Rerupture Rate after Early Weightbearing in Operative Versus Conservative
advertisement

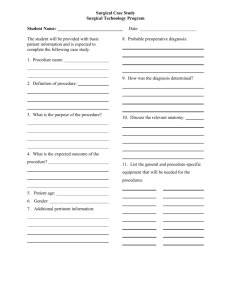
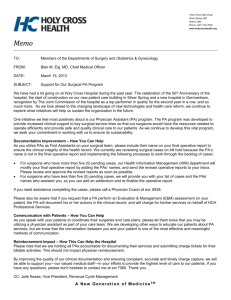
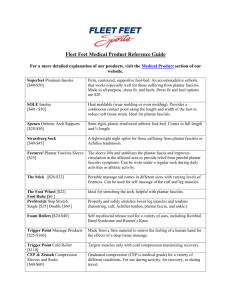
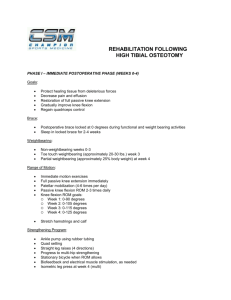
The Journal of Foot & Ankle Surgery 52 (2013) 622–628 Contents lists available at ScienceDirect The Journal of Foot & Ankle Surgery journal homepage: www.jfas.org Rerupture Rate after Early Weightbearing in Operative Versus Conservative Treatment of Achilles Tendon Ruptures: A Meta-analysis Dorien M. van der Eng, MD 1, Tim Schepers, MD, PhD 2, J. Carel Goslings, MD, PhD 2, Niels W.L. Schep, MD, PhD, MSc 2 1 2 Department of Surgery, Academic Medical Centre, Amsterdam, The Netherlands Trauma Unit, Department of Surgery, Academic Medical Centre, Amsterdam, The Netherlands a r t i c l e i n f o a b s t r a c t Level of Clinical Evidence: 1 Keywords: Achilles tendon braces rupture surgical procedure weightbearing Whether Achilles tendon rupture benefits from surgery or conservative treatment remains controversial. Moreover, the outcome can be influenced by the rehabilitation protocol. The goal of the present meta-analysis was to compare the rerupture rate after surgical repair of the Achilles tendon followed by weightbearing within 4 weeks versus conservative treatment with weightbearing within 4 weeks. In addition, a secondary analysis was performed to compare the rerupture rates in patients who started weightbearing after 4 weeks. Seven randomized controlled trials published from 2001 to 2012, with 576 adult patients, were included. The primary outcome measure was the rerupture rate. The secondary outcomes were minor and major complications other than rerupture. In the early weightbearing group, 7 of 182 operatively treated patients (4%) experienced rerupture versus 21 of 176 of the conservatively treated patients (12%). A secondary analysis of the patients treated with late weightbearing showed a rerupture rate of 6% (7 of 108) for operatively treated patients versus 10% (11 of 110) for conservatively treated patients. The differences concerning the rerupture rate in both groups were not statistically significant. No differences were found in the occurrence of minor or major complications after early weightbearing in both patient groups. In conclusion, we found no difference in the rerupture rate between the surgically and nonsurgically treated patients followed by early weightbearing. Weightbearing after 4 weeks also resulted in no differences in the rupture rate in the surgical versus conservatively treated patients. However, surgical treatment was associated with a twofold greater complication rate than conservative treatment. Ó 2013 by the American College of Foot and Ankle Surgeons. All rights reserved. Rupture of the Achilles tendon is a common injury, mostly affecting adult males who participate in sports (1). Whether Achilles tendon rupture requires surgery or nonoperative treatment remains controversial. The outcome can also be influenced by the methods of rehabilitation. Specifically, weightbearing or non-weightbearing might be of importance. Research has shown lower rerupture rates after surgery compared with nonsurgical treatment but not always with a significant difference. In previously conducted meta-analyses, the rerupture rates for surgically treated patients varied from 3.1% to 5.0% versus 8.8% to 13% for nonsurgically treated patients (1–4). One drawback of surgery has been the greater rate of complications. The pooled results of the Cochrane collaboration showed a 29% Financial Disclosure: None reported. Conflict of Interest: None reported. Address correspondence to: Dorien M. van der Eng, MD, Department of Surgery, Academic Medical Centre, Nachtwachtlaan 120, Amsterdam 1058 ED, The Netherlands. E-mail address: d.m.vandereng@hotmail.com (D.M. van der Eng). complication rate in the surgical group versus 8% in the nonsurgical group (2). Animal studies have shown that immobilization compromises the healing process of tendons and could indicate that a functional rehabilitation protocol is warranted (5,6). Krapf et al investigated operatively and nonoperatively treated Achilles tendon ruptures in rat models with immediate weightbearing (7). They found no difference in the maximum failure load between the operative and nonoperative groups, nor did they find a difference in tendon stiffness during the 8-week research period. However, a nonoperatively treated Achilles tendon rupture showed a nearly normal histologic pattern, although a sutured tendon showed scar tissue and less organized collagen fibers (7). Earlier research also showed that loading of healing tendons leads to essential changes in the biologic process of tendon healing (8). Moreover, early weightbearing could theoretically prevent muscle