Tees Valley Treatment Centre Quality Account

Tees Valley Treatment
Centre
Quality Account
2014/15
Contents
Welcome to Ramsay Health Care UK
Introduction to our Quality Account
PART 1 – STATEMENT ON QUALITY
1.1 Statement from the General Manager
1.2 Hospital accountability statement
PART 2
2.1 Priorities for Improvement
2.1.1 Review of clinical priorities 2014/15 (looking back)
2.1.2 Clinical Priorities for 2015/16 (looking forward) 12 - 14
2.2
Mandatory statements relating to the quality of NHS services provided
2.2.1 Review of Services 15 - 16
2.2.2 Participation in Clinical Audit
2.2.3 Participation in Research
2.2.4 Goals agreed with Commissioners
2.2.5 Statement from the Care Quality Commission
2.2.6 Statement on Data Quality
2.2.7 Stakeholders views on 2015/16 Quality Accounts
PART 3
– REVIEW OF QUALITY PERFORMANCE
3.1 The Core Quality Account indicators
3.2 Patient Safety
3.3 Clinical Effectiveness
3.4 Patient Experience
3.5 Case Study
Appendix 1 – Services Covered by this Quality Account
Appendix 2 – Clinical Audits
16 - 17
17
17
17
18
19
20 - 25
25 - 28
28 - 29
30 - 31
32
33
34
6
4
5
8
10
10 - 12
Welcome to Ramsay Health Care UK
Tees Valley Treatment Centre is part of the Ramsay Health Care
Group
The Ramsay Health Care Group, was established in 1964 and has grown to become a global hospital group operating over 100 hospitals and day surgery facilities across Australia, the United Kingdom, Indonesia and France. Within the
UK, Ramsay Health Care is one of the leading providers of independent hospital services in England, with a network of 31 acute hospitals.
We are also the largest private provider of surgical and diagnostics services to the NHS in the UK. Through a variety of national and local contracts we deliver
1,000s of NHS patient episodes of care each month working seamlessly with other healthcare providers in the locality including GPs and Clinical
Commissioning Groups.
The provision of high quality patient care is and will always be the highest priority of Ramsay Health Care UK. Of course our team of clinical staff and consultants are very much at the forefront of achieving this but there is also very much an organisation wide commitment to ensure that we continue to improve out outcomes every day, week, month and year.
Delivering clinical excellence depends on everyone in the organisation. Clinical excellence cannot be the responsibility of just a few, it takes all of us to be responsible and accountable for our performance in the various roles we all play.
Having an organisational culture that puts the patient at the centre of everything we do is key to ensuring we enable everyone to perform at their peak to attain great outcomes.
Whilst I firmly I believe that across Ramsay we nurture the teamwork and professionalism on which excellence in clinical practice depends, we will continue to strive to get ever better.
I am very proud of our long standing and major provider of healthcare services across the world and of our Ramsay very strong track record as a safe and responsible healthcare provider. It gives us pleasure to share our results with you.
Mark Page
Chief Executive officer Ramsay Health Care UK
Quality Accounts 2014/15
Page 5 of 36
Introduction to our Quality Account
This Quality Account is Tees Valley Treatment Centre’s annual report to the public and other stakeholders about the quality of the services we provide. It presents our achievements in terms of clinical excellence, effectiveness, safety and patient experience and demonstrates that our managers, clinicians and staff are all committed to providing continuous, evidence based, quality care to those people we treat. It will also show that we regularly scrutinise every service we provide with a view to improving it and ensuring that our patient’s treatment outcomes are the best they can be. It will give a balanced view of what we are good at and what we need to improve on.
Our first Quality Account in 2010 was developed by our Corporate Office and summarised and reviewed quality activities across every hospital and treatment centre within the Ramsay Health Care UK. It was recognised that this didn’t provide enough in depth information for the public and commissioners about the quality of services within each individual hospital and how this relates to the local community it serves. Therefore, each site within the Ramsay Group now develops its own Quality Account, which includes some Group wide initiatives, but also describes the many excellent local achievements and quality plans that we would like to share.
Quality Accounts 2014/15
Page 6 of 36
Part 1
1.1 Statement on quality from the General
Manager
.
“Tees Valley Treatment Centre is committed to being a leading provider of outpatient, diagnostic and day case services by delivering high quality outcomes and an excellent patient experience.”
I am delighted to introduce our Quality Account for 2014/15 which demonstrates our commitment to delivering high quality care. The report focuses upon our performance over the last year and describes our priorities for 2015/16.
Our approach to quality is having in place a robust framework which enables us to monitor and measure outcomes and experience, using this information to drive further improvement in patient safety, patient experience and clinical outcomes.
Our team is at the forefront of delivering a quality service
. “ People caring for people” remains our philosophy and we are committed to training and developing our workforce and ensuring attitudes and behaviour aligned to our values.
