In Vitro Study of Cancer Cell Extravasation in Microfluidic
Platform
by
Jessie Sungyan Jeon
S.B., Mechanical Engineering
Massachusetts Institute of Technology, 2008
MASSACHUSETTS ISnE
OF TECHNOLOGY
S.M., Mechanical Engineering
Massachusetts Institute of Technology, 2010
MAY 08 21
Submitted to the Department of Mechanical Engineering
in partial fulfillment of the requirements for the degree of
LIBRARIES
Doctor of Philosophy in Mechanical Engineering
at the
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
February 2014
C 2014 Jessie Sungyun Jeon. All rights reserved
The author hereby grants to MIT and The Charles Stark Draper Laboratory, Inc. permission to reproduce and to distribute
publicly paper and electronic copies of this thesis document in whole or in any part medium now known or hereafter created.
Author...............
..
.. .
.. ... ... ... ... .. ....
... ... . .. ... ... ... ... ... ... ... ... ... ... .. . . ... .
Department of Mechanical Engineering
Jan 14, 2014
V
........................--
Certified by.
Joseph L. Charest
Senior Membmer Technical Staff, Draper Laboratory
Thesis Supervisor
Certified by ..............
..
......
- ---..
.-.-.--........................ ....... ...... ............. .-
-.
.
Roger D. Kamm
Cecil and Ida Green Distinguished Professor of Bioloieil and Mechanical Engineering
ie"sdSuneziawr
Accepted by .....................................
David E. Hardt
Chairman of the Departmental Committee for Graduate Students
In Vitro Study of Cancer Cell Extravasation in
Microfluidic Platform
by
Jessie Sungyun Jeon
Submitted to the Department of Mechanical Engineering
on Jan 14, 2014 in partial fulfillment of the
requirements for the degree of
Doctor of Philosophy in Mechanical Engineering
Abstract
Cancer metastases arise from the cancer cells that disseminate from the primary tumor, intravasate
into the vascular system and eventually transmigrate across the endothelium into to a secondary site
through a process of extravasation. Microfluidic systems have a major advantage in studying cancer
extravasation since they can mimic aspects of the 3D in vivo situation in a controlled environment
while simultaneously providing in situ imaging capabilities for visualization, thereby enabling
quantification of cell-cell and cell-matrix interactions. Moreover, microfluidics enable parametric
study of multiple factors in controlled and repeatable conditions.
This thesis describes novel 3D microfluidic models to mimic the tumor microenvironment and
vasculature during cancer cell extravasation in order to investigate the critical steps of extravasation.
First, a general non-organ-specific cancer cell extravasation model is developed in which the
endothelial cells that cover the walls of the microfluidic channel represent the vessel endothelium,
and the entire extravasation process including tumor cell adhesion to the endothelium and
subsequent transmigration can be observed. A second model is then introduced to mimic organspecific extravasation and investigate the preference of certain types of cancer to target specific
organs for metastass. The improved model was used to study the specificity of human breast cancer
metastases to bone, by recreating a vascularized bone-mimicking microenvironment. The tri-culture
system allowed us to study the transendothelial migration of highly metastatic breast cancer cells
2
and to monitor their behavior within the bone-like matrix. Next, functional microvascular networks
were generated in the microfluidic system through vasculogenesis with addition of mural cells and
pro-angiogenic factors to better replicate the normal physiological vasculature of the remote site for
metastasis. Lastly, the vasculogenesis approach was combined with the bone-mimicking model to
develop a functional osteo-cell conditioned vasculature model to study physiologically relevant
extravasation in a bone-like microenvironment. In addition to the quantification of extravasation
rates and subsequent tumor cell migration into the model tissue, the vascular networks were
characterized by measuring permeability, and immunostaining of proteins secreted by osteo-cell and
mural cell markers confirmed the creation of microenvironments and the presence of multiple cell
types within the matrix.
This study provides novel 3D in vitro quantitative data on cancer cell extravasation and
micrometastasis of breast cancer cells within a bone-mimicking microenvironment. The developed
microfluidic system represents an advanced in vitro model to study complex biological phenomena
such as extravasation involving functional microvascular networks under organ-specific conditions
and demonstrates the potential value of microfluidic technologies to better understand cancer
biology and screen for new therapeutics.
Thesis Supervisor: Joseph L. Charest
Title: Senior Member Technical Staff, Draper Laboratory
Thesis Supervisor: Roger D. Kamm
Title: Cecil and Ida Green Distinguished Professor of Biological and Mechanical Engineering
31
Acknowledgment
I would like to express my deepest gratitude to people who had shaped me over the years while I
was pursuing PhD. First, I am exceptionally thankful to my advisor Prof. Roger Kamm. I do not
think my experience as a graduate student would have been as fruitful or enjoyable as it had been
without Roger's dedicated guidance and support. His gentle and thoughtful but keen advice allowed
me to constantly motivate myself over the years and encouraged me to be independent not only in
work environment, but also in everything else I engage. Roger has been the example of what a true
scholar and mentor should be, and I am really fortunate to have him as my academic and research
advisor.
I am very grateful to my committee members, Prof. Richard Hynes, Prof. Rohit Karnik, and Dr.
Joseph Charest, whom all provided me with enormous constructive feedbacks and professional
support. I would also like to thank all previous and current Kammster for many helps and sharing
all moments, whether wonderful or tough, together, in lab.
I am also thankful to all my friends. As much as I love MIT, it is also inevitably a greatly
challenging place to be, and I would have never survived nearly a decade of MIT life without
support from friends. Particularly, friends in KSGAME have been a family away from home, and
have been an immense help personally as well as academically. I'm grateful that friends from
church for providing me spiritual support. Moreover, in fellowship with them, I have learned to
share love, joy and passion in Jesus.
Finally, I would like to thank my parents, who have always given me never-ending love and
support.
The project described in this thesis was supported by Draper Internal Research and Deveolopment
(IRAD) funds, Repligen Fellowship in Cancer Research, and also by NIH Award Number R33
CA174550-01 R21 CA140096-01 from the National Cancer Institute. The content is solely the
responsibility of the author and does not necessarily represent the official views of the National
Cancer Institute or the National Institute of Health.
4
Table of Contents
1. Introduction ....................................................................................................................
1. 1. Cancer cell extravasation and microfluidics ...................................................................
1. 1. 1. Cancer cell odyssey in the metastatic cascade ...................................................
13
13
14
1. 1. 2. In vivo and in vitro cancer models for invasion, migration, extravasation and
colonization.................................................................................................
1. 1. 3. M icrofluidic tools for in vitro cancer models ...................................................
17
18
1. 1. 4. Targeting cancer cell extravasation: in vitro and in vivo drug screening models to
block the metastatic cascade .......................................................................
1. 2 M icrofluidic platforms for angiogenesis and vasculogenesis ..........................................
23
28
1. 2. 1. M imicking angiogenesis in microfluidics ..........................................................
30
1. 2. 2. Inducing angio/vasculogenesis..........................................................................
34
1. 2. 2. 1 Chemical factors .........................................................................
34
1. 2. 2. 2 M echanical factors .......................................................................
35
1. 2. 2. 3 M icro-environmental factors........................................................
36
1. 2. 3. Co-culture methods ............................................................................................
37
1. 2. 3. 1 Co-culturing in microfluidic platform ...........................................
37
1. 2. 3. 2 Tumor angiogenesis model ..........................................................
37
1. 2. 4. M aturation/sabilization of blood vessels..........................................................
39
1. 3. Pros and cons of microfluidics........................................................................................
41
1. 4. Thesis overview ..................................................................................................................
42
2. In vitro m odel of tum or cell extravasation...............................................................
51
2 . 1. In tro du ction .........................................................................................................................
53
2. 2. M aterials and methods ..................................................................................................
53
2. 2. 1. M icrofluidic system ...........................................................................................
53
2. 2. 2. Cell culture and cell selection ............................................................................
55
2. 2. 3. Permeability of endothelial monolayer ..............................................................
56
2. 2. 4. Immunofluorescent staining and image acquisition...........................................
57
5
2. 2. 5. M etrics for extravasation...................................................................................
58
2. 2. 6. Statistics .................................................................................................................
58
2. 3. Results and dicussion .....................................................................................................
59
2. 3. 1. M odeling the extravasation process ...................................................................
59
2. 3. 2. Confirmation of endothelial layer integrity........................................................
59
2. 3. 3. Optimization of tumor cell seeding...................................................................
61
2. 3. 4. Extravasation.....................................................................................................
63
2. 3. 5. Beyond extravsation..........................................................................................
68
3. 3D in vitro model for specificity of breast cancer metastasis to bone...........73
3. 1. Introduction.........................................................................................................................73
3. 2. M aterials and methods ..................................................................................................
75
3. 2. 1. M icrofluidic system ...........................................................................................
75
3. 2. 2. Cell culture .............................................................................................................
77
3. 2. 3. Immunofluorescent staining...............................................................................
78
3. 2. 4. Conditioned assays: addition of CXCL5 and CXCR2 blocking agent ..............
79
3. 2. 5. Extravasation and micrometastasis metrics .......................................................
80
3. 3. Results and discussion ....................................................................................................
3. 3. 1. Generation of the osteo-cell conditioned microenvironment.............................
80
80
3. 3. 2. Extravasation of cacner cells in the osteo-cell conditioned microenvironment.....81
3. 3. 3. Addition of CXCL5 and anti-CXCR2- effect on extravasation........................
84
3. 3. 4. Formation of micrometastases .........................................................................
86
3. 4. Appendix .............................................................................................................................
3. 4. 1. Generation of the osteo-cell conditioned microenvironment.............................
88
88
3. 4. 2. Extravasation of cacner cells in the osteo-cell conditioned microenvironment.....89
3. 4. 3. Addition of CXCL5 and anti-CXCR2- effect on extravasation.........................
89
3. 4. 4. Live/Dead assay ................................................................................................
90
3. 4. 5. Endothelial cell monolayer quality ..................................................................
90
3. 4. 6. Collagen structure ..............................................................................................
91
3. 4. 7. Effect on endothelial monolayer permeablity of cancer cells ............................
91
6
3. 4. 8. Quantification of CXCL5 production -Ensyme-linked immunosorbenet assay
(ELISA) ........................................................................................................
93
3. 4. 9. CXCR2 immunofluorescence ............................................................................
94
3. 4. 10. Quantifying CXCL5 gradient generation within the osteo-cell conditioned
microenvironment - Computational simulations.........................................
3. 4. 11. Statistics
94
.................................................
95
4. Generation of 3D functional microvascular networks with mural cell-differentiated
hum an m esenchym al stem cells.......................................................................................105
4. 1. Introduction.......................................................................................................................105
4. 2. Experimental section.........................................................................................................108
4. 2. 1. M icrofluidic system .............................................................................................
108
4. 2. 2. Cell culture ...........................................................................................................
109
4. 2. 3. Immunofluorescent staining .................................................................................
110
4. 2. 4. Data Analysis .......................................................................................................
111
4. 2. 4. 1 M icrovascular Network M orphology..............................................111
4. 2. 4. 2 Quantification of BM -hM SC differentiation ..................................
112
4. 2. 4. 3 Microvascular network perfusion and permeability quantification 112
4. 2. 4. 4 Statistics ..........................................................................................
4. 3. Results nad discussion ......................................................................................................
113
113
4. 3. 1. Differentiation of BM -hM SCs into mural cells ...................................................
113
4. 3. 2. Generation of microvascular networks ................................................................
116
4 . 4 . A p p en d ix ...........................................................................................................................
12 1
5. Extravasation of cancer cell to bone-mimicking microenvironment in functional 3D
vasculature generated through vasculogenesis ..............................................................
128
5 . 1. Introd uction .......................................................................................................................
12 8
5. 2. M aterials and methods ......................................................................................................
129
5. 2. 1. M icrofluidic system .............................................................................................
129
5. 2. 2. Cell culture and cell selection ..............................................................................
130
7
5. 2. 3. Immunofluorescence and image acquisition........................................................131
5. 2. 4. M etrics for extravasation......................................................................................131
5. 2. 5. Permeability .......................................................................................................
132
5. 2. 6. Flow in vasculature generated..............................................................................132
5 . 2 . 7 . S tatistics ...............................................................................................................
13 3
5. 3. Results and discussions.....................................................................................................133
5. 3. 1. Generation of functional 3D vasculature in bone-mimicking microenvironment
........................................................................................................................
13 3
5. 3. 2. Extravassation of cancer cells in bone-mimicking microenvironment ................ 135
5. 3. 3. Effect of shear stress on vasculature and cacner cell extravsation.......................137
6. Conclusion and O utlook...............................................................................................141
8
List of Figures
Fig 1.1. Schem atic of extravasation cascade.................................................................................
15
Fig 1.2. Microfluidic models for extravasation............................................................................
21
Fig 1.3. In vivo and in vitro models developed for screening drugs acting on extravasation........25
Fig 1.4. A ngiogenic sprouting........................................................................................................
29
Fig 1.5. Exam ples of m icrofluidic platform ...................................................................................
33
Fig 1.6. Co-culture of endothelial cells with tumor cells in microfluidic system ..........................
38
Fig 1.7. Maturation of naked endothelial cells (ECs) into stable blood vessel is achieved with
addition of cytokines, recruitment of smooth muscle cells (SMC) and flow...................40
Fig 2.1. G eneral schem atic of the device. ......................................................................................
55
Fig 2.2. Size selective perm eability...............................................................................................
57
Fig 2.3. Confirmation of endothelial monolayer integrity. ...........................................................
61
Fig 2.4. Optimization of tumor cell seeding density .....................................................................
63
Fig 2.5. Observation of extravasation and permeability of endothelium
65
......................................
Fig 2.6. Permeability of endothelium measured with 70kDa fluorescently-labelled dextran. ......... 67
Fig 2.7. Beyond extravasation. The tumor cell extravasation is observed for up to 3 days after tumor
cell seeding and compared to the ones fixed and analyzed on day I ............................................
69
Fig 3.1. Generation of the osteo-cell conditioned microenvironment...........................................
77
Fig 3.2. Extravasation of cancer cells into the collagen gel matrix with and without osteodifferentiated hB M -M SC s.................................................................................................
Fig 3.3. Effect of CXCL5 and CXCR2 in cancer cell extravasation.............................................
83
85
Fig 3.4. Generation of micrometastases within the osteo-cell conditioned microenvironment.........87
Fig 3.A 1. C alcium production........................................................................................................
96
Fig 3.A2. Osteo-differentiation immunofluorescence assays. ......................................................
96
F ig 3.A 3. L ive/D ead assay . ................................................................................................................
97
Fig 3.A4. Endothelial monolayer quality and collagen gel structure within microfluidic devices....97
Fig 3.A5. Confocal reflectance image of 6.0 mg/ml gel with and without osteo-cells 3 days after the
gel-filling. No significant difference was detected in the matrix structure......................
Fig 3.A6. Confocal reflectance images of 6.0 mg/mi collagen gel + osteo-cells with and without
9
98
cancer cells 24 h after cancer cell seeding. The presence of cancer cells does not induce
clearly detectable structural changes.................................................................................
98
Fig 3.A7. Endothelial monolayer permeability change before and after cancer cell seeding........99
Fig 3.A8. Endothelial monolayer permeability change of devices with and without osteo-
differentiated hBM-MSCs in gel.....................................................................................
99
Fig 3.A9. CXCL5 quantification assay and CXCR2 detection........................................................100
Fig 3.A 10. Scatter plot representing the relationship between number of cancer cells per
micrometastasis and number of cancer cell micrometastases per region of interest (ROI).
.............................................................................................................................................
Fig 3.A 11. Day-to-day progression of cancer cell clusters. .............................................................
10 0
101
Fig 3.A 12. Computational simulation of the CXCL5 gradient within the microfluidic device.......101
Fig 4.1. Schematic of the microfluidic vasculogenesis system........................................................109
Fig 4.2. Differentiation of BM-hMSCs in presence of HUVECs ....................................................
114
Fig 4.3. Co-localization of HUVECs and BM-hMSCs enabled differentiation of BM-hMSCs into
mu ral cells. ..........................................................................................................................
1 15
Fig 4.4. Formation of microvascular network by vasculogenesis....................................................117
Fig 4.5. Generation of mature microvascular network in presence of BM-hMSC and different
b iom o lecu les........................................................................................................................1
19
Fig 4.A 1. Live/Dead assay showing cell viability at day 1..............................................................122
Fig 4.A2. SM22a immunofluorescent staining highlighting BM-hMSC differentiation toward a
m ural cell lineage. ...............................................................................................................
122
Fig 4.A3. Confocal microscopy image representing mural cell differentiated BM-hMSCs (a-smooth
muscle actin, green) co-localization with ECs (red). ..........................................................
123
Fig 4.A4. Microvascular network analysis: number of branches.....................................................123
Fig 4.A5. Vessel perfusion with 70 kDa fluorescent dextran revealing patent lumen and absence of
4
fo cal leak s............................................................................................................................12
Fig 5.1. VE-cadherin staining for vasculature...............................................................................134
Fig 5.2. a-smooth muscle actin staining for mural cell ...................................................................
134
Fig 5.3. Staining for osteocalcin (O CN )...........................................................................................135
Fig 5.4. Live imaging of cancer cell extravasation in the generated microvascular network..........135
10
Fig 5.5. Percent of extravasation in bone-mimicking microenvironment........................................136
Fig 5.6. Permeability of the vessel network ...................................................................................
137
Fig 5.7. Percent of extravasation for static and flow conditions in bone-mimicking
m icroenvironm ent ............................................................................................................................
137
Fig 5.8. Permeability of the vessel network for static and flow condition in bone-mimicking
m icroen vironm ent. ..............................................................................................................
138
Fig 5.9. Elongation of endothelial cells during application of shear stress......................................138
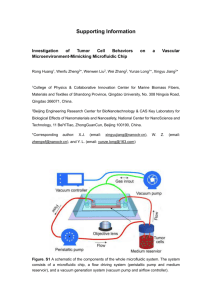
Fig 6.1. High-throughput device for multi-organ mimicking system. .............................................
11
144
List of Tables
Table 1.1 In vivo extravasation models.........................................................................................
26
Table 1.2. In vitro Microfluidic extravasation models...................................................................27
Table 1.3. Angiogenic activators and inhibitors as well as their functions...................................
12
30
Chapter 1
Introduction'
1.1 Cancer cell extravasation and microfluidics
The last four decades were characterized by promising successes in cancer treatment and
detection, through the development of devices reducing surgical invasiveness or allowing early diagnosis,
and the discovery of drugs blocking primary tumor progression, thus reducing cancer mortality and
improving life quality for terminally ill patients [3]. As discussed in a recent scientific report of the
American Cancer Society, the relative 5-year survival rate for all cancers diagnosed between 2002 and
2008 in the US was 68%, significantly higher compared to 49% reported for 1975-1977 [4]. However,
despite great advances in basic cancer molecular and cell biology with the discovery of oncogenes [5],
tumor suppressor mechanisms [6] and cytokines involved in cancer progression [7], the spread of primary
tumors to distant organs and the subsequent metastatic colonization is still responsible for 90% of cancerassociated mortality [8].
In vitro assays can be beneficial to study cancer cell invasion and migration, and develop new
anti-cancer drugs [9]. Particularly, human three-dimensional (3D) models can closely mimic the pathophysiological microenvironment [10], combining multiple cell types and molecular factors in a controlled
system, thus bridging the gap between simplified two-dimensional (2D) assays, which lack the structural
architecture of body tissues and force cells to adapt to an artificial flat and stiff surface [11] and complex,
This chapter is modified from Ref. [1-2] with the publisher's permission.
13
expensive in vivo studies, often performed through animal models which may fail to reproduce features of
human tumors [12]. Significant advances have been made since the development of soft lithography
techniques, which allow microfabrication of structures and channels with PDMS (poly-dimethyl-siloxane)
for microfluidic applications, thus overcoming the limitations of traditional plastic surface devices, and
allowing for more complex patterning of cells and biomolecules [13]. Microfluidic devices with
embedded
3D cultures
are
currently used to study
cancer cell behavior
within
in vivo-like
microenvironments [14].
Modeling the multiple steps of the metastatic cascade represents a challenge that, if overcome,
could pave the way to the discovery of new anti-metastatic drugs [15]. Particularly, extravasation
represents a critical point which leads to the invasion of cancer cells at specific secondary sites with the
subsequent growth of metastatic tumors, hence detailed studies are necessary to clarify the interaction
between specific primary tumors and secondary target organs [16].
Following an introductory section on cancer metastases, this chapter will focus on in vitro models
to study cancer cell invasion, migration and particularly, extravasation. Microfluidic applications to
investigate extravasation processes and other metastasis-related phenomena will also be discussed. The
final section will present in vitro and in vivo models to study the effects of therapeutics on cancer cell
extravasation, underscoring how highly specific microfluidic models could provide a significant
breakthrough in the screening process of anti-metastasis drugs. This chapter concludes with an overview
of the entire thesis.
1.1.1 Cancer cell odyssey in the metastatic cascade
Tumors arising from epithelial tissues represent around 80% of life-threatening cancers due to
their ability to metastasize in different secondary organs [17]. The complex metastatic process can be
conceptually divided into two main phases, namely the physical translocation of cancer cells from the
primary tumor to distant sites, and their subsequent colonization (Figure 1.1). More specifically, several
14
sequential and interrelated steps can be recognized in the former phase, including loss of cellular
adhesion, acquisition of increased invasiveness and motility due to genetic and epigenetic alterations, and
induction of tumor angiogenesis leading to entry into the circulatory or lymphatic systems - a process
known as intravasation [8, 18]. After intravasation, those cells that survive in the circulation might
undergo extravasation, which includes several steps: cells becoming trapped in a remote vessel or adhered
to its endothelium and transmigrating into tissues, to initiate the development of secondary tumors [19-
23].
brain
lung
Sbone
extravasating
cancer cells
in circulation
lier
Figure 1.1 Schematic of extravasation cascade. Primary cancer cells travel in circulatory system and
transmigrate across the endothelium to extravasate into secondary site and colonize at organs such as
lung, bone, liver, and brain. Predominant primary cancer sites where initial dissemination occurs include
breast, pancreas, prostate gland, colon and lung.
In one scenario of extravasation, circulating tumor cells (CTCs) showing a leukocyte-like rolling
behavior on the vascular walls [24] establish transient, metastable contacts with the endothelium mediated
by endothelial cell surface molecules, e.g. E-selectin and P-selectin, and cancer cell counter-receptors
such as sialyl Lewis-a/x [25, 26]. Subsequently, a firmer adhesion is mediated by adhesive molecules on
the endothelium such as vascular cell adhesion molecules (VCAMs), whose expression can be triggered
15
by cancer cells themselves [27], and cancer cell integrins, while chemo-attractant molecules promote
trans-endothelial migration toward the surrounding tissues [10]. An alternative view is that CTCs, being
relatively large, are physically trapped in the small vessels of the microcirculation, become activated, and
transmigrate [28].
Steven Paget's "seed and soil" hypothesis represents a milestone in the study of mechanisms
governing metastases, based on the assumption that the interplay between specific cancer cell types and a
properly receptive microenvironment guides the metastatic spread of primary tumors to distant
organs[29]. However, Paget's theory was challenged by James Ewing, who proposed that the main factor
leading to metastases is represented by the anatomy of blood and lymphatic vessels and by circulatory
patterns between primary tumors and specific secondary sites [30]. It is now accepted that these theories
are not mutually exclusive: scientists have shown how CTCs migrating from the primary tumors target a
well defined sub-set of organs, specific for each tumor type. This tissue tropism is partially due to the
anatomy of the circulatory system, leading to physical trapping as described above, but also influenced by
the interaction between "seed cells" and "receptive soils"[]6-18, 31].
Endothelial cells in the vasculature of different organs express different surface receptors and
specific chemokines are secreted by host cells of individual tissues [32, 33]. Moreover, the "premetastatic niche model" states that growth factors secreted by the primary tumor can prime specific
tissues for cancer engraftment, determining the attraction of tumor-associated cells, which contribute to
the development of a receptive environment [30, 34-36] and promoting specific cancer cell homing.
Particularly, breast cancer cells often metastasize to the bone and autopsy studies have demonstrated that
70% of breast cancer patients have skeletal metastases, which represent the major cause of lethality and
induce pain, spinal cord compression and fractures, severely compromising quality of life [37, 38].
Unraveling the multiple steps of extravasation could enable the identification of new anti-cancer drugs to
inhibit the adhesion and/or transendothelial migration of metastatic cells. In vitro testing platforms
represent an extremely useful tool but the lack of organ-specific models, reproducing the human in vivo
16
microenvironment and tissue tropism shown by specific cancer cells, constitutes a significant limitation
among current systems.
1.1.2 In vivo and in vitro cancer models for invasion, migration, extravasation and colonization
While no in vivo or in vitro model fully replicates the complex milieu of factors that influence
metastasis in humans, there have been numerous studies devoted to understand cancer cell invasion,
migration, and interactions with the endothelium, which comprise different stages of cancer metastasis.
Conventional studies of metastasis have been mostly limited to in vivo mouse models as there is a lack of
tumor models and methods to study the associated processes in vitro. Mouse models provide a platform to
screen for genes involved in metastasis for specific organs or proteins that mediate cancer invasion [3941]. Roles of chemical factors and different signaling mechanisms that lead to trigger each step of
metastasis have been studied as well [42-44]. Particularly, in the case of cancer cell extravasation, in vivo
videomicroscopy of tail-vein injected cancer cells to mouse has been the primary means of investigation
[22, 45]. Moreover, advanced in vivo models were developed to study metastasis through direct injection
of breast cancer cells either intravenously or directly to specific organs [46, 47], and intravital
videomicroscopy was employed to visualize the interactions of cancer cells in the circulatory system and
the metastatic site in a more physiologically relevant manner. However, the main disadvantages of in vivo
models are that they make it difficult to perform tightly-regulated, parametric studies and quantification is
limited [48].
Earlier in vitro models relating to cancer metastasis investigated cancer cell invasion and
migration across matrix of various types under different mechanical and/or chemical cues [49]. There
were also studies that focused on interactions of two cell types by modeling cancer cell adhesion to the
endothelium, with emphasis on the changes imposed in cell morphology and monolayer biomechanical
properties [50, 51]. Furthermore, use of the Boyden chamber/transwell assays for simulating cell
migration and cancer cell invasion across the endothelium has been widely accepted. These models have
17
been a popular choice as they have advantages to overcome some limitations of in vivo experiments
(parametric studies, quantification, non-human cells, etc.) by providing more regulated environments with
tunable parameters and using human cell types. However, limitations still exist in that Boyden chamber
allows limited control over the local environment and complex multicellular interactions cannot be
accurately analyzed due to limited imaging capabilities.
In recognition of the need for a new generation of in vitro platforms, optically accessible and
better mimicking physiological conditions through controlled-microenvironments, a recent research has
led to the creation of a new class of in vitro testing methodologies using the emergent technologies of
microfluidics. While acknowledging that in vitro systems cannot fully reproduce the complexity of in vivo
situation, microfluidic devices allow an opportunity to create organ-specific microenvironments and
explore the development of metastasis of different cancer types, including migration through gels as well
as real-time imaging of invasion and extravasation.
1.1.3 Microfluidic tools for in vitro cancer models
Microfluidics has revolutionized the field of cell biology, allowing researchers to develop
advanced 3D assays in highly controlled microenvironments [52], characterized by spatio-temporal
tunable chemical gradients, interstitial flows and shear stresses, complex interactions among multiple cell
types and small reagent volumes compared to traditional assays [14, 53, 54].As a result, microfluidics is
one of the most promising technologies to develop and optimize complex in vitro cancer models,
mimicking multiple steps of the metastatic cascade from primary tumor local invasion to extravasation in
secondary loci.
In recent work by Haessler and co-authors [55], migratory behavior and migrational speed of
metastatic breast cancer cells MDA-MB-231 were investigated under a controlled interstitial flow within
a 3D microfluidic chamber. Collected results demonstrated how the interstitial flow increased the
percentage of migrating cancer cells and induced a superior persistence (the ratio between the cell net
18
displacement in a specific direction and the cell total path length) for specific cell sub-populations,either
in the positive or negative interstitial flow direction. These data promote the idea that small, aggressive
and resistant sub-populations of cells play a critical role in cancer, being characterized by phenotypes
leading to drug resistance and metastatic dissemination. Morphology and invasiveness of breast cancer
cells were also investigated by Liu and colleagues [56], who showed that MCF-7 breast cancer cells
generated protrusions and migrated up an epidermal growth factor (EGF) gradient within a 3D basement
membrane extract gel with a matrix metalloproteinase (MMP)-dependent proteolytic activity. On the
same topic, the Beebe group developed a simple and effective microfluidic device to study the transition
from Ductal Carcinoma In Situ (DCIS) to Invasive Ductal Carcinoma (IDC) in a co-culture system with
human mammary fibroblasts, demonstrating that the presence of both soluble factors and cell-cell
contacts accelerates the transition and that increasing the distance between cell populations leads to
incomplete transition, with carcinoma cells retaining their rounded morphology [57]. An advanced
microfluidic model was recently proposed by Zervantonakis et al. to investigate the mechanism
underlying cancer cell intravasation, showing how tumor necrosis factor alpha (TNF-a) secreted by
macrophages interacting with cancer cells can promote endothelial barrier impairment and subsequent
cancer cell transmigration [58].
The above mentioned models represent just a few of the promising and smart studies recently
developed to investigate the initial events of the metastatic cascade while other specific assays were
designed to analyze the final steps of cancer cell journey within the circulatory system. Particularly, a few
interesting models were developed in the last five years to study adhesion and extravasation of cancer
cells (Figure 1.2). The Takayama group designed a microfluidic device to recreate the adhesion of cancer
cells to an endothelial monolayer under physiological flow conditions. They demonstrated both that breast
cancer cell receptors CXCR4 and CXCR7 are involved in the adhesion process and that a CXCL12conditioned environment can act on endothelial cells, enhancing breast cancer cell adhesion in a CXCR4
or CXCR7 independent manner [59]. Similarly, Shin and co-authors developed a complex platform to
19
analyze the metastatic process from intravasation to the downstream endothelial adhesion in a single chip.
Particularly, they showed how colon cancer cell adhesion is dependent both on E-selectin expression by
endothelial cells and shear stress levels, finding an optimal value at 3 dyne/cm2. Moreover, they found a
significant decrease in cell adhesion when cancer cells were treated with the extravasation inhibitor
CA19-9
antibody
[60].
Extravasation
events were monitored by Zhang et al., who analyzed
transmigration of salivary gland adenoic cystic carcinoma (ACC) cell aggregates in a gel matrix,
demonstrating how cell clusters can adhere to but not extravasate through the endothelium without
CXCL12 stimulation. Interestingly, a CXCL12 concentration-dependent transmigration behavior was
highlighted, and the addition of the CXCR4 antagonist AMD3 100 inhibited cell aggregate extravasation,
but it failed to cause detachment of aggregates from the endothelial monolayer. Finally, cell-cell junctions
in the endothelial monolayer appeared completely destroyed at the site of transmigration[6 1]. A similar
model was designed by the Kamm group to investigate single breast cancer cell extravasation through an
endothelial monolayer within a collagen gel matrix. Transmigration can be closely monitored in this
microfluidic device with a high resolution imaging system, showing that extravasation events within the
matrix occur in the first 24 hours following cancer cell introduction, and are associated with a significant
increase in endothelial monolayer permeability due to disruption of vascular endothelial (VE)-cadherin
junctions [62]. A more physiological model was recently developed by the same group to analyze the
extravasation ability of different cancer cell types within a microvascular network, demonstrating the
effect of inflammatory
cytokines and accurately describing the transmigration
event, which is
characterized by initial thin cancer cell protrusions followed by extrusion of the nucleus and cell body
[63]. It is well known that cancer cells undergo deformation processes prior to adhesion and extravasation
through the endothelial lining. Chaw and colleagues developed a multistep microfluidic device to study
the effect of cell deformation on viability and proliferation, revealing that different cancer cell lines under
mechanical stresses were characterized by reduced viability and increased doubling times, thus suggesting
a significant change in their biological activity. Moreover, they quantified migration rate and the
20
percentage of cells capable of migrating through 30 pm wide microgaps coated with Matrigel, with or
without an endothelial cell lining. They demonstrated the different roles played by basement membrane
coating and the endothelial monolayer, the former slowing down cancer cell migration and the latter
reducing the total number of transmigrating cells [64].
3D view2D
D
E
top view
Matrigal
PDOSp
dsuiflsg
Dissolved region
lop Cancer cell
Main
Valv%-E
M rtC
mber
Poly--Lyslaye
0Cancer cell
q&
HUVEC
Fibronectin layer
Poly-L-Lys
layer
Figure 1.2 Microfluidic models for extravasation. (A) Multi-step microfluidic device developed by Chaw
and colleagues. Deformation chamber with 10 pim wide gaps through which cells are forced (i) and
transmigration chamber with a row of 30 Am wide gaps where cell migration and invasion take place (ii).
