Break-Technique Handheld Dynamometry: Relation Between Angular Velocity and Strength Measurements ORIGINAL ARTICLE
advertisement

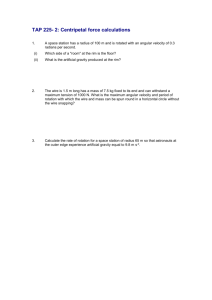
1420 ORIGINAL ARTICLE Break-Technique Handheld Dynamometry: Relation Between Angular Velocity and Strength Measurements Stephen P. Burns, MD, David E. Spanier, MD ABSTRACT. Burns SP, Spanier DE. Break-technique handheld dynamometry: relation between angular velocity and strength measurements. Arch Phys Med Rehabil 2005;86: 1420-6. Objectives: To determine whether the muscle strength, as measured with break-technique handheld dynamometry (HHD), is dependent on the angular velocity achieved during testing and to compare reliability at different angular velocities. Design: Repeated-measures study. Participants underwent HHD by using make-technique (isometric) and break-technique (eccentric) dynamometry at 3 prespecified angular velocities. Elbow movement was recorded with an electrogoniometer. Setting: Inpatient spinal cord injury unit. Participants: Convenience sample of 20 persons with tetraplegia with weakness of elbow flexors or extensors. Interventions: Not applicable. Main Outcome Measures: Elbow angular velocity and muscle strength recorded during HHD. Results: With the break technique, angular velocities averaging 15°, 33°, and 55°/s produced 16%, 30%, and 51% greater strength measurements, respectively, than velocities recorded by using the make technique (all P⬍.006 for comparisons between successive techniques). The intraclass correlation coefficient for intrarater reliability was .89 or greater for all testing techniques. Conclusions: Greater strength is recorded with faster angular velocities during HHD. Differences in angular velocity may explain the wide range previously reported for break- versus make-technique strength measurements. Variation in angular velocity is a potential source of variability in serial HHD strength measurements, and for this reason the make technique may be preferable. Key Words: Muscle spasticity; Rehabilitation; Reproducibility of results; Spinal cord injuries. © 2005 by American Congress of Rehabilitation Medicine and the American Academy of Physical Medicine and Rehabilitation ELIABLE AND PRECISE MEASUREMENTS of muscle strength are essential for clinical care and research. AccuR rate measurements allow clinicians to monitor strength im- From the Spinal Cord Injury Service, Veterans Affairs Puget Sound Health Care System (Burns); the Department of Rehabilitation Medicine, University of Washington (Burns, Spanier); and Harborview Injury Prevention and Research Center (Burns), Seattle, WA. Supported by the Department of Veterans Affairs (DVA). The views expressed in this article are those of the authors and do not necessarily represent the views of the DVA. No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the author(s) or upon any organization with which the author(s) is/are associated. Correspondence to Stephen P. Burns, MD, SCI (128), VA Puget Sound Health Care System, 1660 S Columbian Way, Seattle, WA 98108, e-mail: spburns@u.washington.edu. Reprints are not available from the authors. 0003-9993/05/8607-9405$30.00/0 doi:10.1016/j.apmr.2004.12.041 Arch Phys Med Rehabil Vol 86, July 2005 provement with exercises or other prescribed treatments or to monitor disease progression or development of secondary conditions. Manual muscle testing (MMT), the most widely used method for measuring muscle strength, has many desirable properties, such as ease of performance and the need for no testing equipment. However, the 6-point (range, 0 –5) Medical Research Council scale is ordinal, has only fair reliability when assessed for individual muscles, and has limited utility in discriminating between degrees of weakness for grade 4/5 strength.1,2 MMT also requires considerable training to achieve this modest degree of reliability.3 Instrumented strength measurements produce continuous (ie, nonordinal) measurements of muscle strength and in general have better reliability than MMT.4,5 Most methods require either large instruments, such as isokinetic dynamometers, or placement of fixed gauges against which the patient exerts maximal effort. This requirement makes these techniques somewhat cumbersome in some clinical settings, and the equipment cannot easily be configured to assess some clinically relevant muscles. Handheld dynamometry (HHD) overcomes some of these limitations by having the examiner stabilize the force gauge, allowing multiple muscles to be tested at the bedside with a single portable instrument. Prior studies6-8 have confirmed excellent reliability with HHD under most conditions. Excellent reliability has been shown even with use of inexperienced examiners.9-12 HHD is performed with 1 of 2 testing techniques: make or break. The make technique requires the patient to exert a maximal isometric contraction while the examiner holds the dynamometer in a fixed position. The break technique, in contrast, requires the examiner to overpower a maximal effort by the patient, thereby producing a measurement of eccentric muscle strength. Both methods produce strength