9080 02245 1980 3 MIT LIBRARIES
advertisement

MIT LIBRARIES
3 9080 02245 1980
DUPL
28
14
M
DEWEY
1
The Impact of novel Treatments on A6 Burden
Disease: Insights from a Mathematical
David
L. Craft,
in
Model
Lawrence M. Wein, Dennis
Sloan Working Paper
J.
Number 4 56
January 31,2001
1
Alzheimer's
Selkoe
The Impact
in
of Novel Treatments on A/5
Burden
Alzheimer's Disease: Insights from a Mathematical Model
David
L.
Ciaft\ Lawrence M. Wein"^, Dennis
J.
Selkoe^*
^Operations Research Center, MIT. Cambridge, K4A 02139
'^
3
Sloan School of Management, MIT, Cambridge,
MA
02139
Center for Neurologic Diseases, Harvard Medical School, Brigham and Women's Hospital,
Boston,
'Person to
whom
MA
02115
correspondence should be addressed: email:
si'lkoe
fend. bwh. harvard. eihi
Abstract
Motivated by recent therapeutic
initiatives for Alzheimer's disease,
mathematical model of the accumulation of amyloid /3-protein
we developed a
(A/i) in the brain.
The
model incorporates the production and clearance of kl5 monomers, and the elongation
and fragmentation of polymers by monomer aggregation and
Our
break-off, respectively.
analysis suggests that A/3 dynamics are dictated by a single tmitless measure re-
ferred to as the polymerization ratio,
which
is
the product of the production and elon-
gation rates divided by the product of the clearance and fragmentation rates. Cerebral
k(i
burden attains a
sustained growth
if
finite
steady-state level
this ratio
is
if
this ratio
greater than one.
The
is
less
than one, and undergoes
highly nonlinear relationship be-
tween the polymerization ratio and the steady-state A/3 burden implies that a modest
reduction in the polymerization ratio
(e.g.,
a
a 7-secretase inhibitor) achieves a significant
Our model
40%
reduction
(e.g., 18-fold)
in
the production rate by
decrease in the A/3 burden.
also predicts that after initiation or discontinuation of treatment,
take months to reach a
new steady-state
suggest that the research
A/3 burden.
may
Taken together, our findings
comnumity should focus on developing agents that provide
a modest reduction of the polymerization ratio while avoiding long-term
nally,
it
toxicity.
Fi-
our model can be used to indirectly estimate several crucial parameters that
are difficult to measure directly: the production rate, the fragmentation rate
strength
(i.e.,
percentage inhibition or enhancement) of treatment.
and the
Introduction
The
cerebral build-up of amyloid /^-protein (A/3)
and
its
aggregation into oligomers and
polymers are key components of the pathogenesis of Alzheimer's disease (AD)
studies suggest that A/3 accumulation plays an important role in
^'^,
AD
'.
Recent
neurodegeneration
and a variety of A(5 treatment strategies are being aggressively pursued, including the
enhancement of A/? clearance via immunization with A/3
production by inhibiting 7-secretase, which
precursor protein
(APP)
is
^'^^
and the reduction of A/3
one of the two enzymes that cuts the amyloid
to release the A/3 fragment ^•^.
The
kinetics of A/3 production,
aggregation (polymerization), disaggregation and clearance, and the effect of these novel
treatments on the time-dependent variation of A/3 levels are not well understood. Although
^"^^ or plaque
there exist several mathematical models that focus on either fibrillogenesis
formation
^''^'^^
these studies neither consider the impact of treatment nor allow for a
contiiniously renewable source of A/3 from
APP
molecules. Here
we formulate and analyze a
simple mathematical model that tracks the dynamics of A/3 production, polymer elongation,
fragmentation and clearance during the course of treatment. Simple formulas and numerical
results are presented that elucidate the
impact of treatment on A/3 burden.
Mathematical model
In
AD
brain tissue, the level of extracellular (and perhaps intracellular) k[5 (particularly
A/342, the
tion.
42 amino-acid form of A/3) increases over time, which gives
Some
of A/342,
rise to
polymeriza-
of these polymers cluster into light microscopically-visible particles consisting
which can accumulate to create diffuse (amorphous)
neuropathological lesion of
AD.
Further,
platiues, the
some polymers containing
A/^42
apparent
and/or
initial
A/340 t'^n
eventually fold into long hlamentous assemblies called amyloid hbrils, and clumped masses
of these are referred to as amyloid (senile) plaques.
Our mathematical model
idealizes this
process in several iinjxjrtaiit ways. First, we only consider extracellular A/?, which
be
in
and
a dynamic equilibrium with intracellular A/i.
A/?42, or
do not
also
between soluble and insoluble AS, because there
dynamic changes
the current literature about the precise
and
preclinical
We
clinical
is
distinfi,uish
the
we
restrict
is
we discuss how
incorporate
in the
to understand
number and
size
fibrillization or
plaque formation
model might be interpreted
this
in
However, later
in vivo.
in
terms of - and generalized to
plaque formation.
Our model
an
is
infinite
system of nonlinear
differential equations that tracks the
temporal evolution of the concentration of extracellular A/3 i-mers, for
variant of the
time
in
our attention to A/3 polymerization, and do not attempt to capture
downstream processes of
the paper
between A/i4o
in these species over
the impact of treatment on total cerebral A/3 burden (as opposed to the
of plaques),
likely to
information
insufficient
phases of AD. Finally, because our primary goal
is
Smoluchowski equation
-'^^~\
which has been used
2
=
for nearly a
1,2,....
It is
a
century to study
aggregation processes such as polymerization, galaxy formation, crystallization, and cloud
2-2-23
formation
vVfhiie this nrodel typically considers
novelty of our model
is
to simultaneously incorporate fragmentation, a source (A/i
production) and a sink (A/i
For
t
=
1. 2,
.
denotes monomer,
of change of
r,(i),
,
.
.
t
=
aggregation in closed systems, the
we
monomer
let c,(f)
loss).
denote the concentration of A/? z-mer at time
2 denotes dimer, etc.
denoted by
Cj(t),
monomer
The
t\
differential equations dictate the
i.e.,
i
=
1
time rate
and are given by
oo
ci(f)
monomers
=
p
/^c,(0
+
s-l::^
production
all
'
fragmentations
+ ^c,(0)-
-eci(t)(2c,(f)
——
1=2
^
v
all
elongations
'
lc,{t)
loss (e.g.,
by
degradation)
;i:
+
ec,(OQ(0
of
and
for
c,(0
i
>
=
monomers
+
er,(f)r,_i(0_
of
elongation
(? - l)-mers
The model captures
constant rate
-
/c,+i(0.
ec,{t)r,{t
fragmentation
(i + l)-mers
(3)
1.
p.
fragmentation
of ^-mers
elongation
of /-mers
of
four processes - production, elongation, fragmentation, and loss
monomers
In equation (1), A/3
and are
lost at
time
t
cell
mnemonic parameters
are produced via cleavage of the
at rate lci{t).
time units on average before being cleared by
That
is,
A/3
monomers
are
APP
live for
/"^
internalization (e.g., microglial ingestion),
degradation by proteases or removal from the brain via the circulation.
