Hazard (Edition No. 72) Summer 2010/11 Victorian Injury Surveillance
advertisement
 Summer 2010/11 Victorian Injury Surveillance")
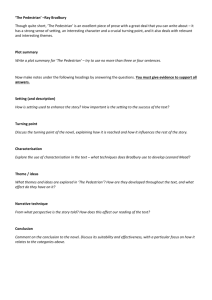
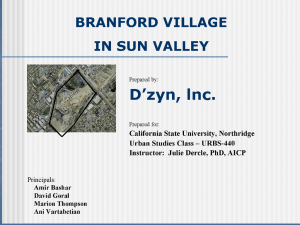
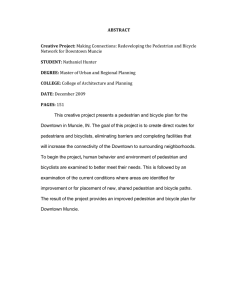
Hazard (Edition No. 72) Summer 2010/11 Victorian Injury Surveillance Unit (VISU) www.monash.edu.au/muarc/visu Monash University Accident Research Centre Traffic-related pedestrian injury in Victoria (2): Fatal injury Erin Cassell, Emily Kerr, Nicolas Reid, Angela Clapperton, Hafez Alavi This is a companion edition to Hazard 71 in which results from the investigation of hospital-treated traffic-related pedestrian injury were presented. This edition deals with fatalities. Summary Death data from the ABS Death Unit Record File (ABS-DURF), held by VISU, were used for trend analysis. All other analyses utilised data on traffic-related pedestrian deaths extracted from the National Coroners Information System (NCIS). Only closed cases were selected, 11 pedestrian deaths were still under investigation at the time of extraction. • The number of traffic-related pedestrian deaths fell significantly by 32% and the age adjusted death rate fell significantly by 42% in the period 1997-2006. Data for more recent years are not yet available from the ABS. • There were 120 traffic-related pedestrian deaths recorded on NCIS for the 3-year period January 2006 to December 2008. Pedestrian deaths still under investigation were excluded. • 57% of pedestrian deaths were male (n=68). The death rate for males (0.9/100,000) was higher than that for females (0.7/100,000). • Just over one-third (34%) of pedestrian deaths were in age group 75 years and older. Overall, the death rate was highest in persons aged 80-84 years (5.6 per 100,000), followed by persons aged 85+ years (3.4 per 100,000) then persons aged 75-79 years (3.3 per 100,000). The all-ages pedestrian fatality rate was 0.8/100,000. • Residents of 43 of the 79 Victorian Local Government Areas (LGAs) were killed in pedestrian crashes. Most pedestrians were fatally injured in crashes that occurred in the LGA in which they lived (72%, n=86). • Saturday was the peak day for pedestrian deaths (23%). • Pedestrian road manoeuvre at time of crash: 56% were killed when crossing the road, mostly at uncontrolled crossings; 9% were killed on the footpath or median by vehicles VICTORIAN INJURY SURVEILLANCE UNIT UNIT that left the road and crashed into them; 6% were killed on the footpath, nature strip or road by reversing vehicles. A further 19% were killed when lying, standing or walking on the road or when they jumped/stepped unexpectedly onto the road (most of these victims were intoxicated), 2.5% were killed when attending to broken down vehicles and 2.5% when operating mobility devices. • 40% of pedestrian fatalities occurred on urban arterial roads, 26% on rural roads and 23% on highways or freeways. • Up to three contributory factors were recorded for each fatality. The major contributory factors were (in rank order): pedestrians’ unsafe road use behaviour or failure to observe/misjudgements of traffic (implicated in 51 pedestrian deaths); drivers’ unsafe or dangerous behaviour (32 deaths); pedestrians’ misuse of alcohol and/or licit or illicit drugs (31 deaths); poor visibility and/or poor conspicuity of pedestrians (23 deaths); and medical or health condition of pedestrians (11 deaths). HAZARD HAZARD72 72 page page1 1 • Analysis of coroners’ findings and information on causality in coroners’ investigation reports indicated that the pedestrian was primarily responsible for the fatal crash in 44% of cases, the driver in 25% and there was no finding with regard to primary responsibility in 32% of cases. • Sixty percent (n=72) of pedestrian deaths resulted from multiple injuries, 27% (n=32) were due to severe head injury. The high risk groups for pedestrian deaths are persons aged 75 years and older and intoxicated males. Readers are referred to the last issue of Hazard on hospital-treated pedestrian injury for an extensive discussion of risk and protective factors and evidencebased prevention measures (http://monash. edu.au/muarc/VISU/hazard/Haz71.pdf). This information is summarised in tables in the two Appendices to this edition. 1. Introduction The last issue of Hazard (Hazard No 71) was focused on traffic-related hospital-treated pedestrian injury. In this issue we report the results of an in-depth study of traffic-related pedestrian deaths utilising data extracted from the National Coroners Information System (NCIS). We investigated the frequency, trend, patterns and contributory factors to trafficrelated pedestrian injury deaths in Victoria to provide information to underpin interventions to reduce the occurrence of pedestrian crashes and the severity of crash outcomes. 2. Methods 2.1 Case selection For the main analyses, cases were selected from the NCIS. Only ‘closed’ trafficrelated pedestrian fatalities were selected, 11 additional traffic-related fatalities were found but excluded as the coronial investigation was still open. Cases were selected using the following variables: 1. Case type on completion = death due to external causes 2. Intent type on completion = unintentional 3. Case jurisdiction = Victoria 4. Mechanism of injury = blunt force > transport injury event > pedestrian 5. Case year = 2006-2008 3. Results After initial selection, cases were further examined then excluded if the cause of death was recorded as due to: • suicide; • a medical condition; or • a collision with a railway vehicle that occurred off-road OR • if the on-road death of a user of a pedestrian conveyance such as a wheelchair, skateboard, inline skates or a toy scooter was due to a fall or other cause unrelated to a collision with a motor vehicle or other form of on-road transport. 3.1 Counts Over the three-year period 2006-8 there were 120 traffic-related pedestrian deaths recorded on the NCIS for Victoria (Table 1). Of these deaths, 50 (42%) occurred in 2006, 30 (25%) in 2007, and 40 (33%) in 2008. However, these data may be incomplete as coronial investigations into 11 further pedestrian deaths are still open (1 in 2006, 4 in 2007 and 6 in 2008) and there may be other open cases that were not coded or recorded on the NCIS at the time of selection. 2.2 Rates and trends Table 1 shows the counts of traffic-related pedestrian deaths provided or published by 3 agencies: the NCIS, the Transport Accident Commission (based on police reports) and the Australian Bureau of Statistics (ABS). The difference in counts is explained by different sources of data and inclusion and exclusion criteria employed by the three agencies when classifying cause of death. Death data from the ABS Death Unit Record File (ABS-DURF), held by VISU, were used for trend analysis. Age-adjusted rates were calculated using the direct method with the Victorian population at June 30, 2001 as the standard. Trends were determined using a log-linear regression model of the rate data assuming a Poisson distribution of deaths. A trend was considered statistically significant if the p-value of the slope of the regression model was less than 0.05. Table 1 Frequency of traffic-related pedestrian fatalities by data source, Victoria 2006-2008 DATA SOURCE 2006 2007 2008 TOTAL National Coroners Information System (NCIS) 50 (51 if all open cases included) 30 (34 if all open cases included) 40 (46 if all open cases included) 120 (131) Transport Accident Commission (TAC) 58 41 59 158 Australian Bureau of Statistics (ABS-DURF) 58 N/A* N/A* N/A Note: ABS-DURF 2007 and 2008 not yet released to VISU due to data and administrative issues at the ABS end. VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 2 3.2 Trend ABS-DURF data were used to estimate rates and trends as this is the most complete and reliable dataset available to VISU for the 10year period 1997-2006. The release of the Cause of Death Unit Record File for 2007 and 2008 has been delayed by the ABS due to technical and administrative issues. Figure 1 Trend in unintentional traffic-related pedestrian injury deaths, Figure 1 Trend in unintentional frequency and rate, Victoria 1997-2006 traffic-related pedestrian injury deaths, frequency and rate, Victoria 1997-2006 According to the ABS-DURF, there were 669 traffic-related pedestrian deaths over the decade 1997-2006, an average of 67 deaths per year (range 48 to 89). As shown in Figure 1 both the frequency and rate of traffic-related pedestrian deaths increased at the very start of the decade then decreased to 2004 (except for the sharp increase in 2001) before trending upward thereafter. Trend analysis (using Poisson regression modelling) showed that: • the frequency of traffic-related pedestrian deaths decreased significantly over the decade – the estimated annual decrease in the number of deaths was 4.1% (95% confidence interval -7.7% to -0.5%) and the overall decrease was 34% (-55% to -5%) • the death rate also decreased significantly – the estimated annual decrease in the death rate was 5.3% (95% confidence interval -9.1% to -1.7%) and the overall reduction in the death rate was 42% (-61% to -16%). Over the decade male death rates were consistently higher than those for females. Death rates for males and females both fell significantly, by 40% and 44% respectively. There was a significant 41% fall in the adult pedestrian death rate over the decade (95% confidence interval -63% to -11%). The 54% decrease in the child pedestrian death rate, though large, did not reach statistical significance (95% confidence interval, -84% to +14%). 