BIO PHOTONICS Photonics-based In Vivo total hemoglobin monitoring and clinical relevance
advertisement
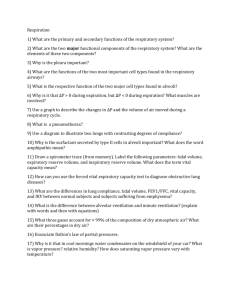
J. Biophoton. 2, No. 5, 277–287 (2009) / DOI 10.1002/jbio.200910019 Journal of BIOPHOTONICS REVIEW ARTICLE Photonics-based In Vivo total hemoglobin monitoring and clinical relevance John McMurdy1, Gregory Jay1; 2, Selim Suner1; 2, and Gregory Crawford *; 1; 3 1 2 3 Division of Engineering, Brown University, Providence, RI 02912, USA Department of Emergency Medicine, Rhode Island Hospital, Providence, RI 02903, USA College of Science and Department of Physics, University of Notre Dame, Notre Dame, Indiana 46556, USA Received 28 October 2008, revised 10 February 2009, accepted 6 March 2009 Published online 22 April 2009 Key words: Anemia, hemoglobin, spectroscopy, tissue optics, noninvasive PACS: 81.15.M, 82.80.d, 87.85.Ox, 87.85.Pq Anemia is a serious disorder which, as a result of antiquated invasive blood testing, is undiagnosed in millions of people in the U.S. As a result of the clinical need, many technological solutions have been proposed to measure total blood hemoglobin, and thus diagnose anemia, noninvasively. Because hemoglobin is the strongest chromophore in tissue, spectroscopic methods have been the most prevalently investigated. Difficulties in extracting a quantitative estimation of hemoglobin based on tissue absorption include variability in the absorption spectra of hemoglobin derivatives, interference from other tissue chromophores, and interpatient physiological variations affecting the effective optical pathlength of light propagating in tissue. In spite of these challenges, studies with a high degree of correlation between in vitro and in vivo measured total hemoglobin have been disclosed using variants of transmission and diffuse reflection spectroscopy in assorted physiological locations. A review of these technologies and the relevant advantages/disadvantages are presented here. Reflectance image of blood vessels in the sublingual mucosa from a healthy (top) and anemia (bottom) patient collected using the orthogonal polarization spectral imaging technique to enhance vessel contrast. Adapted from [7]. # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim * Corresponding author: e-mail: gregory_crawford@nd.edu # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim Journal of BIOPHOTONICS 278 1. Introduction Anemia is clinically defined as a significant reduction (two standard deviations) in either the number of red blood cells (RBCs) per unit volume of whole blood, the amount of packed RBCs per unit volume of whole blood, or most generally the amount of the oxygen/CO2 transporting protein hemoglobin (Hgb) from the clinically determined ‘normal’ value [8]. It is vital to screen for anemia as it has been reported to affect 2 billion people worldwide, or roughly onethird of the worlds population [9]. Anemia is a complication of dietary deficiencies including iron deficiency, vitamin B12 deficiency, and folic acid deficiency, but also appears concurrent with more serious disorders including cancer, HIV/AIDS, leukemia, chronic kidney disease, and rheumatoid arthritis. The appearance of anemia with numerous disorders makes Hgb concentration monitoring a vital parameter in assessing overall public health. Invasive determination of blood hemoglobin levels through the complete blood count (CBC) remains the most clinically embraced method of anemia detection. Parameters of the CBC are obtained using biochemical assays, flow cytometry, and analysis of blood smears, contemporarily in a fully integrated workstation. Although remaining invaluable as a test for many specific anemias, CBCs are time consuming, costly, and increase risks of phlebotimist exposure to blood-borne pathogens. If the full CBC results are not necessary, blood can be centrifuged in a small volume device at the bedside providing a hematocrit (Hct, volume fraction of RBC’s and roughly correlated with Hgb) determination; however, this remains an invasive technique and creates cross-contamination possibilities for neighboring patients and physicians. In the contemporary climate of non-invasive diagnostics, the CBC and finger prick methods remain antiquated. While it is not anticipated that non-invasive techniques in their infancy will provide as much diagnostic information as the CBC, screening technologies will alert physicians to a patients Hgb level and encourage further investigation. Repeated anemia screening is necessary high-risk demographics including pregnant women, children, and the elderly, all drawing great benefit from rapid non-invasive anemia detection. This need propelled studies as early as the 80’s on conductive and early optical techniques of total hemoglobin/hematocrit monitoring [1, 6]. More recently, the necessity of enhanced techniques to rapidly screen for anemia has resulted in investigations on numerous non-invasive methods, the majority of which are based on interrogation of light-tissue interactions. Presented here is a brief discussion of the clinical decision making altered by the presence of such advice, the fundamental tissue spec- # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim J. McMurdy et al.: In vivo hemoglobin determination troscopy challenges to overcome in extracting Hgb concentration, and a survey of the most recent photonics-based methods of detection reported in the literature. 2. Clinical decision making There are numerous clinical circumstances where rapid determination of Hgb is vital and other situations where immediate knowledge of Hgb can be used to enhance patient care. With the development of non-invasive, rapid, low cost, painless devices which could be easily used with little training, Hgb can be added to the list of variables collected from each patient during every health care encounter (vital signs) such as blood pressure, heart rate, temperature, respiratory rate, blood oxygen saturation (SpO2 ) and blood glucose concentration. Any entry point to the health care system such as emergency departments, clinics and doctors offices universally measure vital signs. In the future, insertion of technological advances in engineering, materials science, photonics and chemistry to the bedside will expand this list. Patients who arrive to the emergency department, of which there were 119.2 million during 2006 in the United States, require proper triage to determine which group must be seen immediately [10]. The median time for emergency department visits is 2.6 hours with only 21.9% of patients seen within 15 minutes of arrival. Objective data such as vital signs, available