Parameter
(2)
fragmentation
of dimers
of dimers
clearance) - and for ease of reference the corresponding
displayed in Table
at a
elongation
C2{t)
3,
t-mers
(i.e.,
fragmentation
of 3-mers
elongation
diiners
/
ec,{t)c2{t)
f<-3{t)
factor 2 in equation (1) arises because the elongation to a
The
and the term //2
in
equation
(2)
stems from the
dimer requires two monomers,
fact that a
dimer can only fragment
one location, while larger «-mers possess two potential fragmentation
cancel each other out in the fco term in ecjuation
alternate modeling approach
is
2
and 1/2
(1).
to allow direct clearance of
monomers
off of i-mers
represent microglial ingestion of polymers), rather than requiring a two-step proce-
(e.g., to
dure of
Fragmentation
//2 and creates two monomers, and hence the factors
of dimers occurs at rate
An
sites.
in
monomer fragmentation
sult in the
omission of the
"all
followed by
fragmentations" term
of / as an ingestion rate, but
monomer and dimer
a post-treatment steady-state.
in
clearance. This alternative would re-
equation
(1)
and the re-interpretation
would not change the qualitative nature of our
would mainly change the precise conditions
ues of steady-state
monomer
for a steady-state solution
and the
results:
it
relative val-
concentrations, and slightly hasten the approach to
Finally, while AjS treatment
parameters are not explicitly
incorporated into equations (l)-(3), treatment can be included in the model, as explained
later.
Results
Steady-state solution
Our
analysis begins by seeking a steady-state
(3).
To describe our
which
is
results in a concise
Ci
equilibrium) solution,
Cj,
(i.e.,
to equations (1)-
manner, we define the polmerization ratio
a unitless quantity that incorporates the four model parameters.
side of equations (l)-(3)
for
(i.e.,
Setting the
left
the rates of change of i-mer concentration) to zero and solving
reveals that there are two regimes: a steady-state (or subcritical) regime
6
where
/
<
1
.
and a supercritical regime where
>
r
In the former case, the A/? levels settle into a
1.
steady-state where
d =
and
y,
c,
=
2^r'-'
for
Hence, ?— mer concentrations decay geometrically for
lent
than dimers
<
r
if
and
0.5,
less
i
>
/
2,
prevalent than dimers
>
2.
(5)
and monomers are more prevaif
r
>
In contrast,
0.5.
r
if
>
1
then the A/j burden grows indefinitely. Because the A/? burden appears to remain relatively
stable over time in
symptomatic
AD
patients
^-^-'^s,
we focus primarily on the steady-state
regime, and defer until later a discussion of the supercritical regime.
Equation
number
total
which
is
implies that the steady-state value for the total A/3 concentration
(5)
of Af3 molecules in the system, whether they exist as
denoted by
r
= ^j^i
ic^
and referred to as the
Ap
burden,
monomers
is
(i.e.,
or ?'-mers).
given by
Notice that the total Aft burden c approaches infinity as the polymerization ratio r appoaches
1.
We now
use equations (5)-(6) to estimate the values of the model parameters, and these
parameter values,
in turn,
allow us to calibrate the key relationship (6)
(i.e.,
A/i burden) to
the clinical setting.
Parameter estimation
The
value of the
which
is
brains of
A;:^
monomer
/
in
Table
1
corresponds to a
close to the crude experimental value of 38
APP
transgenic mice
primaril\- via A.J
monomer
a synthetic fibril analysis
and
loss rate
protofibrils
^.
Protofibrils
addition, and
^'*,
which
is
half-life of 41.6
minutes reported by one group
~', fibrils
''
" and plaques
we use an elongation
^^
7
in the
appear to grow
rate e in Table
1
taken from
within a factor of two of other estimates for
^'
minutes,
fibrils
^^
The fragmentation
empirically. Fortunately,
man AD
/ and the monomer production rate p are
rate
we can use equations
brains, to estimate these
1.4% of A/?
in
the
human
brain
is
difficult to
estimate
(5)-{6), together witli A/i estimates
from hu-
two quantities as
soluble,
and found that
primarily of monomers, dimers and trimers.
A
A
follows.
this soluble
related study
human
erage (of A/i4o and A/?42) soluble fraction of A/i in
study
rec(Mit
the fraction of A/? that consists of monomers, ci/c, to 0.013.
soluble dimers and trimers in
and setting
AD
brain.
is
only 0.05%
We
By
By equations
this expression equal to 0.013 yields the
consists
taking the
and assuming
'^'')
monomers, we equate
recognize that this analysis
in the brain if there are large
equate the A/i burden on the right side of equation
(A/3.}o
compartment
measured the weighted av-
'-^^
that the soluble dimers and trimers are exactly offset by any insoluble
underestimate the percentage of soluble A/3
estimated that
brains to be 1.2%.
average of these two estimates (we ignore a third estimate that
will
*
(5)-(6), Ci/c
=
-
(2/(1
=
polymerization ratio r
amounts
r)''
- 1)^\
We
0.84.
of
also
the average of the total A/3 levels
(6) to
plus A/342) found in five different cortical regions of wet brain tissue of patients with a
clinical
of 2819
dementia rating (CDR) score of
pmol/g
is
similar in magnitude to those in
wet cortical tissue (which
estimates for
pmol/g
/
and
5.0 (severe dementia) in
is
about 87% water)
r into the right side of
is
=
equal to that of water.
equation
(6)
times smaller than the value of the loss rate
^' ^
of
-
/,
that directly ingests
represented as a fragmentation enhancer.
1.
estimate
(this
and equating
1.
