Detecting ECG Abnormalities via Transductive Transfer Learning Kang Li Nan Du
advertisement

Detecting ECG Abnormalities via Transductive Transfer
Learning
Kang Li
Department of Computer
Science and Engineering
SUNY at Buffalo
Buffalo, 14260, U.S.A.
kli22@buffalo.edu
Nan Du
Department of Computer
Science and Engineering
SUNY at Buffalo
Buffalo, 14260, U.S.A.
nandu@buffalo.edu
Aidong Zhang
Department of Computer
Science and Engineering
SUNY at Buffalo
Buffalo, 14260, U.S.A.
azhang@buffalo.edu
ABSTRACT
Detecting Electrocardiogram (ECG) abnormalities is the process of identifying irregular cardiac activities which may lead
to severe heart damage or even sudden death. Due to the
rapid development of cyber-physic systems and health informatics, embedding the function of ECG abnormality detection to various devices for real time monitoring has attracted
more and more interest in the past few years. The existing machine learning and pattern recognition techniques developed for this purpose usually require sufficient labeled
training data for each user. However, obtaining such supervised information is difficult, which makes the proposed
ECG monitoring function unrealistic.
To tackle the problem, we take advantage of existing well
labeled ECG signals and propose a transductive transfer
learning framework for the detection of abnormalities in
ECG. In our model, unsupervised signals from target users
are classified with knowledge transferred from the supervised
source signals. In the experimental evaluation, we implemented our method on the MIT-BIH Arrhythmias Dataset
and compared it with both anomaly detection and transductive learning baseline approaches. Extensive experiments
show that our proposed algorithm remarkably outperforms
all the compared methods, proving the effectiveness of it in
detecting ECG abnormalities.
Categories and Subject Descriptors
I.5.3 [Pattern Recognition]: Clustering—algorithms; J.3
[Computer Applications]: Life and Medical Science—
health
General Terms
Algorithms, Performance
Keywords
ECG, anomaly detection, transductive learning
Permission to make digital or hard copies of all or part of this work for
personal or classroom use is granted without fee provided that copies are
not made or distributed for profit or commercial advantage and that copies
bear this notice and the full citation on the first page. To copy otherwise, to
republish, to post on servers or to redistribute to lists, requires prior specific
permission and/or a fee.
ACM-BCB’12 October 7-10, 2012, Orlando, FL, USA
Copyright 2012 ACM 978-1-4503-1670-5/12/10 ...$15.00.
ACM-BCB 2012
Figure 1: A Cyber-Physical System.
1.
INTRODUCTION
ECG is an important and commonly used interpretation
of cardiac electrical activities over time and can be used to
assess different heart related biological processes and diseases including cardiac arrhythmias [21], mental stress [24],
morbid obesity [5], etc. The collected ECG signals can be
naturally divided into sequenced instances, each of which is
an observed cardiac cycle (heart beat). In ECG signal monitoring, existing studies usually classify these instances into
two classes: normal and abnormal, which represent normal
state of the heart and abnormal biological events that may
lead to heart damage or even sudden death, respectively. An
automatic ECG abnormality detection approach is thus very
meaningful towards promptly responses of heart attacks and
a better understanding of the underlying biological mechanisms.
Due to the rapid development of health informatics and
cyber-physical systems, embedding the function of ECG abnormality detection into wearable devices for health monitoring and timely alarm has attracted more and more interests during the past few years. Such a typical system
usually contains electro-nodes attached to human bodies,
carry-on devices such as smart phones for signal collection,
and a remote database for data management and analysis,
as presented in Figure 1. One of the major factors limiting the popular usage of these cyber-physical systems is
that the existing machine learning and pattern recognition
techniques developed for ECG abnormality detection usually require sufficient labeled training data for each user to
make the model user-specified and accurate. However, for
ECG signals, such supervised information is very difficult to
obtain without professional knowledge and a lot of effort.
Moreover, since abnormal instances are usually much less
than normal ones, supervised methods require more data in
210
these cases to capture enough variability on data distributions, which makes the labels expensive to obtain.
To solve the problem, we take advantage of existing well
labeled ECG signals and use them as sources into a novel
transductive transfer learning framework for ECG abnormality detection. We propose to unsupervisedly learn ECG
signals from target patients with knowledge transferred from
these supervised sources. In detail, knowledge transferring is
achieved by the Kernel Mean Matching (KMM) [8] method,
in which source instances are weighted to match the distribution of target instances in a reproducing kernel Hilbert
space (RKHS). A novel weighted transductive one class support vector machine (WTOSVM) as well as a labeling process are then proposed to discriminatively classify instances
in the target.
The rest of this paper is organized as follows: we will
briefly discuss the related work of this topic in Section 2;
after giving out the notation used in this paper, we present
the theoretical work of our method in Section 3; the experiments and corresponding analysis are shown in Section 4;
and finally we come to the conclusions and perspectives in
Section 5.
2.