atrophy, stiffness, adhesions, and deep venous thrombosis and has been associated with faster healing and stronger tendons because of improved vascularization and an improved immunologic response 1067-2516/$ - see front matter Ó 2013 by the American College of Foot and Ankle Surgeons. All rights reserved. http://dx.doi.org/10.1053/j.jfas.2013.03.027 D.M. van der Eng et al. / The Journal of Foot & Ankle Surgery 52 (2013) 622–628 (5–7). It is also considered to be more patient friendly. Therefore, early mobilization after operative and nonoperative treatment of Achilles tendon ruptures has been advocated (9–11). Previous reviews and trials that compared surgical and nonsurgical treatment did not specifically focus on the rehabilitation protocol. Therefore, the goal of the present meta-analysis was to compare the rerupture rate after surgical repair of the Achilles tendon followed by early weightbearing versus conservative treatment with early weightbearing. An additional analysis was performed of surgical versus conservative management with weightbearing after 4 weeks. The secondary outcomes were minor and major complications. Patients and Methods The present study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (12). Eligibility Criteria Randomized controlled trials of adults patients with acute rupture of the Achilles tendon, published from 2001 to 2012, were included. The intervention was defined as surgical repair of the Achilles tendon followed by early weightbearing. The control group consisted of those who had undergone nonoperative treatment with early weightbearing. The surgical treatment could include open or minimally invasive repair. Nonoperative treatment could consist of casting, bracing, orthosis, and taping. Early weightbearing was defined in the present study as weightbearing initiated within the first 4 weeks after treatment. The follow-up period had to be at least 1 year. In addition, a subgroup analysis was performed to compare the rerupture rates in surgically versus nonsurgically treated patients for whom weightbearing was initiated 4 weeks after the beginning of treatment. Primary and Secondary Outcomes The primary outcome measure was the rerupture rate. The secondary outcomes were minor and major complications. Minor complications included superficial wound infections, painful or hypertrophic scars, and transient pain. Major complications included deep vein thrombosis, pulmonary embolism, deep infection, and sural nerve injury. 623 Results Data Search The search resulted in 32 potentially relevant studies. Of these, 10 met the inclusion criteria. However, 3 studies were excluded because no comparison had been done between operative and nonoperative treatment. Thus, 7 randomized controlled trials, with 624 patients, were included in the present meta-analysis (Fig. 1). After 1 year of follow-up, a total of 576 patients were eligible for evaluation. Of these 576 patients, 290 were treated operatively and 286 were treated nonoperatively. Of the 7 studies, 6 had included 496 patients and compared open operative treatment and nonoperative treatment, followed by functional rehabilitation after 1 year of follow-up (13–18). The seventh study compared minimally invasive surgical treatment and conservative treatment and included 80 patients (9). Description of Included Studies The characteristics and rehabilitation protocols of the studies are summarized in Tables 1 and 2. The study by Costa et al (13) consisted of 2 independent trials. The patients chose either operative or nonoperative treatment. Subsequently, the patients from the 2 treatment arms were randomized by computer for the rehabilitation method. In the first trial, all the patients underwent surgical repair of the Achilles tendon. Rehabilitation consisted of functional bracing with early weightbearing or a plaster cast without weightbearing. The choice of surgical technique was left to the operating surgeon. In the second trial, every patient was treated nonoperatively. Similar to their first trial, the patients were randomized for functional rehabilitation after treatment with immediate weightbearing or a plaster cast without weightbearing. After 6 months, an independent Information Sources and Search Methods The Ovid MEDLINE electronic database (January 2001 to December 2012) and the Cochrane Library were used for the data search. A systematic search was performed with the following terms: Achilles tendon (MeSH), rupture (MeSH) AND surgery (all fields) or surgical procedures, operative (MeSH). The studies were limited to randomized controlled trials. The following search strategy was used: ((“achilles tendon”[MeSH Terms] OR (“achilles”[All Fields] AND “tendon”[All Fields]) OR “achilles tendon”[All Fields]) AND (“rupture”[MeSH Terms] OR “rupture”[All Fields])) AND (“surgery”[Subheading] OR “surgery”[All Fields] OR “surgical procedures, operative”[MeSH Terms] AND Randomized Controlled Trial[ptyp] AND (“2001/01/01”[PDAT] : “2012/12/31”[PDAT])). Study Selection Two physicians assessed the abstracts of the studies during the initial search. Fulltext copies of potentially relevant studies were assessed by the same physicians and subsequently verified by a trauma surgeon. Quality Assessment For evaluation of the methodologic quality of the included studies, the guidelines of the Cochrane Bone, Joint and Muscle Trauma group were used. The quality assessment of the included studies was performed in duplicate by 2 physicians. 