3.3.1 Pedestrian demographic characteristics Gender and age Table 2 shows the frequency and rate of pedestrian fatalities by age groups and gender. Victorian population data form the denominator for rate calculations due to the lack of a commonly accepted or adopted measure of pedestrian exposure to risk. Further analysis of data for persons aged 75 years and older showed that the number of Overall, 57% of pedestrian fatalities were fatalities was highest in age group 80-84 years male (n=68) and males were over-represented (n=18, 15% of all pedestrian deaths), followed in pedestrian deaths in all 15-year age groups by age group 75-79 years (n=14, 12%) and except in children aged 0-14 years The age group 85+ (n=9, 8%). The fatality rate pedestrian fatality rate was higher in males (0.9 was also highest in persons aged 80-84 years per 100,000 males) than females (0.7/100,000 (5.6 per 100,000), followed by persons aged 85+ years (3.4 per 100,000) then persons aged per 100,000 females). 75-79 years (3.3 per 100,000). The all-ages pedestrian fatality rate was 0.8/100,000. Table 2 Frequency and rate of pedestrian fatalities by age group and gender, Victoria 2006-2008 (n=120) AGE 3.3 Characteristics of trafficrelated pedestrian fatalities The data used in these analyses were derived from coroners’ findings, police reports and toxicology reports available on the NCIS. In both sexes the risk of fatal injury in pedestrian crashes generally increased as age increased, with a sharp increase in risk from age 75 years. In total, 34% of all trafficrelated pedestrian fatalities were in age group 75 years and older. Over the study years, persons in this age group comprised 6% of the Victorian population which underscores the over-representation of older people in pedestrian fatalities. GROUP 0-14 MALE FEMALE N (%) Rate/100,000 ALL N (%) Rate/100,000 N (%) Rate/100,000 1 ( 1.5) 0.07 5 ( 9.6) 0.35 6 ( 5.0) 0.20 15-29 10 (14.7) 0.59 7 (13.5) 0.44 17 (14.2) 0.52 30-44 14 (20.6) 0.82 5 ( 9.6) 0.29 19 (15.8) 0.55 45-59 11 (16.2) 0.73 9 (17.3) 0.58 20 (16.7) 0.65 60-74 10 (14.7) 1.10 7 (13.5) 0.73 17 (14.2) 0.91 75 + 22 (32.3) 5.29 19 (36.5) 3.17 41 (34.2) 4.04 68 (100.0) 0.88 52 (100.0) 0.66 120(100.0) 0.77 All ages Source: National Coroners Information System (NCIS) VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 3 Location (LGA) of residence and crash site Pedestrian fatality data were compared by Local Government Area (LGA) in which the fatally injured pedestrian lived (Table 3) and the LGA where the fatal crash occurred (Table 4). Over the period 2006-8, residents of 43 of the 79 Local Government Areas (LGAs) in Victoria were killed in pedestrian crashes. The top 12 LGAs for deaths, ranked separately on frequency and rate, are shown in Table 4. Four LGAs —Mildura, La Trobe, Maribyrnong and Stonnington— had both a comparatively high number and rate of deaths. The high ranking of Mildura is due to 6 residents being killed in a single pedestrian crash in 2006 so should be regarded as a statistical aberration. Nine of the 12 LGAs that were highly ranked on the number of their residents killed were in metropolitan Melbourne, whereas 10 of the 12 LGAs with the highest pedestrian fatality rates were in rural Victoria. Cross tabulation of crash location data with place of residence data showed that most pedestrians (72%, n=86) were killed in the LGA in which they lived i.e. relatively close to home. The 12 highest ranked LGAs for fatal pedestrian crashes are listed in Table 4 along with figures that show the number of crashes that involved their own residents. None of the fatal pedestrian crashes that occurred in the City of Melbourne involved their own residents. Table 3 RANK Top 12 Local Government Areas (LGAs) for pedestrian deaths (among residents) ranked on the frequency and population rate of pedestrian fatalities in their area, Victoria 2006-8 NUMBER OF RESIDENTS OF LGA KILLED IN PEDESTRIAN CRASHES RESIDENTS’ PEDESTRIAN FATALITY RATE LGA N LGA 1 2 3 4 5 6 7 8 9 10 11 12 Casey Mildura La Trobe Greater Dandenong Monash Greater Geelong Maribyrnong Stonnington Glen Eira Darebin Moreland Brimbank 7 6 6 6 6 6 5 5 4 4 4 4 RATE/100,000 RESIDENTS (N) Mount Alexander Mildura Moorabool Glenelg Gannawarra La Trobe South Gippsland Maribyrnong Benalla Wodonga Horsham Stonnington 5.6 (3) 3.9 (6) 3.7 (3) 3.2 (2) 2.9 (1) 2.7 (6) 2.5 (2) 2.4 (5) 2.4 (1) 1.9 (2) 1.7 (1) 1.7 (5) Note: 1Where LGAs had the same number of deaths they were ranked according to population size, with the LGA with the lowest population given the highest ranking in the group and so forth Source: National Coroners Information System (NCIS) Table 4 Top 12 Local Government Areas (LGAs) for fatal pedestrian crashes, Victoria 2006-8 LGA NUMBER OF FATAL PEDESTRIAN CRASHES IN LGA (NUMBER INVOLVING OWN RESIDENTS) 1 Monash 7(5) 2 Mildura 6(6) 3 La Trobe 6(6) 4 Greater Dandenong 6(5) 5 Greater Geelong 6(6) 6 Casey 6(4) 7 Maribyrnong 5(3) 8 Stonnington 5(3) 9 Yarra 4(3) 10 Glen Eira 4(2) 11 Kingston 4(2) 12 Melbourne2 4(0) Notes: Source: VICTORIAN INJURY SURVEILLANCE UNIT Where LGAs had the same number of fatal crashes they were ranked according to population size, with the LGA with the lowest population given the highest ranking in the group and so forth 2 City of Melbourne has a lower resident population than Kingston and Glen Eira but is ranked 12th because of the estimated 771,000 people who use the city each day. National Coroners Information System (NCIS) 1 HAZARD 72 page 4 3.3.2 Time of occurrence of crash Season of year Figure 2 Season in which the pedestrian-related fatalities occurred by age group, Victoria 2006-2008 Fatal pedestrian crashes were fairly evenly distributed across autumn (n=34, 28%), winter (n=32, 27%) and summer (n=30, 25%), with the lowest number occurring in spring (n=24, 20%). Figure 2 shows the seasonal pattern by age group. Among persons aged 30-44 and 75 years and older, winter was the most common season in which fatalities occurred whereas autumn was more common in fatalities among 0-14 and 45-59 year olds. Among 15-29 year olds, there was a high proportion of deaths in summer but this was due to a multiple fatality. Day of week Figure 3 shows the distribution of pedestrian fatalities by day of week. Twenty-three percent of all pedestrian-related deaths occurred on a Saturday (n=28), the peak day for deaths, compared with 9% (n=11) on a Sunday. There was a fairly even spread of pedestrian fatalities across week days (1316%), except for Wednesday (10%). Figure 3 Distribution of pedestrian deaths by day of week, Victoria 2006-2008 Day of week by gender The commonest day for fatal pedestrian crashes involving males was Saturday (n=19, 28%) whereas it was Thursday for females (n= 13, 25%). Time of day The Geoscience Australia website was used to determine whether the fatal crashes occurred during daytime, night time, dawn or dusk (Figure 4). Forty-nine percent (n=59) of fatal pedestrian crashes occurred during daytime, 39% (n=47) occurred at night and 4% (n=5) occurred at dawn or dusk. The time of day for 9 deaths (8%) was not recorded on the NCIS. Figure 4 Distribution of pedestrian deaths by time of day, Victoria 2006-2008 Time of day by age More than two-thirds of children aged 0-14 (n=4, 67%) and adults aged 60 years and older (n=40, 69%) were killed in daytime. In contrast, persons aged between 15 and 44 were much more likely to be killed at night than during the day (72% versus 17%). In the 15-19 age group, 90% (n=9) of male fatalities occurred at night as did 71% (n=5) of female fatalities. Persons aged 45-59 were equally likely to be killed in daytime as night-time. VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 5 3.3.3 Type of vehicle involved in collision Figure 5 Vehicles involved in fatal pedestrian crashes, Victoria 2006-2008 As shown in Figure 5, most pedestrian deaths occurred in crashes with passenger cars (n=85, 71%), followed by light trucks, vans or utility vehicles (n=15, 13%) and trucks (n=11, 9%). 3.3.4 Nature of crash Pedestrian road manoeuvre and crash circumstances Information on the road manoeuvre being performed by the pedestrian at the time of the fatal crash is summarised in Table 5. Crossing road Fifty-six percent of all pedestrian fatalities (n=67) occurred when the pedestrian was crossing the road. These were mostly at uncontrolled crossings either from the kerb/ median strip (n=44, 37% of all pedestrian fatalities) or through parked or stationary vehicles (n=7, 6%). Thirteen percent of all fatal crashes (n=16) occurred on controlled crossings. Crossing road at uncontrolled crossings Fifteen pedestrians were struck on the far side of the road at uncontrolled crossings. They mostly had traversed several lanes and then misjudged the distance of an oncoming vehicle and walked or ran into its path. Only one was reported to be under the influence of drugs or alcohol. All but two were aged 65 years or older (87%). Of the 15 pedestrians involved in near-side fatal collisions at uncontrolled crossings, nine suffered fatal injuries when they stepped out from the kerb or median strip in front of vehicles. Another two occurred when the pedestrian changed his or her mind, hesitated, stopped or double backed into the path of a vehicle. Three of the remaining four cases happened when the pedestrian suddenly ran onto the road, two of whom were children. Only two of the near-side crash victims had high BAC levels. In total, eight of the fifteen pedestrians (53%) involved in fatal near side collisions at uncontrolled crossings were aged 70 years or older. At least four of these older pedestrians suffered from dementia and/or vision and hearing problems and two others appeared