Substituting our
this expression to
=
Finally, because r
0.84, together with our earlier estimates of
yield the value for the fragmentation rate / in Table
model an A/3 vaccine
1
by assuming that the density of
'^),
yields the value of the production rate p in Table
the polymerization ratio estimate r
Table
Note that
this value of
/
pe/{fl),
e,
is
2819
I
and
p,
about 70
which suggests that within the context of our
monomers
off of
oligomers can be accurately
A/3
With
burden
we now return
these parameter values in hand,
A/3 burden
c.
to equation (6) for the steady-state total
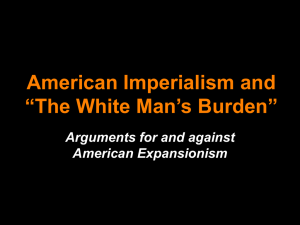
This nonlinear relationship between the polymerization ratio and the steady-
state A/? burden
is
shown
in
Figure
1,
and implies that a given treatment
will generally
achieve a greater (relative and absolute) reduction in steady-state A/? burden for patients
To position
with higher pretreatment A/3 burdens.
context,
^.
we convert the A/3 burden
Figure
in
1
this relationship within the clinical
CDR scale
to the
using the data in Table
This conversion allows us to explore the potential clinical impact
(i.e.,
neurodegeneration associated with A/9 can be reversed) of a reduction
ratio via treatment.
is
APP
fall in
transgenic mice
at least partially reversible in mice.
the right ordinates of Figures
not
of
assuming that the
in the
polymerization
Recent studies reveal that A/? peptide vaccination reduces not only
A/3 burden but also cognitive impairment in
neurodegeneration
1
1,
2
and
3
synchrony with A/3 burden
in
can be ignored
humans; the
if
We
^~-
", implying that the
CDR
note that the
the reader believes that
latter ordinate
is still
scales on
CDR
will
valid.
7-secretase inhibitors
Because of their potentially adverse
effect
on Notch signalling 34-3(^ 7-secretase inhibitors
might best be used to reduce only modestly the A/^
by 20-6U%.
To
assess the effect of such treatment,
assuming that a symptomatic patient
is
in
monomer production
we numerically
rate,
solve equations (l)-(3)
a pretreatment steady-state on days 0-250, and
administered a 7-secretase inhibitor that decreases the A/j production rate p by
250-620
(i.e.,
for
an 18-fold drop
1
year).
in the A,3
As shown
in
Figure
2,
is
40% on days
the post-treatment steady-state represents
burden and a theoretical decrease
in the
concommitant
from 5.0 (severe dementia) to 0.0 (no dementia). The perturbation dynamics
are rather sluggish:
perhaps
CDR score
in
Figure 2
the relaxation time, which we define to be the time from the start of
9
treatment until the A/? burden drops to
state
(i.e.,
90%
of the
way towards the post-treatment steady-
time until the A/i burden equals the steady-state post-treatment A/? burden
tlie
plus 0.1 times the difference of the steady-state pretreatment and post-treatment burdens)
is
113 days. Interestingly,
treatment
for the A/3
it
takes
much
longer ~ about 600 days after the discontinuation of
burden to revert to 90% of
a polymerization ratio r of 0.84 (Table
Comparing
Equation
(6)
**,
different treatments
allows us to provide a comparison across various treatment approaches. Witliin
(e.g.,
four parameters: 7-secretase inhibitors
all
upstream mechanism by which A/3
or other agents that target the
APP
pretreatment steady-state (assuming
1)).
the context of our model, treatments can affect
^'
its
is
produced from
promote the
/j-secretase inhibitors), reduce the production rate p; agents that
fragmentation of monomers from polymers and/or enhance the
monomer
increase the fragmentation rate / and loss rate
and agents that
deposition of A/3
production rate p
monomers reduce
is
the elongation rate e
is
reduced by x%;. Similarly,
/
is
y%
By equations
if
has the same effect as a
(4)
c is
x%
higher than
if
the loss rate
e
is
^
inhibit the
and
(6), if
the
lower than
the fragmentation rate /
have somewhat more leverage than
reducing the A/3 burden. Moreover, an
respectively),
e.
reduced by x%, then the resulting A/^ burden
Hence, the parameters p and
rate, respectively)
respectively;
the elongation rate
by y%, then the resulting A/3 burden
in
/,
*•
clearance rate
is
if
increased
increased by y%.
and
/, respectively,
x%
reduction in the production rate (elongation
y%
increase in the loss rate (fragmentation rate,
where
lOOx
^~
For example. Figure
2,
100
-x"
which was computed using a 7-secretase inhibitor that reduces the
production rate by 40%i, would also
resvilt
from a treatment that increased the
10
loss rate
by
66.7%.
Unfortunatt'ly, there
by changes
in
p
is
no simple formula to compare the A/? burden reduction achieved
/ or by changes
vs.
in e vs.
/.
However,
treatment steady-state Af3 burden (and corresponding
in
CDR
Figure 3 we plot
th(>
post-
score) as a function of Ijoth
the percentage reduction in production rate p achieved by a 7-secretase inhibitor and the
percentage increase in fragmentation rate / achieved by,
70 times larger than / in Table
10%) change
in these
rate
still
only a modest
/
is
(e.g.,
Because A/3 monomers
on dementia.
this figure also
off,
tliat
(recall that
recjuired to achieve a several-fold reduction in A(3
is
clinically significant effect
need to be cleared after they break
an A/i vaccine
This graph strongly suggests
1).
parameter values
burden and potentially a
e.g.,
shows that an
infinite
leads to a finite steady-state A/3 burden, given the limits of the
fragmentation
monomer
loss rate
/.
Additional computational results (not shown here) reveal that a fragmentation rate
enhancer has a smaller
(i.e.,
faster) relaxation
because the relaxation time depends
time than a production rate inhibitor, probably
in large part
on the fragmentation
rate.
For example,
an agent that increases the fragmentation rate by 118%! achieves the same post-treatment
steady-state A/3 burden as the
is
40%
7-secretase inhibitor in Figure
but the relaxation time
2,
only 40 days compared to 113 days for the 7-secretase inhibitor.
Supercritical regime
Thus
far,
we have assumed that
/•
<
1.
so that a steady-state
the A/3 burden grows indefinitely, eventually (perhaps after
at rate p{r
—
l)/r.
Moreover,
for all r
>
1,
is
many
achieved.
If r
>
1
then
years) increasing linearly
the distribution of polymers no longer decays
geometrically, but tends over time to a uniform distribution, where each ?-mer (starting with
smaller values of
t)
successively achieves the concentration
11
ci
=
//e,
c,
=
2//e
for
i.
>
2.
Heme,
in
is
there are three possibilities for the effect of treatment:
(i)
the A/3 burden
a pretreatment steady-state and drops to a lower post-treatment steady-state, as in
Figure
2;
(ii)
treatment causes the A/i burden to
steady-state regime (Figure 4a); and
the supercritical regime, although
(iii)
(ii)
than
in case
from the supercritical regime to the
treatment does not allow the A.i burden to exit
does lower the growth rate (Figure 4b).
it
of Figure 4a to Figure 2 shows that
steady-state in case
shift
may
it
nmch
take
Comparison
longer to achieve a post-treatment
(i).