32 articles identified through search strategy 3 articles removed (duplicates) 29 articles screened 19 articles excluded, because not meeting eligibility criteria 10 full-text articles assessed for eligibility 3 articles excluded, because no comparison between operative and non-operative treatment 7 studies included in qualitative synthesis Data Collection and Analysis The Cochrane Review Manager software, version 5.1 (RevMan, Cochrane Collaboration, Oxford, UK) was used for data analysis. Two physicians extracted the data from all included studies. All outcomes were dichotomous variables. The risk ratios (RRs) and 95% confidence intervals (CIs) were calculated. A treatment effect was defined as significant if p < .05. The random effects model was used. Heterogeneity was explored using the chisquare test, with significance set at p < .100. For quantification, I2 was used, with values less than 30% indicating low heterogeneity. 7 of studies included in quantitative synthesis (meta-analysis) Fig. 1. Study flow diagram of the systematic review. 624 D.M. van der Eng et al. / The Journal of Foot & Ankle Surgery 52 (2013) 622–628 Table 1 Characteristics of included studies, including number of patients, follow-up, and study type Investigator Costa et al (13), 2006 Keating et al (14), 2011 Metz et al (9), 2008 €ller et al (15), 2001 Mo Nilsson-Helander et al (16), 2010 Twaddle et al (17) 2007 Willits et al (21), 2010 Total Initially Included Patients (n) After 1 y of Follow-Up (n ¼ 576) Total Operative Operative Conservative Patients Lost to Follow-Up (%) Conservative Mean Age (y) Operative Technique Study Type Operative Conservative 55 80 83 112 100 23 39 42 59 50 22 41 41 53 50 20 37 41 59 49 19 39 39 53 48 10.9 5 3.6 0 3 42.0 41.2 40.0 39.6 40.9 53.0 39.5 41.0 38.5 41.2 Unknown Open, Kessler stitch Minimally invasive, Bunnell Open, Kessler stitch Open, Kessler stitch Multicenter Single center Multicenter Multicenter Single center 50 144 624 25 72 310 25 72 304 22 62 290 23 65 286 10 11.8 41.8 39.7 40.3 41.1 Open, Krackow Open, Krackow Single center Multicenter physiotherapist performed muscle function tests and a clinical assessment to measure the ankle range of motion. For the present meta-analysis, the immediate weightbearing group of the surgical trial was compared with the immediate weightbearing group of the conservative trial (13). In the study by Keating and Will (14), the patients were randomly allocated to operative or nonoperative treatment. The surgically treated patients had undergone surgery within 7 days of presentation. The operation was performed by 1 of the 4 involved consultant orthopedic surgeons or by a senior trainee under supervision. The complete postoperative treatment was a plaster cast in both groups. The patients were allowed to start weightbearing after 6 and 8 weeks in the operative and nonoperative groups, respectively. Range of motion and isokinetic tests were performed by a research physiotherapist (14). The study by Metz et al (9) was unique in that minimal invasive surgery was used (i.e., an incision of <5 cm). In the randomization process, block stratification was applied to balance the groups among the 4 participating hospitals. Treatment in the surgical and conservative group was initiated within 3 days after rupture. All the physicians were familiar with the minimally invasive technique. The patients in the surgical group received 1 week of plaster casting and were not allowed to load their leg during that week. The rehabilitation phase for the nonsurgically treated patients consisted of a brace (VacopedÒ, OPED, Valley, Germany). The patients were not allowed to remove it by themselves. Both groups were allowed to start weightbearing after 1 week (9). € ller et al (15) randomized their patients between surgical repair Mo with bracing and nonsurgical treatment with a plaster cast. The treatment started within 7 days after rupture. Surgically treated patients were allowed to remove the brace and were encouraged to exercise. Weightbearing was allowed in the third week for the surgically treated patients and in the fourth week for the nonsurgically treated patients. Diagnostic tests were performed by