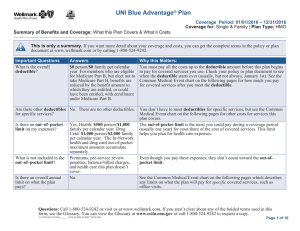
Summary of Benefits and Coverage: Coverage for: Coverage Period: 01/01/2014 - 12/31/2014
advertisement

Coverage Period: 01/01/2014 - 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs In-Network Provider $0 copay $0 copay $0 copay $0 copay Out-of-Network Provider 20% coinsurance 20% coinsurance 20% coinsurance Same as In-Network Bone Mass Measurement Exam Breast Screening/Mammography Cardia Rehab/Intensive Cardiac Rehab Cardiovascular Disease Testing Cardiovascular Disease Therapy $0 copay $0 copay $0 copay $15 copay $0 copay $0 copay 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance Cervical Cancer Screening $0 copay 20% coinsurance Chemotherapy Drugs Chemotherapy Services Chiropractic Services Colorectal Screenings Complex Radiology Depression Screening Diabetes Screening Diabetes Supplies and Self-monitoring Training $0 copay $0 copay $10 copay $0 copay $0 copay $0 copay $0 copay 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance $0 copay 20% coinsurance Dialysis $0 copay Services You May Need Abdominal Screening Allergy Immunotherapy Allergy Testing Ambulance Annual Wellness Visit/Routine Physical Examination QM87- Drexel Coverage for: Group | Plan Type: PPO Limitations & Exceptions none none none Non-emergent requires prior authorization. You are covered up to 1 exam every year. none none none none none You pay $0 for each additional Pap Smear and Pelvic Exam up to 1 Pap Smear(s) and Pelvic Exam(s) every two years. Prior authorization is required for certain Part B injectable drugs when administered in a physician's office or outpatient setting. none none none none none none none If dialysis is performed at the PCP or Specialist office Same as In-Network setting, only the dialysis copayment will apply. Coverage Period: 01/01/2014 - 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Durable Medical Equipme Services You May Need In-Network Provider Disease Management Durable Medical Equipment EKG Screening $0 copay $0 copay Emergency Care $40 copay Fitness Center Glaucoma Screening Hearing Services-Hearing Aids Hearing Services-Medicare Covered Hearing Exam Hearing Services-Non-Medicare Covered Home Health Care Hospice Human Immunodeficiency Virus (HIV) Screening Immunizations (influenza vaccine, Hepatitis B vaccine, Pneumonia vaccine $0 copay Non-covered Services QM87- Drexel Out-of-Network Provider Limitations & Exceptions Refer to your Evidence of Coverage for Benefit Information. none Covered annually with routine physical exam. N/A 20% coinsurance 20% coinsurance Services performed in the U.S. will be covered same as (innetwork) Copay waived if admitted Receive a basic fitness membership to a participating facility. N/A 20% coinsurance none N/A Covered up to $500 for hearing aids every three years $15 copay 20% coinsurance Non-covered Service N/A $0 copay 20% coinsurance Same as In-Network none none none Covered in full at a Medicare Certified Hospice. $0 copay 20% coinsurance none $0 copay $0 [visits 1-90] 20% coinsurance none 20% coinsurance You are covered for unlimited days each benefit period 190 Day Lifetime Maximum includes Mental Health and Substance Abuse Treatment received in a Medicare Approved Mental Health Facility. Inpatient Hospital Care Inpatient Mental Health/Substance Abuse Facility Days Coverage for: Group | Plan Type: PPO $0 [visits 1-90] 20% coinsurance Coverage Period: 01/01/2014 - 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Durable Medical Equipme Services You May Need Medical Nutrition Therapy Medicare Part B Drugs Obesity Screening/Therapy Outpatient Diagnostic Procedures/Lab Outpatient Mental-Psychiatric Services Outpatient Occupational Therapy Outpatient Physical Therapy Outpatient Speech Language Outpatient Substance Abuse Outpatient Surgery-Ambulatory Surgical Center Outpatient Surgery-Outpatient Hospital Partial Hospitalization Includes Intensive Outpatient Programs In-Network Provider Out-of-Network Provider Limitations & Exceptions $0 copay $0 copay $0 copay $0 copay $15 copay $15 copay $15 copay $15 copay $15 copay 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance Up to 6 nutrition counseling sessions yearly with an in-network doctor or registered dietician. none none none none none none none none $0 copay $0 copay 20% coinsurance 20% coinsurance none none $15 copay $15 copay $10 copay $0 copay $0 copay $15 copay $0 copay $0 copay 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance none none none none none none none none 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance none none Covers up to six sessions No prior hospitalization required. none Podiatry Services Primary Care Office Visit Prostate Cancer Screenings Prosthetics Pulmonary Rehab Radiation Therapy Routine Radiology Screening Sexually Transmitted Infections Counseling $0 copay Screening/Counseling Alcohol Misuse $0 copay Services Kidney Disease Education $0 copay Skilled Nursing Facility $0 [visits 1-100] Smoking Cessation $0 copay QM87- Drexel Coverage for: Group | Plan Type: PPO Coverage Period: 01/01/2014 - 12/31/2014 Summary of Benefits and Coverage: What this Plan Covers & What it Costs In-Network Provider Durable Medical Equipmen Services You May Need Smoking Cessation Program Specialist Office Visit Urgent Care Vision Care-Medicare Covered Vision Care-Non-Medicare Covered Vision Care-Medicare Covered Eye Wear Weight Management Out-of-Network Provider Coverage for: Group | Plan Type: PPO Limitations & Exceptions Up to $200 will be covered as long as there is proof of N/A enrollment. $15 copay 20% coinsurance none Services performed in the U.S. will be covered same as (in$15 copay See below for additional details. network) $15 copay 20% coinsurance none Non-covered services N/A none You are covered for one pair of eyeglasses or contact lenses after each cataract surgery. Access to plan -approved weight manangement programs. N/A IN Network Maximum Out-of-Pocket (MOOP) Combined IN/Out of Network Pocket Maximum Out of Network Deductable $6,700 $10,000 $250.00 * If there is a separate and distinct office visit evaluation and service, a copay will apply. * The copayment amount depends on the provider type. * Worldwide Coverage available. Amounts you pay for Emergency and Urgently needed care services received outside the U.S. do not count toward your maximum out-of-pocket amount (MOOP) * Normal plan rules apply. Please refer to your Evidence of Coverage for more information. * You are covered for each Medicare covered urgently needed care visit. If seeking services from a PCP or Specialist normal cost-share will apply. Outside the U.S. you pay $65.00. QM87- Drexel