⟨ ⟩ Clinical Research
advertisement

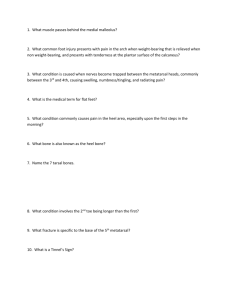
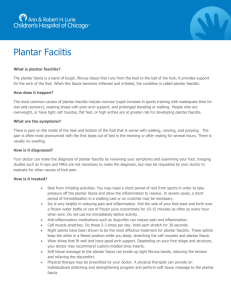
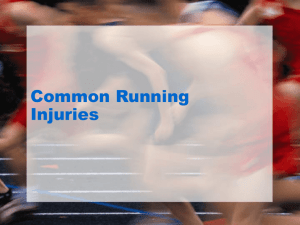
86 April 2011 Foot & Ankle Specialist ⟨ Clinical Research ⟩ Low-Dye Taping Versus Medial Arch Support in Managing Pain and PainRelated Disability in Patients With Plantar Fasciitis Abstract: Plantar fasciitis is thought to develop because of repeated mechanical stresses. This study aimed to compare 2 means of foot arches support—lowDye tape (LDT) and medial arch support (MAS)—in patients with plantar fasciitis. Thirty patients with unilateral plan­ tar fasciitis (23 men and 7 women) were randomly assigned to the LDT or MAS groups. Both groups were assessed before and after experiment for pain and foot function. Both groups received 9 sessions over 3 weeks consisting of ultra­ sound and calf muscles stretching. They were instructed to maintain support­ive intervention (LDT or MAS) through­out this period. Pre–post comparison showed reduced pain and improved function in both groups. Between-groups analy­ sis showed non-significant difference in pre-VAS and pre-FPDS. Post-VAS and post-FPDS showed signif­icant improvement in patients in MAS group. Results indicate that MAS is more convenient for short-term management of pain and disability in patients with plantar fasciitis than LDT. Level of Evidence: Therapeutic, Level II Keywords: low-Dye taping; medial arch support; plantar fasciitis; foot pain P Mohammed Shawki Abd El Salam, PhD, and Yehia Nassef Abd ELhafz, PhD condition can have a dramatic impact on physical mobility.4 Although poorly understood, the development of plantar fasciitis is thought to have a mechanical origin, since the plantar fascia acts as a stabilizer of the lantar fasciitis is considered the most common Although poorly understood, the cause of foot pain. It is a common disorder in development of plantar fasciitis is thought both athletic and sedentary populations.1,2 to have a mechanical origin, since the Buchbinder3 reported that plantar fasciitis is plantar fascia acts as a stabilizer of the a clinical diagnosis that is most commonly seen longitudinal arch, which is very important in in younger runners and the propulsive phase of gait.” patients aged between 40 and 60 years. The disorder is thought to be multifactorial in origin with longitudinal arch, which is very imporseveral predisposing factors, such as obe- tant in the propulsive phase of gait as it serves to make the foot a rigid lever sity, excessive periods of weight-bearing activity, and decreased ankle range of via the “windlass effect” mechanism.5 Particularly important mechanical facmotion, suggested to be involved.3 Pain tors that contribute to the development of and discomfort associated with this “ DOI: 10.1177/1938640010387416. From the Faculty of Physical Therapy, Cairo University, Giza, Egypt (MSAS, YNAE); College of Applied Medical Sciences, University of Dammam, Dammam, Saudi Arabia (MSAS); College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia (YNAE). Address correspondence to Mohammed Shawki Abd El Salam, PhD, Department of Physical Therapy, College of Applied Medical Sciences, University of Dammam, Dammam, Kingdom of Saudi Arabia; e-mail: attmanonly@hotmail.com. For reprints and permissions queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav. Copyright © 2011 The Author(s) Downloaded from fas.sagepub.com at UNIV OF DELAWARE LIB on February 10, 2015 vol. 4 / no. 2 Foot & Ankle Specialist plantar fasciitis are pes planus foot type and other lower-limb biomechanical factors that result in a lowered medial longitudinal arch, which are thought to create excessive tensile strain within the plantar fascia and produce microscopic tears and chronic inflammation.6 Moreover, Wearing et al7 reported that pain severity and fascial thickening seen in cases of plantar fasciitis have an association with static medial arch posture and midfoot mechanical loading. Several physical therapy interventions have been used in the treatment of plantar fasciitis, including off-the-shelf