independent physiotherapists (15). The patients from the surgical and nonsurgical groups in the study by Nilsson et al (16) were treated within 3 days. Surgery was performed by 1 of 28 orthopedic surgeons. The patients from both groups wore a brace and were not allowed to remove it (DonJoy ROM Wal€ , Sweden). Weightbearing was allowed after kerÒ, DJO Nordic, Malmo 6 weeks. The evaluation of leg function and physical activity was performed by 2 independent physiotherapists (16). In the study by Twaddle and Poon (17), the patients had to have presented within 10 days after their injury. Allocation was performed by tossing a coin 50 times. The sequence of “heads” (operative) and “tails” (nonoperative) was used to allocate the sequence of blinded envelopes with the treatment option. Within 2 days after presentation, the patients in the surgical group underwent surgery by a senior Table 2 Description of postoperative protocol of surgical and nonsurgical groups Investigator Costa et al (13), 2006 Keating et al (14), 2011 Metz et al (9), 2008 €ller et al (15), 2001 Mo Nilsson-Helander et al (16), 2009 Twaddle et al (17), 2007 Willits et al (18), 2010 Protocol Surgical Group Brace: 4.5-, 3.0-, 1.5-, 0-cm heel raise for 2, 2, 2, 2 wk Cast: equinus, semi-equinus for 4, 2 wk Cast: 30 plantar flexion for 1 wk, followed by functional taping þ heel raise: 2 cm, 1 cm, 0 cm for 2, 2, 2 wk Cast: equinus for 12 days, followed by brace: maximal 30 plantar flexion, 10 plantar flexion, maximal 10 dorsiflexion for 4, 2, 2 wk Cast: equinus for 2 wk, followed by brace: 30 plantar flexion, 10 plantar flexion, dynamic, maximal 10 dorsiflexion for 2, 2, 2 wk Cast: equinus for 10 days, followed by brace: 20 plantar flexion, neutral for 2, 4 wk Cast: 20 plantar flexion for 2 wk, followed by brace: 20 plantar flexion, neutral for 4, 2 wk Protocol Conservative Group Brace: 4.5-, 3.0-, 1.5-, 0-cm heel raise for 2, 2, 2, 2 wk Cast: equinus, semi-equinus, neutral for 4, 4, 2 wk Cast: 30 plantar flexion for 1 wk, followed by brace: 30 plantar flexion, 15 plantar flexion, dynamic neutral for 2, 2, 2 wk Cast equinus, neutral for 4, 4 wk Cast: equinus for 2 wk, followed by brace: 30 plantar flexion, 10 plantar flexion, dynamic, maximal 10 dorsiflexion for 2, 2, 2 wk Cast: equinus for 10 days, followed by brace: 20 plantar flexion, neutral for 2, 4 wk Cast: 20 plantar flexion for 2 wk, followed by brace: 20 plantar flexion, neutral for 4, 2 wk Start Weightbearing Follow-Up Visits Operative Nonoperative Immediate Immediate 2, 3, 6, 12 mo 6 wk 8 wk 3, 4, 6, 12 mo 1 wk 1 wk 1, 3, 5, 7 wk, 3, 6, 12 mo 3 wk 4 wk 2, 3, 6, 12, 24 mo 6–8 wk 6–8 wk 2 wk, 2, 3, 6, 12 mo 6 wk 6 wk 2 wk, 2, 3, 6, 12 mo 2 wk 2 wk 3, 6, 12, 24 mo D.M. van der Eng et al. / The Journal of Foot & Ankle Surgery 52 (2013) 622–628 surgeon. After 2 weeks of plaster casting, the patients in both groups received a removable, functional orthosis for 6 weeks. The patients were instructed to remove the brace for 5 minutes every hour to practice active dorsiflexion (not beyond neutral) and passive plantar flexion. At 6 weeks after the beginning of treatment, the patients were allowed to remove the brace during the night and were allowed to start weightbearing (17). In the study by Willits et al (18), the patients had to have presented within 14 days after the injury. No mention was made of the number or experience level of the surgeons. The rehabilitation protocol was identical in the 2 groups. After 2 weeks of plaster casting, the patients were placed in a brace (Aircast, Summit, NJ). After 2 weeks, partial weightbearing was permitted, and weightbearing as tolerated was allowed in the fourth week. The patients were required to wear the brace during the night but were allowed to remove it for bathing (18). Methodologic Quality The methodologic scoring items and individual scores for each study are listed in Table 3. Low scores indicate poor methodology. Two items from the list (blinding of patients and care providers) were excluded because they proved negative for all 7 studies. Outcome Parameters Rerupture Rate All 7 studies (n ¼ 576 patients) reported information on the rerupture rate. The 4 studies in which weightbearing was initiated within 4 weeks after treatment demonstrated no significant difference in the rerupture rate (9,13,15,18). Of the 182 patients in the operative group, 7 (4%) experienced a rerupture compared with 21 of 176 patients (12%) in the nonoperative group. The RR was 0.4 (95% CI 0.12 to 1.32, p ¼ .13, I2 ¼ 38%). In the subgroup of 3 studies in which weightbearing was allowed after 4 weeks, no difference between the groups could be demonstrated (11,16,17). Of the 108 patients in the operative group, 7 (6%) experienced rerupture compared with 11 of 110 (10%) patients in the nonoperative group. The RR was 0.64 (95% CI 0.25 to 1.63, p ¼ .35, I2 ¼ 0%). An analysis of all the included studies combined showed no significant difference in the rerupture rate between the operatively and nonoperatively treated patients (9,13–18). The rerupture rate was 5% (14 of 290) in the operatively treated group and 11% (32 in 286) in the nonoperatively treated group (RR 0.50, 95% CI 0.25 to 1.00, p ¼ .05, I2 ¼ 8%; Fig. 2). Complications Data on the complications other than reruptures were reported in all 7 studies. 