Reprinted with permission [64]. Copyright 2007 RSC. (B) Microfluidic device for the study of
transendothelial migration of cancer aggregates (Zhang and co-authors). Reprinted with permission [61].
Copyright 2012RSC. (C) In vitro model developed by Jeon et al. to investigate breast cancer cell
extravasation in a collagen gel matrix. Reprinted with permission [62]. Copyright 2013 PLOS. (D)
Microdevice designed by the Takayama group to analyze intravascular adhesion of breast cancer cells.
Reprinted with permission [65] Copyright 2009 PLOS. (E) Microfluidic platform for the study of intraand extravasation events (Shin et al.). Chamber-I represents the intravasation chamber for cell migration
and invasion while chamber-E constitutes the extravasation chamber where cancer cell adhesion events
on an endothelial monolayer can be detected. Reprinted with permission [60]. Copyright 2012 RSC.
21
Leukocyte extravasation, which shares many similarities to cancer cell extravasation, has been
more extensively studied. Schaff and co-authors [66] designed a microfluidic device to test neutrophil
capture, rolling and deceleration on an endothelial monolayer under controlled shear stress conditions,
with the capability of including chemokine gradients; moreover, they coupled a computational model to
predict shear stresses and leukocyte trajectories. This platfonn could potentially be applied to analyze
cancer cell adhesion and extravasation if 3D hydrogels mimicking an extracellular matrix were to be
included. Chau and colleagues [67] focused on the development of a microdevice to study the effect of
multiple shear stress conditions on endothelial cell morphology, nuclear size, perimeter and secretory
activity. Although they did not investigate the adhesion of circulating cells, this platform could be easily
adapted to perform detailed studies on cancer cell or leukocyte adhesion. An exhaustive discussion of in
vitro assays for leukocyte adhesion with useful insights on computational models can be found in recent
reviews by Bianchi [68] and Hanzlik [69]. Finally we want to highlight the versatility of a previously
described platform [9], which was employed to analyze leukocyte transendothelial migration under the
influence of inflammatory stimuli [70] as well as cancer cell extravasation [62].
The extravasation assays discussed in this section (Table 1-2) allowed investigation for the first
time of adhesion and transmigration processes of single or aggregated cancer cells, eventually coupled
with chemokine gradients or inhibitory molecules. Despite the significant step forward provided by these
models they lack the organ specificity that different cancer cell types exhibit in vivo. With the increasing
interest in organ-specific chemokines and endothelium adhesion molecules guiding extravasation of
specific CTCs, microfluidic devices mimicking different organ microenvironments could prove useful in
identifying which surface receptor/ligand interactions are most critical and in developing targeted
therapeutics.
22
1.1.4 Targeting cancer cell extravasation: in vitro and in vivo drug screening models to block the
metastatic cascade
Inhibiting cancer cell extravasation represents a promising strategy to break the metastatic
cascade, coupled with other therapies to stop tumor growth, inhibit tumor angiogenesis and prevent
epithelial to mesenchymal transition (EMT) and intravasation events. These, in combination with early
diagnosis techniques could significantly improve the efficacy of cancer therapies.
One of the first studies performed on cancer cell extravasation was conducted by Saiki and coauthors, who investigated the effects of synthetic sialyl Lewis X and fibronectin-derived RGDS peptide
analogue on lung metastases generated by in vivo intravenous injection of melanoma cells. The former
molecule was found to inhibit the interaction with the endothelium while the latter limited cancer cell
invasion into the basement membrane, thus affecting a later step of the extravasation process [71]. A
second pioneering study was conducted by Hangan and colleagues who analyzed VLA-6, an integrin
receptor mediating cancer cell adhesion to the endothelium. By performing in vivo studies on mice and
simple in vitro models with chemotaxis chambers, researchers discovered that although the VLA-6
monoclonal antibodyMA6 did not affect adhesion, it inhibited melanoma cell movement on laminin
substrates. Thus, their findings suggested an active role for the VLA-6 receptor in providing both cell
movement and adhesion and more specifically demonstrated an absence of alterations in the focal
adhesion kinase phosphorylation, which is involved in motility [72]. Furthermore, in vivo experiments
demonstrated a reduced ability of MA6 treated mouse melanoma cells to extravasate the liver vasculature.
Recent works concentrated on a wide spectrum of biomolecules involved in cancer cell extravasation. The
Jirik group found that the extracellular matrix remodeling enzyme lysyl oxidase (LOX) inhibitor
p-
aminopropionitrile (BAPN) was able to reduce the number of breast cancer metastases in treated mice,
without affecting established loci. Then, LOX seemed to be involved in the initial steps of extravasation
and tissue colonization and could represent a potential candidate for advanced drug screening tests [73].
Based on findings reporting that radiotherapy can increase the metastatic potential of surviving cells [74],
23
Hamalukic and colleagues performed a promising study in which ionizing radiation-stimulated cancer
cells/endothelial cells adhesion was limited by treatment with HMG-CoA reductase inhibitor lovastatin,
sialyl Lewis X mimetic drug and Raci inhibitor (Figure 1.3). In vivo studies confirmed the potential role
played by the lipid-lowering drug lovastatin in mice, counteracting the increased extravasation effect
induced by radiation therapy [75]. Tanaka and co-authors used the osteosarcoma cell line OS LM8 within
standard transendothelial migration assays to show the ability of these malignant cells to compromise an
endothelial barrier and demonstrate that inhibiting the vascular endothelial growth factor (VEGF)
signaling through the tyrosine kinase inhibitor pazopanib limited extravasation. In vivo studies seemed to
confirm that anti-VEGF therapies could limit lung metastases from osteosarcoma [76]. Furthermore, the
reduced
02
availability within the tumor environment can promote the expression of hypoxia inducible
factors (HIFs) which increase the level of proteins involved in cancer progression. HIFs can induce
angiopoietin-like 4 and LI cell adhesion molecules production by cancer cells, which in turn promote
extravasation into lungs [44]. A recent elegant in vivo model on transparent zebrafish developed by the
Klemke group demonstrated that MDA breast cancer cells engineered to overexpress the metastatic gene
Twist were characterized by increased extravasation ability compared to wild type cells. Moreover, they
reported the process switched to a
p1-integrin
independent mechanism, with interesting implications on
the use of small interfering RNAs [77]. Finally, we would like to highlight a recent study on tumor cellactivated platelets which were shown to release adenine nucleotides that interact with the P2Y 2
endothelial cell receptor, thus promoting openings in the endothelial barrier and subsequent cancer cell
extravasation [78].
24
A
)
Qend@othakal
F-eronectin
r
B
labeled LM or Dunn cells
F
cells
coat
BIssd
Fluorescence
J~'bkclng
PET mernrane
Exciaon
(577 nrn)
a aP=0.005
Emission
(602 nm)
P-.022
10'
Exrvston
Lung mftasbas
p-0.OO3
150
100
aU
CAF(EC)
(n-3)
(n-3)
(n-3)
CAF(TC)
(n=3)
Figure 1.3 In vivo and in vitro models developed for screening drugs acting on extravasation. (A)
Transendothelial migration of highly metastastic LM8 osteosarcoma (OS) cell line and Dunn OS cell line
(Tanaka et al.). Cancer cells were applied on a monolayer of endothelial cell coated fluorescence-blocking
membrane and transmigration investigated after 12 h (i). Comparison between control LM8 cells,
pazopanib (vascular endothelial growth factor (VEGF)-inhibitor), VEGF or a combination of VEGF and
pazopanib (ii). Reprinted with permission [76]. Copyright 2012 Springer. (B) Bioluminescence imaging
showing the metastatic progression of breast cancer cells between day 7 and day 21 after cancer cell
intracardiac injection. Reprinted with permission [73]. Copyright 2009 PLOS. (C) Ionizing radiation (IR)
can increase tumor cell (TC)-endothelial cell (EC) adhesion and subsequent TC extravasation and
generation of lung metastases. Reprinted with permission [75]. Copyright 2011 PLOS.
The identified molecules (Table 1-2) could represent promising targets for future anti-metastatic
therapies but additional studies are required to clarify their mechanisms of action and possible interactions
with different cell types. In this framework, microfluidic cancer models, as reported in the previous
section, pave the way to a new class of assays between traditional 2D models and in vivo studies. These
advanced in vitro models allow strict control of multiple spatio-temporal parameters, while maintaining
drug gradients and co-cultures of multiple human cell types in physiological 3D matrices. Their
optimization can lead to develop more focused in vivo screenings, which although being essential, are
becoming increasingly expensive and surrounded by ethical problems.
25
Table 1.1 In vivo extravasation models
Animal Model
Primary
CanrmCells
Cancer
Cels
Metastati
M e
c Site
mouse (intavenous
injection)
mouse
melanoma cells
mouse (mesenteric
vein injection)
mouse
melanoma cells
liver
mouse (intracardiac
injection)
breast cancer
bone and
other
cells
tissues
breast cancer
cells
tail intersegmental
vessels
transparent
zebrafish embryos
(intracardiac
injection)
mouse (lateral tail
vein injection)
mouse (intravenous
injection)
Key Molecule/
Gene
Investigated
Blocking Molecule/Drug
______________
Ref
__
E-selectins
integrins
synthetic sialyl Lewis
X/fibronectin-derived RGDS
peptide analogue
Ar(DRGDS)3
VLA-6 (a6pl)
integrin
VLA-6 monoclonalantibody
MA6
[72]
lysyloxidase
P-aminoproprionitrile
[73]
Twist/ITGB/[77
VEGFA
_esses
tumorigenic
chinese
hamster
fibroblasts and
colon
carcinoma cells
breast cancer
cells
lung
NF-kB/Eselectin
lovastatin/glycyrrhizic
acid/Rac1 inhibitors
[75]
lung
HIF/Ang-like
4/L1-CAM
digoxin
[44]
pazopanib
[76]
mouse
otoacm
(subcutaneous
tissue of the back)
lung
VEGF
mouse
osteosarcoma
cells
mouse
melanoma cells
(subcutaneous or
lateral tail vein
injection)
and mouse
Lewis lung
lung
g
P2Y/Munc3-8]
cai
s
carcinoma cells
_
26
Table 1.2 In vitro Microfluidic extravasation models
Vascular Cells
Cancer Cells
Process
cl
rodees
modeled
microvascular
endothelial cells
hepatocellular
carcinoma-cervical
carcinoma-breast
carcinoma
Extravasation
(no
matrix)
dermal
microvascular
cells
breast cancer cells
adhesion
CXCL 2TNFal1G8
polyester
membrane 400
nm pores
+
colon cancer cells
adhesion
MMP2 inhMMP 9 inhGM6001CA 19-9
Matrigel +
fibronectin
coating
(extravasation
chamber)
+
salivary gland
adenoic cystic
adenocarcinoma
cells
Extravasation
CXCL 12AMD3 100
umbilical vein
endothelial cells
umbilical vein
endothelial cells
microvascular
endothelial cells
umbilical vein
endothelial cells
breast cancer cells
breast cancer cells,
fibrosarcoma cell
line
Key
Molecule
Investigated
Matrix
Flow
Perme
ability
Ref
matrigel
(microgap
coating) -No
matrix
Extravasation
TNF-a
27
-
[60]
+
[62]
+
[63]
basement
membrane extract
collagen type I (2
mg/ml)
Extravasation
[59]
fibrin gel (2.5
mg/ml)
1.2 Microfluidic platforms for angiogenesis and vasculogenesis
Angiogenesis,
the development of new blood vessels from pre-existing vasculature,
and
vasculogenesis, the development of vascular networks from endothelial precursor cells, are essential
events in development and in a vast range of physiologic and pathologic conditions. And despite the
existence of numerous routine procedures to culture endothelial cells under various culture conditions, our
ability to study the angiogenic process in vitro has progressed only slowly.
One of the primary motivations for the in vitro simulation of angiogenesis stems from the seminal
work of Dr. Judah Folkman who identified suppression of tumor vascularization as a new approach to the
treatment of cancer. Indeed, tumor growth and metastatic dissemination are critically dependent on the
tumor's blood supply [79].
And while the promise of anti-angiogenic therapies has yet to be fully
realized, interest remains high in the identification of new factors that either promote or inhibit the
formation of new microvascular networks. Angiogenesis also plays an important role more generally in
vascular biology because it is an essential process that occurs in various normal and pathological events.
Wound healing and the reperfusion of ischemic regions following myocardial infarct or stroke are cases
where angiogeneis needs to be stimulated.
Cancer and diabetes, are cases in which anti-angiogenic
therapies are targeted. In addition to these, there are more than 70 disorders that are directly or indirectly
linked with angiogenesis, and the list of conditions continues to grow [80]. A better understanding of the
biology of angiogenesis may reveal new targets for treating these diseases.
28
b
LModulation
a Selection of sprouting ECs
rof
h
VR!GF-Vit
of
Spmsut outgrowth and guidne
Maintenance
wpoMeupHPn
Deposition
EC-EC Contacts eEo
C
nhibItion e
behviur
In
ChangeGrwhfca
inhibitors
Cells
Gr
n
..
Moduladon of
PC contacts
thf
iand
wC
profer CEe
adtion
E
E
Pro-quiescent signals
(aocal and systemic)gl
CSpout fusion ad tswn formifson
stakcell
ndels
and maturation
d Perfuion
CDC42 sd Rad
of
iriStabilin ad
proliferation
Vacu#l formation
ECAC adeion
Fization 1
of PC contacts
and fusion
encounrtering
ordi i on e
EC
proliferation
Pro-quiescent
s fcnals
t
are applied.
Figure 1.4 Angiogenic sprouting event occurs at a) pre-existing vessel when growth factors
lumen
forms
c)
and
space,
(ECM)
matrix
b) Endothelial cells (ECs) starts to sprout out into extracellular
mature
and
other
each
to
adhere
stably
ECs
Finally,
d)
as more sprouts form fuse and cells proliferate.
perftisable vessel is formed - Adapted by permission from Macmillan Publishers Ltd: [81. Copyright
2007 NPG.
There are multiple steps involved in angiogenesis, often classified as vasodilation, endothelial cell
proliferation and migration, survival/maturation, and remodeling [82] (Figure 1.4). It has long been
known that hypoxic conditions stimulate the local cells to release various factors that induce the
recruitment of new blood vessels. A variety of factors have been identified (see Table 1), many of which
can be traced to the upregulation of hypoxia inducible factor (HIF-1) [83, 84]. Tumor growth and
metastatic dissemination are critically dependent on the tumor's supply of blood vessel [79], making
angiogenesis a putative target for cancer therapy. It is commonly believed that blocking the vessel
formation in tumor mass will limit tumor growth as well as metastasis. Therefore, many inhibitors of
angiogenesis are under intense clinical investigation as anti-angiogenic factors. Current efforts in antiangiogenic therapies either act by inhibiting one of the various receptors of these factors, or by
29
suppressing the degradation of HIF-1, but the approaches are numerous and a need clearly exists for a
method that is capable of screening many factors rapidly in an in vitro setting that recapitulates many of
the features of the in vivo microenvironment.
Table 1.3 Angiogenic activators and inhibitors as well as their functions are listed [85, 86].
Activators/Inhibitors
Functions
VEGF
Stimulate angio/vasculogenesis, permeability, leukocyte adhesion
ANGI
Stabilize vessels, inhibit permeability
PDGF-BB
Recruit smooth muscle cells
TNF-a
Induces production of bFGF in endothelial cells and enhances its
secretion, activates macrophages
TGF-a
Stimulate endothelial mitogenicity
TGF-P
Stimulate extracellular matrix production, Inhibits endothelial
mitogenicity
aFGF, bFGF
Stimulate angio/arteriogenesis
In this chapter, we will explore how angiogenesis is described in a microenvironment formed using
microfluidic system how it can be used to introduce many stimuli that are known to induce angiogenesis.
As the relevance of angiogenesis in physiological function extends much more than the growth of
endothelial cells to interactions of different cell types, the co-culturing of multiple cell types will be
discussed. These interactions of endothelial cell and heterotypical cells not only induce angiogenesis
when particular chemokines are secreted, but also matures the newly created vessels.
Finally, we will
describe various methods for quantifying the angiogenic response.
1.2.1 Mimicking angiogenesis in microfluidics
Microfluidics has the potential to overcome many of the practical limitations that have impeded
progress in the study of angiogenesis. One of the major advantages of microfluidic systems in studying
angiogenesis is that it has the potential to mimic the true three dimensional (3D) nature of the in vivo
situation while maintaining its in situ imaging capabilities. In addition, because of the ready access to the
30
cell-seeded regions, media can be changed frequently with little disturbance to the cells, or lows can be
generated to create the shear stress conditions that are found in vivo. And perhaps most importantly,
multiple cell types can be seeded into these devices so that they can interact over physiologically-relevant
length scales. These interactions between endothelial cells and heterotypic cell types not only induce
angiogenesis when particular chemokines are secreted but also play a critical role in the maturation of the
newly created vessels. Finally, since the developing microvasculature can be readily imaged, a wide range
of methods has been developed for quantifying the angiogenic response from various imaging modalities.
In recent years, there has been considerable progress in the development of microfluidic designs to
replicate a diverse range of physiological events. Micro-fabrication technology using soft lithography has
enabled tremendous utilization of sub-micron scale designs for micropatterns, narrow channels and
chambers as well as microscale design to accommodate optimal cell-to-cell or cell-to-matrix interactions.
Larger designs including arrays of hundreds of micron-scale features can also be fabricated using this
technique, providing the opportunity of high throughput testing, but at the cost of added complexity [87,
88]. Furthermore, not only can heterotypic cell co-cultures be accommodated in certain microfluidic
designs, but so can living tissue or biopsy specimens be introduced [89], raising the prospect of even
greater realism and the potential to screen for patient-specific therapies.
The three dimensionality of microfluidic platform arises as a result of the integration of various
hydrogels or nanofiber constructs, which allows the matrix regions in the microfluidic system to mimic
the role of extracellular matrix (ECM) comprising the microenvironment of cell or tissue samples. The gel
region(s) in a microfluidic device can take several forms, depending on the most suitable design for a
particular experiment. One approach that has been proposed introduces microchannels surrounded on
three sides by matrix, and that could contain both tumor cells and other tissue cells [90]. These latter cells
might serve the purpose of simulating the natural organ or they could be pericytes or smooth muscle cells,
introduced for the purpose of creating a more realistic environment for a sprouting or pre-formed vessel.
Another approach that has recently been put into practice introduces matrix on one wall of a channel
31
imprinted
in
the
microfluidic
device
[91,
92]
(Figure
1.5).
This
design
utilizes
multiple
polydimethylsiloxane (PDMS) posts to contain the hydrogel solution within the gel region through the
forces of surface tension, and thus keeps the matrix separate from the media channels where culture
medium is introduced and endothelial cells can be seeded.
The most commonly used hydrogels are matrigel, collagen type I or fibrin gel all of which are
commercially available [93-97]. In the case of matrigel, it may be used directly as obtained commercially,
while for the others, simple synthesis of at most few reagents is required for gelation. The introduction of
a region of hydrogel in a microfluidic system allows capillary growth in 3D, thereby producing the most
realistic model for angiogenesis in vivo and at the same time, allowing spatio-temporal imaging.
Either of these approaches can also be used to recreate in vitro the process of vasculogenesis. The
primary difference is that endothelial precursor cells would be seeded within the gel, and no endothelial
cells would be seeded inside the channels. Channels might not even be necessary, other than to provide
fresh media to the system, or to generate a flow through the formed vascular network if desired.
In the following discussion, we focus on the experiments performed in the devices depicted in
Figure 1.5, or one of several variations on these basic designs. The first system (Figure 1.5A) is one in
which the hydrogel needs to be injected into the gel region prior to affixing the glass coverslip.
One
advantage of this system are that a linear gradient can be maintained (without the artifacts associated with
the gel-filling ports of the other systems) especially when the two channels are merged downstream of the
gel region and a slow flow is maintained in both channels. Another advantage is that the gel can be
slightly "over-filled" so that it spreads out into the channel slightly, offering a smooth, continuous face to
which the cells can adhere.
Other systems have gel-filling ports (e.g., Figure 1.5B) that allow for the
system to be fully assembled in advance with the gel added at a later time, making them somewhat easier
to use. An additional advantage of the system shown is that it provides for an internal control in the sense
that the test agent (chemical or cell type) can be placed in one of the side channels, and the opposite side
can be used for an internal control.
The third system shown (Figure 1.5C) provides for a longer gel
32
region, allowing for greater data collection in a single device.
Also, with the greater length, any
perturbation in gradients caused by the filling ports at the ends are confined, leaving gradients relatively
unperturbed over most of the system length.
For experiments in which another cell type is introduced either into the gel or into the opposite
channel with the aim of using secreted factors from these cells to induce angiogenesis, migration of the
second cell type into the gel and intermingling with the endothelial sprouts can be an undesired
consequence. In such cases, where the cells need to be kept separated, the cells can be encapsulated in a
more rigid, more slowly degradable gel, and introduced in encapsulated form either suspended in the gel
or flowed into the channel.
(a)
(b)
((b)
(W
(d)
Figure 1.5 Examples of microfluidic platform [91, 98, 99]. (a) requires the hydrogel to be injected into
the gel region prior to affixing the glass coverslip where as (b)-(d) have gel-filling ports inject hydrogel.
Design (b) can monitor control and condition by having three channel system, and design (c) incorporates
longer gel region for more experimental area. The T-shaped gel region in (d) allows studying of
directional effects due to biochemical gradients.
For studying chemotaxis effects such as those related to a VEGF gradient in guiding angiogenic tip
cells of endothelial cells, the T-shaped gel region can be advantageous (Figure 1.5D) [99] since the
turning is then a direct consequence of the biochemical gradient. Chemical gradients can also be created
33
in any of these designs, but tend to be time dependent, both during start-up but also as a result of
depletion of the chemoattractant from the media and during media changes.
These fluctuations can be
avoided by using a design in which the channels are joined at the downstream end and a constant flow of
medium is drawn through the channels. In this case, there is a single start-up phase lasting a time that
scales with the time for diffusion across the gel region (L 2/D where L is the distance across the gel and D
is the diffusivity of the chemoattractant), and the flows need to be maintained at a level that provides
sufficiently high convective effects relative to diffusion, as characterized by the Peclet number,
Pe =
vw
D
where V is the mean flow velocity in the channel, W is the channel width, and D is the
diffusivity of chemoattractant in the medium. When the goal is to observe as many sprouting events as
possible in a single device, a longer gel area can be employed and as many as 30 experimental regions
attained [100].
1.2.2 Inducing angio/vasculogenesis
The first isolation of angiogenic factors from tumor cells occurred in 1970s. Since then, much
effort in vascular biology has been directed toward identifying other possible biochemical as well as
biophysical factors that are thought to promote angiogenesis and to understand their significance in
forming vascular network [101, 102]. The following sections discuss different ways that angiogenesis can
be induced and regulated.
1.2.2.1 Chemicalfactors
Creation and maintenance of chemical gradients in microfluidic platform described above has been
confirmed [92]. Throughout the culture period, daily replenishment of medium along with the chemical
factor of interest allows stable linear gradient that the effect of application of each factors can be
systematically investigated in the platform. As mentioned earlier, active research to identify biochemical
34
factors inducing angiogenesis resulted in great advancement of determining and analyzing both pro and
anti-angiogenic factors. While vascular endothelial growth factor (VEGF) family has been recognized as
the most potent inducer of angiogenesis, there are many others including angiopoietins, fibroblast growth
factors (FGF), transforming growth factors (TGF), platelet-derived growth factors (PDGF), tumor
necrosis factor (TNF) and interleukins [103-109]. Table 1 below lists factors that are known so far to be
involved in angiogenesis whether their functions are activation or inhibition.
Among many angiogenic factors identified as listed in Table 3, members of VEGF family are the
best-characterized for angiogenesis [82, 99, 110, 111]. VEGF stimulates VEGFR which is a tyrosine
kinase receptors causing endothelial cells to be activated. The signaling cascade then stimulates the
secretion of factors leading to increased proliferation, maturation, migration, and vessel permeability
[103, 112]. These latter two are a reflection of the delocalization of the VE-cadherins that occurs, thereby
loosening the cell-cell adhesions [113, 114]. In addition, other factors such as angiopoietins are also
known to be involved in the part of process for attracting supporting cells as well as for stabilizing newly
formed blood vessels.
In microfluidic systems, it is possible to explore not only the effects of individual factors, but also
the orchestrated effects of multiple angiogenic factors. In particular, the effects have been studied for case
when both VEGF and ANG-1 gradients are applied [99]. VEGF gradients alone induce the proliferation
of tip cells that initiates angiogenic sprouting, but the addition of ANG-l gradient greatly enhances the
tendency to form a stable, continuous new vessel in which the tip cell remains attached to the stalk cells.
1.2.2.2 Mechanicalfactors
Application of shear stress to endothelium for mimicking flow condition of blood vessel is
achieved in a microfluidic system by integrating some form of pumping, such as a syringe pump,
peristaltic pump or some form of on-chip pumping [115]. The fluidic access ports to the micro-channels
inherently support the addition of external flow sources to the existing platform.
35
Shear stress has been shown to be a major biophysical factor for inducing angiogenesis, and that it
initiates angiogenesis by stimulates endothelial migration as well as proliferation of capillaries through an
upregulation of VEGF expression [116, 117]. In addition to increased production of growth factors, shear
stress also promotes development of cell-cell and cell-matrix junctions, and maturation of vascular
networks [118-120]. However, it has also been shown that shear stress stabilizes the endothelial layer in
the microfluidic devices [115, 121]. The actual effect of shear stress is likely to be complex and is a topic
of continuing study [122].
1.2.2.3 Micro-environmentalfactors
It is becoming
increasingly recognized that the local microenvironment
surrounding the
endothelium affects angiogenesis in various ways and its importance in cell function has been of
considerable recent interest. Microfluidic platforms that incorporate hydrogels offer a unique opportunity
to vary the properties (e.g., composition, stiffness) or conditions (hypoxia) of the extracellular matrix
(ECM), and at the same time, make detailed observations of the resulting response.
Hypoxia arises from a number of pathological conditions, but especially in the case of rapid tissue
growth as in a tumor, or impainnent of the local circulation as a result of an infarct or stroke [123]. In
hypoxia, low oxygen tensions lead to a delay in the inactivation of hypoxia inducible factor 1-a (HIF 1 -a),
a transcription factor for numerous angiogenic factors including VEGF-A and stromal-derived factor,
SDF- 1, oxygen sensing enzymes of endothelial cells are activated and produce hypoxia-inducible factor
(HIF) which then upregulates angiogenic factors for inducing angiogenesis [I1], 124]. Methods to control
the oxygen tension in a microfluidic system have not yet been reported, but their small size and the gas
permeability of PDMS offer new opportunities.
Another feature that has been shown to influence angiogenesis and the formation of a vascular
network is ECM stiffness. This can easily be accomplished with microfluidics simply by altering the gel
concentration, the type of gel, or the degree of polymerization as in the case of photopolymerizable gels
36
or gels such as collagen for which the stiffness of the formed gel can be controlled by varying the pH at
which the gel is formed [125].
1.2.3 Co-culture methods
1.2.3. 1 Co-culturing in microfluidic platform
An important advantage of microfluidic cell culture platforms is their ability to better mimic the
conditions that exist in vivo. In the previous section, we discussed the feasibility of introducing chemical
or physical factors and how they affect endothelial cell function in the context of angiogenesis. However,
in order to truly replicate physiological conditions, we must also consider the effects of interactions
between multiple cell types. Microfluidic systems with channels or gel regions that can be individually
seeded allow a simple integration of heterotypical cells types in a single device and recent studies have
shown this to be unique for the study of cell-cell interactions [98, 100]. This can be also be accomplished
through the addition of a porous membrane with different cells seeded on either side [65, 126, 127] or by
seeding one cell type on top of the other as is readily done in a Trans-well® assay, but these methods can
be constraining in terms of their ability to image the cell-cell interactions or the growth of the vascular
networks. Microfluidics allow for both spatial and temporal organization.
For example, multiple cell
types can be seeded into the different channels or gel regions, separated by distances of less than one mm,
similar to physiological length scales. Similarly, one cell type can be seeded initially, left to adhere and
stabilize, with another added at a later time point. Using these capabilities, numerous biological
conditions can be simulated including tumor angiogenesis and metastasis [91]. In all cases, chemical
factors secreted by the cells are transported through the hydrogel region that is separating the channels.
1.2.3.2 Tumor angiogenesismodel
Expanding tumors, in particular, actively promote the growth of new blood vessel. Their demands
for gas exchange and nutrients lead to the conditions described above that promote angiogenesis. Not only
37
do tumor cells secrete various growth factors such as VEGF and bFGF in response to the local hypoxia,
but they also disrupt the production of anti-angiogenic enzymes [128]. It has also been found that tumor
cells can create their own blood vessels through a process in which tumor associated stem cells
differentiate into endothelium [129, 130].
The use of microfluidics in studying tumor angiogenesis enables a parametric in vitro study with
tumor cells in close proximity to and actively signaling with endothelial cells. Studies have been
conducted in microfluidic systems under co-culture of human endothelium and various tumor cell lines
(Figure 1.6) [65, 90, 91, 96]. By designating one channel in a 3-channel system as the "condition" channel
and the opposite one as the "control", the effect of different types of cancers on endothelial migration and
vascular sprouting can easily be monitored and quantitatively compared. Such studies could be used to
investigate, for example, phenotypic variations sometimes found in endothelial cells in a tumor
environment [131, 132].
Tumor blood vessels have increased permeability due to vessel dilation and
detachment of pericytes and their morphology is also distorted [133-135].
Figure 1.6 Co-culture of endothelial cells with tumor cells in microfluidic system. Two types of tumor
cells, adenocarcinoma, MTLn3, (a) and glioblastoma, U87MG, (b) cells are migrating towards human
microvascular endothelial cells (HMVECs) through collagen gel region [91] -Copyright 2009 RSC.
38
1.2.4 Maturation/stabilization of blood vessels
The fundamental goal of tissue engineering in regenerative medicine does not end in the creation of
neo-vasculature, but rather, in the construction of a stable vascular network. Once endothelial cells sprout,
proliferate and recruit new cells to the developing vascular network, naked tubular structures of
endothelial cells initially form, but vessel maturation is required for stable, long-term perfusion of blood
[80]. Fully-functional blood vessels are characterized by a central conduit fonned by endothelial cells that
are adherent to basement membrane and encompassed by perivascular cells of various types, and the
overall structure resides in ECM. Depending on the location or function of the vessel, ranging from
arterioles to distal capillaries for example, their functional requirements in terms of size, permeability, or
cell-cell adhesion strength or tightness all vary. Their stability as fully functional microvascular network
is governed by proper organization among the different cells and their environment [136]. Therefore, the
importance of perivascular cells should not be underestimated. Perivascular cells include smooth muscle
cells and pericytes, and they are recruited by endothelial cells once the tubular structures are formed [106,
137]. Initially the naked vessel is highly permeable [114, 138], and perivascular cells work to achieve
stabilization and maturation by means of providing structural integrity and supplying necessary survival
factors. They also secrete proteins that are used to create extracellular matrix [139].
39
Vessel stabilization
S
ECM
Flow
Tightening of vessel
Drot si
Vessel regression
NkdECs
M-j
Bisetng
Vessel regression
VEGF, PIGF, Ang-1, POGF
I TSP, IFN, Ang-2, Inhibitors
Figure 1.7 Maturation of naked endothelial cells (ECs) into stable blood vessel is achieved with addition
of cytokines, recruitment of smooth muscle cells (SMC) and flow. Naked ECs will otherwise regress.
Adapted by permission from Macmillan Publishers Ltd. [140], Copyright 2003 NPG.
The importance of these accessory cells is underscored by the fact that the engineered blood vessels
have often been found to be immature and unstable [113, 141]. However, it has been reported that when
endothelial cells were co-cultured with appropriate perivascular cells, a stable and long lasting vasculature
could be formed in vivo [136, 142, 143]. The necessity of the presence of pericytes and smooth muscle
cells for providing structural strength and regulation of perfusion on nascent endothelial vessels is once
again confirmed.
Fluid shear stress has also been found to be a crucial factor in maturation of blood vessels in
addition to its aforementioned effects in inducing angiogenesis. The growth factors induced by shear that
are particularly involved with collateral growth through stimulation of endothelium and smooth muscle
cells include TGF-pl, TNF-a, PIGF, and MCP-l [105, 144, 145]. Under low- or no shear conditions,
vessel regression has been observed, which indicates that fluid shear is an important factor in vessel
maturation and maintenance [84, 115, 140, 146].
