/lipid film was resuspended in lmL H2 0 after one hour of
shaking at 65C to enable preferential encapsulation of combretastatin A4 within the lipid
bilayer. The resulting suspension was extruded through a 200nm membrane at 65°C
using a hand held extruder (Avestin, Ottawa, ONT) to create unilamellar lipid vesicles.
The average vesicle size was determined by dynamic light scattering (Brookhaven
Instruments Corp, Holtsville, NY). Encapsulation efficiency was determined by passage
of the drug/lipid vesicle mixture through a PD-10 column containing Sephadex G-25
(Pharmacia Biotech) with UV monitoring of combretastatin A4 elution at 290nm.
2.1.c. Encapsulation of Nanocores within Lipid Vesicles
PLGA-I)OX nanocores were prepared as described above, and nanocores -100nm
were selected for encapsulation in nanocells by extrusion through a 100nm membrane.
When synthesizing combretastatin A4 lipid vesicles, nanocores containing 250ktg
14
doxorubicin were added to the aqueous lipid resuspension buffer. The mixture was
analyzed using TEM to determine encapsulation efficiency. Briefly, the sample was
fixed in 2.5% gluteraldehyde, 3% paraformaldehyde with 5% sucrose in 0. 1M sodium
cacodylate buffer (pH 7.4), embedded in low temperature agarose and post fixed in 1%
Os04
in veronal-acetate buffer. The sample was stained overnight with 0.5% uranyl
acetate in veronal-acetate buffer (pH 6.0), and then dehydrated and embedded in epon812 resin. Sections were cut on a Leica ultra cut UCT at a thickness of 70nm using a
diamond knife, stained with 2.0% uranyl acetate followed by 0.1% lead citrate and
examined using a Philips EM410.
2.2. In Vitro Evaluation in Co-culture Assay
Cell incubation was performed at 37°C in a humidified atmosphere containing 5%
CO2 . B 16F 10 murine melanoma cells were obtained from ATCC (Rockville, Maryland)
and were previously transfected with yellow fluorescent protein (YFP) and selected under
puromycin pressure. YFP-B16F10 colonies were confirmed to express YFP using
epifluorescence microscopy and fluorescence activated cell sorting. B 16F 10 were
cultured in MEM-a (Invitrogen, Rockville, Maryland) supplemented with 10% fetal
bovine serum (FBS). Human umbilical vein endothelial cells (HUVECs) were obtained
from Cambrex (East Rutherford, NJ) and were pooled from three donors. HUVECs were
cultured in EBM media (Cambrex) supplemented with bullet kit (Cambrex) and 20%
FBS.
YFP-B 16F 10 and HUVEC cells were co-cultured to determine the differential
effects of nanocells on tumor and vasculature. Briefly, growth factor reduced Matrigel
15
(Invitrogen) was plated on glass coverslips where it was allowed to gel at 37°C.
HUVECs were trypsinised and plated on the Matrigel coated coverslips at a density of 3
x 104 cells per coverslip. Coverslips were cultured in 12 well tissue culture plates for 24
hours allowing HUVECs to form tube-like structures. YFP-B 16F10 cells were then
trypsinized and plated in each well at a density of 1 x 104 cells/well. The co-culture was
allowed to develop a further 24 hours before treatment formulations were added.
Treatment formulations consisted of i.) control, ii.) lipid vesicles containing 351LM
combretastatin A4, iii.) nanocores containing 25gM doxorubicin, and iv.) drug-loaded
nanocells. After incubation with treatment for 12 or 30 hours, the cells were fixed with
4% paraformaldehyde on ice for 20 minutes and then incubated with propidium iodide to
label the nuclei. The coverslips were washed with phosphate buffer saline (PBS), and
analyzed using a Leica LSM510 confocal microscope. Images were captured randomly
from four sectors at a resolution of 510X510 pixels. The FITC and Rhodamine images
were merged to create the final image. Quantification of the area covered by endothelial
cells or YFP-B 16F 10 cells was carried out using a planimetric point-count method using
a 224-intersection point square reticulum. Data were expressed as the ratio of each
component to the total area covered by cells.
2.3. In Vivo Evaluation in Murine Melanoma Model
2.3.a. Murine Melanoma Tumor Model
Twenty-four male C57/BL6 mice (Charles River Laboratories, Wilmington, MA)
weighing approximately 25g were subcutaneously injected with 3x 105 YFP-B 16F10 cells
into the right flank on day 1. Fifteen of these mice were selected for tumors of
16
approximately 150mm3 in volume on day 9 and randomized into five different treatment
groups. Treatments consisted of tail vein injections of 100pL sterile H20 containing
either i.) control, ii.) lipid vesicles containing 50mg/kg or 25mg/kg combretastatin A4,
iii.) nanocores containing lmg/kg doxorubicin, iv.) combretastatin A4 lipid vesicles
simultaneously injected with doxorubicin nanocores, and v.) drug-loaded nanocells. A
total of three treatments were administered through the tail vein every alternate day until
the animals were sacrificed on day 14 and the tumors were excised for histopathology.