RELATED WORK
As a classical problem in machine learning and pattern
recognition, ECG abnormality detection can be categorized
into the areas of anomaly detection and imbalanced learning,
due to the imbalance between numbers of instances of normal and abnormal classes in the ECG data. Similar datasets
exist in a lot of research and applications, such as text mining [28], video indexing [27] and network security [7]. In such
datasets, one or more classes have significantly less instances
than the others, which conflicts with the assumption made
by regular machine learning methods that each class should
be equal or nearly equal in size. Failing to cover the distributions of imbalanced datasets by traditional methods invokes
general interest of developing new algorithms for them. The
developed methods are further applied to many relevant areas such as noise filtering [1], intrusion detection [9] and
innovation detection [19].
To solve the problem, several solutions have been proposed at both data and algorithmic levels. The former one
includes many different re-sampling methods favoring rebalancing class distributions, such as random under-sampling
of majority instances [15] and synthetic minority oversampling technique (SMOTE) [4]. The algorithmic approaches
usually give higher weights to minority instances in costsensitive and discriminative methods, aiming at rebalancing
the biased decision boundaries [6, 3]. These popular approaches always require supervised information to guide the
rebalancing process, which is expensive to obtain, as explained in the Introduction.
Several methods have been proposed for unsupervised learning on imbalanced datasets. One class support vector machine (OCSVM) [26] adapts the support vector machine
(SVM) algorithm to bound data into a circle while minimizing the diameter of it. Kernel nearest neighbors (KNN)
[23] assumes that majority instances are dense and minorities are sparse, then classify them according to their kernel distances. [10] makes another assumption that each
minority instance should either not belong to any cluster
or be far from its cluster center, and presents a clustering
based method for detecting local outliers. Other unsuper-
ACM-BCB 2012
vised methods could be generally divided into these three
categories.
The main challenge in unsupervised learning on imbalanced ECG datasets is how to uncover the real distribution
of each class without any labeled information. Inspired by
the success of transfer learning on many areas, we propose
a transductive transfer learning algorithm for ECG abnormality detection. Instead of assuming the distributions of
normal and abnormal instances, we classify each target with
assistance of a well labeled source, which fits our common
experience in real life, such as diagnosing a disease on a target patient with cases of similar patients having the same
disease.
The formulated problem in this paper is related to transfer learning, which is the process of transferring information
from a source domain to help learning in a target domain. It
is commonly used when sources and targets are drawn from
the same feature space. Specifically, transductive transfer
learning is the process of knowledge transferring when only
labeled sources and unlabeled targets are available. It has
been successfully implemented in various areas [22, 2]. The
major difficulty in knowledge transferring is that source and
target data are not likely to be drawn from the same distribution, thus directly estimating target data through source
will cause covariance shift and is not applicable in most
cases. To address the problem, we follow the framework proposed in [8] which matches the kernel means of the source
and the target in an RKHS for knowledge transferring.
The main contributions of this paper are:
• We propose a novel anomaly detection algorithm to solve
the problem of detecting irregular events in the collected
ECG signals.
• We investigate the problem from the transductive transfer
learning point of view. Since our model is general, it can
be further expanded to transductive learning on imbalanced
datasets in other areas.
• In the experimental study of our method on the MITBIH Arrhythmias Dataset [18], our model outperforms all
the other baseline methods for ECG abnormality detection
and achieves 25% to 60% performance improvement than
the baselines, which demonstrates the effectiveness and superority of our proposed algorithm.
3.
METHOD
Notice that the preprocessing method of dividing ECG
signals into instances (heart beats) is not the focus of this
paper. Instead, we aim at unsupervised recognition of the
preprocessed instances. Before diving into the details of our
framework, let’s first define the notation used in the following sections. Suppose for a target user/patient, we obtain
an ECG signal including t instances T = {xi | i ∈ [1, t]} to
be classified into normal and abnormal classes. A selected
source labeled signal S = {xˆi | i ∈ [1, s]} will be used to help
the learning process of T . For simplicity here, we assume
that xi and xˆi are drawn from the same feature space and
the label vector for the source is Ŷ = {yˆi |yˆi ∈ {−1, +1}, i ∈
[1, s]}, where −1 represents majority (normal) instances and
+1 represents minority (abnormal) instances, respectively.
The aimed problem in this paper can be expressed as:
given a target imbalanced dataset T , a source dataset S
and its labels Ŷ , learn a mapping f = T → Y , in which
Y = {yi |yi ∈ {−1, 1}, i ∈ [1, t]}.
211
to observations that are under-represented in Pˆr and lower
weights to over-represented instances. The estimation of
β(x, y) thus does not require any supervised information in
both the source and the target.