2014/15 has been a busy and successful year with a wider number of GPs referring to our services and an increased number of patients choosing to access our treatment centre. Our mission remains, to be expert in delivering elective day case services to patients in our local community and beyond, delivering services we would be happy to receive ourselves. We have had our commitment to quality recognised this year in a number of key achievements:
The number of patients who have taken time to enter reviews on NHS choices and it is particularly pleasing to see that the treatment centre has an overall 4 star rating.
In addition, all of our patient feedback mechanisms show consistently high satisfaction
We meet all CQC standards
Only nine formal complaints received in the last 12 months
Maintaining Joint Advisory Group (JAG) accreditation for endoscopy services
Quality Accounts 2014/15
Page 7 of 36
Despite these accolades we are not complacent and our priorities for 2015/16 are focused upon ensuring continuous improvement, creating services centred around the patient, getting it right first time and putting patient safety at the heart of everything we do.
Donna Thornton
General Manager, Tees Valley Treatment Centre
Quality Accounts 2014/15
Page 8 of 36
1.2 Hospital Accountability Statement
To the best of my knowledge, as requested by the regulations governing the publication of this document, the information in this report is accurate .
Donna Thornton
General Manager
Tees Valley Treatment Centre
Ramsay Health Care UK
This report has been reviewed by:
Peter Hodgkinson, Medical Advisory Group Chair
Alex Clason, Clinical Governance Committee Chair
Helen White, Regional Director
South Tees CCG, Lead Commissioner
Quality Accounts 2014/15
Page 9 of 36
Welcome to Tees Valley Treatment Centre
Tees Valley Treatment Centre, was opened in 2007 and is a modern, purposebuilt unit designed for the diagnosis, assessment and treatment of conditions on a day case basis for adults aged 18 years and over. The treatment centre is a single level building comprising of a modern and airy reception area, an outpatient unit with a suite of consulting rooms and a surgical unit housing two theatres and dedicated recovery areas. Located within the One Life facility in
Middlesbrough there is free car parking, good public transport links and easy access to main road networks.
Tees Valley Treatment Centre currently provides NHS services for the following specialties: dermatology, GI endoscopy, general surgery, oral surgery, orthopaedics, plastic surgery, gynaecology and urology. Patients who self pay or have private medical insurance are seen under our Premium Care scheme for the following specialties: dermatology, GI endoscopy, general surgery, oral surgery, orthopaedics, plastic surgery, gynaecology and urology.
South Tees Clinical Commissioning Group were our lead commissioner of NHS
Services for 2014/15, on behalf of neighbouring clinical commissioning groups, with regular service review meetings held to discuss performance. Patients were referred and travelled from Middlesbrough, Redcar, Stockton, Darlington,
Hartlepool, County Durham and North Yorkshire.
Referral to the treatment centre for NHS services is direct from GP via Choose and Book and we have dedicated Choose and Book Co-ordinators and GP
Liaison team to facilitate the referral process.
This year saw over 6,000 patient procedures at Tees Valley Treatment Centre with a breakdown of work being 99% NHS patients and 1% private patients. In terms of workforce there are 38 members of staff employed at Tees Valley
Treatment Centre, a mix of full time and part time, of which 64% are clinical posts and 36% support staff.
Quality Accounts 2014/15
Page 10 of 36
Part 2
2.1 Quality priorities for 2013/2014
Plan for 2014/15
On an annual cycle, Tees Valley Treatment Centre develops an operational plan to set objectives for the year ahead.
We have a clear commitment to our private patients as well as working in partnership with the NHS ensuring that those services commissioned to us, result in safe, quality treatment for all NHS patients whilst they are in our care. We constantly strive to improve clinical safety and standards by a systematic process of governance including audit and feedback from all those experiencing our services.
To meet these aims, we have various initiatives on going at any one time. The priorities are determined by the Senior Management Team taking into account patient feedback, audit results, national guidance, and the recommendations from various hospital committees which represent all professional and management levels.
Most importantly, we believe our priorities must drive patient safety, clinical effectiveness and improve the experience of all people visiting our treatment centre.
Priorities for improvement
2.1.1 A review of clinical priorities 2014/15 (looking back)
Surgical safety checklist -
There have been no ‘Never Events’ at Tees Valley
Treatment Centre in the period and audit of compliance maintains a key focus
Quality Accounts 2014/15
Page 11 of 36
with qquarterly audits of the WHO surgical safety checklist continued with 100% compliance demonstrated. A WHO training DVD was produced by Ramsay and this was shared with all clinical and medical staff demonstrating a gold standard approach to the process.
VTE assessment – We audited our compliance and results were submitted to
UNIFY and national health data base. The results confirm that more than 98% of patients were risk assessed where indicated.
However additional quarterly audits of ten random patient records showed some poor compliance in accuracy in documentation by medical staff with scores ranging from 81% to 97%.
Consultants were identified and additional training given with improvement targets set. Audit results were reviewed at Clinical Governance and Medical Advisory
Committees with poor practice identified and action plans for improvement supported by the committee chairs. Compliance continues to be a focus both at a local and national level with the Group Medical Director leading expectations in terms of the clinicians across the Ramsay Group.