Sensitivity analysis
Because we do not possess precise estimates
sitivity analysis that varies the
for
our parameter values, we performed a sen-
pretreatment polymerization ratio
driver of the A/3 dynamics, according to our analysis.
technique as before:
monomer
fix
/
and
e to their values in
ci/c, use the average A/?
wide range of values
we
for r,
which
Table
1,
in
investigate the effect caused by a
'^
which
find r
it
the primary
from the fraction of A/?
to derive p,
we now allow
is
same parameter estimation
use the
burden of 2819 pmol/g
calculate /. Rather than eciuating Ci/c to 1.3%,
a
We
/•,
and use
r
and p to
to vary in order to generate
turn causes p and / to change. In Figures 5a and 5b,
40%
reduction in the production rate (via a 7-secretase
inhibitor) as a fvmction of the pretreatment polymerization ratio
7".
Figure 5a plots the pre-
treatment steady-state A/3 burden divided by the post-treatment steady-state A/3 burden
(i.e.,
the fold-reduction in A/3 burden), and Figure 5b shows the relaxation time, which was
defined earlier. Recalling our assumption that a three-fold reduction in AI3 burden leads to
a clinically significant improvement in
CDR
score (Figure
1),
Figure 5a shows that the
40%
production inhibition appears capable of a significant clinical improvement for essentially
practical values of r
(i.e..
corresponding to percentages of monoiueric A/3, ci/c,
30%), and a l-to-2 log drop
in A,3
burden as
r increases
12
less
all
than
from 0.76 to 0.93. Figure 5b shows
=
that our base case of r
0.84
polymerization ratio. Hence,
is
if
on the steep portion of the curve of relaxation time versus
the fraction of
is
actually
5%
rather than
1%
and the relaxation time decreases from 113 days
of total A/i, then r drops from 0.84 to 0.7
to only
monomeric A/3
two weeks.
Discussion
Despite the existence of some mathematical models for A/i fibrilli/ation and plaque growth,
this
paper appears to represent the
attempt to use a mathematical model to assess
first
the effect of treatment on A/3 burden in Alzheimer's disease.
Our model
is
monomer production
purposefully
rate (p), A/3
parsimonious, and contains only four parameters:
A/3
monomer
and polymer fragmentation rate
loss rate (/),
The most
polymer elongation rate
basic result of our analysis
upon the value of the polymerization
less
than
1,
ratio
which equals pe/{fl).
If this
unitless quantity
then the A/9 burden enters a steady-state regime and takes on a
polymerization ratio
is
(/).
that there are two possible regimes, depending
is
r,
(e),
finite value. If
is
the
greater than one, then the A/3 burden grows indehnitely, eventually
increasing linearly at rate p{r
-
l)/r.
Researchers
in
other disciplines have found that
the dynamics of their complex systems are dictated by a unitless measure that leads to a
subcritical regime
greater than
in
1;
epidemiology
if
the measure
is
less
than
1
and a supercritical regime
if
the measure
is
two examples are the basic reproductive rate Rq of an infectious pathogen
^^
and the
in these disciplines the
traffic intensity
p in queueing theory
^^.
Moreover, as with AD,
ultimate measures of performance (size of the epidemic and queue
length, respectively) have a highly nonlinear relationship with the unitless measure. Applied
researchers in these disciplines have adopted these unitless measures as a central part of
\hc\r
mental model of these complex systems, and routinely estimate them and monitor
achieved reductions in them.
We
propose that
13
AD
researchers follow suit by adopting the
polymerization ratio pe/{fl) as the key "A/3 driver" in this disease.
Several studies have
with
th(>
ratio
is
shown that the A/3 burden does not appear
duration or clinical severity of
less
than
1
for
of plaque formation
symptomatic
'*' '^
""^
-
^^
of plaque via a feedback
may
exist,
patients.
which suggests that the polymerization
Although previous mathematical models
requires that the disaggregation rate be
modulated by the
mechanism that minimizes the changes that occur
While some feedback mechanism
brain.
21-26^
have also proposed a dynamic equilibrium of aggregation and
disaggregation, the model in
amount
AD
AD
to be tightly correlated
- for
in the
example, a cytotoxic T-lymphocyte response
our model shows that when A/3 production
is
A/3 burden can be achieved by a constant fragmentation rate
incorporated, a steady-state
(i.e.,
in the
absence of any
feedl)ack).
Nonetheless, our estimate for r
so
is
it
conceivable that certain aggressive forms of the disease in
amyloidogenic presenilin mutations)
importantly, while studies
measures
is
AP
'^"^--^
may
burden
and
or mice (strongly
1.
More
burden by counting plaques, a more recent study
burden biochemically, and these more refined data suggest that A/3 burden
(i.e.,
AD, which
is
not inconsistent with linear growth of
the supercritical regime in our model).
be required to further elucidate whether A/3 burden
continual growth in symptomatic
state
humans
achieve a polymerization ratio greater than
assess Af3
correlated with clinical severity of
A3
of the order of 10"' (rather than 10"^ or smaller),
is
AD
is
Although further research may
in a steady-state or
patients, our identification of
is
experiencing
two regimes (steady-
and supercritical) suggests that there are three types of possible treatment outcomes:
a reduction in
(Figure
1),
A3
burden from a pretreatment steady-state to a post-treatment steady-state
a change in regime from pretreatment growth to post-treatment steady-state
(Figure 4a), and a reduction
in
growth rate from a pretreatment supercritical regime to a
post-treatment supercritical regime (Figure 4b), These results suggest that the failure of a
14
drug to reduce the A/i burden
drug
inactivity,
in
a subset of mice or
than
is less
1,
burden within several months after treatment
is
necessarily be due to
but rather could signal a pretreatment supercritical regime. Also, even
pretreatment polymerization ratio
it
humans may not
a patient
may
if
the
revert to his pretreatment A/3
discontinued (see Figure 5b); consequently,
is
important to attempt to measure the A/3 burden throughout the course of treatment
a cliniial
trial.
In contrast,
if
the pretreatment polymerization ratio
after discontinuation of treatment a patient's A/3
burden
will
is
greater than
1,
always be smaller than
in
then
if
he
had not received treatment.