According to Equation 2, knowledge transferring from a
source to a target is accomplished by estimating the target
data distribution P r(x) by β(x)Pˆr(x). The idea of KMM
in learning the β vector is to minimize the discrepancy between the centers of instances in the target and the weighted
instances
in the source in an RKHS. Moreover, a constraint
| 1s si=1 βi − 1| ≤ is enforced to ensure that β(x)Pˆr(x) is
close to a probability distribution. The objective function
for KMM is then expressed as:
140
Dataset
Dataset
Dataset
Dataset
120
100
1:
1:
2:
2:
Normal
Abnormal
Normal
Abnormal
Dimension #2
80
60
40
20
0
−20
−40
0
50
100
150
200
Dimension #1
250
300
350
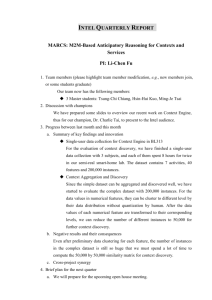
Figure 2: Distributions of two imbalanced datasets.
3.1
β = arg min Ex∼P r [ϕ] − Ex∼Pˆr [βϕ]2
Knowledge Transferring
= arg min Our aim is to classify instances in an unsupervised target with assistance of labeled instances in a source. However, directly classifying data in the target by using models
trained on the source is not applicable, because the source
and the target are not independently and identically drawn
(iid ) from the same distribution. As shown in Figure 2,
in a two dimensional space, two imbalanced datasets 1 and
2 are presented in different shapes, and abnormal instances
of them are marked in red. If we directly classify data in
dataset 2 by classifiers learned on dataset 1, most normal
instances will be labeled as abnormal due to the different
distributions of these two datasets.
To enable knowledge transferring between datasets with
different distributions, we use the KMM method [8]. Suppose we obtain the target samples Z = {(x1 , y1 ), . . . , (xt , yt )} ⊆
X × Y from a Borel probability distribution P r(x, y), and
the source samples Ẑ = {(xˆ1 , yˆ1 ), . . . , (xˆs , yˆs )} ⊆ X̂ × Ŷ
from another such distribution Pˆr(x, y).
A learning method on sources generally minimizes the expected risk:
θ = arg min R[Pˆr, θ, l(x, y, θ)] = arg min E(x,y)∼Pˆr [l(x, y, θ)],
(1)
where l(x, y, θ) is a loss function that depends on a parameter vector θ, such as negative log-likelihood − log P r(y|x, θ)
and misclassification loss; E is the expectation; and R is the
over all loss that we wish to minimize. Since P r(x, y) and
Pˆr(x, y) are different, what we would really like to minimize
is R[P r, θ, l]. An observation from the field of importance
sampling [11] is that
θ = arg min R[P r, θ, l(x, y, θ)]
= arg min E(x, y)∼P r [l(x, y, θ)]
= arg min E(x,
y)∼Pˆr [
P r(x, y)
l(x, y, θ)]
Pˆr(x, y)
(2)
= arg min R[Pˆr, θ, β(x, y)l(x, y, θ)],
P r(x, y)
.
Pˆr(x, y)
Through the function, we can
compute the risk with respect to P r using Pˆr. But the
key problem is that the coefficient vector β(x, y) is usually
unknown, and we need to estimate it from the data. In our
context, since P r and Pˆr differ only in P r(x) and Pˆr(x), we
P r(x)
have β(x, y) = P
ˆr(x) . β then can be viewed as a weighting
factor for the source instances and it gives higher weights
where β(x, y) =
ACM-BCB 2012
s
t
1
1
βi ϕ(xˆi ) −
ϕ(xi ) 2
s i=1
t i=1
= arg min
(3)
1 T
2
β Kβ − K̂ T β + const,
s2
st
where ϕ is a mapping function, which maps data of the
source
t and the target into an RKHS; Kij = k(xˆi , xˆj ); K̂i =
1
ˆi , xj ); and const represents an unknown constant
j=1 k(x
t
which could be ignored in the optimization process. The
function k could be an arbitrary kernel function specified
according to the aimed task. In our experiments, we set k
to be the commonly used Gaussian Kernel, which is
k(xi , xj ) =
3.2
(xi − xj )T (xi − xj )
1
exp[−
].
2πσ 2
2σ 2
(4)
Weighted Transductive One Class SVM
OCSVM [26], which bounds data in a circle while minimizing the diameter of the boundary, has been successful used
in many imbalanced datasets. However, it is not applicable
to directly use it in our transductive transfer learning framework. The major difficulty is that each instance is weighted
by β for knowledge transferring. To solve this, we propose
a variant objective function called Weighted Transductive
OCSVM (WTOSVM) which can be expressed as:
min R2 +
2
s
1 ξi ,
sγ i=1
(5)
2
s.t. βi ϕi − O ≤ R + ξi , ξi ≥ 0,
where R is the diameter of the decision boundary; O is the
center of the bounding circle; ξi is the slack variable, which
measures the degree of misclassification of data xˆi ; and γ is
a measurement for the trade-off between a small diameter
of the boundary and a small error penalty.