to the clinician, make the rapid triage decision more accurate. Adding Hgb to vital signs obtained at the point of triage will enhance the triage process and improve patient care by immediately identifying patients with severe anemia and reducing their wait times. In most instances, new technologies related to vital sign monitoring are rapidly adopted by the emergency medical services community and integrated into ambulance services, indeed the use of electrocardiography and pulse oximetry were rapidly adopted by EMS shortly after being implemented and most recently carboxyhemoglobin monitoring has been incorporated into EMS practice almost simultaneously with hospital based health care systems. The use of these technologies by EMS allows objective data to be collected in the ambulance even before the patient arrives in the emergency department. We envision light, non-invasive, inexpensive devices that measure Hgb will follow this trend and make it into the pre-hospital setting. Anemia is most prevalent in developing countries where nutritional resources and access to health are lacking. Also, these regions of the world have parasitic and other diseases, which contribute to anemia. Anemia leads to higher infant mortality, loss of man- www.biophotonics-journal.org REVIEW ARTICLE J. Biophoton. 2, No. 5 (2009) power and productivity in the work force and exacerbates co-morbid disorders such as heart disease. These are precisely the communities where wide spread surveillance could be used to identify anemia and institute treatment measures. However, current screening and detection methods rely on an established healthcare infrastructure, which is often lacking in these regions of the world. An inexpensive and point of care device to measure Hgb could be deployed in this context for surveillance. Non-invasive Hgb measurements can also be used for continuously monitoring patients with frequent repeated testing since the Hgb in the blood changes slowly (on the order of hours, even with massive blood loss). This application can be particularly useful for those patients with on-going hemorrhage, those receiving blood transfusion or hemodialysis and patients undergoing major surgical procedures. It is difficult to assess what a clinically acceptable level of accuracy in monitoring total hemoglobin concentration may be. This is directly tied to the intended use of the device and the individual making a decision on the patients care. For example, in using the device as a continuous monitor of total hemoglobin, the required error levels may be significantly less than 1.0 g/dL in order to observe trends. Alternatively, in using the device as a rapid screening tool, an error level of 1.0 g/dL may be tolerable as subsequent testing will be required. The situation and how the information will change a patients course of treatment will ultimately determine the acceptance of these performance levels. 279 A ¼ " c l, where " is the molar extinction coefficient of the analyte, c is the concentration of the analyte, l is the optical pathlength integrating the refractive index. While this is a straightforward calculation in an in vitro controlled environment, in an in vivo tissue model it becomes significantly more complex. In the case of a transmission measurement system, cellular structures such as nuclei and cell membranes contribute a significant amount of optical scatter to the system having the effect of artificially increasing the optical pathlength. As the scattering properties are wavelength dependent, changes in scatter not only have the effect of changes overall intensity, but distort spectral signatures through wavelength dependent pathlength variation. Additionally, the structure itself may vary in thickness (e.g. changing finger/earlobe thickness from person to person) while the volume of blood experienced during propagation can also vary as a result of both physiological variability and from pulsatilechanges in vessel diameter. Diffuse reflectance measurements suffer from these same sources of error, explicitly changing blood volumes and a combination of scattering and layer thickness variations affecting the average penetration depth of light into the tissue and distorting spectral signatures. What results are equations for transmission and reflected intensity calculated from steady state diffusion theory with a dependence on numerous parameters as shown in Eq. (1). Rd ðlÞ ¼ e B pffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi 3ð1þms ðlÞ ð1gÞ ma ðlÞÞ ð1Þ There exists fundamental technological challenges in determining Hgb concentration quantitatively using an optical or photonics based solution. In general, these difficulties arise from inter-patient variation in physiological characteristics causing significant deviation in experimental conditions from one patient to the next. Three of the most significant concerns in quantitatively measuring Hgb are fluctuations in the concentrations of melanin and other chromophores, the presence of several hemoglobin derivatives, and changes in optical path length used in a Beer-Lambert law calculation. Here, I1 and I0 are the output and input intensities, respectively, ma is the absorption coefficient where ma " c, ms is the scattering coefficient describing the concentration of scattering particles and their scattering efficiency (which may or may not be the same as absorption particles), g is the scattering anisotropy describing the directionality of scatter, and B is some tissue dependent constant. Explicitly modeling all of these parameters for each patient is not feasible, thus alternative methods of reconciling this source of error have been explored, as are discussed here. One such technique may be using the absorption spectra of water or another biomarker to calibrate for this pathlength variability; however, this has yet to be successfully implemented in conjunction with hemoglobin monitoring. 