HEALTH POLICY AND PUBLIC HEALTH IN SPAIN AND FRANCE: COMPARING EUROPEAN UNION
advertisement

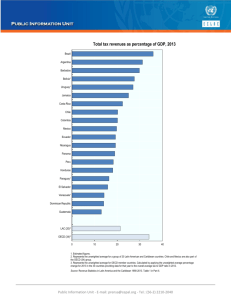
HEALTH POLICY AND PUBLIC HEALTH IN SPAIN AND FRANCE: COMPARING EUROPEAN UNION NATIONAL HEALTH SYSTEMS Public Health, Comparative Health Policy and Law in the European Union: A Transatlantic Dialogue F. SEVILLA April 24-25, 2006 WELFARE STATE • “LIBERAL” MEANS-TESTED ASSISTANCE MODEST UNIVERSAL TRANSFERS (USA, AUSTRALIA) • NATIONAL INSURANCE MODELS – SOCIAL INSURANCE MODEL RIGHTS ATTACHED TO WAGE-EARNERS UNIVERSAL ACCESS PAID BY STATE PRIVATE INSURANCE & OCCUPATIONAL FRINGE BENEFITS HAVE A MARGINAL ROLE STATE’S REDISTRIBUTIVE ROLE: SMALL (GERMANY, AUSTRIA, FRANCE) – UNIVERSAL MODEL RIGHTS ATTACHED TO CITIZENSHIP STATE’S REDISTRIBUTIVE EFFECTS: SUBSTANTIAL (SWEDEN, NORWAY, DENMARK) F.Sevilla Madison 06 HEALTH CARE SYSTEMS MODELS NATIONAL HEALTH SERVICE NATIONAL HEALTH INSURANCE LIBERAL WELFARE STATE MODEL UNIVERSAL SOCIAL INSURANCE LIBERAL RIGHT TO SERVICES YES YES NO MEANS-TESTED FINANCING TAXES WAGES CONTRIBUTIONS INSURANCE POLICIES Direct COVERAGE UNIVERSAL TENDENCY UNIVERSAL % UNINSURED % UNDERINSURED BENEFITS EQUAL TENDENCY EQUAL Insurance Policy USER’S CHOICE RESTRICTED PROVIDER YES ALLOCATION RESOURCES ADMINISTRATIVE CONTRACTS MARKET HEALTH CENTERS OWNERSHIP PUBLIC PUBLIC/PRIVATE PRIVATE CONTROL SYSTEM ADMINISTRATION SOCIAL PARTNERS ? F.Sevilla Madison 06 PUBLIC SOCIAL EXPENDITURE %GDP 35,00 30,00 25,00 20,00 15,00 10,00 5,00 0,00 Canada France Germany Mexico Spain United States EU15 average 1990 18,61 26,61 22,80 3,84 19,55 13,37 23,27 1995 19,62 29,24 27,46 5,43 21,39 15,40 25,44 2001 17,81 28,45 27,39 5,10 19,57 14,73 23,86 Source: OECD Fact Book 2006 TOTAL TAX REVENUE %GDP 50,0 45,0 40,0 35,0 30,0 25,0 20,0 15,0 10,0 5,0 0,0 Canada France1 Germany Mexico Spain United States EU15 average 1990 35,9 42,2 35,7 17,3 32,1 27,3 39,3 1995 35,6 42,9 37,2 16,7 31,8 27,9 40,1 2000 35,6 44,4 37,2 18,5 34,8 29,9 41,7 2003 33,8 43,4 35,5 19,0 34,9 25,6 40,5 Source: OECD Fact Book 2006 CITIZENS DEMAND TAXES WAGES CONTRIBUTION INSURANCE POLICIES OUT OF POCKET PAYMENTS FINANCIAL ALLOCATIONS EQUITY EFFICIENCY HEALTH GAIN EMPOWERMENT (Competitive / Cooperative) BENEFITS GUARANTEE Financing/Coverage Results Management Organization EXPENDITURES PURCHASES INVESTMENT KNOWLEDGE&DEVELOPMENT HUMAN RESOURCES POLICIES PROFESSIONAL RULES CONTRACTS: Control & Results LONGITUDINAL CARE QUALITY POLICIES CHOICE EFFICIENCY CENTERS SUPPLY HEALTH CARE SERVICES F.Sevilla Madison 06 SPAIN • Health Care System: – Universal, in transition from a Social Security Model – Decentralized to the Regional Governments • Financing: Taxes – CentralG