Using multipliers αi , ζi ≥ 0, we introduce the Lagrangian
as:
L(R, γ, β, ξ, α, ζ) = R2 +
s
i=1
s
1 ξi +
sγ i=1
αi [ βi ϕi − O 2 −R2 − ξi ] −
s
(6)
ζi ξi .
i=1
Set the derivatives with respect to the primal variables R,
212
ξ and O to be zero, yielding:
dL
= 2R(1 −
dR
s
⇒
αi ) = 0
i=1
s
αi = 1,
i=1
dL
1
=
− α i − ζi = 0
dξi
sγ
s
dL
αi (βi ϕi − O) = 0
= −2
dO
i=1
⇒ 0 ≤ αi ≤
⇒O=
s
1
,
sγ
α i β i ϕi .
i=1
(7)
Substituting Equation 7 into Equation 5, and using kernel
function method:
K(x, y) = (ϕ(x) · ϕ(y)),
(8)
we then obtain the dual problem as:
min
s
2
αi βi K(xˆi , xˆi ) −
s s
i=1
αi αj βi βj K(xˆi , xˆj )
i=1 j=1
s
1 αi = 1, 0 ≤ γ ≤ 1.
,
s. t. 0 ≤ αi ≤
sγ i=1
(9)
The optimal value of αi and the corresponding center of
the decision boundary are determined by solving the quadratic
programming (QP) problem in (9). There are many off-shelf
QP solvers which are convenient for such tasks. In our case,
we take advantage of the Optimization Toolbox in MATLAB
to solve the objective function of WTOSVM. The distances
between weighted instances in the source and the center of
the round boundary are:
(10)
DS(xˆi ) = βi ϕ(xˆi ) − O2 .
3.3
Labeling Process
After transferring knowledge from a source to a target
via KMM method, the weighted supervised instances in the
source can then participate in the process of learning on the
unsupervised target. The crucial problems are how to use
the supervised information provided by the weighted source
instances and how to discriminate abnormal instances in the
target. Through the WTOSVM, weighted instances in the
source are re-distributed into a circle and a round decision
boundary is learned. However, labeling instances in the target using the trained decision boundary of the source is impractical for mainly two reasons. First, distances calculated
through parameters trained for the source will be comparatively larger for data in the target because of the discrepancy existing between the distributions of P r and β Pˆr, even
if they are perfectly matched in the kernel means. Second,
labeling data solely by WTOSVM actually adopts an assumption in OCSVM that minorities are sparse and majorities are dense, which may work well if the assumption is met
and cause high bias otherwise.
Notice that in WTOSVM, distance from each weighted
instance to the center is calculated, and the instances with
larger distances are supposed to be abnormal with higher
probability and vice versa. Since there is supervised information of the source, we can estimate the probability distribution of normal instances over different distances as:
s
· yˆi ) · sgn(DS(xˆi ) − d)]
i=1 [sgn(−1
s
,
(11)
pn (d) =
ˆi )
i=1 sgn(−1 · y
ACM-BCB 2012
where pn (d) measures the probability that an instance is
normal given that its distance to the center is d; sgn(x) = 1
if x > 0 and sgn(x) = 0 otherwise. In the same way, we
estimate the probability distribution of abnormal instances
over different distances as:
s
yˆi ) · sgn(d − DS(xˆi ))]
i=1 [sgn(
s
,
(12)
pa (d) =
ˆi )
i=1 sgn(y
where pa (d) measures the probability that an instance is
abnormal given that its distance to the center is d. Using
OCSVM, we can re-distribute instances in the target in the
same way as the source trained by WTOSVM, and the distances between instances in the target dataset and the center
in the round boundary are:
(13)
DT (xi ) = ϕi − OT 2 ,
in which OT is the center of target instances determined by
OCSVM. Our idea of discriminating them is using the distance to calculate the probabilities for normal and abnormal
states, according to the statistically estimated probability
distributions pn and pa in the source. The decision making
process is:
−1 if pn (DT (xi )) > pa (DT (xi )),
yi =
(14)
+1 otherwise.
Our algorithm of transductive transfer learning on imbalanced datasets is then summarized in Algorithm 1. Notice
that this framework is for transductive transfer learning using a single source.
Algorithm 1: ECG Abnormality Detection
via Transductive Transfer Learning
Input: A supervised source S and an unsupervised
target T , a subset Nt ∈ T , kernel covariance σ
and trade-off parameter γ.
Output: The label vector Y for instances in T
1. use subset Nt to weight instances in S through
KMM and obtain weighting vector β.
2. implement WTOSVM on βS to calculate DS, pn
and pa .
3. use OCSVM on T to obtain DT .
4. for i = 1 to t do:
5.
if pn (DT (xi )) > pa (DT (xi )):
6.
yi = −1;
7.
else:
8.
yi = +1;
9.
end if
10. end for.
11. return: Y = {yi }ti=1 .
3.4
Source Selection
Given the above framework for transductive learning on
a target ECG signal with a single source, a noticeable unsolved problem is how to take advantage of different sources
for each target. Considering each source as a decision maker,
then for data in the target, ideally we could combine opinions
from all the sources and make a better decision. However,
it is not the case for our problem because no supervised information is provided for the target. Existing unsupervised
multiple sources ensemble approaches can be divided into
two categories: unweighted and weighted combination. The
former equals the weights of opinions from different decision
makers, ignoring the fact that they should have different
213
suitability and reliability for the same target, causing a lot
of bias and driving down the overall performance; the latter
always assumes that opinions from majority sources should
be close to each other, which does not hold in our cases due
to the difficulty in handling data imbalance. These ensemble
methods will then introduce much randomness into the decision making process. To avoid this and to refrain distraction
of this paper, we will focus on selecting the most reasonable
source for each target, and we present a straight-forward
approach for it based on cross-validation.