measurements that have excellent reliability, although the break technique produces higher values.6-9,13 However, prior studies do not agree about the magnitude of the difference between the 2 techniques. Some8,13 report that the break technique produced 3% to 5% greater strength measurements, whereas others6,7 report that the break technique produces 30% greater strength measurements, and up to 70% greater strength measurements in patients with stroke. In a previous study,9 we noted no relation between the angular velocity achieved by using the break technique and the strength recorded but that study had limited power to detect this relationship. In vitro studies show increased muscle strength (tension) with increased velocity of muscle stretching, as shown with classic force-versus-velocity curves representing muscle contractile properties.14 In contrast, in vivo studies performed with isokinetic dynamometers show at most a small increase in strength with eccentric contractions, and strength does not increase with greater velocity of eccentric contraction.15 The primary objective of the present study was to determine the relation between strength measurements and the angular velocity achieved during break-technique HHD. The hypothesis was that greater angular velocity would be associated with higher strength measurements. Secondary objectives included comparing the reliability of HHD performed at different angu- BREAK-TECHNIQUE HANDHELD DYNAMOMETRY, Burns 1421 lar velocities, and determining whether spasticity would be associated with proportionally greater break versus make strength measurements. METHODS Participants Study participants were inpatients on the spinal cord injury (SCI) ward at VA Puget Sound Health Care System, where they were undergoing hospitalization for annual medical evaluations, treatment of pressure ulcers, prescription of new equipment, or additional physical and occupational therapy. The study protocol received approval from institutional review boards at the University of Washington and VA Puget Sound Health Care System, and written informed consent was obtained from all participants. Inclusion criteria for study participation included the following: history of SCI (traumatic or nontraumatic etiology), and weakness of either the elbow flexors or extensors with MMT grades of 3/5 or 4/5. Exclusion criteria included the following: upperlimb pathology that would preclude maximal strength testing (eg, recent upper-limb fracture), medical contraindications to maximal strength testing, or cognitive dysfunction with inability to reliably follow commands. During the data collection period, consecutive patients who were admitted to the ward and met study criteria were offered participation. One patient who participated had also participated in our previous investigation of HHD.9 Participants underwent clinical examination by the senior author (SPB) for muscle strength, sensation, reflexes, and spasticity. Muscle strength was initially assessed with MMT and performed for the American Spinal Injury Association (ASIA) key muscles, including elbow flexion and extension, by using whole number muscle grades, as described in the ASIA Reference Manual.16 Classifications were assigned for motor levels and ASIA Impairment Scale.17 Deep tendon reflexes (DTR) for the bilateral biceps and triceps brachii, assessed by tendon reflex hammer, were graded on a 0 to 3⫹ scale (absent, hypoactive, normal, hyperactive). Spasticity was assessed for the elbow flexors and extensors with passive movement of the upper limb and grading of the degree of resistance to movement using the Modified Ashworth Scale (MAS).18 Based on the clinical examination, we selected a single muscle group (either elbow flexors or extensors) unilaterally for HHD testing. We selected the muscle with greatest MAS score or, if muscle tone was normal, the maximal DTR, provided that the MMT score for the muscle was 3/5 or 4/5. Strength Testing Protocol Participants were positioned supine on a hospital bed, with the posterior aspect of the arm contacting the bed and the forearm in a vertical, gravity-eliminated position. An electrogoniometer was fabricated by using a CP-2FC rotary potentiometera with ⫾1% linearity. The electrogoniometer was placed across the elbow joint and secured to the arm and forearm (fig 1), and a TSD-150 preamplified surface electromyography electrodeb was placed over the muscle group undergoing testing. The electrogoniometer was calibrated with the elbow at 90° of flexion and at maximal extension (0°, or a positive angle if the participant lacked full elbow extension). A universal goniometer was used to determine elbow angles, with axis alignment along the humerus and radius, with the fulcrum centered over the lateral epicondyle.19 The electrogoniometer was recalibrated at the start of each testing session. The electromyographic signal was used to assist the identification of Fig 1. Setup for strength testing of biceps and data acquisition by the HHD and electrogoniometer. During individual strength measurements, the examiner stabilized the proximal limb with 1 hand and applied