40
1.3 Pros and cons of a microfluidic approach
Many of the advantages to be gained by using microfluidics have been discussed above. Included
among these are: the capability of simultaneous 2D and 3D culture, heterotypic culture methods, ease of
imaging, ease of attaining physiological length scales to allow for realistic cell-cell communication, the
capability to establish gradients in growth factors or fluid pressure, and for the application of shear stress.
Although there is much to be gained through a microfluidic approach to simulating angiogenesis or
vasculogenesis, there are also some drawbacks that need to be recognized. First, while the small volume
is advantageous from the perspectives of facilitating high throughput studies, keeping costs low, and ease
of imaging, it can also pose problems, chief among them being that many of the more conventional assays
of biological function (e.g., Western blots, Northern blots) are difficult or even impossible to perform
with such small numbers of cells. Small volumes can also pose challenges in terms of the initial filling of
the device and subsequent media changes.
Surface properties of the devices are paramount since the
wetting characteristics determine to a large extent the ease with which the gel solutions or media can be
introduced into an initially dry system.
Small volumes also lead to large surface-to-volume ratios,
meaning that conventional rules of thumb for frequency of medium changes, for example, need to be reevaluated. This topic has been addressed by Young & Beebe through the introduction of the concepts of
"effective culture time" and "critical perfusion rate" [147], the latter being relevant to systems in which
the cells are nourished by means of a slow, constant rate of flow of medium through the system channels.
Another complication arises when cells or vascular structures experience a strong interaction with the
device boundaries. As was seen in one set of experiments on angiogenesis, if cell adhesion to the walls of
the system dominates over matrix adhesion, endothelial cells can migrate into the gel along the surface
(sometimes referred to as migration in 2.5D) [92]. And even though surface migration can give way to the
formation of tubular structures, the process by which these form and their morphology can differ
considerably from the process that occurs in vivo. These concepts pertain not just to angiogenesis, but to
all cell culture methods in microfluidic systems.
41
1.4 Thesis overview
This thesis aims to develop an in vitro microfluidic assay and to use it for studying cancer cell
extravasation. Following the introduction and background information in this chapter 1, a general nonorgan specific microfluidic model for extravasation is described in detail in chapter 2. In this model, the
endothelial cells that cover the walls of the microfluidic channel represent the vessel endothelium, and the
entire extravasation process including tumor cell adhesion to the endothelium and the subsequent
transmigration can be observed. Chapter 3 provides a comprehensive description of a model, which is
developed for mimicking the organ-specific extravasation and investigating the preference of cancer cells
in targeting the specific organs for metastasis. The improved model was used to study the specificity of
human breast cancer metastases to bone, by recreating a vascularized bone-mimicking microenvironment.
The tri-culture system allowed us to study the transendothelial migration of highly metastatic breast
cancer cells and to monitor their behavior within the bone-like matrix. In chapter 4, the functional
microvascular networks were generated in the microfluidic system by vasculogenesis with addition of
mural cell types and pro-angiogenic factors to better replicate the normal physiological vasculature of the
remote site for metastasis. Chapter 5 describes a system in which the vasculogenesis approach was
combined with the bone-mimicking model to develop a functional osteo-cell conditioned vasculature
model to study physiologically relevant extravasation in a bone-like microenvironment. Finally in chapter
6, the findings of each chapter are summarized and directions for future research as well as the
implications of using in vitro microfluidic system for cancer cell extravasation are discussed. In addition,
I would like to note that parts of this dissertation cover research reported in the following articles:
1.
2.
3.
Bersini, S., Jeon, J.S., et al., In vitro models of metastatic cascade: from local invasion ot
extravasation. Drug Discovery Today: Technologies, in press.
Jeon, J.S., S. Chung, and R.D. Kamm, Chapter 16 - Microfluidic Platforms for Evaluating
Angiogenesis and Vasculogenesis, in Microfluidic Cell Culture Systems, C. Bettinger, J.T.
Borenstein, and S.L. Tao, Editors. 2013, William Andrew Publishing: Oxford. p. 385-403.
Jeon, J.S., et al., In Vitro Model of Tumor Cell Extravasation.Plos One, 2013. 8(2).
42
4.
Bersini, S., Jeon, J.S., et al., 3D in vitro model br speciaicity of breast cancer metastasis to bone.
Biomaterials, in press.
5.
Jeon, J.S., et al., Generation of 3D functional microvascular networks with mural celldifferentiated human mesenchymal stem cells. submitted.
43
References
1.
2.
3.
4.
5.
6.
7.
8.
Bersini, S., et al., In vitro models of metastatic cascade: from local invasion ot extravasation.
Drug Discovery Today: Technologies, in press.
Jeon, J.S., S. Chung, and R.D. Kamm, Chapter 16 - Microfluidic Platforms for Evaluating
Angiogenesis and Vasculogenesis, in Microfluidic Cell Culture Systems, C. Bettinger, J.T.
Borenstein, and S.L. Tao, Editors. 2013, William Andrew Publishing: Oxford. p. 385-403.
Sporn, M.B., The war on cancer. Lancet, 1996. 347(9012): p. 1377-81.
AmericanCancerSociety, Cancer Facts & Figures 2013, 2013.
Leung, C.T. and J.S. Brugge, Outgrowth of single oncogene-expressing cells from suppressive
epithelialenvironments. Nature, 2012. 482(7385): p. 410-3.
Kaplon, J., et al., A key role for mitochondrialgatekeeperpyruvate dehydrogenase in oncogeneinduced senescence. Nature, 2013. 498(7452): p. 109-12.
Owens, P., et al., Bone morphogenetic proteins stimulate mammary fibroblasts to promote
mammary carcinoma cell invasion. PLoS One, 2013. 8(6): p. e67533.
Chaffer, C.L. and R.A. Weinberg, A perspective on cancer cell metastasis. Science, 2011.
331(6024): p. 1559-64.
9.
10.
11.
12.
13.
Shin, Y., et al., Microfluidic assayfor simultaneous culture of multiple cell types on surfaces or
within hydrogels. Nat Protoc, 2012. 7(7): p. 1247-59.
Roussos, E.T., J.S. Condeelis, and A. Patsialou, Chemotaxis in cancer. Nat Rev Cancer, 2011.
11(8): p. 573-87.
Lee, J., M.J. Cuddihy, and N.A. Kotov, Three-dimensionalcell culture matrices: state of the art.
Tissue Eng Part B Rev, 2008. 14(1): p. 61-86.
Yamada, K.M. and E. Cukierman, Modeling tissue morphogenesis and cancer in 3D. Cell, 2007.
130(4): p. 601-10.
Whitesides, G.M., et al., Soft lithography in biology and biochemistry. Annu Rev Biomed Eng,
2001. 3: p.
14.
15.
3 3 5 -7 3 .
Chung, S., et al., Microfluidicplatformsfor studies of angiogenesis, cell migration,and cell-cell
interactions. Sixth InternationalBio-Fluid Mechanics Symposium and Workshop March 28-30,
2008 Pasadena,California.Ann Biomed Eng, 2010. 38(3): p. 1164-77.
Thuma, F., H. Ngora, and M. Zoller, The metastasis-associatedmolecule C4.4A promotes tissue
invasion and anchorage independence by associatingwith the alpha6beta4 integrin. Mol Oncol,
2013.
16.
17.
Chambers, A.F., A.C. Groom, and I.C. MacDonald, Disseminationand growth of cancer cells in
metastatic sites. Nat Rev Cancer, 2002. 2(8): p. 563-72.
Valastyan, S. and R.A. Weinberg, Tumor metastasis: molecular insights and evolving paradigms.
18.
Cell, 2011. 147(2): p. 2 7 5 - 9 2 .
Fidler, 1.J., The pathogenesis of cancer metastasis: the 'seed and soil' hypothesis revisited. Nat
19.
Rev Cancer, 2003. 3(6): p. 453-8.
Gupta, G.P. and J. Massague, Cancer metastasis: building a framework. Cell, 2006. 127(4): p.
679-95.
20.
21.
22.
23.
Hanahan, D. and R.A. Weinberg, The hallmarks of cancer. Cell, 2000. 100(1): p. 57-70.
Joyce, J.A. and J.W. Pollard, Microenvironmental regulation of metastasis. Nat Rev Cancer,
2009. 9(4): p. 239-52.
Al-Mehdi, A.B., et al., Intravascularorigin of metastasisfrom the proliferation of endotheliumattached tumor cells: a new modelfor metastasis.Nat Med, 2000. 6(l): p. 100-2.
Kebers, F., et al., Induction of endothelial cell apoptosis by solid tumor cells. Exp Cell Res, 1998.
240(2): p. 197-205.
44
24.
25.
26.
27.
28.
29.
Miles, F.L., et al., Stepping out of the flow: capillary extravasation in cancer metastasis. Clin
Exp Metastasis, 2008. 25(4): p. 305-24.
Fukuda, M., N. Hiraoka, and J.C. Yeh, C-type lectins and sialyl Lewis X oligosaccharides.
Versatile roles in cell-cell interaction. J Cell Biol, 1999. 147(3): p. 467-70.
Zipin, A., et al., Tumor-microenvironment interactions: the fIicose-generating FX enzyme
controls adhesive properties of colorectal cancer cells. Cancer Res, 2004. 64(18): p. 6571-8.
Khatib, A.M., et al., Characterizationof the host proinflammatory response to tumor cells during
the initialstages of liver metastasis. Am J Pathol, 2005. 167(3): p. 749-59.
Crissman, J.D., et al., Morphological study of the interaction of intravasculartumor cells with
endothelialcells and subendothelialmatrix. Cancer Res, 1988. 48(14): p. 4065-72.
Paget, S., The distributionof secondary growths in cancer of the breast. 1889. Cancer Metastasis
Rev, 1989. 8(2): p. 98-101.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
Psaila, B. and D. Lyden, The metastatic niche: adapting thefJreign soil. Nat Rev Cancer, 2009.
9(4): p. 285-93.
Nguyen, D.X., P.D. Bos, and J. Massague, Metastasis: from dissemination to organ-specific
colonization. Nat Rev Cancer, 2009. 9(4): p. 274-84.
Pasqualini, R. and E. Ruoslahti, Organ targeting in vivo using phage display peptide libraries.
Nature, 1996. 380(6572): p. 364-6.
Uehara, H., et al., Effects of blocking platelet-derived growth factor-receptor signaling in a
mouse model of experimentalprostate cancer bone metastases. J Natl Cancer Inst, 2003. 95(6): p.
458-70.
Hiratsuka, S., et al., Tumour-mediated upregulation of chemoattractants and recruitment of
myeloid cells predetermines lung metastasis. Nat Cell Biol, 2006. 8(12): p. 1369-75.
Hiratsuka, S., et al., The SJ0OA8-serum amyloid A3-TLR4 paracrinecascade establishes a premetastaticphase. Nat Cell Biol, 2008. 10(11): p. 1349-55.
Kaplan, R.N., et al., VEGFR]-positive haematopoietic bone marrow progenitors initiate the premetastatic niche. Nature, 2005. 438(7069): p. 820-7.
Bussard, K.M., C.V. Gay, and A.M. Mastro, The bone microenvironment in metastasis: what is
specialabout bone? Cancer Metastasis Rev, 2008. 27(1): p. 41-55.
Coleman, R.E., Skeletal complications of malignancy. Cancer, 1997. 80(8 Suppl): p. 1588-94.
Bos, P.D., et al., Genes that mediate breast cancer metastasis to the brain. Nature, 2009.
459(7249): p. 1005-9.
Minn, A.J., et al., Genes that mediate breast cancer metastasis to lung. Nature, 2005. 436(7050):
p. 518-24.
Kang, Y., et al., A multigenic program mediating breast cancer metastasis to bone. Cancer Cell,
2003. 3(6): p. 537-49.
Hsu, Y.L., et al., Breast tumor-associated osteoblast-derived CXCL5 increases cancer
progressionby ERK/MSKI/Elk- i/Snail signalingpathway. Oncogene, 2012.
Claffey, K.P., et al., Expression of vascular permeability factor/vascular endothelial growth
factor by melanoma cells increases tumor growth, angiogenesis, and experimental metastasis.
Cancer Res, 1996. 56(1): p. 172-81.
Shibue, T. and R.A. Weinberg, Integrin betal-focal adhesion kinase signaling directs the
proliferation of metastatic cancer cells disseminated in the lungs. Proc Natl Acad Sci U S A,
2009. 106(25): p. 10290-5.
MacDonald, I.C., A.C. Groom, and A.F. Chambers, Cancer spread and micrometastasis
development: quantitativeapproachesfor in vivo models. Bioessays, 2002. 24(10): p. 885-93.
Goldstein, R.H., R.A. Weinberg, and M. Rosenblatt, Of mice and (wo)men: mouse models of
breast cancer metastasis to bone. J Bone Miner Res, 2010. 25(3): p. 431-6.
Kuperwasser, C., et al., A mouse model of human breast cancer metastasis to human bone.
Cancer Res, 2005. 65(14): p. 6130-8.
45
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
Hendrix, M.J., et al., A simple quantitative assay fr studying the invasive potential of high and
low human metastatic variants.Cancer Lett, 1987. 38(1-2): p. 137-47.
Mercurio, A.M. and I. Rabinovitz, Towards a mechanistic understanding of tumor invasion-lessonsfrom the alpha6beta 4 integrin. Semin Cancer Biol, 2001. 11(2): p. 129-41.
Mierke, C.T., Cancer cells regulate biomechanical properties of human microvascular
endothelial cells. J Biol Chem, 2011. 286(46): p. 40025-37.
Kramer, R.H. and G.L. Nicolson, Interactions of tumor cells with vascular endothelial cell
monolayers: a modelfor metastatic invasion. Proc Natl Acad Sci U S A, 1979. 76(11): p. 5704-8.
Abbott, A., Cell culture: biology's new dimension. Nature, 2003. 424(6951): p. 870-2.
Lii, J., et al., Real-time microfluidic system for studying mammalian cells in 3D
microenvironments. Anal Chem, 2008. 80(10): p. 3640-7.
Huang, Y., et al., Microfluidics-baseddevices: New tools for studying cancer and cancer stem
cell migration.Biomicrofluidics, 2011. 5(1): p. 13412.
Haessler, U., et al., Migration dynamics of breast cancer cells in a tunable 3D interstitialflow
chamber. Integr Biol (Camb), 2012. 4(4): p. 401-9.
Liu, T., et al., A microfluidic device for characterizingthe invasion of cancer cells in 3-D matrix.
Electrophoresis, 2009. 30(24): p. 4285-91.
Sung, K.E., et al., Transition to invasion in breast cancer: a microfluidic in vitro model enables
examination ofspatialand temporal effects. Integr Biol (Camb), 2011. 3(4): p. 439-50.
Zervantonakis, I.K., et al., Three-dimensionalmicrofluidic model for tumor cell intravasationand
endothelial barrierftnction.Proc Natl Acad Sci U S A, 2012. 109(34): p. 13515-20.
Song, J.W., et al., Microfluidic endothelium for studying the intravascularadhesion of metastatic
breastcancer cells. PLoS One, 2009. 4(6): p. e5756.
Shin, M.K., S.K. Kim, and H. Jung, Integration of intra- and extravasation in one cell-based
microfluidic chipfor the study of cancer metastasis. Lab Chip, 2011. 11(22): p. 3880-7.
Zhang, Q., T. Liu, and J. Qin, A microfluidic-baseddevice for study of transendothelialinvasion
of tumor aggregates in realtime. Lab Chip, 2012. 12(16): p. 2837-42.
Jeon, J.S., et al., In vitro model of tumor cell extravasation.PLoS One, 2013. 8(2): p. e56910.
Chen, M.B., et al., Mechanisms of tumor cell extravasation in an in vitro microvascularnetwork
platform. Integr Biol (Camb), 2013. 5(10): p. 1262-7 1.
Chaw, K.C., et al., Multi-step microfluidic devicefbr studying cancer metastasis. Lab Chip, 2007.
7(8): p. 1041-7.
Song, J.W., et al., Microfluidic Endothelium for Studying the Intravascular Adhesion of
MetastaticBreast Cancer Cells. Plos One, 2009. 4(6): p. -.
Zhang, H., et al., HIF-1-dependent expression of angiopoietin-like 4 and LiCAM mediates
vascular metastasis of hypoxic breast cancer cells to the lungs. Oncogene, 2012. 31(14): p. 1757-
70.
67.
Chau, L., M. Doran, and J. Cooper-White, A novel multishear microdevice for studying cell
mechanics. Lab Chip, 2009. 9(13): p. 1897-902.
68.
69.
70.
71.
Bianchi, E., et al., Microfluidics for in vitro biomimetic shear stress-dependent leukocyte
adhesion assays. J Biomech, 2013. 46(2): p. 276-83.
Hanzlik, J., E. Cretekos, and K.A. Lamkin-Kennard, Biomimetic leukocyte adhesion: a review of
microfluidic and computational approaches and applications. Journal of Bionic Engineering,
2008. 5: p. 317-327.
Padua, D., et al., TGFbeta primes breast tumors for lung metastasis seeding through
angiopoietin-like 4. Cell, 2008. 133(1): p. 66-77.
Saiki, I., et al., Functional role of sialyl Lewis X andfibronectin-derivedRGDSpeptide analogue
on tumor-cell arrestin lungsfollowed by extravasation.Int J Cancer, 1996. 65(6): p. 833-9.
46
72.
73.
74.
75.
Hangan, D., et al., An epitope on VLA-6 (alpha6betal) integrin involved in migration but not
adhesion is requiredfbr extravasation of murine melanoma B16F] cells in liver. Cancer Res,
1997. 57(17): p. 3812-7.
Bondareva, A., et al., The lvsyl oxidase inhibitor, beta-aminopropionitrile,diminishes the
metastatic colonization potential of circulating breast cancer cells. PLoS One, 2009. 4(5): p.
e5620.
Camphausen, K., et al., Radiation therapy to a primary tumor accelerates metastatic growth in
mice. Cancer Res, 2001. 61(5): p. 2207-11.
Hamalukic, M., et al., Rac1-regulated endothelial radiationresponse stimulates extravasation
and metastasis that can be blocked by HMG-CoA reductase inhibitors. PLoS One, 2011. 6(10): p.
e26413.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
Tanaka, T., et al., Dynamic analysis of lung metastasis by mouse osteosarcoma LM8: VEGF is a
candidatefJranti-metastasistherapy. Clin Exp Metastasis, 2013. 30(4): p. 369-79.
Stoletov, K., et al., Visualizing extravasation dynamics of metastatic tumor cells. J Cell Sci, 2010.
123(Pt 13): p. 2332-41.
Schumacher, D., et al., Platelet-derived nucleotides promote tumor-cell transendothelial
migration and metastasis via P2Y2 receptor. Cancer Cell, 2013. 24(1): p. 130-7.
Folkman, J., Angiogenesis in Cancer, Vascular, Rheumatoid and Other Disease. Nature
Medicine, 1995. 1(1): p. 27-3 1.
Carmeliet, P., Angiogenesis in life, disease and medicine. Nature, 2005. 438(7070): p. 932-936.
Adams, R.H. and K. Alitalo, Molecular regulation of angiogenesis and lymphangiogenesis.
Nature Reviews Molecular Cell Biology, 2007. 8(6): p. 464-478.
Carmeliet, P., Mechanisms of angiogenesis and arteriogenesis.Nature Medicine, 2000. 6(4): p.
389-395.
Carmeliet, P., et al., Role of HIF-I alpha in hypoxia-mediated apoptosis, cell proliferation and
tumour angiogenesis (vol 394, pg 485, 1998). Nature, 1998. 395(670 1): p. 525-525.
Jain, R.K., Molecular regulation of vessel maturation. Nature Medicine, 2003. 9(6): p. 685-693.
Carmeliet, P. and R.K. Jain, Angiogenesis in cancer and other diseases. Nature, 2000. 407(680 1):
p. 249-257.
Folkman, J. and Y. Shing, Angiogenesis. Journal of Biological Chemistry, 1992. 267(16): p.
10931-10934.
87.
88.
89.
90.
91.
92.
93.
94.
Quake, S.R., T. Thorsen, and S.J. Maerkl, Microfluidic large-scale integration. Science, 2002.
298(5593): p. 580-584.
Rajaraman, S., et al., Microfabrication technologies fJr a coupled three-dimensional
microelectrode, microfluidic array. Journal of Micromechanics and Microengineering, 2007.
17(1): p. 163-171.
Kothapalli, C.R., et al., A high-throughputmicrofluidic assay to study neurite response to growth
factor gradients. Lab on a Chip, 2011. 11(3): p. 497-507.
Stroock, A.D. and C. Fischbach, Microfluidic Culture Models of Tumor Angiogenesis. Tissue
Engineering Part A, 2010. 16(7): p. 2 1 4 3 - 2 14 6 .
Chung, S., et al., Cell migration into scaffolds under co-culture conditions in a microjluidic
platform. Lab on a Chip, 2009. 9(2): p. 269-275.
Vickerman, V., et al., Design,fibrication and implementation of a novel multi-parametercontrol
microfluidic platfbrm for three-dimensional cell culture and real-time imaging. Lab on a Chip,
2008. 8(9): p. 1468-1477.
Jeon, N.L., et al., Engineering microscale cellular nichesfor three-dimensional multicellular cocultures. Lab on a Chip, 2009. 9(12): p. 1740-1748.
Manimaran, M., et al., Multi-step microfluidic device fbr studying cancer metastasis. Lab on a
Chip, 2007. 7(8): p. 1041-1047.
47
95.
96.
Manimaran, M., et al., Matrigel coated polydimethylsiloxane based microfluidic devices for
studying metastatic and non-metastatic cancer cell invasion and migration. Biomedical
Microdevices, 2007. 9(4): p. 597-602.
Cross, V.L., et al., Dense type I collagen matrices that support cellular remodeling and
microfabrication for studies of tumor angiogenesis and vasculogenesis in vitro. Biomaterials,
2010. 31(33): p. 8596-8607.
97.
98.
99.
100.
101.
102.
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
Amadi, O.C., et al., A low resistancemicrofluidic system for the creation of stable concentration
gradients in a defined 3D microenvironment. Biomedical Microdevices, 2010. 12(6): p. 10271041.
Chung, S., et al., Microfluidic Platformsfor Studies of Angiogenesis, Cell Migration, and CellCell Interactions.Annals of Biomedical Engineering, 2010. 38(3): p. 1164-1177.
Shin, Y., et al., In vitro 3D collective sprouting angiogenesis under orchestrated ANG-] and
VEGF gradients.Lab on a Chip, 2011. 11(13): p. 2175-2181.
Zervantonakis, I.K., et al., Microfluidic devices for studying heterotypic cell-cell interactionsand
tissue specimen cultures under controlled microenvironments. Biomicrofluidics, 2011. 5(1): p. -.
Folkman, J. and M. Klagsbrun, Angiogenic Factors. Science, 1987. 235(4787): p. 442-447.
Folkman, J. and M. Klagsbrun, A Family of Angiogenic Peptides. Nature, 1987. 329(6141): p.
671-672.
Giraudo, E., et al., Tumor necrosis factor-alpha regulates expression of vascular endothelial
growth factor receptor-2 and of its co-receptor neuropilin-I in human vascular endothelial cells.
Journal of Biological Chemistry, 1998. 273(34): p. 22128-22135.
Au, P., et al., Paradoxical Effects of PDGF-BB Overexpression in Endothelial Cells on
EngineeredBlood Vessels In Vivo. American Journal of Pathology, 2009. 175(1): p. 294-302.
Cao, R.H., et al., Angiogenic synergism, vascular stability and improvement of hind-limb
ischemia by a combination of PDGF-BB and FGF-2. Nature Medicine, 2003. 9(5): p. 604-613.
Gerhardt, H. and C. Betsholtz, Endothelial-pericyteinteractions in angiogenesis. Cell and Tissue
Research, 2003. 314(1): p. 15-23.
Klagsbrun, M. and M.A. Moses, Molecular angiogenesis. Chemistry & Biology, 1999. 6(8): p.
R217-R224.
Kamihata, H., et al., Improvement of collateralperfusion and regionalfunction by implantationof
peripheral blood mononuclear cells into ischemic hibernating myocardium. Arteriosclerosis
Thrombosis and Vascular Biology, 2002. 22(11): p. 1804-1810.
Verbridge, S.S., et al., Oxygen-Controlled Three-Dimensional Cultures to Analyze Tumor
Angiogenesis. Tissue Engineering Part A, 2010. 16(7): p. 2 1 3 3 -2 1 4 1 .
Gerhardt, H., et al., VEGF guides angiogenic sprouting utilizing endothelial tip cell filopodia.
Journal of Cell Biology, 2003. 161(6): p. 1163-1177.
Carmeliet, P. and R.K. Jain, Molecular mechanisms and clinical applications of angiogenesis.
Nature, 2011. 473(7347): p. 298-307.
Joukov, V., et al., A novel vascular endothelial growth factor, VEGF-C, is a ligandfor the Flt4
(VEGFR-3) and KDR (VEGFR-2) receptor tyrosine kinases. Embo Journal, 1996. 15(2): p. 290-
298.
113.
114.
115.
116.
Albelda, S.M., et al., Permeability Characteristicsof Cultured Endothelial-Cell Monolayers.
Journal of Applied Physiology, 1988. 64(1): p. 308-322.
Pettersson, A., et al., Heterogeneity of the angiogenic response induced in different normal adult
tissues by vascular permeability factor/vascular endothelial growth factor. Laboratory
Investigation, 2000. 80(1): p. 99-115.
Tien, J., et al., Effect of mechanical factors on the function of engineered human blood
microvessels in microfluidic collagen gels. Biomaterials, 2010. 31(24): p. 6182-6189.
Milkiewicz, M., et al., Association between shear stress, angiogenesis, and VEGF in skeletal
muscles in vivo. Microcirculation, 2001. 8(4): p. 229-241.
48
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
135.
136.
137.
Resnick, N., et al., Fluid shear stress and the vascular endothelium: for better and for worse.
Progress in Biophysics & Molecular Biology, 2003. 81(3): p. 177-199.
Risau, W., Mechanisms of angiogenesis.Nature, 1997. 386(6626): p. 671-674.
Franke, H., Nature and Significance of Polypathy and Multimorbiditv in Geriatrics. Internist,
1984. 25(8): p. 451-455.
Resnick, N. and M.A. Gimbrone, Hemodynamic Forces Are Complex Regulators of Endothelial
Gene-Expression.Faseb Journal, 1995. 9(10): p. 874-882.
Cummins, P.M., et al., Regulation of bovine brain microvascular endothelial tight junction
assembly and barrierfunction by laminar shear stress. American Journal of Physiology-Heart
and Circulatory Physiology, 2007. 292(6): p. H3190-H3197.
Yamamoto, K., et al., Proliferation,dif/erentiation,and tube formation by endothelial progenitor
cells in response to shear stress. Journal of Applied Physiology, 2003. 95(5): p. 2081-2088.
Wilson, W.R. and M.P. Hay, Targeting hypoxia in cancer therapy. Nature Reviews Cancer, 2011.
11(6): p. 393-410.
Mole, D.R. and P.J. Ratcliffe, Cellular oxygen sensing in health and disease. Pediatric
Nephrology, 2008. 23(5): p. 681-694.
Wang, N. and D.E. Ingber, Control of Cytoskeletal Mechanics by Extracellular-Matrix, CellShape, and Mechanical Tension. Biophysical Journal, 1994. 66(6): p. 2181-2189.
Takayama, S., et al., Leakage-free bonding of porous membranes into layered microfluidic array
systems. Analytical Chemistry, 2007. 79(9): p. 3504-3508.
Lammertink, R.G.H., J. de Jong, and M. Wessling, Membranes and microfluidics: a review. Lab
on a Chip, 2006. 6(9): p. 1125-1139.
Ying, L. and L.J. Hofseth, An emerging role for endothelial nitric oxide synthase in chronic
inflammation and cancer. Cancer Research, 2007. 67(4): p. 1407-14 10.
Wang, R., et al., Glioblastoma stem-like cells give rise to tumour endothelium. Nature, 2010.
468(7325): p. 829-U128.
Ricci-Vitiani, L., et al., Tumour vascularization via endothelial differentiation of glioblastoma
stem-like cells. Nature, 2010. 468(7325): p. 824-U121.
Hida, K., et al., Tumor-associated endothelial cells with cytogenetic abnormalities. Cancer
Research, 2004. 64(22): p. 8249-8255.
Hida, K. and N. Klagsbrun, A new perspective on tumor endothelial cells: Unexpected
chromosome and centrosome abnormalities.Cancer Research, 2005. 65(7): p. 2507-2510.
Ryschich, E., et al., Transfbrmationof the microvascular system during multistage tumorigenesis.
International Journal of Cancer, 2002. 97(6): p. 719-725.
van Kempen, L.C.L., et al., Epithelialcarcinogenesis:dynamic interplay between neoplastic cells
and their microenvironment. Differentiation, 2002. 70(9-10): p. 610-623.
Chen, J., D. Brantley-Siders, and J.S. Penn, Eph receptor tyrosine kinases: Modulators of
angiogenesis.Retinal and Choroidal Angiogenesis, 2008: p. 203-219.
Koike, N., et al., Creation of long-lasting blood vessels. Nature, 2004. 428(6979): p. 138-139.
Hirschi, K.K. and P.A. DAmore, Pericytes in the microvasculature. Cardiovascular Research,
1996. 32(4): p. 687-698.
138.
139.
140.
141.
Au, P., et al., Bone marrow-derivedmesenchymal stem cells facilitateengineering of long-lasting
functional vasculature.Blood, 2008. 111(9): p. 4551-8.
Hirschi, K.K., et al., Vascular assembly in natural and engineered tissues. Reparative Medicine:
Growing Tissues and Organs, 2002. 961: p. 223-242.
Carmeliet, P., Angiogenesis in health and disease. Nature Medicine, 2003. 9(6): p. 653-660.
Schechner, J.S., et al., In vivo formation of complex microvessels lined by human endothelial cells
in an immunodeficient mouse. Proceedings of the National Academy of Sciences of the United
States of America, 2000. 97(16): p. 9191-9196.
49
142.
143.
Au, P., et al., Differential in vivo potential of endothelialprogenitor cells from human umbilical
cord blood and adult peripheral blood to form functional long-lasting vessels. Blood, 2008.
111(3): p. 1302-1305.
Jain, R.K., et al., Engineering vascularized tissue. Nature Biotechnology, 2005. 23(7): p. 821-
823.
144.
145.
Pipp, F., et al., VEGFR- I-selective VEGF homologue PIGF is arteriogenic - Evidence for a
monocyte-mediated mechanism. Circulation Research, 2003. 92(4): p. 3 78-385.
Luttun, A., et al., Revascularization of ischemic tissues by PIGF treatment, and inhibition of
tumor angiogenesis, arthritis and atherosclerosis by anti-Fltl. Nature Medicine, 2002. 8(8): p.
831-840.
146.
147.
Conway, E.M., D. Collen, and P. Carmeliet, Molecular mechanisms of blood vessel growth.
Cardiovascular Research, 2001. 49(3): p. 507-521.
Beebe, D.J. and E.W.K. Young, Fundamentals of microfluidic cell culture in controlled
microenvironments. Chemical Society Reviews, 2010. 39(3): p. 1036-1048.
50
Chapter 2
In vitro model of tumor cell extravasation2
2.1 Introduction
Tumor metastasis is the hallmark of malignant cancer and the cause of 90% human cancer deaths
[2, 3]. Thus the real threat of cancer is that malignant tumor cells are able to escape from the primary site
and form metastatic colonies in secondary sites. During metastasis, epithelial cancer cells undergo
epithelial-mesenchymal transition (EMT), disperse from the primary tumor, and intravasate into the
vascular system. Cancer cells, once in the circulation, are transported to a remote site where they can
extravasate from the vascular system into the surrounding tissue to colonize at remote sites, completing
the dissemination process [4, 5]. While there exists an enormous literature on oncogenic transformation
and emergence of the primary tumor, much less research addresses issues related to metastasis [6]. There
is little doubt that a deeper understanding of cancer metastasis could lead to novel therapeutic strategies
targeting the invasion pathways and improving cancer survival rates [7].
Extravasation is a vital step in cancer cell dissemination, which enables successful establishment
of a secondary metastasis. The process of extravasation consists of: 1) transport via blood circulation, 2)
arrest adjacent to a vessel wall, and 3) transmigration across the endothelial monolayer into the secondary
site [8]. For tumor cell arrest on vessel wall, two possible modes have been proposed. One, proposed by
2
This chapter is modified from Ref. [1] with the publisher's permission.