In detail, suppose we are going to choose one optimal
source from n well labeled candidate datasets S1 , S2 , S3 , ..., Sn ,
we iteratively set each of them to be the source and other
candidates to be the targets. The source which has the
highest accumulated performance is set to be the optimal
source for an aimed target. The underlying assumption of
this strategy is that a source consistently performs well on
other targets will be a reasonable source for the aimed target. In the experiment, we will experimentally verify this
assumption and show that the simple source selection strategy can obtain results well fitting the highest performance of
each target and outperforms comparative methods in most
cases. Moreover, this source selection framework can be executed beforehand and easily implemented in a parallel way,
which highly decreases the computing time.
4.
EXPERIMENTS
In this section, we demonstrate the effectiveness of the
transductive learning based ECG abnormality detection framework. The algorithm is evaluated on the MIT-BIH Arrhythmias Dataset [18], and compared to a set of baseline approaches. Results show that the proposed framework could
successfully transfer knowledge from sources to targets to
better identify irregular events in ECG signals with significant improvements. Beside these, the optimal source selection method is also experimentally tested. The results
fit the highest performance of each target well and outperform all those of the comparative methods, which verify the
practicality and superiority of our method. Finally, experiments on parameter sensitivity are performed to prove the
robustness of our model against various settings.
4.1
Dataset Description and Preprocessing
The MIT-BIH Arrhythmias Dataset [18] contains 48 half
hours excerpts of ECG signals, obtained from 47 subjects.
Each heart beat is labeled as normal or abnormal by clinical
experts. From it, we randomly picked 10 records, including
the following files: 100, 101, 103, 105, 109, 115, 121, 210, 215
and 232. The preprocessing and feature extraction of each
signal are implemented in a similar way to [17]. The percentage of abnormal instances in each preprocessed dataset
varies from 0.7% to 29.38% with only 9.09% on average,
which indicates these datasets are highly imbalanced.
4.2
Evaluation Metric
The overall accuracy on a test dataset is commonly used
in evaluating the performance of a classifier. However, for
imbalanced datasets, especially in severely imbalanced cases,
overall accuracies could be extremely high even if misclassifying all the minorities to the class of majority, thus alternative measurement is employed here. In the binary classification, we refer minority to be Positive and majority to be
Negative. After obtaining the numbers of four values: TP
ACM-BCB 2012
(True Positive), TN (True Negative), FP (False Positive)
and FN (False Negative), G-Mean [16] is calculated as:
TN
TP
•
.
(15)
G-M ean =
TP + FN TN + FP
The G-Mean is a combinatory measurement on accuracies of the two classes. The range of it is from 0 to 1, and
the higher it is the better the performance is in evaluation.
The reason why we use this measurement is that it is extremely sensitive towards classification errors on minority
instances in severely imbalanced dataset. In some ECG signals, there are only less than 10 abnormal heart beats and
several thousand normal ones, which means a model misclassifying only 1% of the data may have a G-Mean as low
as 0. For this evaluation metric, perfect recognition on most
instances does not guarantee a high outcome.
4.3
Baseline Approaches
We compare the transductive transfer learning based ECG
abnormality detection framework with a set of baseline approaches from both anomaly detection and transductive learning areas, including:
OCSVM [26]: Our model is built upon OCSVM, we
hereby set it as a comparative approach.
Local Distance Based Outlier Factor (LDOF) [29]:
LDOF is a local distance based and unsupervised anomaly
detection method. It defines a distance factor measuring
how much an object deviates from its neighborhood. Objects with higher deviation degree measured by the factor
are supposed to be more abnormal than others. In the implementation, the major difference of this approach to others
is that it requires an estimation of total number of abnormal instances (ECG heart beats). We set the number to be
9.09% of each target dataset, according to the actual average
percentage of minority instances in the datasets.
Clustering Based Outlier Detection (CBOD) [30]:
It is a clustering based unsupervised anomaly detection method.
It assumes that abnormal instances are either in small clusters or far from the centers in large clusters. Partitioning
Around Medoids (PAM) [14] and a defined distance based
factor are used in clustering and detecting outliers in large
clusters, respectively.
Transductive Support Vector Machine (TSVM) [13]:
TSVM is one of the most popular knowledge transferring
method in existing research. It builds the discriminative
structure based on the margin of separating hyperplanes on
both the source and the target data. In experiment, we
implemented it through the SVM light [12].
Modified Bisecting DBSCAN (BRSD-DB) [25]: It
is another transductive learning approach. It estimates the
data structure of both source and target through clustering, and aims to re-balance the distribution of the source
through uniformly drawing samples from each clusters. The
re-balanced source data could then be viewed as supervised
training dataset for the target. In experiment, we use SVM
for the final learning and classification goal.