Staffing
– An electronic rostering tool ‘Allocate’ has been in use since February
2014 and supports an annualised hours approach to managing staffing hours allowing flexibility for both the service and staff. The staff satisfaction survey is completed biannually and a staff engagement group was formed to review the results from the end of 2013. Overall feedback was very positive with staff endorsing Tees Valley Treatment Centre as a great place to work. An action plan was developed and included the introduction of an improved induction program for new staff, regular team briefs by department heads and a social events calendar to encourage team building across the hospital. Staff have continued to utilise the Ramsay Academy to develop skills and knowledge in their field. We have increased the number of Health Care Assistant (HCA) within the endoscopy department with HCAs completing competency assessments in decontamination and day case pathways. We have also introduced an HCA apprentice role into theatre. The Team Leaders have all completed a heads of department development program specifically tailored to identified learning needs; this was completed over a six month period with excellent feedback.
Clinical effectiveness
Meeting Endoscopy Standards
– Following successful JAG (Joint Advisory
Group on Gastrointestinal Endoscopy) accreditation at the beginning of 2014 annual submission to GRS (Global Rating Score) was completed at the end of
March 2015 with 99% of standards at level A and the remaining 1% at level B.
Quality Accounts 2014/15
Page 12 of 36
This tool enables us to assess how well we provide a patient-centered service.
Demonstrating compliance against the four domains:
clinical quality
quality of patient experience
workforce
training
We hold quarterly endoscopy user group meetings with medical and clinical representation and annual patient representation to ensure our patient’s views on the service are heard.
Patient experience – informing patient choice
Patient satisfaction survey – We continue to encourage patients to provide feedback using our web based satisfaction survey in a bid to improve our average response rate of 37%. Overall satisfaction rates remain high at 95.3% with 95% of patients likely to recommend the treatment centre to friends and family. Patients who choose to give individual feedback do so via a ‘hot alerts’ section in the questionnaire and this feedback has been reviewed by the General Manger and
Matron as well as the lead CCG and action taken where there are areas identified for improvement.
All ‘hot alerts’ have been shared with the whole team along with a monthly patient satisfaction dashboard. We continue to monitor posts on NHS choices and are pleased to have attained a five star rating.
Friends and Family Test - This national CQUIN indicator was met with early implementation of F&F in outpatients and day case departments achieved ahead of the target date of 31 st
October 2014. Patients have been invited to complete a paper questionnaire at the end of their hospital visit and many have included additional comments on their experience. A monthly report is generated and shared with all staff and where individual team members are named in a patient comment a customer service nomination is made in line with the customer service excellence program. Our response rates have been low and an action plan to improve by modifying the process for requesting and encouraging patients to complete is ongoing with both clinical and administration teams. The average recommendation rate for day case is 95% and 86% for outpatients. The lower score for outpatients is affected by low participation rates.
Patient reported outcome measures studies (PROMS) – We continued to monitor patient response rates as part of a local CQUIN indicator with a graduated quarterly target to achieve 70% compliance by March 2015. We have exceeded this target each quarter with quarterly response rates ranging from 78%
Quality Accounts 2014/15
Page 13 of 36
to 100%. This improvement on previous years is as a result of the surgeon ensuring patients are fully informed and inviting patients to take part in the survey by completing a questionnaire prior to their surgery.
Information Security – Tees Valley Treatment Centre achieved the information security accreditation ISO 27001in August 2014. The process of raising the importance of data protection and information security has been successful and fully embraced by our staff.
2.1.2 Clinical Priorities for 2015/16 (looking forward)
For 2015-16 Tees Valley Treatment Centre will strive to continue delivering a safe, high quality experience for all patients. In particular we will focus on:
Patient Safety
VTE risk assessment
– We will continue to audit our compliance and submit our results to UNIFY and national health data base. Additional quarterly audits of compliance with accuracy of documentation by medical staff will be a focus to ensure improvements are made with an improvement target set of 95% compliance.
Care of the deteriorating patient
– Audit of compliance with Ramsay policy identified some training needs in September 2014 which were addressed with all registered staff completing AIM training and additional training for HCAs in recognition of the deteriorating patient and documentation requirements. A further audit in March 2015 identified some examples of poor documentation in completion of the EWS chart. Additional training and supervision of nonregistered staff has been put in place and we plan to carry out quarterly audits of compliance in the next year to ensure results exceed 90%.
Staff training – We will continue to ensure good levels of compliance with mandatory training to ensure that patients are cared for by well trained, competent staff. Competency assessments will be completed in all clinical areas for registered and non-registered staff identifying training needs across the unit and encouraging staff development opportunities.
Clinical effectiveness
We will be recruiting a Quality Improvement Lead in the second half of 2015 who will ensure all audits are undertaken in a timely manner and who will implement new systems where the requirement arises to improve levels in both participation
Quality Accounts 2014/15
Page 14 of 36
and results. We will be able to monitor our improvement using statistical evidence. This priority will support improvement within the domains of patient safety and clinical effectiveness.