625 Minor Complications. In the early weightbearing group, the incidence of minor complications in the surgical group was 15% (28 of 182 patients) compared with 9% (15 of 176 patients) in the nonsurgical group. The RR was 3.54 (95% CI 0.4 to 31.61, p ¼ .26, I2 ¼ 82%). In the group that started weightbearing after 4 weeks, 5 complications developed in the 108 surgically treated patients (5%) versus 0 complications in the 110 nonsurgically treated patients. The RR was 5.53 (95% CI 0.65 to 46.88, p ¼ .12, I2 ¼ 0%). The pooled results of the 2 groups showed a greater incidence of complications in the surgically treated group; however, no significant difference was found. Of the 290 patients in the surgical group, 33 (11%) developed minor complications compared with 15 of the 286 patients (5%) in the nonsurgical group (RR 3.85, 95% CI 0.72 to 20.56, p ¼ .12, I2 ¼ 74%; Fig. 3A). Major Complications. The incidence of major complications was lower than that of the minor complications. In the immediate weightbearing patients, 6% of the surgically treated group versus 3% of the nonsurgically treated group developed a major complication (RR 1.79, 95% CI 0.64 to 5.01, p ¼ .27, I2 ¼ 0%). In the group that started weightbearing after 4 weeks, complications occurred in 6 of 108 surgically treated patients (6%) and 4 of 110 nonsurgically treated patients (4%; RR 1.24, 95% CI 0.19 to 7.93, p ¼ .82, I2 ¼ 38%). For the total group, the incidence of major complications was greater in the surgically treated patients (16 of 290 [6%] versus 7 of 286 [2%]). Again, no significant difference was found (RR 1.56, 95% CI 0.68 to 3.59, p ¼ .29, I2 ¼ 0%; Fig. 3B). Fig. 4 shows a greater total complication rate for the surgically versus conservatively treated patients. In the surgical group, 49 of 290 (17%) developed a complication versus 22 of 286 (8%) in the nonsurgical group (RR 3.00, 95% CI 0.88 to 10.21, p ¼ .08, I2 ¼ 74%). Strength and Range of Motion Four studies provided information on isokinetic ankle strength, tested with dynamometry (13–15,18). All tests were performed using dynamometers with different settings and patient positioning. Furthermore, the results were not uniformly reported. Because of various measuring methods used and nonuniform reporting of the results, no comparison could be made in the present study. Costa et al (13) found no significant difference in eccentric or concentric peak torque strength between the surgical and nonsurgical groups. Keating and Will (14) found no difference in dorsiflexion or plantar flexion peak strength after 1 year in the operative and nonoperative € ller et al (15) found that groups. Both Keating and Will (14) and Mo both groups showed increased range of dorsiflexion. In neither group was a significant difference provable (14,15). Willits et al (18) could not demonstrate clinically important differences between the Table 3 Quality assessment of included studies using methodologic quality evaluation guidelines of Cochrane Bone, Joint and Muscle Trauma group Investigators Factors Affecting Quality Randomization or Allocation Concealment Costa et al (13), 2006 Keating et al (14), 2011 Metz et al (9), 2008 € ller et al (15), 2001 Mo Nilsson-Helander et al (16), 2009 Twaddle et al (17), 2007 Willits et al (18), 2010 * 1, 2, 2, 2, 2, Patient choice þ computer Blinded envelope Computer Blinded envelope Computer 1, Tossing a coin 2, Computer Total (maximum 18 points) Intention to Treat Blinding Treatment to Outcome Assessors Comparable Treatment Groups Care Programs Identical Clear Inclusion and Exclusion Criteria Interventions Clearly Defined Clear Outcome Measures Adequate Active Follow-Up Length 0 1 1 1 1 1 0 0 1 1 0 2 2 2 2 0 0 0 0 2 0 2 2 2 2 1 2 2 2 2 2 2 2 2 2 2 2 2 2 2 7 13 13 14 16 1 1 0 0 2 2 2 2 2 2 2 2 1* 2 2 2 13 15 No confidence intervals or standard deviations mentioned. 