3.1. Optical pathlength 3.2. Hemoglobin variants Determination of the unknown concentration of an analyte of interest through diffuse reflectance or transmissive spectroscopy methods is based upon the Beer-Lambert law, which states the absorption Although differences in the absorption spectra between hemoglobin species are exploited to determine relative amounts of each in saturation measurements, they acts as an interference to determining 3. Technology considerations www.biophotonics-journal.org # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim Journal of BIOPHOTONICS 280 Figure 1 Absorption spectra in the NIR regime of oxy-, deoxy-, met-, and carboxyhemoglobin. Adapted from [11]. the summation of these species, termed total hemoglobin (Hgb) concentration. The primary derivatives of hemoglobin that may be observed in significant concentration levels in many disorders are methemoglobin (MetHb) and carboxyhemoglobin (HbCO), both of which have differing absorption spectra from normal oxyhemoglobin (HbO2 ) and deoxyhemoglobin (Hb). As is the case in normal hemoglobin, these derivates vary significantly in the NIR spectral regime (as pictures in Figure 1) and there exist no isosbestic points between all four. As a result, extraction of total hemoglobin (Hgb ¼ HbO2 þ Hb þ HbCO þ MetHb) becomes more complex requiring many wavelength bands to discern these species. J. McMurdy et al.: In vivo hemoglobin determination amount of oxyhemoglobin to oxy- plus deoxyhemoglobin has the effect of normalizing the pathlength term and all other constant terms out of the equations, making determination of the saturation capable in a highly variable population. Determining the actual concentration of one of these species, or the summation for total hemoglobin, unfortunately does not have the same benefit ofpatient independence, and thus in this case the same predictive model cannot be utilized. However, recent efforts have been made to vary pulse oximetry optics and modify signal processing to create a CO-oximeter capable of using comparable pulsatile signals to determine methemoglobin [12], carboxyhemoglobin [13] concentration, and total hemoglobin concentration [14]. This technology along with other technologies to resolve the pathlength fluctuation issue are discussed later in Section 4. In spite of the challenges, many groups have investigated alternative technologies to try and achieve the success of the pulse oximeter for Hgb. This approaches are broadly categorized here into two classes, NIR transmission spectroscopy systems and visible/NIR diffuse reflectance spectroscopy systems. A summary of these devices is presented in the following two sections. It is important to note that the accuracy and correlation values are given as a gross reference point and not an absolute indicator of the device potential. These studies were all carried out under different clinical conditions with different patient populations, different invasive methods used as benchmarks, and different comparison techniques. 3.3. Melanin and other interference analytes 4. Transmission spectroscopy technologies Complicating interpatient changes in optical pathlength are fluctuations of other chromophores unrelated to Hgb. Primary chromophores in the visible spectral regime, in addition to total Hgb and its derivates, include melanin, various flavins, cytochrome-coxidase, carotenoids and extravasated hemoglobin and its derivatives induced through hemorrhage or contusion. Absorption at longer wavelength NIR radiation also includes contributions from myoglobin, other cytochromes, and water (at wavelengths longer than 1 mm). Although the extinction coefficient of most of these species is small compared to that of Hgb, the net effect of the sum of all these factors can vary significantly from patient to patient and from tissue to tissue, creating a significant source of error to extracting pure Hgb quantitative information. Interestingly, pulse oximetry overcomes many of these interpatient variations to determine systolic pulse hemoglobin saturation by performing calculation based on the change in absorption during systole and diastole periods. Looking at the relative # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim The primary physiological location used for transmission spectroscopy quantification of Hgb is the fingertip [14–23], enabling many similar probe configurations utilized in pulse oximetry to be exploited. A brief discussion of the state of art in these devices and their ability to overcome the challenges discusses in Section 3 is presented here. One method of directly monitoring changes in optical pathlength through the fingertip is reported by Aldrich et. al. [21]. NIR transmittance through the fingertip at a single wavelength (905 nm, non-isosbestic for oxy- and deoxyhemoglobin) is used in conjunction with acoustic transducers to kinetically quantify both the bulk thickness of the tissue segment and small variations in this thickness from blood vessel dilation during systole. Sonomicrometers are positioned at opposite sides of the finger to estimate the effective optical pathlength and subsequent pulsatile pathlength variation, as is shown in Figure 2(a). Transmitted intensity of the 905 nm NIR LED through the finger at this same position is then www.biophotonics-journal.org REVIEW ARTICLE J. Biophoton. 2, No. 5 (2009) Figure 2 Setup of transcutaneous illumination coupled with path length modulation detection using sonomicrometer transducers (a) and the detected variation in light intensity corresponding to the sonomicrometer detected variation in optical pathlength (b). Adapted from [21]. normalized by this acoustically determined optical pathlength and correlated to an in vitro Hgb determination. Figure 2(b) shows this pathlength and transmission variation during systolic pulsation. This group reports a correlation r ¼ 0.84 (n ¼ 24) for Hgb, sensitivity and specificity of 94% and 78% for detecting anemia respectively, and mean predictive error of 1.1 g/dL for Hgb. While the acoustic method of pathlength monitoring can account for interpatient fingertip thickness changes through signal intensity normalization, sources of error remain from varying blood volume fractions, scattering properties, and interfering analytes which are not rejected in the processing method currently described. It remains unclear in this case (1) whether the difference in transmitted intensity between the minimum and maximum sonomicrometer determined pathlength can be used to normalize for tissue variation and correlate to Hgb and (2) how the use of sonomicrometers might be suited ina true clinical application. Jeon et. al. disclosed an alternative method of pathlength correction in fingertip transmissive Hgb measurement using the pulse varying optical signal themselves [20]. On transcutaneous illumination of the finger with visible/NIR diodes, as light diffuses through the fingertip, a fraction interacts with the arterial vessels while another fraction interacts only with veins and soft tissue in the fingertip, as is shown in Figure 3. As a result, photons reaching the photodetectorafter passing through an arterial vessel are subject to pulsatile modulation in intensity from changing vessel diameter (and subsquent interaction www.biophotonics-journal.org 281 length with whole blood) while photons bypassing