I
advertisement

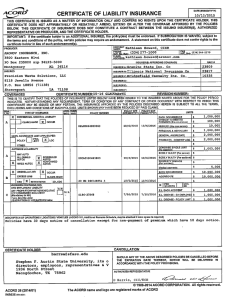
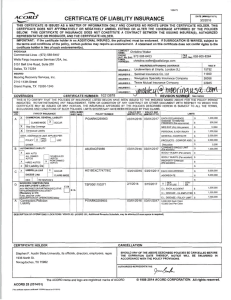
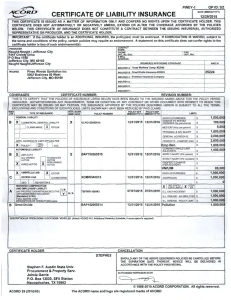
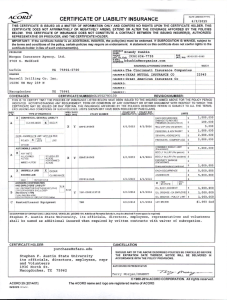
3 ACORD I CERTIFICATE OF LIABILITY INSURANCE ~ DATE (MM/DD/YYYY) 6/ 12 /2015 THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THIS CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZED REPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER. IMPORTANT: If the certificate holder is an ADDITIONAL INSURED, the policy(ies) must be endorsed . If SUBROGATION IS WAIVED, subject to the terms and conditions of the polic y , certain policies may req uire a n endorsement. A statement on this certificate does not confer rights to the certificate holde r in lie u of such endorsement(s). ~2:1~CT Rhonda Wood PRODUCER M o rga n Ins ura n ce Agency, 3708 s. I IA/C FAX Nol: (936)632-3862 ~H~NJnExtl: (936)634-7755 Ltd. ~D~~ss: rwood@morganins.com Medford INSURER(S) AFFORDING COVERAGE Lufkin 7590 1 -5700 TX NAIC # INSURER A :ALLIED INSURANCE COMPANIES INSURED INSURER B :TEXAS MUTUAL INSURANCE CO Greater Overhead Door Company of Lufkin LLC , OBA : 10575 HWY 90 West 22945 INSURERC : INSURER D : INSURER E : Beaumont 77713 TX COVERAGES INSURER F : CERTIFICATE NUMBER:CL1561 203 1 77 REVISION NUMBER: THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIOD INDICATED. NOTllVITHSTANDING ANY REQUIREMENT, TERM OR CONDITIO N OF ANY CONTRACT OR OTHER DOCUMENT WITH RESPECT TO WHICH THIS CERTIFICATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS, EXCLUSIONS AND CONDITIONS OF SUCH POLICI ES. LIMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS. INSR ADDL SUBR POUCYEFF POLICY EXP l uft•~ TYPE OF INSURANCE LIMITS LTR POLICY NUMBER IMM/DD/YYYYl IMM/DD/YYYYl x COMMERCIAL GENERAL LIABILITY 1,000 ,000 EACH OCCURRENCE $ ,____ DAMAc;t; I U RcNTED 100 ,000 CLAIMS·MADE OCCUR A $ PREM1<:s::<: fEa occurrence' ACP7216206000 6/10/2015 6/10/2016 5,000 MED EXP (Any one person) $ ,___ ... ~~ w D ~ GEN'L AGGREGATE LIMIT APPLIES PER: ~ POLICY D r;~8-r D Loc A ~ ,___ ,___ x ,____ A B 1 , 000,000 $ 2,000 , 000 PRODUCTS · COMP/OPAGG $ 2,000 ,000 COMBINED SINGLE LIMIT tEa accidenll BODILY INJURY (Pe< person) ANY AUTO ALLOVVNED AUTOS .....__ HIRED AUTOS ~ UMBRELLA LIAS $ GENERAL AGGREGATE $ OTHER: AUTOMOBILE LIABILITY ,___ x PERSONAL & ADV INJURY - H EXCESS LIAS SCHEDULED AUTOS NON·OVVNED AUTOS ACP7216206000 6/10/2015 6/10/2016 OCCUR CLAIMS·MADE I I OED RETENTION$ WORKERS COMPENSATION AND EMPLOYERS' LIABILITY ANY PROPRIETOR/PARTNER/EXECUTIVE OFFICER/MEMBER EXCLUDED? (l,land<1f "')' '"NH) If yes, descnbe under DESCRIPTION OF OPERATIONS below ACP7216206000 6/10/20 15 D Underinsured molonst $ 1 ,000,000 EACH OCCURRENCE $ 4 000 000 AGGREGATE $ I OTH· I PER STATUTE I ER E.L. EACH ACCIDENT N /A TSF-0001289095 6/10/2015 6/10/2016 1 , 000 ,000 $ BODILY INJURY (Pe< accidenl) $ PROPERTY DAMAGE $ !Per accidenll 6/10/2016 YIN $ $ $ 1 000 000 E.L. DISEASE • EA EMPLOYEE $ 1 000 000 E.L. DISEASE · POLICY LIMIT 1 000 000 $ DESCRIPTION OF OPERATIONS I LOCATIONS I VEHICLES (ACORD 101, Addilional Remarks Schedule, may be attached if more space Is required) CANCELLATION CERTIFICATE HOLDER ( 936 )4 68-4282 purchase@sfasu.edu Stephen F Austin State University, its officials, director s, employee , representatives and vol unteers 1936 North St. Nacogdoc hes, TX 75962 SHOULD ANY OF THE ABOVE DESCRIBED POLICIES BE CANCELLED BEFORE THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN ACCORDANCE WITH THE POLICY PROVISIONS. AUTHORIZED REPRESENTATIVE Terry Morgan/RHON DA -;r-~~ © 1988-2014 ACORD CORPORATION . ACORD 25 (2014/ 01) INS025 (2014011 The ACORD name and logo are registered marks of ACORD All rig hts reserved.