626 D.M. van der Eng et al. / The Journal of Foot & Ankle Surgery 52 (2013) 622–628 Operative Conservative Risk Ratio Study or Subgroup Events Total Events Total Weight M-H, Random, 95% CI 1.1.1 Start weight before 4 weeks 1.90 [0.19, 19.27] 8.5% 19 1 20 2 Costa 2006 0.32 [0.07, 1.48] 39 18.1% 6 41 2 Metz 2008 0.08 [0.01, 0.61] 53 11.1% 11 59 1 Möller 2001 0.70 [0.12, 4.04] 65 14.3% 3 62 2 Willits 2010 0.40 [0.12, 1.32] 176 51.9% 182 Subtotal (95% CI) Risk Ratio M-H, Random, 95% CI 21 7 Total events Heterogeneity: Tau² = 0.55; Chi² = 4.81, df = 3 (P = 0.19); I² = 38% Test for overall effect: Z = 1.50 (P = 0.13) 1.1.2 Start weight bearing after 4 weeks Keating 2011 Nilsson 2009 Twaddle 2007 Subtotal (95% CI) 2 3 2 37 49 22 108 4 6 1 39 48 23 110 16.2% 23.5% 8.4% 48.1% 0.53 [0.10, 2.71] 0.49 [0.13, 1.85] 2.09 [0.20, 21.45] 0.64 [0.25, 1.63] 11 7 Total events Heterogeneity: Tau² = 0.00; Chi² = 1.20, df = 2 (P = 0.55); I² = 0% Test for overall effect: Z = 0.94 (P = 0.35) Total (95% CI) 290 286 100.0% 32 14 Total events Heterogeneity: Tau² = 0.07; Chi² = 6.52, df = 6 (P = 0.37); I² = 8% Test for overall effect: Z = 1.96 (P = 0.05) Test for subgroup differences: Chi² = 0.35, df = 1 (P = 0.56), I² = 0% 0.50 [0.25, 1.00] 0.01 0.1 1 10 100 Favours operative Favours conservative Fig. 2. Table and Forest plot illustrating the rate of reruptures, divided into 2 groups. The first group started weightbearing before 4 weeks after initiation of treatment. The second group started weightbearing after 4 weeks. Chi2, chi-square; CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel. operative and nonoperative patients concerning the range of dorsiflexion or plantar flexion. Also, no difference in strength could be measured (18). Discussion The present meta-analysis showed no significant differences in the rate of rerupture in surgically treated patients and conservatively treated patients after early weightbearing. An analysis of patients with delayed weightbearing after 4 or more weeks also did not demonstrate a difference in the rerupture rate. Also, no differences were seen in the incidence of minor or major complications after early weightbearing in the surgically and conservatively treated patients. However, for the total group of patients, surgery resulted in significantly more complications compared with conservative treatment. No less than 1 of 6 surgically treated patients experienced a complication compared with 1 of 13 conservatively treated patients. Three previously conducted reviews concluded that surgical repair of Achilles tendon rupture was associated with the lowest rerupture rate (1–3). Nevertheless, the results of these previous reviews cannot simply be transferred to our findings, because the present analysis focused especially on the effect of weightbearing and used only recent randomized controlled trials. In the review by Soroceanu et al (19), 10 studies, including 826 patients, were analyzed. The pooled results showed that surgical repair significantly reduced the rerupture rate (RR 0.4, p ¼ .001) compared with nonsurgical treatment. However, the results of the stratified analysis showed that when early range of motion was practiced, surgical and nonsurgical treatment were equivalent regarding the rerupture rate (p ¼ .45). This suggests that surgical intervention did not contribute to a risk reduction if a rehabilitation protocol with early weightbearing was used. The focus in the review by Soroceanu et al (19) was on early range of motion, which is not the same as weightbearing. However, the threshold to discriminate between early and late range of motion was not reported (19). Wallace et al (20) followed up more than 900 patients from 1996 to 2008 and treated all patients with functional bracing and weightbearing within the fourth week. They found a surprisingly low rerupture rate of 2.8% (20). The rerupture rate in the early versus late weightbearing group was more or less the same, stratified by the treatment modality. Consequently, we found no evidence that early weightbearing is unsafe. One limitation of the present meta-analysis was the heterogeneity present when analyzing minor complications, mainly caused by the inclusion of 1 study (9). In that study, the complication rate in the nonoperatively treated group was greater than in the surgically treated group, in contrast to all the other studies. In that study, skinrelated problems occurring in the patients who had worn a brace were responsible for the high number of complications in the conservatively treated group. The patients were not allowed to remove the brace. If that study were excluded from our subgroup analysis, the RR would change from 3.54 to 8.96. Moreover, the difference in the minor complication rate between the operative and nonoperative patients in the early weightbearing group would reach significance (p ¼ .0008, I2 ¼ 0%). Another limitation was that the incidence of deep venous thrombosis (DVT) could not be accurately reported. In 1 study (21), all the patients underwent ultrasonography of the leg at 8 weeks postoperatively or after the beginning of bracing. A high number of (asymptomatic) DVTs was found in 32 of 95 screened patients; 14 of 49 surgically treated patients developed a DVT compared with 18 of 46 nonsurgically treated patients. The study reported that 10 of 32 