Equation
(6)
provides a simple formula for the steady-state A/3 burden in terms of the
polymerization ratio
pictured in Figure
<
1)
the A/3 burden
is
r
1,
(provided
the polymerization ratio,
a
modest reduction
in r
r
and the production rate-to-loss rate
ratio,
pi I. As
a highly nonlinear (increasing, convex) function of
and approaches
infinity as r
approaches
1.
Hence, the impact of
appears to be sufficient to produce a many-fold reduction
A/3 burden; for the parameter values in Table
a
1,
40%
reduction in the production rate
via a 7-secretase inhibitor achieves an 18-fold reduction in A/3 burden.
consistent with recently reported data in mice
^'
*
in the
and appears to be
Such a reduction
sufficient to convert
the disease process to a non-pathological state 2,3,29^ assuming neuronal dysfunction
concommitantly decreased. Figure
1
also
is
is
shows that, while the magnitude of the A/3 burden
reduction increases with the strength of treatment, there are decreasing returns to scale as
the treatment gets stronger.
in A/3
Finally, our analysis predicts that the percentage reduction
burden achieved by a given treatment
then decreasing) of the polymerization ratio
burden increases with
would be achieved
AD
mutation
^',
in
r,
is
r.
a unimodal function
For
r
<
1,
(i.e.,
first
increasing,
the percentage reduction in A/3
and hence one might expect that a larger percentage reduction
forms of
AD
that are particularly aggressive
the trisomy 21 nnitation that occurs in
15
(e.g.,
the Swedish familial
Down's syndrome
''^).
However,
as explained in the previous paragraph, the A/3
treatment
if
the post-treatment polymerization ratio
Our model
affect
burden continues to grow
is
flexible
enough
greater than
is
in the face of
1.
to incorporate a variety of treatment approaches that
any of the four model parameters. Equation
(5)
allows us to perform an apples-to-
apples comparison of production inhibitors, elongation inhibitors, clearance enhancers, and
For a given percentage change
fragmentation enhancers.
in
parameters caused by a treat-
ment, this analysis shows that the production inhibitors (clearance enhancers, respectively)
are
somewhat more
effective in reducing the A/3
Equation
tation enhancers, respectively).
(7)
burden than elongation inhibitors (fragmen-
and Figure 3 provide an
explicit
comparison
between production inhibitors and fragmentation enhancers, and computational results show
that a fragmentation enhancer attains
tion inhibitor.
in
its
post-treatment steady state faster than a produc-
These comparisons, coupled with future data on drug
determining the optimal mix and
level of
toxicity,
may be
useful
treatments that minimize the A/3 burden subject
to toxicity constraints.
Figure 2 shows that
new post-treatment
it
takes several
months
for
treatment to reduce the
A.(5
burden to a
steady-state, and the return to a pretreatment steady-state A/3 burden
following the discontinuation of treatment
that the rate of A/3 turnover
is
even more gradual. However, Figure 5b shows
is
highly sensitive to the pretreatment polymerization ratio
suggesting that aggressive forms of
AD
(having high
r)
are likely to take
much
r,
longer to
get under control. Hence, our lack of a precise estimate for the pretreatment polymerization
ratio prevents us
some
from accurately predicting the rapidity of response to treatment, but
cases this response
may be
This general state of
in
two seminal papers
the research
HIV
affairs is similar to
^^'•*.
community
considerably quicker than suggested in Figure
The
stability of
into believing that
HIV was
16
2.
infection, as revealed several years
plasma HIV
levels over
many
in
ago
years lulled
a relatively static disease process.
but a perturbation of this steady-state by a powerful protease inhibitor revealed a highly
dynamic equilibrium, where a high
virus production rate
was
offset
by an equally high virus
chvirance rate. Hence, antiviral therapy led to a precipitous drop in plasma
HIV
discontinuation of treatment allowed for a rapid return of
steady-state.
To borrow
A/9 level) in the bath
APP) and
AD
(i)
the analogy often used in the
may change
drain {A(5 loss)
field,
may be
lessons learned by the
HIV
toxicities of various types of agents are non-overlapping,
if
the water level
operating at deceptively high rates.
It is
the Achilles heel of
is
worthwhile
clinical research
dynamic equilibrium oi A/3 - which implies that
and the interaction between
Ap
toxicity,
which
is
(iii)
(ii)
(e.g.,
watch
given the
require chronic treatment -
production and Notch signalling
on developing drugs that avoid long-term
community
AD patients may
and
'*'';
for
community:
then drug combinations
HIV treatment
the
(i.e..
monomer from
a 7-secretase inhibitor plus an A/i vaccine) are likely to outperform monotherapy;
out for drug resistance, which
and
levels,
pretreatment
levels to the
very slowly, but the tap (production of A/i
mind the
researchers to keep in
HIV
HW
'^^-•^''^
efforts
should focus
beginning to plague the
HIV
^^.
Several of the model parameters, particularly the production rate and the fragmentation rate, are difficult to
and
(6)
measure
in vivo.
benefit of our analysis
is
that equations (5)
allow an indirect estimation of the production rate p and the fragmentation rate /
given pul)lished data on the A/9 burden
more
One
generally,
^
and the fraction of Afl that
is
monomer
^-
^^ (or,
any quantity, such as mean polymer length, that can be derived from the
steady-state distribution of i-mers). Equation (5) can also be used to measure the strength
(i.e.,
percentage inhibition or enhancement) of a treatment
treatment and post-treatment steady-state Al3 burdens.
in vivo,
given data on the pre-
Moreover, a transient analysis of
our model (not provided here) would allow for indirect estimation of a third model parameter
from
serial
measurements of post-treatment A(i burden.
17
Our study has two important
limitations. First, our
entiate between the various forms of A/3 {A(3iQ vs.
model does not currently
A/342, soluble vs.
differ-
However,
insoluble).
while we have been careful to restrict the model to A/i polymerization per sc and ignore
protofibril-to-fibril conversion
and plaque growth,
viewed as a representation of plaque growth
plaques are primarily due to
deposition onto plaques
is
monomer
believed to be the
more
may be more complex than
realistic
=
2/3 or
1,
model can,
the
be
in fact,
deposition onto plaques and fragmentation of
main form
monomer
'^^' '*'',
of aggregation in vitro
Similarly, fragmentation of oligomers
^^.
monomer
release that
is
assumed
here.
it
''^
is
and
Hence, a
model of plaque growth might use a variation of Smoluchowski's equation that
allows i-mers and /-mers to coalesce
A;
clear that our
addition and break-off, respectively. While
quite likely that polymers coalesce in vivo
plaques
if
it is
(e.g.,
at a rate proportional to 'i''j^Ci{t)cj{t),
where
depending on the porosity of plaques) and allows fragmentation of monomers
from the plaque surface
(at rate fi^'^Ci{t)) or the entire
plaque (at rate
While such
ftCi{t)).
a model would drastically change the distribution of A/3 ?;-mers relative to the current model
(skewing the distribution towards huge polymers that represent plaques),
significantly alter the basic nature of our results pertaining to the A/3 burden.
the extent that the model parameters
including the effect of treatment
A/342 or soluble vs. insoluble A/3, then these
in
-
unlikely to
is
it
However, to
vary for A/34o
vs.
model generalizations would be worth pursuing
the future.