51
Paget as the "seed and soil" hypothesis, is that tumors of different organs show unique patterns of
metastatic colonization to specific organs through site-selective adhesion [9]. In a second mode, tumor
cells become trapped in small vessels due to size restriction as tumor cells tend be larger than other
circulating cells and can also aggregate with platelets [10-12]. While both modes have been observed
during extravasation [4, 13-15], it is still not clear which is dominant or whether different tumor types
preferentially exhibit a particular type of arrest prior to transmigration. Furthermore, invasive behavior of
tumor cells depends on cross-talk between tumor and host cells in a complex three dimensional (3D)
microenvironment [16]. Direct observation of tumor cell arrest on an endothelium with controlled
microenvironmental conditions would provide useful insight into this crucial step of extravasation. Also
the establishment of secondary metastases at a distant organ after transmigration requires tumor cell
interaction with a diverse array of extracellular matrix (ECM) components, such as collagen, laminin and
fibronectin [17]. However, the roles of microenvironmental cues and cytokine gradients within the tissue
during the process of extravasation are not well understood.
Conventional studies of extravasation rely primarily on tail-vein injection of tumor cells with
subsequent imaging and analysis in vivo [18, 19]. Although these in vivo experiments provide the most
physiologically representative conditions for extravasation, they have limitations in studying tumor and
vessel interactions as videomicroscopy provides only limited visualization of the event, and tightlyregulated parametric studies are not possible. In vitro models offer solutions to these problems, which led
to widespread use of the Boyden chamber for simulating the invasion or migration of cancer cells [20,
21]. The relative simplicity of operation is an advantage of this system, but there are limitations in using it
for studying complex interactions between cancer cells and the endothelium. The Boyden chamber has
limited control over the local microenvironment and less than optimal imaging capabilities. In an attempt
to address these needs, there has been a growing interest using microfluidic technology since it provides a
simple yet effective means to investigate these phenomena under tight control of the biochemical and
biophysical environment [22-25].
52
We have previously reported an in vitro microfluidic platform that offers the capability to more
realistically mimic the 3D in vivo situation in a controlled environment while simultaneously providing in
situ imaging capabilities for visualization, thereby enabling quantification of cell-cell and cell-matrix
interactions [26-29]. Moreover, the system enables parametric study of multiple factors in controlled and
repeatable conditions as well as study with multiple cell types with an endothelial barrier [27, 30, 31].
While no in vitro systems can fully replicate the in vivo situation, microfluidics offers the opportunity to
create organ-specific microenvironments to explore the different metastatic patterns of different cancer
types in a regulated, and easily-visualized model.
Microfluidic platforms of various designs have been previous employed to study cell migration
and tumor cell intravasation [25, 32]. In this chapter, we used the established microfluidic system to
investigate the critical steps of cancer extravasation -- tumor cell adhesion to the endothelium,
transmigration across the endothelial monolayer, proliferation in remote tissues -- and its consequences.
Our experimental platform mimics the tumor microenvironment, allows for high resolution imaging of
tumor cell extravasation and early steps of colonization, thus enabling better quantification of the critical
metrics of cancer cell invasiveness.
2.2 Materials and Methods
2.2.1 Microfluidic system
In these studies we used a previously developed microfluidic system consisting of three
independently addressable media channels, separated by chambers into which an ECM-mimicking gel can
be injected (Figure 2.IA). Details of the design and the steps required for fabrication of the systems in
PDMS have been described previously [26, 29, 31]. In brief, the microfluidics system consists of molded
PDMS (poly-dimethyl siloxane; Silgard 184; Dow Chemical, MI) through which access ports are bored
and bonded to a cover glass to form a microfluidic channels. Channel cross-sectional dimensions are Imm
(width) by 120 [tm (height). The PDMS layer is formed from a patterned SU8 photoresist on a silicon
53
wafer using soft-lithography.
To enhance matrix adhesion, the PDMS channels are coated with a PDL
(poly-D-lysine hydrobromide; I mg/ml; Sigma-Aldrich, St. Louis, MO) solution. Next, collagen type I
(BD Biosciences, San Jose, CA, USA) solution (2.0 mg/ml) with phosphate-buffered saline (PBS; Gibco)
and NaOH is injected into the gel regions of the device via 4 separate filling ports using a 10 [tl pipette
and incubated for 30 min to form a hydrogel, chosen to represent ECM in 3D space. When the gel is
polymerized, endothelial cell medium is immediately pipetted into the channels to prevent dehydration of
the gel. Upon aspirating the medium, diluted Matrigel T" (BD science) solution (3.0 mg/ml) is introduced
into the cell channel and the excess Matrigel'" solution is washed away I minute later using cold
medium. 2D top and face views of the device are shown in Figure 2.lB-C to show how this microfluidic
system is used to model extravasation. Endothelial cells are first introduced to cover the entire middle
channel and later cancer cells are introduced so they adhere to and transmigrate across the already formed
endothelium into the gel region. The middle channel acts as a cell channel where both endothelial cells
and cancer cells are introduced to form a monolayer and transmigrate, respectively.
54
(a)
3D view
2D top view
(1)front view
0
collanw geo
0
Figure 2.1. General schematic of the device. Microfluidic system consisting of three independently
addressable media channels, separated by chambers into which an ECM-mimicking gel can be injected
(a). Figure 2.1b shows the inside view of the device with endothelial monolayer (blue) covering the center
channel. This channel acts as cell channel where both endothelial cells and cancer cells are introduced to
form monolayer and transmigrate respectively (b). The green region indicates the 3D space filled with
collagen gel and the pink regions indicate the channel filled with medium. Cancer cells which adhere to
endothelial monolayer can extravasate into the collagen gel region as shown in (c).
2.2.2. Cell culture and cell selection
Human microvascular endothelial cells (hMVECs) were commercially obtained (Lonza) and
cultured in endothelial growth medium (EGM-2MV, Lonza).
Cells were cultured in standard culture
flasks and the medium was changed every two days until seeding. During the seeding process, 40RI of
hMVEC suspension at 2x 106 cells/ml was introduced into the prepared microfluidic device. The cells
were kept in a 37*C incubator for 1 hour to allow the adhesion of cells to the collagen scaffold wall. All
experiments were conducted using hMVECs of passage 8 or lower. Human mammary adenocarcinoma
cells (MDA-MB-23 1) were chosen due to their invasiveness and their ability to metastasize in vivo [33,
34].
A GFP-expressing version of the MDA-MB-231 cell line (provided by F. Gertler, MIT) enabled
55
live-cell imaging via fluorescent microscopy. Cancer cell lines were cultured in standard DMEM media
(Sigma) with 10% fetal bovine serum (Invitrogen) and antibiotics. The human mammary epithelial cell
line MCF- I OA (provided by Brugge Lab, Harvard Medical School) was cultured as described previously
[35]. Two days after endothelial cell seeding, tumor cells were introduced into the same channel where
endothelial cells had formed a complete monolayer. Culture flasks containing the tumor cells were first
washed with PBS and the cells were later trypsinized for 5 min to make the cell suspension in cancer cell
medium. For seeding, 40 [l of 50,000 cells/ml tumor cell suspension medium was placed in one side of
the channel reservoir and left to equilibrate. The tumor cell suspension medium in the channel was
removed I hour later and all channels in the device were filled with endothelial cell culture medium.
Control experiment with MCF-IOA was done following the exact tumor cell seeding protocol. All
cultures were kept in a humidified incubator, which was maintained at 37'C and 5% CO 2 .
2.2.3. Permeability of endothelial monolayer
Upon formation of a complete endothelial monolayer by day 2, the diffusive permeability was
measured with fluorescently labeled dextrans in culture medium as shown in Figure 2.2 (10 kDa cascade
blue and 70 kDa MW Texas red, Invitrogen). The endothelial monolayers grown in our microfluidic
system exhibited lower diffusive permeability values for the smaller molecular weight dextran confirm
the presence of a size-selective endothelial barrier. To characterize changes in permeability upon
extravasation, we used the 70 kDa dextran. Before introducing dextran into the device, the endothelium
was first examined using a phase contrast microscope (Nikon, Tokyo, Japan) to confirm monolayer
formation on both the top and the bottom of the channel by focusing at different heights. All medium in
the device reservoirs was aspirated first and later re-filled with control medium in the side channels
whereas the cell-seeded middle channel was filled with fluorescent dextran solution (10 gg/ml) in
medium in the cell-seeded middle channel. Precisely 110 Rl was promptly added to each channel so as to
maintain equal pressures and thereby avoid convective flow across the hydrogel. Devices were then
56
placed in the incubator for 3 hours to reach steady state, fluorescent images of dextran distributions were
taken using an epi-fluorescent microscope (Nikon TE300, Hamamatsu ORCA-ER camera) and processed
using OPENLAB 4.0.4 software. Images were later analyzed using MATLAB to calculate fluorescence
intensity across the monolayer. To determine the diffusional permeability, we calculated the distribution
of fluorescence intensity change as a function of distance perpendicular to the plane of the endothelial
layer. A detailed procedure for measuring permeability has been described previously [25, 36-38]. Briefly,
we used the equation P = D [dC/dx]/ACec
where P is the diffusive permeability (cm/s), dC/dx is the
gradient of the dextran concentration, ACec is the concentration difference across the monolayer, and D is
diffusion coefficient of dextran.
20
E
~15
10
:5
0
10
kDa
70 kDa
Figure 2.2. Size selective permeability.
2.2.4. Immunofluorescent staining and image acquisition
All cells in the device were washed with Phosphate Buffered Saline (PBS) and later fixed with 4%
paraformaldehyde for 15 min. After washing twice with PBS, cells were permeabilized with 0.1% TritonX 100 solution for 5 min and blocked with 5% BSA solution for 5 h. VE-cadherin was labeled with rabbit
57
polyclonal antibody (polyclonal; Alexis Biochemical) at 1:100 dilution and subsequently applied
fluorescently labeled secondary antibody. Cell nuclei were stained with DAPI (Invitrogen) at 1:1000
dilution. All images were obtained using a confocal microscope (Leica) and processed with IMARIS
software.
2.2.5. Metrics for extravasation
Quantitative cell counting was performed after immunofluorescent staining. Confocal data were
analyzed using IMARIS and its tracking algorithms for selecting and counting for nuclei in the specific
region of interest (ROI). The ROI was the 3D gel region between a PDMS post and the wall as seen in
boxed area of Figure 2.lB that was selected during confocal imaging and contained both the endothelial
lining channel region as well as the collagen gel. ROls were selected such that edge effects associated
with PDMS walls and posts were avoided. The dimensions of the ROI were 250 um x 250
sim
x 120 [tm
(height) and each microfluidic device contained total eight RO1s. While each ROls were analyzed
individually, the extravasation percentage was measured per device. As the tumor cells express GFP, cells
with both green and blue signal were counted to track the number of tumor cells.
2.2.6. Statistics
All values reported are averages of measurements from a minimum of 4 devices, each with a
minimum of 2 and maximum of 8 ROls with standard errors. The comparisons between unpaired groups
were assessed using unpaired Student's t-test and the nonparametric Mann-Whitney U statistic whereas
paired permeability measurements were assessed using a paired t-test. Tumor seeding density statistics
were obtained using one-way ANOVA. Statistical significance was assumed for p < 0.05. All tests were
performed with SigmaPlot v.12.
58
2.3 Results and Discussion
2.3.1 Modeling the extravasation process
Although there remains considerable uncertainty regarding the critical, rate-limiting step in the
formation of metastatic tumors, the ability of circulating tumor cells (CTCs) to adhere to and transmigrate
across the endothelium at a remote site is certainly essential. Numerous studies have addressed this issue,
but the challenges of constructing a meaningful in vitro testing platform has been a strong impediment to
improved understanding, and as importantly, has posed a barrier to the identification of drugs that could
inhibit extravasation. Recent studies have begun to address this need using advanced microfluidics [2224], but each is has its limitations. In the current model, we demonstrate the capability of monitoring the
entire process of extravasation. Our previous studies in a similar system have demonstrated changes in
endothelial permeability are closely associated with intravasation [25], so we sought to study similar
changes that might occur during extravasation. In addition, by tracking the cells over time, we were able
to explore the time-dependent behavior, an important factor that impacts both the survival of the CTCs
prior to extravasation as well as their ability to reconfigure the immediate microenvironment prior to
transmigration.
2.3.2 Confirmation of endothelial layer integrity
The microfluidic system was designed to model tumor cell extravasation where the tumor cells
are introduced into a channel lined with a confluent endothelial monolayer. Using phase contrast
microscopy, hMVECs were observed forming a confluent monolayer on the microchannel surfaces and
ECM-endothelial channel interface two days after endothelial cell seeding. The integrity of the
endothelial monolayer was confirmed by both fluorescence imaging of the dextran distribution and
confocal microscopy of fixed and labeled cells. An intact endothelial monolayer gives rise to an abrupt
intensity drop between the channel and the gel region once the fluorescently labeled dextran is introduced,
and persists over time as dextran slowly diffuses across the monolayer into the gel (Figure 2.3A-B).
59
Samples fixed on the third day after cell seeding and stained for VE-cadherin and nuclei (DAPI-blue)
exhibit well-defined junctions with no apparent gaps in the confluent monolayer (Figure 2.3C).
Quantification and analysis of fluorescence intensity yields values for the endothelial permeability to a 70
kDa dextran (3.70 t 0.59)-
10-6
cm/s, or roughly one order of magnitude higher than published in vivo
values but consistent with previously reported values in in vitro systems [36, 39]. The higher values of
permeability may be due to a variety of factors present in vivo but missing from the in vitro model. For
example, it is well known that the presence of pericytes helps to establish the low permeability of vessels
in vivo [39]. In view of our previous work demonstrating that increased permeability correlates with
increased rates of intravasation [25], to the extent that cells use similar mechanisms for extravasation as
intravasation, the present extravasation rates may be viewed as being biased toward higher values than
physiologic.
60
(a)
top view
,0.s
C0.6
0OA
0.2
6500
0
1000
100
20
distance (pm)
Figure 2.3. Confirmation of endothelial monolayer integrity. The integrity of the endothelial
monolayer was confirmed by both fluorescence imaging of the dextran distribution and confocal
microscopy of fixed and labeled cells. An intact endothelial monolayer gives rise to an abrupt intensity
drop between the channel and the gel region once the fluorescently labeled dextran is introduced. Three
hours after dextran injection, a sharp drop in fluorescence intensity is seen across the endothelial layer
demonstrating its function as a barrier to macromolecules (a). Fluorescence intensity is quantified using
Matlab (b). The dashed arrow in (a) the location and direction for the quantification. The intensity value
drops to 15% of is peak value due to the barrier effect. The endothelial monolayer is located near the
400gm point on the plot (shown with dashed line). Samples fixed on the third day after cell seeding and
stained for VE-cadherin and nuclei (DAPI-blue) exhibit well-defined junctions with no apparent gaps in
the confluent monolayer (c). The confocal image shows the front view of the microfluidic device.
2.3.3. Optimization of tumor cell seeding
From clinical data, the number of tumor cells that have intravasated and travel in circulation has
been measured to be less than ~100 in 7.5mL of blood on average [40, 41]. For the purpose of these
a
experiments, we chose to use a seeding density which was neither so low we were unable to view
significant number of extravasation events in a reasonable number of experiments, nor so high the tumor
cells were densely packed at the endothelial surface.
61
This latter situation might lead to tumor cell
interactions that poorly represent the situation in vivo. Hence, in this experiment, the tumor cell seeding
density was optimized to have only a limited number of tumor cells in the ROI while maintaining as
many experimental ROts as possible that contain at least one tumor cell to facilitate extravasation event
observation. Histograms of number of total tumor cells present in each ROI show different trends in
distribution of tumor cells for three different tumor seeding densities: 20,000 cells/ml, 50,000 cells/mI,
and 200,000 cells/ml (Figure 2.4A). Although the smallest tumor seeding density results in the smallest
average number of tumor cells in each ROI as shown in Figure 2.4B, this is due to having ROs without
any tumor cells 55% of the time. The average value and the histogram can be used for choosing the
optimal tumor seeding condition and a seeding density of 50,000 cells/ml was chosen as a compromise
between mimicking the low number of tumor cells of the in vivo of extravasation condition and increasing
the chance to have at least one tumor cell to analyze in any given RO.
62
(a)
120,000 cells/mI
14
I:
50,000
--
2'
cells/mI
200,000 cells/mI
*
6-
2
0
@ 2
4
051616
# of cells In ROI
(b)
205
# of cells In ROI
@
0
3
3,
U
# of cells in ROI
18
16
0 14
12
10
08
E6
0I
20000 cells/mI 50000 cells/mI 200000 cells/mi
tumor seeding density
Figure 2.4. Optimization of tumor cell seeding density. The tumor cell seeding density was optimized
to have only a limited number of tumor cells in ROI while maintaining as many experimental ROs as
possible that contain at least one tumor cell so tumor cell events can be observed. Histograms of number
of total tumor cells present in each ROT (250Rm x 250gm x 120Rm) show different trends in distribution
of tumor cells for three different tumor seeding densities: 20,000 cells/ml, 50,000 cells/ml, and 200,000
cells/ml (a). The average value and the histogram can be used for choosing the optimal tumor seeding
condition (b). Seeding density of 50,000 cells/ml was chosen as a compromise between mimicking the
low number of tumor cells of the in vivo of extravasation condition and increasing the chance to have at
least one tumor cell to analyze in any given ROI. The statistical significance was tested with one way
ANOVA (p < 0.05).
2.3.4 Extravasation
Tumor cells that disseminate from the primary tumor and survive the vascular system can
eventually transmigrate across the endothelium to recolonize at a secondary tumor site. With the
microfluidic system developed, we can mimic the extravasation step where tumor cells can transmigrate
across an endothelial monolayer into a hydrogel which models the extracellular space of a secondary
63
tumor site. The extravasation event is observed in devices that are fixed I day after tumor cells are
introduced, and direct quantification of the number of extravasated cells provides a metric of
extravasation. The region of interest (ROI) is captured in one confocal image scan and shows one cancer
cell, labeled green, that has transmigrated across the endothelium, denoted by VE-cadherin staining in red,
and extravasated into the gel region (Figure 2.5A). Surface views of the confocal scan from other samples
show three different possible locations of tumor cells 1 day after the seeding: 1) extravasated and in gel, 2)
adhered and located on endothelium adjacent to gel region, and 3) in the channel not near the gel (Figure
2.5B). The surface and sectional views of the device shown in Figure 2.5B. All three scenarios of where
tumor cells could be are observed here. There are cases where all tumor cells present in the ROI
extravasated as well as cases where none of the tumor cells crossed the endothelium. However, it is more
common to find regions that contain both extravasated and non-extravasated cells as in Figure 2.5B. This
is seen quantitatively in Figure 2.5C where 51% of ROIs exhibited tumor cells with contrasting fate. The
graph shows how many tumor cells have extravasated, as shown by dots, among the total tumor cells
present in the each region of interest. The tumor cells are categorized as having extravasated only when
they have clearly passed the endothelial monolayer into the gel region.
64
(a)
(b)
(
total tumor cells
30
e xtravasated cells
25
20
15
E 10
0
12
3 4 5 6 7 8 9 1011 121314 IS16171019202122
All ROls
(d)
~18
day 3
16
day4
2
o 12
tumor added
65
control
Figure 2.5. Observation of extravasation and permeability of endothelium. The extravasation event is
observed in a sample, which is fixed 1 day after tumor cells are introduced. The region of interest is
captured in one confocal image scan and shows one cancer cell (green) that has transmigrated across the
endothelium (denoted by VE-cadherin staining in red) and extravasated into the gel region (a). The
surface view of the confocal scan shows three different possible locations of tumor cells: 1) extravasated
and in gel, 2) adhered and on endothelium adjacent to gel region, and 3) in channel not near the gel. The
sectional view of the same confocal scan confirms the different location of the tumor cells (b). The graph
shows how many tumor cells have extravasated (dot) among the total tumor cells present (bar) for each
region of interest analyzed (c). The tumor cells are categorized as extravasated only when the tumor cells
have clearly passed the endothelial monolayer into the gel region. The permeability of endothelial
monolayer changes significantly with addition of tumor cells (d). Fluorescently labeled dextran was
introduced on day 3 after endothelial seeding to measure the permeability before tumor and again to same
samples on day 4 to see the after tumor seeding effects. The tumor cells are introduced on day 3 after day
3 permeability measurements are taken. The statistical significance was tested with paired t-test (p < 0.05).
Measuring penreability of the endothelium is one method for quantifying the quality of
endothelial monolayer. In addition, the permeability serves as a metric to quantify the change in
endothelium when tumor cells are added to the system and interact via physical attachment to the
endothelial surface. Leakiness of the vessel with or without tumor cells provides a possible explanation
for events leading to cancer extravasation in that signaling by the tumor CTCs could impair barrier
function. Alternatively, the increase in permeability could be a result of tumor cell transmigration. From
the present experiments, it is not possible to distinguish between these two scenarios. In this experiment,
the permeability changed significantly with addition of tumor cells compared to the permeability change
occurring during the same 24 h period when no tumor cells are added (Figure 2.4D). Fluorescently
labeled dextran was introduced on day 3 after endothelial cells were seeded to measure the penneability
before introducing tumor cells. Images were taken 3 hours after dextran insertion in order to achieve a
quasi-steady state. Tumor cells are introduced immediately after the permeability measurements are taken.
24 hours later, fluorescently labeled dextran was again introduced to measure the permeability after tumor
cell - endothelial cell interactions. The initial penneability value was (3.70 t 0.59)-10~6 cm/s and the
tumor seeding increased endothelial permeability to (14.2 - 2.6)-10- 6 cm/s (p < 0.05) whereas there was
no significant change in the control ((6.0 - 1.1)- 10-6 to (6.4 t 1.9) 10~6 cm/s) over the same 24 hour period.
As a control, we measured the change in endothelial permeability and extravasation rates of a
66
normal epithelial cell line, MCF-IOA, in our microfluidic system. While extravasation was observed for
38.8 t 7.9% of the tumor cells in contact with the endothelium 1 day after seeding, the corresponding rate
of MCF-1OA extravasation across the endothelium was lower, 23.8
±
4.7%, although not significantly
different. Addition of MCF-1OA also induced a 2-fold increase in permeability of endothelium from (5.78
± 0.47)-10-6 to (11.88
±
2.15)-10-6 cm/s (p < 0.05) as shown in Figure 2.6. This increase is smaller than the
permeability increase obtained after the addition of MDA-MB-231 (3.8-fold). Therefore, the MDA-MB231 cells show an increased tendency to extravasate and compromise endothelial barrier function
compared with normal epithelial cells. These results show that our microfluidic system is capable of
detecting differences among different epithelial cells lines and our results are consistent with
extravasation studies in a transwell assay [42].
,25
E
0 20
S16
10
5
0
after
before
MCF-IOA added
Figure 2.6. Permeability of endothelium measured with 70kDa fluorescently labeled dextran.
The change in permeability of endothelium is regulated by VE-cadherin expression through the
Src pathway, and the studies of in vivo models have shown that disruption of endothelial barrier function
enhanced extravasation efficiency [43]. Several mechanisms exist which could explain changes in
permeability due to tumor cell interactions; the permeability increase may also be due to tumor cells
67
locally disrupting endothelial monolayer by contact [44-46] or through secretion of chemical factors
which then compromises the endothelial barrier function [47], but more investigation is needed for clear
identification of the cause of the permeability increases.
2.3.5 Beyond extravasation
Tumor cells are observed for up to 3 days after tumor cell seeding and compared to tumor cells on
day 1. Average of total number of tumor cells present in ROI increases significantly from 7.9
on day 1 to 13.4
±1.5
±
1.6 cells
cells on day 3 while all experimental conditions including the tumor seeding density
remained the same (Fig 2.7A). This significant increase in number of tumor cells demonstrates
proliferation from day 1 to day 3 overall. The total number of tumor cells are further subdivided in Figure
2.7B into 2 subgroups depending on their location, either 1) extravasated and in the gel or 2) adherent to
the endothelium adjacent to gel. The number of tumor cells per ROI in the gel increased from 1.9
cells on day I to 6.1
±
±
0.4
1.7 cells on day 3 while the cells on endothelium changed from 4 cells on day 1 to
7 cells on day 3. This increase in tumor cell number from day 1 to day 3 for the extravasated cells could
be due to either more cells extravasting over the extra 2 day period, to proliferation, or both. Noting,
however, that the percentages of ROIs containing extravasated cells event did not show a significant
change for day I and day 3 (72% of ROIs exhibited at least 1 extravasated cancer cell by day 1 after
introducing tumor cells, and 79% of ROIs included extravasation event by day 3) (Figure 2.7C), and
assuming the proliferation rates are similar to both populations, this suggests most extravasation events
occur within the first day the tumor cells are introduced. This observation is similar in terms of time scale
for extravasation seen in vivo [18, 48].
68
(a)
(b)
5
16-
a-
12
-
0
E
10
T
8
(a
8
U
61
1~
on endoteliwn adjacent to gel
(not extravasated)
0
S
6.
4
*9
4,
0
I-
in gel (.xtravasatd)
10
14,
2
2
01
0
day I
day 3
day I
days after Introducing tumor
day 3
days after introducing tumor
(c)
0
100
80
T
I
Ce 60
40
6- 20
day I
day 3
days after introducing tumor
Figure 2.7. Beyond extravasation. The tumor cell extravasation is observed for up to 3 days after tumor
cell seeding and compared to the ones fixed and analyzed on day 1. The total number of tumor cells
present in region of interest (ROI) increases significantly from 8 cells on day 1 to 13.5 cells on day 3
while the tumor seeding density as well as other experimental condition remained the same between
devices (a). The total number of tumor cells are further subdivided into 2 groups depending on their
location, either 1) extravasated and in the gel or 2) adherent to the endothelium adjacent to gel (b). 72% of
ROIs exhibited at least 1 extravasated cancer cell (denoted % extravasation occurrence) by day 1 after
introducing tumor cells, and 79% of ROIs included extravasation event by day 3, which the difference is
not significant (c). The images show number of tumor cell increase (d). The phase contrast image shows
the top view of the region of interest on day 1 after tumor seeding. The tumor cells (green) have
proliferated from day 1 to day 3 (shown by arrows). The confocal image shows both the tumor cells and
endothelium lining. All images are from the same ROI (VE-cadherin: red, nucleus: DAPI-blue, tumor cell:
GFP-green).
69
References
1.
2.
3.
4.
5.
Jeon, J.S., et al., In Vitro Model of Tumor Cell Extravasation.Plos One, 2013. 8(2).
Sporn, M.B., The war on cancer. Lancet, 1996. 347(9012): p. 1377-1381.
Hanahan, D. and R.A. Weinberg, The hallmarks of cancer. Cell, 2000. 100(1): p. 57-70.
Chambers, A.F., A.C. Groom, and I.C. MacDonald, Disseminationand growth of cancer cells in
metastatic sites. Nature Reviews Cancer, 2002. 2(8): p. 563-572.
Joyce, J.A. and J.W. Pollard, Microenvironmental regulation of metastasis. Nature reviews.
Cancer, 2009. 9(4): p. 239-52.
6.
7.
Gupta, G.P. and J. Massague, Cancer metastasis: building a framework. Cell, 2006. 127(4): p.
679-95.
Roussos, E.T., J.S. Condeelis, and A. Patsialou, Chemotaxis in cancer. Nature Reviews Cancer,
2011. 11(8): p. 573-587.
8.
Wirtz, D., K. Konstantopoulos, and P.C. Searson, The physics of cancer: the role of physical
interactions and mechanicalforces in metastasis. Nature Reviews Cancer, 2011. 11(7): p. 512-
522.
Fidler, I.J., The pathogenesis of cancer metastasis: the 'seedand soil' hypothesis revisited. Nature
reviews. Cancer, 2003. 3(6): p. 453-8.
10.
Crissman, J.D., et al., Morphological study of the interaction of intravasculartumor cells with
endothelial cells and subendothelialmatrix. Cancer Research, 1988. 48(14): p. 4065-72.
11.
Koop, S., et al., Overexpression of metalloproteinase inhibitor in B16F10 cells does not affect
extravasation but reduces tumor growth. Cancer Research, 1994. 54(17): p. 4791-7.
12.
Ewing, J., Neoplastic Disease: A Treatise on Tumors. 3 ed1928
, Philadelphia: W. B. Saunders.
Schluter, K., et al., Organ-specific metastatic tumor cell adhesion and extravasation of colon
13.
carcinoma cells with different metastatic potential. The American journal of pathology, 2006.
169(3): p. 1064-73.
Naumov, G.N., et al., Cellular expression of green fluorescent protein, coupled with high14.
resolution in vivo videomicroscopy, to monitor steps in tumor metastasis. Journal of Cell Science,
1999. 112 ( Pt 12): p. 1835-42.
Gassmann, P., et al., Metastatic tumor cell arrest in the liver-lumen occlusion and specific
15.
adhesion are not exclusive. International journal of colorectal disease, 2009. 24(7): p. 851-8.
Mareel, M. and A. Leroy, Clinical, cellular, and molecular aspects of cancer invasion.
16.
Physiological Reviews, 2003. 83(2): p. 337-376.
17.
Psaila, B. and D. Lyden, The metastatic niche: adaptingthe f/reign soil. Nature Reviews Cancer,
9.
2009. 9(4): p. 285-293.
18.
19.
20.
21.
22.
23.
Al-Mehdi, A.B., et al., Intravascularorigin of metastasisfrom the proliferation of endotheliumattached tumor cells: a new model for metastasis. Nature Medicine, 2000. 6(1): p. 100-102.
Vargo-Gogola, T. and J.M. Rosen, Modelling breast cancer: one size does not fit all. Nature
Reviews Cancer, 2007. 7(9): p. 659-672.
Hendrix, M.J.C., et al., A Simple Quantitative Assay for Studying the Invasive Potential of High
and Low Human Metastatic Variants. Cancer Letters, 1987. 38(1-2): p. 137-147.
Dimilla, P.A., et al., Measurement of Individual Cell-Migration ParametersJbr Human TissueCells. Aiche Journal, 1992. 38(7): p. 1092-1104.
Song, J.W., et al., Microfluidic endotheliumfor studying the intravascularadhesion of metastatic
breastcancer cells. Plos One, 2009. 4(6): p. e5756.
Shin, M.K., S.K. Kim, and H. Jung, Integration of intra- and extravasation in one cell-based
microfluidic chipfor the study of cancer metastasis. Lab on a chip, 2011. 11(22): p. 3880-7.
70
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
Zhang, Q., T. Liu, and J. Qin, A microfluidic-baseddevice for study of transendothelialinvasion
of tumor aggregatesin realtime. Lab on a chip, 2012. 12(16): p. 2837-42.
Zervantonakis, I.K., et al., Three-dimensional microfluidic modelfor tumor cell intravasationand
endothelial barrierfnction. Proceedings of the National Academy of Sciences of the United
States of America, 2012. 109(34): p. 13515-20.
Vickerman, V., et al., Design,flibricationand implementation of a novel multi-parametercontrol
microfluidic platfbrm for three-dimensional cell culture and real-time imaging. Lab on a chip,
2008. 8(9): p. 1468-1477.
Sudo, R., et al., Transport-mediatedangiogenesis in 3D epithelial coculture. Faseb Journal, 2009.
23(7): p. 2155-2164.
Shin, Y., et al., In vitro 3D collective sprouting angiogenesis under orchestrated ANG-1 and
VEGF gradients. Lab on a chip, 2011. 11(13): p. 2175-2181.
Chung, S., et al., Cell migration into scaffblds under co-culture conditions in a microfluidic
platform. Lab on a chip, 2009. 9(2): p. 269-275.
Chung, S., et al., Surface-Treatment-Induced Three-Dimensional Capillary Morphogenesis in a
Microfluidic Platform. Advanced Materials, 2009. 21(47): p. 4863-+.
Shin, Y., et al., Microfluidic assay Jbr simultaneous culture of multiple cell types on surfaces or
within hydrogels. Nature Protocols, 2012. 7(7): p. 1247-59.
Polacheck, W.J., J.L. Charest, and R.D. Kamm, Interstitialflow influences direction of tumor cell
migration through competing mechanisms. Proceedings of the National Academy of Sciences of
the United States of America, 2011. 108(27): p. 11115-11120.
Minn, A.J., et al., Genes that mediate breastcancer metastasis to lung. Nature, 2005. 436(7050):
p. 518-24.
Bos, P.D., et al., Genes that mediate breast cancer metastasis to the brain. Nature, 2009.
459(7249): p. 1005-9.
Muthuswamy, S.K., et al., ErbB2, but not ErbBI, reinitiatesproliferation and induces luminal
repopulation in epithelialacini. Nature cell biology, 2001. 3(9): p. 785-92.