force to the distal limb through the HHD using the opposite hand. The photo depicts the testing setup on a neurologically intact individual. periods of HHD and electrogoniometer signals that occurred during individual strength measurements, but the electromyographic signal was not otherwise analyzed. HHD was performed for either elbow flexion or extension by using a Chatillon CSD-200 dynamometer,c with the distal edge of the HHD aligned with the radial or ulnar aspect of the radiocarpal joint. The HHD has a continuous analog signal output that is proportional to the applied force, along with the conventional digital display showing the peak force recorded during the test. The examiner attempted to maintain the direction of force application perpendicular to the forearm. The peak force recorded by the HHD was noted after each test. During HHD testing, the analog outputs of the HHD, electrogoniometer, and electromyography electrode were synchronously recorded by means of an MP100WS interface and AcqKnowledge softwareb with sampling at 500Hz. The testing protocol is in appendix 1. A single examiner (DES) performed testing on each participant by using make technique and 3 target angular velocities for the break technique. The examiner had relatively little experience performing HHD, having occasionally tested patients during the preceding 3 years. We selected target angular velocities for break testing so that the medium velocity would represent the velocity typically used by clinicians at our institution and that was used by novice physical therapists in our previous study.9 The target angular velocities were the following: high angular velocity was defined as 90° to 100°/s, medium velocity as 30° to 40°/s, and low velocity as 10° to 20°/s. During the first testing session, the examiner tested the participant 8 times, twice by using the make technique, and twice each at low, medium, and high angular velocities by using the break technique. After a 5-minute rest, this procedure was repeated. Using scripted instructions, participants were asked to exert a maximal effort against the HHD when instructed by the examiner. They were also told that the technique would vary between successive trials, but in all cases they were to provide a maximal effort. Although not depicted in figure 1, the examiner stabilized the proximal limb with 1 hand while applying force through the myometer with the other hand during each strength measurement. Consistent verbal encouragement was provided to parArch Phys Med Rehabil Vol 86, July 2005 1422 BREAK-TECHNIQUE HANDHELD DYNAMOMETRY, Burns ticipants by the examiner during each measurement. The order in which the 4 techniques were performed was randomized for successive participants. Completion of all testing required approximately 30 minutes per participant. After testing of the first participant, the investigators reviewed the electrogoniometer and force data to confirm that the angular velocities were close to the target ranges. The examiner did not view any subsequent angular velocity data until testing was completed on all 20 participants. Analysis Electrogoniometric data were first reviewed graphically along with the continuous HHD output and the electromyographic signal. For each test, we identified periods of peak force application on the HHD signal tracing, and this was confirmed by using the electromyographic signal. For breaktechnique trials, we calculated the angular velocity for the portion of the force application during which the participant’s muscle was overcome into an eccentric contraction. The joint angle at which the peak force occurred and the total degrees through which the limb was moved during the period of maximal muscle contraction was also recorded. Similar calculations were performed for make technique trials. In keeping with our clinical practice and that of other investigators,20,21 we used the highest strength measurement achieved from each testing session with each technique in our primary analyses. Other investigators have compared use of the maximum, mean, or median for repeated HHD trials, or have compared the mean to a single trial, and have shown similar reproducibility with each method.10,11 We chose to repeat contractions only twice per technique session because we wanted to minimize the number of muscle contractions and resulting fatigue. We combined data from elbow flexor and extensor testing for most analyses because mean strength was similar for the 2 muscle groups. Strength as a proportion of predicted strength was calculated for make technique tests from session 1 by using previously published age- and sex-specific reference values for the dominant extremity.22 Mean strengths and velocities were compared by using the Friedman and Wilcoxon signed-rank tests. Break/make (B/M) ratios were calculated by dividing the peak force obtained with each break technique (low, medium, high) by the peak force obtained with the make technique. The correlations between the 3 B/M ratios and the DTR score for the muscle were assessed with the Spearman correlation coefficient. The initial analysis for strength versus