unaware of approaching vehicles. There was no information on the side of the road on which the pedestrian was hit for 12 cases that occurred at uncontrolled crossings. Source: NCIS (2006-2008) Three were rushing across the road, two to catch public transport. Two pedestrians were highly intoxicated and in a further case the pedestrian and the vehicle driver had BAC levels of 0.11 and 0.09, respectively. A variety of factors contributed to the other deaths: visibility issues (vegetation obscuring vision of pedestrian and driver and bad weather); the pedestrian was vision impaired; and pedestrian misjudgement. Two other pedestrians were hit during uncontrolled crossings when they unexpectedly turned back into the path of vehicles. A further seven fatalities at uncontrolled crossings happened when the pedestrian emerged through parked or stationary vehicles into the path of moving vehicles. Crossing road at controlled crossings Of the 16 fatalities (13% of all pedestrian fatalities) that happened on controlled crossings, seven occurred when the pedestrian was crossing illegally against a red light and one other when the pedestrian was using a non-operational children’s crossing. Of the six fatalities that occurred when the pedestrian was crossing with the green light, three people were killed by speeding vehicles that were driven/ridden through the red light, one by a vehicle turning right onto a highway when the driver failed to see the pedestrian on the crossing, and two when the driver was distracted at the time of the crash. Two other deaths occurred on controlled crossings with no information given on the light cycle and sparse information on the circumstances. VICTORIAN INJURY SURVEILLANCE UNIT Pedestrian hit by reversing vehicles Seven pedestrians (6% of fatalities), including one person riding a mobility scooter, were killed by reversing vehicles, five by vehicles backing out of driveways and two by vehicles backing on the roadway. Pedestrian on footpath, kerb, traffic island or verge hit by vehicle Eleven pedestrians (9% of fatalities) were killed by vehicles that left the road and crashed into them either when they were walking on a footpath or the verge of a roadway (not on the road), standing on a kerb or traffic island, or sitting on outdoor seating of a cafe. Dangerous/erratic driving (due to speeding) and driver error caused most of these crashes. Pedestrian hit when lying, standing, walking or stepping/jumping on road Twenty-three deaths (19% of all pedestrian fatalities) occurred when the victim was lying, standing, walking on the road or jumped/ stepped unexpectedly onto the road. Nine of the 10 pedestrians killed when lying or standing on the road were highly intoxicated, five by alcohol alone and four by a combination of alcohol and other drugs. Eleven pedestrians were walking on the road when killed, most commonly on rural roads. Seven of these were under the influence of alcohol or a combination of alcohol and drugs and in two further cases the driver was highly intoxicated and lost control of the vehicle. Other contributory factors mentioned in reports on these crashes included mental illness/impairment, wearing dark clothing when walking on poorly lit roads, walking with back to traffic and lack of care when walking in a group (stepping out onto road). HAZARD 72 page 6 Person attending to broken down vehicles Three people (2.5% of fatalities) were killed when attending to broken down vehicles on the road either by being crushed or run over. Mobility device users Three fatalities involved persons using mobility devices (2.5% of fatalities), two when driving mobility scooters unsafely. Pedestrian’s point of fatal impact with vehicle Frontal impact collisions were most common (n=90, 75%). There were no further details of point/s of impact in 82% of these cases, but in 18% (n=16) it was reported that the pedestrian impacted with the windscreen. In 11% of cases (n=13) the point of impact was the wheel or undercarriage, and in 8% of cases (n=10) the pedestrian was struck by the rear end of the vehicle. 3.3.5 Crash environment Type of road Forty percent (n=48) of pedestrian fatalities occurred on urban arterial roads, 26% (n=31) on rural roads and 23% (n=27) on highways or freeways. Fifty-nine percent (n=16) of pedestrian fatalities that occurred on highways/freeways were on urban highways/ freeways. Proximity to an intersection Fifty-seven percent (n=68) of pedestrian fatalities occurred mid-block (i.e. between intersections), while 13% (n=16) occurred at intersections and 6% (n=7) occurred on driveways (outside the fence line of a residence) or laneways. Weather conditions Weather conditions at the time of the crash were inconsistently reported on the NCIS with no information given for 65% (n=78) of cases. In the one-third of fatalities (n=42) for which information was available, 74% (n=31) occurred in fine weather compared with 26% (n=11) in rain, fog or other adverse conditions. Light level Fifty-nine pedestrian fatalities (49%) occurred in daytime. There was no information on lighting in 30 of the 61 fatalities (51%) that occurred at night, dawn or dusk. Of the remainder, 13 (11% of all fatalities) occurred on roads where there was no street lighting, 13 (11%) occurred on roads with poor street lighting and 5 (4%) occurred on roads with good street lighting. Table 5 Pedestrian road manoeuvre at the time of the crash ROAD MANOEUVRE N 1. Pedestrian crossing road • At uncontrolled crossing from kerb/median % 67 55.8 44 36.7 7 5.8 16 13.3 – pedestrian hit by vehicle on far side of road from kerb/median (15) – pedestrian hit by vehicle on near side of road from kerb/median (15) – pedestrian hit by vehicle, no information on side (12) – pedestrian hit by vehicle when unexpectedly turned back into path of vehicle (2) • At uncontrolled crossing through parked or stationary vehicles or after alighting from vehicle – collision on near side of road after a person emerged from in front of or behind vehicle at the kerb or on far side when person emerged into lane of moving traffic from between stationary traffic (4) – after alighting from vehicle (2) – other (1) • At controlled crossing from kerb/median – ran/walked across road against red pedestrian light (7) – crossing with green pedestrian light when hit by vehicle (6) – other/no information on light cycle (3) 2. Pedestrian hit by reversing vehicle 7 • Collision involving vehicle reversing out of driveway 5 4.2 • Collision involving vehicle reversing on road 2 1.7 3. Pedestrian on footpath/verge hit by vehicle when vehicle left road 11 • Person on footpath or pedestrian island when vehicle left road and crashed into person 5 4.2 • Person walking on verge of road (no footpath) when vehicle left road and crashed into person 6 5.0 4. Collision involving person walking, lying or standing on road or jumping onto road when hit by vehicle 5.8 9.2 23 19.2 • Person walking on the road when hit by vehicle 11 9.2 • Person standing on road when hit by vehicle 5 4.2 • Person walking on road when hit by vehicle 5 4.2 • Person stepped/jumped onto road in front of vehicle 2 1.7 5. Prior vehicle occupant or mechanic struck when attending vehicle at roadside (or run over by vehicle being attended) 3 2.5 6. Person using mobility device/walking aid struck by vehicle 3 2.5 6 5.0 • Person on mobility scooter driving unsafely (2) • other (1) 7. Other TOTAL VICTORIAN INJURY SURVEILLANCE UNIT 120 HAZARD 72 100 page 7 3.3.6 Contributory factors: top 5 in detail This information was primarily drawn from the Coroner’s Record of the Investigation into the Death. Police reports were consulted in a small number of cases where the Coroners’ Records lacked information. No contributory factors were recorded in nine cases. Up to three factors were recorded per case in the other 111 cases. In total 152 contributory factors were recorded (mean: 1.4; range 1-3 factors). The contributory factors to pedestrian fatalities were (in rank order): pedestrians’ unsafe road use behaviour or failure to observe/misjudgements of traffic (implicated in 51 pedestrian deaths); drivers’ unsafe or dangerous behaviour (32 deaths); pedestrians’ use of alcohol and/or drugs (31 deaths); poor visibility/poor conspicuity of pedestrians (23 deaths); medical or health condition of pedestrians (11 deaths); drivers’ use of alcohol – BAC reading above 0.05gm/100ml (5 deaths); driver distraction (4 deaths); lack of awareness by driver and pedestrian (3 deaths); lack of parental supervision of child pedestrians (3 deaths); vehicle faults (3 deaths: faulty handbrake, bald tyres, fuel contamination); and drivers’ health or medical condition (2 deaths). Major factor 1 - Pedestrians’ unsafe road use behaviour (implicated in 51 deaths) The behaviour of pedestrians at the time of the crash is analysed in detail in 3.3.4. Unsafe pedestrian behaviours mainly involved misjudgements of speed and/or distance of oncoming vehicles and failure to look or observe on-coming vehicles when crossing the road. Reckless road crossing behaviours included crossing either between stationary or parked vehicles without keeping a proper lookout and running across the road including arterial roads and multi-lane highways. Major factor 2 - Drivers’ unsafe or dangerous behaviour including driver distraction and lack of awareness (implicated in 32 deaths) Driving at excess speed (above speed limit or too fast for safe performance of driving task) was the major driver-related contributory factor to pedestrian deaths (implicated in 11 deaths), followed by lack of general awareness/failure to keep proper lookout especially when reversing (9 