Albelda, S.M., et al., Permeability Characteristicsof Cultured Endothelial-Cell Monolayers.
Journal of Applied Physiology, 1988. 64(1): p. 308-322.
Vickerman, V. and R.D. Kamm, Mechanism of aflow-gated angiogenesis switch: early signaling
events at cell-matrix and cell-cell junctions. Integrative biology : quantitative biosciences from
nano to macro, 2012. 4(8): p. 863-74.
Han, S., et al., A versatile assay for monitoring in vivo-like transendothelial migration of
neutrophils. Lab on a chip, 2012.
Michel, C.C. and F.E. Curry, Microvascularpermeability. Physiological Reviews, 1999. 79(3): p.
703-761.
Nagrath, S., et al., Isolation of rare circulating tumour cells in cancer patients by microchip
technology. Nature, 2007. 450(7173): p. 1235-U10.
Hayes, D.F., et al., Circulating tumor cells at each fblow-up time point during therapy of
metastatic breast cancer patients predict progression-free and overall survival. Clinical Cancer
Research, 2006. 12(14): p. 4 2 1 8 -4 2 24 .
Sahni, A., et al., The VE-cadherin binding domain of fibrinogen induces endothelial barrier
permeability and enhances transendothelial migration of malignant breast epithelial cells.
International journal of cancer. Journal international du cancer, 2009. 125(3): p. 577-84.
Weis, S., et al., Endothelial barrierdisruption by VEGF-mediated Src activity potentiates tumor
cell extravasationand metastasis. Journal of Cell Biology, 2004. 167(2): p. 223-229.
Mierke, C.T., Cancer cells regulate biomechanical properties of human microvascular
endothelial cells. The Journal of biological chemistry, 2011. 286(46): p. 40025-37.
Li, Y.H. and C. Zhu, A modified Boyden chamber assayfor tumor cell transendothelialmigration
in vitro. Clinical & Experimental Metastasis, 1999. 17(5): p. 423-9.
71
46.
47.
48.
Kumar, S. and V.M. Weaver, Mechanics, malignancy, and metastasis: the force journey of a
tumor cell. Cancer metastasis reviews, 2009. 28(1-2): p. 113-27.
Weis, S.M. and D.A. Cheresh, Pathophysiological consequences of VEGF-induced vascular
permeability.Nature, 2005. 437(7058): p. 497-504.
Qian, B., et al., A distinct macrophage population mediates metastatic breast cancer cell
extravasation,establishmentand growth. Plos One, 2009. 4(8): p. e6562.
72
Chapter 3
3D in vitro model for specificity of breast cancer
metastasis to bone 3
3.1. Introduction
The systemic nature of cancer metastases coupled with the resistance to most current therapeutic
agents explains why metastases are responsible for as much as 90% of cancer-related mortality [2, 3]. The
dissemination of circulating tumor cells (CTCs) represents a "hidden" process leading to micrometastases
where quiescent cells can survive for prolonged periods before their activation [4, 5].
In order to generate secondary tumors, CTCs must survive in the circulation and undergo a
process known as extravasation [6-8]. Extravasation into the parenchyma of distant tissues represents a
multistep sequence within the metastatic cascade, in which cancer cells establish transient, metastable
contacts with the endothelium [9-11], firmly adhere to the vascular walls [12] and finally transmigrate
across the endothelial and pericyte layers [13] as microcolonies or isolated cells [14, 15].
Although it is well known that circulatory patterns play a pivotal role in the spread of metastatic
cells to secondary sites, the cross-talk between specific cancer cell types and receptive environments also
preferentially guides the dissemination process [16]. In this context, it has been shown that breast cancer
metastasizes to bone, liver, lung and brain while prostate cancer frequently disseminates to bone [4].
3
This chapter is modified from Ref. [1] with the publisher's permission.
73
Particularly, autoptic studies have demonstrated that 70% of advanced breast cancer patients have skeletal
metastases, leading to pain, due to spinal cord compression and fractures, and often mortality [17, 18].
Despite the clinical importance of metastases, research has largely focused on the oncogenic
transformations leading to the development of primary tumors and much remains to be learned about the
metastatic process [6]. Moreover, a deeper understanding of the metastatic cascade and particularly of
extravasation to a specific organ could promote the development of new therapeutic strategies, thus
improving cancer survival rates [13].
In vivo and ex vivo models have been developed to study the extravasation process in mice and
zebrafish embryos through intravital microscopy [14, 19, 20] and advanced models of bone metastasis
employ intravenous, intracardiac or direct skeletal injection of breast cancer cells [21, 22]. Although these
experiments replicate physiological conditions, they cannot model all aspects of the interaction and crosstalk between human cancer cells, human endothelial cells and human tissue parenchyma. Moreover,
strictly regulated, reproducible parametric studies are difficult to perform.
In vitro models, although unable to fully replicate the in vivo situation, can overcome some of
these limitations by using human cells throughout and providing highly controllable environments where
single culture parameters can be modified [23, 24]. Traditional assays (e.g. Boyden chamber, wound
assay, and others) have been widely used to study cell migration in response to chemotactic gradients,
particularly cancer cell invasion and migration. However, they do not provide tight control over the local
environment, complex interactions cannot be accurately analyzed, and imaging is limited [25-27].
Microfluidics can provide useful model systems to investigate complex phenomena under
combination of multiple controllable biochemical and biophysical microenvironments, coupled with high
resolution real time imaging [28-31]. The synthesis of these features is technically impossible with
traditional assays as the Boyden chamber [32, 33]. Toward this goal, several microfluidic devices have
been developed to investigate cancer cell transition to invasion and migration from a primary site [34-36],
74
cell transition effects across mechanical barriers [37], intravasation [38], adhesion [39] and extravasation
[40-45] processes.
However, despite supporting experimental evidence, none of the previously reported in vitro
systems has reproduced the specific cross-talk among several cell types in a complex cancer
microenvironment during extravasation and none have gone beyond the study of transendothelial
migration towards a non-organ-specific extracellular matrix (ECM). Indeed, the importance of organspecific cancer models lies in the possibility to better clarify the mutual interactions between different cell
populations in a well-defined microenvironment, in order to develop highly focused and more effective
therapies.
We develop here a new tri-culture microfluidic 3D in vitro model demonstrating the key role
played by an osteo-cell conditioned microenvironment, a collagen gel with embedded osteo-differentiated
bone marrow-derived human mesenchymal stem cells (hBM-MSCs) [46] and lined with endothelium, in
the extravasation process of highly-metastatic MDA-MB-231 human breast cancer cells [17, 47]. Our
new results demonstrate how the interaction between an inflammatory chemokine secreted by osteoblasts
(CXCL5) and the correspondent surface receptor expressed by breast cancer cells (CXCR2) can modulate
circulating breast cancer cell homing within the bone microenvironment, significantly affecting the
extravasation rate. In addition, cancer cells monitored after 2, 3 and 5 days survive in the new matrix,
proliferate and generate micrometastases.
3.2 Materials and methods
3.2.1 Microfluidic system
A previously developed microfluidic device consisting of 3 media channels and 4 independent gel
channels was adopted in the present study. Specifications and microfabrication details of the system were
previously described [48, 49]. Inlet and outlet ports of the PDMS (poly-dimethyl-siloxane; Silgard 184,
Dow Chemical) devices were bored using disposable biopsy punches and the PDMS layer was bonded to
75
a cover glass to create microfluidic channels 150 pm deep with oxygen plasma treatment. Eight gel
regions (225 pm by 150 pm) interfacing with the central media channel are provided to study cell
interactions. The PDMS channels were coated with a PDL (poly-D-lysine hydrobromide; I mg/ml;
Sigma-Aldrich) solution to promote matrix adhesion. Then, collagen type I (BD Biosciences) solution
(6.0 mg/mI) with Phosphate Buffered Saline (PBS; Invitrogen) and IN NaOH, and embedded with osteodifferentiated hBM-MSCs was injected within the 4 independent gel channels using a 10 pl pipette and
incubated for 30 min inside humid chambers to form a hydrogel. A representative schematic of the model
is provided in Figurel, showing the generated tri-culture system with particular emphasis on the osteocell conditioned microenvironment. After 3 days, diluted MatrigelTM (BD Biosciences) solution (3.0
mg/ml) was introduced as a thin layer coating the central media channel; cold medium was injected after
1 min to wash and prevent channel clogging. Endothelial cells were introduced into the central media
channel to generate a monolayer covering channel walls and gel-channel interfaces. Cancer cells were
injected after 3 additional days in the same channel and transmigration into the osteo-cell conditioned
regions was analyzed after 24 h [43]. Additionally, proliferation and clustering of transmigrated cancer
cells within the osteo-cell conditioned matrix were studied after 2, 3 and 5 days.
76
(brown) were
Figure3.1. Generation of the osteo-cell conditioned microenvironment. (A) hBM-MSCs
they
cultured for 2-3 weeks within osteogenic medium and seeded within microfluidic devices where
started depositing extracellular matrix (yellow filaments). After 3 days endothelial cells (ECs) (red) were
(green) were
seeded and a monolayer covering the media channel was generated. Finally, cancer cells
were
generation
micrometastasis
and
ability
introduced after 3 additional days and their extravasation
a
represents
stack
confocal
a
of
monitored for I to 5 days. (B and C) Three-dimensional reconstruction
while
walls
channel
the
top (B) and a front view (C) of a single ROI. HUVECs (RFP) completely covered
Cells were
osteo-differentiatedhBM-MSCs were homogeneously distributed within the collagen gel.
calcium
stained with DAPI (nuclei, blue) and phalloidin (F-actin, green). (D) Alizarin Red staining of
Two-dimensional
(E)
field).
bright
microscopy,
(optical
deposits (dark region) within a gel channel
to secrete
projection of a confocal stack highlights the ability of osteo-differentiatedhBM-MSCs
blue) and
(nuclei,
DAPI
with
osteocalcin (green) within a 3D microenvironment. Cells were stained
bars: 50
Scale
osteo-cells.
as
phalloidin (F-actin, yellow). Osteo-differentiated hBM-MSCs are labeled
Pm.
3.2.2. Cell culture
bone
Bone marrow-derived human mesenchymal stem cells were obtained harvesting whole
according to an
marrow aspirates from patients undergoing hip surgery and selected by plastic adherence
Loptimized protocol [50]. Cells of passage 7 or lower were cultured in osteogenic medium containing
ascorbic acid,
P-glycerophosphate, cholecalciferol and dexamethasone for at least 2 weeks. Before the
77
seeding, collagenase type I (Gibco) solution (15 mg/ml) was applied for 20 min on an orbital shaker to
promote cell matrix dissolution; then, cells were trypsinized for 10 min. Next, collagen gel with 750,000
cells/ml suspension was used to fill the gel ports. The cell suspension density was optimized by balancing
the maximum effect induced by osteo-differentiated hBM-MSCs while limiting the possible gel
degradation. Cells were cultured for 6 days before cancer cell injection in order to recreate an osteo-cell
conditioned microenvironment (3 days supplemented with osteogenic medium, 3 days supplemented with
endothelial cell medium). Red fluorescent protein (RFP)-transfected human umbilical vein endothelial
cells (HUVECs) were commercially obtained (Angio-Proteomie) and cultured in endothelial growth
medium (EGM-2MV; Lonza). According to a previously optimized cell seeding protocol [43], 40 p1l
HUVEC suspension at 2x 106 cells/ml were introduced 3 days after seeding osteo-differentiated hBMMSCs. All the experiments were conducted using HUVECs of passage 8 or lower. Human mammary
adenocarcinoma cells MDA-MB-231 (American Type Culture Collection (ATCC)) were selected for high
invasiveness and their ability to metastasize in vivo [51, 52]. Green fluorescent protein (GFP)-expressing
MDA-MB-231 were cultured in standard Dulbecco's Modified Eagle Medium (DMEM; Invitrogen)
supplemented with 10% Fetal Bovine Serum (FBS; Invitrogen), 1%
L-glutamine and antibiotics, and
were introduced 3 days after endothelial cell seeding by injecting 40 pl of 50,000 cells/ml cell suspension.
The medium was replaced 1 h later with endothelial cell culture medium. All cultures were kept in a
humidified incubator maintained at 37'C and 5% CO 2 . Control experiments were performed with a
collagen gel-only matrix, following the same protocol.
3.2.3. Immunofluorescent staining
Samples were washed with PBS and fixed with 4% paraformaldehyde (PFA) for 15 min at room
temperature. Next, cells were washed twice with PBS and incubated with 0.1% Triton-X 100 solution for
5 min at room temperature. After washing twice with PBS, cells were blocked with 5% BSA + 3% goat
serum solution for at least 3 h at 4'C. Vascular endothelial-cadherin (VE-cadherin) was labeled with
78
rabbit polyclonal antibody (Abcam) at 1:100 dilution, Ki-67 was labeled with rabbit polyclonal antibody
(Abcam) at 1:500 dilution, osteocalcin was labeled with rabbit polyclonal antibody (BTI) at 1:500
dilution, osteonectin was labeled with rabbit polyclonal antibody (Santa Cruz Biotechnology) at 1:60
dilution and osteopontin was labeled with rabbit polyclonal antibody (Abcam) at 1:100 dilution.
Fluorescently labeled secondary antibodies (Invitrogen) were used at 1:200 dilution. Cell nuclei were
stained with 4'6-Diamidino-2-Phenylindole (DAPI; 5 mg/ml; Invitrogen) at 1:500 dilution while F-actin
filaments were stained with AlexaFluor633 phalloidin (Invitrogen) at 1:100 dilution. If not differently
specified, all the images were captured using a confocal microscope (Olympus IX81) and processed with
Imaris software (Bitplane Scientific Software).
3.2.4. Conditioned assays: addition of CXCL5 and CXCR2 blocking agent
The cross-talk between MDA-MB-231 and osteo-differentiated hBM-MSCs was analyzed by
investigating a signaling pathway involving the osteoblast-secreted inflammatory chemokine CXCL5 and
the breast cancer cell surface receptor CXCR2 [53-55]. The selected chemokine was used to test the
extravasation ability of breast cancer cells without the presence of an osteo-cell conditioned matrix while
blocking experiments were performed to quantify the extravasation rate of CXCR2-blockedcancer cells
within the standard osteo-cell conditioned matrix. Recombinant human CXCL5/ENA-78 (R&D Systems)
was diluted to 12 nM and added to the lateral media channels of collagen gel-only devices30 min before
cancer cell seeding; fresh CXCL5-containing medium was replaced I h after the seeding and 12 h later to
guarantee a stable gradient through the gel regions. In CXCR2 blocking experiments, cancer cells were
incubated with 5 ptg/ml mouse monoclonal antibody anti-CXCR2 (R&D Systems) lh before the seeding;
additionally, fresh antibody suspension was added lh after the seeding to the central media channel of
osteo-differentiated hBM-MSC-containing devices to saturate all cancer cell target receptors. Control
experiments were performed by adding IgG antibody at the same CXCL5 or anti-CXCR2 concentrations,
following identical protocols.
79
3.2.5. Extravasation and micrometastasis metrics
Confocal data were analyzed using Imaris software and its tracking algorithms for selecting and
counting cell nuclei and GFP-derived signals within a specific region of interest (ROI). The ROI was
defined as the 3D region between two PDMS walls, containing both the gel matrix and the endothelial
monolayer interfacing the central media channel (Figure 3.1 B). The ROI dimensions were 250 pm
pm
x
x
250
150 pm (height) and each device contained 8 ROts. The extravasation percentages were measured
per device and subsequently averaged while the extravasation distance was quantified averaging data
extracted from each specific condition as a single group. Extravasation events were observed using real
time confocal microscopy. According to our previous studies demonstrating that extravasation events
mostly occur within the first 24 h, we quantified cell proliferation by counting the total number of cells
per device at day 1,
2, 3 and 5. The number of cells per micrometastasis, the percentage of
micrometastasis-positive ROIs and the number of micrometastases per ROI were computed.
3.3. Results and discussion
3.3.1. Generation of the osteo-cell conditioned microenvironment
The originality and relevance of the present work lie in the ability to specifically recreate for the
first time an organ-specific tumor microenvironment by combining a well known biocompatible material,
collagen gel type I, conditioned by bone-specific proteins secreted directly from primary human cells,
thus modeling the extravasation process of breast cancer cells into an osteo-cell conditioned
microenvironment. A key point of our system is that the extracellular matrix with secreted proteins from
osteo-differentiated cells better mimics the complex cell signaling present in the in vivo environment,
with naturally-formed gradients rather than imposed nutrition or chemokine gradients. Primary hBMMSCs were obtained from bone marrow samples of patients undergoing hip arthroplasty and predifferentiated in osteogenic medium for at least 14 days before being introduced into microfluidic
devices. FigurelA shows a schematic of the developed assay: osteo-differentiated hBM-MSCs (brown)
80
embedded in a collagen matrix were initially introduced into the gel channels, while RFP HUVECs (red)
were seeded 3 days later within the central media channel to create a monolayer covering the channel
walls and the gel-channel interfaces, thus generating an endothelium. At day 6 GFP MDA-MB-231
human breast cancer cells (green) were injected into the same cell channel and the extravasation rate
promoted by the osteo-cell conditioned microenvironment was analyzed during the following 24 h.
High resolution confocal imaging shows that osteo-differentiated hBM-MSCs are homogeneously
dispersed within the gel regions and extend their cytoplasmatic protrusions in the 3D microenvironment
(Figure 3.1B and C). Samples stained for nuclei (4'6-Diamidino-2-Phenylindole (DAPI), blue) and F-actin
(phalloidin, green) together with RFP-HUVECs clearly highlight the endothelial monolayer generation on
the gel-channel interface and the optimal distribution of osteo-differentiated hBM-MSCs within the
collagen gel. The tight connections of endothelium are further confirmed with VE-cadherin staining of the
monolayer (Figure 3.A4). hBM-MSCs produce calcium and secrete bone-marker proteins such as
osteocalcin, as demonstrated by Alizarin Red-S assay and immunofluorescent staining, respectively.
Calcium deposits (Figure 3.1D and 3.AIA) appear as darker regions within the osteo-cell conditioned
microenvironment while osteocalcin (Figure lE and A2A, green) encloses actively secreting osteodifferentiated hBM-MSCs. Moreover, the expression of two additional bone markers, i.e. osteonectin and
osteopontin, was evaluated within 2D flasks to provide complete evidence of osteogenic differentiation
(Figure 3.A2C
and D)
[56-58].
Taken together, these findings confirm hBM-MSC osteogenic
differentiation, thus providing the potential to better study the specific transendothelial migration of
breast cancer cells into bone.
3.3.2. Extravasation of cancer cells in the osteo-cell conditioned microenvironment
Extravasation of cancer cells into the 6.0 mg/ml collagen type I gel matrix with and without
osteo-differentiated hBM-MSCs is shown in Figure 2. MDA-MB-231 cancer cells transmigrated across
the endothelial monolayer covering the microchannel into the collagen gel whether the matrix contained
81
osteo-differentiated hBM-MSCs or not. However, the average percentage of cancer cells extravasated in
each ROI was significantly different comparing the abovementioned conditions. In collagen gel-only
matrix, 37.6 ± 7.3% cancer cells extravasated, nearly identical to 38% extravasation rate previously
reported in 2.0 mg/ml collagen gel, suggesting that matrix density alone is not a major factor [43]. With
the addition of osteo-differentiated hBM-MSCs to the collagen gel, cancer cell extravasation rate
increased to 77.5 ± 3.7% (Figure 3.2A and B). Moreover, the extravasated cancer cells travelled
significantly further into the matrix as compared to the collagen gel-only matrix. Indeed, the extravasation
distance into the gel during the first 24 h was 50.8 ± 6.2 pm when osteo-differentiated hBM-MSCs were
present, while cancer cells travelled 31.8 ± 5.0 pm in collagen alone (Figure 3.2C and D), showing a
similar migration behavior compared to 2.0 mg/ml collagen gels (25.9 ± 3.4 pm) and thus suggesting a
minor influence of ECM density. If we define 40 pm (approximately twice the average length of a cancer
cell and the mean distance travelled by the cells) as the threshold distance to distinguish between strongly
and weakly migrating cancer cells, our data show that only 25% of extravasated cancer cells in the
collagen gel-only condition were detected beyond the threshold while the rest remained close to the
endothelial monolayer (Figure 3.2C (i)). On the other hand, 45.8% of transmigrated cancer cells in the
osteo-cell conditioned microenvironment were detected beyond the threshold (Figure 2C (ii)), suggesting
the presence of factors not only promote cancer cell transendothelial migration, but also migration within
the matrix [54]. No significant modifications in the osteo-cell conditioned matrix were detected 24 h after
cancer cell injection suggesting that extravasated cells do not alter the physical properties of the
microenvironment in the observed time interval (Figure 3.A6).
82
A
B
ostoo-cell
C
ctri
D
distance
so
Figure 3.2 Extravasation of cancer cells into the collagen gel matrix with and without osteo-differentiated
hBM-MSCs (labeled as osteo-cells). (A) Three-dimensional confocal reconstruction shows MDA-MB231 cancer cells (GFP) transmigrated across the endothelial monolayer into the collagen gel containing
osteo-differentiatedhBM-MSCs. VE-cadherin (red) and DAPI (nuclei, blue) staining. (B) Average
percentage of extravasated cancer cells was significantly higher (n=27(min)-39(max) regions, p<0.005)
inthe collagen gel with osteo-differentiatedhBM-MSCs. (C) Projected images show extravasated cancer
cells (GFP) travelled farther into the osteo-cell conditioned microenvironment (ii) compared to the
collagen gel-only matrix (i). Cells were stained with (i) DAPI (nuclei, blue) and (ii) VE-cadherin (red) +
DAPI (nuclei, blue). HUVECs were RFP labeled.(D) Average distance travelled by extravasated cells into
the gel matrix increased significantly in osteo-cell conditioned microenvironment (n= 1 (min)- 1 7(max)
regions, p<0.05). Scale bars: 50 im.
To investigate the possibility that extravasation and migration behavior of breast cancer cells
were influenced by structural changes in the ECM induced by the osteogenic differentiation of hBMMSCs we performed experiments to compare collagen gel structure with or without osteo-differentiated
hBM-MSCs. Confocal reflectance images did not show a clearly detectable difference in the matrix
structure, suggesting the ECM remodeling was not the key factor affecting breast cancer cell migration
(Figure A5). However, we hypothesize a longer culture could induce changes in the structural properties
and composition of the matrix, potentially influencing cancer cell behavior. Indeed, such changes in the
83
microenvironment, characterized by secreting cells and active remodeling of the matrix toward an even
more physiological-like bone niche, could represent a significant improvement of the model.
3.3.3. Addition of CXCL5 and anti-CXCR2 - Effect on extravasation
As we found striking differences
in extravasation of cancer cells in the two different
microenvironments, we tried to investigate the effects of possible cytokines that are produced in the
osteo-cell conditioned microenvironment on promoting extravasation. CXCL5 is one of the major
chemokines that osteoblasts secrete and CXCR2 is a breast cancer cell surface receptor for this ligand.
CXCL5 is known to activate Snail, a transcription factor involved in cancer cell invasiveness and
migration [54]. Moreover, it has been demonstrated that Snail over-expression in breast cancer cells can
up-regulate Axl expression, a tyrosine kinase receptor [53], which in turn is important for breast cancer
cell extravasation [55]. Furthermore, the CXCR2 ligands CXCL5 and CXCL1 were recently shown to be
secreted by mouse BM-MSCs and promote mammary cancer cell migration[59]. An enzymatic assay
(CXCL5/ENA-78 enzyme-linked immunosorbent assay (ELISA)) confirmed the production of CXCL5
from osteo-differentiated hBM-MSCs at 3 weeks, showing a higher concentration (375 ± 1.65 pg/ml)
compared to non-differentiated hBM-MSCs (162 ± 11.3 pg/ml) (Figure A9A). No CXCL5 was detected
within control osteogenic medium or endothelial cell medium. Moreover, immunofluorescent staining
demonstrated the presence of CXCR2 surface receptor on MDA-MB-231 cells (Figure A6B). Based upon
these findings, we further investigated their role in extravasation (Figure3). Incubation of cancer cells
with CXCR2 blocking antibody reduced extravasation in osteo-differentiated hBM-MSC-embedded
collagen gel from 77.5 ± 3.7% to 45.8 + 5.4%, whereas incubation of cancer cells with control IgG had no
significant effect on extravasation (81.4 ± 7.4%) (Figure3A and B). Moreover, the addition of CXCL5
ligand to collagen gel-only matrices led to an increase in the percentage of cancer cell extravasation from
37.6 + 7.3% to 78.3 ± 9.7%, while the addition of control IgG produced no significant effect (25.7
16.7%) (Figure 3.3C and D).
84
C
n.s.
A
xmn.s.
1001
0
1
I -
cancer cells
cmvi
01*
ant.CXCR2
cmvi
IgG
CXCL.
E
CXCLS
gradient
-
anti-CXCR2
'Incubated
cancer cells
conde
antl-XCR2
CXCL5
blocking
Figure 3.3 Effect of CXCL5 and CXCR2 in cancer cell extravasation. (A) Addition of CXCR2
osteocontaining
gel
collagen
antibody significantly reduced cancer cell average extravasation within
cells
cancer
incubated
IgG
differentiatedhBM-MSCs compared to non-treated cancer cells (ctrl) or
that
shows
stack
(n=9(min)-24(max) regions, p<0.005). (B) Two-dimensional projection of a confocal
channel and
cancer cells (GFP, white arrows) generally remained within the endothelial cell (RFP)-coated
anti-CXCR2
did not extravasate into the collagen gel containing osteo-differentiatedhBM-MSCs when
yellow). (C)
(F-actin,
phalloidin
and
blue)
(nuclei,
antibody was added. Cells were stained with DAPI
of
percentage
average
the
enhanced
Addition of CXCL5 within collagen gel-only devices significantly
(n=9(min)-24(max)
IgG
cancercell extravasation compared to unconditioned devices (ctrl) and addition of
cancer
regions, p<0.05). (D) Two-dimensional projection of a confocal stack showing two extravasated
stained with
cells (GFP, white arrows) inside CXCL5-conditioned collagen gel-only devices. Cells were
average
DAPI (nuclei, blue) and phalloidin (F-actin, yellow). HUVECs were RFP labeled. (E) The
collagen
within
(condition)
CXCL5
of
addition
the
extravasation distance was significantly higher with
difference
gel-only devices compared to unconditioned devices (p<0.05) whereas there was no significant
in
incubation
cell
cancer
within a osteo-cell conditioned matrix with (condition) or without (control)
CXCR2 blocking antibody (n=l (min)-17(max) regions). Scale bars: 50 pm.
after
Interestingly, the distance that extravasated cancer cells travelled into the gel matrix
collagen geltransmigration was significantly greater with the addition of CXCL5 compared to control
produced no effect on
only experiments (54.7 ± 5.8 [tm vs. 31.8 ± 5.0 gm). However, blocking CXCR2
with hBM-MSCs
the distance travelled by extravasated cancer cells migrating into collagen gel embedded
± 6.2 gm),
compared to experiments performed with non-treated cancer cells (46 ± 5.7 [tm vs. 50.8
85
suggesting that the role of CXCR2 in breast cancer cell migration within the bone tissue could be less
critical compared to that of other receptors (Figure 3.3E).
Several factors secreted in vivo by the bone microenvironment can promote the extravasation of
breast cancer cells including CXCL12/SDF-la [60] and CX3CL1/fractalkine [61]. Although we did not
investigate the specific role played by different molecules, our data show a significant difference when
osteo-differentiated hBM-MSCs were embedded in the collagen matrix both in terms of extravasation rate
and migration distance, thus highlighting the potential for organ-specific in vitro models to clarify
features of different cancer types. To better characterize the effect of CXCL5 on breast metastatic cells
we generated a gradient through a collagen gel-only matrix (Figure A12), anticipating a critical role for
this molecule in transendothelial migration and chemoattraction to bone.
3.3.4. Formation of micrometastases
Lethality of metastatic tumors depends on the formation of a metastatic niche, which develops
when cancer cells extravasate into a secondary organ site and proliferate [3]. In our system, cancer cells
were cultured up to 5 days after being introduced into the vessel-mimicking channel, covered with an
endothelial monolayer and adjacent to an osteo-cell conditioned collagen matrix embedded with osteodifferentiated hBM-MSCs. Our earlier results show that there was no significant difference in the
percentage of ROIs containing extravasated cancer cells between day 1 and day 3 after their introduction
(72% vs. 79%) [43]. While this seems to indicate that most cancer cells extravasate within the first 24 h of
their introduction, the prolonged tri-culture allowed us to better characterize the behavior of cancer cells
after extravasation, leading to colonization within the microenvironment, as seen in Figure 3.4A and B.
The extravasated cancer cells proliferated and formed micrometastases of various sizes ranging from 4
cells to more than 60 cells (Figure 3.4C). We defined a cell cluster as a micrometastasis with at least 4
cancer cells either in direct contact or separated by less than one cell body length (assuming average
cancer cell diameter -20 pm), consistent with previous studies [19, 62]. The percentage of regions
86
containing micrometastases was 48.4% (n=31 ROIs were analyzed in 5 independent devices). In total, 38
micrometastases were detected: 6 clusters contained at least 10 cells while 4 were constituted by more
than 35 cells each (Figure 3.4C). The number of cancer micrometastases per gel region was equally
distributed among ROIs containing 1 to 4 micrometastases each (Figure 3.4D). Notably, large
micrometastases
(>30 cells) tended to be found in isolation or associated with another small
micrometastasis (Figure 3.A 10).
The average number of cancer cells per device found within the gel regions was 13.8 at day 1,
increasing to 17.8 and 34 at days 2 and 3, respectively, and reaching 132 at day 5 (Figure 3.A 11). While it
is possible that all cell types moved around in the system during the culture, it seems the increased
number of cancer cells leading to the formation of clusters is primarily due to proliferation, since we
observed the number of cancer cells increasing exponentially in each device during 5 days of culture.
Moreover, all extravasated cancer cells were shown to be in active cell cycle within the new colonized
microenvironment, as indicated by positive Ki-67 staining (Figure 3.4A and B insets).
A
B
D5
C2
10
4
3
4.4
2I
70
30
15
10
5
# cancer cells per micrometastasis
5
4
3
2
1
# cancer cell clusters per ROi
Figure 3.4 Generation of micrometastases within the osteo-cell conditioned microenvironment. Threedimensional confocal images of a single gel region show a representative large (A) and small (B) cancer
cell (GFP) micrometastasis. Ki-67 staining (red) demonstrates all cancer cells were proliferating within
the colonized microenvironment. Cells were stained with DAPI (nuclei, blue). (C) Histogram showing
micrometastasis distribution. Although 4 large clusters (>35 cells) were detected, micrometastases
generally contained fewer than 10 cells. (D) Histogram represents the number of micrometastases per gel
region (n=1 5 regions). Scale bars: 50 im.
87
Several studies were previously reported to study the generation of metastases to bone and bone
marrow. While these works provided much new insight into cancer cell-parenchyma cell interactions,
they did not address the extravasation process itself. Mastro and Vogler adapted a bioreactor to grow
multiple-cell-layer osteogenic tissues from osteoblast cell lines analyzing the ossification process over a
time period up to 10 months. Breast cancer cells were added to tissues at different stages of phenotypic
maturity and their ability to proliferate, generate microtumors and degrade the osteoblast-derived matrix
were observed [63]. Lescarbeau and colleagues showed that paracrine factors secreted by hMSCs can
increase prostate cancer cell survival while the interaction with a bone marrow-like ECM can lead to
cancer cell morphological changes, chemoresistance and increased levels in the phosphorylation of
proteins involved in cancer-related signaling pathways [64].
Overall, our data lead us to conclude that breast cancer cells found a receptive microenvironment
that supported their growth, proliferation and formation of micrometastases. Extrapolating these results, a
longer culture time could promote the generation of much more organized structures secreting
chemokines and growth factors affecting the local microenvironment.
3.4 Appendix
3.4.1 Calcium production - Preliminary experiments
Preliminary experiments were performed to assess osteo-differentiated (14 days in osteogenic
medium) bone marrow-derived human mesenchymal stem cell (hBM-MSC) production of calcium
deposits in a 2D environment. Cells of passage 7 or lower were cultured for 14 days in standard culture
flasks and Alizarin Red-S assay was performed according to an optimized protocol (see Alizarin Red-S
assay section). Figure AlA shows characteristic dark regions representative of calcium deposits, thus
demonstrating
the
ability
of osteo-differentiated
hBM-MSCs
to
produce
mineralized
matrix.