Progress against all of these priorities will be monitored by the Senior
Management Team and reported to our local Clinical Governance and Medical
Advisory Committees.
Patient Experience
We will continue to work hard to ensure that those who use our service have a positive experience. We will monitor this through ratings in the patient satisfaction survey and national ‘Friends and Family’ test for both day case and outpatient services. We will focus on improving response rates in both surveys and maintaining the overall level of satisfaction at greater than 90% as well as achieving recommendation rates of over 90%.
Quality Accounts 2014/15
Page 15 of 36
2.2 Mandatory Statements
The following section contains the mandatory statements common to all Quality
Accounts as required by the regulations set out by the Department of Health.
2.2.1 Review of Services
During 2014/15 Tees Valley Treatment Centre provided NHS services across eight specialties.
Tees Valley Treatment Centre has reviewed all the data available to them on the quality of care in all of these NHS services.
The income generated by the NHS services reviewed 1 April 2014 to 31 st
March
15 represents 100 per cent of the total income generated from the provision of
NHS services by Tees Valley Treatment Centre for 1 April 2014 to 31 st
March 15.
Ramsay uses a balanced scorecard approach to give an overview of audit results across the critical areas of patient care. The indicators on the Ramsay scorecard are reviewed each year. The scorecard is reviewed each quarter by the hospitals senior managers together with Regional and Corporate Senior Managers and
Directors. The balanced scorecard approach has been an extremely successful tool in helping us benchmark against other hospitals and identifying key areas for improvement.
In the period for 2014/15, the indicators on the scorecard which affect patient safety and quality were:
Human Resource
Staff Cost % Net Revenue
HCA Hours as % of Total Nursing
13.5%
28%
Agency Cost as % of Total Staff Cost 2.5%
Admitted Care Hours Worked PPD 4.83
Staff Turnover
Sickness
Lost Time
Appraisal %
Mandatory Training %
34.6%
5.71%
21.2%
90%
86%
Quality Accounts 2014/15
Page 16 of 36
Number of Significant Staff Injuries 2013-14 score
No significant staff
Patient injuries
Formal Complaints in year
Patient Satisfaction Score 95.3%
Significant Clinical Events
Quality
Readmission per 1000 Admissions
Workplace Health & Safety Score
1
0.003%
96%
2.2.2 Participation in clinical audit
The national clinical audits and national confidential enquiries that Tees Valley
Treatment Centre participated in, and for which data collection was completed during 1 April 2014 to 31 st
March 2015, are listed below alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry.
Name of audit / Clinical Outcome
Review Programme
% cases submitted
Small volumes
Elective surgery (National PROMs Programme)
The reports of the national clinical audit from 1 April 2014 to 31 st
March 2015 were reviewed by the Clinical Governance Committee and Tees Valley Treatment
Centre has worked to improve participation rates for preoperative surveys for inguinal hernia repair by consultant engagement with patients preoperatively.
Local Audits
The reports of over 70 local clinical audits from 1 April 2014 to 31 st
March 2015 were reviewed by the Clinical Governance Committee and Tees Valley Treatment
Centre ensures action plans are written with clear time frames for improvement and responsibilities assigned.
Quality Accounts 2014/15
Page 17 of 36
Over all good compliance is demonstrated and action plans are completed to ensure improvements are made. Our focus for 2015/16 is to further improve record keeping in relation to VTE compliance and compliance with documentation in EWS charts in the management of the deteriorating patient.
The clinical audit schedule can be found in Appendix 2.
2.2.3 Participation in Research
There were no patients recruited during 2014/15 to participate in research approved by a research ethics committee.
2.2.4 Goals agreed with our Commissioners using the CQUIN
(Commissioning for Quality and Innovation) Framework
A proportion of
Tees Valley Treatment Centre’s income from 1 April 2014 to 31 st
March 2015 was conditional on achieving quality improvement and innovation goals agreed. Tees Valley Treatment Centre and any person or body they entered into a contract, agreement or arrangement with for the provision of NHS services, through the Commissioning for Quality and Innovation payment framework.
2.2.5 Statements from the Care Quality Commission (CQC)
Tees Valley Treatment Centre is required to register with the Care Quality
Commission and its current registration status on 31 st
March 2015 is registered without conditions.
Tees Valley Treatment Centre has not participated in any special reviews or investigations by the CQC during the reporting period.
Quality Accounts 2014/15
Page 18 of 36
2.2.6 Data Quality
Tees Valley Treatment Centre works hard to ensure accurate data quality is at the heart of everything we do, evidenced by excellent SUS submission rates.
Where applicable, using findings from the internal audit programme, the hospital works to develop data capture and validation methods, ensuring continuous improvement in quality standards.
