File - Hannah Atwell
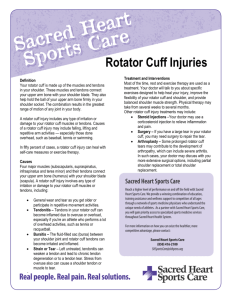
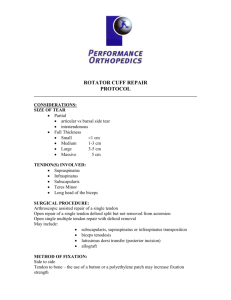
advertisement

Atwell 1 Hannah Atwell Prof Bertie KINE 232 November 18, 2014 Epidemiology 1. A rotator cuff tear is a tear of one or more of the tendons of the four rotator cuff muscles of the shoulder. A rotator cuff injury can include any type of irritation or overuse of those muscles or tendons and is among the most common conditions affecting the shoulder. A torn rotator cuff has four grades of classification. Grade 1 is tear >1 cm after debridement, grade 2 is tear 1-3 cm after debridement, grade 3 is <5 cm, and grade 4 is global tear, no cuff left. 2. Tendinosis, partial and full thickness tears of the rotator cuff are common, especially as people get older. The supraspinatus tendon is most often involved, followed by the infraspinatus and Subscapularis tendons. The teres minor is rarely abnormal, and when it is torn, it is often related to posterior shoulder instability. Rotator cuff defects can be seen in 30% of asymptomatic persons over the age of 60 years (1) and 65% of asymptomatic persons over 70 years of age (2). Tears can be seen in professional throwing athletes without any pain or decrease in performance (3). Many tears do not interfere with normal shoulder activity (4). Yet, there are many symptomatic patients with rotator cuff tears who benefit from therapeutic intervention by arthroscopic or open repair. 3. The prevalence of rotator cuff disease increases with age, with 4% of asymptomatic patients aged less than 40 years and 54% of patients aged 60 years and over, having partial or complete tears of the rotator cuff on magnetic resonance scanning. Ultrasound scanning has demonstrated that 13% of the population in the fifth decade, 20% in the sixth decade and 31% in the seventh decade of life have a rotator cuff tear. More than half of asymptomatic rotator cuff tears become symptomatic within 3 years and progressed in size during this time period. 4. Degenerative rotator cuff tears tend to occur in older patients (50 and over) and often have no history of trauma, presenting with progressive shoulder pain and/or dysfunction. As people age, the muscle and tendon tissues of the rotator cuff lose some elasticity. When muscles and tendons become less elastic, their ability to stretch is reduced, and they become more susceptible to tears. 5. Lifting heavy loads, repetitive movements in awkward positions, and vibrations influence the level of symptoms and disability. Repeating the same shoulder motions again and again can stress your rotator cuff muscles and tendons. Baseball, tennis, rowing, and weightlifting are examples of sports activities that can put you at risk for overuse tears. Many jobs and routine chores can cause overuse tears, as well. As we get older, the blood supply in our rotator cuff Atwell 2 tendons lessens. Without a good blood supply, the body's natural ability to repair tendon damage is impaired. This can ultimately lead to a tendon tear. As we age, bone spurs (bone overgrowth) often develop on the underside of the acromion bone. When we lift our arms, the spurs rub on the rotator cuff tendon. This condition is called shoulder impingement, and over time will weaken the tendon and make it more likely to tear. 6. Patients with possible rotator cuff tears commonly present with complaints of shoulder pain, stiffness, weakness, or loss of active motion. Pain that is characteristic of rotator cuff tears is more intense at night and with overhead activities. Partial-thickness tears are often more painful than full-thickness tears. Tearing of the rotator cuff also include the loss of active or passive range of motion, painful range of motion, presence of muscle atrophy, weakness, swelling, or tenderness. 