1
ml of blood was drawn through cardiac puncture and profiled for white blood cell counts
and hemoglobin levels.
2.3.b. Immunohistocytochemistry of Tumor Vasculature
Tumor samples were snap frozen on dry ice and embedded in TissueTek on day
14. Thin cryosections (0tm)
were made using a Reichart cryostat and fixed in
methanol. The sections were then permeabilized in Tris buffer with Triton-X and Tween
and blocked with 1% goat serum. The sections were probed overnight with a rabbit
primary antibody against von Willebrand Factor (DakoCytomation, Carpinteria, CA)
diluted 1:2000 as an endothelial cell marker. The sections were washed and re-probed
with a goat secondary antibody coupled to Texas Red. The sections were coated with
slowfade (Molecular probes, Eugene, OR) and imaged using a Leica LSM5 10 confocal
microscope.
Images were captured randomly from three sectors at 51 0X5 10 pixels
resolution. Vessel density was quantified stereologically through a planimetric pointcount method using a 224-intersection point square reticulum.
17
2.3.c. Quantifying Apoptosis in Tumor Sections
Tumor cryosections were processed for TUNEL staining using Texas Red labeled
nucleotide per the manufacturer's instruction (Roche Diagnostics, Indianapolis, IN). The
sections were coated with slowfade (Molecular probes), and imaged using a Leica
LSM5 10 confocal microscope.
Images were captured randomly from three sectors at
510X510 pixels resolution. Apoptosis was quantified through stereological approaches
using a planimetric point-count method using a 224-intersection point square reticulum.
2.3.d. Analysis of Metastatic Nodes
Liver and lungs were harvested from the animals at sacrifice and fixed inl 0%
formaldehyde to check for metastasis.
The tissues were paraffin embedded, and thin
section slides were prepared for H&E staining. The slides were imaged with a Leica
LSM5 10 confocal microscope using FITC and Rhodamine filters, and merged images
were captured at a resolution of 51 0X5 10. Metastatic nodes were quantified by counting
the number of yellow foci in each section.
18
Chapter 3. Results
3.1. Synthesis/Characterization
of Nanocells
3.1.a. Synthesis/Characterization of Nanocores
Covalently conjugating chemotherapeutic agents to polymers is an established
method for obtaining efficient passive targeting to tumor. The use of small <100nm
polymeric nanoparticles as drug delivery vehicles enables both prolonged circulation in
vivo as well the preferential accumulation within tumor tissue via the enhanced
permeation and retention (EPR) effect(30, 35). The EPR effect refers to the extravasation
of macromolecules within tumor tissue in combination with inhibited clearance due to
diminished tumor lymphatic function.
Doxorubicin, one of the most commonly used anti-cancer agents, acts by
inhibiting nucleic acid synthesis thereby inducing apoptosis in rapidly dividing cells(21,
36). Doxorubicin was first conjugated to the terminal hydroxyl end group of PLGA via
an ester linkage (fig. 1a). This coupling has previously been shown to enable sustained
release profiles without any significant burst effect.(37) Conjugation efficiency was
determined by weighing a known amount of conjugate and dissolving it in
dimethylsulfoxide (DMSO). The extent of conjugation was determined by measuring the
absorbance of the solution at 480 nm (wavelength for doxorubicin absorbance). A
standard curve of absorbance of a series of doxorubicin concentrations in DMSO was
used to determine the doxorubicin amount in the conjugate (data not shown). The yield of
the conjugation reaction was -90%.
PLGA-DOX was formulated into nanocores by an emulsion-solvent evaporation
method with PVA as a stabilizer of the emulsion. SEM measurements demonstrated a
19
heterogeneous size population of nanocores ranging from 70-200nm in diameter (fig. 1b).
Nanocore size fractions were isolated by centrifugation at 8,000 rpm, 15,000 rpm, 20,000
and 22,000 rpm. Nanocores from the smallest size fractions were further extruded
through a 100nm membrane. Light scattering measurements of extruded nanocores
revealed an average diameter of 11 7nm (SE 9nm). Nanocores were found to aggregate
soon after extrusion, so all particles were used within 2 hours of preparation. The amount
of doxorubicin contained within the extruded fraction was determined by the ratio of
absorbance at 480nm of the extruded fraction to the whole, and average yields were
-30% of starting material.
3.1.b. Synthesis/Characterization of Lipid Vesicles
Combretastatin A4 is a stilbene isolated from the South African tree Combretum
caffrum that has been shown to prevent tubulin polymerization and induce vascular
shutdown in tumors with little cytotoxic effect on quiescent endothelial cells(38).