NHS Number and General Medical Practice Code Validity
The Ramsay Group submitted records during 2014/15 to the Secondary Users
Service for inclusion in the Hospital Episode Statistics which are included in the latest published data. The percentage of records in the published data included:
The patie nt’s valid NHS number:
99.97% for admitted patient care;
99.96% for outpatient care; and
Accident and emergency care N/A (as not undertaken at Ramsay hospitals).
The General Medical Practice Code:
100% for admitted patient care;
100% for outpatient care; and
Accident and emergency care N/A (as not undertaken at Ramsay hospitals).
Information Governance Toolkit attainment levels
Ramsay Group Information Governance Assessment Report score overall for
2014/5 was 75% and was graded ‘green’ (satisfactory).
This information is publicly available on the DH Information Governance Toolkit website at: https://www.igt.hscic.gov.uk
Statement on relevance of Data Quality and your actions to improve your
Data Quality
Clinical coding error rate
A clinical coding audit was completed in February 2015 with the following findings
Primary
Diagnosis
100%
Secondary
Diagnosis
100%
Primary
Procedure
100%
Secondary
Procedure
100%
Quality Accounts 2014/15
Page 19 of 36
2.2.7 Stakeholders views on 2013/14 Quality Account
Reviewed by South Tees CCG but comments not received prior publication
Quality Accounts 2014/15
Page 20 of 36
Part 3: Review of quality performance 2013/2014
Statements of quality delivery
Review of quality performance 1st April 2014 - 31st March 2015
Introduction
This publication marks the sixth successive year since the first edition of Ramsay
Quality Accounts. Through each year, month on month, we analyse our performance on many levels, we reflect on the valuable feedback we receive from our patients about the outcomes of their treatment and also reflect on professional opinion received from our doctors, our clinical staff, regulators and commissioners. We listen where concerns or suggestions have been raised and, in this account, we have set out our track record as well as our plan for more improvements in the coming year. This is a discipline we vigorously support, always driving this cycle of continuous improvement in our hospitals and addressing public concern about standards in healthcare, be these about our commitments to providing compassionate patient care, assurance about patient privacy and dignity, hospital safety and good outcomes of treatment. We believe in being open and honest where outcomes and experience fail to meet patient expectation so we take action, learn, improve and implement the change and deliver great care and optimum experience for our patients.”
Vivienne Heckford
Director of Clinical Services
Ramsay Health Care UK
Ramsay Clinical Governance Framework 2015
The aim of clinical governance is to ensure that Ramsay develop ways of working which assure that the quality of patient care is central to the business of the organisation.
The emphasis is on providing an environment and culture to support continuous clinical quality improvement so that patients receive safe and effective care, clinicians are enabled to provide that care and the organisation can satisfy itself that we are doing the right things in the right way.
It is important that Clinical Governance is integrated into other governance systems in the organisation and should not be seen as a “stand-alone” activity. All
Quality Accounts 2014/15
Page 21 of 36
management systems, clinical, financial, estates etc, are inter-dependent with actions in one area impacting on others.
Several models have been devised to include all the elements of Clinical
Governance to provide a framework for ensuring that it is embedded, implemented and can be monitored in an organisation. In developing this framework for Ramsay Health Care UK we have gone back to the original Scally and Donaldson paper (1998) as we believe that it is a model that allows coverage and inclusion of all the necessary strategies, policies, systems and processes for effective Clinical Governance. The domains of this model are:
• Infrastructure
• Culture
• Quality methods
• Poor performance
• Risk avoidance
• Coherence
Ramsay Health Care Clinical Governance Framework
Quality Accounts 2014/15
Page 22 of 36
National Guidance
Ramsay also complies with the recommendations contained in technology appraisals issued by the National Institute for Health and Clinical Excellence
(NICE) and Safety Alerts as issued by the NHS Commissioning Board Special
Health Authority.
Ramsay has systems in place for scrutinising all national clinical guidance and selecting those that are applicable to our business and thereafter monitoring their implementation.
3.1 The Core Quality Account indicators
National Mortality Rates:
Period Best
Jan13-Dec13 RKE 0.62
Apr13-
Mar14
RKE 0.54
Tees Valley Treatment Centre:
Period Tees Valley
2013/14 NVC35 0
RXL
Worst
1.18
RBT 1.20
Average
Eng
Eng
1
1
2014/15 NVC35 0
Tees Valley Treatment Centre considers that this data is as described, we have had no reported deaths.
National PROMs: Hernia repair
Period Best Worst
Apr13 -
Mar14
Apr14 -
Sep14
NT415 0.139 NVC11 0.008 Eng
RXR 0.125 Several 0.009 Eng
Tees Valley Treatment Centre
Average
0.085
0.081
Period Tees Valley
Apr13 -
Mar14
Apr14 -
Sep14
NVC35
NVC35
0.077
*
Tees Valley Treatment Centre considers that this data is as described as we have low volumes of patients admitted for inguinal hernia repair.