the arterial vessel remain constant during pulsatile waveforms. The ratio of pulsatile varying signals to constant signals is then used to minimize effects from pathlength variation and interference from other analytes. This group initially reported correlation r ¼ 0.80 (n ¼ 129) and standard deviation of error (standard error) of 1.14 g/dL for Hgb relative to in vitro determined levels using the aforementioned ratio as a correlation variable [20] and has since estimated potential clinical performance to a correlation of r ¼ 0.87 and standard error of 0.81 g/dL with a more optimized finger probe [24]. This degree of performance is achieved using a five diode array with multiple wavelength ratios found to most effectively reject additional errors from saturation state and wavelength dependent tissue scattering changes. Additionally, other earlier studies have shown similar signal processing techniques to extract Hgb concentration using pulsatile variation in pathlength in transmission through the earlobe with correlation coefficient r ¼ 0.79 (n ¼ 14) [25]. Although the change in vessel diameter and thus blood volume during systole provides a method to determine Hgb in the presence of other varying factors, the change in vessel diameter is often only a few percent, making this signal modulation relatively weak. An alternative method is to create an artificial variation in local Hgb concentration and thus transmitted intensity by artificially controlling blood flow. Enhancement though artificial blood volume fraction modulation has been explored by several groups. Gravenstein et. al. was one of the earliest to discuss this type of measurement when disclosing a canine animal model using volumetric constriction of blood flow to measure Hgb noninvasively [23]. An 810 nm diode laser was transilluminated through a canine tongue while a micrometer was used to restrict blood flow through applied pressure. Diluting Hgb concentration using an intravenous NaCl solution, variations in transmitted signal were correlated to applied pressure in each canineleading to a corre- Figure 3 Schematic of light diffusing through the fingertip artery showing a fractional portion propagating through a pulsatile varying vessel and fraction remaining stable with pulse. Adapted from [20]. # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim Journal of BIOPHOTONICS 282 lation range of r ¼ 0:87 0:97. Although this technique showed efficacy in dynamically monitoring Hgb, discrepancy between the correlation of NIR transmission with applied pressure precluded an assessment of the ability of this technique to measure interpatient Hgb concentration noninvasively [23]. More contemporarily, Rendell et. al. has explored modulating NIR transmission through the fingertip using inserts that volumetrically constrict and release blood flow [19]. The modulation in transmitted intensity with different inserts is then correlated to Hgb using a linear regression method. A regression algorithm applied to the artificially modulated signal intensities achieves an optimal correlation r ¼ 0.862 (n ¼ 121) and mean error of prediction of 1.28 g/dL for Hgb compared to invasively determined levels. A second group has explored a similar method they term occlusion spectroscopy which utilizes combined fingertip transmission specroscopy and blood flow modulation [26, 27, 15]. Transmitted intensity is varied by occluding blood flow using a restrictive finger cuff (similar to a blood pressure cuff) accelerating ischemia driven red blood cell aggregation. The occluding finger cuff is later released allowing red blood cells to disaggregate while the changein optical transmission at multiple NIR/visible wavelengths is monitored [28]. This enhancement in contrast using the difference of these two signals enables a more accurate parameter correlation to Hgb. Figure 4 shows an in vitro demonstration of the change in blood transmission, attributed to the variation in scattering properties, observed during pulsations of blood in a capillary tube. The most recently reported clinical performance of this technology shows a correlation coefficeint r ¼ 0.9 (n ¼ 309) and standard error values of 3.3% (for hematocrit), or 1.0 g/dL (using the relationship Hgb(g/ dL) ¼ 0.34 Hct(%)) [15]. A third variant of this class of technology also uses a finger cuff to modulate the volume of blood flow into the finger and measure transcutaneous optical absorptions to infer Hct, having shown a correlation r ¼ 0:78 ðn ¼ 121Þ for Hct in the most recent published results [16]. Figure 4 In Vitro demonstration of the change in optical scattering and thus transmission during pulsatile action attributed to variation in red blood cell aggregates. Adapted from [28]. # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim J. McMurdy et al.: In vivo hemoglobin determination Alternatively, implementing an imaging device in a pulse oximetry probe configuration allows for a direct determination of Hgb by monitoring the transmitted intensity and imaging the blood vessels probed in vivo. Kanashima et. al. has recently reviewed the performance of a NIR imaging based noninvasive Hgb monitor in patients with and without hematological disorders [17, 29, 22]. Photometric absorbance measurements from the vascular portions of the image using multiple discrete NIR bands are coupled with an estimation of the blood vessel optical pathlength. This pathlength is estimated based on in vivo imaged vascular diameter, and assuming circular vessel cross sections. Intensity measurements can then be normalized for changing optical pathlength, and Hgb subsequently correlated to this parameter, again using regression analysis. This group discloses sensitivity and specificity of 78.3% and 69% for clinically defined anemia, respectively, with correlation r ¼ 0.53 for anemic patients (n ¼ 174), correlation r ¼ 0.34 (n ¼ 135) for patients with normal Hgb levels, and an overall correlation r ¼ 0:591 ðn ¼ 309Þ for all measurements [17]. It is unclear why this recent study has shown this device tobe so much more inaccurate than an earlier report disclosing a correlation r ¼ 0.896 (n ¼ 91) [22]. While this technique has the benefit of correction for blood vessel dilation with pulse, a significant source of error remains due to other chromophores influencing transmitted intensity independent of Hgb and vessel diameter. This is likely why the authors report a high precision in single patient Hgb tracking, but observe a significant drop in accuracy in determining interpatient Hgb concentration from a single reading. 