to guarantee Equity and Solidarity – RegionalG to finance Health Care Expenditures • Provision: Mostly public, owned and managed • Territorial Organization: – Health Areas: Hospital care – Health Zones (less 25.000 inhabitants): Primary Care F.Sevilla Madison 06 SPAIN (2) • Access: – Free except Ambulatory Pharmacy – Choice of GP inside Health Area – No Hospital Choice • Health delivery system: Integrated – Primary Health Care: Health Care Centers in a Professional team, Gatekeeper role: • • • • Health Promotion Health Prevention Curative care: GPs, Pediatrician, nurses Follow-up patients – Hospital Care: • Inpatient care • Ambulatory specialized care including Ambulatory surgery • Emergency care F.Sevilla Madison 06 SPAIN (3) • Payment Professionals: Salary, status similar to civil servants • Problems: – Coordination of care • Primary-Hospital • Health-social care – Waiting times for elective surgery – Comfort and administrative procedures – Staff Satisfaction F.Sevilla Madison 06 FRANCE • Health Care System: – Social Security Model – UNIVERSAL COVERAGE – Centralized: • STATE: Regulation, Public Health and “National Expenditure Ceiling” • Health Insurance Funds: General (84%), Rural (7,2%), SelfEmployees (5%), Others (3,8%) • Financing: Wage Contributions • Provision: – Liberal: Ambulatory care – Hospitals: Public 25%, Private non profit 35%, for profit 40% F.Sevilla Madison 06 FRANCE (2) • Territorial Organization – GP’s and Ambulatory care Specialists: Freedom of Installation – Hospital Sector: Regional Strategic Health Plan & Medical Map • Access: – Direct Payment with reimbursement afterwards (voluntary coinsurance) – Statutory copayments, exemption is granted (chronic conditions,…) – Choice of Practitioner – Choice of Hospital F.Sevilla Madison 06 FRANCE (3) • Health Delivery System: – Public Health Services – Ambulatory care: • Curative care • Self-employed professionals: Physicians, Dentists, nurses • GP’s can play a role of gatekeepers – Hospital Care • Private: focus on surgical procedures • Public: focus on emergency, rehabilitation, longterm and psychiatric care F.Sevilla Madison 06 FRANCE (4) • Payment Professionals – Fee for service: Ambulatory care and Private Hospitals – Salary: Public hospitals • Problems: – High Health Expenditure – No financial risk to Insurance Funds – Coordination of care – Shortage of Professionals F.Sevilla Madison 06 HEALTH STATUS HEALTH: STATUS Life expectancy at birth years Women Men Fertility rate Infant mortality Children per woman per 1 000 live births 15-49 Total 2003 Tobacco consumption % of population smoking daily Overweight or obese Obese population population % total pop. BMI>25 kg/m 2 % total pop. BMI>30 kg/m 2003 1993 2003 1993 2003 1993 2003 2003 1993 Canada 82,1 77,2 79,7 1,52 1,66 5,4 6,8 17,0 25,5 46,5 14,3 12,1 France 82,9 75,8 79,4 1,89 1,65 3,9 6,5 28,6 29,0 37,5 9,4 6,6 Germany 81,3 77,4 75,5 78,4 1,34 72,4 74,9 2,40 1,28 4,2 3,04 20,1 5,8 29,6 24,3 26,4 22,9 25,1 49,2 62,3 12,9 24,2 .. .. 