Combretastatin A4 has poor water solubility, and so its more hydrophilic prodrug
combretastatin A4 disodium phosphate is most often used in clinical and experimental
studies. The activities of both combretastatin A4 and its prodrug have been demonstrated
to be comparable(39), so we utilized the hydrophobicity of combretastatin A4 to
encapsulate the drug with high efficiency within the bilayer membrane of pegylated lipid
vesicles. Combretastatin A4 was dissolved into choloroform with a mixture of
PC:CHOL:DSPE-PEG (2:1:0.2 molar) lipids. After rehydration in distilled water, the
lipid/drug mixture was extruded through a 200nm membrane to create unilamellar
vesicles with the hydrophobic drug partitioned within the lipid bilayer. Average
20
liposome diameter was determined by particle sizing to be 188nm (SE 6nm).
Encapsulation efficiency of combretastatin A4 was determined by passage of loaded
liposomes through a PD-10 column containing Sephadex G-25 (Pharmacia Biotech) with
UV monitoring of drug elution at 290nm. A standard curve of absorbance of a series of
combretastatin A4 concentrations was used to determine the encapsulation efficiency
(data not shown), with >85% of the drug encapsulated within the lipid vesicles. Lipid
vesicles were used within 2 hours of preparation to minimize drug leakage.
3.1.c. Encapsulation of Nanocores within Lipid Vesicles
Doxorubicin nanocores were encapsulated within combretastatin A4 lipid vesicles
by the addition of concentrated nanocores to the lipid/drug rehydration buffer. Due to
comparisons of the lipid vesicles and encapsulated nanocores with the plasma membrane
and nucleus of living cells, we have coined the term 'nanocells' for these delivery
vehicles. Nanocells were visualized by TEM (fig. l.c) in order to determine the nanocore
encapsulation efficiency. On average, 55% of nanocores were encapsulated within lipid
vesicles, and 80% of lipid vesicles were found to contain nanocores.
21
(A)
'LGA 5050 DL 4A
1. pNC, pyridine, CH2CI 2
2. Doxorubicin, DMF, TEA
H3(
CH3
OH3
200 nm
o0o
(C)
Doxorubicin - PLGA conjugate
Liquid phase separation
& ultracentrifugation
sizing
(B)
-------- P.
Lipid membrane
coating. Combretastatin
partitioned into lipid phase.
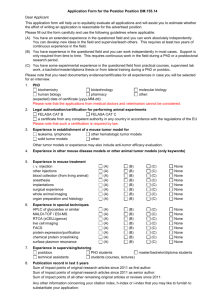
Figure 1. Synthesis of nanocells. A. Doxorubicin (DOX) is coupled to PLGA through
an ester linkage as described. B. DOX-PLGA is formulated into nanocores as described
and imaged via SEM. Small nanocore fractions are isolated by centrifugation and
passaged through a 100nm membrane. C. Nanocores are encapsulated within
combretastatin A4 containing lipid vesicles and sized by extrusion through a 200nm
membrane. Nanocells are imaged by TEM.
22
3.2. Evaluation of the Therapeutic Benefit of Nanocells
In order to determine the effect of nanocells on the cellular and vasculature
components of solid tumor, a novel co-culture assay system was developed. B 16F10
mouse melanoma cells were stably transfected with YFP and were co-cultured with
HUVECS on coverslips in a 12-well tissue culture format. After incubation with
nanocells, all cells were stained with propidium iodide to label the nuclei red. Confocal
imaging merging both FITC and rhodamine filters enabled the colorimetric distinction of
endothelial and tumor cells with tumor cells fluorescing green and endothelial cells
fluorescing red (fig 2a). Incubation separately with doxorubicin nanocores and
combretastatin A4 lipid vesicles demonstrated near complete specificity of the two agents
for tumor and vasculature respectively after 30 hours (figure 2a,b). Incubation with
nanocells demonstrated comparable disruption of tumor and vasculature after 30 hours,
however after 1.2hours only vasculature exhibited significant toxicity (fig 2b). This is
expected due to both the sequential release of combretastatin A4 prior to doxorubicin
nanocore exposure as well as the relatively fast action of combretastain A4 for disrupting
tumor vasculature. A recent study has demonstrated almost complete vascular shutdown
in MAC 15 orthotopic tumors in the presence of combretastatin A4 within only 4
hours(39).
23
a
Control JU n
A \ _......
LX
Jo1
a
I
·
1
·
omDretastatin
._._._
Control 12h
Irr
u n!
an
raw _. ::
uoxoruFDcin .3U
-
Nanocell 12h
Nanocell 30 h
A IN
(B)
cn30
O20
0
10
L
n
Control NC Control NC
12 h
ND Control NC Control NC
30 h
12 h
ND
30 h
Figure 2. In vitro efficacy of nanocells in a HUVEC/YFP-B 16F10 co-culture model. A.