5. Reflectance spectroscopy and imaging technologies Various approaches using diffuse reflectance have also been examined. Reflectance spectroscopy and imaging can be advantageous as deep transmission through highly scattering turbid tissue is not necessary, but rather properties of blood vessels proximal to the surface can be probed. Unfortunately, issues still arise from other absorption events affecting reflected signal. Also, the pathlength variation problem persists, manifesting as a variability in photon penetration depth that is dependent on tissue layers absorption, reflectance, and scattering properties, and can result in nonlinear intensity responses with linear variation in Hgb concentration. Reflectance based methods mitigating these challenges can be grouped as either reflectance and spectral reflectance imaging based modes or single point detection reflection spectroscopy modes. www.biophotonics-journal.org REVIEW ARTICLE J. Biophoton. 2, No. 5 (2009) 283 5.1. Imaging based modalities In the case of highly superficial blood vessels, as is the case in many vessels of mucosal surfaces (retina, sublingual mucosa, tongue, conjunctiva), hemoglobin concentration can be estimated through reflectance imaging with multiple wavelength bands and subsequent image processing analysis. Mucosal blood vessels are the most desirable access point to estimate blood component parameters due to the lack of thick overlaying tissues, and subsequent minimization of other interfering analytes not related to whole blood. One of the most interesting imaging based methods of in vivo Hgb determination is orthogonal polarization spectral (OPS) image analysis of the vascular network in the sublingual mucosal surface [7, 30–32]. Hemoglobin is determined based upon a computational estimation of vascular network density from collected images and the intensity of reflectance signal from the vessel area. Images collected using OPS imaging of the microvascular network for anemic and healthy patients are shown in Figure 5(a–d). A polarized light source in a spectral region of high hemoglobin absorbance (550 nm) is used to illuminate the vasculature while a polarizer at 90 with respect to incident light polarization is placed at the detection focal plane. The detection plane polarizer only transmits light that has been depolarized through scattering after penetrating superficial tissue layers, enhancing the proportion of photons detected that interact with microvasculature and rejecting light reflected through Fresnel reflection at the surface. An image-processing algorithm is then applied to the OPS image data to estimate Hgb based on the optical density over a number of individual vessels. This group has reported a correlation r ¼ 0.93 (n ¼ 71). Interestingly, high resolution OPS images can also potentially be used to infer morphological red blood cell characteristics such as mean corpuscu- Figure 6 Two SD-LCI images of the retina where blood vessels are denoted by white arrows. Properties such as the depth and slope of intensity decrease are correlated to total Hgb. Adapted from [36]. lar volume and abnormal shaped RBC seen in sickle cell anemia. Complementary standard imaging analysis (not OPS based) has also been applied to both blood vessels in the retina [33] using multiple discrete NIR/visible bands propagated through the pupil with a correlation r ¼ 0.89 ðn ¼ 24Þ, and much earlier using blood vessels in the bulbar conjunctiva through high magnification assessment of capillary bed absorption [34]. A more complex variant of reflectance imaging, spectral domain low coherence interferometry (SDLCI) [35], has been used to probe the Hgb dependent absorption and scattering profiles of retinal vessels [36]. SD-LCI is a type of optical coherence tomography, a technique already widely implemented in retinal vessel imaging to assess various retinal disorders. Penetration depth of photons into a blood vessel is inversely related to the scattering coefficient, which in turn is correlated to the hematocrit. This generates a reflectivity depth profile for each individual blood vessel which, when determined with an LCI technique, can be used a parameter to correlate with Hct. As most of the light scattered from a blood vessel is in the forward direction, minimal intensity is projected back into the collection system and thus long integration/exposure times are required. As a result, a retinal tracking system is also implemented to maintain fixation on the vessel of interest in the presence of rapid eye movements. Figure 6 shows two SD-LCI images of retinal blood vessels where the vessel absorption notches used to estimate Hct are indicated. Although this technique is still in the pilot study stage, it is a creative one that can be implemented with OCT systems used for other purposes in an ophthalmology setting. An initial data set of seven volunteers has estimated normal HCT ranges for both males and female [36]. 5.2. Single point detection Figure 5 Microcirculation images collected using OPS imaging of a healthy patient (a, b) and an anemic patient (c, d). Reproduced with permission from [7]. www.biophotonics-journal.org Inferences on hemoglobin concentration can also be made from light after diffusing through a tissue segment of interest and collecting on a single detector. These single point measurements are effectively collecting signal over a summation of many diffuse photon pathlengths. Estimation of hemoglobin con- # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim Journal of BIOPHOTONICS 284 centration is then made based on this signal summation using a regression technique of some sort. In essence, while often more simplistic than transmission approaches, this indirect method of hemoglobin monitoring the quality of the prediction becomes a function of the consistency of data collection conditions and subsequent reliability of the calibration model in a fluctuating physiological environment. In the scope of identifying optical properties of the skin, studies have disclosed the ability to determine contributions to scattering and absorption coefficients attributed to cutaneous hemoglobin [2–5]. The studies discussed here are limited to those which have disclosed measurement of total hemoglobin concentration concentrations. In one approach, steady state visible and NIR diffuse reflectance spectra were collected from the dorsal side of the arm and correlation to Hgb using regression methods [37]. Diffuse reflectance spectra were collected using a 10 nm resolution commercial diffuse reflectance spectrometer equipped with integrating sphere. A classical least squares linear regression analysis and leave-one-out cross validation of the