patients had complaints. However, it was not stated how many DVTs were considered clinically relevant. Therefore, it was impracticable to combine these DVTs with those from the other studies. Thus, the number of DVTs from that study (21) was not included in the present analysis. Another point of concern for our study was the difference in the rehabilitation protocols of the included studies. Some studies had D.M. van der Eng et al. / The Journal of Foot & Ankle Surgery 52 (2013) 622–628 A Operative Conservative Study or Subgroup Events Total Events Total Weight 1.2.1 Start weight bearing before 4 weeks Costa 2006 Metz 2008 Möller 2001 Willits 2010 Subtotal (95% CI) 6 5 9 8 20 41 59 62 182 0 13 1 1 19 39 53 65 176 Risk Ratio M-H, Random, 95% CI 627 Risk Ratio M-H, Random, 95% CI 12.38 [0.75, 205.75] 0.37 [0.14, 0.93] 8.08 [1.06, 61.71] 8.39 [1.08, 65.12] 3.54 [0.40, 31.61] 14.5% 22.6% 17.9% 17.9% 72.9% 15 28 Total events Heterogeneity: Tau² = 3.96; Chi² = 17.12, df = 3 (P = 0.0007); I² = 82% Test for overall effect: Z = 1.13 (P = 0.26) 1.2.2 Start weight bearing after 4 weeks Keating 2011 Nilsson 2009 Twaddle 2007 Subtotal (95% CI) 1 4 0 37 49 22 108 0 0 0 39 48 23 110 13.0% 14.1% 27.1% 3.16 [0.13, 75.16] 8.82 [0.49, 159.51] Not estimable 5.53 [0.65, 46.88] 0 Total events 5 Heterogeneity: Tau² = 0.00; Chi² = 0.23, df = 1 (P = 0.63); I² = 0% Test for overall effect: Z = 1.57 (P = 0.12) 286 100.0% 290 Total (95% CI) 3.85 [0.72, 20.56] 15 Total events 33 Heterogeneity: Tau² = 3.00; Chi² = 19.15, df = 5 (P = 0.002); I² = 74% Test for overall effect: Z = 1.58 (P = 0.12) Test for subgroup differences: Chi² = 0.08, df = 1 (P = 0.78), I² = 0% B Operative Conservative Study or Subgroup Events Total Events Total Weight 1.3.1 Start weight bearing before 4 weeks Costa 2006 Metz 2008 Möller 2001 Willits 2010 Subtotal (95% CI) 2 4 1 3 20 41 59 62 182 0 2 1 2 19 39 53 65 176 7.8% 25.7% 9.1% 22.4% 65.0% 0.01 0.1 1 10 100 Favours operative Favours conservative Risk Ratio M-H, Random, 95% CI Risk Ratio M-H, Random, 95% CI 4.76 [0.24, 93.19] 1.90 [0.37, 9.81] 0.90 [0.06, 14.01] 1.57 [0.27, 9.10] 1.79 [0.64, 5.01] Total events 10 5 Heterogeneity: Tau² = 0.00; Chi² = 0.69, df = 3 (P = 0.88); I² = 0% Test for overall effect: Z = 1.11 (P = 0.27) 1.3.2 Start weight bearing after 4 weeks Keating 2011 Nilsson 2009 Twaddle 2007 Subtotal (95% CI) 2 4 0 37 49 22 108 2 0 2 39 48 23 110 19.0% 8.2% 7.8% 35.0% 1.05 [0.16, 7.10] 8.82 [0.49, 159.51] 0.21 [0.01, 4.12] 1.24 [0.19, 7.93] Total events 6 4 Heterogeneity: Tau² = 1.04; Chi² = 3.22, df = 2 (P = 0.20); I² = 38% Test for overall effect: Z = 0.22 (P = 0.82) Total (95% CI) 290 286 100.0% Total events 16 9 Heterogeneity: Tau² = 0.00; Chi² = 4.06, df = 6 (P = 0.67); I² = 0% Test for overall effect: Z = 1.05 (P = 0.29) Test for subgroup differences: Chi² = 0.12, df = 1 (P = 0.73), I² = 0% 1.56 [0.68, 3.59] 1 0.01 0.1 10 100 Favours operative Favours conservative Fig. 3. (A) Table and forest plot illustrating the number of minor complications. A subdivision in weightbearing before and after 4 weeks was made. (B) Table and Forest plot illustrating the number of major complications. A subdivision in weightbearing before and after 4 weeks was made. Chi2, chi-square; CI, confidence interval; df, degrees of freedom; M-H, MantelHaenszel. different protocols for the surgical and nonsurgical groups. No previously completed meta-analysis could answer the question of which protocol is the most effective and safe. This was mainly because of the small number of patients. Future randomized controlled trials should be of high methodologic rigor (concealment and blinding of outcome assessors and large patient numbers) and should contain clear operative protocols and similar rehabilitation protocols for the surgical and nonsurgical groups. The use of the same, validated instruments to measure the functional outcome should be encouraged. In conclusion, we found no difference in the rerupture rate between the surgically and nonsurgically treated patients followed by early weightbearing. The analysis of patients who started weightbearing after 4 weeks also showed no difference in the rerupture rate in the surgically versus conservatively treated patients. Concerning the similar rerupture rate in the surgical and nonsurgical groups, no rehabilitation protocol seemed superior for patients with acute Achilles tendon rupture. However, surgical treatment was associated with a twofold greater complication rate compared with conservative treatment. 