• Cardiovascular Embryology
advertisement

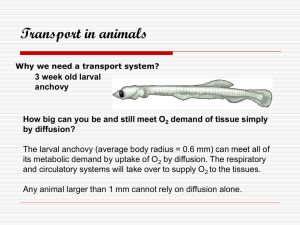
• Cardiovascular Embryology – Describe cardiovascular embryology – Discuss aspects of cardiovascular embryology with pathologic consequence HUMAN EMBRYO: WEEK 3 • Woodburne RT and Burkel W. Essentials of Human Anatomy. Oxford Press 1994 • Cardiogenic mesoderm forms the primitive heart tube with endocardium at approximately 3 weeks • The myocardium and epicardium develop from mesoderm surrounding the primitive heart tube • Hematopoiesis begins in the yolk sac wall about the third week of development • Erythrocytes produced in the yolk sac have nuclei • Blood formation does not begin inside the embryo until fifth week • Angiogenesis starts at the beginning of the third week • Blood vessels first start to develop in the extraembryonic mesoderm of the yolk sac, connecting stalk and chorion • Blood vessels develop in the embryo about two days later VENOUS-ARTERIAL CELL TYPE DIFFERENTIATION • • • • • • As in humans, angioblast precursors reside in the mesoderm in zebrafish Increased expression of gridlock (grl), an artery-restricted gene, ablates arteries and leads to development of veins and expression of venous marker EphB4 receptor (ephb4) Decreased creased notch signalling also leads to increased grl and venous development “notch-grl pathway controls assembly of the first embryonic artery, apparently by adjudicating an arterial versus venous cell fate decision” ZhongTP et al. Nature. 2001 Nov 8;414(6860):216-20 EMBRYONIC CIRCULATION • J. Villenue, MD, McGill http://sprojects.mmi.mcgill.ca/embryology/cvs/ VENOUS EMBRYOLOGY VENOUS EMBRYOLOGY • Infrahepatic IVC develops between the 6th and 8th weeks • Requires partial regression of three paired embryonic veins: the posterior cardinal, the subcardinal and the supracardinal veins • A left IVC results from regression of the right supracardinal vein with persistence of the left supracardinal vein. The prevalence is 0.2%–0.5% • http://radiographics.rsnajnls.org/cgi/co ntent/full/20/3/639 • Right anterior cardinal vein: superior vena cava • Right common cardinal vein superior vena cava • Right posterior cardinal vein azygous vein • Right anterior cardinal vein: left brachiocephalic vein • Left horn of sinus venosus: coronary sinus • Superior vena cava anomalies (including double superior vena cava and left-sided superior vena cava). • Inferior vena cava anomalies (including transposition or left-sided inferior vena cava, retroaortic left renal vein, circumaortic left renal vein, retrocaval ureter and absent suprarenal inferior vena cava). • radiopaedia.org/.../703/IVC_left_thumb.jpg VASCULAR MALFORMATIONS • Mulliken JB, Glowaki J Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 69:412--422, 1982 • Vascular malformations: congenital lesions with normal endothelial turnover • Hemangiomas: neoplastic lesions with endothelial hyperplasia Vascular Malformations • Klippel-Trenaunay syndrome is characterized by a triad of port-wine stain, varicose veins, and bony and soft tissue hypertrophy involving an extremity • Predisposition to thrombophlebitis and thrombotic events in as many as 25% of patients ARTERIAL EMBRYOLOGY • Six pairs of pharyngeal arches develop from 6-8 weeks – 1 and 2nd arches involute – 3rd: common and internal carotid arteries – 4th: L aortic arch; R subclavian a – 5th: no derivatives – 6th: pulmonary arteries and ductus arteriosus Diagrams showing transformation of the early aortic arch pattern (6–8 weeks) into the adult pattern. Moore KL. The developing human: clinically orientated embryology WB Saunders Company, 1982. DOUBLE AORTIC ARCH • Is a vascular web encircling the trachea and esophagus • Occurs due to persistence of part of the 6th pharyngeal arch • Band 22q11 deletion is common as are associated abnormalities including TOF • Treatment requires thoracotomy and division of the minor arch http://www.emedicine.com/ped/topic2541.htm#Multimediamedia1 DOUBLE AORTIC ARCH DSYPHAGIA LUSORIA: Retroesophageal right subclacvian artery • Congenital extremity arterial anomalies: – persistent sciatic artery – popliteal entrapment syndrome PERSISTENT SCIATIC ARTERY • Is an artery that usually regresses during development of fetal circulation • Incidence: 0.02% • Can present as a gluteal mass and is prone to aneurysmal degeneration and emboli • Originates from an internal iliac and travels posterior to the femoral head Persistent Sciatic Artery • Classified as complete: in continuity from the internal iliac artery to the popliteal artery) with varying degrees of superficial femoral artery development • Incomplete interrupted superiorly at the internal iliac artery or inferiorly at the popliteal artery with an intact superficial femoral artery • home.flash.net/~drrad/tf/090197.htm Popliteal Entrapment Syndrome • Conclusions: • Complex and partially understood mechanisms determine the embryology of the cardiovascular system • Additional understanding of these mechanisms will improve our ability to treat or avert the clinical consequences of embryologic derangements in the cardiovascular system