The confocol micrographs depict YFP-B 16F 10 melanoma cells in yellow while the
vessel forming endothelial cells are red in color. The administration of doxorubicin
nanocores (ND) causes the selective destruction of tumor cells at 30 hours, while
incubation with combretastatin A4 lipid vesicles (LC) leads to the selective disruption of
the endothelial cells. B. Graphs show the percent area covered by endothelial cells
(light) and tumor cells (dark). Treatment with nanocells (NC) results in a rapid (< 12hrs)
disruption of the endothelial network without affecting the density of tumor cells. Both
tumor cells and endothelial cells show significant death by 30 hours. ***P<0.001 vs
controls, ANOVA followed by Dunnets Post Hoc test.
24
Nanocells were next evaluated for their ability to disrupt tumor growth in vivo.
Twenty-four C57/BL6 mice were subcutaneously injected with 3*105 YFP-Bl6F10 cells
into the right flank on day 1. On day nine, 15 mice were selected for tumors nearest to an
average volume of 150mm 3 and randomized into five treatment groups. Treatments were
administered intravenously every other day in 100[tL sterile H2 0 and consisted of blank
control, nanocores containing mg/kg doxorubicin, lipid vesicles containing 50mg/kg or
25mg/kg combretastatin A4, doxorubicin nanocores simultaneously with combretastatin
A4 lipid vesicles, and nanocells. On day 14, all mice were sacrificed and tumor volume
was measured (fig 3a.). While combretastatin A4 lipid vesicles and doxorubicin
nanocores both demonstrated significantly reduced tumor size from control when
delivered separately (50% and 58% respectively), the simultaneous administration of
these two vehicles only showed a slight additive effect (66% from control). Treatment
with nanocells, however, demonstrated a highly significant benefit over the additive
treatment of the two agents with an 88% reduction in tumor size as compared to control.
Further, measures of white blood cell (WBC) counts demonstrated that nanocells
provided a decrease in systemic toxicity over all other treatment formulations. WBC
counts after nanocell treatment were not significantly different from control, however all
other treatment groups showed a significant decrease (P < 0.01, ANOVA followed by
Dunnets Post Hoc). Inhibition of systemic toxicity may be explained by a preferential
trapping of doxorubicin within the solid tumor after treatment with nanocells.
25
(A)
Control
LC
ND
LC+ND
NC
I
7500
-
Control
LC
-
ND
LC + ND
=
E
= 5000
=ontrol)
NC
.
o
E
1-
LC)
ND)
2500
LC + ND)
NC)
0
9
10
11
12
13
14
Days
(B)
n
E
E
4
10
15
_14
3
0o
110
0
M1 0
CZ
Control ND
LC ND NC
+ LC
5
Control ND LC ND NC
+LC
Figure 3. Increased in vivo efficacy of nanocells. A. Injections every other day
beginning nine days after subcutaneous tumor implantation with either doxorubicin
nanocores (ND), combretastatin A4 lipid vesicles (LC), doxorubicin nanocores +
combretastatin A4 lipid vesicles (LC + ND), or nanocells (NC) resulted in an inhibition
of tumor size from control of 50%, 58%, 66% and 88% respectively 14 days post tumor
implantation. The addition of nanocells provided a significantly greater inhibition of
tumor growth compared to the additive inhibition of co-injecting LC and ND (P < 0.001,
ANOVA). B. Differential white blood cell counts and hemoglobin levels at day 14 post
tumor implantation. WBC counts did not differ significantly from control after nanocell
treatment suggesting a preferential trapping of doxorubicin within the tumor.
26
The effect of nanocells on the vasculature and cellular components of solid tumor
in vivo was determined by immunohistochemistry
after animal sacrifice (figure 4a, 5a).
Von Willebrand Factor antibody labeling indicated that doxorubicin nanocores did not
significantly disrupt the tumor vasculature as compared to control. The administration of
combretastatin A4 lipid vesicles, combretastatin A4 lipid vesicles and doxorubicin
nanocores, and nanocells all exhibited similar vascular toxicity with 60% less new vessel
formation from control (fig 4b). TUNEL staining was used to quanitify tumor cell
apoptosis in histological samples taken from excised tumors. Combretastatin A4 lipid
vesicles did not induce significant tumor cell apoptosis as compared to control. While
the administration of doxorubicin nanocores and combretastatin A4 lipid vesicles
simultaneously with doxorubicin nanocores exhibited a somewhat greater degree of
tumor apoptosis than control, treatment with nanocells showed a highly synergistic effect
related to increased tumor cell apoptosis (fig 5b). This effect may also be explained by
the preferential trapping of doxorubicin within the tumor in nanocell treatment groups.
Histological slides were taken from the lungs and liver to check for the presence of
metastatic YFP-B 16F10 cells. Metastasis to both organs was over 80% less in nanocell
formulations when compared to control, and significantly less than all other treatment
formulations (fig 6a,b.).
