CERTIFICATE OF LIABILITY INSURANCE
advertisement

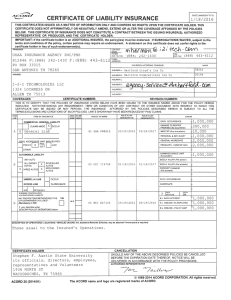
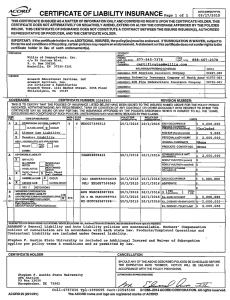
DATE (MM/ODIYYYY) CERTIFICATE OF LIABILITY INSURANCE 4/ 15/2016 THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THIS CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZED REPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER. IMPORTANT: If the certificate holder is an ADDITIONAL INSURED, the policy(ies) must be endorsed. If SUBROGATION IS WAIVED, subject to the terms and conditions of the policy, certain policies may require an endorsement. A statement on this certificate does not confer rights to the certificate holder in lieu of s uch endorsement(s). PRODUCER Hylant Group, Inc. - C leveland 6000 Freedom Sq Dr, Ste 400 Independence OH 44131 INSURED I FAX , (AJC, SHERCOM-01 The Sherwin-Williams Company 101 W . Prospect A venue Cleveland O H 4411 5 No.):2,_,_,,=::LLC:::uL.:""'-- -1 =-:JJ:LI"-lo<.1..UJ.J.l'<J-ll.....__""""..><.1....u...uuW<J."""'' - - - - -- - -p.>L"-'"'"--- --f INSURER B INSURER.fC_j:~t.J:.J[JLlJ!Il.QieOMIJ~S...J.(is_;!.£Q_ _ _ _ __ _~W,l!L_ _ , D~:- - IN SURER""'_:_ _ _ _ _ _ __ INSURER_E INSURER F : REVISION NUMBER: CERTIFICATE NUMBER: 387100928 COVERAGES THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIOD INDICATED. NOTWITHSTANDING ANY REQUIREMENT, TERM OR CONDITION OF ANY CONTRACT OR OTHER DOCUMENT WITH RESPECT TO WHICH THIS CERTIFICATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS, EXCLUSIONS AND CONDITIONS OF SUCH POLICIES. LIMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS. ADUL SUBR INSR ~IOLICY EFF() I l OLICY EXfvi LIMITS TYPE OF INSURANCE POLICY NUMBER M/ODIYYYY MM/00/YYY IN~~ wvn LTR 5/1/2017 511/2016 HDOG274054B4 A EACH OCCURRENCE GENERAL LIABILITY s2.ooo.ooo 5/1/2017 5/1/2016 HDOG27405496 A IJAMA l.>t. TO Kt.NI t.U x COMMERCIAL GENERAL LIABILITY $2,000,000 PREMISF!'; IFa occurrence\ person) one (Any EXP MED s CLAIMS.MADE ~ OCCUR I - D I ~ GEN'L AGGREGATE LIMIT APPLIES PER: n 1 ~r-& POLICY ti:"OMOBILE LIABILITY xi A ANY AUTO ALL OWNED t-----1 AUTOS X ~ HIRED AUTOS X LOC ISA H09042416 AUTOS NON.OWNED ~ AUTOS I I ~ EXCESS LIAB I B c A I I OCCUR 5/1/2016 5/1/2017 RETENTION s OED WORKERS COMPENSATION AND EMPLOYERS' LIABILITY YIN ANY PROPRIETORIPARTNERIEXECUTIVE ~ N / A OFFICERIMEMBER EXCLUDED? (Mandatory In NH) If~· dosalbo ood« Excess Workers' Comp and Employers Llab s2.ooo.ooo GENERAL AGGREGATE S10,000,000 PRODUCTS · COMP/OP AGG Prod/Comp Ops Ea Occ $10,000,000 $5,000,000 _fu'.:;:~~~_tu _;>n• \iLt LIMI I ldentl BODILy INJURY (Per person) ~.000000 $ BODILY INJURY (Per accident) $ ~OPERTY DAMAGE $ Per accident) s I I EACH OCCURRENCE - $ ~ I CLAIMS·MADE - D SCRIPTION OF OPERATIONS below A I ~ SCHEDULED ~ UMBRELLA LIAB PERSONAL & ADV INJURY r-- --- H AGGREGATE s $ 5/1/2017 15/1/2017 5/112017 5/112016 5/1/2016 51112016 WLRC4B60206A SCFC4B6020B3 WLRC 48602071 x 1T~~;m1¥;; 1 E.L. EACH ACCIDENT 1 °1~· s2.ooo.ooo E.L. DISEASE - EA EMPLOYEE s2.ooo.ooo E.L. DISEASE· POLICY LIMIT 12,000.000 I I I 5/1/2017 5/1/2016 WCUC4B602095 Wor1<ers' comg Employers Lia Statutofuo $2,000, I I DESCRIPTION OF OPERATIONS I LOCATIONSI VEHICLES (Attach ACORD 101, Addltlonel Remar1ts Schedule, Ir more space Is required) ALL LOCATIONS AND OPERATIONS OF THE NAMED INSURED AND ITS DIVISION S IN ALL STATES. WC SELF-INSURED STATES: A L,AR,CA ,FL,GA, IL,IN, KS, KY,LA,MD,MA,Ml,MO , NJ. N Y, NV,NC, OH, OK,PA, SC,TN,TX.VA CANCELLATION CERTIFICATE HOLDER STEPHEN F. AUS TIN STAT E UNIVERS ITY PURCHASING DEPARTMENT PO BOX 13030 NACOGDOCHES TX 7 5962 SHOULD ANY OF THE ABOVE DESCRIBED POLICIES BE CANCELLED BEFORE THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN ACCORDANCE WITH THE POLICY PROVISIONS. AUTHORIZED REPRESENTATIVE flJJJ._~~ C 1988-2010 ACORD CORPORATION. All rights reserved. ACORD 25 (2010/05) The ACORD name and logo are re gistered marks of ACORD