The second main weakness
indicative of
human
AD
brains:
of our study
that our parameter values
is
the loss rate
/
soluble.
Our
fraction of A/3 that
is
pH environment
monomer with
our parameter estimates are, a modest (several-fold) change^
in
i'- '*.
^,
and
Also,
the fraction of A/3 that
sensitivity analysis (Figures 5a-5b) suggests that, regardless of
18
not necessarily
was derived from the brains of mice
the elongation rate e was measured from synthetic A/3 in a low
we crudely equated the
ar(>
how
is
inaccurate
a parameter value caused by
lead to a clinically significant
treatiiieiit will still
(i.e.,
at last three-fold) reduction in the
steady-state k(5 burden, but that the time to achieve this post-treatment steady-state
relaxation time)
is
(i.e.,
quite sensitive to our parameter values.
Despite the model's simplicity, our analysis elucidates the basic nat ure of the kinetics
of the .\d burden in the face of etiologic treatments, and provides a framework
metric, the polymerization ratio
-
^'
and a novel
within which to interpret the laboratory and clinical
results that are likely to be generated during the next few years.
on the identity of the toxic moiety
-
^^
,
As more progress
is
made
the elucidation of the inflammatory and neurotoxicity
cascade, and the parameter values and mechanisms related to A/9 polymerization and plaque
growth, our hope
is
that models such as this one will be refined and generalized to provide
some guidance about the optimal way
to
employ the emerging anti-A/3 drug
arsenal.
Acknow^ledgment
This research was partially supported by the Singapore-MIT Alliance
Foundation
for
Neurologic Diseases (DJS).
19
(LMW) and
by the
References
[1]
Selkoe, D.
Translating
J.
cell
biology into therapeutic advances in Alzheimer's disease.
Nature 399 (Supp). A23-A31 (1999).
[2]
Naslund,
Haroutunian, V., Mohs,
,).,
Buxbauin.
JAMA
A., Cheriiy, R. A., Fraser, F.
Bush, A.
&
W.,
Sclienk,
Huang,
I.,
S.,
D.,
J.
in
P.
k
the brain
Fuller, S. J.,
Smith, M.
J..
Beyreuther, K.,
Masters, C. L. Soluble pool of A/3 amyloid as a determinant of severity
of neurodegeneration in Alzheimer's disease.
[4]
Greengard,
283, 1571-1577 (2000).
McLean, C.
I.
P.,
D. Correlation between elevated levels of amyloid /^-peptide
.J.
and cognitive decline.
[3]
Davis, K. L., Davies,
R.,
Ann
Neurol 46, 8G0-866 (1999).
Barbour, R., Dunn, W., Gordon, G., Grajeda, H., Guido, T., Hu, K.,
Johnson-Wood,
Motter, R., Mutter,
L.,
K..
Khan,
K.,
Kholodenko, D., Lee, M., Liao,
Lieberburg,
Z.,
Soriano, F., Shopp, G., Vasquez, N., Vandevert, C., Walker,
Wogulis, M., Yednock, T., Games, D.
k
Seubert, P. Immunization with amyloid-/?
attenuates Alzheimer-disease-like pathology in the
PDAPP
mou.se. Nature 400, 173-177
Games,
D., Grajeda, H.,
(1999).
[5]
Bard,
F.,
Cannon, C, Barbour,
Hu, K.. Huang,
I.,
P.,
.].,
R., Burke, R.-L.,
.Johnson-Wood, K., Khan. K., Kholodenko, D., Lee, M., Lieberburg,
Motter, R., Nguyen, M., Soriano,
Schenk, D.
&
Guido, T.,
F., Vascjuez,
N., Weiss, K.,
Welch, B., Seubert,
Yednock, T. Peripherally administered antibodies against amyloid
/9-peptide enter the central nervous system
and reduce pathology
in
a
mouse model
of
Alzheimer disease. Nature Medicine 6 916-919 (2000).
[6]
Weiner, H.
L.,
Isscizadeh, S.,
Lemere, C. A., Maron, R., Spooner, E. T., Grenfell. T.
Hancock, W. W.
&
Selkoe, D.
20
J.
.L,
Mori,
C,
Nasal administration of amyloid-beta
peptide decreases cerebral amyloid burden
in a
mouse model
of Alzheimer's disease.
An7i. Neurol. 48, 567-579 (2000).
[7]
Wolfe,
T.,
Xia, W., Moore, C. L., Leatherwood, D. D., Ostaszevvski, B. L., Rahmati,
iM. S.,
Donkor,
O.
I.
k
Selkoe, D.
.Alzheimer's 7-secretase
is
.J.
Peptidomimetic probes and molecular modeling suggest
an intramembrane-cleaving aspartyl protease. Biochem. 38,
4720-4727 (1999).
[8]
Felsenstein, K.
from
M. The next generation
of
AD
therapeutics: the future
is
now. Abstracts
annual conference on Alzheimer's disease and related disorders, Abstract
the 7th
613 (2000).
[9]
Naiki, H., Higuchi, K., Nakakuki, K.
polvmerization in
[10]
k
Naiki, H.
Lomakin.
Takeda, T. Kinetic analysis of amyloid
vitro.
A..
Chung, D.
S.,
Benedek, G.
B., Kirschner, D. A.
and
J.
D.
Lansbury,
P.
scrapie: mechanistic truths
solulnlity of
[13]
k
fibrils:
USA
of rate constants. Proc. Natl. Acad. Sci.
Harper.
fibril
Labaratory Investigation 74, 374-383 (1996).
nucleation and growth of amyloid /^-protein
[12]
fibril
Laboratory Investigation 65, 104-110 (1991).
Nakakuki, K. First-order kinetic model of Alzheimer's /3-amyloid
extension in
[11]
vitro.
k
k
Teplow, D. B.
On
the
detection of nuclei and quantitation
93, 1125-1129 (1996).
T. Models of amyloid seeding in Alzheimer's disease
and physiological consequences of the time-dependent
amyloid proteins. Annu. Rev. Biochem. 66, 385-407 (1997).