7. A physical examination by a doctor may be done on the patient. The doctor will assess range of motion and pain tolerance of the patient. Tests that may be done in order to diagnose the injury are an MRI, ultrasound and x-rays. 8. Nonsurgical treatment includes rest, activity modification, non-steroidal anti-inflammatory medication, strengthening exercises and physical therapy and steroid injection. Nonsurgical treatment helps avoid infection, permanent stiffness, anesthesia complications and a nonlengthy recovery time. If pain does not subside with the nonsurgical treatment then the doctor will suggest surgery to fix the rotator cuff tear. 9. One possible way of preventing a torn rotator cuff is to strengthen it through exercise or conduct everyday shoulder stretches to keep the elasticity of the shoulder making it harder to tear. Avoid lifting objects that are too heavy for you, especially lifting over the head. Avoid sports involving forceful contact or falls. Things as simple as overuse of the rotator cuff may cause a tear. 10. These prevention strategies are effective because the elasticity and strength of the shoulder are in good condition. Also avoiding lifting objects too heavy help prevent strain on the rotator cuff causing no stress to cause a tear. Avoiding contact sports is an effective way because you are less at risk of tearing the rotator cuff. The cost effectiveness is not being able to play contact sports in order to prevent a tear. 11. There are not specific tools that can be used besides an MRI, ultrasound, or x-ray. MRI’s correctly depict 95% of full thickness tears and 85% of partial thickness tears. Ultrasounds have good sensitivity and specificity for partial and full thickness rotator cuff tears. The diagnostic test accuracy of ultrasound is superior for the detection of full-thickness compared to partialthickness cuff tears. X-rays are able to detect rotator cuff tears but are not as accurate as an MRI or an ultrasound mainly because X-rays are meant for bones rather than muscles and tendons. Atwell 3 12. Depending on how severe the tear of the rotator cuff is determines of the athlete can engage in athletics or not. If the tear is only a partial tear and needs nonsurgical treatment, then the athlete should be able to engage in any sport they wish after they strengthen the tear a little bit. But, if the tear is sever and is a full tear and the treatment needed is surgery, then the athlete can play in any sport because the tear cannot get any worse and they can just receive surgery later. The athlete will just have to take medication for the pain or receive a cortisone shot until they decide to have surgery to fix the torn rotator cuff. 13. The health care provider should assess how it happened, the symptoms, if the athlete has had this type of injury before or if it is new, and the history of the injury. The restrictions to participation depend on the severity of the injury. There most likely will be restrictions because of the area of injury. The shoulder is used for many things and the athlete should recover and strengthen the shoulder before returning to play and participating. 14. Sports that an athlete with a torn rotator cuff should not participate in are baseball, tennis, weightlifting, and rowing. This is because the use of the rotator cuff in these sports is prominent and necessary and it would only cause the athlete pain or even a bigger tear. Atwell 4 References Ainsworth, Roberta, and Jeremy Lewis. "Exercise Therapy for the Conservative Management of Full Thickness Tears of the Rotator Cuff: A Systematic Review." British Journal of Sports Medicine 41.4 (2007). Print. Atkinson, Mary. "Rotator Cuff Tears." Orthopedic Nursing 29.5 (2010): 319-22. Print. Clement et al.: Management of degenerative rotator cuff tears: a review and treatment strategy. Sports Medicine, Arthroscopy, Rehabilitation, Therapy & Technology 2012 4:48. Forster, Bruce. "Rotator Cuff Troublemakers." Open Access Journal of Sports Medicine 1.9 (2009). Print. Papalia, Rocco. "Shoulder Stiffness and Rotator Cuff Repair." British Medical Bulletin10.1093 (2012). Print. "Rotator Cuff Tears." OrthoInfo. American Academy of Orthopedic Surgeons, 1 May 2011. Web. 1 Nov. 2014. "Treatment Options for Rotator Cuff Tears." Agency for Healthcare Research and Quality. U.S. Department for Health and Human Services, 29 Oct. 2010. Web. 1 Nov. 2014.