628 D.M. van der Eng et al. / The Journal of Foot & Ankle Surgery 52 (2013) 622–628 Study or Subgroup Costa 2006 Keating 2011 Metz 2008 Möller 2001 Nilsson 2009 Twaddle 2007 Willits 2010 Total (95% CI) Operative Conservative Events Total Events Total Weight 19 10.9% 0 20 8 39 16.7% 2 37 3 39 23.2% 15 41 9 53 18.4% 2 59 10 48 10.7% 0 49 8 23 0 22 0 65 20.0% 3 62 11 290 286 100.0% 22 49 Total events Heterogeneity: Tau² = 1.56; Chi² = 19.52, df = 5 (P = 0.002); I² = 74% Test for overall effect: Z = 1.76 (P = 0.08) Risk Ratio M-H, Random, 95% CI Risk Ratio M-H, Random, 95% CI 16.19 [1.00, 262.45] 1.58 [0.28, 8.93] 0.57 [0.28, 1.15] 4.49 [1.03, 19.58] 16.66 [0.99, 280.85] Not estimable 3.84 [1.13, 13.13] 3.00 [0.88, 10.21] 0.01 1 0.1 10 100 Favours operative Favours conservative Fig. 4. Table and Forest plot illustrating the minor and major complications and the subgroups together. Chi2, chi-square; CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel. Acknowledgment The authors would like to thank N. Keulen, MD, for her contribution during the initial search, the assessment of the abstracts, studies, and quality assessment, and data extraction. References 1. Khan RJ, Fick D, Keogh A, Crawford J, Brammar T, Parker M. Treatment of acute Achilles tendon ruptures. A meta-analysis of randomized, controlled trials. J Bone Joint Surg Am 87:2202–2210, 2005. 2. Khan RJ, Carey Smith RL. Surgical interventions for treating acute Achilles tendon ruptures. Cochrane Database Syst Rev 9:CD003674, 2010. 3. Bhandari M, Guyatt GH, Siddiqui F, Morrow F, Busse J, Leighton RK, Sprague S, Schemitsch EH. Treatment of acute Achilles tendon ruptures: a systematic overview and meta-analysis. Clin Orthop Relat Res 400:190–200, 2002. 4. Wilkins R, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. Am J Sports Med 40:2154, 2012. 5. Andersson T, Eliasson P, Aspenberg P. Tissue memory in healing tendons: short loading episodes stimulate healing. J Appl Physiol 107:417–421, 2009. 6. Enwemeka CS, Spielholz NI, Nelson AJ. The effect of early functional activities on experimentally tenotomized Achilles tendons in rats. Am J Phys Med Rehabil 67:264–269, 1988. 7. Krapf D, Kaipel M, Majewski M. Structural and biomechanical characteristics after early mobilization in an Achilles tendon rupture model: operative versus nonoperative treatment. Orthopaedics 35:1383–1388, 2012. 8. Palmes D, Spiegel HU, Schneider TO, Langer M, Stratmann U, Budny T, Probst A. Achilles tendon healing: long-term biomechanical effects of postoperative mobilization and immobilization in a new mouse model. J Orthop Res 20:939–946, 2002. 9. Metz R, Verleisdonk EJ, van der Heijden GJ, Clevers GJ, Hammacher ER, Verhofstad MH, van der Werken C. Acute Achilles tendon rupture: minimally invasive surgery versus nonoperative treatment with immediate full weight bearingda randomized controlled trial. Am J Sports Med 36:1688–1694, 2008. €m a € la €inen M, Leppilahti J. Early functional treatment 10. Kangas J, Pajala A, Siira P, Ha versus early immobilization in tension of the musculotendinous unit after Achilles rupture repair: a prospective, randomized, clinical study. J Trauma 54:1171–1180, 2003. LA, Durand DC, Jomha NM. The influence of early 11. Suchak AA, Bostick GP, Beaupre weight-bearing compared with non-weight-bearing after surgical repair of the Achilles tendon. J Bone Joint Surg Am 90:1876–1883, 2008. 12. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097, 2009. 13. Costa ML, MacMillan K, Halliday D, Chester R, Shepstone L, Robinson AH, Donell ST. Randomised controlled trials of immediate weight-bearing mobilisation for rupture of the tendo Achillis. J Bone Joint Surg Br 88:69–77, 2006. 14. Keating JF, Will EM. Operative versus non-operative treatment of acute rupture of tendo Achillis: a prospective randomised evaluation of functional outcome. J Bone Joint Surg Br 93:1071–1078, 2011. € ller M, Movin T, Granhed H, Lind K, Faxe n E, Karlsson J. Acute rupture of tendon 15. Mo Achillis: a prospective randomised study of comparison between surgical and nonsurgical treatment. J Bone Joint Surg Br 83:843–848, 2001. R, Faxe n E, Olsson N, Eriksson BI, 16. Nilsson-Helander K, Silbernagel KG, Thomee Karlsson J. Acute Achilles tendon rupture: a randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am J Sports Med 38:2186–2193, 2010. 17. Twaddle BC, Poon P. Early motion for Achilles tendon ruptures: is surgery important? A randomized, prospective study. Am J Sports Med 35:2033–2038, 2007. 18. Willits K, Amendola A, Bryant D, Mohtadi NG, Giffin JR, Fowler P, Kean CO, Kirkley A. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am 92:2767–2775, 2010. 19. Soroceanu A, Sidhwa F, Aarabi S, Kaufman A, Glazebrook M. Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. J Bone Joint Surg Am 94:2136–2143, 2012. 20. Wallace RG, Heyes GJ, Michael ALR. The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of rerupture. J Bone Joint Surg Br 93:1362–1366, 2011. 21. Nilsson-Helander K, Thurin A, Karlsson J, Eriksson BI. High incidence of deep venous thrombosis after Achilles tendon rupture: a prospective study. Knee Surg Sports Traumatol Arthrosc 17:1234–1238, 2009.