"Walsh, D. M..
Lomakin,
A.,
Benedek, G.
B.,
Condron, M. M.
k
Teplow, D. Amyloid d-
protein fil)rillogenesis: detection of a protofibrillar intermediate. Journal of Biochemistry
272. 22364-22372 (1997).
21
[14]
Lomakin,
Teplow, D.
A.,
{ihrillogenesis of
[15]
[16]
B.,
Kirschner, D. A.
k
Benedek, G. B. Kinetic theory of
amyloid /i-protein Proc. Natl. Acad.
Naiki, H., Hasegawa, K., \aiiiaguchi,
I.,
Set.
Nakamura,
USA
94, 7942-7947 (1997).
H., Gejyo,
F.
&
Nakakuki, K.
antioxidants have different mechanisms of inhibiting Alzheimer's
Apolipoprotein
E and
/3-amyloid
fibril
formulation zn
Inouye, H.
k
Biochemistry Z7
vitro.
,
17882-17889 (1998).
Kirschner, D. A. A/^ fibrillogensis: kinetic parameters for
fibril
formation
from Congo red binding. Journal of Structural Biology 130, 123-129 (2000).
[17]
Hyman,
B. T., West, H. L., Rebeck, G. W., Buldyrev, S. V.,
M., Havlin,
S.
k
ferences associated with apolipoprotein
Proc. Natl. Acad. Set.
Cruz,
L.,
Urbane,
B.,
USA
E.
and molecular epidemiology of
E genotype and
S.
Dynamics
L.,
(Down syndrome).
V., Christie, R., Gomez-Isla, T., Havlin, S.,
k Hyman,
B. T. Aggregation
plaques in Alzheimer disease. Proc. Natl. Acad. Set.
Urbane, B., Cruz,
trisomy 21
dif-
92, 3586-3590 (1995).
Buldyrev,
Namara, M., Stanley, H.
[19]
N., Ukleja,
Stanley, H. E. Quantitative analysis of senile plaques in Alzheimer
disease: observation of log-normal size distribution
[18]
Mantegna, R.
Buldyrev
S.
V.,
Havlin,
USA
S.,
and disaggregation of
Mc-
senile
94, 7612-7616 (1997).
Stanley, H. E.
k Hyman,
B. T.
of plaque formation in Alzheimer's disease. Biophy.sical .Journal 76, 1330-
1334 (1999).
[20]
von Smoluchowski, M. Drei vortrage iiber diffusion, brownsche bewegung und koagulation
[21]
von kolloidteilchen.
Z. Phys. 17,
557-585 (1916).
von Smoluchowski, M. Versuch einer mathematischen theorie der koagulationskinetic
koUoider losungen.
Z. Phy.s. 92,
129-168 (1917).
22
[22]
&
Family, F.
Landau, D.
Kinetics of Aggregation and Gelation. North-Holland,
P.
Am-
sterdam (1984).
[23]
Sonntag, H.,
New York
[24]
Hyman,
k
Strenge, K. Coagulation Kinetics and Structure Formation. Plenum,
(1987).
K&
B. T. Marzloff",
or amyloid
burden
in
Arriagada,
P. V.,
V.
P.
The
lack of accumulation of senile plaques
Alzheimer's disease suggests a dynamic balance between amyloid
deposition and resolution.
[25]
Arriagada,
J.
Growdon,
Neuropathol. Exp. Neurol. 52, 594-600 (1993).
Hedley-Whyte, E. T.
J. H.,
k Hyman,
B. T. Neurofibril-
and severity of Al/heimer
lary tangles but not .senile plaques parallel duration
disease.
Neurology 42, 631-639 (1992).
[26]
Berg,
McKeel, D. W.,
L..
Miller,
indexes of Alzheimer's disease
and
[27]
older. Arch. Neurol.
Harper,
D.,
.1,
Amyloid
'Wong,
protofibrils:
in
S.,
an in
.J.
k
Morris,
.J.
C. Neuropathological
(1993).
Lieber, C.
vitro
Baty,
demented and nondemented persons aged 80 years
50 349-358
S.
P.,
.J.
model
M.
k
Lansbury,
P.
T.
.Ir.
for a possible early event in
Assembly of A/J
Alzheimer's disease.
Biochemi.Htry 38, 8972-8980 (1999).
[28]
Tseng, B.
Mantyh,
P., Esler,
P.
W., Lee,
W.
P., Clish,
J. P.
k
C. B., Stimson. E. R., Ghilardi,
Maggio,
J.
E. Deposition of
J.
R., Vinters, H. V.,
monomeric, not oligomeric, A/3
mediates growth of Alzheimer's disease amyloid plaques
in
human
brain preparations.
Biochemistry Z%, 10424-10431 (1999).
[29]
Wang,
.J.,
Dickson, D. VV.. Trojanowski,
.J.
Q.
k
Lee. V. M.-Y.
The
levels of soluble
versus insoluble brain A/J distinguish Alzheimer's disease from normal and pathologic
aging. Experimental Neurology 158, 328-337 (1999).
23
[30]
Lue, L.-F., Kuo, Y.-M., Roher, A. E., Brachova, L., Shen, \., Sue,
J.
H., Rydel, R. E.
k
Rogers,
J.
Soluble amyloid
Am.
of synaptic change in Alzheimer's disease.
[31]
Gravina,
S.
Suzuki, N.
Eckman, C.
A.. Ho, L.,
&
Younkin,
S.
G. Amyloid
/^
Pathol. 155, 853-862 (1999).
Long, K.
B.,
Beach, T., Kurth,
peptide concentration as a predictor
/i
J.
L.,
Otvos, L.
E.,
Jr.,
Younkin,
L. H.,
(A/i) in Alzheimer's Disease Brain: biochemical
and immunocytochemical analysis with antibodies
specific for
forms ending at A/340 or
A/342(43). Journal of Biochemistry 270. 7013-7016 (1995).
[32]
Janus, C., Pearson,
Chishti, M.,
Home,
J.,
P.,
McLaurin,
J.,
Mathews,
Heslin, D., French,
J.,
P.
M., Jiang, Y.. Schmidt,
Mount, H. T.
M., Bergeron, C., Eraser, P. E., St. George-Hyslop, P.
k
immunization reduces behavioral impairment and plaques
disease.
[33]
Morgan,
Dufi",
J.,
S. D.,
Azhar
Nixon, R. A., Mercken,
VVestaway, D. A/5 peptide
in a
model of Alzheimer's
Naturt 408, 979-982 (2000).
Diamond, D. M., Gottschall,
D.,
P. E.,
K., Jantzen, P., DiCarlo, G., VVilcock, D.,
Gordon, M.
k
Arendash, G.