deaths); driver distraction e.g., eating, operating vehicle radio controls, texting (6 deaths); and failure to obey traffic signals (4 deaths). Driving operational errors caused three crashes and loss of control of vehicle (no other details) another two. Unlicensed driving only contributed to one death. Drivers’ use of alcohol In addition, drivers’ use of alcohol was a factor in 5 deaths; 4 of the 5 drivers having a BAC of 0.05gm/100ml and higher. Major factor 3 - Pedestrians’ alcohol and other drug misuse (implicated in 31 deaths) Alcohol Toxicology findings were available for 99 of the 120 pedestrian fatalities. Twenty-seven pedestrians (27% of fatal cases with toxicology findings) had BAC readings of 0.05 gm/100ml or greater. Most of these pedestrians (74%, n=20) had readings of 0.15 gm/100ml and above. Figure 6 Figure 6 shows BAC level by gender. Overall, 22 males (37% of the 60 males with toxicology reports) had a BAC level of 0.05 gm/100ml or greater, 73% (n=16) of whom had a BAC of 0.15 gm/100ml or greater. By contrast, only 13% (n=5) of the 39 females with toxicology reports available had a BAC level of 0.05gm/100ml and above, but four of these cases (80%) had BAC readings of 0.15 gm/100ml and above. Of the 27 pedestrian fatalities with BAC readings of 0.05 gm/100ml or greater, 41% (n=11) were aged 30-44 years, 30% (n=8) were aged 15-29, 19% (n=5) were aged 4559, 7% (n=2) were aged 75 years and older and 4% (n=1) was aged 60-74 years. Usage rate at 0.05gm/100mg and above was lowest in the oldest age group with alcohol use detected at this level in only two of the 41 deceased pedestrians aged 75 years or older (5%). Of the 20 cases with a BAC reading of 0.15 gm/100ml or greater, 50% (n=10) were aged 30-44 years, 30% (n=6) were aged 15-29, 15% (n=3) were aged 45-59 and 5% (n=1) was aged 60-74 years. The coroners’ reports provided information on where 12 of these highly intoxicated pedestrians had been drinking prior to the crash. Five were killed after drinking at pubs and/or clubs, four at celebrations (weddings and parties) in public halls/reception places and three after social drinking in other settings. Blood Alcohol Concentration (BAC) among pedestrian fatalities, Victoria 2006-2008 A small number of deaths (7) were due to illegal road crossing when the pedestrian crossed against the red pedestrian signal or disobeyed traffic signals at an intersection. In a few cases pedestrians ignored controlled crossings nearby and made uncontrolled crossings. Pedestrians hit when lying, standing or walking on the road were mostly under the influence of alcohol and/or other drugs or, in two cases, suffering from a mental illness/ impairment. VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 8 Other drugs ‘Other’ drugs (licit and illicit) were detected in 14% (n=14) of the 99 fatalities with toxicology reports available, however in one case a single licit drug was detected at a level consistent with therapeutic use so was omitted from the analysis. In the 13 remaining cases, ‘other’ drugs were taken in combination or with alcohol. Cannabis was present in 5% (n=5) of deceased pedestrians; all these pedestrians had BAC readings of 0.05 gm/100ml or above. Other illicit drugs such as methamphetamine (speed), methylenedioxymethamphetamine (ecstasy) and methylenedioxyamphetamine (MDA) were present in 3% (n=3) of deceased pedestrians; BAC readings in these pedestrians were all 0.05 gm/100ml and above. Licit drugs (including caffeine, sertraline and diltiazem) used alone or in combination above the therapeutic range were present in 6% (n=6) of deceased pedestrians. Major factor 4 - Poor visibility and/or conspicuity of pedestrian (implicated in 23 deaths) The factors found to have adversely affected the visibility of pedestrians to drivers, often operating in tandem, were: lack of natural light (9 deaths), inclement weather - rain or fog (10 deaths), no or dim street lighting (7 deaths) and obstructions to the sightline between driver and pedestrian, for example trees and shrubs (2 deaths). In 10 of these cases, the dark clothing being worn by the pedestrian was cited as a secondary contributory factor. In one further death the driver was dazzled by headlights from an oncoming vehicle. Major factor 5 - Medical or health condition of pedestrian (implicated in 11 deaths) The medical and health conditions suffered by pedestrians that contributed to their involvement in fatal pedestrian crashes included: hearing and/or sight impairments, mental illness/condition, restricted mobility, hypertension and a ‘medical complaint’, not further specified. Given that around one-third of fatally injured pedestrians were aged 75 years and older it is likely that medical or health conditions are under-reported. 3.3.7 Overall responsibility for crash Analysis of coroners’ findings, and when a formal finding of responsibility was not made, information in the coroners’ investigation report, indicated that the pedestrian was primarily responsible for the fatal crash in 44% of cases, the driver in 25%, both driver Figure 7 Body region injured: traffic-related pedestrian fatalities, Victoria 2006-2008 Source: NCIS (2006-2008) and pedestrian were held equally responsible in one case (0.8%) and another, involving a crane under repair on a roadway, was due to safety systems failure (0.8%). There was no finding with regard to primary responsibility in 32% of cases as causes were either multifactorial or, less commonly, there was a lack of information. In two cases the coroners report was incomplete, but information in the attached police report indicated that the pedestrian bore primary responsibility in one case and the driver in the other. 3.3.8 Nature of injuries to pedestrians Sixty percent (n=72) of pedestrian deaths resulted from multiple injuries, 27% (n=32) were due to severe head injury, and 3% (n=4) to severe head and chest injury. Three percent (n=3) of pedestrians died from the secondary effects of their injuries. (Figure 7). 3.3.9 Place of occurrence of death Over half of pedestrian deaths (n=64, 53%) occurred in hospital, 41% (n=49) occurred before hospitalisation (i.e. at the scene of the crash), and 3% (n=4) occurred during assistance by medical/ambulance officers or in transit to hospital. 4. Discussion An extensive discussion of the pattern of pedestrian injury, risk and protective factors VICTORIAN INJURY SURVEILLANCE UNIT and evidenced-based pedestrian injury countermeasures was included in the last issue of Hazard. The discussion covered both fatalities and hospital-treated injury so only a few additional points will be made here. Similar to the pattern for pedestrian hospitalisations, the number and rate of pedestrian fatalities have declined significantly since the late 1990s, with much of the decrease occurring between 2002 and 2004, attributed to the reduction in default speed limit in 2001 and the strengthened approach to speed enforcement from early 2002. As for hospitalisations, the benefits of these interventions have been absorbed and an increase, then levelling off, of fatalities is evident in 2005 and 2006. As reported in the previous Hazard, trafficrelated pedestrian hospitalisations in 2006-8 peaked in young people aged 15-29 years, although the hospital admissions rate was highest in persons aged 75 years and older followed by persons aged 15-29. By comparison, the current study shows that over the same 3-year period more than one-third of pedestrian fatalities occurred in persons aged 75 years and older with the remaining two-thirds (less six child deaths) fairly evenly spread across adult age groups to age 74 years. Fatality rates increased with age, sharply climbing from age 75 years. The difference in age pattern between hospital admissions and deaths is most likely due to the greater physical vulnerability of older people (including underlying health conditions) that renders them more likely to die of comparable injury than their younger counterparts (Martin et al., 2008). HAZARD 72 page 9 In the previous issue of Hazard we reported that alcohol use was a contributory factor to 12% of pedestrian hospitalisations in Victoria that occurred in 2006-8. We also noted that a recent Australian research study indicates that this figure is a gross underestimate due to poor recording at the hospital level of known alcohol involvement in transport injury hospitalisations (McKenzie et al., 2010). In the current study, toxicology reports were available for 83% of pedestrian fatalities recorded on the NCIS and alcohol use was detected in around one-third of pedestrians with toxicology reports. Twenty-seven percent of deceased pedestrians for whom information on alcohol involvement was available had blood alcohol readings of 0.05gm/100ml or greater, three-quarters of whom were highly intoxicated with readings of 0.15gm/100ml and above. We found that alcohol involvement was low in females and those aged 75 years and older. Twenty of the 27 deceased pedestrian with BAC readings at or above 0.05 were in age group 15-44 years (18 males and two females) and 16 of the 20 who were highly intoxicated (BAC 0.15 and above) were also in this age group (14 males and 2 females). The high involvement of alcohol in male pedestrian deaths was previously reported in an earlier coronial study covering pedestrian deaths that occurred in Australia over the period 19982002 (ASTB, 2003). The current study indicates that priority populations for prevention are older adults and heavy/binge drinkers especially young males. Readers are referred to the last issue of Hazard on hospital-treated pedestrian injury for an extensive discussion of the risk and protective factors for pedestrian injury and evidencebased prevention measures (http://monash. edu.au/muarc/VISU/hazard/Haz71.pdf). This information is summarised in a table appended to this report - see Table A in Appendix 1. A list of the recommended pedestrian safety countermeasures relevant to the safety issues identified by our analysis of Victorian deaths and hospital-treated injury data can be found in Table B, Appendix 2. References Abdel-Aty M, Keller J. Exploring the overall and specific crash severity levels at signalized intersections. Accid Anal Prev. 2005; 37(3): 417-425. Al-Ghamdi AS. Pedestrian-vehicle crashes and analytical techniques for stratified contingency tables. Accid Anal Prev. 2002; 34(2): 205-214. Anderson RW, McLean AJ, Farmer MJ, Lee BH, Brooks CG.Vehicle travel speeds and the incidence of fatal pedestrian crashes. Accid Anal Prev. 1997; 29(5): 667-674. Australian Bureau of Statistics. 