83,7 80,7 79,9 77,2 80,5 1,29 76,2 78,5 1,71 74,5 77,2 2,04 1,27 1,75 2,05 6,7 6,3 8,4 28,1 26,0 17,5 32,1 27,0 20,4 48,4 62,0 65,7 13,1 23,0 30,6 8,8 15,0 23,3 Mexico Spain United Kingdom1 United States1 Source: OECD Health Data 2005 4,1 5,3 7,0 2 LIFE EXPECTANCY AT BIRTH, TOTAL POPULATION 2003 1960 67,8 81,8 Japan Iceland Spain Switzerland1 Australia Sweden Italy Canada1 Norway France New Zealand1 Netherlands Austria United Kingdom Finland Germany Luxembourg1 Greece Belgium1 OECD Ireland1 Portugal United States1 Denmark Korea1 Czech Republic Mexico Poland Slovak Republic1 Hungary Turkey 72,9 80,7 69,8 80,5 71,6 80,4 70,9 80,3 73,1 80,2 69,8 79,9 71,3 79,7 73,6 79,5 70,3 79,4 71,3 78,7 73,5 78,6 68,7 78,6 70,8 78,5 69,0 78,5 69,6 78,4 69,4 78,2 69,9 78,1 70,6 78,1 68,5 77,8 70,0 77,8 64,0 77,3 69,9 77,2 72,4 77,2 52,4 76,9 75,3 70,7 57,5 74,9 74,7 67,8 73,9 70,6 72,4 68,0 48,3 68,7 90 Source: OECD Health Data 2005 80 70 60 Years 50 40 INFANT AND NEONATAL MORTALITY RATES, 2003 Iceland 2,4 Infant mortality Japan 3,0 Neonatal mortality 3,1 Finland 3,1 Sweden Norway 3,4 Czech Republic 3,9 3,9 France 4,1 Portugal 4,1 Spain 4,2 Germany 4,3 Belgium 4,3 Italy 4,3 Switzerland 4,4 Denmark 4,5 Austria 4,8 Australia 4,8 Greece 4,8 Netherlands 4,9 Luxembourg 5,1 Ireland 5,3 United Kingdom 5,4 Canada1 5,6 New Zealand2 6,1 OECD 6,2 Korea3 6,9 United States 7,0 Poland 7,3 Hungary 7,9 Slovak Republic 20,1 Mexico 29,0 40 Source: OECD Health Data 2005 30 1. 2002. 2. 2001. 3. 1999 Turkey 20 10 0 Deaths per 1 000 live births HEALTH SPENDING HEALTH: SPENDING AND RESOURCES Health spending and financing Public expenditure Pharmaceutical Total as % of total Average Health expenditure expenditure as % of expenditure as expenditure on growth rate Per capita USD PPP total expenditure on % of GDP health health 2003 1993 2003 1993 1998-2003 2003 1993 2003 1993 Acute care beds per 1 000 population Practising physicians Per 1 000 population MRI scanner units Per million population 2003 1993 2003 1993 2003 1993 Canada 9,9 9,9 69,9 72,7 4,2 3 003 2 014 16,9 13 3,2 3,6 2,1 2,2 4,5 1,0 France 10,1 9,4 76,3 76,5 3,5 2 903 1 878 20,9 17,5 3,8 4,9 3,4 3,2 2,8 1,4 Germany Mexico 11,1 9,9 78,2 80,2 6,2 5,8 46,4 43,2 1,8 4 2 996 1 988 14,6 583 397 21,4 13,2 .. 6,6 1,0 7,7 .. 