Quality Accounts 2014/15
Page 23 of 36
National PROMs Varicose veins
Period Best Worst
Apr13 -
Mar14
Apr14 -
Sep14
RTH
RYJ
11.292 NT350 -16.849 Eng
-4.567
Tees Valley Treatment Centre
RWA -16.762 Eng
Average
-8.698
-9.479
Period
Apr13 -
Mar14
Apr14 -
Sep14
Tees Valley
NVC35
NVC35
*
*
Tees Valley Treatment Centre considers that this data is as described as we have low volumes of patients admitted for varicose vein surgery, as the policy around procedures of limited value are followed.
National Readmissions
Period Best Worst Average
2010/11 Multiple 0.0 5P5 22.76
41.65 2011/12 Multiple 0.0 5NL
Tees Valley Treatment Centre
Period Tees Valley
Eng
Eng
11.43
11.45
2010/11
14/15 Q2
NVC35
Several 100%
0
2011/12 NVC35 0
Tees Valley Treatment Centre considers this data to be incomplete compared to
SUS readmission reports. This is because we are not always notified of a readmission into another facility.
National VTE assessment
Period Best Worst Average
RNL 86.4% Eng 96.2%
96.0% 14/15 Q3 Several 100% NT322 85.1% Eng
Tees Valley Treatment Centre
Period Tees Valley
14/15 Q2 NVC35 99.9%
14/15 Q3 NVC35 100.0%
Tees Valley Treatment Centre considers that this data is as described. We consistently maintain compliance above the national average.
Quality Accounts 2014/15
Page 24 of 36
National C Difficile rate
Period
2012/13
Best
Several
Worst
0 RVW 30.8
32.5 2013/14 Several 0 RMP
Tees Valley Treatment Centre
Period Tees Valley
2012/13 NVC35 0.0
Eng
Average
17.4
Eng 14.7
2013/14 NVC35 0.0
Tees Valley Treatment Centre considers that this data is as described as there have been no reported cases of C Difficile and intends to maintain this rate by ensuring robust infection control measures are in place.
National SUI’s Severity level 1
Best Worst Average Period
Oct 13 - Mar
14
Apr - Sep 14
RBD
Several
0 R1F
0 RBZ
3.72
1.09
Eng
Eng
0.43
0.17
Tees Valley Treatment Centre
Period
Oct13-
Mar14
Apr-Sep14
Tees Valley
NVC35
NVC35
0.00
0.00
Tees Valley Treatment Centre considers that this data is as described, there have been no level 1 severity incidents reported. Tees Valley Treatment Centre intends to maintain this rate by ensuring an effective clinical governance framework.
3.2 Patient safety
We are a progressive hospital and focussed on stretching our performance every year and in all performance respects, and certainly in regards to our track record for patient safety.
Risks to patient safety come to light through a number of routes including routine audit, complaints, litigation, adverse incident reporting and raising concerns but more routinely from tracking trends in performance indicators.
Quality Accounts 2014/15
Page 25 of 36
3.2.1 Infection prevention and control
Tees Valley Treatment Centre has a very low rate of hospital acquired infection and has had no reported MRSA Bacteraemia in the past 5 years.
We comply with mandatory reporting of all Alert organisms including
MSSA/MRSA Bacteraemia and Clostridium Difficile infections with a programme to reduce incidents year on year.
Infection Prevention and Control management is very active within our hospital.
An annual strategy is developed by a corporate level Infection Prevention and
Control (IPC) Committee and group policy is revised and re-deployed every two years. Our IPC programmes are designed to bring about improvements in performance and in practice year on year.
A network of specialist nurses and infection control link nurses operate across the
Ramsay organisation to support good networking and clinical practice.
Programmes and activities within our hospital include:
The infection control link nurse has provided training in hand hygiene to all staff and completes a hand hygiene training session during the staff induction day for all new staff.
The consultant microbiologist has provided training sessions for the infection control link nurse on a number of subjects including blood borne viruses and
Carbapenamase-producing Enterobacteriaceae (CPE) to allow dissemination of knowledge to the wider clinical team.
Our annual hand hygiene awareness day was held in May and was lead by the infection control link nurse and this involved staff and patients visiting an information stand on the ward. Demonstrations were given and patients and staff were given individual hand hygiene gel dispensers for their own use.
Observational hand hygiene audits were undertaken by the Consultant
Microbiologist and Infection Control Link Nurse resulting in additional gel dispensers being placed in the unit. A poster campaign targeting staff to ‘gel in and gel out’ was successful in increasing patient satisfaction scores in questions relating to staff hand hygiene but further improvements targets have been set.
Quality Accounts 2014/15
Page 26 of 36
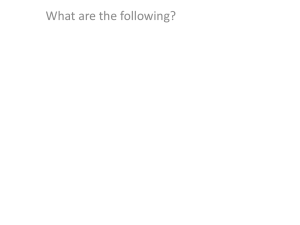
Infection Rates
0.5
0.45
0.4
0.35
0.3
0.25
0.2
0.15
0.1
0.05
0
2012/13 2013/14
Tees Valley Treatment Centre
2014/15
The above graph shows a reduction in infection rates on the previous year with the actual numbers remaining very low. The infection control committee has demonstrated improved reporting and investigating of potential infections.