9309.0 – Motor Vehicle Cencus, Australia, 31 Mar 2009. Australian Transport Safety Bureau. Road fatalites among older pedestrians. ATSB Monograph 13, Canberra 2002 http:/ www.infrastructure.gov.au/roads/safety/ publications/2002/Ped_Age_2.aspx. Dowloaded 14/04/2010. Australian Transport Safety Bureau. Male pedestrian fatalities. ATSB Monograph 14, Canberra 2003. http:/www.infrastructure.gov.au/roads/ safety/publications/2003/Ped_Male_1. aspx. Dowloaded 14/04/2010. Austroads. Pedestrian and cycling safety – pedestrian crashes at pedestrian facilities. Report No. AP-R156, Austroads, Sydney, 2000. Bartley Consulting Pty Ltd. Walking and cycling census analysis. Consultancy report prepared for the Victorian Department of Transport, Walking and Cycling Branch. September 2008. Beck LF, Paulozzi LJ, Davidson SC. Pedestrian fatalities, Atlanta Metropolitan Statistical Area and United States, 20002004. J Safety Res. 2007; 38(6): 613-616. Bradbury A. Pattern and severity of injury sustained by pedestrians in road traffic accidents with particular reference to the effect of alcohol. Injury.1991; 22(2): 132134. Bungum TJ, Day C, Henry LJ. The association of distraction and caution displayed by pedestrians at a lighted crosswalk. J. Community Health. 2005; 30(4): 269-79. Bunn F, Frost C, Ker K, et al. Area-wide traffic calming for preventing traffic related injuries. Cochrane Database of Systematic Reviews 2003, Issue 1. Art. No.: CD003110. Cairney P, Stephenson W, Macaulay J. Preventing crashes involving intoxicated pedestrians. Stage 2 – An analysis of Australian coronial records, 1999-2001. In: Austroads Research Report AP-R260/04 pp. 63-119. Sydney: Austroads. VICTORIAN INJURY SURVEILLANCE UNIT Chalabi Z, Roberts I, Edwards P, et al.Traffic and the risk of vehicle-related pedestrian injury: a decision analytic support tool. Inj Prev. 2008; 14(3): 196-201. Chang L, Wang H. Analysis of traffic injury severity: An application of non-parametric classification tree techniques. Accid Anal Prev. 2006; 38(5): 1019-1027. Charlton J, Oxley J, Scully J, et al. Selfregulatory driving practices of older drivers in the ACT and NSW. Monash University Accident Research Centre; October 2006. Report No.: 254. www.monash.edu.au/ muarc/reports/muarc254.pdf Chisholm SL, Caird JK, Lockhart J. The effects of practice with MP3 players on driving performance. Accid Anal Prev. 2008; 40(2): 704-713. Clapperton A, Cassell E. The impact of area socioeconomic inequity on serious injury in Victoria. Hazard Edition No 70 Summer 2009/10. Victorian Injury Surveillance Unit. Melbourne. Clifton K, Burnier C, Akar G. Severity of injury resulting from pedestrian-vehicle crashes: What can we learn from examining the built environment? Transp. Res.: Part D: Transport Environ. 2009; 14(6): 425-436. Connelly ML, Conaglen HM, Parsonson BS, et al. Child pedestrian’s crossing gap thresholds. Accid Anal Prev. 1998; 30(4): 443-453. Connelly LB, Supangan R. The economic costs of road traffic crashes: Australia, states and territories. Accid Anal Prev. 2006; 38(6): 1087-1093. Corben B, D’Elia A, Healy DJ. Estimating pedestrian fatal crash risk. In: Proceedings, 2006 Australasian Road Safety Research, Policing and Education Conference. October 2006, Gold Coast, Australia. Corben B.F. Achieving safe traffic environments for pedestrians. Melbourne, Victoria: Monash University, 2007. Thesis. Corben BF, Diamantopoulou K, Mullan N, Mainka B. Environmental countermeasures for alcohol-related pedestrian crashes. Monash University Accident Research Centre; 1996, Report No. 101. Delaney A, Newstead S, Corben B. Outcome evaluation of the effectiveness of the Safe Routes to Schools program. Monash University Accident Research Centre; 2004, Report No. 225. Delaney A, Diamantopoulou K, Cameron M. Strategic principles of drink-driving enforcement. Monash University Accident Research Centre; July 2006. Report No.: 249. www.monash.edu.au/muarc/reports/ muarc249.pdf HAZARD 72 page 10 Demetriades D, Murray J, Martin M, et al. Pedestrians injured by automobiles: relationship of age to injury type and severity. J Am Coll Surg. 2004; 199(3): 382-387. Desapriya E, Subzwari S, Sasges D, et al. Do light truck vehicles (LTV) impose greater risk of pedestrian injury than passenger cars? A meta-analysis and systematic review. Traffic Inj Prev. 2010; 11(1): 48-56. Dobson A, Smith N, McFadden M, et al. In Australia are people born in other countries at higher risk of road trauma than locally born people? Accid Anal Prev. 2004; 36(3): 375-381. Drews FA, Yazdani H, Godfrey CN et al. Text messaging during simulated driving. Hum Factors. 2009; 51(5): 762-70 Duperrex OJM, Roberts IG, BunnF. Safety education of pedestrians for injury prevention. Cochrane Database of Systematic Reviews 2002, Issue 2. Art. No.: CD001531. Durkin MS, Davidson LL, Kuhn L, O’Connor P, Barlow B. Low-income neighborhoods and the risk of severe pediatric injury: a small-area analysis in Northern Manhattan. Am J Public Health. 1994; 84(4): 587-592. Eluru N, Bhat CR, Hensher DA. A mixed generalized ordered response model for examining pedestrian and bicyclist injury severity level in traffic crashes. Accid Anal Prev. 2008; 40(3): 1033-1054. Federal Office of Road Safety (FORS). Pedestrian fatalities in Australia. Monograph 7, Federal Office of Road Safety, Canberra, Australia, 1996. http://www.rsconference. com/pdf/RS07037.pdf?check=1 Fontaine H, Gourlet Y. Fatal pedestrian accidents in France: A typological analysis. Accid Anal Prev. 1997; 29(3): 303-312. Gårder PE. The impact of speed and other variables on pedestrian safety in Maine. Accid Anal Prev. 2004; 36(4): 533-542. Giles-Corti B, Kelty SF, Zubrick et al. Encouraging walking for transport and physical activity in children and adolescents: how important is the built environment? Sports Med. 2009; 39(12): 995-1009. Graham DJ, Stephens DA. Decomposing the impact of deprivation on child pedestrian casualties in England. Accid Anal Prev. 2008; 40(4): 1351-1364. Harkey D, Zegeer C. PEDSAFE: Pedestrian safety guide and countermeasure selection system. Washington D.C., FHWA 2004. Harrison JE & Berry JG. Injury of Aboriginal and Torres Strait Islander people due to transport, 2001–02 to 2005–06. Injury research and statistics series number 46. Cat. no. INJCAT 120. Adelaide: AIHW, 2008 Harruff RC, Avery A, Alter-Pandya AS. Analysis of circumstances and injuries in 217 pedestrian traffic fatalities. Accid Anal Prev. 1998; 30(1): 11-20. Hatfield J, Murphy S. The effects of mobile phone use on pedestrian crossing behaviour at signalized and unsignalized intersections. Accid Anal Prev. 2007;39(1):197-205. Hatfield J, Fernandes R, Soames Job RF, Smith K. Misunderstanding of right-of-way rules at various pedestrian crossing types: observational study and survey. Accid Anal Prev. 2007; 39(4): 833-42. Haworth N, Johnson IR, Vulcan AP. Mid-term review of arrive alive!, Victoria’s road safety strategy 2002-2007, Part 2: Comparison of actual and predicted road trauma reduction of each initiative, Monash University Accident Research Centre, contract report prepared for VicRoads, Victoria, Australia, 2005. Hedelin A, Björnstig U, Brismar B. Trams--a risk factor for pedestrians. Accid Anal Prev. 1996; 28(6): 733-738. Hewson P. Deprived children or deprived neighbourhoods? A public health approach to the investigation of links between deprivation and injury risk with specific reference to road safety in Devn County, UK. BMC Public Health. 2004; May 10;4:15 Hippisley-Cox J, Groom L, Kendrick D, Coupland C, Webber E, Savelyich B. Cross sectional survey of socioeconomic variations in severity and mechanism of childhood injuries in Trent 1992-7. BMJ. 2002; 324(7346): 1132. Holubowycz OT. Age, sex, and blood alcohol concentration of killed and injured pedestrians. Accid Anal Prev. 1995; 27(3): 417-422. Hoareau E, Newstead S, Cameron M. An evaluation of the default 50 km/h speed limit in Victoria. Melbourne: Monash University Accident Research Centre; November 2006. Report No.: 261. www.monash.edu. au/muarc/reports/muarc261.pdf Hosking SG, Young KL, Regan MA. The effects of text messaging on young drivers. Hum Factors. 2009;51(4):582-92. Hotz G, Kennedy A, Lufti K et al. Preventing pediatric pedestrian injuries. J Trauma. 2009;66:1492-1499. Hutchinson TP, Kloeden CN, Lindsay VL. Countermeasures to the problem of accidents to intoxicated pedestrians. J Forensic Leg Med. 2010; 17(3):115-9. Kim JK, Ulfarsson GF, Shankar VN, et al. Age and pedestrian injury severity in motorvehicle crashes: A heteroskedastic logit analysis. Accid Anal Prev. 2008; 40(5): 1695-1702. VICTORIAN INJURY SURVEILLANCE UNIT King MJ, Soole D, Ghafourian A. Illegal pedestrian crossing at signalised intersections: incidence and relative risk. Accid Anal Prev. 2009;41(3):485-90. Kwan I, Mapstone J. Interventions for increasing pedestrian and cyclist visibility for the prevention of death and injuries. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD003438. LaScala EA, Gerber D, Gruenewald PJ. Demographic and environmental correlates of pedestrian injury collisions: a spatial analysis. Accid Anal Prev. 2000; 32(5): 651-658. Lee C, Abdel-Aty M. Comprehensive analysis of vehicle-pedestrian crashes at intersections in Florida. Accid Anal Prev. 2005; 37(4): 775-786. Loo BP, Tsui KL. Pedestrian injuries in an ageing society: insights from hospital trauma registry. J Trauma. 2009; 66(4): 1196-201. Lorenc T, Brunton G, Oliver S et al. Attitudes to walking and cycling among children, young people and parents: a systematic review. J. Epidemiol Community Health 2008; 62: 852-857. Lyons RA, Jones SJ, Deacon T, Heaven M. Socioeconomic variation in injury in children and older people: a population based study. Inj Prev. 2003; 9: 33-37. Mabunda MM, Swart LA, Seedat M. Magnitude and categories of pedestrian fatalities in South Africa. Accid Anal Prev. 2008; 40(2): 586-593. Martin A. Factors influencing fatality and injury severity risk in pedestrian crashes. Report PPR241 Transport Research Laboratory, prepared for TFL, London Road Safety Unit 2006. Martin AJ, Hand EB, Trace F, O’Neill D. Pedestrian fatalities and injuries involving Irish older people. Gerontology 2010;56:266-271. McCartt AT, Hellinga LA, Bratiman KA. Cell phones and driving: review of research. Traffic Inj Prev. 2006; 7(2): 89-106. McEvoy SP, Stevenson MR, McCartt AT, et al. Role of phones in motor vehicle crashes resulting in hospital attendance: a casecrossover study. BMJ. 2005; 331(7514): 428. McKenzie K, Harrison JE, McClure RJ. Identification of alcohol involvement in injury-related hospitalisations using routine data compared to medical record review. Aust NZ J Public Health 2010;34:146-152. Nasar J, Hecht P, Wener R. Mobile telephones, distracted attention, and pedestrian safety. Accid Anal Prev. 2008;40(1):69-75. HAZARD 72 page 11 Olson, R.L., Hanowski, R.J., Hickman, J.S., & Bocanegra, J. Driver Distraction in Commercial Vehicle Operations. FMCSA RRR 09 042. Washington, DC: Federal Motor Carrier Safety Administration. 2009, September. Öström M; Eriksson A. Pedestrian fatalities and alcohol. Accid Anal Prev. 2001; 33(2): 173-180. Oxley J, Fildes B, Ihsen E et al. Differences in traffic judgments between young and old adult pedestrians. Accid anal Prev. 1997; 29(6): 962-971 Oxley JA, Ihsen E, Fildes BN et al. Crossing roads safely: an experimental study of age differences in gap selection by pedestrians. Accid Anal Prev. 2005 Sep; 37(5):962-71. Oxley J, Lenne M, Corben B. The effect of alcohol impairment on road crossing behaviour. Transportation Research Part F: Traffic Psychology and Behaviour 2006; 9(4): 258-268. Oxley JA, Congiu M, Whelan M, D’Elia A, Charlton J. The impacts of functional performance, behaviour and traffic exposure on road-crossing judgements of young children. Annu Proc Assoc Adv Automot Med. 2007; 51: 81-96. Oxley J, Congiu M, Whelan M, D’Elio A, Charlton J. Teaching young children to cross roads safely. Annu Proc Assoc Adv Automot Med. 2008; 52: 215-23. Paulozzi LJ. United States pedestrian fatality rates by vehicle type. Inj Prev. 2005; 11(4): 232-236. Peng RY, Bongard FS. Pedestrian versus motor vehicle accidents: an analysis of 5,000 patients. J Am Coll Surg. 1999; 189(4): 343-348. Pitt R, Guyer B, Hsieh CC, Malek M. The severity of pedestrian injuries in children: An analysis of the Pedestrian Injury Causation Study. Accid Anal Prev. 1990; 22(6): 549-559. Plurad D, Demetriades D, Gruzinski G, et al. Pedestrian injuries: the association of alcohol consumption with the type and severity of injuries and outcomes. J Am Coll Surg. 2006; 202(6): 919-927. Poulos RG, Hayen A, Finch C, Zwi A. Area socioeconomic status and childhood injury morbidity in NSW. Inj Prev. 2007; 13: 322327. Preusser DF, Well JK, Williams AF et al. Pedestrian crashes in Washington, DC and Baltimore. Accid Anal Prev. 2002; 34: 703710. PROMISING Measures for pedestrian safety and mobility problems. Final report of workpackage 1. NTUA National Technical University of Athens, Greece. 2001. http:// ec.europa.eu/transport/roadsafety_library/ publications/promising_deliverable_1.pdf Redelmeier DA, Tibshirani RJ. Association between cellular-telephone calls and motor vehicle collisions. N Engl J Med. 1997; 336(7): 453-458. Retting RA, Ferguson SA, McCartt AT. A review of evidence-based traffic engineering measures designed to reduce pedestrianmotor vehicle crashes. Am J Public Health. 2003;93(9):1456-1463 Rifaat SM, Chin HC. Accident severity analysis using ordered probit model. J Adv Transport. 2007; 41(1): 91-114. Roudsari B, Mock C, Kaufman R.An evaluation of the association between vehicle type and the source and severity of pedestrian injuries. Traffic Inj Prev. 2005; 6(2): 185-192. Roudsari B, Kaufman R, Koepsell T. Turning at intersections and pedestrian injuries. Traffic Inj Prev. 2006; 7(3): 283-289. Ryb GE, Dischinger PC, Kufera JA, et al. Social, behavioral and driving characteristics of injured pedestrians: a comparison with other unintentional trauma patients. Accid Anal Prev. 2007; 39(2): 313318. Sandt L, Zegeer C. Characteristics Related to Midblock Pedestrian—Vehicle Crashes and Potential Treatments. Transport Res Rec. 2006; 1982(1): 113-121. Schwebel DC, McClure LA. Using virtual reality to train children in safe street crossing skills. Inj Prev 2010; 16(1); e1-5. Shults RA, Nichols JL, Dinh-Zarr TB, et al. Effectiveness of primary enforcement safety belt laws and enhanced enforcement of safety belt laws: A summary of the Guide to Community Preventive Services systematic reviews. J Safety Research 2004; 34: 189-196. Small TJ, Sheedy JM, Grabs AJ. Cost, demographics and injury profile of adult pedestrian trauma in inner Sydney. ANZ J. Surg. 2006; 76: 43-47. Starnes MJ, Hadjizacharia P, Chan LS, et al. Automobile versus pedestrian injuries: does gender matter? J Emerg Med. 2008; [Epub ahead of print]. Stavrinos D, Byington KW, Schwebel DC. Effect of cell phone distraction on pediatric pedestrian injury risk. Pediatrics. 2009; 123(2): e179-185. Sze NN, Wong SC. Diagnostic analysis of the logistic model for pedestrian injury severity in traffic crashes. Accid Anal Prev. 2007; 39(6): 1267-1278. Telstra. Telstra, police & NRMA Insurance join forces to target mobile phone use on Australian Roads. Telstra News Release, 2003 www.telstra.com.au/newsroom. VICTORIAN INJURY SURVEILLANCE UNIT Thomson JA, Tolmie AK, Foot HC, Whelan KM, Sarvary P, Morrison S. Influence of virtual reality training on the roadside crossing judgments of child pedestrians. J Exp Psychol Appl. 2005; 11(3): 175-186. Timperio A, Crawford D, Telford A, Salmon J. Perceptions about the local neighbourhood and walking and cycling among children. Prev Med. 2004; 38(1): 39-47. Transport Accident Commission. Pedestrian Statistics. www.tacsafety.com.au/jsp/ content/NavigationController.do?areaID=1 2&tierID=1&navID=57348A10&navLink= null&pageID=149. Accessed 17/6/2010. Unger R, Eder C, Mayr JM, Wernig J. Child pedestrian injuries at tram and bus stops. Injury. 2002; 33(6): 485-488. VicRoads Safety Rules. Mobile phones and Visual Display Units. http:// w w w. v i c r o a d s . v i c . g o v. a u / H o m e / SafetyAndRules/RoadRules/ MobilePhonesandvisualdisplayunits.htm. Accessed 9/6/2010 Violano P, Davis KA, Lane V, Lofthouse R, Carusone C. Establishing an injury prevention program to address pediatric pedestrian collisions. J Trauma Nurs 2009;16(4):216-219 Walkinginfo website (2009). Retrieved 18 September 2009 from: http://www. walkinginfo.org/why/ Yannis, G, Kanellaidis G, Dimitropoulos J, et al. Assessment of pedestrian safety measures in Europe. ITE. 2007; 77(12): 4048. Zajac SS, Ivan JN. Factors influencing injury severity of motor vehicle-crossing pedestrian crashes in rural Connecticut. Accid Anal Prev. 2003; 35(3): 369-379. Zegeer CJ, Stewart RJ, Huang H, et al. Safety effects of marked versus unmarked crosswalks at uncontrolled locations: analysis of pedestrian crashes in 30 cities. Transport Res Rec. 2001; 1773(-1): 56-68. HAZARD 72 page 12 BOX 1 Database and case selection The National Coronial Information System (NCIS) The main source of death data is the NCIS. The NCIS is a national internet based data storage and retrieval system for Australian coronial cases. Details of the data collection system and data fields are available on the NCIS website. www.vifp.monash.edu.au/ncis/. The NCIS was accessed by Angela Clapperton (VISU researcher and co-author of the report) who has a user licence. Case selection For the main analyses, cases were selected from the NCIS. Only ‘closed’ traffic-related pedestrian fatalities were selected, 11 additional traffic-related fatalities were found but excluded as coronial investigations were still open. Cases were selected using the following variables: 1. 2. 3. 4. 