3,4 1,5 2,9 1,4 6,0 0,2 1,4 .. Spain 7,7 7,5 71,2 76,6 2,6 1 835 1 089 21,8 19,2 3,1 3,5 3,2 2,5 7,3 2,1 United Kingdom 7,7 6,9 83,4 85,1 15 13,2 44,4 43,1 5,7 4,6 2 231 1 232 15,8 5 635 3 357 12,9 14,8 8,6 3,7 2,8 3,9 3,5 2,2 2,3 1,7 1,9 5,2 8,6 .. 5,9 United States2 Source: OECD Health Data 2005 HEALTH EXPENDITURE AS SHARE OF GDP, 2003 15,0 United States Switzerland Germany Iceland Norway France Canada Greece Netherlands Belgium (1) Portugal Sweden Australia (2) Denmark OECD Hungary Italy New Zealand Japan (2) Spain United Kingdom (2 Austria Czech Republic Finland Ireland Turkey Luxembourg Poland Mexico Slovak Republic Korea 11,5 11,1 10,5 10,3 10,1 9,9 9,9 9,8 Private 9,6 9,6 9,4 Public 9,3 9,0 8,8 8,4 8,4 8,1 7,9 7,7 7,7 7,5 7,5 7,4 7,4 7,4 6,9 6,5 6,2 5,9 5,6 15 10 5 0 % of GDP 1. Public/private data refers to current health expenditure. 2. 2002. Source: OECD Health Data 2005 HEALTH EXPENDITURE AND GDP PER CAPITA, 2003 Health expenditure per capita 6 000 USA 5 000 4 000 CHE NOR LUX ISL DEU CA N NLD FRA B EL DNK A US SWE A UT IRL GB R JPITA N GRC FIN ESP P RT NZL 3 000 2 000 CZE KOR SVK P OL M EX TUR HUN 1000 0 0 20 000 40 000 GDP per capita (USD P P P ) Source: OECD Health Data 2005 60 000 Source: OECD Health Data 2005 9,6 9,5 Austria Czech 7,5 7,4 7,4 Mexico Slovak Poland Korea 9,0 9,7 Finland Turkey 9,8 Italy Spain 10,2 10,0 Japan (2) 11,0 Ireland 10,3 11,1 OECD Hungary 11,2 11,3 Greece 11,2 11,4 Portugal Australia (1) 11,6 Sweden Luxembourg 11,9 12,3 France 11,8 12,4 Canada Belgium 12,5 Netherlands Denmark 12,6 13,8 0 Germany 4 13,9 7,8 8 Norway 12 Iceland 17,0 15,5 16 Switzerland United States CURRENT HEALTH EXPENDITURE, 2003 Share of final consumption 20 SHARE OF POPULATION AGED 65 AND OVER 20 19 18 18 17 16 16 16 14 13 12 12 12 12 10 10 9 9 8 8 6 5 4 2 0 ITALY GERMANY SPAIN FRANCE UNITED KINGDOM 1960 Source: OECD Health Data 2005 2003 CANADA UNITED STATES MEXICO Ja p K an o M rea ex Tu ico G rke r y S Hueec lo n e N vak ga et R ry he e r p P land . or s t P uga ol l S an w d ed en O E C U D A aK us vg t Fi rali nl a Ire and C Ca lan ze n d ch ad D Ra en ep m . Fr ar G an k er c m e an S w itz It y er aly la S nd pa i U n A SA N B ust ew e ria l Zegiu al m an d 0 0,0 0,0 0,0 0,0 Source: OECD Health Data 2005 0,1 0,1 0,2 0,2 0,2 0,1 0,3 0,3 0,4 0,4 0,4 0,4 0,4 0,3 0,6 0,5 0,5 0,5 0,5 0,5 0,5 0,5 0,7 0,8 0,8 0,7 1,2 1,2 1,1 Heart transplants 2003 Number of transplants per 100 000 population 1,4 1 Ja Tupan Ic rke e y M lan Lu ex d x K ic S emor o lo b ea va o k urg R G ep A ree . us c tra e lia N I ew P ta Zeola ly al nd an d G er U mK O Fi an E nl y C a D D and en v g H ma un rk g Ire ar P la y or n C tug d a a S nad l w a e Fr de N B an n et el ce C hergiu z la m S ech nd w R s itz e er p . N lan or d A wa us y t S ria