27
Control
Doxorubicin (ND)
Combretastatin (LC)
(A)
LC + ND
(B)
I`C$
40
Nanocell (NC)
-
30 -*
?-
20 -
C.)
Qn
**
,
rn
lU
.,
**
-1r
**
10 -
cn
au
A
II
m
-
Control LC
ND ND+LC NC
Figure 4. Effect of nanocells on tumor vasculature at day 14 post implantation.
Confocal imaging of vasculature (A) and stereological vessel density measurements (B)
indicate that treatment with doxorubicin nanocores (ND) has no significant effect on the
vasculature as compared to control. Combretastatin A4 lipid vesicles (LC), ND + LC and
nanocells (NC) all had a similar reduction in vessel density of-60%.
vs Control. ANOVA followed by Dunnets Post Hoc Test.
28
*P<0.05, **P<0.01
A \
tA)
IL
Control
41.
41+
IomnureUastati
I' .
lr~
{l
IAl)
40 -e
_l f lrT-
(iNJ)
I
I
I
c 40
t
A
Nanocell (NC)
LC + ND
(B)
oxorulcin
-
I
-?n-
*
420E.d
l0.,
_
i
Veh
ND
LC
ND
NC
+LC
Figure 5. Effect of nanocells on tumor cell apoptosis at day 14 post implantation. (A)
Cells undergoing apoptosis are stained red as they are TUNEL positive. (B)
Combretastatin A4 lipid vesicles (LC) did not induce significant apopotosis in tumor cells
as compared to control. Doxorubicin nanocores (ND) and ND + LC induced comparable
levels of tumor apoptosis while nanocells (LN) induced a significantly greater level of
apoptosis than any of the other formulations.
***P<0.01, *P<0.05 vs control. ANOVA
followed by Dunnets Post Hoc test
29
liver
__
-- ·--
,- 5.0Cn
_
0
o
-r
7d
4
"
2.5-
-r
._
.a...a
· -.
i-.-
nI
Control ND N
.
-
I-
- - -- - - -
-
)
_
-
r
I
LC NC
+LC
%~~~I
I
I I
,_
1i .I
Control ND LC ND NC
+LC
Figure 6. The effect of nanocells on metastasis of tumor nodules to lungs and liver.
Organ tissues were paraffin embedded, and thin section slides were prepared for H&E
staining. The slides were imaged with a Leica LSM5 10 confocal microscope using FITC
and Rhodamine filters, and merged images were captured at a resolution of 51 0X5 10.
Metastatic nodes were quantified by counting the number of yellow foci in each section.
The administration of nanocells (NC) prevented metastasis to both organs by over 80%
from control and over 50% from all other treatment formulations. (P<0.01, ANOVA
followed by Dunnets Post Hoc Test). ND: Doxorubicin Nanocores; LC: Combretastatin
A4 Lipid Vesicles.
30
Chapter 4. Discussion
We demonstrate here a novel nanodelivery system for achieving the delivery of
two chemotherapeutic agents with different mechanisms of action and distinct release
profiles. The delivery system consists of a 200nm diameter spherical lipid bilayer
membrane surrounding a 100nm diameter polymeric nanocore. The parallels of such a
system to a nucleus encapsulated within a plasma membrane have led us to term these
vehicles 'nanocells.' Combretastatin A4, a tubulin-destabilizing and established antivascular agent, was encapsulated within the hydrophobic interior of the lipid membrane
for release upon membrane fusion, membrane bursting, or cellular uptake of the
nanocell(40). Doxorubicin, an established anti-cancer agent, was covalently linked to a
PLGA polymeric nanocore by means of an ester linkage. The PLGA-DOX ester linkage
has previously been demonstrated to enable sustained drug release, thus facilitating the
prolonged release of doxorubicin after exposure of the nanocore(37).
We demonstrated the sequential action of combretastatin A4 and doxorubicin
after delivery via nanocells by means of a novel in vitro co-culture assay system. The
specificity of combretastatin A4 for vasculature and doxorubicin for tumor was
confirmed via this system. Nanocell treatment resulted in significant toxicity to
vasculature within 12 hours, while toxicity to tumor cells was shown to take place over
days. Intraveneous administration of nanocells in a subcutaneously implanted murine
melanoma model confirmed the in vivo specificity of treatments for the vasculature and
cellular components of tumor. While treatment with doxorubicin nanocores enabled
significant tumor cell apoptosis in vivo, there was no disruption to tumor vasculature as
compared to control. Lipid vesicles containing combretastatin A4 induced little apoptosis
31
in tumor cells, however they demonstrated significant disruption to tumor vasculature.