4.4
Performance Study
The results are summarized in Table 1, where we denote
the name of each dataset by Data Index and mark the highest G-Means over different methods in bold font. For each
target, when using transductive learning approaches including TSVM, BRSD-DB and WTOSVM, other datasets are
214
Data Index
100
101
103
105
109
115
121
210
215
232
OCSVM
0.8713
0.8609
0.8230
0.3343
0.9431
0.7191
0.6734
0.6293
0.6097
0.4665
LDOF
0.5190
0.8662
0.6753
0.4124
0.5331
0.7219
0.6255
0.4631
0.3267
0.2921
CBOD
0.9798
0.8770
0.7701
0.4722
0.9323
0.5248
0.6428
0.6857
0.5989
0.4259
TSVM
0.1715
0.5222
0.3927
0.6079
0.7068
0.4578
0.2671
0.4717
0.8638
0.9676
BRSD-DB
0.5941
0.6735
0.3534
0.5639
0.7269
0.5928
0.2646
0.6867
0.4541
0.9595
WTOSVM
0.9876
0.9444
0.8910
0.7291
0.9056
0.7590
0.7820
0.9063
0.9082
0.9754
Table 1: Compare our method to baselines on the MIT-BIH Arrhythmias Dataset.
ACM-BCB 2012
1
Using Best Sources
0.95
Using Optimal Sources
0.9
G−Mean
iteratively set to be the source and the highest G-Mean of
these results is presented in the table. The parameter settings will be explained in the section Parameter Sensitivity.
In the implementation, we ran our algorithm in MATLAB
using a PC with 3.17 GHz Intel Core 2 Duo processor and
4GB RAM. The average time of classifying an instance by
our algorithm is 0.0127 second, which only takes 1.59% of
the duration of a usual heart beat according to [20].
Since our framework is based on OCSVM, comparison
with it can best verify the effectiveness of our model. It can
be clearly seen that for 9 out of the 10 tasks, the proposed
ECG abnormality detection framework can significantly outperform the original OCSVM method and achieve improvement by 26.79%. The only exception is for Data 109, in
which our result is lower for 0.04. These facts indicate that
in most cases the proposed framework could transfer knowledge from sources into targets successfully, and these transferred knowledge does help in the classification of data in
the targets.
The other two anomaly detection methods also show much
lower performance than ours in most cases. Each of them
can get relatively high G-Means in several cases, and CBOD
can even achieve slightly higher than our method for data
109. However, these two methods show obviously unstable performance over different datasets. Such instability
also exists in TSVM and BRSD-DB. There are two explanations for it. One is due to the sensitivity of the evaluation metric G-Mean, which stresses the misclassification
on minority instances and exaggerates overall performance
variations. Another reason is that all the comparative methods are built based on their proposed assumptions. LDOF
assumes minorities are in ’sparse area’; CBOD makes assumption that abnormal instances are either in small clusters or far from cluster centers; TSVM assumes there are
shared hyperplanes for source and target; and BRSD-DB
assumes clustering could mine the shared data distributions
of sources and targets. Different from them, our method
only assumes that for a given target there are sources that
have close distributions with it, thus can produce more stable performance with enough candidate sources. According to this assumption, the relatively lower performance of
our method on the dataset 109 can be explained as there
is no investigated source having sufficiently close data distribution to it. In spite of this, the result of our method
shows significantly higher stability than those of the comparative methods, demonstrating the robustness of the proposed algorithm. On average, our method improves the
performance of the listed five baseline methods for 26.79%,
0.85
0.8
0.75
0.7
0.65
100
101
103
105
109
115
Data Index
121
210
215
232
Figure 3: Cross-Validation Based Source Selection.
61.68%, 27.18%, 61.86% and 49.72%, respectively.
4.5
Source Selection Study
The experimental results of the cross-validation based source
selection method are shown in Figure 3, in which we denote
the selected sources as Optimal Sources and sources with
best performance as Best Sources. In the results, Optimal
Sources for 100, 103, 121 and 215 are also the Best Sources
for them, thus produce the highest possible G-Means in our
framework. In all the cases, the deviations of the G-Means
using Best and Optimal Sources are less than 0.03, and the
root-mean-square deviation (RMSD) is only 0.0146, proving
that the Optimal Sources well fit the Best Sources.
When compared with the listed baseline approaches, our
method using the Optimal Sources could still outperform
them in 8 out of the 10 ECG signals. For 109, the G-Means
is lowered to 0.8829 and lower than OCSVM and CBOD; and
for 232, the performance is reduced to 0.9531 thus slightly
lower than TSVM and BRSD-DB. However, notice that the
presented G-Means of TSVM and BRSD-DB are for the best
sources of the targets. On average, our method using the
selected optimal sources improves the performance of the
baseline methods for 25.44%, 59.95%, 25.82%, 60.13% and
48.11%, respectively.