Supplementary experiments were performed to quantitatively characterize osteo-differentiated hBM-MSC
calcium deposition within 96-well plates (cells embedded within collagen gel). Specifically, multiple
88
combinations were tested with cell densities spanning from 150,000 to 750,000 cells/ml and collagen
concentrations
ranging from 2.0 to 6.0 mg/ml. Moreover, gel retraction and degradation were
qualitatively analyzed to choose the optimal condition to apply within microfluidic devices. As shown in
Figure 3.AIB and C, calcium deposition was higher with higher cell densities and stiffer gels, although
not significantly. Furthermore, no apparent gel degradation was noticed within cultured wells. For these
reasons, we decided to use 750,000 cell/ml as optimal cell density and 6.0 mg/ml as ideal collagen
concentration to guarantee the best signaling between osteo-differentiated hBM-MSCs and breast cancer
cells, and at the same time a stiff matrix, better reproducing the in vivo microenvironment and preventing
undesired gel degradation. Pictures were captured through an inverted optical microscope (Nikon Eclipse
Ti), bright field mode.
3.4.2 Alizarin Red-S assay
Calcium deposition by osteo-differentiated hBM-MSCs was characterized through the Alizarin
Red-S assay. Briefly, samples were washed twice with PBS and fixed with ice-cold 70% ethanol (EtOH)
for 1 h at room temperature. Once completely dried after EtOH removal, samples were washed with
double distilled water (ddH 2 O) and incubated with 80 mM Alizarin Red-S (pH 4-4.2) for 15 min at room
temperature. Next, samples were washed with ddH2 O and PBS to remove the excess of staining and
reduce the unspecific staining, respectively. Once completely dried, representative pictures were taken
using an inverted optical microscope (Nikon Eclipse Ti), bright field mode.
3.4.3 Osteo-differentiation immunofluorescence
Osteo-differentiated (14 days in osteogenic medium) hBM-MSC ability to secrete marker
proteins characteristic of bone-specific
cells was tested evaluating osteocalcin,
osteonectin
and
osteopontin production. Preliminary experiments were performed in standard culture flaks and cells were
fixed and labeled with rabbit anti-human osteocalcin (polyclonal; BTI) at 1:500 dilution according to the
89
immunofluorescence protocol described. Figure A2A shows osteocalcin (green) secreted by osteodifferentiated hBM-MSCs. Additionally, control experiments were performed with human umbilical vein
endothelial cells (HUVECs) following the same protocol and a representative image is shown in Figure
3.A2B.
Figure 3.A2C
and D
highlight
osteonectin
(green,
polyclonal
antibody,
Santa
Cruz
Biotechnology, 1:60 dilution) and osteopontin (green, polyclonal antibody, Abcam, 1:100 dilution)
secretion, respectively. Cells were stained for nuclei (4'6-Diamidino-2-Phenylindole (DAPI); 5 mg/ml;
Invitrogen). Pictures were captured through an inverted epi-fluorescence microscope (Nikon Eclipse Ti).
To provide a clear characterization of the microfluidic 3D environment, control experiments were carried
out without the osteo-cell conditioned matrix, demonstrating the absence of osteocalcin (Figure 3.A2E,
3D confocal image).
3.4.4 Live /Dead assay
Preliminary experiments were performed to analyze osteo-differentiated hBM-MSC viability
within microfluidic devices. Cells were cultured within standard devices before breast cancer cell seeding
and stained with 1 pl fluorescein diacetate (FDA, green; Sigma-Aldrich) and 3.5 tl propidium iodide (PI,
red; Sigma-Aldrich) diluted in 1 ml PBS. Samples were incubated for 5 min, washed with PBS and
observed through confocal microscopy. Figure 3.A3 shows a confocal image of the osteo-cell conditioned
matrix in which homogeneously dispersed cells appear viable.
3.4.5 Endothelial cell monolayer quality
To demonstrate the generation of a confluent endothelial cell barrier, samples were fixed (see
Immunofluorescent staining section) and stained with vascular endothelial-cadherin
(VE-cadherin)
antibody (polyclonal; Abcam) at 1:100 dilution, and cell-cell junctions were visualized (green).
Endothelial cells (stained for nuclei, DAPI, blue) formed a continuous monolayer spanning the area of the
microchannel surfaces and the matrix-channel interfaces (Figure 3.A4A). The presence of osteo-
90
differentiated hBM-MSCs did not affect the generation of the intercellular junction network and no
apparent gaps were detected.
Additional experiments were performed to evaluate the presence of a functional basal membrane
underlying
the
endothelial
monolayer.
Laminin
was
chosen
as
representative
protein
and
immunofluorescence pictures were captured through confocal microscopy. Samples were fixed and
subsequently stained (see Immunofluorescent staining section) with laminin antibody (polyclonal; abcam)
at 1:100 dilution. The presence of laminin (Figure 3.A4B) is due both to the Matrigel"
coating applied
before endothelial cell seeding and to the secretory activity of HUVECs, that concurs to the generation of
a physiological microenvironment.
3.4.6 Collagen structure
The matrix generated by different collagen gel concentrations (2.0 and 6.0 mg/ml), collagen gel
with and without osteo-differentiated hBM-MSC, and with and without cancer cells were analyzed by
means of confocal microscopy - reflectance mode. Figure 3.A4 C-D, Figure 3.A5, and Figure 3.A6 show
the different fiber thickness and organization within the two matrices.
3.4.7 Effect on endothelial monolayer permeability of cancer cells
Fluorescent dextran (70 kDa Texas Red; Invitrogen) was mixed with endothelial growth medium
(EGM-2MV; Lonza) at a concentration of 12.5 ptg/ml and injected in the central media channel of the
microfluidic device while control endothelial growth medium was added to the lateral media channels.
Imaging of the concentration profiles was performed with confocal microscopy (30 min time-lapse) and
dextran diffusion was analyzed by means of a custom software written in MATLAB (MathWorks)
language. The diffusive permeability coefficient
PD
of the endothelial monolayer was computed according
to the following equation:
PD=
-D
91
C/dx
AC
where C represents the dextran concentration proportional to the fluorescence intensity, AC is the
concentration drop across the monolayer, dC/dx the slope of the concentration profile, D the dextran
diffusion coefficient in the osteo-cell conditioned matrix and
P the area
correction factor.
Mass conservation was applied assuming a steady state condition considering that the dextran
flux across the endothelium into the gel region
(PD
- AC - AMonolayer) is equal to the dextran diffusional flux
in the gel (D - dC/dx - AgeI). The area correction factor
p
is equal to the ratio
Agel/AMonolayer
and was
applied to consider changes in the cross-sectional area along the dextran diffusion main direction. Dextran
diffusion coefficient within the matrix was assumed equal to 4.5
x 1011
m 2/s, based on our previous
works [38]. Despite the gel considered in the present model is more concentrated (6.0 mg/mI vs. 2.5
mg/ml), we decided to use the same value considering the small differences found for molecules with
multiple hydrodynamic radii, diffusing in collagen gels of different concentrations [65, 66]. Fluorescence
intensity images were analyzed to compute the concentration gradient and the concentration drop across
the endothelium. Average values were obtained considering at least n = 5 gel regions, including data from
2 independent devices with at least 4 gel regions analyzed per device.
Permeability experiments were performed before breast cancer cell seeding and 24 h later and the
difference was quantified. The basal endothelial permeability was equal to (1.44 ± 0.098)
increased to (5.00 ± 0.84)
x 10-5
x 10-5
cm/s and
cm/s after cancer cell interaction (time point 24 h), thus determining a
3.5-fold increase (Figure 3.A7), whereas there was no significant difference in the control without cancer
cells over the same 24 h period ((1.25 ± 0.21)
x 10-5
cm/s to (1.61
+
0.22)
x 10-5
cm/s). Also the
permeability was measured for devices with and without osteo-differentiated hBM-MSCs in gel, and did
not show significant difference (1.01 ± 0.21)
x
10-5 CM/s to ((1.25 ± 0.21)
x 10- 5 cm/s)
(Figure 3.A8). Our
basal value is higher than in vivo data but lies in the range of previously reported data within in vitro
systems [38, 67, 68]. The higher penneability values compared to in vivo systems could be due to several
physiological factors lacking in our in vitro model. Moreover, mural cells surrounding blood vessels
92
contribute to the stability of the vascular network and help to establish the low permeability value of in
vivo networks [68].
Consistent with our previous works [38, 43], cancer cell interaction determines a significant
increase in the endothelial monolayer permeability that probably plays a pivotal role in the extravasation
(and intravasation) processes. Indeed, several studies have shown how cancer cells can increase vessel
permeability promoting the disruption of the endothelial monolayer integrity. Different mechanisms could
explain these phenomena: direct cell-cell contact between cancer and endothelial cells can alter the
mechanical properties of the endothelium and decrease vessel wall stiffness through the down-regulation
of VE-cadherin and PECAM-I (platelet endothelial cell adhesion molecule) expression [69] or cancer cell
secreted factors (e.g. vascular endothelial growth factor) can determine the disruption of the VE-cadherin-
p-catenin complex [70]. However, more investigations are required to better clarify the causes of
permeability increase.
3.4.8 Quantification of CXCL5 production - Enzyme-linked immunosorbent assay (ELISA)
The ability of osteo-differentiated hBM-MSCs to secrete CXCL5 was analyzed through
CXCL5/ENA-78 Quantikine ELISA Kit (R&D Systems). hBM-MSCs were cultured for 3 weeks within
osteogenic medium and CXCL5 production was quantified and compared to the one of non-differentiated
hBM-MSCs cultured for 1 week in common hBM-MSC growth medium (Figure 3.A9A). As additional
control, CXCL5 concentration was quantified within osteogenic medium and endothelial growth medium
(EGM-2MV; Lonza).
Standard and samples were pipetted into 96-well plates pre-coated with a specific monoclonal
antibody for CXCL5 and incubated for 2 h. Next, after washing to remove unbound molecules, an
horseradish peroxidase-conjugated polyclonal antibody against CXCL5 was added and incubated for 2 h.
Finally, after washing, a substrate solution containing hydrogen peroxide and tetramethylbenzidine was
added and incubated for 30 min. A stop solution containing 2N sulfuric acid was then added and
93
absorbance detected through a microplate reader set to 450 nm. A calibration curve was determined and
data corrected considering optical imperfections within the 96-well plate.
3.4.9 CXCR2 immunofluorescence
Breast cancer cells commonly express CXCR2 receptor [71], a surface protein involved in the
signaling with the chemokine CXCL5. Immunofluorescent staining was performed to demonstrate the
presence of this receptor in the cell line used in our model. Cells were fixed (see Immunofluorescent
staining section) and mouse anti-human CXCR2 (monoclonal; R&D Systems) incubated at a final
concentration of 5 ptg/mI.
Figure 3.A9B shows MDA-MB-231 stained for nuclei (DAPI, blue) expressing CXCR2 (red),
thus confirming the presence of this key surface receptor in our cell line. Picture captured through an
inverted epi-fluorescence microscope (Nikon Eclipse Ti).
3.4.10 Quantifying CXCL5 gradient generation within the osteo-cell conditioned microenvironment
- Computational simulations
To quantify CXCL5 (8.4 kDa; R&D Systems) diffusion within the osteo-cell conditioned matrix,
two dimensional (2D) computational simulations were performed using a finite element method (FEM)
software (COMSOL Multiphysics 4.0; AB, Sweden). The endothelial cell monolayer was modeled as a
barrier with CXCL5 diffusion coefficient 6.32
gel was assumed to be 6.75
x
x 1012
m2 /s, while diffusion coefficient within the collagen
10-1 m 2/s according to our previous works [72]. CXCL5 diffusion
coefficient in the cell culture medium was considered equal to 1.3
x
10-10 m2/s, consistent with literature
values for 10 kDa-dextran. The lateral media channels were considered as CXCL5 sources at time point 0
and diffusion was simulated over 12 h (time-dependent solver: generalized-a; time step: I h). Zero mass
flux conditions were imposed on the device boundaries. The numerical grid for performing the
simulations consisted of approximately 500,000 finite elements.
94
Our results show that a chemoattractant gradient was maintained across the extracellular matrix
(ECM) channels even 12 h after adding stimuli (Figure 3.A12), thus demonstrating the efficacy of our
experimental protocol, optimized to condition cancer cells for a long time period.
3.4.11 Statistics
Extravasation values are averages of measurements in 9 to 39 regions from a minimum of 3 to a
maximum of 9 independent devices. Proliferation data are obtained considering 3 to 10 independent
devices while micrometastasis data come from 15 regions within 4 independent devices. Extravasation
distance values are averaged from a minimum of 11 to a maximum of 17 regions within 4 to 6
independent devices. Results are shown as mean ± standard error of the mean (SEM). The comparisons
between groups were assessed using unpaired Student's t-test or one-way
ANOVA.
Statistical
significance was assumed for p<0.05 (*) or p<0.005 (***). All tests were performed with SigmaPlotl2.
95
B
14
14
12
12,
10
10
T
4
22
0
0
1W0k
300k
460k
600k
760k
density of osteo-cells In gel (cellslml)
6
4
2
coflagen gel density (mglml)
Figure 3.A1. Calcium production. (A) Qualitative analysis of calcium deposition by osteo-differentiated
demonstrating
hBM-MSCs within standard culture flasks. Alizarin Red staining shows dark regions, thus
field. (B
bright
microscope,
the generation of a mineralized matrix. Image obtained with inverted optical
osteoas
(labeled
and C) Quantitative analysis of calcium production by osteo-differentiated hBM-MSCs
from
cells) within 96-well plates (cells embedded within collagen gel). Different cell densities spanning
Error bars
150,000 to 750,000 cells/ml and collagen gel type I concentrations (2-4-6 mg/ml) were tested.
significance
statistical
The
respectively.
(C),
samples
10
=
n
represent SEM for n = 6 samples (B) and
was tested using one-way ANOVA with Bonferroni correction (p<0.05).
AB
of (A)
Figure 3.A2. Osteo-differentiation immunofluorescence assays. 2D osteocalcin immunostaining
(D)
osteo-differentiated hBM-MSCs and (B) control cells (HUVECs). 2D osteonectin (C) and osteopontin
are
nuclei
while
immunostaining of osteo-differentiated hBM-MSCs. Osteo-markers are shown in green
epi-fluorescence
stained with DAPI (blue). Pictures A, B, C and D were captured with inverted
device
microfluidic
a
within
region
gel
representative
a
of
microscope. (E) Confocal 3D reconstruction
protein
fluorescent
(red
HUVECs
deposit.
osteocalcin
without osteo-cell conditioned matrix showing no
(RFP)) were stained with DAPI (nuclei, blue) and phalloidin (F-actin, yellow). Scale bars: 100 pm.
96
Figure 3.A3. Live/Dead assay. Cell viability was assessed within microfluidic devices before cancer cell
seeding. Cells were incubated for 5 min with fluorescein diacetate (green) and propidium iodide (red).
Confocal 3D reconstruction showing osteo-differentiated hBM-MSC viability within the osteo-cell
conditioned microenvironment.
Figure 3.A4. Endothelial monolayer quality and collagen gel structure within microfluidic devices. (A)
Three-dimensional rendering of a confocal stack of a single gel region showing the confluency of the
endothelial monolayer on the 3D extracellular matrix (ECM). Cells were stained with DAPI (nuclei, blue)
and VE-cadherin antibody (green). (B) Laminin immunostaining (green) demonstrating the presence of a
basal membrane underlying the endothelial monolayer (HUVECs, RFP). Two-dimensional projection of a
confocal stack. (C and D) Confocal reflectance image of a single gel region showing the ECM
architecture for (C) 6.0 mg/ml and (D) 2.0 mg/ml collagen gel. Two-dimensional projection of a confocal
stack. Collagen fibers are shown in red.
97
I
osteo-cell (+)
osteo-cell (-)
Figure 3.A5. Confocal reflectance image of 6.0 mg/ml gel with and without osteo-cells 3 days after the
gel-filling. No significant difference was detected in the matrix structure.
osteo cell (+)
osteo-cell (+)
cancer cell (-)
cancer cell (+)
Figure 3.A6. Confocal reflectance images of 6.0 mg/mi collagen gel + osteo-cells with and without
cancer cells 24 h after cancer cell seeding. The presence of cancer cells does not induce clearly detectable
structural changes.
98
7
06am
3
7
0 hr
24 hr
21
0
wl cancer cell w/o cancer cell
Figure 3.A7. Endothelial monolayer permeability change. Fluorescent dextran (70 kDa) was introduced
to measure the endothelial monolayer permeability before and after (24 h later) cancer cell seeding (left).
The same measurements were made with device without addition of cancer cells over 24 h time (right).
Average values across at least n=12 gel regions including data from 2 independent devices. Error bars
represent SEM. The statistical significance was tested with unpaired Student's t-test (p<0.05).
2.0
T
T
1.6
0. 0
0.0.
wlo Osteo
W/ osteo
Figure 3.A8. Endothelial monolayer permeability change. Fluorescent dextran (70 kDa) was introduced
to measure the endothelial monolayer permeability of devices with (right) and without (left) osteodifferentiated hBM-MSCs in gel. Average values across at least n=5 gel regions including data from 2
independent devices. Error bars represent SEM. The statistical significance was tested with unpaired
Student's t-test (p<0.05).
99
A
10.
osteo-cenl
MSC
0.1-*
___---
I
II1
0.01.
0.001
I
I
C100pm
10
10000
1000
100
(pg/ml)
concentration
Figure A9. CXCL5 quantification assay and CXCR2 detection. (A) Enzyme-linked immunosorbent assay
(ELISA) was used to analyze the chemokine production of 3 weeks old osteo-differentiated hBM-MSCs
and I week old non-differentiated hBM-MSCs. Calibration curve shows absorbance (arbitrary unit, log
scale) vs. CXCL5 concentration (pg/ml, log scale). Mean detected values for the 2 samples are shown
with red triangular spots. (B) Immunofluorescence assay was performed to assess the presence of CXCR2
receptor (red) on the surface of MDA-MB-231 breast cancer cells. Cells were stained with DAPI (nuclei,
blue). Image captured with an inverted epi-fluorescence microscope.
70.
o.l
-301
10.
0
0
1
3
2
4
5
6
# cancer cell clusters per ROI
per
Figure A10. Scatter plot representing the relationship between number of cancer cells
Large
micrometastasis and number of cancer cell micrometastases per region of interest (ROI).
micrometastases (>30 cells) were detected in isolation or associated with another small micrometastasis
containing 5 cells (n=15 regions).
100
day 3
day 2
day I
day 5
day 4
200UISO.
160.1401120100-
o,
60'
C
40,
a
20
0
0
2
1
3
6
5
4
days after cancer cell seeding
device
Figure All. Day-to-day progression of cancer cell clusters. Cancer cell number increase per
of one
images
day-to-day
show
Images
within ROIs was analyzed among day 1, 2, 3 and 5 after seeding.
n=3(min)-10(max)
representative ROL. Scale bars: 30 tm. Average values are considered across
independent devices. Error bars represent SEM.
B
- EC
channel
q gelI
120.
0h
1
qb
I
so.
o.
h
I
I
6h
---
0 nglmI
)k
6h
-200
200
00
0
1000
2000
12h
3000
pos-on (pm)
1(
12 h
device.
Figure A12. Computational simulation of the CXCL5 gradient within the microfluidic
in the
Colorimetric maps and concentration profiles (measured along the horizontal dashed line drawn
(0points
time
different
at
device
microfluidic
the
within
top-left map) showing the chemokine diffusion
1-6-12 h).
101
References
I.
2.
Bersini, S., et al., 3D in vitro model for specificity of breast cancer metastasis to bone.
Biomaterials, in press.
Chaffer, C.L. and R.A. Weinberg, A perspective on cancer cell metastasis. Science, 2011.
331(6024): p. 1559-64.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Valastyan, S. and R.A. Weinberg, Tumor metastasis: molecular insights and evolving paradigms.
Cell, 2011. 147(2): p. 275-92.
Chambers, A.F., A.C. Groom, and I.C. MacDonald, Dissemination and growth of cancer cells in
metastatic sites. Nat Rev Cancer, 2002. 2(8): p. 563-72.
Fidler, I.J., The pathogenesis of cancer metastasis: the 'seed and soil' hypothesis revisited. Nat
Rev Cancer, 2003. 3(6): p. 453-8.
Gupta, G.P. and J. Massague, Cancer metastasis: building a framework. Cell, 2006. 127(4): p.
679-95.
Hanahan, D. and R.A. Weinberg, The hallmarks of cancer. Cell, 2000. 100(1): p. 57-70.
Joyce, J.A. and J.W. Pollard, Microenvironmentalregulationof metastasis. Nat Rev Cancer, 2009.
9(4): p. 239-52.
Fukuda, M., N. Hiraoka, and J.C. Yeh, C-type lectins and sialyl Lewis X oligosaccharides.
Versatile roles in cell-cell interaction.J Cell Biol, 1999. 147(3): p. 467-70.
Miles, F.L., et al., Stepping out of the flow: capillary extravasation in cancer metastasis. Clin
Exp Metastasis, 2008. 25(4): p. 305-24.
Zipin, A., et al., Tumor-microenvironment interactions: the fucose-generating FX enzyme
controls adhesiveproperties of colorectalcancer cells. Cancer Res, 2004. 64(18): p. 657 1-8.
Khatib, A.M., et al., Characterizationof the host proinflammatory response to tumor cells during
the initialstages of'liver metastasis.Am J Pathol, 2005. 167(3): p. 749-59.
Roussos, E.T., J.S. Condeelis, and A. Patsialou, Chemotaxis in cancer. Nat Rev Cancer, 2011.
11(8): p. 573-87.
Al-Mehdi, A.B., et al., Intravascularorigin of metastasisfrom the proliferationof endotheliumattachedtumor cells: a new model for metastasis.Nat Med, 2000. 6(1): p. 100-2.
Kebers, F., et al., Induction of endothelial cell apoptosis by solid tumor cells. Exp Cell Res, 1998.
240(2): p. 197-205.
Paget, S., The distributionof secondary growths in cancer of the breast. 1889. Cancer Metastasis
Rev, 1989. 8(2): p. 98-101.
Bussard, K.M., C.V. Gay, and A.M. Mastro, The bone microenvironment in metastasis; what is
special about bone? Cancer Metastasis Rev, 2008. 27(1): p. 41-55.
Coleman, R.E., Skeletal complications of malignancy. Cancer, 1997. 80(8 Suppl): p. 1588-94.
Naumov, G.N., et al., Cellular expression of green fluorescent protein, coupled with highresolution in vivo videomicroscopy, to monitor steps in tumor metastasis. J Cell Sci, 1999. 112
( Pt 12): p. 1835-42.
Stoletov, K., et al., Visualizing extravasation dynamics of metastatic tumor cells. J Cell Sci, 2010.
123(Pt 13): p. 2332-41.
Goldstein, R.H., R.A. Weinberg, and M. Rosenblatt, Of mice and (wo)men: mouse models of
breast cancer metastasis to bone. J Bone Miner Res, 2010. 25(3): p. 431-6.
Kuperwasser, C., et al., A mouse model of human breast cancer metastasis to human bone.
Cancer Res, 2005. 65(14): p. 6130-8.
Kemppainen, J.M. and S.J. Hollister, Differential effects of designed scaffold permeability on
chondrogenesis by chondrocytes and bone marrow stromal cells. Biomaterials, 2010. 31(2): p.
279-87.
102
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
Florczyk, S.J., et al., Porous chitosan-hyaluronic acid scaffolds as a mimic of glioblastoma
microenvironmentECM. Biomaterials, 2013. 34(38): p. 10143-50.
Hendrix, M.J., et al., A simple quantitative assay for studying the invasive potential of high and
low human metastatic variants. Cancer Lett, 1987. 38(1-2): p. 137-47.
Sagnella, S.M., et al., Human microvascular endothelialcell growth and migrationon biomimetic
surfactantpolymers. Biomaterials, 2004. 25(7-8): p. 1249-59.
Uygur, B. and W.S. Wu, SLUG promotes prostate cancer cell migration and invasion via
CXCR4/CXCLI2 axis. Mol Cancer, 2011. 10: p. 139.
Kothapalli, C.R. and R.D. Kamm, 3D matrix microenvironmentfor targeted differentiation of
embryonic stem cells into neural and glial lineages. Biomaterials, 2013. 34(25): p. 5995-6007.
Nie, F.Q., et al., On-chip cell migration assay using microfluidic channels. Biomaterials, 2007.
28(27): p. 4017-22.
Yang, K., et al., A microfluidic array for quantitative analvsis of human neural stein cell selfrenewal and differentiation in three-dimensionalhypoxic microenvironment. Biomaterials, 2013.
34(28): p. 6607-14.
Leclerc, E., et al., Study of osteoblastic cells in a microfluidic environment. Biomaterials, 2006.
27(4): p. 586-95.
Huang, Y., et al., Microfluidics-baseddevices: New tools for studying cancer and cancer stem
cell migration. Biomicrofluidics, 2011. 5(1): p. 13412.
Chung, S., et al., Cell migration into scaffolds under co-culture conditions in a microfluidic
platform. Lab Chip, 2009. 9(2): p. 269-75.
Sung, K.E., et al., Transition to invasion in breast cancer: a microfluidic in vitro model enables
examination ofspatial and temporal effects. Integr Biol (Camb), 2011. 3(4): p. 439-50.
Liu, T., et al., A microfluidic devicefor characterizingthe invasion of cancer cells in 3-D matrix.
Electrophoresis, 2009. 30(24): p. 4285-91.
Haessler, U., et al., Migration dynamics of breast cancer cells in a tunable 3D interstitialflow
chamber. Integr Biol (Camb), 2012. 4(4): p. 401-9.
Mak, M., C.A. Reinhart-King, and D. Erickson, Elucidating mechanical transition ejfects of
invading cancer cells with a subnucleus-scaledmicrofluidic serial dimensionalmodulation device.
Lab Chip, 2013. 13(3): p. 340-8.
Zervantonakis, I.K., et al., Three-dimensionalmicrofluidic model Jor tumor cell intravasationand
endothelial barrierfunction. Proc Natl Acad Sci U S A, 2012. 109(34): p. 13515-20.
Song, J.W., et al., Microfluidic endothelium for studying the intravascularadhesion of metastatic
breast cancer cells. PLoS One, 2009. 4(6): p. e5756.
Zhang, Q., T. Liu, and J. Qin, A microfluidic-baseddevice for study of transendothelialinvasion
of tumor aggregatesin realtime. Lab Chip, 2012. 12(16): p. 2837-42.
Shin, M.K., S.K. Kim, and H. Jung, Integration of intra- and extravasation in one cell-based
microjluidic chipfor the study of cancer metastasis. Lab Chip, 2011. 11(22): p. 3880-7.
Ma, C. and X.F. Wang, In vitro assays fJr the extracellular matrix protein-regulated
extravasationprocess. CSH Protoc, 2008. 2008: p. pdb prot5034.
Jeon, J.S., et al., In vitro model of tumor cell extravasation. PLoS One, 2013. 8(2): p. e56910.
Heyder, C., et al., Realtime visualization of tumor cell/endothelial cell interactions during
transmigrationacross the endothelial barrier.J Cancer Res Clin Oncol, 2002. 128(10): p. 533-8.
Chaw, K.C., et al., Multi-step microfluidic devicefor studying cancer metastasis. Lab Chip, 2007.
7(8): p. 1041-7.
Roodman, G.D., Mechanisms of bone metastasis. N Engl J Med, 2004. 350(16): p. 1655-64.
Mundy, G.R., Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev
Cancer, 2002. 2(8): p. 584-93.
Shin, Y., et al., Microfluidic assay for simultaneous culture of multiple cell types on surfoces or
within hydrogels. Nat Protoc, 2012. 7(7): p. 1247-59.
103
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
Chung, S., et al., Microfluidic platformsfor studies of angiogenesis, cell migration, and cell-cell
interactions.Sixth InternationalBio-Fluid Mechanics Symposium and Workshop March 28-30,
2008 Pasadena,California.Ann Biomed Eng, 2010. 38(3): p. 1164-77.
Lopa, S., et al., Orthopedic bioactive implants: Hydrogel enrichment of macroporoustitaniumfor
the delivery of mesenchymal stem cells and strontium. J Biomed Mater Res A, 2013.
Minn, A.J., et al., Genes that mediate breast cancer metastasis to lung. Nature, 2005. 436(7050):
p. 518-24.
Bos, P.D., et al., Genes that mediate breast cancer metastasis to the brain. Nature, 2009.
459(7249): p. 1005-9.
Gjerdrum, C., et al., Axl is an essential epithelial-to-mesenchymal transition-inducedregulatorof
breast cancer metastasis andpatientsurvival. Proc Natl Acad Sci U S A, 2010. 107(3): p. 1124-9.
Hsu, Y.L., et al., Breast tumor-associated osteoblast-derived CXCL5 increases cancer
progressionby ERK/MSKJ/Elk-1/snail signalingpathway. Oncogene, 2013. 32(37): p. 4436-47.
Vuoriluoto, K., et al., Vimentin regulates EMT induction by Slug and oncogenic H-Ras and
migration by governingAxl expression in breast cancer.Oncogene, 2011. 30(12): p. 1436-48.
Chung, E.J., et al., Osteogenic potential of BMP-2-releasingself-assembled membranes. Tissue
Eng Part A, 2013.
Huang, C. and R. Ogawa, Effect of hydrostatic pressure on bone regeneration using human
mesenchymal stem cells. Tissue Eng Part A, 2012. 18(19-20): p. 2106-13.
Perez, R.A., et al., Utilizing core-shellfibrous collagen-alginatehydrogel cell delivery system for
bone tissue engineering.Tissue Eng Part A, 2013.
Halpern, J.L., A. Kilbarger, and C.C. Lynch, Mesenchymal stem cells promote mammary cancer
cell migration in vitro via the CXCR2 receptor. Cancer Lett, 2011. 308(1): p. 91-9.
Muller, A., et al., Involvement of chemokine receptors in breast cancer metastasis. Nature, 2001.
410(6824): p. 50-6.
Jamieson-Gladney, W.L., et al., The chemokine receptor CX(3)CRJ is directly involved in the
arrest of breast cancer cells to the skeleton. Breast Cancer Res, 2011. 13(5): p. R9 1.
Cserni, G., et al., Variations in sentinel node isolated tumour cells/micrometastasis and nonsentinel node involvement rates accordingto different interpretationsof the TNM definitions. Eur
J Cancer, 2008. 44(15): p. 2185-91.
Mastro, A.M. and E.A. Vogler, A three-dimensional osteogenic tissue model for the study of
metastatic tumor cell interactionswith bone. Cancer Res, 2009. 69(10): p. 4097-100.
Lescarbeau, R.M., et al., In vitro model of metastasis to bone marrow mediates prostate cancer
castrationresistantgrowth through paracrineand extracellularmatrix factors. PLoS One, 2012.
7(8): p. e40372.
Armstrong, J.K., et al., The hydrodvnamic radii of macromolecules and their effect on red blood
cell aggregation.Biophys J, 2004. 87(6): p. 4259-70.
Ramanujan, S., et al., Diffusion and convection in collagen gels: implicationsfor transport in the
tumor interstitium.Biophys J, 2002. 83(3): p. 1650-60.
Albelda, S.M., et al., Permeabilitycharacteristicsof cultured endothelial cell monolayers. J Appl
Physiol, 1988. 64(1): p. 308-22.
Michel, C.C. and F.E. Curry, Microvascularpermeability.Physiol Rev, 1999. 79(3): p. 703-61.
Mierke, C.T., Cancer cells regulate biomechanical properties of human microvascular
endothelial cells. J Biol Chem, 2011. 286(46): p. 40025-37.
Weis, S., et al., Endothelial barrierdisruption by VEGF-mediated Src activity potentiates tumor
cell extravasationand metastasis. J Cell Biol, 2004. 167(2): p. 223-9.
Hsu, Y.L., et al., Breast tumor-associated osteoblast-derived CXCL5 increases cancer
progression by ERK/MSK1/Elk-i/Snail signalingpathway. Oncogene, 2012.
Han, S., et al., A versatile assay for monitoring in vivo-like transendothelial migration qf
neutrophils.Lab Chip, 2012. 12(20): p. 3861-5.
104
Chapter 4
Generation 3D functional microvascular
networks with mural cell-differentiated human
mesenchymal stem cells 4
4.1 Introduction
A functional microvascular network is essential to deliver nutrients, oxygen and immune cells to
tissues and organs [2]. Endothelial cells (ECs) contribute to the maintenance of vascular integrity by
developing tight and adherens junctions [3] and express a broad spectrum of receptor molecules such as
selectins, vascular cell adhesion molecules and intercellular adhesion molecules involved in multiple cellcell interactions [4, 5]. However, the generation of a functional vasculature involves the recruitment of
mural cells, and the development of organ-specific matrices and elastic laminae surrounding blood vessels
[2, 6].