absorbance data resulted in correlation r ¼ 0.8 and standard error of 0.9 g/dL for Hgb prediction. Wavelength regions found to be most correlated to Hgb/Hct were logically similar to those used optically to assign an erythema index using reflectance spectroscopy. This group interestingly explored the effects of thermal modulation on tissue diffusion characteristics, shown to modify absorption and scattering coefficients through changing cutaneous blood flow [38], and demonstrated improved predictive accuracy by controlling skin temperature correlation r ¼ 0.8 ðn ¼ 26Þ and standarderror of 0.8 g/dL for Hgb in patient set with 10 light-skinned patients tested multiple times (total data points n ¼ 26). This study also points out the drop in predictive accuracy with an ethnically diverse patient set, correlation r ¼ 0.6 (n ¼ 28) and standard error of 1.2 g/dL for Hgb, resulting from the variability in melanin concentration affecting tissue diffusion, which is not factored in the regression analysis. Zhang et. al. reported on the utility of a similar visible/NIR diffuse reflectance spectroscopy technique using the probe pictured in Figure 7. This group focused more on the ability to monitor inpatient Hgb Figure 7 Reflectance probe to detect HCT (a) and a close up of the irradiation, collection fibers in the probe (b). Reproduced with permission from [39]. # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim J. McMurdy et al.: In vivo hemoglobin determination fluctuation during operative procedures, in this case cardiopulmonary bypass. Collecting both diffuse reflectance spectra and determining Hct through in vitro fingerstick method, a correlation is made to concentration fluctuations during the procedure. Using a partial least squares regression, this group reports an intra-patient correlation r ¼ 0.844 (n ¼ 10 patients) between the fingerstick and diffuse reflectance method, but only an interpatient correlation r ¼ 0.509 when comparing cross patient data using a single PLS model. This group has reported variations of this technology with similar results in additional human patient studies [40] as well as animal models [41]. In both of these cases, correlating diffuse reflectance signals to Hgb or Hct showns a low degree of correlation as a result of the high variability in optical parameters from one patient to the next. This technique is likely more suited as it is applied in the latter study, to track hemoglobin fluctuations dynamically, as the tissue properties other than Hgb are more consistent in sequential measurement from an individual patient One method of minimizing the effects of varying tissue properties is to collect a diffuse reflectance spectra from a mucosal surface, as explored in the imaging systems above. This can have the advantage of simplifying the device to a single point spectrometer, but making the calibration and regression analysis less susceptible to variation in tissue optical properties. Our group has disclosed the use of visible reflectance spectroscopy analyzing the palpebral conjunctiva (inner lining of the eyelid) as a method of noninvasively monitoring Hgb [42, 43]. Diffuse reflectance spectra were collected from the palpebral conjunctiva and analyzed using a partial least squares regression calibration and leave one out cross validation with the prediction set also used as the calibration set. A correlation r ¼ 0.92 ðn ¼ 30Þ and standard error of 0.67 g/dL were obtained for Hgb in the initial trial using a opthalmoscope-type configuration (pictured in Figure 8(a)), while a second study showed correlation r ¼ 0.82 ðn ¼ 102Þ and standard error of 1.05 g/ dL using a fiber optic reflectance probe (pictured in Figure 8(b)). Both these data sets were across an eth- Figure 8 Experimental configurations to collect diffuse reflectance spectra from the palpebral conjunctiva using a slit-lamp type configuration (a) and fiber optic array reflectance probe (b). www.biophotonics-journal.org REVIEW ARTICLE J. Biophoton. 2, No. 5 (2009) nically diverse population to demonstrate the potential advantages of the palpebral conjunctiva over other tissue segments, reported by physicians as the optimal physiological location to quantitatively look for pallor to identify severe anemia [44]. The ideal configuration for a reflection device is most likely a hybrid of these two classes of device, a high resolution spectral imaging device implemented to blood vessels of a mucosal surface. This can minimize background effects while maintaining reliability of Hgb determination across a diverse group of patients and conditions. 6. Conclusions and future directions While research has been ongoing in this field for twenty five years, and intensely over the past ten years with more cost effective optical component solutions, the actual clinical adoption of one of these technologies will be a result of two factors, the ability to integrate the device with current standards of care and the accuracy and reliability of results across a random patient demographic. In the current standard of care, devices that can be implemented as modified pulse oximeters are likely the strongest candidate for rapid adoption. This may or may not be a function of the long term performance of the device, but more in the infrastructure in place and familiarity of staff and patients with this device. Particularly if Hgb can be inferred from physiological variation and not an extrinsically induced event, the shift from the current pulse oximeter to a higher functioning device will be more straightforward. Regarding accuracy, blood vessels in mucosal surfaces hold the highest potential as a gateway access point to monitoring Hgb and other blood parameters. Regardless of how much engineering is integrated into the transmissive type devices, the fundamental limits of interpatient variability in many optical parameters limit the theoretical performance. In the case of vessels under a thin mucous layer, these effects are significantly minimized yielding the potential for higher performing devices using less advanced instrumentation and signal processing. However, it remains to be seen if quantitatively probing a new physiological location (retina, sublingual mucosa, palpebral conjunctiva) can overcome the adoption barrier to change the standard of care rather than embrace current practices. It is clear that many of these technologies are ready or close to ready for application and the coming years will show which is found to be the best solution. Acknowledgements The authors wish to acknowledge financial support for their own research from the NASA GSRP Program (NNG05GL57H) and