pa i U n SA 1 1,0 0,9 0,7 2 2,1 1,9 1,8 1,8 1,6 3 Source: OECD Health Data 2005 4 4,0 3,9 3,7 3,7 3,6 3,5 3,5 3,4 3,4 3,3 3,3 3,1 3,1 3,0 2,9 2,8 2,7 2,7 2,7 5 0 5,2 5,1 4,7 4,6 Kidney transplants 2003 Number of transplants per 100 000 population 6 Source: OECD Health Data 2005 3 1 4 9 13 11 16 21 21 20 19 18 19 17 24 30 29 29 29 34 33 2003 43 40 40 39 39 37 40 9 8 9 8 9 18 20 1990 U SA 0 0 6 13 24 30 5 4 4 10 1980 S pa in A us tri a D en m N ar ew k Ze al an d A us tra lia Fr an ce O E C D av g P or tu ga l Fi nl an d C an ad a 2 10 U K G er m an y Ic el an d Functioning kidney transplants, 1980, 1990 and 2003 Number of patients per 100 000 population 50 EUROPEAN SOCIAL MODEL VALUES • SOLIDARITY AND EQUITY • REJECTIONS OF ALL FORMS OF DISCRIMINATION • GENDER EQUALITY • UNIVERSAL ACCESS TO EDUCATION AND HEALTH CARE OF GOOD QUALITY • EMPLOYMENT, PROTECTION AGAINST UNEMPLOYMENT • PENSIONS F.Sevilla Madison 06 EUROPEAN SOCIAL MODEL CHARACTERISTICS • EUROPE IS DEFINED BY ITS DIVERSITY • THE EUROPEAN SOCIAL MODEL IS NOT MONOLITHIC • THERE ARE DIFFERENT MODELS AND POLICY CHOICES TO DEVELOP THE COMMON VALUES • SUBSIDIARITY: POLICIES MUST BE DESIGNED AND IMPLEMENTED AT THE LEVEL WHICH IS THE MOST EFFECTIVE • EMPLOYMENT AND SOCIAL POLICIES ARE ESSENTIALLY OF THE DOMAIN AND COMPETENCES OF MEMBER STATES • SOCIAL POLICY IS SEEN AS A PRODUCTIVE FACTOR IN THE MOST DYNAMIC COUNTRIES F.Sevilla Madison 06 EU HEALTH CARE: LEGAL FRAMEWORK • PRINCIPLE OF TERRITORIALITY AND SUBSIDIARITY: The responsibility lies with the Member States • SOCIAL SECURITY COORDINATION: a mechanism was set up in 1958 to ensure workers mobility. No discrimination. Recognition of Social Security benefits elsewhere in the Union • EU’s ROLE IS MAINLY SUPPORTING, COORDINATING AND COMPLEMENTARY • EUROPEAN COURT OF JUSTICE: to make compatible the national systems and the free movement. Only barrier to hospital access and only in case of similar treatment at home F.Sevilla Madison 06 WHO MIGHT SEEK HEALTH CARE ABROAD? • TEMPORARY VISITORS: E-111 scheme -enables to obtain care abroad in the event of an emergency- / health care insurance card – TOURISM: Young, Active Life – BUSINESS TRAVEL • LONG-TERM RESIDENTS ABROAD: Health care entitlement is transferred to the new residence country – TOURISM: Retired, social care – WORK • “EUROPEAN CONMUTERS”: There is not yet mechanisms to link two health care entitlements • PEOPLE USING FACILITIES LOCATED IN BORDER REGIONS: Hospital of Puigcerda (SpanishFrench Border); double-access eligibility of frontier workers • PEOPLE SENT ABROAD BY THEIR OWN HEALTH FUNDER: E-112 scheme, Highly-specialized facilities, pre-authorization required F.Sevilla Madison 06