angular velocity used the classification of the testing technique (make, low, medium, or high) for the trial with the greatest strength value, whereas the subsequent analysis used the angular velocity recorded by the electrogoniometer for each of the 16 tests. By using the latter data, Spearman correlation coefficients were calculated separately for each participant to assess for correlations between strength and angular velocity. Additionally, the slope of the strength versus angular velocity correlation was determined by calculating a slope for each participant by using all 16 strength and angular velocity measurements, normalizing strength data for the mean of the participant’s 4 make-technique tests. Reliability of the measures was assessed with the intraclass correlation coefficient (ICC) 2-way mixed-effects model. We also plotted differences versus means for strength measurements, as described by Bland and Altman,23 to assess for systematic differences across the range of strength values. All statistical analyses were performed by using SPSS, version 10.0.5.d A P value of less than .05 was considered significant. Arch Phys Med Rehabil Vol 86, July 2005 Table 1: Angular Velocities for Each Testing Technique Technique Angular Velocity (°/s) Make Low break Medium break High break 1⫾5 15⫾0 33⫾15 55⫾26 NOTE. Values are mean ⫾ standard deviation (SD). P⬍.001 for make vs low, low vs medium, and medium vs high comparisons. RESULTS Participants The 20 participants included 19 men and 1 woman, all with tetraplegia. The mean age of participants was 57⫾15 years, and the mean duration of SCI was 19⫾21 years. The ASIA Impairment Scale scores were grades A, B, C, and D for 6, 4, 4, and 6 participants, respectively. The motor level on the tested side was C5, C6, and C7 for 11, 5, and 4 participants, respectively. The test muscles were the elbow flexors for 5 participants and the elbow extensors for 15 participants. MMT scores for the test muscle were 3/5 for 7 participants and 4/5 for 13 participants. DTR scores were 0, 1⫹, and 3⫹ for 10, 6, and 4 participants, respectively, and MAS scores were 0, 1, 1⫹, and 2 for 16, 1, 1, and 2 participants, respectively. Participants with motor-incomplete tetraplegia (ASIA grades C or D) had greater DTR scores for the test muscle than did those with motorcomplete tetraplegia (ASIA grades A or B; P⫽.05 for difference). Angular Velocity and Strength The mean angular velocities achieved for each testing technique during all trials are in table 1. The angular velocities for the 4 testing techniques differed significantly from each other (P⬍.001). The mean velocities for low and medium velocity break testing were close to the target velocities we had specified before the study, but high velocity testing (mean, 55°/s) was lower than the 90° to 100°/s we had planned to achieve. The examiner used a significantly greater (P⫽.008) angular velocity during the initial high velocity trial (61°/s) than on the final high velocity trial (51°/s), and there was a similar trend with medium velocity testing. Over the course of testing the 20 participants, the examiner showed no trend in the angular velocities used for any of the 4 testing techniques. The examiner moved the participant’s elbow through a mean ⫾ standard deviation (SD) of 3°⫾2°, 16°⫾10°, 20°⫾14°, and 20°⫾13° for make, low, medium, and high testing techniques, respectively. For the 15 participants who underwent testing of elbow extensors, the peak force was recorded at elbow angles of 89°, 99°, 111°, and 114° for make, low, medium, and high testing techniques, respectively. For the 5 participants who underwent testing of elbow flexors, the respective elbow angles at peak force were 83°, 68°, 60°, and 56°. However, during most tests, force was relatively constant over a range of degrees of elbow movement, without a pronounced peak force. Mean strength for each technique and each testing session is shown in figure 2 and table 2. The strength recorded for the make technique in session 1 averaged 33%⫾18% of predicted strength. Strength was significantly greater with increased velocity (make vs low, low vs medium, medium vs high) for all comparisons in both testing sessions, with the exception of low versus medium in the second testing session (P⫽.09; see table 2). Strength comparisons are also reported as mean B/M ratios for the 3 break techniques (table 3). In both sessions, low- 1423 BREAK-TECHNIQUE HANDHELD DYNAMOMETRY, Burns Table 3: B/M Ratios* Ratio Session 1 Session 2 Low B/M Medium B/M High B/M 1.16⫾0.16 1.30⫾0.26 1.51⫾0.46 1.16⫾0.21 1.33⫾0.33 1.43⫾0.36 NOTE. Values are mean ⫾ SD. *P⫽.005 and P⫽.009 for low B/M vs medium B/M, and P⫽.003 and P⫽.048 for medium B/M vs high B/M comparisons for sessions 1 and 2, respectively. Fig 2. Mean strength for the 4 testing techniques, session 1. Error bars represent the standard error of the mean. The differences between strength with each of the 4 techniques were statistically significant. See table 2. velocity testing produced significantly lower B/M ratios than medium-velocity testing, and medium-velocity testing resulted in significantly lower ratios than