RI Science and www.biophotonics-journal.org 285 Technology Advisory Committee (STAC) Grant and thank members of the Display and Photonics Laboratory for feedback on manuscript preparation. Conflict of Interest Authors are working with and have a financial interest in Corum Medical, a company pursing one technology for measuring anemia noninvasively. John McMurdy recently completed his Ph.D. in biomedical engineering at Brown University, USA, under the support of a NASA Graduate Student Researcher Program Fellowship. The scope of his research has been in the clinical testing of spectroscopic techniques and the design of compact and inexpensive optical sensors to non-invasively measure blood components. Dr. McMurdy’s expertise is in spectroscopic techniques and spectral processing, liquid crystal optics, and biomedical optical diagnoses methods. He has authored nine peer-reviewed publications as well as three book chapter contributions. In addition to a three year NASA GSRP award, he has also been awarded three consecutive SPIE educational scholarships and an Advanced E-Team Grant from the National Collegiate Inventors and Innovators Alliance to foster commercialization of a non-invasive anemia sensor in third world and impoverished countries. Gregory Jay is an Associate Professor in the Department of Emergency Medicine and Division of Engineering at Brown University, USA. He also serves as an Adjunct Professor in the Department of Biomedical Sciences at the University of Rhode Island. In addition to his academic activities, he brings over 15 years of experience as an emergency medicine physician, and he is currently employed in that capacity by University Emergency Medicine Foundation, practicing at Rhode Island Hospital and Miriam Hospital in Providence, Rhode Island. Dr. Jay, who holds an M.D., Ph.D. (in Biophysics) and double bachelor degrees (in engineering and biochemistry) from State University of New York at Stony Brook, is a member of numerous professional societies and holds over a dozen issued patents and pending patent applications. He has published 50+ articles in medical and scientific journals and is a recipient of support form NIH. # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim Journal of BIOPHOTONICS 286 Selim Suner graduated from Brown Medical School after completing a Masters degree in Biomedical Engineering, also at Brown University, USA. Dr. Suner, who is on the staff at Rhode Island Hospital and the director of Disaster Medicine and Emergency Preparedness in the Department of Emergency Medicine, completed the Brown University/Rhode Island Hospital Residency Program in Emergency Medicine. He is currently an associate professor of Emergency Medicine, Surgery and Engineering at Brown University. Dr. Suner is the leader of the Rhode Island Disaster Medical Assistance Team (DMAT), and he has served during multiple disaster deployments including the responses to Hurricane Katrina, the World Trade Center attacks and the Egypt Air crash off the shores of Massachusetts. Dr. Suner also serves as Chairman of Rhode Island Hospital Emergency Preparedness Committee. He is an international expert in emergency preparedness and disaster medicine and has given over a 100 lectures related to disaster management, world-wide. Gregory Crawford is currently the William K. Warren Foundation Dean of the College of Science and Professor Physics at Notre Dame University, USA. Previously, he was the Dean of Engineering at Brown University and formerly the Richard and Edna Salomon Assistant Professor and Assistant Professor of Engineering at Brown University. His basic research interests include liquid crystals, polymers, and their application in display technology, telecommunications, and medical device technology. Professor Crawford did his postdoctoral work at the Naval Research Laboratory in Washington D.C. focusing on electroclinic and ferroelectric materials for fast switching spatial light modulator applications. He received his B.S. in both Physics and Mathematics and a Ph.D. from Kent State University where he performed his doctoral research at the Liquid Crystal Institute and NSF ALCOM Center. He has over 200 research publications, review articles and book chapters, and holds 14 US patents. # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim J. McMurdy et al.: In vivo hemoglobin determination References [1] K. I. Yamakoshi, H. Shimazu, T. Togawa, M. Fukuoka, and H. Ito, Non-invasive measurement of hematocrit by electrical admittance plethysmography technique. Ieee Transactions on Biomedical Engineering 27(3), 156–161 (1980). [2] G. Zonios, J. Bykowski, and N. Kollias, Skin melanin, hemoglobin, and light scattering properties can be quantitatively assessed in vivo using diffuse reflectance spectroscopy. Journal Of Investigative Dermatology 117(6), 1452–1457 (2001). [3] H. Yang, S. Xie, H. Li, and Z. Lu, Determination of human skin optical properties in vivo from reflectance spectroscopic measurements. Chinese Optics Letters 5(3), 181–183 (2007). [4] T. Shi and C. A. DiMarzio, Multispectral method for skin imaging: development and validation. Applied Optics 46(36), 8619–8626 (2007). [5] G. Zonios and A. Dimou, Modeling diffuse reflectance from semi-infinite turbid media: application to the study of skin optical properties. Optics Express 14(19), 8661–8674 (2006). [6] J. M. Steinke and A. P. Shepard, Reflectance measurements of hematocrit and oxyhemoglobin saturation. American Journal of Physiology 253(1), 147–153 (1987). [7] R. G. Nadeau and W. Groner, The role of a new noninvasive imaging technology in the diagnosis of anemia. Journal Of Nutrition 131(5), 1610S–1614S (2001). [8] M. B. Pugh, editor. Stedman’s Medical Dictionary. Lippincott, Williams and Wilkins, Baltimore, MD, 27th edition, 2000. [9] R. J. Stoltzfus, Defining iron-deficiency anemia in public health terms: A time for reflection. Journal Of Nutrition 131(2), 565S–567S (2001). [10] C. W. Burt. National Health Care Statistics, 7, 2008. [11] J. G. Webster, Design of Pulse Oximieters. Institute of Physics Publishing, Bristol, UK, 1997. [12] S. J. Barker, J. Curry, S. Morgan, and W. Bauder, New pulse oximeter measures methemoglobin levels in human volunteers. Anesthesia & Analgesia 102, S5, 2006. [13] S. Suner, R. A. Partridge, A. Sucov, J. Valente, K. Chee, and G. D. Jay, Non-invasive pulse co-oximetry for carboxyhemoglobin screening in the emergency department: Identifying occult carbon monoxide toxicity. Journal of Emergency Medicine 34(4), 441–450 (2008). [14] Mark R. Macknet, Suzanne Norton, Penny L. KimballJones, Richard L. Applegate, Robert D. Martin, and Martin W. Allard, Noninvasive measurement of continuous hemoglobin concentration via pulse CO-Oximetry. CHEST 132(4, Suppl. S), 493S–494S, OCT (2007). [15] Alain Berrebi, Orna Amir, Aharon Weinstein, Emmanuel Monashkin, and Paul Holland, A non-invasive evaluation of hemoglobin with a new optical sensor. BLOOD 108 (11, Part 1): 381A, NOV 16 (2006). [16] J. S. Powell, C. J. Gresens, D. Miller, W. Dummer, and P. Holland, Non-invasive measurement of hematocrit to screen potential blood donors. Transfusion, 45(3), 157A–157A (2005). Suppl. S. www.biophotonics-journal.org REVIEW ARTICLE J. Biophoton. 