insoles, custom-fabricated insoles, custom-made night splints, stretching of the plantar fascia and plantar flexors of the ankle, corticosteroid iontophoresis, and extracorporeal shock wave therapy, which should be used in chronic resistant conditions.1 Roxas4 pointed out a wide range of agreement in the literature with regard to the importance of rest, activity modification, and shoes with adequate arch support and cushion heel in controlling plantar heel pain; he also reported that the experimental works reviewed suggest higher efficiency of mechanical intervention (tape, shoe inserts, orthosis) when compared with anti-inflammatory (corticosteroid injection) and accommodative interventions. Low-Dye tape has been reported as an alternative for achieving mechanical support of foot arches, correction of foot pronation, and controlling mobility of the rear foot. Low-Dye taping techniques are reported to be short-term interventions, used as a temporary support until custom-made orthosis is applied.8 Despite being frequently used, we found, to the best of our knowledge, no comparative study of low-Dye taping and medial arch support, as a commonly used shoe insert, in short-term use. Thus, the purpose of this study was to compare the effect of low-Dye taping and medial arch support in managing pain and painrelated disability in patients with unilateral plantar fasciitis. We hypothesized that there would be no significant difference in effects when low-Dye taping and medial arch support are used to manage pain and pain-related disability in patients with unilateral plantar fasciitis in the short term. Methods Design This study was designed as a doubleblind randomized clinical trial. Patient Characteristics Thirty patients (23 men and 7 women) suffering from unilateral plantar fasciitis were randomly selected from a list of patients of a musculoskeletal physical therapy university clinic. The patients were then randomly allocated to a lowDye tape (LDT) group or to a medial arch support (MAS) group. Patients were included in the study if they had a diagnosis of unilateral plantar fasciitis; were aged between 40 and 60 years; had a painful attack that started at least 4 weeks prior to inclusion; had pain at the plantar heel, which was worse when first standing or walking after rest and improved initially after first standing but worsened with increasing activity; and were nonathletes. Patients were excluded from the study if they had any other cause of localized or referred plantar foot pain, had any lower limb deformity or surgery, had a corticosteroid injection during the past 3 months prior to participation in the study, or had any known allergies to taping (Figure 1). Patients in the LDT group included 12 men and 3 women with a mean age of 52.933 years (±4.542), a mean height of 1.684 m (±0.081), and a mean weight of 86.2 kg (±8.231). The patients in the MAS group included 11 men and 4 women with a mean age of 52.8 years (±4.003), a mean height of 1.694 m (±0.073), and a mean weight of 87 kg (±8.569). Body mass index (BMI) was calculated and compared between patients in both groups. Procedures To ensure blinding of the participating therapists, 3 therapists other than the authors were involved in implementing different parts of the study. The first therapist carried out both preexperimental and postexperimental assessment procedures; the therapist did not participate in, and had no knowledge of, any intervention allocation or procedures. The second therapist, who was well trained, carried out taping at the end of each session to patients in the LDT group. Again, this therapist was unaware of any details about the study procedures other than simply applying the low-Dye tape to the patients. The third therapist was in charge of implementing physical therapy sessions for patients in both groups. This therapist was blind to the patients’ group allocation, evaluation procedures, and type of supportive interventions. Prior to the onset of the experimental procedures, one of the authors interviewed each patient and gave a complete background of the