high velocity testing. Comparing a technique between sessions 1 and 2, we found that strength was lower in session 2 (range, 3.9% to 7.8% lower) with significant decrements for medium (P⫽.04) and high techniques (P⫽.007). We had planned to analyze B/M ratios versus MAS scores. Because only 4 participants had increased muscle tone (MAS score, ⱖ1) in the test muscle, we instead assessed the relation between B/M ratio and DTR scores for test muscles. The B/M ratios were correlated ( range, .533–.788; all P⬍.016) with DTR scores for all B/M ratios in session 1 and for medium and high B/M ratios in session 2. Figure 3 shows the relation between B/M ratio and DTR for medium velocity testing from session 1. When the same analysis was performed by using MAS scores, significant correlations were found for low-velocity B/M ratios in both sessions and medium-velocity B/M ratios in the second session, and there was a trend (P⫽.051) toward a correlation with high-velocity B/M ratio in the second session. However, given the low number of participants with abnormal MAS scores, these findings should be interpreted with caution. Representative strength and angular velocity data for a single participant using all 16 tests recorded in the 2 sessions are in figure 4. The mean correlation coefficient (Spearman ) for the 20 participants was .60, and 15 of 20 participants showed statistically significant positive correlations. The mean slope for the correlation between strength and angular velocity corresponded to an 8%⫾6% increase in strength for every 10° increase in angular velocity. Reliability of Testing Techniques The ICC for each testing technique from session 1 to 2 is shown in table 4, along with 95% confidence intervals (CIs) for the coefficients. The ICCs for all testing techniques were .89 or greater, with the lowest value for the make technique, but CIs for all techniques overlapped. Bland-Altman plots of mean strength versus difference in strength between sessions 1 and 2 showed no consistent relationship between the 2 variables for any testing technique. DISCUSSION The findings confirmed our hypothesis that greater angular velocity during break technique HHD testing is associated with higher strength measurements. Break-technique testing, performed at angular velocities averaging 15°, 33°, and 55°/s, produced 16%, 30%, and 51% greater strength, respectively, than isometric testing by using the make technique during the first session. Large differences were seen between high-velocity break versus make testing for some participants; for 4 participants, this difference exceeded 100%. Our prior study9 did not show an association between angular velocity and strength measurements. However, the 2 examiners in that study did not intentionally perform break testing over a wide range of angular velocities, and the velocities used by the 2 examiners for testing were similar. Table 2: Mean Strength for Each Testing Technique Difference Between Sessions Strength (kg) Technique Make Low break Medium break High break Session 1 Session 2 % P 6.6⫾3.4 7.6⫾3.8 8.2⫾3.9 9.0⫾3.5 6.3⫾4.1 7.3⫾4.3 7.8⫾4.0 8.3⫾4.0 4.5 3.9 4.9 7.8 .09 .51 .04 .007 P Comparison Session 1 Session 2 Make vs low break Low break vs medium break Medium break vs high break .003 .007 .006 .004 .09 .045 NOTE. Values are mean ⫾ SD or otherwise indicated. Fig 3. B/M ratio for medium velocity testing (session 1) versus DTR scores. Arch Phys Med Rehabil Vol 86, July 2005 1424 BREAK-TECHNIQUE HANDHELD DYNAMOMETRY, Burns Fig 4. Angular velocity versus strength for all measurements on a single participant. ⴝ80; the trend line indicates a 7% greater strength measurement for every 10° increase in angular velocity. Additionally, electrogoniometric data were obtained from only a subset of participants. This velocity dependence of break-technique strength measurements may be an explanation for conflicting results from prior HHD studies that compared strength by using make and break techniques. Van der Ploeg and Oosterhuis13 reported B/M ratios of 1.03 for normative subjects and up to 1.11 for subjects with organic weakness. They concluded that a ratio of greater than 1.2 supported the diagnosis of functional weakness (eg, conversion disorder). Stratford and Balsor8 reported B/M ratios of 1.05 to 1.06 in neurologically intact subjects. These ratios were similar to those they obtained using an isokinetic dynamometer set to perform eccentric testing at an angular velocity of 2°/s. In contrast, Bohannon6,7 reported B/M ratios of 1.3 in normative subjects and on the nonparetic side in patients with stroke. The B/M ratios obtained in the current study with medium velocity testing and in our prior study9 agree most closely with those reported by Bohannon. Other investigators did not measure or describe the angular velocity that occurred with break testing, and the description of break testing has varied considerably between studies,6-8,11,13,21 so variability in technique may account for the wide range previously reported for B/M ratios. Differences in break-technique angular velocity are a potential source of variability over serial