2, No. 5 (2009) [17] H. Kanashima, T. Yamane, T. Takubo, T. Kamitani, and M. Hino, Evaluation of noninvasive hemoglobin monitoring for hematological disorders. Journal Of Clinical Laboratory Analysis 19(1), 1–5 (2005). [18] I. Fine, D. Geva, O. Amir, and E. Monashkin, Clinical evaluation of non-invasive hemoglobin (hb) testing device. American Society of Anesthesiologists Annual Meeting 1, A597 (2004). [19] M. Rendell, E. Anderson, W. Schlueter, J. Mailliard, D. Honigs, and R. Rosenthal, Determination of hemoglobin levels in the finger using near infrared spectroscopy. Clinical And Laboratory Haematology 25(2), 93–97 (2003). [20] K. J. Jeon, S. J. Kim, K. K. Park, J. W. Kim, and G. Yoon, Noninvasive total hemoglobin measurement. Journal Of Biomedical Optics 7(1), 45–50 (2002). [21] T. K. Aldrich, M. Moosikasuwan, S. D. Shah, and K. S. Deshpande, Length-normalized pulse photoplethysmography: A noninvasive method to measure blood hemoglobin. Annals Of Biomedical Engineering 30(10), 1291–1298 (2002). [22] Y. Kinoshita, T. Yamane, T. Takubo, H. Kanashima, T. Kamitani, N. Tatsumi, and M. Hino, Measurement of hemoglobin concentrations using the astrim (tm) noninvasive blood vessel monitoring apparatus. Acta Haematologica 108(2), 109–110 (2002). [23] D. Gravenstein, S. Lampotang, N. Gravenstein, and M. Brooks, Noninvasive hemoglobinometry. Anesthesiology 81(3A), A576–A576 (1994). Suppl. S. [24] G. Yoon, S. J. Kim, and K. J. Jeon, Robust design of finger probe in non-invasive total haemoglobin monitor. MEDICAL & BIOLOGICAL ENGINEERING & COMPUTING 43(1), 121–125 JAN (2005). [25] R. R. Steuer, D. H. Harris, R. L. Weiss, M. C. Biddulph, and J. M. Conis, Evaluation of a noninvasive hematocrit monitor: A new technology. American Clinical Laboratory 10(6), 20–22 (1991). [26] A. Berrebi and I. Fine, Non-invasive measurement of hemoglobin/hematocrit over a wide clinical range using a new optical signal processing method. Blood 94(10), 10B–10B (1999). Part 2 Suppl. 1. [27] D. Geva, B. Z. Sklar, E. Menashkin, and I. Fine, New approach in non-invasive measurement of hb/hct/ sp0(2). Anesthesiology 93(3A), U154–U154 (2000). [28] L. D. Shvartsman and I. Fine, Optical transmission of blood: Effect of erythrocyte aggregation. Ieee Transactions On Biomedical Engineering 50(8), 1026–1033 (2003). [29] K. Saigo, S. Imoto, M. Hashimoto, H. Mito, J. Moriya, T. Chinzei, Y. Kubota, S. Numada, T. Ozawa, and S. Kumagai, Noninvasive monitoring of hemoglobin – the effects of wbc counts on measurement. American Journal of Clinical Pathology 121(1), 51–55 (2004). [30] J. W. Winkelman, Noninvasive blood bell measurements by imaging of the microcirculation. American Journal of Clinical Pathology 113(4), 479–483 (2000). [31] O. Genzel-Boroviczeny, A. G. Harris, G. D. Fletcher, and F. Christ, Non invasive determination of hemoglobin in neonates with orthogonal polarization spectral (ops) imaging. Pediatric Research 47(4), 332A– 332A (2000). Part 2 Suppl. S. www.biophotonics-journal.org 287 [32] W. Groner, J. W. Winkelman, A. G. Harris, C. Ince, G. J. Bouma, K. Messmer, and R. G. Nadeau, Orthogonal polarization spectral imaging: A new method for study of the microcirculation. Nature Medicine 5(10), 1209–1213 (1999). [33] M. J. Rice, R. H. Sweat, Jr., J. M. Rioux, W. T. Williams, and W. Routt, Non-invasive measurement of blood components using retinal imaging, 2002. [34] J. W. Winkelman. Apparatus and method for in vivo analysis of red and white blood cells, 1991. [35] R. Leitgeb, C. K. Hitzenberger, and A. F. Fercher, Performance of fourier domain vs. time domain optical coherence tomography. Optics Express 11(8), 889–894 (2003). [36] N. V. Iftimia, D. X. Hammer, C. E. Bigelow, D. I. Rosen, T. Ustun, A. A. Ferrante, D. Vu, and R. D. Ferguson, Toward noninvasive measurement of blood hematocrit using spectral domain low coherence interferometry and retinal tracking. Optics Express 14(8), 3377–3388 (2006). [37] X. M. Wu, S. Yeh, T. W. Jeng, and O. S. Khalil, Noninvasive determination of hemoglobin and hematocrit using a temperature-controlled localized reflectance tissue photometer. Analytical Biochemistry 287(2), 284–293 (2000). [38] O. S. Khalil, S. Yeh, M. G. Lowery, X. Wu, C. F. Hanna, S. Kantor, T. W. Jeng, J. S. Kanger, R. A. Bolt, and F. F. de Mul, Temperature modulation of the visible and near infrared absorption and scattering coefficients of human skin. Journal of Biomedical Optics 8(2), 191–205 (2003). [39] B. R. Soller, M. Cabrera, S. M. Smith, and J. P. Sutton, Smart medical systems with application to nutrition and fitness in space. Nutrition 18(10), 930–936 (2002). [40] B. R. Soller, S. Zhang, S. Kaur, S. O. Heard, C. Gaca, M. J. Rohrer, B. S. Cutler, and T. J. V. Salm, Application of near infrared spectroscopy for the noninvasive measurement of hematocrit on surgical patients. Critical Care Medicine 27(12), A144–A144 (1999). Suppl. S. [41] B. R. Soller, N. Cingo, J. C. Puyana, T. Khan, C. Hsi, H. Kim, J. Favreau, and S. O. Heard, Simultaneous measurement of hepatic tissue ph, venous oxygen saturation and hemoglobin by near infrared spectroscopy. Shock 15(2), 106–111 (2001). [42] J. W. McMurdy, G. D. Jay, S. Suner, F. M. Trespalacios, and G. P. Crawford, Diffuse reflectance spectra of the palpebral conjunctiva and its utility as a noninvasive indicator of total hemoglobin. Journal of Biomedical Optics 11(1), 014–019 (2006). [43] G. D. Jay, J. Racht, J. W. McMurdy, Z. Mathews, A. Hughes, S. Suner, and G. P . Crawford, Point-ofcare noninvasive hemoglobin determination using fiber optic reflectance spectroscopy. Proceedings of IEEE: Engineering in Medicine and Biology Society 1, 2932–5, 2007. [44] O. L. Hung, N. S. Kwon, A. E. Cole, G. R. Dacpano, T. Wu, W. K. Chiang, and L. R. Goldfrank, Evaluation of the physician’s ability to recognize the presence or absence of anemia, fever, and jaundice. Academic Emergency Medicine 7(2), 146–156 (2000). # 2009 by WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim
 0
0
advertisement
Related documents




Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users