5. Case type on completion = death due to external causes Intent type on completion = unintentional Case jurisdiction = Victoria Mechanism of injury = blunt force > transport injury event > pedestrian Case year = 2006-2008 After initial selection, cases were further examined then excluded if the cause of death was recorded as due to: • suicide; • a medical condition; or • a collision with a railway vehicle that occurred off-road OR • if the on-road death of a user of a pedestrian conveyance (mobility scooter, wheelchair, skateboard, inline skates, toy scooter etc.) was due to a fall or other cause unrelated to a collision with a motor vehicle or other form of on-road transport. VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 13 Appendix 1 Table A Common pedestrian safety measures: aim of measure and effectiveness Area Aim of measure Effectiveness Managing Reducing Facilitating Enhancing Increasing Special Safe Low / High cost Vehicle pedestrian pedestrians visibility environment’s road behaviours moderate – High / speeds exposure movements readability users cost – High / moderate moderate effectiveness Engineering Measure effectiveness Sidewalks and walkways 3 3 3 3 Curb ramps 3 3 3 Marked crosswalks and enhancement 3 3 3 3 Transit stop treatment 3 3 3 Roadway lighting improvements 3 3 Pedestrian barriers and fencing 3 3 3 Pedestrian overpass/underpass 3 3 Street furniture/walking environment 3 3 Bicycle lane 3 Roadway narrowing 3 3 3 Lane reduction 3 3 Driveway improvements 3 3 Raised medians 3 3 3 One-way/two-way street conversions 3 3 3 Curb radius reduction 3 3 Improved left-turn slip-lane design 3 3 3 Roundabouts 3 3 Modified T-intersections 3 3 3 Intersection median barriers 3 3 Curb extension 3 3 3 Chokers 3 3 Crossing islands 3 3 Chicanes 3 3 3 3 3 3 3 3 Mini-circles Speed humps Speed tables VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 3 3 page 14 Appendix 1 (cont...) Table A Common pedestrian safety measures: aim of measure and effectiveness Area Aim of measure Effectiveness Managing Reducing Facilitating Enhancing Increasing Special Safe Low / High cost Vehicle pedestrian pedestrians visibility environment’s road behaviours moderate – High / speeds exposure movements readability users cost – High / moderate moderate effectiveness Education Engineering Measure Enforce ment effectiveness Raised intersections 3 3 Raised pedestrian crossings 3 3 3 3 Gateways 3 3 3 Landscaping 3 3 3 Specific pavement treatment 3 3 3 Serpentine design 3 3 Woonert 3 3 3 3 Diverters 3 3 Full street closure 3 3 Partial street closure 3 3 Pedestrian streets/malls 3 3 Traffic signals 3 3 3 Pedestrian signals 3 3 3 Pedestrian signal timing 3 3 3 Traffic signal enhancements 3 3 3 Left-turn-on-red restrictions 3 3 Advanced stop lines 3 3 Signing 3 3 School zone improvement 3 3 3 3 Neighbourhood identity 3 3 Speed-monitoring trailer 3 3 On-street parking enhancements 3 3 Friendly vehicle fronts 3 3 Pedestrian education 3 3 Driver education 3 3 Special group education 3 3 Enforcement 3 3 VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 3 page 15 Appendix 2 Table B Recommended pedestrian safety countermeasures Pedestrian safety issues Recommended pedestrian safety countermeasures POPULATION GROUPS • Refuge islands to make crossing task easy for the elderly • More elderly-friendly footpaths and crossings • Changing behaviour of younger drivers toward the elderly • Traffic safety education • Providing more pedestrian crossings • Longer green light cycles Elderly pedestrians Adolescents and young adults (15-29) • Traffic calming measures in residential areas • Traffic safety education (see below for alcohol/drug users) Heavy or binge users of alcohol and/ or drugs • Traffic restraints such as street closures in high-alcohol-consumption areas during high-alcohol hours • Side-walk barriers to deter pedestrians from jay-walking or exiting pubs/clubs directly onto road • All-red signal design for intersections located near to licensed alcohol dealers • More alcohol sobriety checks and testing • Installing more alcohol-testing devices in premises alcohol is served • Improved provision of night-time public transport or taxi services especially in rural areas Persons born in non-English speaking countries, tourists and visitors • Provide educational material (leaflets and posters) in English and main languages of visitors at entry points to Victoria such as airports, visitor information centres at state borders, main train stations and tourist accommodation • Provide education and training in road crossing behaviour for new arrivals (students and migrants) • Improve signings and markings to increase the readability of the environment Students and children • Traffic calming measures in residential areas and around schools • School crossing patrol • Close supervision of children in vicinity of roads • Traffic safety education and training • 30 km/hr speed zones in high pedestrian areas CRASH TYPE ‘Crossing the road’ crashes VICTORIAN INJURY SURVEILLANCE UNIT • Relocate bus/tram stops where warranted • Improve/add night time lighting • Install overpass or underpass • Install medians or pedestrian crossing islands • Provide curb extensions at intersections or midblock to improve direct line of sight between vehicle and pedestrian • Apply traffic calming measures • Provide staggered crosswalk through the median • Install midblock traffic signal with pedestrian signals, if warranted • Adjust school district boundaries • Use speed-monitoring trailer • Enforce speed limits, pedestrian ordinances • Reduce road width • Narrow travel lanes HAZARD 72 page 16 Appendix 2 (cont...) Table B Recommended pedestrian safety countermeasures Pedestrian safety issues Recommended pedestrian safety countermeasures Speeding and high-impact speed crashes • Modern roundabouts • Speed-limiters in vehicles • Anti-skid road surfaces and anti–skid technologies for vehicles • Equipping vehicles with intelligent pedestrian-detectors • 30 km/hr speed zones in high pedestrian areas • Police enforcement and speed cameras Visibility and conpiscuity–related crashes • Signing and pedestrian marking • Pedestrian zones and streets • Providing good street lighting • Special lighting at pedestrian crossings and intersections • Removing visual obstacles • Pedestrian wearing conspicuous clothing (retroreflective jackets bands) ‘Trapped pedestrians’ crashes • Relocate bus stop to far side of crossing area • Improve roadway lighting • Provide midblock or intersection curb extensions • Install traffic calming devices such as speed tables or raised pedestrian crossings on local and neighborhood streets • Provide raised crosswalks to improve pedestrian visibility • Install traffic signals if warranted, including pedestrian signals • Install flashers or advance warning signs • Recess stop lines • Install barriers or signs to prohibit crossings and direct pedestrians to safer crossing locations nearby • Enforce crosswalk laws ‘Emerging from between cars’ or ‘dart-out’ crashes • Provide good nighttime lighting • Add on-street bike lanes • Narrow travel lanes • Provide curb extensions • Install spot street narrowing at high midblock-crossing locations • Implement traffic-calming measures such as chicanes, speed humps, or speed tables • Provide raised pedestrian crossings • Design gateway to alert motorists that they are entering neighborhood with high level of pedestrian activity • Convert street to driveway link/serpentine, woonerf, or a pedestrian street • Install street diverters or full/partial street closures at selected intersections • Provide adult crossing guard (in school zone) • Remove or restrict on-street parking • Educate children about safe crossing behavior and adults about speeding ‘Hit while walking on the road’ crashes • Provide walkable sidewalks • Provide safer routes to schools • Provide better street lighting • Use barriers to keep pedestrians off the road • Improve public transport and taxi services at night especially in rural areas VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 17 Appendix 2 (cont...) Table B Recommended pedestrian safety countermeasures Pedestrian safety issues Recommended pedestrian safety countermeasures ‘Hit on driveway’ crashes • Provide sidewalk or walkway • Maintain level sidewalks across driveways or alleys • Provide clear walking path across driveway • Remove unneeded driveways and alleys • Remove sight obstructions (e.g., trim hedges or lower fencing) • Narrow driveways and reduce turning radii • Add adequate planting strip or sidewalk separation • Provide advance warning signs for drivers ‘Reversing car’ crashes • Provide clearly delineated walkways for pedestrians in parking Lots • Relocate pedestrian walkways • Improve night time lighting • Remove unneeded driveways and alleys • Remove landscaping or other sight obstruction near driveways • Provide curb extensions or raised pedestrian crossings to improve the visibility of pedestrians to backing motorists • Eliminate, modify, or relocate parking if feasible • Enhance pedestrian education • Enhance driver education • Provide auditory backing alert on vehicle. ‘Playing or working on the road’ crashes • Provide accessible sidewalks or walkways on both sides of street • Improve street lighting • Introduce traffic-calming measures (e.g., street narrowing, speed humps) • Convert streets to a woonerf or use signs to identify neighborhood as area with high levels of pedestrian activity • Consider street closures (full or partial) or use diverters • Implement pedestrian and motorist education programs • Provide community park/playground • Improve lighting around workers and wearing of retroreflective garments by workers • Improve traffic control measures (e.g., signs, markings, cones, barricades, and flashers) warning motorists of workers’ presence • Increase worker safety training • Increase police enforcement of speed limits in work zones • Provide better physical separation/protection of worksite from motor vehicles ‘Hit while boarding/alighting’ crashes • Improve road lighting • Restrict on-street parking near bus/tram stops Heavy (bus, truck, tram etc.) and semi-heavy (light trucks and 4WD vehicles) vehicle-related crashes • Pedestrian-friendly vehicle