general idea of the study, and each patient signed a consent form to approve his or her participation according to the general outlines described. The patients allocated to the MAS group were given instruction about the type (Powerstep Original Men’s/ Women’s Full-Length Insoles [FootSmart Co, Norcross, Georgia]), size, and fitting of the MAS to their most comfortable footwear. Later, they were asked to remove the MAS before they met any of the involved therapists at any scheduled evaluation or intervention session and to fit the MAS by themselves immediately after each session. They were also instructed to maintain the MAS throughout their activities of daily living. Similarly, patients in the LDT group were asked to remove the tape immediately before they met any of the participating therapists at any evaluation or intervention session, and when the tape was applied after sessions, they were asked to maintain it until the next session. Patient recruitment, group allocation, information given to patients, obtaining informed consent, evaluation, and the interventions in this study were strictly according to the Helsinki Declaration and approved by the council of postgraduate studies and research of physical therapy at the university where the study was carried out. However, patients were blind to their exact group differences related to Downloaded from fas.sagepub.com at UNIV OF DELAWARE LIB on February 10, 2015 87 88 April 2011 Foot & Ankle Specialist Figure 1. Study consort form. ASSESSMENT FOR ELIGIBILITY (N = 35) Excluded (n = 5) Not meeting inclusion criteria (n = 2) Refused to participate (n = 3) Enrollment Allocated to intervention (N = 15) Received allocated intervention (N = 15) Did not receive allocated intervention (N = 0) Give reasons Lost for follow-up (n = 0) Give reasons Discontinued intervention (n = 0) Give reasons Analyzed (n = 15) Excluded from analysis (n = 0) Give reasons the intervention in both groups and the expected outcomes. Evaluation Procedures Evaluation of pain severity was carried out using a 10-cm visual analog scale, where the 0-cm end was “No pain” and the 10-cm end was “Intractable pain.” A patient was asked to mark his or her perceived pain severity anywhere throughout the continuum, and the mark was then measured to the nearest millimeter. Manchester Foot Pain and Disability Schedule9 was administrated to report patients’ pain-related disability. It is a 19-item questionnaire, with each item having 3 possible responses: 1 = none of the time; 2 = On some days; and 3 = On most Allocation Allocated to intervention (N = 15) Received allocated intervention (N = 15) Did not receive allocated intervention (N = 0) Give reasons Follow-up Analysis days or every day. Lower scores denoted no/less disability and higher scores denoted higher disability because of foot pain. The questionnaire was translated into Arabic, and the preexperimental responses of patients in both groups were used to ensure internal consistency of the Arabic questionnaire, which was to be used as an outcome measure. Treatment Procedures Patients in each group received 9 sessions of conventional physical therapy, 3 sessions weekly (alternate day) for 3 weeks, that consisted of identical programs for both groups: ultrasound therapy to the plantar surface of the foot Lost for follow-up (n = 0) Give reasons Discontinued intervention (n = 0) Give reasons Analyzed (n = 15) Excluded from analysis (n = 0) Give reasons applied for 8 minutes, 1.2 W/cm2, 1 MHz, pulsed mode 1:2; stretching of calf muscles for 5 repetitions; holding for 30 seconds each.10 The author who carried out the initial interview discussed the fitting of the MAS with the patients in the MAS group. Taping was carried out by another welltrained therapist at the end of each session with patients in the LDT group, using 5-cm Leukoplast rigid tape (Westons, England). Statistical Procedures BMI of the patients in the LDT and MAS groups was compared using an independent t test. Only BMI was analyzed as it was the only parameter that has been Downloaded from fas.sagepub.com at UNIV OF