measurement. Although previous studies have shown high interrater reliability for make and break techniques, study factors (small sample sizes, short time interval between testing sessions, concurrent training of examiners) may have limited the variability in technique. Use of examiners who trained separately could allow differences in the break technique to affect strength recordings. It may be more practical to have examiners perform make technique testing because reproduction of an isometric test should be simpler than attempting to train examiners to produce a specific angular velocity for break testing. Upper motoneuron (UMN) weakness is a second factor that may have contributed to the variability in B/M ratios in prior studies because some of these have included subjects with UMN disorders.7,13 We found higher B/M ratios in participants with preserved DTRs in the test muscle. The presence of a DTR in a muscle at or below the motor level is likely to be associated with some degree of UMN weakness because their presence was more common in patients with motor-incomplete (ASIA grades C, D) Arch Phys Med Rehabil Vol 86, July 2005 injuries. The recovery of strength seen in the first few months postinjury is in part because of collateral sprouting from intact motor units innervating the muscle.24 For this reason, lower motoneuron weakness predominates in paretic muscles at or below the motor level in persons with motor-complete tetraplegia. Bohannon7 previously noted elevated B/M ratios in paretic muscles in persons with UMN weakness. In that study of 22 patients with stroke, B/M ratios were 1.7 on the hemiparetic side compared with 1.3 on the less involved side, and the side-to-side difference in B/M ratios correlated positively with MAS scores. The elevated ratio is presumably due to augmentation of breaktechnique strength measurements because break-technique testing involves the same type of muscle stretching for assessment of muscle tone with the MAS. In our previous study,9 we did not find a correlation between MAS and B/M ratios, whereas in the present study significant correlations were seen for some tests. The small number of participants with elevated MAS grades was a limitation in both studies. This relation could be investigated in an SCI population with greater spasticity or in a different population. If B/M ratios are associated with muscle spasticity, then the ratios could be altered if a patient’s spasticity changes, either with worsening as spasticity develops after onset of the neurologic deficit or with improvement through use of antispasticity medications or neurolytic injection procedures. This hypothesis could be confirmed by studying patients before and after initiation of antispasticity medications, such as intrathecal baclofen. As Bohannon7 has noted, it would be useful in future studies to measure function, to determine which strength measurement technique produces the highest correlation with function. Our present findings are in agreement with prior observations on differences between isometric and eccentric strength derived from in vitro studies but are in conflict with most from in vivo studies.14 With maximal electric stimulation of animal whole muscle preparations, muscle tension during eccentric contraction increases with the velocity of muscle stretch and can exceed isometric tension by up to 100%.14 When maximal voluntary contractions are performed in human experiments using isokinetic dynamometers, eccentric strength only slightly exceeds isometric strength.15 With the application of electric stimulation on intact human muscles, the force-velocity relationship becomes more similar to that of in vitro muscle preparations, with greater forces recorded for faster eccentric contrations.25 These observations have been interpreted as reflecting a neural force-regulating mechanism that prevents development of potentially injurious tension with eccentric contractions, and evidence supports the presence of separate neural control mechanisms for eccentric contractions.26 Control of force generation may be altered in patients with neurologic disorders, which may in part explain the B/M ratios seen in this study and others.7 We also considered whether the greater strength at faster angular velocities could reflect the force required by the examiner to accelerate the mass of the distal limb to the desired angular velocity. We believe that, for several reasons, this is unlikely to account for much of the strength difference with increased angular velocity. First, the peak forces on the continuous myometer output occurred after the limb had been accelerated to a relatively con- Table 4: ICC for Testing Techniques, Session 1 Versus Session 2 Technique ICC 95% CI Make Low break Medium break High break .89 .93 .97 .97 .74–.96 .83–.97 .93–.99 .92–.99 1425 BREAK-TECHNIQUE HANDHELD DYNAMOMETRY, Burns stant angular velocity and not during the periods corresponding to maximal limb acceleration, and peak forces typically occurred during a long period of relatively stable force. Also, the force required to accelerate the forearm and hand to the target angular velocities