The administration of these two agents in combination demonstrated only a small
additive effect on tumor growth inhibition compared to the two agents delivered
individually. Treatment with nanocells, however, resulted in significantly reduced tumor
growth, reduced systemic toxicity, increased tumor cell apoptosis, and less liver and lung
metastasis than all other treatment formulations used in this study. The increase in
efficacy of this formulation over the additive treatment of doxorubicin nanocores and
combretastatin A4 lipid vesicles demonstrates that there is a highly synergistic effect on
tumor inhibition with nanocell treatment.
We propose that this effect can be explained by the ability of nanocells to
circumvent certain types of tumor micro-environment mediated drug resistance. Until
recently, chemotherapeutic drug resistance has been almost exclusively defined in terms
of cellular mechanisms by which genetically unstable tumor cells are selected for clones
resistant to treatment. Recent findings have shown that the tumor microenvironment may
also contribute significantly to drug resistance through non-cellular mechanisms(41).
One such non-cellular mechanism of drug resistance with considerable impact on the
field of anti-angiogenic cancer therapy is the formation of isolated regions of hypoxia
resulting from the heterogeneous vascularization of solid tumor(42). Hypoxia is a
double-edged sword, as not only are hypoxic cells less accessible to blood-borne
chemotherapeutic agents, these cells have also been shown to release factors responsible
for the promotion of tumor growth, angiogenesis, and metastasis(23, 43).
Further, anti-angiogenic treatments may actually contribute to the promotion of
tumor hypoxia through their effect on the tumor vasculature(24). Tumor cells that are
32
less vessel-dependent may be selected for over time with successful anti-angiogenic
treatment(4 1), and subsequent anti-cancer therapy will be faced with hypoxia-induced
drug resistance as well as a decreased tumor volume of distribution after intravenous
administration(25). Current combination therapy regimens commonly consist of frequent
dosing of anti-angiogenics interspersed with single large doses of anti-cancer agents(2 1,
22, 44). We theorized that a delivery system enabling the loading of an anti-cancer drug
within vascularized regions of the tumor prior to blood vessel collapse would not only
allow for greater access of drug within the tumor but also prevent the formation of new
regions of hypoxia after anti-angiogenic treatment. Many of the therapeutic benefits of
nanocells presented here support this hypothesis. Nanocell treatment promotes greater
tumor apoptosis and significantly reduced tumor size than the addition of antiangiogenics and anti-cancer agents separately and in combination, suggesting the
preferential uptake of doxorubicin within tumor after nanocell treatment. In addition,
there are significantly fewer instances of liver and lung metastases after treatment with
nanocells, and the degree of metastasis has previously been shown to correlate with the
degree of hypoxia in solid tumor(43). A recent study has demonstrated that upregulation
of hypoxia activates transcription of the met protooncogene, resulting in higher levels of
Met tyrosine kinase, a high affinity receptor for hepatocyte growth factor (HGF). As a
result HGF signaling is amplified, and tumor invasion and metastasis is increased(23).
Vascular shutdown at the site of doxorubicin delivery may provide the added therapeutic
benefit of trapping the drug within the tumor and thereby decreasing systemic toxicity as
seen with WBC profiling.
33
The sequential effect of anti-angiogenics and anti-cancer agents achieved using
nanocells could also be accomplished in several other ways. A delivery regimen could
consist of the simultaneous delivery of a 'fast-homing' anti-cancer agent with a 'slowhoming' anti-vascular agent, or a 'fast-acting' anti-cancer agent with a 'slow-acting' antivascular agent. Drug administration could also be staggered to enable a similar effect.
The delivery of multiple agents in this fashion may provide some benefit for
circumventing hypoxia-mediated drug resistance, however we suggest that it is the spatial
as well as the temporal component of nanocell drug delivery that increases the efficacy of
the agents to the degree demonstrated. Using a single delivery vehicle enables the
loading of cytotoxic agents at the precise site of blood vessel collapse, thus enabling a
preferential trapping of drug within the tumor at regions most likely to become hypoxic.
The delivery of multiple agents separately also offers less control over the
pharmacokinetics of drug-drug interactions within the tumor, as well as difficulties with
patient compliance and comfort common to the administration of multiple agents.
Encapsulating drugs within nanocells provides the added benefits of sustained release
from polymeric drug delivery vehicles, with further control over the kinetics of drug
release available through alterations to the polymer chain length and the method of drugpolymer conjugation(34). In addition, an external pegylated lipid vesicle compartment
enables both increased circulation times and the potential for tumor-specific ligandreceptor binding and uptake(40).
The enhanced anti-tumor effect demonstrated with the use of nanocells over
traditional combination therapy warrants further study into its mechanism of action as
well as optimization of multi-drug release from this system in specific tumor models. We
34
are currently investigating the regulation of hypoxia-induced factors in response to
nanocell treatment as well as the effect of nanocells on drug distribution in vivo. We are
also examining the use of receptor-targeted nanocells as a means of actively targeting
tumors for an enhanced therapeutic effect. In addition, we are exploring how the
increased therapeutic efficacy of nanocells over traditional combination tumor therapy
may translate to the development of new treatments for other angiogenesis-mediated
pathologies including diabetes retinopathy and arthritis.