DELAWARE LIB on February 10, 2015 vol. 4 / no. 2 Foot & Ankle Specialist Patients in the current study had comparable BMI in both groups, showing a mean BMI of 30.092 (±1.471) in the LDT group and 30.267 (±1.507) in the MAS group. Both groups showed a nonsignificant difference with regard to BMI (P = .750). Within-group analysis showed significant improvement in mean pain intensity values and mean pain-related disability values at posttest evaluation when compared with pretest evaluation in both the groups (see Table 1 and Figures 2 and 3). Between-groups comparison showed nonsignificant differences at preexperimental evaluation for both pain intensity mean values and pain-related foot disability questionnaire. At postexperimental evaluation significant improvements in mean pain intensity values and mean pain-related disability questionnaire values were detected in the MAS group (see Table 2 and Figures 4 and 5). Within-Group Comparison of Mean Difference in Visual Analog Scale (VAS) and Foot Pain and Disability Schedule (FPDS) at Preexperimental and Postexperimental Evaluations Pre–Post Evaluations of Paired Differences 95% CI of the Difference Mean Difference SD Lower Upper t Value Significance LDT (VAS) 0.873 0.698 0.487 1.260 4.843 .000a MAS (VAS) 3.347 1.234 2.663 4.030 10.504 .000a LDT (FPDS) 6.267 1.579 5.392 7.141 15.365 .000a MAS (FPDS) 11.801 3.005 10.136 13.464 15.210 .000a Abbreviations: CI, confidence interval; LDT, low-Dye taping; MAS, medial arch support. a P < .05. Figure 2. Figure 3. Comparison of mean preexperimental and postexperimental Visual Analog Scale (VAS) values of patients in the LDT and MAS groups. Comparison of mean preexperimental and postexperimental Foot Pain and Disability Schedule (FPDS) scores of patients in the LDT and MAS groups. 50 10 8 5.873 6 6.681 5.001 Nonsignificant differences in patients’ BMI in the LDT and MAS groups indicated that patients in both groups are comparable with each other and that patients’ BMI group distribution would not affect the outcome parameters. Patients in the LDT group showed significant reduction in pain intensity as well as significant improvement in painrelated foot disability postexperimentally when compared with the preexperimental evaluation. This finding is consistent with that in the literature, as some authors had reported improvement in pain intensity in cases of plantar fasciitis 3.333 4 2 0 LDT Groups Post followings the application of lowDye taping combined with iontophorsis12 and low-Dye taping combined with sham ultrasound.8 Several authors provided mechanical explanations of the role of low-Dye taping in reducing symptoms of plantar fasciitis. O’Sullivan et al13 reported that the application of low-Dye tape seemed to reduce rear foot pronation through limitation of general rear foot mobility. Saxelby et al14 suggested that the effects of low-Dye taping may lie in its ability to 40 43.667 37.401 44.201 32.401 30 20 10 0 MAS Pre Discussion Paired t Test Group/ Outcome FPDS (SCORE) Results Table 1. PAIN INTENSITY (VAS) reported to be significantly related to disability in patients with unilateral plantar fasciitis.11 Within-group analysis of the outcome parameters, namely, VAS for pain intensity and the foot pain disability questionnaire for pain-related disability, was carried out to compare preexperimental and postexperimental outcomes in each group applying a paired t test. Betweengroups comparison of preexperimental and postexperimental outcomes was made using an independent t test. LDT Groups Pre MAS Post simply reduce tension in the plantar fascia; however, they failed to show conclusively that low-Dye taping reduced foot pronation. Patients in the MAS group, similarly, showed significant reduction of pain intensity, and pain-related disability improved postexperimentally when compared with the preexperimental evaluation. Previous investigations suggested that the effects of MAS, along with several other types of orthosis, were because of the support of the medial longitudinal Downloaded from fas.sagepub.com at UNIV OF DELAWARE LIB on February 10, 