There are numerous factors that are involved in vessel development and maturation. A variety of
vascular endothelium-specific molecules cooperate to promote the generation of microvascular networks,
including five members of the vascular endothelial growth factor (VEGF) family, four molecules
belonging to the angiopoietin group and one of the large ephrin family [7], Other non-endothelium
4 This chapter is modified from Ref. [1].
105
specific growth factors are also required for blood vessel formation, such as proteins of the transforming
growth factor-P family [8]. The newly formed microvessels are stabilized by recruited mural cells, i.e.
pericytes, smooth muscle cells and fibroblasts, which contribute to the deposition of the local extracellular
matrix (ECM)
[2]. ECs secrete proteins such as platelet derived growth factor (PDGF)-B and
sphingosine- 1-phosphate-I (SiP1) to promote mural cell recruitment [9, 10] while mural cells secrete
multiple factors including angiopoietin (Ang)-1, which leads to leak-resistant vessels maximizing the
interactions between ECs and surrounding support cells [11]. Transforming growth factor (TGF)-P I is a
multifunctional cytokine produced by both mural cells and ECs which is involved in multiple processes,
including ECM production and mesenchymal cell differentiation to mural cells, with both pro- and antiangiogenic properties depending on concentration and local microenvironment [12-14].
The generation of physiological-like microvascular systems is required for the development of
both in vivo long-lasting blood vessels [15, 16] and advanced in vitro models able to better replicate
multiple biological phenomena where the interaction between capillaries and organ-specific tissues is
critical. Several 2D in vitro models were developed in the last years to investigate vascular network
related phenomena, such as mesenchymal cell differentiation into smooth muscle cells upon co-culture
with ECs [17, 18] or VEGF-induced vessel permeability [19]. However, the importance of 3D in vitro
models lies in the possibility to mimic physiological cell-cell and cell-matrix interactions within
biological or synthetic matrices where cells show morphologies and differentiation abilities considerably
different from those observed on 2D surfaces [20-24]. Three dimensional assays were perfornmed to study
angiogenesis under controlled chemical gradients [25] and different methods were applied to replicate
microvessel structure including EC-coated microbeads dispersed within fibrin gels [26], collagen
patterned microfluidic vascular networks with perivascular cells [27, 28], templated hydrogels with
sacrificial gelatin channels [29], microtissue chambers with multiple interstitial flow and hypoxia
conditions [30]. Microfluidic devices were developed to investigate the anastomosis of endothelial
sprouts [31, 32], sprouting angiogenesis under chemical gradients [33], tumor-endothelial cell interactions
106
[34] and promising techniques, as the so-called "viscous finger patterning", were optimized to generate
tubular structures within microfluidic platforms [35]. Moreover, recent studies analyzed the effect of
endothelial secreted factors such as PDGF-B in the regulation of pericyte recruitment [36] and the
influence these stabilizing cells provide in terms of endothelial basement membrane generation and
expression of integrins that recognize the newly deposited matrix [37].
The present study is focused on the generation of a 3D functional, perfusable human
microvascular
network
by vasculogenesis,
co-culturing
ECs
and bone
marrow-derived
human
mesenchymal stem cells (BM-hMSCs) within a microfluidic device. The ability of stem cells to acquire a
mural phenotype is critical developing physiological microvessels. In this framework, we investigated the
effect of Ang- 1, a key molecule in vessel stabilization [5], whose role could be related to the recruitment
of mesenchymal cells [38-40]. Moreover, we analyzed the effect of the cytokine TGF-plto better clarify
its influence on mesenchymal cell differentiation, which was not uniquely defined by previous studies
[12-15, 41]. Our model represents a significant step forward toward the generation of more physiological
microvessels compared to endothelialized microchannels or micronetworks generated within 3D gel or
spheroids suspended in standard multiwall plates. We demonstrated the co-culture of ECs and BMhMSCs leads to the generation of physiological-like human microvascular networks in which easily
available bone marrow multipotent cells get a mural cell phenotype and co-localize with ECs.
Particularly, we showed the double role of Ang-I as vessel stabilizer and mural cell differentiation
promoter. This system could be potentially used to develop advanced in vitro models to study and
characterize complex biological phenomena involving blood vessels, such as intra- and extravasation of
circulating tumor cells (CTCs) or immune cells [42], and better clarify pathophysiological shear stress
conditions on in vivo-like capillaries [43, 44].
107
4.2 Experimental Section
4.2.1 Microfluidic System
A microfluidic device consisting of two lateral media channels and a central gel channel was
adopted in the present work. Microfabrication details were previously reported for other systems
developed by our group [45, 46]. Briefly, the microfluidic device was made of PDMS (poly-dimethylsiloxane; Silgard 184, Dow-Chemical) through soft lithography techniques and SU-8 micropatterned
silicon wafers. Inlet and outlet ports were bored by means of disposable biopsy punches and the PDMS
structure was bonded to a glass coverslip after 60 s oxygen plasma treatment to create 200 Pm deep
microchannels. Trapezoidal posts with an inter-post distance of 330 pm were employed to separate the
1,300 pm wide gel channel from the lateral media channels and promote an ideal gel filling. Microfluidic
channels were coated with PDL (poly-D-lysine hydrobromide; I mg/ml; Sigma-Aldrich) solution to
promote matrix adhesion. Next, a thrombin solution, obtained dissolving 10 pl thrombin (100 U/ml)
within 500 pl cell culture medium, was used to resuspend cells and 10 pl aliquots were mixed with 10 pl
fibrinogen solution (5.0 mg/ml) to generate a fibrin gel. A 10 pl pipette was used to fill the gel channel
and microdevices were incubated within humid chambers for 10 min at room temperature to form the
hydrogel. Following gelation, cell culture medium was added to the media channels and microfluidic
devices were cultured for at least 7 days with daily medium replacement.
108
A
B
mural cell
differentiated
BM-hMSCs
vascular network
of HUVECs
Figure 4.1. Schematic of the microfluidic vasculogenesis system. Microfluidic device composed by two
lateral media channels and one interposed 1,300 pm wide gel channel embedding HUVECs and BMhMSCs in a 2:1 ratio (A). A vasculogenesis approach allows the generation of functional, perfusable
microvascular networks with ECs (red) surrounded by mural cell differentiated BM-hMSCs (green) in a
fibrin matrix (B).
4.2.2 Cell Culture
BM-hMSCs were harvested from patients undergoing hip arthroplasty and selected by plastic
adherence according to a previously optimized protocol [47]. Cells of passage 6 or lower were cultured in
standard alpha-minimum essential medium (aMEM; Invitrogen) containing non-essential amino acids,
sodium pyruvate and L-glutamine, supplemented with 10% fetal bovine serum (FBS; Invitrogen),
biological buffer and antibiotics. Red fluorescent protein (RFP)-transfected human umbilical vein
endothelial cells (HUVECs) were commercially obtained (Angio-Proteomie) and cultured in endothelial
growth medium (EGM-2MV; Lonza) with full supplements (EGM-2MV bullet kit; Lonza), which was
considered as standard endothelial growth medium. All the experiments were conducted using HUVECs
of passage 6. HUVECs were suspended at 12x 106 cells/mI in standard endothelial growth medium +
thrombin and mixed with BM-hMSCs (6x 106 cells/ml suspension in BM-hMSC growth medium +
thrombin). The obtained suspension was mixed with fibrinogen solution (1:1 ratio) and injected into the
109
gel channel. After gelation, lateral media channels were filled with standard endothelial growth medium
supplemented with 50 ng/ml VEGF (Peprotech). The medium was replaced every 24 hours. All cultures
were kept in a humidified incubator maintained at 37'C and 5% CO 2 . After day 1, selected microdevices
were cultured with standard endothelial growth medium supplemented with 50 ng/ml VEGF and 100
ng/ml Ang-1 (Peprotech) or 1 ng/ml TGF-p1 (Peprotech) to analyze the effect of these molecules on
microvascular network generation and BM-hMSC differentiation toward a mural cell lineage. In order to
promote the generation of perfusable microvascular networks, HUVECs were seeded at day 2 within
lateral media channels of the identified optimal configuration, introducing 40 pl cell suspension at Ix106
cells/ml cell density. A schematic representing the microfluidic device and the cell culture model is
shown in Figure 4.4.1. Control experiments were performed seeding HUVECs without BM-hMSCs at the
same cell density applied in co-culture assays and the vasculatures generated were analyzed in the same
manner.
Furthermore,
BM-hMSC
differentiation
control
experiments
were
conducted
seeding
mesenchymal stem cells alone at the same cell density set for co-cultures. The influence of the direct
contact between ECs and BM-hMSCs was assessed seeding mesenchymal stem cells into the gel region
and a HUVEC monolayer on the interface between gel and media channels.
4.2.3 Immunofluorescent Staining
Samples were washed with phosphate buffered saline (PBS; Invitrogen) and fixed with 4%
paraformaldehyde (PFA) for 15 min at room temperature. Next, cells were washed twice with PBS and
incubated with 0.1% Triton-X 100 solution for 5 min at room temperature. After washing twice with PBS,
cells were blocked with 5% bovine serum albumine (BSA) + 3% goat serum solution for at least 3h at
4'C. Alpha-smooth muscle actin (a-SMA) was labeled with mouse polyclonal antibody (abcam) at 1:100
dilution, SM22a was labeled with rabbit polyclonal antibody (abcam) at 1:1000 dilution, vascular
endothelial-cadherin (VE-cadherin) and laminin were labeled with rabbit polyclonal antibody (abcam) at
1:100 dilution, and zonula occludens- I (ZO- 1) was labeled with mouse polyclonal antibody (Invitrogen)
110
at 1:100 dilution. Fluorescently labeled secondary antibodies (Invitrogen) were used at 1:200 dilution.
Cell nuclei were stained with 4'6-Diamidino-2-Phenylindole (DAPI;5 mg/ml; Invitrogen)at 1:500 dilution
while F-actin filaments were stained with AlexaFluor633 phalloidin (Invitrogen) at 1:100 dilution. If not
differently specified, all the images were captured using a confocal microscope (Olympus IX81) and
processed with Imaris software (Bitplane Scientific Software).
4.2.4 Data Analysis
4.2.4.1 Microvascular Network Morphology
Microvascular networks were analyzed using Fiji software (http://fiji.sc/Fiji). The endothelial cell
RFP signal was used to compute projected 2D areas of the network and the Fiji 2D skeletonize plugin was
applied to detennine the number of branches, average branch length and total network length. Projected
3D stacks representing each region of interest (ROI, 533x426 Pim2) were pre-processed with Fiji software
to enhance contrast (10%), filter noise (application of "despeckle" algorithm and "gaussian blur" filter)
and convert the image to a binary format by applying the "triangle" threshold method [48]. In addition,
the Fiji 3D skeletonize plugin was used to further analyze the number of branches in the longest structure
detected within each ROI, according to the above-mentioned protocol. Moreover, 3D skeletonize data
were noise filtered applying a 25 im threshold value to remove image artifacts. The threshold value was
calculated by averaging multiple measurements and comparing 3D confocal images to 3D skeleton
reconstructions.
Note that to the extent that vessels cross at different z-planes, this could lead to errors in
estimating the number of branches and vessel segments. To quantify this effect, 2D and 3D skeletons
were compared as described in the "Generation of Microvascular Networks" section.
Finally, the average vessel diameter was quantified with Imaris software. The temporal evolution
of the network was daily monitored by phase-contrast and fluorescence microscopy (Nikon Eclipse Ti).
111
4.2.4.2 Quantification of BM-hMSC Differentiation
BM-hMSC differentiation was quantified through the a-SMA signal in terms of percentage of
active pixels, mean signal intensity and total signal intensity (normalized by the minimum value among
the three conditions) within each ROI. All intensity values were obtained after subtracting the background
signal.
4.2.4.3 Microvascular Network Perfusion and Permeability Quantification
Vessel permeability was quantified according to a previously described method [49]. Briefly, the
medium in all reservoirs was aspirated and two reservoirs of the opposite media channels were injected
with 40pl of fluorescent dextran (70kDa, green, Invitrogen) diluted with endothelial growth medium for a
final concentration of 12.5 pg/ml. Concentrations were then determined by confocal imaging every 1 min
for 5 min once equilibrium was established (i.e. constant intensity within the vessels, 5-10 min).
Penneability was quantified by obtaining the average intensity at the initial and final time points
considering a region of interest including both the vessel and the surrounding ECM. Permeability was
computed considering vessel segments in the central region of the gel channel to avoid border effects
according to the following formula [49]:
P
where IA i
and
'h
(i Ii-
I
Ii - Ib
At
d
4
represent the initial, final and background average intensities, At is the time interval
between two captured images and d is the average diameter of the vessel.
Finally, 40 p of medium containing 10 pm fluorescent microspheres were introduced within a single
reservoir (medium was aspirated from the other reservoirs) of a live sample to demonstrate the presence
of a perfusable microvascular network connecting lateral media channels.
112
4.2.4.4. Statistics
Microvascular network and differentiation data are averages of measurements of 6 (min)-9 (max)
regions from 3 independent devices. Results are shown as mean
±
standard error of the mean (SEM). The
comparisons between groups were assessed using unpaired Student's t-test. Statistical significance was
assumed for p < 0.05. All tests were performed with SigmaPlot12.
4.3 Results and Discussion
4.3.1 Differentiation of BM-hMSCs into Mural Cells
Ability of BM-hMSCs to differentiate into mural cells was increased in presence of HUVECs
(Figure 4.2). Differentiation can be visualized by staining with mural cell marker, a-SMA (Figure 4.2AC, green). Addition of Ang-1 or TGF-p1 in supplement to VEGF-rich standard endothelial growth
medium induced even more differentiation, as quantified by both percent area covered and intensity
signal of mural cell marker. Differentiated BM-hMSCs covered 4.63 - 0.77% of the entire area imaged
on devices supplemented with VEGF only while VEGF+Ang-1 and VEGF+TGF-Pl added devices
showed significantly higher results, with values equal to 14.2± 1.52% and 14.3
(Figure 4.2D). The mean intensity of a-SMA marker was 2.11
devices and 2.36
±
1.13%, respectively
0.32 folds higher with VEGF+Ang-I
0.32 folds higher with VEGF+TGF-pI than VEGF only devices (Figure 4.2E). The
total sum of a-SMA signal was 4.72
devices showed values 5.06
Differentiated
±
±
±
±
0.99 fold higher with VEGF+Ang- I whereas VEGF+TGF-P I
0.79 folds higher when normalized to VEGF only devices (Figure 4.2F).
BM-hMSCs co-localized
with HUVECs and wrapped around the newly formed
microvessels, thus contributing to the generation of a functional microvascular network (Figure 4.3A and
B, a-SMA labeled in green). Culturing BM-hMSCs in VEGF supplemented standard endothelial growth
medium did not induce differentiation nor did the addition of VEGF+Ang-1 or VEGF+TGF-Pl without
113
HUVECs (Figure 4. 3B-D, F-actin stained with phalloidin, yellow). The generation of HUVEC
monolayers on the interface between gel and media channel showed that only those BM-hMSCs that
reached ECs were able to differentiate (Figure 4.3E, a-SMA labeled in green; F-actin stained in with
phalloidin, yellow), thus demonstrating how a direct contact is required to induce a mural cell phenotype.
-"s-
.
D
1412
0
VEGF
E
n.s.
S3.01
VEOF + Angi VEOF + TOF-01
F
ns
4
~.1.0
3
VEGF
VEGF +Arg1
VEGF + TOF-01
VEGF VEGF + Ang1 VEOF +TGF-01
Figure 4.2. Differentiation of BM-hMSCs in presence of HUVECs. When co-cultured with HUVECs,
BM-hMSCs can differentiate into mural cells. Differentiation can be visualized by staining with mural
cell marker, a-smooth muscle actin (green). Cell nuclei were stained with DAPI (blue). (A-C). Addition
of Ang-1 or TGF-p1 in VEGF supplemented standard endothelial growth medium induces even more
differentiation, as quantified by both percent area covered and mural cell marker intensity (D-F). Scale
bars represent 100 pm.
114
Several studies investigated mesenchymal cell differentiation, testing direct contact with
endothelial cells [50], effect of mechanical stress [51] and addition of different molecules, including TGF-
Pl [52] and sphingosylphosphorylcholine (SPC) [53]. However, they did not analyze the influence of the
aforementioned factors in a 3D microenvironment, which plays a critical role within in vitro models [22].
Figure 4.3. Co-localization of HUVECs and BM-hMSCs enabled differentiation of BM-hMSCs into
mural cells. Most of BM-hMSCs that differentiated into mural cells (a-SMA, green) co-localized with
vasculature formed by RFP-transfected HUVECs (red) in fibrin gel (A). Culturing BM-hMSCs in VEGF
of
supplemented standard endothelial growth medium did not induce differentiation nor did addition
VEGF+Ang-l or VEGF+TGF-p1 without HUVECs (F-actin stained with phalloidin, yellow) (B-D).
When HUVECs (red) were cultured within a lateral media channel and BM-hMSCs in the fibrin gel, only
those BM-hMSCs that reached HUVECs showed signs of differentiation (a-SMA, green; F-actin, yellow)
(E). Cell nuclei were F-actin was stained with phalloidin (yellow). Cell nuclei were stained with DAPI
(blue). Scale bars represent 100 4m.
In our project we examined the influence of EC direct contact and the effect of additive
3D
molecules, i.e. Ang-1 and TGF-pl, on BM-hMSC differentiation in a more physiological-like
115
microenvironment. Although the role of Ang-I in vessel stabilization is well described [7], only a few
studies investigated the effect of this molecule on smooth muscle-like cells recruitment [38-40]. In this
framework, we have shown addition of Ang-1 (100 ng/ml) not only recruited smooth muscle-like cells,
but also induced BM-hMSC differentiation toward mural cells, when mediated by EC co-culture.
Furthermore, our results show that the addition of TGF-p1 (1 ng/ml) does not have a significant influence
on BM-hMSC commitment toward a mural cell lineage, in agreement with results shown by Au and coauthors [15], which used even higher concentrations (10 ng/ml). However, other studies highlighted the
effect of this molecule on the expression of mural cell markers [12, 54], thus suggesting how the role of
this multifunctional cytokine is not totally clear and could promote different responses in different
conditions (concentrations, cell type, cell microenvironment) [2]. Addition of TGF-P3
induced a strong
differentiation of BM-hMSC only in presence of an EC direct contact, implying that TGF-PI molecular
pathway promoting mural cell differentiation involves a close interaction with ECs.
4.3.2 Generation of Microvascular Networks
As we found that HUVECs had crucial role in differentiating BM-hMSCs into mural cells, we
investigated, in reverse, the role of differentiated
BM-hMSCs in vasculogenesis.
Formation of
microvascular networks was monitored over time during 6 days of culture in microfluidic system (Figure
4.4). HUVECs and BM-hMSCs were uniformly distributed in fibrin gel at the time of gel filling (12x
cells/ml and 6x
106
106
cells/ml, respectively), and remained mixed at the start of the experiment. RFP-
transfected HUVECs enabled to distinguish between the two cell types throughout the culture and to
monitor the vasculogenesis process. HUVECs connected to each other to form pieces of vessel structures
and gradually formed anastomosis of vessels so that most microvasculature was composed by either one
or two continuous microvascular networks by day 6 of culture.
116
Figure 4.4. Formation of microvascular network by vasculogenesis. HUVECs as well as BM-hMSCs are
uniformly distributed within the gel at the time of gel filling and remain mixed by day I (RFP-HUVECs,
red). HUVECs gradually connect to each other to form a mostly continuous microvascular network by
day 6 of culture. Pictures were captured through an inverted epi-fluorescence microscope (Nikon Eclipse
Ti). Scale bars represent I00[tm.
The effect of mural cell differentiated BM-hMSCs in vasculogenesis was investigated by first
comparing the networks generated with and without BM-hMSCs in 50 ng/ml VEGF supplemented
standard endothelial growth medium. Then, networks formed with BM-hMSCs under VEGF only,
VEGF+Ang-1, and VEGF+TGF-p1 conditions were compared as done in BM-hMSC differentiation
experiments, since each condition gave rise to different degree of differentiation. Clear differences in the
morphology of vascular networks for different conditions were observed (Figure 4.5A-D). HUVEC only
network exhibited the most broad structure with connected and perfusable microvessels, whereas all
networks generated in presence of BM-hMSCs remained limited in expanding their vessel diameter, while
still forming vasculature. Although the same total number of HUVECs was initially seeded in the gel, size
differences in the microvascular networks were quantified by measuring the percent of area that HUVECs
occupied. This value varied from 51.9 ± 1.1% for HUVEC only to 37.1 ± 0.97% for HUVECs with BMhMSCs in VEGF only, and 35.5 t 0.81% and 26.1
117
±
0.72% for VEGF+Ang-l and VEGF+TGF-pl,
respectively (Figure 4.5E). Average vessel diameters were also measured (Figure 4.5F): networks formed
by HUVEC only had an average diameter (84.2 - 2.7[tm) that was more than two folds larger compared
to the one of networks that were co-cultured with BM-hMSCs, regardless of added molecules (40.8 t 1.5
tm VEGF only; 36.2 ± 1.6 [tm VEGF+Ang-1; 21.5 ± 0.68
sm
VEGF+TGF-p1). This is possibly due to
the presence of BM-hMSCs in the gel which restricted the 3D volume that HUVECs could occupy,
therefore limiting vessel size and network area and mimicking a more physiological microvasculature [2,
15]. Both vessel diameter and area covered by the microvascular network were statistically different
comparing
HUVEC
VEGF+TGF-P1
monoculture
and
co-culture
conditions.
Interestingly,
VEGF+Ang-I
and
supplemented systems showed significantly smaller diameters compared to VEGF
devices but the area covered with the addition of VEGF+TGF-P I was statistically lower compared to the
other HUVEC+BM-hMSC conditions.
We further compared networks by quantifying them using different metrics. First, the Fiji
software 2D skeletonize plugin was used to compute the number of network branches. The HUVEC only
condition had 93.8
±
9.4 branches, while HUVEC+BM-hMSC microfluidic devices resulted in nearly a
1.5 fold increase (142.2 ± 5.9) with VEGF, 122.0 ± 4.6 branches with VEGF+Ang-1 and 112.2 ± 9.1
branches with VEGF+TGF-pl (Figure 4.5G). The 3D skeletonize plugin was also applied to investigate
the 3D nature of the microvascular network, resulting in average 7.7% increase of the number of branches
compared to the 2D flat projection method. This difference was due both to the presence of small vessel
protrusions, which were not detected with the 2D plugin, and the increased impact of background noise in
3D imaging, the effect of which was attenuated by applying the 2D protocol. However, the general trend
resulting in a decrease of the number of branches comparing VEGF (152.6 ± 12.2), VEGF+Ang-1 (137.4
± 13.4) and VEGF+TGF-P1 (117.7
±
12.6) condition was confirmed (Figure 4.A4). The length of all
branches was also measured, resulting in an average branch length of 114.3
7.9 Rm for HUVEC only
and lower values for co-culture conditions, with 91.6± 1.8,im for VEGF, 92.5
1.9
and 75.1
±
rn for VEGF+Ang-I
4.8 um for VEGF+TGF-P I (Figure 4. 5H), accrued in a total length of 10.13
118
±
0.39 mm, 12.86
± 0.35 mm, 11.26 ± 0.28 mm, and 8.28 ± 0.60 mm for HUVEC only and co-cultured with BM-hMSC in
VEGF only, VEGF+Ang-1 and VEGF+TGF-p1, respectively (Figure 4.51).
A
BHUVEC+MSC
HUVEC
DHUE+C
HUVEC+MSC
IHVE+S
B
!A
...
...
VEGF
E
--
-i
n.s.
HUVEC
G
I~
HUVEC
j
F
-
HUVEC
.
H --4
120 I
~
HUVEC+MSC
HUVEC
HUVEC+MSC
...
HUVEC+MSC
GF:0'1
VEGF only
VEGF + AngI
===aVEGF + TGF-01
1_Ism
1L
V..L
-
*
*
HUVEC+MSC
.
VEGF+Ang1
...
VEGF
1
t1..1L.
HUVEC
HUVEC+MSC
Figure 4.5. Generation of mature microvascular network in presence of BM-hMSC and different
biomolecules. Initially uniformly dispersed HUVECs form perfusable network by vasculogenesis in
VEGF supplemented standard endothelial growth medium with and without BM-hMSCs or with
VEGF+Ang-1 and BM-hMSCs (A-D). Microvascular networks under various conditions are quantified
E-I). Functionality of microvessels are confirmed by staining with VE-cadherin (J, green) for adheren
junction, laminin (K, green) for matrix secretion, and ZO- 1 for tight-junction (L, green). Cell nuclei were
stained with DAPI (blue). Scale bars represent 200[tm, unless noted.
While the addition of TGF-Pl during the culture enhanced differentiation of BM-hMSCs toward
a mural cell lineage, there seemed no advantage in the generation of a microvascular network. As can be
seen in Figure 4.5D, the TGF-P 1 added system generally resulted in fragmented networks with vessel
119
segments not connected
throughout the
experiment, showing
that the presence
of BM-hMSC
differentiated mural cells does not necessarily lead to the generation of perfusable vasculature.
The addition of VEGF+Ang-1 in co-culture devices promoted the generation of a microvascular
network characterized by total length values comparable to HUVEC monoculture while VEGF
conditioned co-cultures determined even higher total length values. However, the sub-structure of the
network showed more branches and reduced average branch lengths for VEGF+Ang-1 and VEGF only
co-culture conditions, compared to HUVEC only. This seems to be related to the formation of cell
aggregates resembling small islands connected by microvessels with a reduced number of sprouts in
HUVEC only condition, which contribute to the generation of a less organized and less physiological
structure [55].
Interestingly,
VEGF+Ang-1
added
system not only promoted a microvascular network
connecting the lateral media channels, showing the narrowest vessel diameter among the culture
conditions that formed a complete network, but also induced high differentiation of BM-hMSCs into
mural cells, comparable to VEGF+TGF-P1 condition. For these reasons the addition of VEGF+Ang-I
was considered the optimal condition, leading to interconnected microvessels surrounded by pericyte-like
cells (Figure 4.A3). However, this condition alone did not allow perfusion, because while vessel network
have formed inside the fibrin gel, there was no opening into the gel to get to the network from the
channel. Then, EC monolayers were generated within the lateral channels to create anastomosis with the
fibrin gel embedded network, and finally, 10 m fluorescent microbeads were perfused into the system
(Movie S2). Upon encountering an opening of the network in the gel, microbeads were convected from
the media channel into the vessel, travelled through the vascular network and exited from the other side of
the gel into the opposite media channel. These experiments confirmed that even the narrowest network
generated with VEGF+Ang-I was continuous and perfusable. Perfusion of the microvascular network
with 70 kDa dextran (Figure 4.A5) confirmed the presence of lumens and showed a diffusive permeability
of 6.7x10-7 ± 2.74x 10-7cm/s at day 6 after seeding (n=5 within 2 independent devices). Our values are
120
higher compared to in vivo data but lie in the range of previously reported in vitro quantifications [56-58].
This higher permeability could be explained considering our system lacks several physiological factors
characterizing the in vivo environment.
Finally,
the
optimized
VEGF+Ang-1
added
model
was
characterized
through
immunofluorescence assays to demonstrate the presence of a functional microvasculature. Endothelial
adherens and tight junctions were stained with anti-VE-cadherin antibody and anti-ZO-1 antibody
respectively, showing that initially uniformly distributed single cell mixture of HUVECs congregated to
form microvessels in which endothelial cells are tightly adhered (Figure 4. 5J and L and Movie S3).
Furthermore, the functionality of microvessels was confirmed by staining for laminin (Figure 4.5K),
which represents one of the major ECM protein secreted by vasculature [59]. The presence of laminin,
surrounding the entire network, is a clear indication of a functional microvasculature.
4.4 Appendix
Supplementary images are provided showing Live/Dead assays to characterize cell viability
immediately after seeding (Figure 4.AI), SM22cc immunofluorescent staining to characterize BM-hMSC
differentiation toward a mural cell phenotype (Figure 4.A2), confocal reconstruction
of patent
microvessels wrapped by mural cells (Figure 4.A3), 2D-3D skeleton reconstructions of a representative
microvascular network (Figure 4.A4) and fluorescent dextran diffusion within a patent microvessel
(Figure 4.A5). Supplementary videos show microbead perfusion through EC alone (Movie SI) and
EC+BM-hMSC (supplemented with VEGF+Ang-1) (Movie S2) microvascular networks, and the 3D
confocal reconstruction of a VE-cadherin stained microveessel (Movie S3).
121
Figure 4.Al. Live/Dead assay showing cell viability at day 1. Cells were stained with I pl fluorescein
diacetate (FDA, green; Sigma-Aldrich) and 3.5 pl propidium iodide (PI, red; Sigma-Aldrich) diluted in 1
ml phosphate buffered saline (PBS). Samples were incubated for 5 min, washed with PBS and observed
through confocal microscopy.
Figure 4.A2. SM22ct immunofluorescent staining highlighting BM-hMSC differentiation toward a mural
cell lineage. Representative image showing red fluorescent protein (RFP)-transfected human umbilical
vein endothelial cells (HUVECs) organized in a microvessel structure wrapped by differentiated BMhMSCs (SM22cc, green). Cell nuclei were stained with 4'6-Diamidino-2-Phenylindole (DAPI, blue).
122
Figure 4.A3. Confocal microscopy image representing mural cell differentiated BM-hMSCs (a-smooth
muscle actin, green) co-localization with ECs (red). Capillary lumens are indicated by white arrowheads.
A
D
B
1.0
100
50
VEGF
VEGF+ANG1
VEGF.TGFb
Figure 4.A4. Microvascular network analysis: number of branches. The 3D skeletonize plugin of the Fiji
software was applied to compute the number of branches of the longest connected structure within each
2
region of interest (ROI, 533x426 pm ). A25 pm threshold was applied to filter 3D skeleton data (main
text).Representative images ofa confocal 3D reconstruction (A), a2D skeleton obtained with the 2D
skeletonize plugin (B) and a 3D volumetric skeleton (C).3D data for the three different experimental
conditions (addition of VEGF, VEGF+Ang-1 and VEGF+TGF- 1). Average values were obtained fora
minimum of n=8 regions within 2 or 3 independent devicesper condition (D).VEGF: vascular endothelial
growth factor; Ang- 1: angiopoietin- 1; TGF-P 1: transforming growth factor-P.
123
Figure 4.A5. Vessel perfusion with 70 kDa fluorescent dextran revealing patent lumen and absence of
focal leaks. Representative picture of a microvascular network composed by HUVECs and mural cell
differentiated BM-hMSCs treated with VEGF and Ang-1.
124
References
1.
Jeon, J.S., et al., Generation of 3D functional microvascular networks with mural celldifferentiated human mesenchymal stem cells. submitted.
2.
3.
4.
5.
Jain, R.K., Molecular regulationof vessel maturation.Nat Med, 2003. 9(6): p. 685-93.
Dejana, E. and F. Orsenigo, Endothelial adherensjunctions at a glance. J Cell Sci, 2013. 126 Pt
12: p. 2545-9.
Fukuda, M., N. Hiraoka, and J.C. Yeh, C-type lectins and sialyl Lewis X oligosaccharides.
Versatile roles in cell-cell interaction.J Cell Biol, 1999. 147(3): p. 467-70.
Gout, S., P.L. Tremblay, and J. Huot, Selectins and selectin ligands in extravasation of cancer
cells and organ selectivity of metastasis. Clin Exp Metastasis, 2008. 25(4): p. 335-44.
A.J.,
et
al.,
Microvascular repair: post-angiogenesis vascular
dynamics.
6.
LeBlanc,
7.
Yancopoulos, G.D., et al., Vascular-specific growth factors and blood vesselformation. Nature,
Microcirculation, 2012. 19(8): p. 676-95.
8.
9.
10.
11.
2000. 407(6801): p. 242-8.
Carmeliet, P., Mechanisms of angiogenesisand arteriogenesis.Nat Med, 2000. 6(4): p. 389-95.
Hellstrom, M., et al., Lack ofpericytes leads to endothelial hvperplasia and abnormal vascular
morphogenesis. J Cell Biol, 2001. 153(3): p. 543-53.
Kluk, M.J. and T. Hla, Signaling of sphingosine-1-phosphate via the SIP/EDG-family of Gprotein-coupled receptors. Biochim Biophys Acta, 2002. 1582(1-3): p. 72-80.
Thurston, G., et al., Leakage-resistant blood vessels in mice transgenically overexpressing
angiopoietin-1. Science, 1999. 286(5449): p. 2511-4.
12.