W.
Ugen, K.
E., Dickey, C.,
Connor, K., Hatcher,
A.d peptide vaccination prevents
J.,
memory
Hardy,
J.,
Hope,
C.,
loss in
an
animal model of Alzheimer's disease. Nature 408, 982-985 (2000).
[34]
'Wolfe,
J.
M.
S.,
Xia, W., Ostaszewski, B. L., Diehl, T.
Two transmembrane
and 7-secretase
[35]
De Strooper,
Kimberley, 'W. T.,
k
Selkoe. D.
aspartates in presenilin-1 recjuired for presenilin endoproteolysis
activity. Nature.
B.,
S.,
398, 513-517 (1999).
Annaert, W., Cupers,
P., Saftig, P.,
Schroeter, E. H., Schrijvers, V., Wolfe, M.
S.,
Ray,
W.
Craessaerts, K.,
J.,
Goate, A.
k
Mumm,
J.
Kopan. R.
S.,
A
presinilin-1-dependent gamma-secretase-like protease mediates release of Notch intracellular
domain. Nature 398, 518-522 (1999).
24
[36]
Struhl, G.
m
[37]
k
Greenwald,
Drosophila.
Ve,
Presinilin
Natwc 398, 522-525
Lukinova, N.
\'.,
I.
k
required for activity and nuclear access of Notch
(1999).
M.
Fortini,
is
E.
Neurogenic phenotypes and altered Notch pro-
cessing in Drosophila Presinilin mutants. Nature 398, 525-529 (1999).
[38]
Diekniann, O., Heesterbeek,
J.
A.
tion of the basic reproductive ratio
populations.
[39]
[40]
Rq
Metz,
in
J.
A.
models
J.
On
the definition and the computa-
for infectious diseases in
heterogeneous
Math. Biol. 28 365-382 (1990).
J.
Networks and
Kelly. F. P. Stochastic
NY
k
P.
John Wiley and Sons,
Reversibility.
New
York,
(1979).
Monsonego,
role of
T
Maron,
A.,
R.,
cell reactivity to
Bar-Or,
.A..,
Krieger,
J. I.,
A-Beta amyloid peptide
k
Selkoc, D.
in the
Weiner, H.
I.
The
pathogenic processes associ-
ated with Alzheimer's disease. Abstracts from the 7th annual conference on Alzheimer's
disease
[41]
and
related disorders, Abstract 105 (2000).
Citron, M., Oltersdorf, T., Haass,
Pelfrey,
C,
Lieberburg,
I.
k
C, McConlogue,
Selkoe, D.
.J.
L.,
Hung, A.
\'.,
Seubert,
P..
Vigo-
Mutation of the /^-amyloid precursor protein
in
familial Alzheimer's disease increases /i-protein production. Nature 360, 672-674 (1992).
[42]
Lemere, C. A., Blustzjan,
D.
,].
.1.
K.,
Yamaguchi.
H., VVisniewski, T., Saido. T. C.
Sequence of deposition of heterogeneous amyloid /3-peptides and
syndrome: Implications
for initial events in anyloid
k
Apo E
Selkoe,
in
Down
plaque formation. Neurobiol. Disease
3, 16-32 (1996).
[43]
Wei
J.
X..
Ghosh
S. K.,
D., Bonhoeffer, S.,
Taylor M.
E.,
Nowak, M.
Johnson. V.
A.,
Hahn,
25
.A.,
Emini. E. A., Deutsch,
B., H., Saag,
M.
S.
i;
P., Lifson,
Shaw, G. M. Vi-
ral
dynamics
in
human imnumodeficiency
virus type
1
Nature 373, 117-123
infection.
(1995).
[44)
Ho
D. D.,
Neumann
A. U., Perelson A.
Rajiid turnover of plasma virions
and
S.,
CD4
Chen W., Leonard
lymphocytes
in
J.
HIV-1
M.
k
Markowitz M.
infection.
Nature 373,
123- 126 (1995).
[45]
Condra
.1.
H., Schleif
C, Rhodes,
W.
A.,
Blahy O. M., Gabrelski,
A., Robbins, H. L.
k
L. J.,
Graham, D.
,].,
Quintero,
J.
Shivaprakash, M. In vivo emergence of HIV-1 variants
resistant to multiple protease inhibitors. Nature 374, 569-571 (1995).
[46]
Carr. A., K. Samaras, D.
.1.
Chisholm
k
Cooper. D. A. Pathogenesis of HIV-1 protease
inhibitor-associated peripheral lipodystrophy, hyperlipidemia, and insulin resistance.
Lancet 131, 1881-1883 (1998).
[47]
Esler,
W.
P.,
W. k Maggio,
Stimson, E. R., Ghilardi,
J. E.
first-order kinetics.
[48]
k
Mantyh,
P.
Biochemistry 35, 749-757 (1996).
Bush, A.
brain. In Abstracts
R., Vinters, H. V., Lee, J. P.,
In vitro growth of Alzheimer's disease /^-amyloid plaques displays
Cherny, R. A., Guerette,
Masters, C. L.
.J.
from
P. A.,
I.
McLean, C, Legg,
Oligomeric
the 7th
\3
in
J. T.,
Eraser, F.
PBS-soluble extracts of
W.. Volitakis,
I.,
human Alzheimer
annual conference on Alzheimer's disease and related
disorders, Abstract 62 (2000).
26
3
6
c
a
•S
5
5-4
« 3
5.0
I
>>
•o
(0
o
-•
(0
2.0
1,0
0.5
-^^e=^
—~"'^
I
0.1
0.0
—
0.3
0.2
'
0.5
0.4
polymerization
Figure
1:
().()
and
ratio,
(0.5. 1.0, 2.0
and
.severe, respectively)
ordinate) and
CDR
r,
with p and
5.0, respectively)
/
0.9
0.8
r
Steady-state A/3 burden and clinical dementia rating
of the polymerization ratio
of
0.7
0.6
(CDR)
score as a function
fixed at the values in Table
1.
A CDR
corresponds to no (questionable, mild, moderate,
dementia. The relationship between steady-state A/9 burden
score (right ordinate)
score
is
based on Table
1
of'-,
(left
as explained in the text.
2.5
c
0)
1.5
<
0.5
% enhancement in fragmentation rate
iC^
c
•D
3
<
2
pretreatment
a
3
n
<
.£
C
o
.E
=
o
o
E
%
of
monomer
A|5
MOV
^00'
Date Due
Lib-26-67
MIT LIBRARIES
3 9080 02245 1980