would be relatively small compared with the recorded forces for most participants because limb acceleration was relatively slow and the force was applied at a distal point on the limb. However, some force is required for limb acceleration, and for participants with severe weakness this force could contribute significantly to the increased B/M ratio at higher velocities. Review of the elbow movement recorded by the electrogoniometer during strength testing revealed technical factors that could lead to strength measurement errors. When performing break testing on the elbow extensors, the examiner infrequently moved the elbow into excessive flexion (⬎140°), producing a considerably greater strength measurement at the end range of flexion. The peak force recorded in those cases likely occurred as soft tissues of the arm and forearm contacted each other. The examiner tended to produce a greater than intended angular velocity on the first trial of high-velocity break testing if the muscle was relatively weak. Also, the examiner had difficulty achieving the intended high velocity during break testing if the muscle was strong. The examiner rarely produced excessive eccentric (break) movement when attempting to perform make technique. This occurred much less frequently than in our previous study, during which 25% of make trials resulted in excessive break-type movement, which was defined as more than 5° of eccentric movement.9 It is possible that the examiner in the present study was more attentive to how the make technique testing was performed because the intention was to produce movement that was distinct from the low (10°–15°/s) velocity break technique. A number of factors should be considered when choosing a testing technique. The present study showed excellent intrarater reliability for the make technique and the 3 break techniques, and prior studies have also shown high reliability for the 2 techniques.6-9,13 The small decline in strength between testing sessions for some techniques was likely secondary to muscle fatigue from repeated contractions. However, as discussed earlier, if examiners were to perform the break technique at velocities that differ, it could lead to differences in the strength recorded. This source of variability has likely been minimized by study designs, but, in a clinical setting or in a multisite study, it could potentially affect reliability. If muscle spasticity is anticipated to fluctuate over time, then the make technique might be preferable because changes in tone could change break-technique strength to a greater degree than the make technique. In cases in which the examiner is relatively weak or the patient is relatively strong, it may be useful for the examiner to confirm that examiner strength is not limiting the maximal force recorded. This could be accomplished by attempting an additional trial using the break technique, with successful overpowering of the test muscle indicative of adequate examiner strength, and inability to overpower the muscle indicative that examiner strength may have limited the recorded strength. However, it is possible that an examiner could have adequate strength to resist a maximal effort and could thus obtain a measurement of maximal effort but might not have enough strength to overpower the muscle, in which case make testing would be preferable. There are some additional limitations to our findings. This study was performed in a population with tetraplegia, and the findings may not generalize to other patient populations. The participants had a relatively low level of muscle tone, and similar findings regarding B/M ratios may not be present in populations with pure lower motoneuron disorders or greater spasticity. Our planned analysis of strength versus muscle tone involved use of MAS scores, not DTR scores, so these findings should be interpreted with caution. The muscles tested were relatively weak, averaging 33% of predicted strength. Lower strength was recorded during the second session for medium- and high-velocity testing, which likely was caused by muscle fatigue induced by multiple maximal contractions. For this reason, we consider the results from session 1 to be more representative of what would be obtained with conventional HHD testing, and we did not calculate additional measures of repeatability for the 2 testing sessions. Finally, testing was performed by a single examiner, who was given feedback on the velocities he achieved for testing on the first participant. Data on testing velocities are not available to examiners when performed in a clinical setting with standard equipment. CONCLUSIONS Break-technique HHD produces higher strength measurements when it is performed at greater angular velocities in persons with tetraplegia. The velocity dependence of the strength measurements may explain some of the variability previously reported when comparing strength measurements with make and break techniques. Variability in angular velocity during break testing is a potential source of error when longitudinal strength measurements are performed. Patients with signs of UMN weakness may show