Patients presenting with signs of an infection are logged on our reporting system and is reviewed by the infection control link nurse and a root cause analysis completed to determine any possible trends, results are presented at our quarterly infection control committee meetings. There have been no trends identified in the period.
3.2.2 Cleanliness and hospital hygiene
Assessments of safe healthcare environments also include P atientL ed
A ssessments of the C are E nvironment ( PLACE )
PLACE assessments occur annually at Tees Valley Treatment Centre, providing us with a patient’s eye view of the buildings and facilities, giving us a clear picture of how the people who use our hospital see it and how it can be improved. The main purpose of a PLACE assessment is to get the patient view.
2014 PLACE results:
Cleanliness – 93.7%
Condition, Appearance and Maintenance – 95.14%
Privacy, Dignity and Wellbeing – 67.5%%
An action plan was completed, as a day case facility patients do not have access to TV radio or internet this reflected a low score for privacy and dignity. The
Quality Accounts 2014/15
Page 27 of 36
patient assessors on the day did not reflect any concerns in terms of privacy and dignity and we determine that this element is not effectively assessed or scored using the current tool. It is pleasing to see the maintenance programme introduced following the 2013 assessment has had a positive impact on the condition and maintenance of the facilities. High level dust identified was addressed on the day and an improvement plan initiated with the housekeeping team.
3.2.3 Safety in the workplace
Safety hazards in hospitals are diverse ranging from the risk of slip, trip or fall to incidents around sharps and needles. As a result, ensuring our staff have high awareness of safety has been a foundation for our overall risk management programme and this awareness then naturally extends to safeguarding patient safety. Our record in workplace safety as illustrated by Accidents per 1000
Admissions demonstrates the results of safety training and local safety initiatives.
Effective and ongoing communication of key safety messages is important in healthcare. Multiple updates relating to drugs and equipment are received every month and these are sent in a timely way via an electronic system called the
Ramsay Central Alert System (CAS). Safety alerts, medicine / device recalls and new and revised policies are cascaded in this way to our General Manager which ensures we keep up to date with all safety issues.
In addition to mandatory training the Health and Safety Coordinator has coordinated sharps awareness programmes throughout the year ensuring the use of sharps safe devices where these are available. There has also been training on waste management ensuring the correct segregation of waste taking into account the effect on the environment and raising staff awareness on this issue.
3.3 Clinical effectiveness
Tees Valley Treatment Centre has a Clinical Governance committee that meet regularly through the year to monitor quality and effectiveness of care. Clinical incidents, patient and staff feedback are systematically reviewed to determine any trend that requires further analysis or investigation. More importantly, recommendations for action and improvement are presented to hospital management and medical advisory committees to ensure results are visible and tied into actions required by the organisation as a whole.
Quality Accounts 2014/15
Page 28 of 36
3.3.1 Return to theatre
Ramsay is treating significantly higher numbers of patients every year as our services grow. The majority of our patients undergo planned surgical procedures and so monitoring numbers of patients that require a return to theatre for supplementary treatment is an important measure. Every surgical intervention carries a risk of complication so some incidence of returns to theatre is normal.
The value of the measurement is to detect trends that emerge in relation to a specific operation or specific surgical team. Ramsay’s rate of return is very low consistent with our track record of successful clinical outcomes.
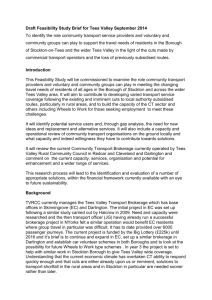
Return to Theatre Score
0.25
0.2
0.15
0.1
0.05
0
2012/13 2013/14
Tees Valley Treatment Centre
2014/15
Tees Valley Treatment Centre continues to have a very low return to theatre rate as a percentage of overall admissions. There were no trends identified and the rate remains below the national average and has reduced further on the previous year.
3.3 Patient experience
All feedback from patients regarding their experiences with Ramsay Health Care are welcomed and inform service development in various ways dependent on the type of experience (both positive and negative) and action required to address them.
Quality Accounts 2014/15
Page 29 of 36
All positive feedback is relayed to the relevant staff to reinforce good practice and behaviour – letters and cards are displayed for staff to see in staff rooms and notice boards. Managers ensure that positive feedback from patients is recognised and any individuals mentioned are praised accordingly.
Any negative feedback or suggestions for improvement are also fed back to the relevant staff using direct feedback. All staff are aware of our complaints procedures should our patients be unhappy with any aspect of their care.
Complaints management training was completed by all heads of department with a focus on resolving at the time of complaint wherever possible.
Patient experiences are fed back via the various methods below, and are regular agenda items on Local Governance Committees for discussion, trend analysis and further action where necessary. Escalation and further reporting to Ramsay
Corporate and DH bodies occurs as required and according to Ramsay and DH policy.