front design (applicable to all vehicle fleet), e.g. removing roo-bars from the front of heavy and semi-heavy vehicles transiting in cities • Heavy vehicle ban in high-pedestrian zones Motorcycles and bicycle–related crashes • Bike lanes • Improved signage and centre line marking on shared pathways VICTORIAN INJURY SURVEILLANCE UNIT HAZARD 72 page 18 - INDEX Subject.....................................................Edition Asphyxia..............................................................................................60 Babywalkers, update.............................................................16,20,25,34 Baseball................................................................................................30 Boating-related recreational injury.....................................................56 Bunkbeds.............................................................................................11 Bicycles - Bicycle related..................................................6,31,34,44,65 - Cyclist head injury study......................................................2,7,8,10 Burns - Scalds, Burns prevention.................................................3,12,25 - Unintentional burns and scalds in vulnerable populations...........57 Child care settings................................................................................16 Client survey results.............................................................................28 Cutting and piercing (unintentional) assaultive.............................52, 55 Data base use, interpretation & example of form..................................2 Deaths from injury (Victoria)..........................................................11,38 Dishwasher machine detergents - Update............................................18 DIY maintenance injuries....................................................................41 Dog bites, dog related injuries......................................3,12,25,26,34,69 Domestic architectural glass........................................................7,22,25 Domestic Violence..........................................................................21,30 Drowning/near drowning, including updates....................2,5,7,30,34,55 Elastic luggage straps...........................................................................43 Escalator...............................................................................................24 Exercise bicycles, update....................................................................5,9 Falls - Child, Older Persons, Home......................................44,45,48,59 Farm, Tractors..................................................................30,33,24,47,68 Finger jam (hand entrapment)..........................................10,14,16,25,59 Fireworks.............................................................................................47 Geographic regions of injury...............................................................46 Home....................................................................................14,32,59,65 Horse related.....................................................................................7,23 Infants - injuries in the first year of life.................................................8 Injury surveillance developments, inc. ICD10 coding....................30,43 Intentional............................................................................................13 Latrobe Valley - First 3 months, Injury surveillance & prevention ....................................................................9, March 1992, Feb 1994 VICTORIAN INJURY SURVEILLANCE UNIT Ladders.................................................................................................63 Lawn mowers.......................................................................................22 Marine animals.....................................................................................56 Martial arts...........................................................................................11 Mobility scooters.................................................................................62 Motor vehicle related, non-traffic, vehicle jack injuires.................20,63 Motorcycles.....................................................................................64,65 Needlestick injuries....................................................................11,17,25 Nursery furniture.............................................................................37,44 Older people.........................................................................................19 Off-street parking areas........................................................................20 Pedestrians......................................................................................71,72 Playground equipment...................................3,10,14,16,25,29,44,61,65 Poisons - Domestic chemical and plant poisoning..............................28 - Drug safety and poisons control......................................................4 - Dishwasher detergent, update.....................................................10,6 - Early Childhood, Child Resistant Closures...........................27,2,47 - Adult overview...............................................................................39 Power saws, Chainsaws..................................................................22,28 Roller Blades, Skateboards..................................................2,5,25,31,44 School..................................................................................................10 Shopping trolleys.......................................................................22,25,42 Smoking-related....................................................................21,25,29,44 Socio-economic status and injury..................................................49, 70 Sports - child sports, adult sports, surf sports, snow sports............................................................8,9,44,15,51,56,66 Suicide - motor vehicle exhaust gas......................................11,20,25,41 Trail bikes............................................................................................31 Trampolines...............................................................................13,42,61 Trends in road traffic fatality and injury in Victoria.......................36,65 Vapouriser units...................................................................................43 Venomous bites and stings...................................................................35 VISS: How it works, progress, A decade of Victorian injury surveillance..............................................................................1,26,40 VISAR: Celebration of VISAR’s achievements, VISAR name change to VISU....................................................50,61 Work-related..............................................................................17,18,58 HAZARD 72 page 19 Acknowledgements Contact VISU at: Guest Editors MUARC - Accident Research Centre Building 70 Monash University Victoria, 3800 VISU Staff Phone: Enquiries (03) 9905 1805 Co-ordinator (03) 9905 1805 Director (03) 9905 1857 Fax (03) 9905 1809 Email: visu.enquire@monash.edu Dr Jennie Oxley, Monash University Accident Research Centre (MUARC) Ms Jessica Pearce, National Coroners Information System (NCIS) Director: Research Fellows: Research Officers: Ms Erin Cassell Ms Karen Ashby Ms Angela Clapperton Mr Nicholas Reid Ms Emily Kerr Participating hospitals From October 1995 Austin & Repatriation Medical Centre Ballarat Base Hospital The Bendigo Hospital Campus Box Hill Hospital Echuca Base Hospital The Geelong Hospital Goulburn Valley Base Hospital Maroondah Hospital Mildura Base Hospital The Northern Hospital Royal Children’s Hospital St Vincents Public Hospital Wangaratta Base Hospital Warrnambool & District Base Hospital Western Hospital - Footscray Western Hospital - Sunshine Williamstown Hospital Wimmera Base Hospital From November 1995 Dandenong Hospital From December 1995 Royal Victorian Eye & Ear Hospital Frankston Hospital From January 1996 Latrobe Regional Hospital From July 1996 Alfred Hospital Monash Medical Centre From September 1996 Angliss Hospital From January 1997 Royal Melbourne Hospital All issues of Hazard and other information and publications of the Monash University Accident Research Centre can be found on our internet home page: www.monash.edu.au/muarc/visu From January 1999 Werribee Mercy Hospital From December 2000 Rosebud Hospital From January 2004 Bairnsdale Hospital Central Gippsland Health Service (Sale) Hamilton Base Hospital Royal Women’s Hospital Sandringham & District Hospital Swan Hill Hospital West Gippsland Hospital (Warragul) Wodonga Regional Health Group VISU is a project of the Monash University Accident Research Centre, funded by the Department of Health Hazard was produced by the From April 2005 Casey Hospital How to access VISU data: VISU collects and analyses information on injury problems to underpin the development of prevention strategies and their implementation. VISU analyses are publicly available for teaching, research and prevention purposes. Requests for information should be directed to the VISU Co-ordinator or the Director by contacting them at the VISU office. VICTORIAN INJURY SURVEILLANCE UNIT Victorian Injury Surveillance Unit (VISU) Illustrations by Debbie Mourtzios ISSN-1320-0593 Printed by Work & Turner Pty Ltd, Tullamarine Layout by Inspired by Graphics, Caroline Springs HAZARD 72 page 20