2015 89 April 2011 Foot & Ankle Specialist Table 2. Comparison of Mean Visual Analog Scale (VAS) and Foot Pain and Disability Schedule (FPDS) Values in LDT and MAS Groups at Preexperimental and Postexperimental Evaluations LDT Group 95% CI of the Difference MAS Group t Test Outcome/ Evaluation Mean VAS pre 5.873 1.435 6.681 1.971 -2.096 0.482 -1.281 .211 VAS post 5.001 1.813 3.333 1.175 2.809 FPDS pre 43.667 5.052 44.201 7.831 -5.462 4.395 -0.222 .826 FPDS post 37.401 4.372 32.401 5.356 8.657 SD Mean SD Lower 0.524 1.343 Upper t Value Sig 2.988 .006a 2.801 .009a Abbreviations: CI, confidence interval; LDT, low-Dye taping; MAS, medial arch support. a P < .05. Figure 4. Figure 5. Comparison of mean Visual Analog Scale (VAS) values at preexperimental and postexperimental evaluations of patients in the LDT and MAS groups. Comparison of mean Foot Pain and Disability Schedule (FPDS) values at preexperimental and postexperimental evaluations of patients in the LDT and MAS groups. 10 8 50 5.873 6.681 5.001 6 4 3.333 2 0 VAS pre VAS post Evaluations LDT group FPDS (score) Pain intensity (VAS) 90 32.401 20 10 FPDS pre FPDS post Evaluations LDT group arch and limitation of rear foot pronation, which reduces the amount of tension on the plantar fascia by realigning the foot and the supporting arch.15 Because of this mechanism, pain on the plantar surface of the foot, especially pain at the calcaneal insertion of the plantar fascia, seems to be alleviated.16 When we compared outcome measures between groups, it was found that improvements in pain intensity and painrelated disability were significantly better in the MAS group when compared with the LDT group. Although the patients 37.401 30 0 MAS group 43.667 44.201 40 MAS group in the LDT and MAS groups generally shared a similar mechanism of correction, namely, reduced foot pronation, elevation and support of the medial longitudinal arch height, and reducing tension along plantar fascia, these mechanisms seemed to be more efficient in patients in the MAS group than in patients in the LDT group. This idea is consistent with several studies that documented a reduced effect of LDT shortly after application. For instance, Fleet et al17 investigated the effect of activity over time on the stiffness of the applied LDT, by assessing the strength of the tape quantified as the moment required to rotate the foot passively into inversion, measured using a handheld dynamometer, and range of motion (ROM), measured using a goniometer. Within 15 minutes a 15% decrease in moment required to rotate the foot was reported, 48% reduction within 1 hour, and 86% reduction over 24 hours. This showed the fast loss in mechanical support that amounted approximately to 50% within 1 hour. This is not the case with MAS, which appears more capable of retaining mechanical correction and rear foot control throughout its application time. Fong et al18 reported that MAS was specially effective in controlling rear foot eversion during functional activities that implied walking and running, which clarifies the better responses reported in patients in the MAS group in the current study regarding foot pain and disability schedule, where several items were related to pain during walking. Although the clinical effect of MAS orthotics in plantar fasciitis was reported to be controversial,2 our results suggest that in short-term evaluation, over 3 weeks, MAS used with exercises sessions were efficient in reducing pain and pain-related disability. Previous research that recommended LDT suggested that it should be used for a short period of time until custommade orthosis is fabricated, because of its adverse effects on the skin and low patient tolerance to longer durations; it has also been reported that LDT was significantly effective in reducing pain at first step in the morning only, not during daily activities, and that it was because patients focused on this symptom in particular.10 We could further suggest that the rapid decrement of supporting action of LDT would not enable it to reduce tension and minimize pain over a prolonged period