Feedback regarding the patient’s experience is encouraged in various ways via:
Continuous patient satisfaction feedback via a web based invitation
Hot alerts received within 48hrs of a patient making a comment on their web survey
Friends and family questions asked on patient discharge
Verbal feedback to Ramsay staff - including Consultants, Matrons/General
Managers whilst visiting patients and Provider/CQC visit feedback.
Written feedback via letters/emails
PROMs surveys
Care pathways
– patients are encouraged to read and participate in their plan of care
3.3.1 Patient Satisfaction Surveys
Our patient satisfaction surveys are managed by a third party company called ‘Qa
Research’. This is to ensure our results are managed completely independently of the hospital so we receive a true reflection of our patient’s views.
Every patient is asked their consent to receive an electronic survey or phone call following their discharge from the hospital. The results from the questions asked are used to influence the way the hospital seeks to improve its services. Any text comments made by patients on their survey are sent as ‘hot alerts’ to the Hospital
Manager within 48hrs of receiving them so that a response can be made to the patient as soon as possible.
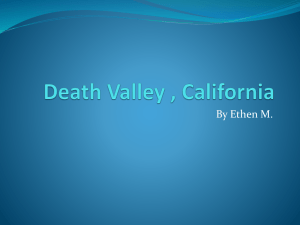
We have consistently maintained a moving quarterly average patient satisfaction score above 95% and proactively seek patient feedback to ensure we maintain high levels of patient satisfaction.
Quality Accounts 2014/15
Page 30 of 36
Satisfaction Scores
NHS/Private Patients
120
100
80
60
40
20
0
97.0 95.3
2013/14 2014/15
Tees Valley Treatment Centre
What our patients say:
‘5 star service, clean unit and location, friendly staff.’
‘From admission to discharge it was an excellent experience. The staff were excellent, friendly and very supportive. I would really recommend the treatment centre thank you .’
‘Excellent care from the initial consultation to leaving after the surgery.’
‘1st class service.’
‘Professional, courteous & friendly service minimum waiting time.’
‘Brilliant service and people from start to finish.’
‘Very clean and friendly hospital, it’s been a pleasure being here, thank you your staff are great .’
Quality Accounts 2014/15
Page 31 of 36
3.4 Tees Valley Treatment Centre Case Study
Health Care Assistant Apprentice Programme
Ramsay Health Care recognises the valuable contribution Health Care Assistants can make to the care environment. Acknowledging that recruiting of apprentices ensures that we are introducing young people into the workforce and allows us to train staff in our ways of working in particular endorsing the Ramsay Way.
Working in partnership with North Hertfordshire College Ramsay commenced an
HCA apprenticeship programme in 2014. Tees Valley Treatment Centre signed up to the programme offering a placement in the theatre department for a candidate commencing in September 2014.
Following a recruitment campaign Frances Tobin joined the theatre team in
September and supported by assessors from Hertfordshire College and an onsite mentor registered nurse Helen Wright. Frances is working towards a Level 2
Health and Social Care qualification a work based qualification working 30 hours per week in theatre with 7.5 hours study time per week.
Working on a fixed term contract for twelve months Frances has grown in confidence and learnt many practical skills which will allow her to become a proficient HCA and also support her long term goal which is to complete a nursing degree.
‘I had just finished college when I started the apprenticeship, I have learned so much since it’s a great place to work.’
Frances Tobin
Quality Accounts 2014/15
Page 32 of 36
Appendix 1
Services covered by the Quality Account
Speciality
Dermatology
General Surgery
GI Endoscopy
Oral Surgery
Orthopaedic Surgery
Plastic Surgery
Urology
Gynaecology
Service
Minor Skin
Varicose Veins
Hernia Repair
Rectal Surgery
Colonoscopy
Flexible Sigmoidoscopy
Gastroscopy
Tooth extraction
Hand
Knee
Shoulder
Wrist
BCC
Skin lesions/cysts
Bladder Dysfunction
Erectile Dysfunction
General Urology
Female Incontinence
Urinary and Prostate Assessment
Vasectomy
Diagnostic and Therapeutic
Hysteroscopy
Quality Accounts 2014/15
Page 33 of 36
Appendix 2 – Clinical Audit Programme 2014/15. Each arrow links to the audit to be completed in each month.
Quality Accounts 2014/15
Page 34 of 36
Tees Valley Treatment Centre
Ramsay Health Care UK
We would welcome any comments on the format, content or purpose of this Quality Account.
If you would like to comment or make any suggestions for the content of future reports, please telephone or write to the
General Manager using the contact details below.
For further information please contact:
Tees Valley Treatment Centre
One Life
Linthorpe Road
Middlesbrough
TS1 3QY
Tel: 01642 737 855 www.teesvalleytreatmentcentre.co.uk
Centres
Quality Accounts 2014/15
Page 35 of 36
Quality Accounts 2014/15
Page 36 of 36