4.6
Parameter Sensitivity
There are three parameters in the proposed algorithm,
including the subset N t of a target data which is involved
in the knowledge transferring process, kernel covariance σ
and trade-off parameter γ used in the objective. Traditional
way of setting parameters through experimenting on training data of each target is not applicable due to the fact
215
1
0.9
0.945
Source is Dataset 100 and Target is Dataset 101
0.8
0.7
Source is Dataset 100 and Target is Dataset 101
0.6
G−Mean
G−Mean
0.94
0.935
0.5
0.4
0.93
0.3
0.2
0.925
0.1
0.92
100
200
300
400
500
600
700
Size of the Subset Nt
800
900
1000
0
1100
0
0.1
0.2
0.3
0.4
0.5
0.6
Trade−off Parameter γ
0.7
0.8
0.9
1
Figure 4: Parameter Sensitivity of N t.
Figure 6: Parameter Sensitivity of γ.
that no supervised information exists in target ECG signals
during the learning process. So here, we show some experimental results on parameter sensitivity and give out some
basic principles in setting parameters. Without losing generality, we choose data 100 as the source and data 101 as
the target for the following experiments.
from 0.7 to 0.9. We could hereby consider 0.3 to 0.7 as a
reasonable range for γ and set it to be 0.5 in experiments in
Table 1.
For baseline approaches, we set parameters in the similar
way to the three above experiments. We could also notice
that in spite of the changes caused by parameter variations,
our proposed WTOSVM significantly outperforms the best
baseline method (LDOF when target is 101) in most of the
cases. This proves the robustness of our method against
various parameter settings.
1
0.98
Source is Dataset 100 and Target is Dataset 101
0.96
0.94
5.
G−Mean
0.92
0.9
0.88
0.86
0.84
0.82
0.8
40
60
80
100
Kernel Parameter σ
120
140
Figure 5: Parameter Sensitivity of σ.
The results on the sensitivity of N t is shown in Figure
4. We fixed σ = 100 and γ = 0.5, and then varied the size
of N t from 100 to 1011, where 1011 is the size of the target data 101. In each setting, if the size is K, then first K
instances in the data are set as the subset N t. The performance is relatively stable, with varance = 1.39×10−4 . This
suggests that the subset does not have significant impact on
the performance in these settings. However, to avoid possible randomness caused by insufficient learning instances
and overfitting caused in the opposite way when using other
sources and targets, we set N t to be the top 500 instances
of each target for the experiments shown in Table 1.
To test the sensitivity of σ, we fixed N t to be the top
100 instances and γ = 0.5, and then varied σ from 40 to
140 as shown in Figure 5. It is clearly evident that when
σ rises from 40 to 80, the G-Mean first reaches the lowest
point when σ = 50 then gradually improves. After the point
of 80, the performance stays almost stable until γ ≥ 120.
Therefore a reasonable setting for σ should be chosen from
[80, 120]. For Table 1, we set it to be 100.
In the similar way, we tested the sensitivity of parameter γ
and show it in Figure 6. When varying the value of it from
0.1 to 0.9, the performance of our framework first increases
to a turning point at γ = 0.3 and then keeps almost the same
to γ = 0.7. A hardly observable decrease happens at the end
ACM-BCB 2012
CONCLUSIONS AND PERSPECTIVES
Unsupervised ECG abnormality detection is an important
problem in health informatics and cyber-physical systems
that has not been well investigated. In this work, we take
advantage of well labeled ECG signals, and propose a transductive transfer learning framework to utilize these labeled
source data into the classification of target unsupervised
ECG signals.
The experimental results on the MIT-BIH Arrhythmias
Dataset show that the proposed method could outperform
both anomaly detection and transfer learning baseline models in most of the cases and improve significantly over each of
them for 25% to 60% on G-Mean. A cross-validation based
source selection framework is also presented. It could determine the optimal source for unsupervised learning on each
target, and the related experimental results could well fit the
highest G-Mean for each target and significantly outperform
baselines in most cases, demonstrating the practicality and
superiority of our framework. Moreover, we have also presented the sensitivity for each parameter used in the model,
and given out principles for their settings. In the future,
we plan to investigate ECG abnormality detection based on
transductive transfer learning using multiple sources.
6.
REFERENCES
[1] B. W. Andrews, T.-M. Yi, and P. A. Iglesias. Optimal
noise filtering in the chemotactic response of
escherichia coli. PLoS Computational Biology,
2(11):12, 2006.
[2] M. T. Bahadori, Y. Liu, and D. Zhang. Learning with
Minimum Supervision: A General Framework for
Transductive Transfer Learning. IEEE, 2011.
[3] X. Chang, Q. Zheng, and P. Lin. Cost-sensitive
supported vector learning to rank. Learning, pages
305–314, 2009.
216
[4] N. V. Chawla, K. W. Bowyer, L. O. Hall, and W. P.
Kegelmeyer. Smote: synthetic minority over-sampling
technique. Journal of Artificial Intelligence Research,
16(1):321–357, 2002.