throughout the day. LDT would require several reapplications for tightening over the time of use. So it would be easier and more effective if prefabricated MAS is used, even for short-term usage, early in the treatment of plantar fasciitis, Downloaded from fas.sagepub.com at UNIV OF DELAWARE LIB on February 10, 2015 vol. 4 / no. 2 Foot & Ankle Specialist as it has a better potential to improve clinical outcomes, maintains mechanical support, fits it easily into patients comfortable footwear without the need for an expert for readjustment as in case of LDT, may be used for a prolonged time when compared with the LDT, and there are no reports of patient discomfort or skin problems as with LDT. LDT might be used for another patient group, such as athletic runners who suffer plantar fasciitis pain while running and cannot perform well with the MAS insert or any other foot orthosis. Conclusion According to the study outcomes, we suggest that medial arch support is more convenient than low-Dye taping technique in the short-term management of pain and pain-related disability in plantar fasciitis. References plantar fasciitis. Clinics (Sao Paulo). 2009;64:97-103. fasciitis? A meta-analysis. Phys Ther Sport. 2009;10:12-18. 3. Buchbinder R. Clinical practice. Plantar fasciitis. N Engl J Med. 2004;350: 2159-2166. 4. Roxas M. Plantar fasciitis: diagnosis and therapeutic considerations. Altern Med Rev. 2005;10:83-93. 5. Hunt GC, Sneed T, Hamannb H, Chisam S. Biomechanical and histiological considerations for development of plantar fasciitis and evaluation of arch taping as a treatment option to control associated plantar heel pain: a single-subject design. Foot. 2004;14:147-153. 6. Ayub A, Yale SH, Bibbo C. Common foot disorders. Clin Med Res. 2005;3:116-119. 7. Wearing SC, Smeathers JE, Sullivan PM, Yates B, Urry SR, Dubois P. Plantar fasciitis: are pain and fascial thickness associated with arch shape and loading? Phys Ther. 2007;87:1002-1008. 8. Radford JA, Landorf KB, Buchbinder R, Cook C. Effectiveness of low-Dye taping for the short-term treatment of plantar heel pain: a randomized trial. BMC Musculoskelet Disord. 2006;7:64. 1. Cole C, Seto C, Gazewood J. Plantar fasciitis: evidence-based review of diagnosis and therapy. Am Fam Physician. 2005;72:2237-2342. 9. Garrow AP, Papageorgioua AC, Silmana AJ, Thomasa E, Jaysonb MIV, Macfarlanea GJ. Development and validation of a questionnaire to assess disabling foot pain. Pain. 2000;85:107-113. 2. Lee SY, McKeon P, Hertel J. Does the use of orthoses improve self-reported pain and function measures in patients with plantar 10. Greve JMD, Grecco MV, Santos-Silva PR. Comparison of radial shock waves and conventional physiotherapy for treating 11. Riddle DL, Pulisic M, Sparrow K. Impact of demographic and impairment-related variables on disability associated with plantar fasciitis. Foot Ankle Int. 2004;25:311-317. 12. Osborne HR, Allison GT. Treatment of plantar fasciitis by low-Dye taping and iontophoresis: short term results of a double blinded, randomized, placebo controlled clinical trial of dexamethasone and acetic acid. Br J Sports Med. 2006;40:545-549. 13. O’Sullivan K, Kennedy N, O’Neill E, Mhainin UN. The effect of low-Dye taping on rearfoot motion and plantar pressure during the stance phase of gait. BMC Musculoskelet Disord. 2008;9:111. 14. Saxelby J, Betts RP, Bygrave CJ. “Low-Dye” taping on the foot in the management of plantar-fasciitis. Foot. 1997;7:205-209. 15. Genova JM, Gross ML. Effect of foot orthotics on calcaneal eversion during standing and treadmill walking for subjects with abnormal pronation. J Orthop Sports Phys Ther. 2000;11:664-675. 16. Gould JS. Chronic plantar fasciitis. Am J Orthop. 2003;1:11-13. 17. Fleet K, Galen S, Moore C. Duration of strength retention of ankle taping during activities of daily living. Injury. 2009;40:333-336. 18. Fong DTP, Lam MH, Lao MLM, et al. Effect of medial arch-heel support in inserts on reducing ankle eversion: a biomechanics study. J Orthop Surg Res. 2008;3:7. Downloaded from fas.sagepub.com at UNIV OF DELAWARE LIB on February 10, 2015 91