Chambers, R.C., et al., Global expression profiling of fibroblast responses to transforming
growth factor-beta] reveals the induction of inhibitor of di/ferentiation-I and provides evidence
of smooth muscle cell phenotypic switching. Am J Pathol, 2003. 162(2): p. 533-46.
13.
14.
Gohongi, T., et al., Tumor-host interactions in the gallbladdersuppress distal angiogenesis and
tumor growth: involvement of'transforminggrowth fbctor beta]. Nat Med, 1999. 5(10): p. 1203-8.
Pepper, M.S., Transfbrming growth factor-beta: vasculogenesis, angiogenesis, and vessel wall
integrity. Cytokine Growth Factor Rev, 1997. 8(1): p. 21-43.
15.
Au, P., et al., Bone marrow-derivedmesenchymal stem cells frcilitate engineeringof long-lasting
functional vasculature. Blood, 2008. 111(9): p. 4551-8.
16.
Koike, N., et al., Tissue engineering: creation of long-lasting blood vessels. Nature, 2004.
428(6979): p. 138-9.
17.
Goerke, S.M., et al., Human endothelialprogenitor cells induce extracellular signal-regulated
kinase-dependent differentiation of mesenchymal stem cells into smooth muscle cells upon
cocultivation. Tissue Eng Part A, 2012. 18(23-24): p. 2395-405.
18.
Guo, X., et al., A novel in vitro model system frr smooth muscle differentiation from human
embryonic stem cell-derived mesenchymal cells. Am J Physiol Cell Physiol, 2013. 304(4): p.
C289-98.
19.
20.
21.
22.
Gavard, J. and J.S. Gutkind, VEGF controls endothelial-cellpermeability by promoting the beta-
arrestin-dependentendocytosis of VE-cadherin. Nat Cell Biol, 2006. 8(11): p. 1223-34.
Derda, R., et al., Paper-supported3D cell culture/fbr tissue-basedbioassays. Proc Natl Acad Sci
U S A, 2009. 106(44): p. 18457-62.
Even-Ram, S. and K.M. Yamada, Cell migration in 3D matrix. Curr Opin Cell Biol, 2005. 17(5):
p. 524-32.
Griffith, L.G. and M.A. Swartz, Capturing complex 3D tissue physiology in vitro. Nat Rev Mol
Cell Biol, 2006. 7(3): p. 211-24.
125
23.
24.
Lee, J., M.J. Cuddihy, and N.A. Kotov, Three-dimensional cell culture matrices: state of the art.
Tissue Eng Part B Rev, 2008. 14(1): p. 61-86.
Yamada, K.M. and E. Cukierman, Modeling tissue morphogenesis and cancer in 3D. Cell, 2007.
130(4): p. 601-10.
25.
27.
Shin, Y., et al., In vitro 3D collective sprouting angiogenesis under orchestratedANG-1 and
VEGF gradients. Lab Chip, 2011. 11(13): p. 2175-81.
Grainger, S.J. and A.J. Putnam, Assessing the permeability of engineeredcapillary networks in a
3D culture. PLoS One, 2011. 6(7): p. e22086.
Zheng, Y., et al., In vitro microvessels for the study of angiogenesis and thrombosis. Proc Natl
28.
Acad Sci U S A, 2012. 109(24): p. 9342-7.
Chrobak, K.M., D.R. Potter, and J. Tien, Formation ofperfused,functional microvasculartubes
26.
29.
30.
31.
32.
33.
34.
35.
36.
in vitro. Microvasc Res, 2006. 71(3): p. 185-96.
Golden, A.P. and J. Tien, Fabrication of microfluidic hydrogels using molded gelatin as a
sacrificialelement. Lab Chip, 2007. 7(6): p. 720-5.
Hsu, Y.H., et al., Full rangephysiologicalmass transportcontrol in 3D tissue cultures. Lab Chip,
2013. 13(1): p. 81-9.
Song, J.W., D. Bazou, and L.L. Munn, Anastomosis of endothelial sproutsfbrms new vessels in a
tissue analogue of angiogenesis. Integr Biol (Camb), 2012. 4(8): p. 857-62.
Yeon, J.H., et al., In vitro formation and characterization of a perfusable three-dimensional
tubular capillarynetwork in microfluidic devices. Lab Chip, 2012. 12(16): p. 28 15-22.
Jeong, G.S., et al., Sprouting angiogenesis under a chemical gradient regulated by interactions
with an endothelialmonolayer in a microfluidicplatform. Anal Chem, 2011. 83(22): p. 8454-9.
Zheng, C., et al., Quantitativestudy of the dynamic tumor-endothelialcell interactionsthrough an
integratedmicrofluidic coculture system. Anal Chem, 2012. 84(4): p. 2088-93.
Bischel, L.L., et al., Tubeless microfluidic angiogenesis assay with three-dimensional
endothelial-linedmicrovessels. Biomaterials, 2013. 34(5): p. 1471-7.
Stratman, A.N., et al., Endothelial-derived PDGF-BB and HB-EGF coordinately regulate
pericyte recruitmentduring vasculogenic tube assembly and stabilization. Blood, 2010. 116(22):
p. 4720-30.
37.
38.
39.
40.
41.
42.
43.
44.
45.
Stratman, A.N., et al., Pericyte recruitment during vasculogenic tube assembly stimulates
endothelial basement membrane matrixformation. Blood, 2009. 114(24): p. 5091-101.
Chen, F., et al., Combination of VEGF(165)/Angiopoietin-1 gene and endothelialprogenitorcells
for therapeutic neovascularization.Eur J Pharmacol, 2007. 568(1-3): p. 222-30.
Saif, J., et al., Combination of injectable multiple growth factor-releasingscaffolds and cell
therapy as an advancedmodality to enhance tissue neovascularization.Arterioscler Thromb Vasc
Biol, 2010. 30(10): p. 1897-904.
Zeng, H., L. Li, and J.X. Chen, Overexpression of angiopoietin-] increases CD133+/c-kit+cells
and reduces myocardial apoptosis in db/db mouse infarcted hearts. PLoS One, 2012. 7(4): p.
e35905.
Lee, W.Y., et al., Core-shell cell bodies composed of human cbMSCs and HUVECsfor functional
vasculogenesis. Biomaterials, 2011. 32(33): p. 8446-55.
Kim, D. and C.L. Haynes, On-Chip Evaluation of Neutrophil Activation and NeutrophilEndothelialcell InteractionduringNeutrophil Chemotaxis. Anal Chem, 2013.
Estrada, R., et al., Endothelial cell culture model for replication of physiological profiles of
pressure,flow, stretch, and shear stress in vitro. Anal Chem, 2011. 83(8): p. 3170-7.
Song, J.W., et al., Computer-controlled microcirculatory support system for endothelial cell
culture and shearing.Anal Chem, 2005. 77(13): p. 3993-9.
Chung, S., et al., Microfluidic platformsfor studies of angiogenesis, cell migration, and cell-cell
interactions. Sixth InternationalBio-Fluid Mechanics Symposium and Workshop March 28-30,
2008 Pasadena,Califbrnia.Ann Biomed Eng, 2010. 38(3): p. 1164-77.
126
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
Shin, Y., et al., Microfluidic assayfor simultaneous culture of multiple cell types on surfaces or
within hydrogels. Nat Protoc, 2012. 7(7): p. 1247-59.
Lopa, S., et al., Orthopedic bioactive implants: Hydrogel enrichment of macroporoustitaniumfor
the delivery of mesenchymal stem cells and strontium. J Biomed Mater Res A, 2013.
Nilufar, S., et al., FiloDetect: automatic detection of filopodia from fluorescence microscopy
images. BMC Syst Biol, 2013. 7: p. 66.
Curry, F.E., V.H. Huxley, and R.H. Adamson, Permeabilityofsingle capillariesto intermediatesized colored solutes. Am J Physiol, 1983. 245(3): p. H495-505.
Ball, S.G., A.C. Shuttleworth, and C.M. Kielty, Direct cell contact influences bone marrow
mesenchymal stem cellfate. Int J Biochem Cell Biol, 2004. 36(4): p. 714-27.
Kobayashi, N., et al., Mechanicalstress promotes the expression of smooth muscle-like properties
in marrow stromal cells. Exp Hematol, 2004. 32(12): p. 1238-45.
Narita, Y., et al., Effects of transforming growth fictor-beta 1 and ascorbic acid on
differentiation of human bone-marrow-derivedmesenchymal stem cells into smooth muscle cell
lineage. Cell Tissue Res, 2008. 333(3): p. 449-59.
Jeon, E.S., et al., Sphingosylphosphorvlcholine induces differentiation of human mesenchymal
stem cells into smooth-muscle-like cells through a TGF-beta-dependent mechanism. J Cell Sci,
2006. 119(Pt 23): p. 4994-5005.
Hirschi, K.K., S.A. Rohovsky, and P.A. D'Amore, PDGF, TGF-beta, and heterotypic cell-cell
interactionsmediate endothelialcell-induced recruitment of I0T]/2 cells and their difftrentiation
to a smooth musclefrite. J Cell Biol, 1998. 141(3): p. 805-14.
McDonald, D.M. and P.L. Choyke, Imaging of angiogenesis:from microscope to clinic. Nat Med,
2003. 9(6): p. 713-25.
Albelda, S.M., et al., Permeabilitycharacteristicsof cultured endothelial cell monolayers. J Appl
Physiol, 1988. 64(1): p. 308-22.
Michel, C.C. and F.E. Curry, Microvascularpermeability.Physiol Rev, 1999. 79(3): p. 703-61.
Zervantonakis, I.K., et al., Three-dimensional microfluidic model Jbr tumor cell intravasationand
endothelial barrierfunction. Proc Natl Acad Sci U S A, 2012. 109(34): p. 13515-20.
Frantz, C., K.M. Stewart, and V.M. Weaver, The extracellular matrix at a glance. J Cell Sci,
2010. 123(Pt 24): p. 4195-200.
127
Chapter 5
Extravasation of cancer cell to bone-mimicking
microenvironment in functional 3D vasculature
generated through vasculogenesis
5.1 Introduction
Extravasation is one of the key steps in the metastatic cascade leading to the generation of cancer
cell microcolonies and potentially, secondary tumors [1, 2]. Although it is well known that cross-talk
between specific cancer cell types and receptive microenvironments can influence the dissemination of
primary tumors [3], no previously developed in vitro model has demonstrated such interactions in a
complex, multicellular, 3D microenvironment. Moreover, despite the invaluable role of in vivo models,
they tend not allow one to fully analyze and quantify specific cell-cell and cell-matrix interactions that are
essential for local extravasation. Indeed, the power of organ-specific in vitro cancer models resides in
their potential for clarifying the complex mutual interactions between the variety of cell populations
involved to discover highly focused and more effective therapies.
The value of an in vitro cancer metastasis model could be further enhanced by the ability to create
a physiologically relevant, functional and perfusable microvasculature. The functionality of vascular
systems relies on their ability to recruit mural cells, which provide structural support to the microvessel
128
walls and interact with endothelial cells through biochemical signals [4, 5]. Particularly, modeling of
microcirculation in 3D has tremendous implications not only in studying cancer extravasation [6], but
also in studying complex biological phenomena such as cancer cell intravasation [7] or neutrophil
migration [8] under in vivo-like flow conditions.
This chapter describes a study of cancer cell extravasation in functional microvascular networks
generated through vasculogenesis in a bone-mimicking microenvironment using a microfluidic system.
Extravasation rates are compared for the osteo-cell containing condition with endothelial cell only
condition in a static culture as well as in the condition where shear stress is imposed to the vasculature.
Characterization of the vasculature is achieved by measuring the permeability of the endothelium at each
condition.
5.2 Materials and Methods
5.2.1 Microfluidic system
The microfluidic system contains a central hydrogel region flanked by two lateral media
channels, as previously used in our group for other studies [9]. The fabrication process of the device has
also been documented in detail [10]. Briefly, the microfluidic device was fabricated with PDMS (polydimethyl-siloxane; Silgard 184, Dow-Chemical) using soft lithography techniques from patterned SU-8
silicon wafers. A 100 ptm cover glass is bonded to the PDMS with oxygen plasma treatment to create the
channel. The hydrogel region is filled with cell suspension containing fibrin gel, obtained through
addition of thrombin solution, a mixture of thrombin (100 U/ml) with cell culture medium in 1:25
dilution, to fibrinogen solution (5.0 mg/ml). The two channel system enables easy access to the hydrogel
for the addition of cancer cell for extravasation, or for inducing of flow within the gel.
129
5.2.2. Cell culture and cell selection
Cells of passage 6 or lower BM-hMSCs, harvested from patients undergoing hip arthroplasty,
were cultured in standard alpha-minimum essential medium (aMEM; Invitrogen) with non-essential
amino acids, sodium pyruvate and L-glutamine, 10% fetal bovine serum (FBS; Invitrogen), biological
buffer and antibiotics. BM-hMSCs
were differentiated to osteo lineage by culturing in osteo-
differentiation medium for two weeks. Red fluorescent protein (RFP)-transfected human umbilical vein
endothelial cells (HUVECs) were commercially obtained (Angio-Proteomie) and cultured in endothelial
growth medium with full supplements (EGM-2MV bullet kit; Lonza). HUVECs at passage 6 were
suspended at 2x 107 cells/ml in EMG2 + thrombin and combined with osteo-differentiated and nondifferentiated BM-hMSCs suspension mixed at 9:1 ratio (4x 10 cells/ml in BM-hMSC growth medium +
thrombin). The mixture is again mixed with fibrinogen solution at 1:1 ratio for few seconds, and inserted
into the gel channel to complete the seeding. The fibrin gel is polymerized within 15 min in humidity box
at room temperature. The devices are hydrated by filling the lateral channels with EGM2 supplemented
with 50 ng/ml VEGF (Peprotech). After day2, the culture medium was replaced
supplemented with 50 ng/ml VEGF and 100 ng/ml Ang-l
with EGM2
(Peprotech). Control experiments were
performed seeding HUVECs without BM-hMSCs at the same cell density applied in co-culture assays. A
RFP-expressing BOKL cell line, which is MDA-MB-231 cell line specific to bone metastasis enabled
live-cell imaging via fluorescent microscopy. Cancer cell lines were cultured in standard DMEM media
(Sigma) with 10% fetal bovine serum (Invitrogen) and antibiotics. The generation of vessel network
through
vasculogenesis
required
minimum three
days of culture
in EGM
supplemented
with
VEGF+ANGI, and cancer cells were introduced four days after seeding of endothelial cells. For cancer
cell seeding 100 tl of 400,000 cells/ml cell suspension medium was added to one reservoir, and left for
one hour for adhesion. Then, EGM+VEGF+ANG I medium was added to all reservoirs including the one
that was used for tumor cell insertion. The medium in the device was replaced every 24 hours, and all
cultures were kept in a humidified incubator at 37*C and 5% CO 2 .
130
5.2.3. Immunofluorescence and image acquisition
All devices were washed with phosphate buffered saline (PBS; Invitrogen), fixed with 4%
paraformaldehyde (PFA) for 15 min, and perneabiliized with 0.1% Triton-X 100 solution for 5 min, all
done at room temperature. The samples are treated with 5% bovine serum albumin (BSA) + 3% goat
serum solution for at least 3h at 4'C before the incubation with primary antibody. Mouse polyclonal
alpha-smooth muscle actin (a-SMA) antibody (abcam, dilution 1:100), rabbit polyclonal vascular
endothelial-cadherin (VE-cadherin) antibody (abcam, dilution 1:100), and rabbit polyclonal osteo calcin
(OCN) antibody (BTI, dilution 1:50) are used for staining. Red fluorescently labeled secondary antibodies
(Invitrogen) were used at 1:200 dilution. Cell nuclei were stained with 4'6-Diamidino-2-Phenylindole
(DAPI;5 mg/ml; Invitrogen) at 1:500 dilution, and F-actin filaments were stained with AlexaFluor 633
phalloidin (Invitrogen) at 1:100 dilution. All the images were captured using a confocal microscope
(Olympus IX8 1) and processed with Imaris software (Bitplane Scientific Software), unless specified.
5.2.4. Metrics for extravasation
Devices were monitored and recorded live after the addition of tumor cell suspension into the
system. Using the live imaging data, each tumor cell that is seen in the vessel as identified by the RFP
signal of the tumor cell, is followed to check whether the cell has indeed go through extravasation process
by the end of the imaging (8 hours). Confocal data were analyzed using IMARIS. The percentage of cells
that had extravasated was determined for each region of interest (ROI) imaged and the percentages were
averaged for a final average value reported for each condition. The dimensions of the ROI were 1405 [tm
x 1124 ,m x 200 [tm (height) and a minimum of four to maximum of six ROls were imaged for each
microfluidic device.
131
5.2.5. Permeability
Permeability of the vasculature was measured as described previously [9]. Briefly, 40ptl of
fluorescent dextran (70kDa, red, Invitrogen) in endothelial growth medium (25 pg/ml) was added to the
reservoirs where all medium is aspirated. The average fluorescence intensities at the initial and final time
points were measured by spatially averaging the intensity along side of the intact vessel as that shown by
the flow of the dextran medium internally. Then, the permeability value can be calculated with the
following formula with assumption that the vessels are of circular cross section [11]:
PD
)
Ii
1
Ii - Ib
At4
d
x4
where Ih I, and If is the background, initial, and final average intensities, At is the time interval between
images and d is the diameter of the vessel imaged.
5.2.6. Application of shear stress in vasculature
Flow was produced in the vasculature by withdrawing medium from one channel at a rate of 2
RI/min using a syringe pump. Medium was supplemented from a reservoir connected to the opposite
channel, enforcing the flow through the vascular network. While the syringe pump was withdrawing the
medium at 2 RI/min, a rough estimate of the flow velocity in the vasculature was obtained by 3
um
microspheres to the perfusion medium and measuring the distances travelled between frames and
multiplying by the frame rate. The measured values of velocity averaged to estimate the average velocity
of medium flowing across the vasculature. Then, shear stress applied on to the vasculature was calculated
assuming Hagen-Poiseuille flow in cylindrical pipe [12]:
8pv
D
where
T
is shear stress, [t is viscosity of water, D is averaged diameter of the vessel, and v is the average
velocity of medium flowing across the vasculature.
The flow was maintained for 14 h prior to addition of the cancer cell suspension for conditioning,
132
and again re-applied one hour after adding cancer cells and maintained for 8 h during the live imaging for
extravasation.
5.2.7. Statistics
All extravasation percentages are reported as averages and standard errors of measurements from
a minimum of 12 ROIs from 3 or more independent devices while all permeability values are averages of
5 (min) to 7 (max) measurement from 2 (min) to 4 (max) independent devices. Measurements were
compared using unpaired Student's t-test. All tests with p < 0.05 were assumed statistically significant,
and SigmaPlot v.12 was used for all tests.
5.3 Results and Discussion
5.3.1 Generation of functional 3D vasculature in bone-mimicking microenvironment
Formation of microvascular networks by vasculogenesis
in fibrin gel has been reported
previously [9, 13]. In this study, we created a functional microvascular network in a bone-mimicking
microenvironment with the addition of osteo-differentiated and non-differentiated hBM-MSCs combined.
We first confirmed the formation of vascular junctions with immunofluorescent staining of VE-cadherin
on the endothelium. (Figure 5.2) The presence of the additional cell types did not hinder HUVECs from
forming a tubular network as seen in Figure 5.2. Immunofluorescent imaging of Q-smooth muscle actin in
the system confirmed the presence of mural cells differentiated from hBM-MSCs wrapped around the
generated vascular network (Figure 5.3). Visual confirmation of flow of fluorescently labeled dextran and
3 tm microspheres through the vessels confirmed that the vascular network generated in this system with
presence of osteo-differentiated
cells was indeed perfusable.
Finally, the osteo-cell
conditioned
microenvironment was confirmed by staining for osteocalcin (OCN), which is a protein secreted by
osteoblasts. (Figure 5.4). Thus, the network generated can be viewed as a physiologically relevant
vascular model with mural cells within a bone-mimicking microenvironment, and could be utilized for
133
studying biological phenomena or screening for therapeutics.
Figure 5.1 VE-cadherin staining for vasculature. VE-cadherin (red), nucleus (DAPI, blue)
Figure 5.2 a-smooth muscle actin staining for mural cell. Mural-differentiated cell, marked with asmooth muscle actin (red), wraps around the micro-vessel formed (green). Nucleus (DAPI, blue)
134
Figure 5.3 Staining for osteocalcin (OCN). Osteo-differentiated hBM-MSCs are cultured with HUVECs
(green) and osteo-cells secrete bone specific protein, OCN. (OCN, red; nucleus, DAPI, blue).
5.3.2 Extravasation of cancer cells in bone-mimicking microenvironment
The perfusable vasculature generated in the microfluidic device by vasculogenesis was used to
model the microcirculatory system during extravasation. GFP-labeled HUVECs and RFP-labeled BOKL
cancer cells enabled clear visualization of the vasculature and the movement of cancer cells when the
devices were monitored with live imaging after addition of the cancer cells (Figure 5.4).
100 Jm
r7:0
0 hr3hr6
Figure 5.4 Live imaging of cancer cell extravasation in the generated microvascular network. Cancer
cells (red) are initially seeded in the vasculature (green), adhere on the endothelium, and move out into
the fibrin gel, which in this system models the extracellular matrix.
135
r
The percent of cancer cell extravasation in a device containing microvascular network seeded
with osteo-differentiated hBM-MSCs was 3.8 fold higher (56.5 t 4.8 %) than the control case for which
the vascular network was generated with HUVECs alone (14.7 t 3.7 %) (Figure 5.6). Permeability values
of the vasculature with and without osteo-differentiatied hBM-MSCs were analyzed using the
fluorescence intensity of 70 kDa dextran perfusing through the vessels over time. The vasculature in the
bone-mimicking microenvironment yielded in higher permeability (4.12 ± 0.75)- 10-6 cm/s compared to
the HUVEC only condition (0.89
±
0.31)- 10-6 cm/s. Despite the addition of hBM-MSCs, which should
lead to more mature and less permeable vessel, osteo-differentiated hBM-MSCs apparently caused the
vessels to be leakier. While the increase in permeability may due to combination of factors, the higher
permeability of the vasculature in osteo-cell conditioned environment may also be one of the factors
contributing to the significant increase of extravasation in this system. However, there was no obvious
morphological difference in the vascular junctions observed by VE-cadherin staining (Figure 5.2) in spite
of the higher permeability values.
-o
60
20
0
HUVEC only
osteo-cell
Figure 5.5 Percent of extravasation in bone-mimicking microenvironment. The osteo-differentiated cell
added system resulted in higher extravasation of cancer cells compared to HUVEC only condition. (p <
0.001)
136
4-
HUVEC only
osteo-cell
Figure 5.6 Permeability of the vessel network. The osteo-differentiated cell added system resulted in
leakier vessels compared to HUVEC only condition. (p < 0.01)
5.3.3. Effect of shear stress on vasculature and cancer cell extravasation
The application of flow in the vessels formed by withdrawing the medium at 2ul/min results in an
average shear stress of 0.5 dynes/cm 2 . Extravasation of cancer cells, which were added 12 hours after the
application of the flow, in the bone-mimicking microenvironment occurred at 38.6 t 4.8 % in the system
with flow, while the static condition resulted in a 56.5
4.8 % extravasation rate.
go.
60
020
flow
static
Figure 5.7 Percent of extravasation for static and flow conditions in bone-mimicking microenvironment.
The static condition resulted in a higher extravasation rate than the system with flow. (p < 0.05)
137
6.
4
T
2
0.-
static
flow
Figure 5.8 Permeability of the vessel network for static and flow condition in bone-mimicking
microenvironment. Application of shear stress reduced the permeability of the vessels. (p < 0.05)
AB
Figure 5.9 Elongation of endothelial cells during application of shear stress. Endothelial cells (green) that
are exposed to shear stress for total 22 h are elongated along the direction of shear (A) compared to the
static condition (B). Actin (red), nucleus (DAPI, blue)
Permeability of the perfusable vasculature in the bone-like environment showed a 2.4 fold
decrease for a vasculature exposed under shear stress (from (4.12 ± 0.75)-10~6 cm/s to (1.72 - 0.53)-10-6
cm/s). From images with actin staining, it was observed that the flow condition caused elongation of the
138
cells compared to the static condition (Figure 5.9). Overall, exposure of shear stress on endothelium
impose morphological change and tightens the vessel as seen by actin staining and permeability
measurement. This tightening of endothelium due to shear is in competitive reaction with the effects due
to the addition of osteo-differentiated hBM-MSCs for change in permeability of the vessel, and dampens
the cancer cell extravasation to the bone-mimicking microenvironment.
139
References
I.
2.
3.
4.
5.
Valastyan, S. and R.A. Weinberg, Tumor metastasis: molecular insights and evolving paradigms.
Cell, 2011. 147(2): p. 275-92.
Chambers, A.F., A.C. Groom, and I.C. MacDonald, Disseminationand growth of cancer cells in
metastatic sites. Nat Rev Cancer, 2002. 2(8): p. 563-72.
Paget, S., The distribution of secondary growths in cancer of the breast. 1889. Cancer Metastasis
Rev, 1989. 8(2): p. 98-101.
Jain, R.K., Molecular regulationof vessel maturation.Nat Med, 2003. 9(6): p. 685-93.
LeBlanc, A.J., et al., Microvascular repair: post-angiogenesis vascular dynamics.
Microcirculation, 2012. 19(8): p. 676-95.
6.
7.
8.
9.
10.
11.
12.
13.
Jeon, J.S., et al., In vitro model of tumor cell extravasation. PLoS One, 2013. 8(2): p. e56910.
Zervantonakis, 1.K., et al., Three-dimensionalmicrofluidic model for tumor cell intravasationand
endothelial barrierfunction.Proc Natl Acad Sci U S A, 2012. 109(34): p. 13515-20.
Kim, D. and C.L. Haynes, On-Chip Evaluation of Neutrophil Activation and NeutrophilEndothelialcell Interaction duringNeutrophil Chemotaxis. Anal Chem, 2013.
Chen, M.B., et al., Mechanisms of tumor cell extravasation in an in vitro microvascular network
platform. Integr Biol (Camb), 2013. 5(10): p. 1262-71.
Shin, Y., et al., Microfluidic assayfor simultaneous culture of multiple cell types on surfaces or
within hydrogels. Nat Protoc, 2012. 7(7): p. 1247-59.
Curry, F.E., V.H. Huxley, and R.H. Adamson, Permeabilityof single capillariesto intermediatesized colored solutes. Am J Physiol, 1983. 245(3): p. H495-505.
White, F.M., Fluid Mechanics. 7 ed20 11: McGraw-Hill Higher Education.
Kim, S., et al., Engineering offinctional, perfusable 3D microvascularnetworks on a chip. Lab
on a Chip, 2013. 13(8): p. 1489-1500.
140
Chapter 6
Conclusion and Future Outlook
Tumor cells that disseminate from the primary tumor and intravasate into the circulatory system
are transported throughout the body. By adhesion to the endothelial wall or becoming stuck by plugging
a small capillary, the cells that survive can transmigrate across the endothelial barrier, thus providing a
potential nucleating site for metastasis. This thesis describes an in vitro model for which one could use to
investigate one crucial step of cancer metastasis: extravasation.
In chapter 2, the microfluidic platform was applied to study the extravasation of a breast cancer
cell line (MDA-MB-23 1) and their subsequent proliferation in collagen gel, which mimics the 3D nature
of the extracellular space. Using this assay, we have cultured and sustained an endothelial monolayer
spanning the entire surface of a microchannel and hydrogel surface, and introduced tumor cells to observe
extravasation. We also quantified the permeability of the endothelial monolayer and showed that
endothelial barrier integrity is compromised by the tumor cells. The average number of tumor cells in
ROIs increased between day 1 and day 3 after tumor cell seeding while the percentage of ROIs with
extravasated cells did not change significantly. These results suggest that extravasation in our system
occurs predominantly within the first 24 hours of tumor cell introduction and that proliferation can
continue both prior to and after extravasation.
141
Chapter 3 describes an advanced human organ-specific microfluidic 3D in vitro model to analyze
the
extravasation
of
highly
metastatic
breast
cancer
microenvironment, generated from bone marrow-derived
cells
into
an
osteo-cell
conditioned
hBM-MSCs. We have provided unique
quantitative results concerning the interplay between a specific "seed and soil couple" by measurng
extravasation rate and extravasated distance of breast cancer cells in the presence of an attractive matrix,
finding that both increased in the presence of the osteogenic microenvironment. Moreover, we have
shown how the molecular pathway involving the breast cancer cell surface receptor CXCR2 and bonesecreted chemokine CXCL5 plays a pivotal role in the extravasation process of breast cancer cells.
Finally, we demonstrated that extravasated cancer cells can proliferate and generate micrometastases
within the osteo-cell conditioned microenvironment.
In Chapter 4, we developed 3D functional, perfusable microvascular networks composed of
human ECs and pericyte-like cells and produced by a process of vasculogenesis. We investigated the role
of factors known to influence vascular network growth, i.e. Ang-1 and TGF-Pl, on BM-hMSC
differentiation toward a mural cell lineage, and showed that addition of these factors along with co-culture
with ECs enhances differentiation. Despite significant results in BM-hMSC differentiation, we found the
addition of TGF-pl does not allow the generation of microvascular networks. On the other hand, Ang-1
supplemented systems formed interconnected and perfusable microvessels, surrounded by mural cells
differentiated from BM-hMSCs and laminin rich ECM.
In chapter 5, the microvasculature generated by vasculogenesis as developed in chapter 4 is
combined with osteo-differentiated cells as in chapter 3 to create more physiologically relevant
vasculature in a bone-mimicking microenvironment. Using the live imaging capabilities, we observed and
quantified the cancer cells flow into the vasculature, adhere, and extravasate into the extracellular space.
The bone-mimicking microenvironment induced greater extravasation rate than in the vasculature
generated by HUVEC alone. Flow was also been added to the bone-mimicking system to better mimic the
physiological condition where the vasculature is exposed to shear stress. Application of shear stress
142
reduced the permeability of vessel and also the cancer cell extravasation compared to the static condition
of hone-mimicking microenvironment.
Utilizing the platforms mentioned above, additional targeted studies on cancer cell extravasation
could be performed, such as addition of immune cell
in the hydrogel to better mimic the
pathophysiological vasculature conditions. Addition of other hematopoetic cells such as platelets along
with tumor cell suspension for modeling extravasation process could also enlighten further the complex
interactions of circulating tumor cells in blood stream.
Instead of using HUVEC cell line for modeling the vasculature, one could generate microvascular
network with endothelial cells derived from induced pluripotent stem cells (iPS cells). Moreover, the
same iPS cell lineage could be differentiated also to a particular organ cell type to model the
microenvironment of a specific organ surrounding the vasculature. The usage of iPS cells could bring a
step closer in truly enabling in vitro systems as described here as a platform for developing anti-cancer
treatments for personalized medicine.
Furthermore, we could extend the organ specific extravasation model to not only mimic the bone
microenvironment, but also many other organ sites that have shown to be the most and/or least
susceptible to metastasis. Using a high-throughput microfluidic system as shown in Figure 6.1, we could
potentially investigate extravasation of cancer cells to multiple organ sites with parametric control of
conditions in a single platform. The single device culture allows systematic control of multiple regions
containing different organ components, and thus, could potentially better elucidate the key rate-limiting
factors for specific organ metastasis.
143
'00
to too
000
Figure 6.1 High-throughput device for multi-organ mimicking system.
In spite of limitations that microfluidics possesses in replicating true in vivo conditions, the
system presented here enables a tightly-regulated and well-visualized study of cancer cell extravasation.
Moreover, this study represents the first organ-specific microfluidic 3D in vitro model developed to study
extravasation and could pave the way to the generation of increasingly detailed assays better able to
replicate the complex in vivo microenvironment. The microfluidic approach as shown here can be also
used to develop advanced in vitro models where the interactions between a functional vasculature and
tissue parenchyma is critical to mimic pathophysiological processes and test the effects of therapeutics in
complex microenvironments.
Significant steps forward have been performed in the last years in the treatment of cancer, but the
development of effective anti-metastatic therapies still remains an issue. Traditional in vitro models do
not allow parametric studies on cell-cell and cell-matrix interactions in complex, spatio-temporal tunable
environments. Microfluidics can contribute to setting up advanced in vitro cancer models, overcoming
144
limitations of traditional methods in cancer modeling and anti-cancer drug screening. Organ-specific
microfluidic models are the leading edge of current in vitro research with possibility of multi organspecific microfluidic models, and our hope is that they can contribute to expand our knowledge on cancer
biology, provide useful data to be subsequently tested through animal models and pre-clinical trials, and
improving our quest for more specific and effective anti-cancer treatments.
145