[5] J. Domienik-Karlowicz, B. Lichodziejewska, W. Lisik,
M. Ciurzynski, P. Bienias, A. Chmura, and
P. Pruszczyk. Electrocardiographic criteria of left
ventricular hypertrophy in patients with morbid
obesity. EARSeL eProceedings, 10(3):1–8, 2011.
[6] P. Domingos. MetaCost: A General Method for
Making Classifiers Cost-Sensitive, volume 55, pages
155–164. ACM, 1999.
[7] E. Eskin, A. Arnold, M. Prerau, L. Portnoy, and
S. Stolfo. A Geometric Framework for Unsupervised
Anomaly Detection: Detecting Intrusions in Unlabeled
Data, volume 6, page 20. Kluwer, 2002.
[8] A. Gretton, A. J. Smola, J. Huang, M. Schmittfull,
K. M. Borgwardt, and B. Sch?lkopf. Covariate Shift by
Kernel Mean Matching, page 131ı̈£¡C160. MIT Press,
2009.
[9] M. Guimaraes and M. Murray. Overview of intrusion
detection and intrusion prevention. Proceedings of the
5th annual conference on Information security
curriculum development InfoSecCD 08, page 44, 2008.
[10] Z. He, X. Xu, and S. Deng. Discovering cluster-based
local outliers. Pattern Recognition Letters,
24(9-10):1641–1650, 2003.
[11] J. Huang, A. Smola, A. Gretton, K. Borgwardt, and
B. SchÃűlkopf. Correcting sample selection bias by
unlabeled data. Distribution, 19:601–608, 2006.
[12] T. Joachims. Making large-scale support vector
machine learning practical, pages 169–184. MIT Press,
Cambridge, MA, 1999.
[13] T. Joachims. Transductive inference for text
classification using support vector machines. Most,
pages 200–209, 1999.
[14] L. Kaufman and P. J. Rousseeuw. Finding Groups in
Data: An Introduction to Cluster Analysis, volume 39.
John Wiley Sons, 1990.
[15] S. B. Kotsiantis and P. E. Pintelas. Mixture of expert
agents for handling imbalanced data sets. Annals of
Mathematics Computing and Teleinformatics,
1(1):46–55, 2003.
[16] M. Kubat and S. Matwin. Addressing the curse of
imbalanced training sets: one-sided selection.
Training, pages 179–186, 1997.
[17] P. Li, K. Chan, S. Fu, and S. Krishnan. An abnormal
ecg beat detection approach for long-term monitoring
of heart patients based on hybrid kernel machine
ensemble. Biomedical Engineering, 3541/2005:346–355,
2005.
[18] G. B. Moody and R. G. Mark. The impact of the
mit-bih arrhythmia database. IEEE Engineering in
Medicine and Biology Magazine, 20(3):45–50, 2001.
[19] M. Nakatsuji, Y. Miyoshi, and Y. Otsuka. Innovation
detection based on user-interest ontology of blog
community. Innovation, 4273(1):9–11, 2006.
[20] P. Palatini. Resting heart rate. Heart, 33:622–625,
1999.
[21] D. Patra, M. K. Das, and S. Pradhan. Integration of
fcm , pca and neural networks for classification of ecg
ACM-BCB 2012
arrhythmias. International Journal, (February), 2010.
[22] B. Quanz and J. Huan. Large margin transductive
transfer learning. Proceeding of the 18th ACM
conference on Information and knowledge management
CIKM 09, page 1327, 2009.
[23] S. Ramaswamy, R. Rastogi, and K. Shim. Efficient
algorithms for mining outliers from large data sets.
ACM SIGMOD Record, 29(2):427–438, 2000.
[24] G. Ranganathan and K. College. Ecg signal processing
using dyadic wavelet for mental stress assessment.
Engineering, 2010.
[25] J. Ren, X. Shi, W. Fan, and P. S. Yu.
Type-independent correction of sample selection bias
via structural discovery and re-balancing, page
565âĂŞ576. Citeseer, 2008.
[26] B. SchÃűlkopf, J. C. Platt, J. S. Shawe-Taylor, A. J.
Smola, and R. C. Williamson. Estimating the support
of a high-dimensional distribution. Neural
Computation, 13(7):1443–1471, 2001.
[27] C. G. M. Snoek, M. Worring, J. C. Van Gemert, J.-M.
Geusebroek, and A. W. M. Smeulders. The challenge
problem for automated detection of 101 semantic
concepts in multimedia. Proceedings of the 14th
annual ACM international conference on Multimedia
MULTIMEDIA 06, pages 421–430, 2006.
[28] L. I. Xin-fu, Y. U. Yan, and Y. I. N. Peng. A New
Method of Text Categorization on Imbalanced
Datasets, pages 10–13. 2008.
[29] K. Zhang, M. Hutter, and H. Jin. A new local
distance-based outlier detection approach for scattered
real-world data. Advances in Knowledge Discovery and
Data Mining, 5476:813–822, 2009.
[30] B. A. Zoubi. An effective clustering-based approach
for outlier detection. European Journal of Scientific
Research, 28(2):310–316, 2009.
217