relatively greater strength with the break versus the make technique, and fluctuations in muscle spasticity could potentially alter break-technique measurements more so than make-technique measurements. To minimize variability in strength measurements related to differing angular velocities and fluctuations in muscle tone, it may be preferable to perform HHD by using the make technique. APPENDIX 1: TESTING PROTOCOL Session Trial 1 1 Test Technique Make Low velocity break Medium velocity break High velocity break Make Low velocity break Medium velocity break High velocity break 2 5-minute rest 2 1 2 Make Low velocity break Medium velocity break High velocity break Make Low velocity break Medium velocity break High velocity break NOTE. For each participant, the techniques (make, low velocity, medium velocity, high velocity) were performed in random order. Arch Phys Med Rehabil Vol 86, July 2005 1426 BREAK-TECHNIQUE HANDHELD DYNAMOMETRY, Burns References 1. Frese E, Brown M, Norton BJ. Clinical reliability of manual muscle testing. Middle trapezius and gluteus medius muscles. Phys Ther 1987;67:1072-6. 2. Dvir Z. Grade 4 in manual muscle testing: the problem with submaximal strength assessment. Clin Rehabil 1997;11:36-41. 3. Mendell JR, Florence J. Manual muscle testing. Muscle Nerve 1990;13:S16-20. 4. Delitto A. Isokinetic dynamometry. Muscle Nerve 1990; 13(Suppl):S53-7. 5. Larsson B, Karlsson S, Eriksson M, Gerdle B. Test-retest reliability of EMG and peak torque during repetitive maximal concentric knee extensions. J Electromyogr Kinesiol 2003;13:281-7. 6. Bohannon RW. Make tests and break tests of elbow flexor muscle strength. Phys Ther 1988;68:193-4. 7. Bohannon RW. Make versus break tests for measuring elbow flexor muscle force with a hand-held dynamometer in patient with stroke. Physiother Can 1990;42:247-51. 8. Stratford PW, Balsor BE. A comparison of make and break tests using a hand-held dynamometer and the Kin-Com. J Orthop Sports Phys Ther 1994;19:28-32. 9. Burns SP, Breuninger A, Kaplan C, Marin H. Hand-held dynamometry in persons with tetraplegia: comparison of make- versus break-testing techniques. Am J Phys Med Rehabil 2005;84:22-9. 10. Goonetilleke A, Modarres-Sadeghi H, Guiloff RJ. Accuracy, reproducibility, and variability of hand-held dynamometry in motor neuron disease. J Neurol Neurosurg Psychiatry 1994;57:326-32. 11. Horvat M, Croce R, Roswal G. Intratester reliability of the Nicholas Manual Muscle Tester on individuals with intellectual disabilities by a tester having minimal experience. Arch Phys Med Rehabil 1994;75:808-11. 12. Ottenbacher KJ, Branch LG, Ray L, Gonzales VA, Peek MK, Hinman MR. The reliability of upper- and lower-extremity strength testing in a community survey of older adults. Arch Phys Med Rehabil 2002;83:1423-7. 13. van der Ploeg RJ, Oosterhuis HJ. The “make/break test” as a diagnostic tool in functional weakness. J Neurol Neurosurg Psychiatry 1991;54:248-51. 14. Lombardi V, Piazzesi G. The contractile response during steady state lengthening of stimulated frog muscle fibres. J Physiol (Lond) 1990;431:141-71. Arch Phys Med Rehabil Vol 86, July 2005 15. Seger JY, Thorstensson A. Electrically evoked eccentric and concentric torque-velocity relationships in human knee extensor muscles. Acta Physiol Scand 2000;169:63-9. 16. American Spinal Injury Association. Reference manual for the standards for neurologic and functional classification of spinal cord injury. Chicago: ASIA; 2003. 17. Marino RJ, Barros T, Biering-Sorenson F, et al. International standards for neurological classifications of spinal cord injury. J Spinal Cord Med 2002;25:S50-6. 18. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987;67:206-7. 19. Norkin CC, White DJ. The elbow and forearm. In: Norkin CC, White DJ, editors. Measurement of joint motion: a guide to goniometry. 2nd ed. Philadelphia: FA Davis; 1995. p 67-77. 20. Merlini L, Mazzone ES, Solari A, Morandi L. Reliability of hand-held dynamometry in spinal muscular atrophy. Muscle Nerve 2002;26:64-70. 21. Phillips BA, Lo SK, Mastaglia FL. Muscle force measured using “break” testing with a hand-held myometer in normal subjects aged 20 to 69 years. Arch Phys Med Rehabil 2000;81:653-61. 22. Bohannon RW. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch Phys Med Rehabil 1997;78:26-32. 23. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1:307-10. 24. Marino RJ, Herbison GJ, Ditunno JF Jr. Peripheral sprouting as a mechanism for recovery in the zone of injury in acute quadriplegia: a single-fiber EMG study. Muscle Nerve 1994;17:1466-8. 25. Dudley GA, Harris RT, Duvoisin MR, Hather BM, Buchanan P. Effect of voluntary vs. artificial activation on the relationship of muscle torque to speed. J Appl Physiol 1990;69:2215-21. 26. Enoka RM. Eccentric contractions require unique activation strategies by the nervous system. J Appl Physiol 1996;81:2339-46. Suppliers a. Midori America Corp, 2555 E Chapman Ave, Ste 400, Fullerton, CA 92831. b. BIOPAC Systems Inc, 42 Aero Camino, Goleta, CA 93117. c. AMETEK, 37 N Valley Rd, Bldg 4, PO Box 1764, Paoli, PA 19301. d. SPSS Inc, 233 S Wacker Dr, 11th Fl, Chicago, IL 60606.