35
References
1.
Rosen, L., Antiangiogenic strategies and agents in clinical trials, Oncologist, 5
Suppl 1, 20 (2000).
2.
Folkman, J., Fundamental concepts of the angiogenic process, Curr Mol Med, 3,
3.
643 (2003).
Gimbrone, M. A., Jr., Leapman, S. B., Cotran, R. S., and Folkman, J., Tumor
dormancy in vivo by prevention of neovascularization, J Exp Med, 136, 261
(1972).
4.
Folkman, J., What is the evidence that tumors are angiogenesis dependent?, JNatl
Cancer Inst, 82, 4 (1990).
5.
Folkman, J., Seminars in Medicine of the Beth Israel Hospital, Boston. Clinical
applications of research on angiogenesis, N Engl JMed, 333, 1757 (1995).
6.
Hanahan, D., and Folkman, J., Patterns and emerging mechanisms of the
angiogenic switch during tumorigenesis, Cell, 86, 353 (1996).
7.
Hori, A., Sasada, R., Matsutani, E., Naito, K., Sakura, Y., Fujita, T., and Kozai,
Y., Suppression of solid tumor growth by immunoneutralizing monoclonal
antibody against human basic fibroblast growth factor, Cancer Res, 51, 6180
8.
(1991).
Liotta, L. A., and Stetler-Stevenson, W. G., Tumor invasion and metastasis: an
imbalance of positive and negative regulation, Cancer Res, 51, 5054s (1991).
9.
10.
Tonini, T., Rossi, F., and Claudio, P. P., Molecular basis of angiogenesis and
cancer, Oncogene, 22, 6549 (2003).
Bhushan, M., Young, H. S., Brenchley, P. E., and Griffiths, C. E., Recent
advances in cutaneous angiogenesis, Br J Dermatol, 147, 418 (2002).
11.
12.
13.
Seymour, L. W., Passive tumor targeting of soluble macromolecules and drug
conjugates, Crit Rev Ther Drug Carrier Syst, 9, 135 (1992).
Baban, D. F., and Seymour, L. W., Control of tumour vascular permeability, Adv
Drug Deliv Rev, 34, 109 (1998).
Hobbs, S. K., Monsky, W. L., Yuan, F., Roberts, W. G., Griffith, L., Torchilin, V.
P., and .Jain, R. K., Regulation of transport pathways in tumor vessels: role of
tumor type and microenvironment, Proc Natl Acad Sci US A, 95, 4607 (1998).
14.
15.
16.
17.
Yuan, F., Dellian, M., Fukumura, D., Leunig, M., Berk, D. A., Torchilin, V. P.,
and Jain, R. K., Vascular permeability in a human tumor xenograft: molecular
size dependence and cutoff size, Cancer Res, 55, 3752 (1995).
Folkman, J., Winsey, S., Cole, P., and Hodes, R., Isolated perfusion of thymus,
Exp Cell Res, 53, 205 (1968).
Ribatti, D., Vacca, A., and Presta, M., The discovery of angiogenic factors: a
historical review, Gen Pharmacol, 35, 227 (2000).
Verheul, H., Voest, E., and Schlingemann, R., Are tumours angiogenesis-
dependent?, J Pathol, 202, 5 (2004).
18.
Bergers. G., Javaherian, K., Lo, K. M., Folkman, J., and Hanahan, D., Effects of
angiogenesis inhibitors on multistage carcinogenesis in mice, Science, 284, 808
(1999).
36
19.
Rak, J., Yu, J. L., Kerbel, R. S., and Coomber, B. L., What do oncogenic
mutations have to do with angiogenesis/vascular dependence of tumors?, Cancer
20.
Res, 62, 1931 (2002).
Kerbel, R. S., Clinical trials of antiangiogenic drugs: opportunities, problems, and
assessment of initial results, J Clin Oncol, 19, 45S (2001).
21.
Pan, Q., Bao, L. W., Kleer, C. G., Brewer, G. J., and Merajver, S. D.,
Antiangiogenic tetrathiomolybdate enhances the efficacy of doxorubicin against
breast carcinoma, Mol Cancer Ther, 2, 617 (2003).
22.
Grosios, K., Loadman, P. M., Swaine, D. J., Pettit, G. R., and Bibby, M. C.,
Combination chemotherapy with combretastatin A-4 phosphate and 5-fluorouracil
in an experimental murine colon adenocarcinoma, Anticancer Res, 20, 229
23.
(2000).
Pennacchietti, S., Michieli, P., Galluzzo, M., Mazzone, M., Giordano, S., and
Comoglio, P. M., Hypoxia promotes invasive growth by transcriptional activation
of the met protooncogene, Cancer Cell, 3, 347 (2003).
24.
Steeg, P'. S., Angiogenesis inhibitors: motivators of metastasis?, Nat Med, 9, 822
(2003).
25.
Koch, S., Mayer, F., Honecker, F., Schittenhelm, M., and Bokemeyer, C.,
Efficacy of cytotoxic agents used in the treatment of testicular germ cell tumours
under normoxic and hypoxic conditions in vitro, Br J Cancer, 89, 2133 (2003).
26.
Kinoshita, M., Johnson, D. L., Shatney, C. H., Lee, Y. L., and Mochizuki, H.,
Cancer cells surviving hypoxia obtain hypoxia resistance and maintain antiapoptotic potential under reoxygenation, Int J Cancer, 91, 322 (2001).
27.
Comerford, K. M., Wallace, T. J., Karhausen, J., Louis, N. A., Montalto, M. C.,
28.
multidrug resistance (MDR1) gene, Cancer Res, 62, 3387 (2002).
Martin, C. R., and Kohli, P., The emerging field of nanotube biotechnology, Nat
and Colgan, S. P., Hypoxia-inducible factor-i-dependent regulation of the
Rev Drug Discov, 2, 29 (2003).
29.
30.
31.
Martin, C. R., Nanomaterials in analytical chemistry, Anal. Chem., 70, 322A
(1998).
Brigger, I., Dubernet, C., and Couvreur, P., Nanoparticles in cancer therapy and
diagnosis, Adv Drug Deliv Rev, 54, 631 (2002).
Dubertret, B., Skourides, P., Norris, D. J., Noireaux, V., Brivanlou, A. H., and
Libchaber, A., In vivo imaging of quantum dots encapsulated in phospholipid
micelles, Science, 298, 1759 (2002).
32.
Savic, R., Luo, L., Eisenberg, A., and Maysinger, D., Micellar nanocontainers
distribute to defined cytoplasmic organelles, Science, 300, 615 (2003).
33.
McPhail, D., Tetley, L., Dufes, C., and Uchegbu, I. F., Liposomes encapsulating
polymeric chitosan based vesicles--a vesicle in vesicle system for drug delivery,
Int JPharm, 200, 73 (2000).
34.
Yoo, H. S., Oh, J. E., Lee, K. H., and Park, T. G., Biodegradable nanoparticles
containing doxorubicin-PLGA conjugate for sustained release, Pharm Res, 16,
1114(1999).
135.
Maeda, H., The enhanced permeability and retention (EPR) effect in tumor
vasculature: the key role of tumor-selective macromolecular drug targeting, Adv
Enzyme Regul, 41, 189 (2001).
37
36.
Colin de Verdiere, A., Dubernet, C., Nemati, F., Poupon, M. F., Puisieux, F., and
Couvreur, P., Uptake of doxorubicin from loaded nanoparticles in multidrugresistant leukemic murine cells, Cancer Chemother Pharmacol, 33, 504 (1994).
37.
Yoo, H. S., Lee, K. H., Oh, J. E., and Park, T. G., In vitro and in vivo anti-tumor
activities of nanoparticles based on doxorubicin-PLGA conjugates, J Control
Release, 68, 419 (2000).
38.
Dark, (J. G., Hill, S. A., Prise, V. E., Tozer, G. M., Pettit, G. R., and Chaplin, D.
J., Combretastatin A-4, an agent that displays potent and selective toxicity toward
tumor vasculature, Cancer Res, 57, 1829 (1997).
39.
40.
41.
42.
Grosios, K., Holwell, S. E., McGown, A. T., Pettit, G. R., and Bibby, M. C., In
vivo and in vitro evaluation of combretastatin A-4 and its sodium phosphate
prodrug, Br J Cancer, 81, 1318 (1999).
Ulrich, A. S., Biophysical aspects of using liposomes as delivery vehicles, Biosci
Rep, 22, 129 (2002).
Yu, J. L., Coomber, B. L., and Kerbel, R. S., A paradigm for therapy-induced
microenvironmental changes in solid tumors leading to drug resistance,
Differentiation, 70, 599 (2002).
Yu, J. L., Rak, J. W., Coomber, B. L., Hicklin, D. J., and Kerbel, R. S., Effect of
p53 status on tumor response to antiangiogenic therapy, Science, 295, 1526
43.
(2002).
Wouters, B. G., Koritzinsky, M., Chiu, R. K., Theys, J., Buijsen, J., and Lambin,
P., Modulation of cell death in the tumor microenvironment, Semin Radiat Oncol,
44.
13, 31 (2003).
te Velde, E. A., Vogten, J. M., Gebbink, M. F., van Gorp, J. M., Voest, E. E., and
Borel Rinkes, I. H., Enhanced antitumour efficacy by combining conventional
chemotherapy with angiostatin or endostatin in a liver metastasis model, Br J
Surg, 89, 1302 (2002).
38